The Embryology of the Telencephalic Fibre Systems in the Mouse

Journal of Neurology, Neurosurgery, and Psychiatry, 1975, 38, 265-271
Cystic degeneration of the telencephalic subependymalgerminal layer in newborn infants
GUILLERMO A. DE LEON AND DAVID J. GIRLING
From the Department of Neuropathology, Institute ofPsychiatry,and The Nuffield Neonatal Research Unit, Institute of Child Health,
The Hammersmith Hospital, London
SYNOPSIS Cystic lesions were found in the telencephalic germinal layer of 12 newborn babies.According to their location, the cysts could be divided into three groups: anterior, middle orthalamostriate, and posterior. The histological appearance of all cysts was essentially the same, butin three cases the germinal layer had a peculiar alveolar type of microcystic degeneration. A constantfeature was the presence in the cyst wall of small white granulations composed of germinal cellsand/or glial tissue. Cystic degeneration of the germinal layer was usually bilateral and sometimesquite extensive. After the involution of the germinal layer, these lesions are likely to persist assubependymal cysts, characterized by their specific location and the presence of glial granulations.
It is the purpose of this paper to describe cysticlesions of the telencephalic subependymalgerminal layer in newborn infants. Brief refer-ence to subependymal or germinal layer cystshas been made by a number of authors but someof the histological characteristics of such lesionsare yet to be defined. The telencephalic germinallayer plays an important role in neonatal neuro-pathology. Bleeding into this structure is prob-ably the single most common abnormality foundin brains of premature babies. However, ourknowledge about the anatomy, physiology, andpathology of this layer is very limited. Therefore,it seems desirable to bring up for discussion oneof the few recognizable morbid changes otherthan haemorrhage affecting this structure.
During the second half of gestation, thetelencephalic subependymal germinal layer is aperiventricular, densely cellular, multistratifiedlayer of undifferentiated cells, which is separatedfrom the ventricle only by the unicellular laminaof the definitive ependyma. The thickness of thegerminal layer is characteristically greater overthe ventricular aspects of the striatum. Due to
Reprints requests: Dr G. A. de Le6n, Division of Neuropathology,Department of Pathology, Temple University Health SciencesCenter, 3400 North Broad Street, Philadelphia, Pennsylvania 19140,U.S.A.(Accepted 3 September 1974.)
265
migration of its cells, the layer gradually dis-appears with advancing fetal age.
METHODS
Included in this investigation were 10 newbornbabies in whom cystic lesions were found macro-scopically in the telencephalic germinal layer. Intwo additional cases, the diagnosis of germinal layercysts was made histologically. The brains were fixedin 10°/ formalin/saline solution. Blocks were takenfrom all cysts as well as from associated lesions andother representative areas of the central nervoussystem, and embedded in paraffin, sectioned andstained with the usual neuropathological techniques.The pertinent clinical data of all cases are includedin Table 1.
RESULTS
MACROSCOPIC FINDINGS For convenience ofdescription, the cysts can be divided into threegroups according to their location in thegerminal layer: anterior, middle or thalamo-striate, and posterior cysts. The distribution ofcysts in the different cases as well as the associ-ated pathological findings are summarized inTable 2.
Anterior germinal layer cysts were present in
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

Guillermo A. de Leon and David J. Girlinv
if,i.'.,,1i/ '
:i
I."
1f eV
.fi;
/
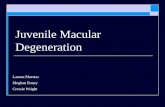
FIG. 1 Case 9. Coronal sections of right cerebralhemisphere, just anterior to the level oftheforamen ofMonro. A germinal layer cyst extends over the headof the caudate nucleus (right). The corpus callosum,the septum, and the fornix are seen on the left side ofthe photograph. The cyst is loculatedby numerous glialsepta. Germinal cell granulations are present (tinydark spots), particularly on the septa. The germinallayer is gliosed. H and E, x 13.
eight babies (cases 1-6, 8, 9), being bilateral insix cases. The cysts were located immediately infront of and/or above the anterior pole of thehead of the caudate nucleus. In coronal sectionsthey varied in size from a small horizontal slit,about 1.5 mm in length, to large cavities measur-ing up to about 10 mm in diameter. Some cystswere loculated by septa. In most cases, variablenumbers of tiny white granulations were presentin the cyst wall. In two cases with neighbouringhaemorrhages (cases 2 and 6), there was evidenceof bleeding into the cysts. In one case withbilateral cysts (case 9), the ependyma overlying
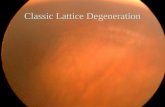
FIG. 2 Case 6. Coronal section through left frontallobe, at the level ofthe anterior pole ofthe head ofthecaudate nucleus. The corpus callosum is seen on theright upper corner, above the narrow lateral angle ofthe ventricular cavity. The caudate nucleus is belowthe cyst. The cystic cavity is loculated by a glialseptum. Numerous germinal cell granulations ofvariable size are seen on the cyst wall. Nissl, x 4.8.
the cysts was torn and there was wide communica-tion between the cysts and the ventricle.
Middle or thalamostriate cysts were found infive babies (cases 7, 9-12), and were bilateral infour of them. Two types of cyst were found atthis level: (1) in cases 11 and 12, the germinallayer, bilaterally, was dark and had a peculiarspongy appearance. Small clusters of tiny cystscould be recognized macroscopically in someareas in case 11. The diagnosis of cystic lesioncould not be made macroscopically in case 12,and was not even suspected in case 10, in whichthe micro-cysts were overshadowed by local
266
I
tN1,
V.
.V
N' .... .
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

Cystic degeneration of the telencephalic subependymal germinal layer in newborn infants
.~~~~~....I
:~ r
or."'
.,.,j~~~~~~~ ~~~~~..E
'22
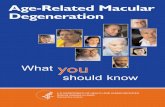
FIG. 3 Case 9. Coronal section of right cerebralhemisphere, rostral to the anterior pole of the head ofthe caudate nucleus. Lined by ependyma, the lateralventricle is seen medial (left) to the cyst, which hasapparently expanded into the periventricular whitematter, beyond the limits of the gliosed germinallayer. There are a few glial granulations on the cystwall. At a more posterior level this cyst was in com-munication with the ventricle (not shown). H and E,x 9.
germinal layer haemorrhages. (2) In the remain-ing two infants (cases 7, 9), the cystic nature ofthe lesions was obvious macroscopically. Theylooked like collapsed tents at the level of theanterior part of the thalamostriate sulcus. Theventricular walls of the cysts were usuallyredundant, suggesting that when distended theywould protrude into the ventricle. The cystsextended to a variable distance along thethalamostriate sulcus, and also had prolonga-tions over the ventricular aspect of the head ofthe caudate nucleus, anterior to the foramen of
FIG. 4 Case 12. Alveolar type of cystic degeneration.Germinal cell granulations of variable size are presenton the walls of every microcyst. Germinal cells, glialtissue, and blood vessels have grown into the lateralventricle (left) through the extensively disruptedependyma, which is seen forming multiple rosettes.Blood vessels are normally cuffed by germinal cells.Nissl, x 45.
Monro. The larger cysts measured up to 2 cm in
length. White granulations were rarely seen
macroscopically in the walls of the thalamo-striate cysts. In case 7, there was unilateralhydrocephalus on the side of the larger thalamo-striate cyst. The foramen of Monro was notsealed with adhesions but the cyst had possiblybeen acting as a valve.A posterior cyst was found in one case only
(case 9), and in this brain there were also bi-lateral anterior cysts, as well as one thalamo-striate cyst on the right side. The posterior cyst
*
.4
:'; !£.-ff a.eb#, o b
e
8,
_ f. .
L s
2&8 i-i. i .S>.
\bSu
a s .wB
t.-#;s ..
ts ;. %..s
A X :- < #r P .
o' ...v . ...g. X . .. . .e s .; --:w
: _w &/ @ ; # * ; .-Si s = ; b-% *A1
<.1
267
i
I
I
I
,:.,N
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

268
Case Sex Age Gestationno. (h) (wk)
1 F 16 28
2 M 62 303 F 13 31
4 M 30 32
5 F 6d 346 M 30 36
7 M 60d 30
8 F 18 39
9 M 10 d ?40
10 F 22 d 30
11 M 2 35
12 F 7d 39
Guillermo A. de Leon and David J. Girling
TABLE 1SUMMARY OF CLINICAL DATA IN PRESENT SERIES OF CASES
Birth Complications of Birth Respiratoryweight asphyxia distress(g) Pregnancy Delivery syndrome
1 300 Rh D Breech Yes YesIUT x 2
1080 APH 0 0 Yes1 625 Rh D CS Yes 0
IUTx2
1610 0 0 0 Yes
2280 Rh D (Induced) 0 02 310 Threatened CS Yes Yes
abortion,placentapraevia
1 640 0 0
2 840 Rh D (Induced)
2250 0 ?
950 0 Breech
2 320 Hydramnios 0
3 500 Hydramnios CS
Apnoeic Other complicationsattacks
Yes DIC
Yes Fits, hypothermiaYes Cardiac arrest, fits,
hypoglycaemia,thypo-thermia
Yes Fits, hypothermia,pneumothorax
Yes Cardiac failure, fitsYes -
0 Yes Yes Cardiac arrest, trachealstenosis, broncho-pneumonia
Yes 0 Yes DIC, fits, hypo-glycaemia
0 0 0 Multiple malformations,bronchopneumonia
Yes 0 Yes Fits, hypothermia,bronchopneumonia
Yes No spontaneous Idiopathic hydrops,respiration pulmonary haemor-
rhageYes 0 0 Multiple malformations,
fits, vomiting
IUT: intrauterine transfusion. APH: antepartum haemorrhage. CS: caesarean section. DIC: disseminated intravascular coagulation. ET:exchange transfusion. Rh D: Rh disease. d: days.
TABLE 2GERMINAL LAYER CYSTS AND ASSOCIATED PATHOLOGICAL FINDINGS IN PRESENT SERIES OF CASES
Case Maudsley Brain Germinal layer cysts GLH* IVHt Multiple Per- Kernic- CNS HMD¶no. no. weight, (R = right, L= left) CNS ventricular terus malforma-
fresh haemor- leuco- tions(g) Ant. Mid. Post. rhagest malacia§
1 5 113 150 R & L 0 0 L Yes Yes 0 0 0 Yes2 5909 140 R & L 0 0 R &L Yes 0 0 0 0 03 5 828 196 R & L 0 0 0 Yes 0 0 0 Yes4 5 523 219 R & L 0 0 R Yes 0 0 0 0 Yes5 6026 283 R & L 0 0 R 0 0 Yes Yes 0 06 5 524 299 L 0 0 R & L Yes 0 Yes 0 0 07 4 505 295 0 R & L 0 L Yes 0 Yes 0 0 08 5 521 390 L 0 0 R Yes Yes 0 0 0 Yes9 5 220 331 R & L R R 0 0 0 Yes 0 Yes 010 6023 173 0 R &L 0 R &L Yes 0 Yes 0 0 011 3 485 315 0 R & L 0 0 Yes 0 0 0 0 012 5 168 388 0 R & L 0 0 0 0 0 0 Yes 0
* Germinal layer haemorrhage. t Intraventricular haemorrhage. t Multiple intracerebellar, leptomeningeal, and intracerebral haemorrhages,often associated with disseminated intravascular coagulation (Chessells and Wigglesworth, 1970). § Coagulation infarcts, usually multiple andmore common in the periventricular region (Banker and Larroche, 1962). ¶1 Hyaline membrane disease.
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

Cystic degeneration of the telencephalic subependymal germinal layer in newborn infants
was larger at the level of the ventricular con-fluence, behind the descending portion of thetail of the caudate nucleus. It extended forwardfor about 0.5 cm above the caudate nucleus andalong the lateral angle of the body of the lateralventricle. There was a tiny perforation on itsventricular wall.
MICROSCOPIC FINDINGS Germinal layer cystswere histologically characterized by the follow-ing features: (1) They were within the germinallayer and sometimes spread extensively throughthis structure. The smaller cysts were containedwithin the normal boundaries of the germinallayer, but the larger cysts tended to bulge intothe ventricle (Fig. 1); some had expanded intothe neighbouring white matter. (2) In cases wherethe germinal layer was relatively well preserved,the walls of the cyst were formed by the paren-chyma of the germinal layer. In cases in whichthis was gliosed or depopulated, the walls wereformed by glial tissue. (3) A feature of allgerminal layer cysts was the presence of smallpolypoid structures corresponding to the whitegranulations described macroscopically. In somecysts these granulations were very numerous,but in others, particularly in the large gliosedlesions, they were rather sparse. Most granula-tions consisted of dense, rounded aggregationsof small, dark germinal cells (germinal cellgranulations) (Fig. 2). In the gliosed, probablyolder cysts, some germinal cell granulations werepartially gliosed, while other granulations wereconiform and consisted of proliferated astro-cytes and glial fibres (glial granulations) (Fig. 3).Some of these contained small nests of germinalcells. Some germinal cell granulations had a rimor core formed by pale eosinophilic matrix.Small PAS-positive areas were seen near thebase of some granulations.Some features of the spongy thalamostriate
lesions in cases 10, 11, and 12, were significantlydifferent. There was no large cavitation as in theother cases, but the area was disrupted by aconglomeration of numerous tiny cysts whichgave the germinal layer an alveolar appearance.The alveoli varied in size and some of the largerones were apparently the result of coalescence ofsmaller cysts. In case 12, the germinal cellgranulations were quite numerous but therewere only one or two in the smaller microcysts.
Some of these cavities were almost filled by thegranulation(s). The germinal layer was moder-ately gliosed and occasional cells were distendedby PAS-positive material. The overlying epen-dyma was extensively disrupted. Germinal cells,glial tissue, and blood vessels had grown throughthe breaks ofcontinuity and proliferated over theventricular wall. The margins of buried frag-ments of ependyma curled up and formedrosettes (Fig. 4). Occasional glial nodules werepresent in the neighbouring caudate nuclei andother areas. Scattered perivascular calcificationwas seen involving the striatal vessels. Nomicro-organisms or inclusion bodies were found.Although germinal layer haemorrhages were
present in eight babies, the cysts were involved byfresh bleeding in only three (cases 2, 6, 10). Incase 6, only a small, loculated, caudal part of thecyst had been involved by an adjacent germinallayer haemorrhage. In case 2, the bleeding intothe anterior germinal layer and the cyst was asmall part of an enormous haemorrhage whichextended from the thalamostriate region to thewhite matter of the anterior frontal lobe.
DISCUSSION
The cystic degeneration of the subependymalgerminal layer described here is frequentlybilateral (10 out of 12 cases) and may be quiteextensive. In case 9, most of the germinal layerhad been replaced on one side by large anterior,middle, and posterior cysts. It seems that onceformed, the cysts tend to increase in size andspread through the germinal layer, whichapparently offers little resistance to expandinglesions. In contrast, the cysts seem incapable oferoding the immediately adjacent basal ganglia.The ganglionic wall of the cysts is characteristic-ally convex and outlines the normal contour ofthe caudatum and thalamus which remain intacteven when the cysts have bulged inside theventricle (thalamostriate cysts) or expanded intothe neighbouring white matter (anterior andposterior cysts).
In general, except for the alveolar type ofcystic degeneration (cases 10, 11, 12), thediagnosis of germinal layer cysts is straight-forward macroscopically. However, the morecommon variety of germinal layer cyst in thisseries, the anterior, may be missed unless a slice
269
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

Guillermo A. de Leon and David J. Girling
is made at about the level of the anterior pole ofthe head of the caudate nucleus. Cysts were notdiagnosed macroscopically in two of the caseswith alveolar microcystic degeneration (cases 10,12), but, in case 12, the germinal layer had apeculiar spongy appearance and so it might bepossible to recognize similar future cases onnaked eye examination.The incidence of germinal layer cysts cannot
be stated at this time. During 1969, germinallayer cysts were found in seven cases (7.7y.) outof a total of 90 examined newborn brains. It ispossible that a higher incidence would be foundby systematic histological examination of thegerminal layer.Germinal cell and/or glial granulations were
present in all the germinal layer cysts of thisseries and probably can be considered to be adistinctive characteristic of these lesions. The co-existence of germinal cell and glial granulationsin the same cyst, as well as the finding of mixedforms (partially gliosed germinal cell granula-tions or glial granulations with nests of germinalcells), strongly suggest that one is the product ofmaturation of the other. From their generalappearance, it seems that the germinal cellgranulations are not surviving islands of a dis-rupted germinal layer but the result of prolifera-tion of germinal cells in contact with the cystcavity. Whether this proliferation is induced bythe chemical composition of the cyst fluid, by thephysical properties of the surface, or by otherfactors is unknown, but similar growths mayoccur in other parts of the infantile centralnervous system in contact with a fluid-filledcavity. Perhaps the more common example ofthis is the supraependymal proliferation ofgerminal cells in areas where there has been adisruption of the ependymal lining.
It is important to differentiate this form ofcystic degeneration of the germinal layer fromother varieties of cystic lesions that can be seenin the periventricular region. Subependymalcysts are seen in the brains of older infants inwhom the germinal layer is no longer present;many are morphologically similar to germinallayer cysts and contain glial granulations. Someof these subependymal cysts are likely to be, infact, gliosed germinal layer cysts in infants sur-viving the neonatal period. Ependymal cysts arecharacterized by their epithelial wall. Post-
necrotic cavitation, the result of infarction and/orhaemorrhage, is not rare in the periventricularregion of older infants, but these lesions are notrestricted to the germinal layer and usually con-tain collections of macrophages full of lipid,pigment or debris. Lesions similar to e'tat cribleare seen in infantile brains but their appearanceis quite different from that of germinal layercysts. There should be no difficulty in differen-tiating germinal layer cysts from intraventricularand choroidal cysts that may be seen in cases ofadhesive ependymitis (Merle, 1910). Periventricu-lar diverticula may occur in older infants second-ary to traumatic tears of the ventricular wall,including those after ventricular needle punc-ture, but these lesions could hardly be confusedwith germinal layer cysts.From the present findings there is no obvious
indication as to the pathogenesis of the germinallayer cysts. Schwartz (1961) briefly describedsubependymal cysts which he considered thesequelae of local haemorrhage. In the presentseries, the apparent incidence of germinal layerhaemorrhage (66%) is higher than in our generalneonatal material (about 50%), but the numberof cases involved is too small (Table 2). In onlythree cases was there evidence of bleeding insidethe cysts, but in all the haemorrhage was recentand the cysts were already well-formed. In mostcases there is no correlation between the site ofthe haemorrhage and the cysts. The majority ofcysts were anterior, while most of the germinallayer haemorrhages originated in the thalamo-striate region.A number of other pathological abnormali-
ties, like periventricular leucomalacia (Bankerand Larroche, 1962), multiple haemorrhagesassociated with disseminated intravascular co-agulation (Chessells and Wigglesworth, 1970),and malformations were present in several of ourcases, but their incidence in this small series wasnot different from that in our general neonatalmaterial. Subependymal or germinal layer cystshave been frequently found in cases of con-genital rubella encephalopathy (Anzil, 1967;Gilles, 1967; Rorke and Spiro, 1967; Stadlanand Sung, 1967; Shaw, 1973), as well as incytomegalovirus disease (Shaw, 1973; person-ally examined case, Maudsley No. 11-57). In therubella cases, as well as in our own micro-polygyric case of cytomegalo-virus disease, the
270
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from

Cystic degeneration of the telencephalic subependymal germinal layer in newborn infants
cysts were located in the thalamostriate regionand there was evidence of widespread vascularinvolvement. Though the possibility of directviral invasion of the germinal layer inducing thecystic change should be considered in cases suchas these, as suggested by Shaw (1973), it is alsoconceivable that some sort of circulatory dis-order could be a common underlying factor inall cases. Similar cysts have also been seen inconditions such as leucoencephalopathy associ-ated with congenital lactic acidosis (Farkas-Bargeton et al., 1971), arrhinencephaly (Shaw,1973; our case 9), pachygyria (Bargeton, 1959),and agyria (unpublished case, Maudsley No.5446). It is possible that cystic degeneration ofthe germinal layer represents a non-specific typeof reaction of this structure to a variety of patho-logical factors.With the exception of blockage to Monro's
foramen by large thalamostriate cysts, such asapparently occurred in case 7, the possibleclinical implications of lesions involving thegerminal layer are uncertain. Little is knownabout the destiny of the cells originating in thetelencephalic subependymal germinal layer dur-ing the second half of gestation. It is generallythought that such cells will mostly generate glialcells. Evidence has been presented by Rakic andSidman (1969) suggesting that part of thepulvinar, a highly developed structure in thehuman brain, may originate from late migratingtelencephalic germinal cells. The possibility ofcerebral hypoplasia (defective myelinization)resulting from devastation of the telencephalicgerminal layer late in gestation was originallysuggested by Patten and Alpers (1933) in cases ofhaemorrhage in that region. It is reasonable tothink that destruction of the subependymalgerminal layer may somehow impair the normaldevelopment of the brain. However, furthercases should be investigated to find out whetheror not cystic degeneration of the germinal layermay occur in the absence of other lesions, such
as were present in our cases. Unless the damageis restricted to the germinal layer, the resultingclinical manifestations cannot be attributed tolesions of that structure.
Dr S. J. Stridh gave valuable advice. The necropsies wereperformed by Dr J. S. Wigglesworth. Miss J. P. Germainand Mr P. Green prepared the histological sections. Weare indebted for the photographs to Mr P. Taylor. Thiswork was supported by a grant from the NuffieldFoundation.
REFERENCES
Anzil, A. (1967). In discussion of paper by Rorke and Spiro.Journal of Neuropathology and Experimental Neurology,26, 116.
Banker, B. Q., and Larroche, J. C. (1962). Periventricularleukomalacia of infancy. A form of neonatal anoxicencephalopathy. Archives of Neurology, 7, 386-410.
Bargeton, E. (1959). Les malformations tardives. In Mal-formations Congenitales du Cerveau, pp. 361-375. Editedby G. Heuyer, M. Feld, and J. Gruner. Masson: Paris.
Chessells, J. M., and Wigglesworth, J. S. (1970). Secondaryhaemorrhagic disease of the newborn. Archives of Diseasesin Childhood, 45, 539-543.
Farkas-Bargeton, E., Goutieres, F., Richardet, J. M.,Thieffry, S., and Brissaud, H. E. (1971). Leucoenc6phalo-pathie familiale associe A une acidose lactique cong6nitale.Acta Neuropathologica (Berl.), 17, 156-168.
Gilles, F. (1967). In discussion of paper by Stadlan and Sung.Journal ofNeuropathology and Experimental Neurology, 26,115.
Merle, P. (1910). ttude sur les tpendymites CUreibrales.Steinheil: Paris.
Patten, C. A., and Alpers, B. J. (1933). Cerebral birth con-ditions with special reference to the factor of hemorrhage.American Journal of Psychiatry, 79, 751-768.
Rakid, P., and Sidman, R. L. (1969). Telencephalic origin ofpulvinar neurons in the fetal human brain. Zeitschrift furAnatomie und Entwicklungsgeschichte, 129, 53-82.
Rorke, L. B., and Spiro, A. J. (1967). Cerebral lesions incongenital rubella syndrome. Journal ofPediatrics, 70, 243-255.
Schwartz, P. (1961). Birth Injuries of the Newborn. Mor-phology, Pathogenesis, Clinical Pathology and Prevention,p. 70. Karger: Basel.
Shaw, Cheng-Mei (1973). Subependymal germinolysis.(Abstract.) Journal of Neuropathology and ExperimentalNeurology, 32, 153.
Stadlan, E. M., and Sung, J. H. (1967). Congenital rubellaencephalopathy. Journal of Neuropathology and Experi-mental Neurology, 26, 115.
271
Protected by copyright.
on April 15, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.38.3.265 on 1 March 1975. D
ownloaded from