Dacryocystocele in Utero: a case report with post-natal histopathological analysis
4
Orbit 0167-6830/97/US$ 12.00 Dacryocystocele In Utero: a case report with post-natal histopathological analysis Orbit-1997, Vol. 16, No. 2. pp. 119-122 0 Eolus Press Buren (The Netherlands) I997 Accepted 20 November 1996 Bruno Fayet Michael Assouline’ Marc Althusser’ Jean-Antoine Bernard Department of Ophthalmology, H8tel-Dieu de Paris, University of Paris VI and *the “Charles Tartrat” Echography Center, Grenoble, France Abstract The authors report a case of dacryocystocele (DCC) diagnosed in utero by ultrasound imaging. Postnatal examination, performed immedi- ately after delivery by cesarean section, revealed a blueish subcutaneous cyst in the medial canthus. This DCC persisted until the 14th day of life, when a superinfection of the cyst, noted at day I I, required the surgical resection of the wall of the intranasopharyngeal cystic expansion. The procedure achieved a complete drainage of the pus and a permanent resolution of the DCC. Histopathological analysis of the resected cyst wall revealed a non- specific nasal mucosa with mild inflammatory infiltrate. These findings con- firm the identity between a prenatal dilation of the lacrimal duct and a true postnatal DCC with a documented intranasopharyngeal cystic expansion. This observation further supports the prevailing theory of a prenatal func- tional “trapdoor” blockage of Rosenmuller’ s valve in the pathogenesis of DCC. Key words phy; intrauterine diagnosis cyst; lacrimal drainage; dacryocele; mucocele; ultrasonogra- Introduction Dacryocystocele (DCC), also known as amniocele, am- niotocele, congenital mucocele, dacryocele or congenital nasolacrimal drain- age system cyst, is a neonatal dilation of the lacrimal sac which may repre- sent up to I .5% of lacrimal disorders in children. This condition is usually diagnosed clinically during the first days of life as a blueish cystic mass in the medial canthus. The cyst is filled with amniotic fluid, suggesting that DCC may arise in utero. ’ In addition, the relationship between early postna- tal DCC and prenatal dilation of the lacrimal sac was suggested by previous reports of three cases, using the newest ultrasound imaging technology in utero.2’3 However, one child had no detectable abnormality at birth and in none of these cases was the presence of a specific intranasopharyngeal cystic expansion reported, malung it difficult to positively link the dilation of the sac in utero and the presumed DCC. We were able to ascertain this relation- Correspondence and reprint requests to : Bruno Fayet, MD Dept. Ophthalmology HBtel-Dieu de Paris I place du Parvis Netre-Dame 75 I 8 I PARIS Cedex 04 France Tel. +33-1-4234 8372 Fax. +33- 1-4634 5364 Acknowtedgements: The authors would like to express their thanks to the Merck-Sharp- Dohme and Chibret documentation center for ophthalmology (CDO- Chibret, Clermont Ferrand), to Mrs. Anne Peterschmidt, Dr. Severin Doumerc and Dr. Jean Michel Basset for their assistance in the evaluation and management of the case, to Prof. Jean Paul Adenis for reviewing the manuscript and to Dr. Jacqueline Zago for her expertise in the histopathological analysis of the sample. Dacryocystocele in utero 119 Orbit Downloaded from informahealthcare.com by University of Miami on 11/24/14 For personal use only.
-
Upload
jean-antoine -
Category
Documents
-
view
221 -
download
2
Transcript of Dacryocystocele in Utero: a case report with post-natal histopathological analysis

Orbit 0167-6830/97/US$ 12.00 Dacryocystocele In Utero: a case report with post-natal histopathological analysis
Orbit-1997, Vol. 16, No. 2.
pp. 119-122
0 Eolus Press Buren (The Netherlands) I997
Accepted 20 November 1996
Bruno Fayet Michael Assouline’
Marc Althusser’ Jean-Antoine Bernard
Department of Ophthalmology, H8tel-Dieu de Paris, University of Paris VI and *the “Charles Tartrat” Echography Center, Grenoble,
France
Abstract The authors report a case of dacryocystocele (DCC) diagnosed in utero by ultrasound imaging. Postnatal examination, performed immedi- ately after delivery by cesarean section, revealed a blueish subcutaneous cyst in the medial canthus. This DCC persisted until the 14th day of life, when a superinfection of the cyst, noted at day I I , required the surgical resection of the wall of the intranasopharyngeal cystic expansion. The procedure achieved a complete drainage of the pus and a permanent resolution of the DCC. Histopathological analysis of the resected cyst wall revealed a non- specific nasal mucosa with mild inflammatory infiltrate. These findings con- firm the identity between a prenatal dilation of the lacrimal duct and a true postnatal DCC with a documented intranasopharyngeal cystic expansion. This observation further supports the prevailing theory of a prenatal func- tional “trapdoor” blockage of Rosenmuller’ s valve in the pathogenesis of DCC.
Key words phy; intrauterine diagnosis
cyst; lacrimal drainage; dacryocele; mucocele; ultrasonogra-
Introduction Dacryocystocele (DCC), also known as amniocele, am- niotocele, congenital mucocele, dacryocele or congenital nasolacrimal drain- age system cyst, is a neonatal dilation of the lacrimal sac which may repre- sent up to I .5% of lacrimal disorders in children. This condition is usually diagnosed clinically during the first days of life as a blueish cystic mass in the medial canthus. The cyst is filled with amniotic fluid, suggesting that DCC may arise in utero. ’ In addition, the relationship between early postna- tal DCC and prenatal dilation of the lacrimal sac was suggested by previous reports of three cases, using the newest ultrasound imaging technology in utero.2’3 However, one child had no detectable abnormality at birth and in none of these cases was the presence of a specific intranasopharyngeal cystic expansion reported, malung it difficult to positively link the dilation of the sac in utero and the presumed DCC. We were able to ascertain this relation-
Correspondence and reprint requests to : Bruno Fayet, MD Dept. Ophthalmology HBtel-Dieu de Paris I place du Parvis Netre-Dame 75 I 8 I PARIS Cedex 04 France Tel. +33-1-4234 8372 Fax. +33- 1-4634 5364
Acknowtedgements: The authors would like to express their thanks to the Merck-Sharp- Dohme and Chibret documentation center for ophthalmology (CDO- Chibret, Clermont Ferrand), to Mrs. Anne Peterschmidt, Dr. Severin Doumerc and Dr. Jean Michel Basset for their assistance in the evaluation and management of the case, to Prof. Jean Paul Adenis for reviewing the manuscript and to Dr. Jacqueline Zago for her expertise in the histopathological analysis of the sample.
Dacryocystocele in utero 119
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mia
mi o
n 11
/24/
14Fo
r pe
rson
al u
se o
nly.

ship in a case of indisputable DCC, documented both in utero by ultrasound imaging and at birth by rhinoscopy and therapeutic excision-biopsy of the infected intranasopharyngeal cystic expansion.
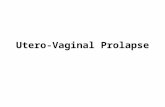
Case report Gabrielle T. was born at term of a primary pregnancy, by means of a ce- sarean section, from a 30 year-old Caucasian mother. Repeated ultrasound imaging of the fetus was performed at 12, 16,20, 25, 31 and $3 weeks of pregnancy, using an Aloka 2000 device with curved 3.5 and 5 MHz probes. At 3 I weeks, a dilated cyst, 7 mni in diameter, was noted in the left medial canthus region (Fig.1). A bulging of the left canthal region, with a normally colored overlying skin, was noted at birth by the parents, both of them being physicians. A presumed superinfection of this cyst was observed at day I I and was treated by antibiotic eyedrops before the child was referred to us. We noted a cystic dilation of the left canthal re- gion with blueish coloration of the adjacent skin. A suspected DCC was confirmed by rhinoscopic examination at day I 2 which revealed a dilated cyst under the inferior turbinate, obstructing the inferior meatus. There was no respiratory impairment from this unilateral DCC, nor any detect- able systemic consequence of the infection. The mucosal wall of the cyst was very similar to the nasal mucosa. The cyst could be enlarged by gen- tle external pressure on the lacrimal sac. Given the accuracy of the ultra- sound and clinical findings, a CT scan was not indicated. At day 13 the infection caused inflammatory changes in the skin.The nasal cyst was ex- cised with simple sedation under the surgical microscope at day I 4. This resulted in the drainage of a large amount of pus (containing numerous coagulase-negative staphylococci), which was further completed by exter- nal pressure on the canthal region. No recurrence of the cyst nor any epiphora could be observed up to I 8 months postoperatively.
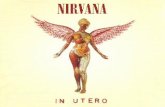
Histopathological analysis of the nasal wall of the cyst was performed, revealing a mucosal aspect most suggestive of nasal mucosal epithelium (Fig. 2).
Fig. I . Ultrasound imaging of a dacryocystocele in utei-0, performed at 31 weeks of pregnancy. A cyst, 7 mm in diameter, is observed in the left canthal region, underlying the skin and lateral to the bony medial wall of the orbit. The wall of this cyst is thin and regular. The content of the cyst is devoid of any echogenic structures. The examination does not reveal any abnormality of the face, nor any abnormal vascular structures in the nasoorbital region.
I 2 0 Bruno Fayet et al.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mia
mi o
n 11
/24/
14Fo
r pe
rson
al u
se o
nly.

Fig. 2. Histopathological analysis of the resected mucosa. A flattened epithelium overlying a highly vascularized connective tissue containing seromucous glands is observed. Rare mononucleated inflammatory cells are present (Hematoxylin-Eosin stain, original magnification 20ox).
Comments The distinction between dacryocystocele (DCC) and simple lacrimo-nasal impatency with a mucocele (LNI) has been clearly estab- lished,’ although some confusion still remains in the recent literature.*I1 In addition to the obstruction at the level of Hasner’s membrane observed in LNI, a partial bloc of Rosenmuller’s valve is also present in DCC. Rosen- muller’s valve may be functionally continent in DCC, thus preventing the normal reflux of amniotic fluid from the lacrimal sac to the canaliculi in utero. Further distension of the lacrimal sac may augment this functional blockage of the canaliculi by means of a trapdoor effect, causing a progres- sive bulge of Hasner’s membrane in the nasal fossa, under the inferior turbi- nate. This intranasopharyngeal cystic expansion can be considered a specific postnatal criterion for DCC since it was never observed in association with simple LNI. However, a rhinoscopy was not systematically performed in most of the recent reports on DCC.’ Using simple direct rhinoscopy, we have observed an intranasopharyngeal cystic expansion in all cases from a personal series of 8 DCC (unpublished data), a fact further supported by computerized tomodensitometry and magnetic resonance imaging tech- niques applied to infants with DCC4
Spontaneous resolution of DCC is generally observed during the first days of life and the current management of DCC is limited to simple observation, since probing may augment recurrences. However, in 30% of cases, DCC may result in infection of the lacrimal sac, presenting as an acute dacryocys- titis. Bilateral intrdnasopharyngeal cystic expansions may cause respiratory distress by obstructing the choanes, masquerading as choanal atresia. In case of complicated intranasopharyngeal cystic expansions associated with subse- quent infection of the sac or respiratory distress, most authors recommend the surgical opening of the dilated lacrimal sac from a nasal or canthal ap- proach. This proved very effective in the present case. Since 1987, only 4 cases of DCC in utero have been reported, a very small figure, given the now mandatory prenatal ultrasound imaging of the face in most developed countries. According to available reports, including the present observation, DCC may not form at an earlier stage than the 30th week of pregnan~y.’.~ DCC may therefore not be detected at the last ultrasound examination re-
Dacryocystocele in utero I 2 1
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mia
mi o
n 11
/24/
14Fo
r pe
rson
al u
se o
nly.

quired by a normal follow-up, usually performed at 3 I weeks. Histopatho- logical examination of a congenital DCC diagnosed in utero has never been reported, given the spontaneous resolution of the few reported cases.*J The pathological analysis performed in the present case was consistent with pre- viously reported findings in postnatal DCC.
This observation clearly demonstrates that a true DCC with documented intranasopharyngeal cystic expansion observed at birth, had arisen in utero. This finding supports the prevailing theory according to which a functional trapdoor blockage of Rosenmuller’s valve may be the primary mechanism for the development of a DCC.
References I Mansour AM, Cheng KP, Muma JV,
Stager DR, et al. Congenital dacryo- cele: a collaborative review. Ophthal- mology 1991;98( I I ) : 1744-5 I .
2 Davis WK, Mahony BS, Carrol BA, Bowie JD. Antenatal sonographic detection of benign dacryocystocde.
J Ultrasound Med 1987;6:461-5. 3 Schaub B, Sainte-Rose D. Dacryo-
cystodle: diagnostic antCnatal Ccho- graphique. J Gynecol Obstet Biol Reprod 1992;21:82-4.
4 Boyton JR, Drucker DN. Distension of the lacrimal sac in the neonates. Ophthalm Surg 1989;20:103-7.
I22 Bruno Fayet et al.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Mia
mi o
n 11
/24/
14Fo
r pe
rson
al u
se o
nly.