Currently Available Methods to Treat Open Angle Glaucoma
123
Adjusting the Faucet or Opening the Drain – Currently Available Methods to Treat the Plumbing Problem of Open Angle Glaucoma
-
Upload
dr-david-richardson -
Category
Health & Medicine
-
view
198 -
download
0
Transcript of Currently Available Methods to Treat Open Angle Glaucoma
Adjusting the Faucet or Opening the Drain –
Currently Available Methods to Treat the Plumbing Problem of Open Angle Glaucoma
Presenter
Presentation Notes
Adjusting the Faucet or Opening the Drain – Currently Available Methods to Treat the Plumbing Problem of Open Angle Glaucoma Introduction Tonight we’ve got two hours of CE, I understand. And I’m not going to talk for the whole two hours, I want to leave some time for Question and Answer. But this is a big topic tonight and the topic is, “Adjusting the Faucet or Opening the Drain.” Basically, what are the current and near future methods of treating glaucoma.
Course Objective
At the end of the presentation audience participants should be familiar with the main benefits and risks of currently available glaucoma treatments as well as have an awareness of the most promising potential future glaucoma treatments.
Presenter
Presentation Notes
Course Objective So by the end of this presentation, besides having a really nice dinner, you should be familiar with the currently available and soon to be available (we hope) methods of treating glaucoma and how they work. So you should be aware of them all and have a pretty good idea of the mechanism.

What is Glaucoma?
Presenter
Presentation Notes
What is Glaucoma? Now this brings up something that’s rather interesting. In order to figure out how to treat it and to talk about mechanisms we first have to discuss, well what is glaucoma? Now, we all have an idea of what it is. It’s got something to do with the optic nerve, it’s a progressive optic neuropathy, and it involves cupping and typical visual field or retinal nerve fiber layer loss. Now, it’s also got something to do with pressure. We know all of those things. <click>

It’s not so simple.
Presenter
Presentation Notes
It’s not so simple But we’re finding out that it’s not so simple. It’s the idea that high pressure is glaucoma so we have to lower it, we figured that out a while ago that it wasn’t that simple (normal tension glaucoma, patients with ocular hypertension but not glaucoma). So clearly there’s something else going on. And what we’re discovering is that blood supply is important, oxidative damage may be important, and there may be some other issues involved such as inflammation. So a lot of the laboratory research that’s being done is actually focusing on those three things, not pressure. But that’s pretty far into the future. Nothing that is involving non-IOP lowering therapy is anywhere near clinical usefulness.

Presenter
Presentation Notes
So we pretty much have to view glaucoma as a problem of plumbing. Even though we know glaucoma is far more complex than flow issues, this is all we’ve got. This is what we have to work with.

Presenter
Presentation Notes
And so given that, what tools do we have available to us? And just like a good plumber if you don’t have the right tools or you don’t know how to use the right tools for the right job you’re not going to be able to fix the faucet.

Adjusting the Faucet
Aqueous Production
Presenter
Presentation Notes
Adjusting the Faucet So we can think about fixing glaucoma or treating glaucoma as fixing the sink. So you’ve got a backed-up sink, what can you do? Well you could potentially just the faucet. So if the water is flowing and the sink is overflowing one thing you can do is simply turn off the faucet. But with glaucoma of course you don’t want to turn off the faucet because if you don’t have any flow then you end up with hypotony and with hypotony you can end up with maculopathy, phthisis—things that you generally don’t want. So we can adjust the flow but we can’t turn it off. Well the problem is that if the drain is stopped up even turning down the flow might not be enough.

Fixing the Drain
Outflow Pathways | Non-physiologic Outflow
Presenter
Presentation Notes
Fixing the Drain So of course then we can look at fixing the drain and if we’re going to fix the drain we have to think about, in terms of glaucoma, the outflow pathways. And there are physiologic pathways—the pathways that are used by everyone’s eye that doesn’t have glaucoma. And then there are the non-physiologic, so basically those that we create.
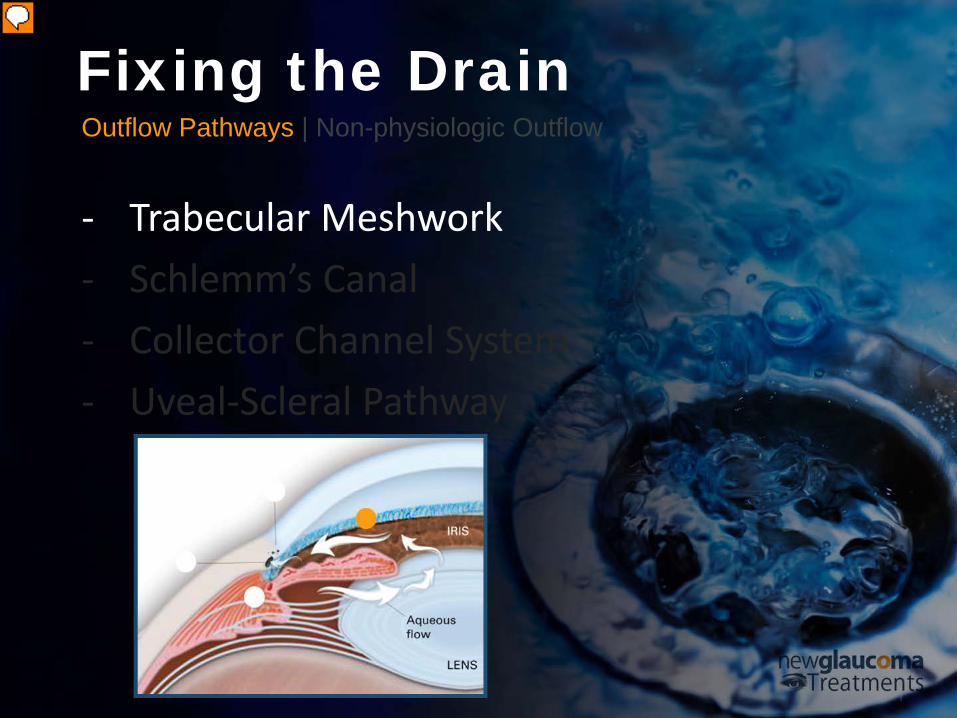
Outflow Pathways | Non-physiologic Outflow
- Trabecular Meshwork - Schlemm’s Canal - Collector Channel System - Uveal-Scleral Pathway
Fixing the Drain
Presenter
Presentation Notes
Physiologic pathways (Outflow Pathways) Now, in terms of the physiologic pathways there’s the trabecular meshwork. Trabecular Meshwork – we can think of is basically the drainage grate here. So that’s the first level at which fluid can come into a resistance.
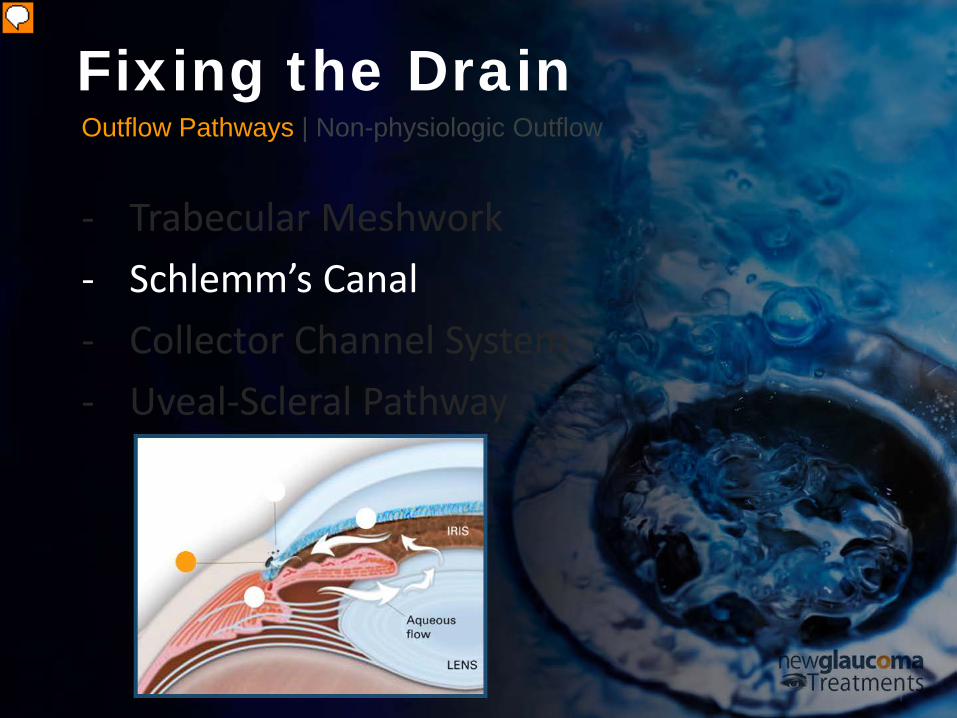
Outflow Pathways | Non-physiologic Outflow
- Trabecular Meshwork - Schlemm’s Canal - Collector Channel System - Uveal-Scleral Pathway
Fixing the Drain
Presenter
Presentation Notes
Behind the grate is the Schlemm’s canal. So this is the canal that encircles the angle, sitting just behind trabecular meshwork as you all know and this can be thought of roughly as the drain that the you drain or whatever in again I’m not a plumber I use the metaphor here of it I don’t know anything beyond that grate when it comes to the sink of my house. Alright, so but Schlemm’s canal we know is basically a tube. And there are ways that we can interact with Schlemm’s canal.

Outflow Pathways | Non-physiologic Outflow
- Trabecular Meshwork - Schlemm’s Canal - Collector Channel System - Uveal-Scleral Pathway
Fixing the Drain
Presenter
Presentation Notes
Then there’s the Collector Channel System. The collector channel system is rather mysterious we don’t have a way of testing it at this point but we know that it’s really important in terms of drainage. If the collector channel system, which takes fluid from Schlemm’s canal to the Venus collector system, does not work then many of the treatments I will be discussing today simply won’t work.
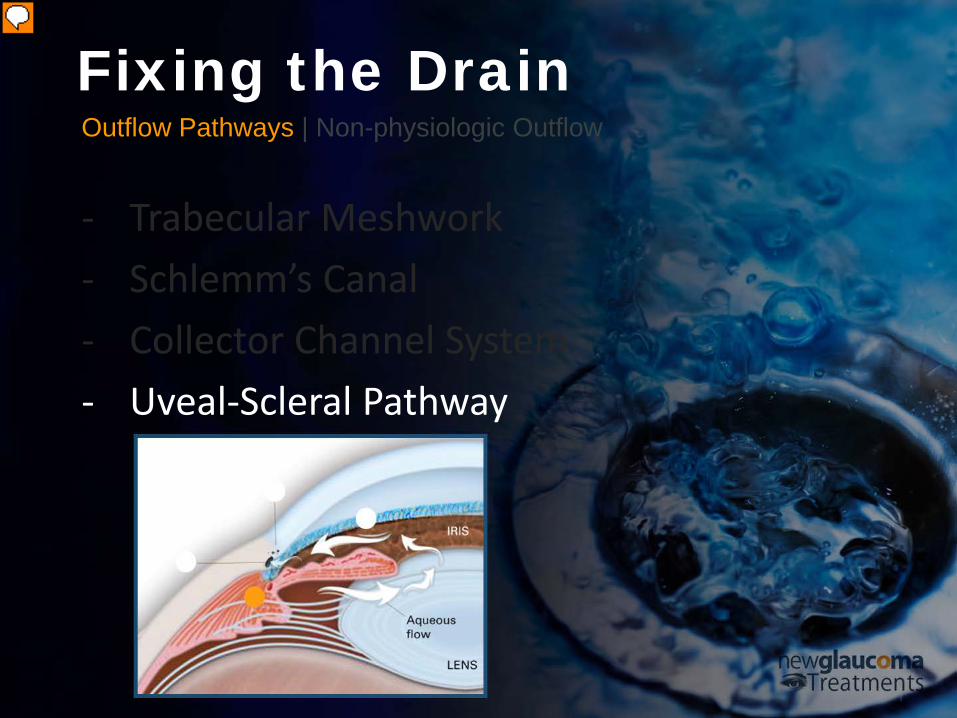
Outflow Pathways | Non-physiologic Outflow
- Trabecular Meshwork - Schlemm’s Canal - Collector Channel System - Uveal-Scleral Pathway
Fixing the Drain
Presenter
Presentation Notes
So that brings us to the next one which is the Uveal-Scleral Pathway, which is a pathway that was little known prior to the advent of prostaglandin analogs. Now this pathway does not use the classical or the usual pathway of the trabecular meshwork, Schlemm’s canal and collector channel system. It actually goes through the uvea here and we’ll talk about that because it’s a very interesting option to take advantage of.
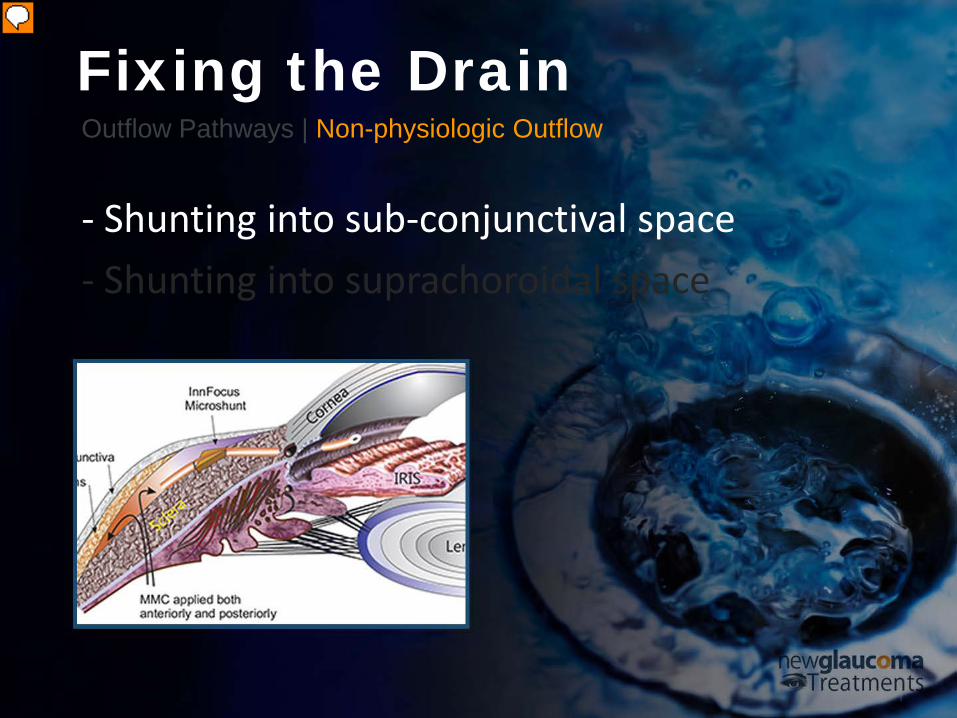
Outflow Pathways | Non-physiologic Outflow
- Shunting into sub-conjunctival space - Shunting into suprachoroidal space
Fixing the Drain
Presenter
Presentation Notes
Non-Physiologic Pathways In terms of the non-physiologic pathways, we can shunt fluid. So whenever we’re using a non-physiologic pathway we’re essentially creating a shunt. So a pathway, which wasn’t there before and the standard pathway that’s been used surgically since 1968 was Trabeculectomy—essentially poking a hole in the eye and shunting fluid from the anterior chamber into the subconjunctival space and creating a bleb.

Outflow Pathways | Non-physiologic Outflow
- Shunting into sub-conjunctival space - Shunting into suprachoroidal space
Fixing the Drain
Presenter
Presentation Notes
Now, the other thing we can do now (and we’ll get to this) is shunt fluid into what’s called the supraciliary or suprachoroidal space which is below the sclera. So we’ve got above the sclera and below the sclera options that are non-physiologic shunts.
Currently Available Glaucoma Treatments
(FDA Approved)
MEDICAL • LASER • INCISIONAL
Presenter
Presentation Notes
Currently Available Glaucoma Treatments So what I’d like to do is review the currently available glaucoma treatments because although you’ve been aware of many of them there are a couple of FDA-approved treatments that are relatively new And it’s helpful to put it in perspective of—put them in perspective in relationship to what’s been available in the past.

Currently Available Medical Treatments
(FDA Approved)
EYE DROPS • ORAL MEDICATIONS
Presenter
Presentation Notes
In terms of the currently available: medical treatments (you’re going to break these up into) medical laser, and surgical. Although, (technically) laser is surgery it’s not incisional. You know most patients they take more kindly to laser than they do incisional surgery.
Eye Drops
Beta-blockers | “Selective” Alpha Adrenergic Agonists | Carbonic Anhydrase Inhibitors (CAIs) | Prostaglandin Analogs | Cholinergic Receptors Agonists | Fixed Combination Agents
Presenter
Presentation Notes
Eye Drops We can look at the FDA-approved Eyedrops and Oral Medications. And I’m not going to spend a lot of time on this although I do want to give it its due. In terms of the eyedrops what we’ve got available here in the US: Beta-blockers, “Selective” Alpha Adrenergic Agonists, Carbonic Anhydrase Inhibitors (both drops and oral) as well, as Prostaglandin Analogs, the Cholinergic Receptors Agonists – so pilocarpine, and then the Fixed Combination Agents, of which we’ve got three.

Eye Drops Beta-blockers
Presenter
Presentation Notes
Beta-blockers So in terms of the Beta-blockers -Timoptic, Betaxolol… and others…pretty much all we use is Timoptic for most of our patients unless they’ve got some cardiovascular issues. These have been around for a very, very long time, we know they work well, and they work by turning down the faucet.

“Turns down the faucet” – Suppresses
– Inhibits
Eye Drops Beta-blockers
Presenter
Presentation Notes
So the Beta-blockers supress aqueous production and they do that do that by inhibiting c-AMP (cyclic mp). Now— again we’re not going to go into all of the scientific, and laboratory bench work on all of this because it’s a lot to take in. And if you want that the papers are available you can break out or dust off your old textbooks but I just want to make sure we get through everything today, which is quite a bit. One other thing is although you’ve got some paper there and some pens to take notes for pearls and what not, don’t worry about getting all of these. My plan is at some point to make these slides available online and when I do so (I will) we’ll send out a notice to everyone.
Ocular irritation
Bradycardia
Arrhythmia
Heart Block
Systemic hypotension
Heart failure
Eye Drops Beta-blockers
Presenter
Presentation Notes
So in terms of the Beta-blockers – although they’re cheap, widely available, and tolerated by most people there are some issues with them. They can cause ocular irritation (topically) but more concerning is Bradycardia (so low heart rate), arrhythmia (irregular heart rate), heart block (systemic just stop the heart), systemic hypotension (so low blood pressure) and even heart failure. And traditionally we’ve been told well you know be careful about using these in your elderly patients because they might be more sensitive to the Beta-blockers. So you know think you’ve got somebody who’s young and healthy shouldn’t be a problem. Be careful though I once had a patient who is in his 40s an athlete, stocky guy— gave him a timolol, told him beforehand (thankfully) that these were issues, he ended up in the emergency room the first night that he took a Beta-blockers because he was—although his heart rate was reasonable for an athlete in the 50s and 60s, when he took the Beta-blockers – because he started off so low, he dropped down below 40. So you do need to be careful about that. Basically anyone who’s not really healthy or really unhealthy should be okay. But if you’ve got an athlete or somebody who’s elderly and in terms of their cardiovascular status not so strong, you should be worried.
Central nervous system
depression
Impotence
May mask signs of hypoglycemia
Exacerbation of Asthma
Death
Eye Drops Beta-blockers
Presenter
Presentation Notes
Now they’re also non-cardiac issues: Central nervous system depression, impotence – if you’ve got somebody who’s taking the blue pill probably not a great candidate for Beta-blockers (by blue pill you all understand Viagra or its fellow agents). More importantly than that, it may mask signs of hypoglycemia. So if you’ve got diabetic patients who fluctuate a lot and occasionally have hypoglycemic episodes, you do not want to use Beta-blockers. It can also exacerbate asthma and you know from the things that I just mentioned, I think it’s pretty clear to see it can also result in death. We don’t see it very often but it does happen.

Eye Drops “Selective” Alpha Adrenergic
Presenter
Presentation Notes
“Selective” Alpha Adrenergic Agonists Selective Alpha Adrenergic Agonist is the next class I’m going to look at and that’s basically Brimonidine works by turning down the faucet and the selective one such as Brimonidine also opened the drain. So it’s nice this particular agent actually does both.
Eye Drops “Selective” Alpha Adrenergic Agonists
“Turns down the faucet”
– Suppresses
“Opens the Drain”
– Increases outflow
Presenter
Presentation Notes
“Selective” Alpha Adrenergic Agonists Mechanism of Action: Turns down the faucet Suppresses Aqueous Humor production Opens the Drain Brimonidine increases Uveoscleral Outflow
Ocular irritation
Follicular conjunctivitis
Eyelid retraction
Contact dermatitis
Headache
Eye Drops “Selective” Alpha Adrenergic Agonists
Presenter
Presentation Notes
But as we’re aware it causes ocular irritation and more worrisome than ocular irritation is the Follicular Conjunctivitis – this can happen up to 15% of the time and when it happens it could be whopping and you have no choice but to discontinue. Of interest is you can also see eyelid retraction, contact dermatitis and occasionally, although, we don’t think of it that often a headache. Other things: dry mouth, systemic hypotension, so it’s not just the Beta-blockers. Bradycardia, Arrhythmia, Death – it’s unlikely but we can see it.

Dry mouth
Systemic hypotension
Bradycardia
Arrythmia
Death
Eye Drops “Selective” Alpha Adrenergic Agonists
Presenter
Presentation Notes
Other things: dry mouth, systemic hypotension, so it’s not just the Beta-blockers. Bradycardia, Arrhythmia, Death – it’s unlikely but we can see it.
infants and small children
treat small (~1mm) ptosis
Normal Tension Glaucoma (NTG)
Eye Drops “Selective” Alpha Adrenergic Agonists
Presenter
Presentation Notes
But with regard to these last three here it’s most worrisome in infants and small children. The adrenergic agonist should not be used in infants and small children because of the risk of central nervous system depression and death. Now interestingly there are a couple of potential benefits of the selective alpha adrenergic agonist such as Brimonidine. One is if you’ve got somebody with a small ptosis of approximately one millimeter, Brimonidine is a great medical way to treat a small ptosis. It’ll lift the eyelid by about a millimeter. Also in terms of normal tension glaucoma there is evidence that between a Beta-blockers and an alpha adrenergic agonist (Brimonidine), that even with the same amount of intraocular pressure lowering, patients do better with Brimonidine. So in other words their visual fields are more stable – less likely to get worse over time.

Eye Drops Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
The Carbonic Anhydrase Inhibitors (the next class that we’ll talk about) so basically the Azopt® Brinzolamide and & Trusopt Dorzolamide.

Eye Drops Carbonic Anhydrase Inhibitors (CAIs)
“Turns down the faucet” – Decreases aqueous
production
Presenter
Presentation Notes
These work by turning down the faucet – decreasing aqueous production. Carbonic anhydrase is present in the ciliary epithelium. Now, the problem is that you have to actually block about 90% of the enzyme in order to get the effect that you want. So the problem with these is that they don’t actually work all that well. Of the drops we’ve talked about so far, they’re the least likely to work.
Ocular irritation
Punctate keratopathy
Blurred vision
Bitter taste
Eye Drops Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
Fortunately they don’t have too many side effects – irritation (that seems to be pretty common with anything that you’re going to use), punctate keratopathy, some blurred vision and some bitter taste.

90%
~15% reduction
corneal endothelial
dysfunction
Eye Drops Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
As I was saying 90% blocking has to occur to get an effect 15% reduction pressure – not that impressive. Now importantly, carbonic anhydrase is also used by the corneal endothelium in order to pump fluid out of the cornea. So if you’ve got somebody with a corneal endothelial dysfunction this may not be the best choice. Lower pressure but might swell the cornea up a bit.

Eye Drops Prostaglandin Analogs
Presenter
Presentation Notes
Prostaglandin Analogs Prostaglandin analogs – there’s a whole bunch of them available now. They open the drain but not through the regular drain.
Eye Drops Prostaglandin Analogs
“Opens the drain” – Increases uveoscleral
outflow
Presenter
Presentation Notes
They open up the drain through the uveal scleral outflow. They work quite well but they do have some local side effects that can be—depending on the patient—either desirable or bothersome.
Conjunctival hyperemia
Iris color change
Lash growth
Periorbitopathy
Eye Drops Prostaglandin Analogs
Presenter
Presentation Notes
Conjunctival Hyperemia almost always bothersome, iris color change almost always thought bothersome and it only happens in the pigmented areas so if you got somebody that has blue eyes and there’s no pigment they’re going to stay blue. If you’ve got somebody that’s got blue with brown spots the spots are going to become more noticeable. Hazel eyes become more brown. If you’ve got somebody with a dark brown iris it’s not going to matter. Lash growth most people appreciate that although some of the prostaglandins do tend at least under this Slit lamp to provide more of **** spidery, unruly lash growth which isn’t always appreciated. And men don’t always appreciate it but the other thing we’ve been seen recently is prostaglandin associated periorbitopathy (that’s a mouthful), which is essentially a reduction of the tissue around the eye now early on again it can be rather desirable right so you’ve got somebody with some excess bags under the eyes, apply the prostaglandins things seem to tighten up a little bit like they’ve had a little laser surgery tightening or sometimes it even looks like they’ve had a lower lid Bleph. That’s great early on but if it progresses too far it can actually tighten the lid so much that it’s difficult to obtain a pressure measurement using Goldman applanation tonometry so this can actually get in the way of your ability to monitor glaucoma.
Intraocular inflammation
Macular edema
Herpes virus reactivation
Headaches
Eye Drops Prostaglandin Analogs
Presenter
Presentation Notes
Now there’s some other things you can get intraocular inflammation. This is controversial but the prostaglandins are part of the inflammatory cascade. So it makes perfect sense that they are pro-inflammatory and indeed there’s evidence that they can increase the risk of macular edema at least in those patients who are already at risk for macular edema, herpes virus reactivation can be an issue so you should generally not use this particular drop to lower the pressure in somebody who has a history of herpes virus infection at least of the eye, and then headaches— there have been reports of pretty severe nocturnal headaches.

Eye Drops Cholinergic Receptors
Presenter
Presentation Notes
Cholinergic Receptors Agonists Speaking of headaches, Cholinergic Receptors. Pilocarpine that’s the one thing we all think about with pilocarpine is headache. Now these are still around because they can still be quite useful for those of our patients with narrow angles but there also still worth being aware of just in terms of general practice.
Eye Drops Cholinergic Receptors Agonists
“Opens the drain” – Increases outflow through
trabecular meshwork
Presenter
Presentation Notes
Because they do work pretty well — they open the drain through a different mechanism than the ones we’ve talked about. Essentially they provide some tension on the posterior trabecular meshwork and allow increased outflow.

Brow ache/Headache
Poor night vision (secondary to miosis)
Induced myopia
Eye Drops Cholinergic Receptors Agonists
Presenter
Presentation Notes
But brow ache poor night vision due to the meiosis induced myopia and then there are these other issues—retinal detachment more of an issue with high myopias but of course if you’ve got a retinal detachment and somebody who has a small pupil that you can’t dilate, that’s an issue. And then less likely but something that was more commonly seen with the older agents in this class and also when we were using this drop a lot more, cicatricial conjunctival pemphigoid, corneal endothelial toxicity, so it’s not just the carbonic anhydrase inhibitors that can give you issues with the corneal endothelium it’s also pilocarpine. And then band keratopathy.

Retinal detachment
Cicatricial conjunctival
pemphigoid
Corneal endothelial toxicity
Band keratopathy
Eye Drops Cholinergic Receptors Agonists
Presenter
Presentation Notes
retinal detachment more of an issue with high myopias but of course if you’ve got a retinal detachment and somebody who has a small pupil that you can’t dilate, that’s an issue. And then less likely but something that was more commonly seen with the older agents in this class and also when we were using this drop a lot more, cicatricial conjunctival pemphigoid, corneal endothelial toxicity, so it’s not just the carbonic anhydrase inhibitors that can give you issues with the corneal endothelium it’s also pilocarpine. And then band keratopathy.

• Cosopt – Timolol + Dorzolamide
• Combigan – Timolol + Brimonidine
• Simbrinza – Brimonidine + Brinzolamide
Eye Drops Fixed Combination Agents
Presenter
Presentation Notes
Fixed Combination Agents Fortunately we now have these Fixed Combination Agents. We have three of them here in the US Cosopt® – Timolol + Dorzolamide, Combigan® ® – Timolol + Brimonidine, Simbrinza® which is Brimonidine + Brinzolamide. My current favorite is Simbrinza® simply because it doesn’t have a Timolol component. Now the other thing to keep in mind here is that these agents, Cosopt® and Combigan® , the two that are Fixed Combination Agents which do have Timolol in them, you’re using these twice a day. It’s a twice a day agent where you’re using timolol twice a day which really is best used once a day in the morning because the night-time dose doesn’t really help you all that much in terms of the aqueous production which drops at night anyway. But the other thing is we now know that using Beta-blockers at night can potentially put patients at risk for what’s called dipping, which is where their blood pressure drops by 10 points patients who dip are at a much, much higher risk of progression with their glaucoma. So why in the world would you want to use a drop that places a beta blocker in the eye but then moves systemically in most patients at night? Now the other issue here is we’re dosing these twice a day Cosopt® and Combigan® . Well, Dorzolamide and Brimonidine both work best three times a day. So the Cosopt® and Combigan® — I’ve almost entirely eliminated from my practice because in my mind these are just bad compromises. You’re not getting the right dosing on the Brimonidine and the Dorzolamide and you’re getting too much Timolol and potentially actually putting your patient at risk if they’re a dipper. Now if you’re worried about dipping, you can get a 24-hour blood pressure monitoring. It’s not that expensive. It’s not that much of a hassle. Generally you work with the internist. Most internists are happy to do it because it’s information they’d like anyway but for that reason I’ve really moved to Simbrinza® using— recommending it three times a day. The patients don’t get that middle of the day dose so I tell them don’t feel guilty about it just try to do it. We’ve all got more guilt than we need. So those are the drops.

Oral Medications Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
Currently Available (FDA-approved) Medical Treatments (Oral Medication) Carbonic Anhydrase Inhibitors (CAIs)
Oral Medications Carbonic Anhydrase Inhibitors (CAIs)
“Turns down the faucet” – Decreases aqueous
production
– more effective
Presenter
Presentation Notes
The Carbonic Anhydrase Inhibitors (CAIs) – Again, they turn on the faucet. But the oral ones are far more effective than the topical ones. So the oral ones, again, are Acetazolamide and Neptazane.
Transient myopia
Frequent urination
Light-headedness
Parasthesias (extremity
tingling)
Oral Medications Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
The issue with the oral ones, though, is systemic side effects: transient myopia, frequent urination, light-headedness, paresthesias/Paresthesias – extremity tingling. These are all bothersome but they’re not horrible.

Dehydration
Malaise
Weight loss
GI symptoms
Hypokalemia
Oral Medications Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
What’s horrible is potentially (in your older patients) dehydration leading to falls, malaise, weight loss, GI symptoms, and hypokalemia. So we all say to our patients, “eat bananas” — bananas actually aren’t the best source of potassium. Much better would be pomegranates, which we now have in abundance here. And soon enough bananas won’t be available anyway. So you might as well start recommending pomegranates before bananas go extinct,

Metabolic acidosis
Kidney stones
Aplastic Anemia
Death
Oral Medications Carbonic Anhydrase Inhibitors (CAIs)
Presenter
Presentation Notes
metabolic acidosis, kidney stones, aplastic anemia, and death. So this is why you don’t see patients on Diamox chronically at least not too many of them. So those are medical treatments.

Currently Available Surgical Treatments
(FDA Approved)
LASER • INCISIONAL
Presenter
Presentation Notes
Currently Available Laser Treatments (Laser Trabeculoplasty) Let’s move on to the Surgical Treatments.

Laser Treatments Iridotomy | Iridoplasty | Trabeculoplasty | Cyclodestructive Procedures
Presenter
Presentation Notes
You’re going to start with the FDA-approved surgical treatments— laser and incisional is what’s available here. In terms of laser treatments, we’ve got Iridotomy, Iridoplasty, Trabeculoplasty, and Cyclodestructive Procedures.
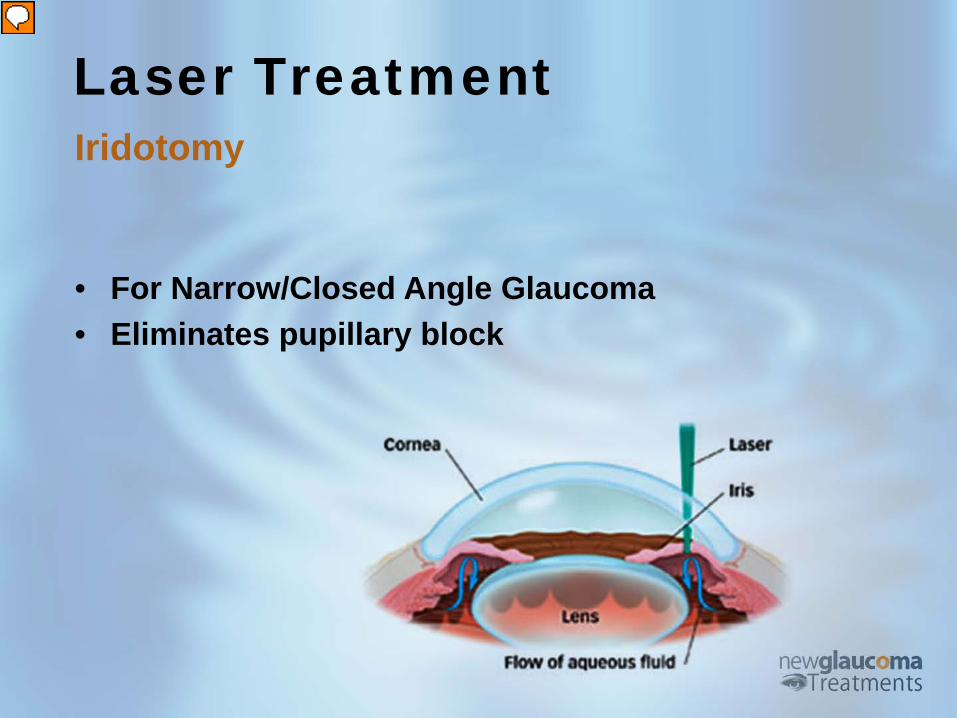
• For Narrow/Closed Angle Glaucoma • Eliminates pupillary block
Laser Treatment Iridotomy
Presenter
Presentation Notes
Iridotomy Iridotomy, I’m not going to spend a lot of time on that – we poke a hole on the Iris, allows fluid through and out the natural drainage system.

• For Plauteau Iris Glaucoma
Laser Treatment Iridoplasty
Presenter
Presentation Notes
Iridoplasty – It’s Plasty. So instead of making a hole you’re basically shrinking the Iris. This is used in plateau iris and what you see here in this picture is here’s the Iridotomy. When Iridotomy doesn’t work in plateau iris you then do a Iridoplasty. So you do is you make a whole bunch of little spots here that pull the iris away from the angle.
Glaucoma Surgery Categories
Non-Invasive Minimally Invasive Penetrating
Presenter
Presentation Notes
At this point, I’d like to primarily focus on the treatment of open angle glaucoma. Before we dive into the individual surgical treatments, I find it helpful to break them into categories: <click> o Non-invasive – these would be laser treatments <click> o Minimally Invasive – what is now being called MIGS for Minimally Invasive Glaucoma Surgery <click> o …and Penetrating – traditional glaucoma surgeries such as trabeculectomy and glaucoma drainage devices (or tubes) <click>
Glaucoma Surgery Categories
Shunt Enhance Ablate
Presenter
Presentation Notes
Now, we can also think about glaucoma surgical treatments in terms of how they work. They can SHUNT, they can ENHANCE–So they can shunt fluid out of the eye. They can enhance the natural outflow, or they can ABLATE – they can basically destroy tissues. So mostly when we’re talking about destroying tissue we’re talking about destroying the ciliary body. So I like to think of this in terms of mnemonics as SEA. Let’s look at Enhancing here.

Laser Trabeculoplasty Argon | Selective | Micropulse
Presenter
Presentation Notes
Laser Trabeculoplasty Laser Trabeculoplasty – you can split this up into Argon, Selective and Micropulse.

For open angle glaucoma
Performed in 1 or 2 sessions
May result in microscopic scars
May limit future surgeries
Laser Treatment Argon Laser Trabeculoplasty (ALT)
Presenter
Presentation Notes
Argon Laser Trabeculoplasty (ALT) This type of laser has been around the longest. It is generally performed in one or two sessions. However, it can result in microscopic scars called “peripheral anterior synechiae”[1] that can limit the effectiveness of the treatment as well as future surgeries (such as canaloplasty). �To this date no one is really sure how laser trabeculoplasty works. Indeed, it’s discovery is similar to many such medical advances in that it involved the marriage of an unexpected outcome and a perceptive researcher. When the argon laser was first used to treat the angle the goal was to actually punch holes through the trabecular meshwork creating microscopic shunts into Schlemm’s canal. The problem was that these tiny holes would scar down. So what did researchers do? They figured that if the laser caused scarring they could instead use this technology to create a model of glaucoma in laboratory animals. By using just enough energy to coagulate rather than punch a hole in the trabecular meshwork the intraocular pressure would elevate allowing researchers to study a monkey model of glaucoma. In an ironic twist, however, some of these monkeys exibited IOP lowering after the initial post-operative inflammation resolved. And so laser trabeculoplasty was discovered more than invented.

Uses a “Q-switched, frequency-doubled Nd:YAG laser”
Can be performed after ALT
Less traumatic compared to ALT
Less damage to the eye tissue
Quick, usually painless
Performed in 2 ways: Gonioscopic or Transscleral
Laser Treatment Selective Laser Trabeculoplasty (SLT)
Presenter
Presentation Notes
Selective Laser Trabeculoplasty (SLT) Selective laser trabeculoplasty is becoming more commonly recommended primarily because it doesn’t destroy tissue. And because it’s now becoming affordable. When this first came out it was $70,000 to buy the laser, who other than glaucoma specialist are going to be able to do that but lately the laser cost has come down into the 20,000-40,000 range. This uses a Q-switched frequency-doubled Nd:YAG laser (not that anybody need to know that). It can be performed on its own or even after ALT. It’s less traumatic because it doesn’t coagulate tissue, less damage, it’s quick and it’s usually painless. And interestingly enough, it can be performed either using a gonio mirror (as with the Alt) or a recent study that was just published showed that you can actually do this Transscleraly.

Laser Treatment Selective Laser Trabeculoplasty (SLT)
Video Credit: Prof. Philippe Denis,University Hospitals of Lyon
Presenter
Presentation Notes
So you can just sit the patient at the slit lamp, aim the beam at the limbus and place 100 spots around the limbus and it works. Perhaps not as well — we don’t know—but it does work. So there it is. There’s a laser spot and it’s lasering. Fascinating.

Micro-pulses
Less damage and scarring
Minimal inflammation
and post-operative IOP
elevation
Laser Treatment Micropulse Laser Trabeculoplasty (MLT)
Presenter
Presentation Notes
Micropulse® Laser Trabeculoplasty (MLT) Micropulse® Laser Trabeculoplasty (MLT) – This basically uses micropulses—really, really, really short pulses. And the idea is if you separate the pulses into tiny little pulses followed by a little pause and then another little pulse and then a little pause what happens is you get what’s called “thermal relaxation”. So the tissue heats up and then cools off and then heats up and cools off and you do not get coagulative damage when you do this. Basically this is a newer version of SLT. It’s a cheaper version of SLT, seems to work as well as SLT and so there’s some benefits to having this. �

• Continuous Wave Cyclophotocoagulation
– Ab-Externo (i.e. IRIDEX G6 laser)
– Ab-Interno (EndoCycloPhotocoagulation (ECP)
• Micropulse Cyclophotocoagulation (MP3)
Laser Treatment “Cyclodestructive” Procedures
Presenter
Presentation Notes
Currently Available (FDA-approved) Laser Treatments (“Cyclodestructive” Procedures for Glaucoma) Continuous Wave Cyclophotocoagulation Ab-Externo Continuous Wave Cyclophotocoagulation This is, traditionally been, reserved for those patients who have end-stage glaucoma where there’s no potential for vision. It’s just a blind, painful eye. And you’d place this laser spots transscleraly, you destroy the ciliary body and you’d lower the pressure. But you could also lower it too much—you could essentially destroy the aqueous production and end up with a hypotenuse or even Phthisical Eye. So this is not really used for too many patients. But it did have its use.

Laser Treatment Ab-Externo CW Cyclophotocoagulation
• Destruction of the ciliary body to to reduce
aqueous humor secretion and lower IOP
• Anesthesia is needed, as the procedure is painful.
× Inflammation and hyptotony
Presenter
Presentation Notes
Ab-Externo Continuous Wave Cyclophotocoagulation This is, traditionally been, reserved for those patients who have end-stage glaucoma where there’s no potential for vision. It’s just a blind, painful eye. And you’d place this laser spots transscleraly, you destroy the ciliary body and you’d lower the pressure. But you could also lower it too much—you could essentially destroy the aqueous production and end up with a hypotenuse or even Phthisical Eye. So this is not really used for too many patients. But it did have its use.

For mild to moderate glaucoma
Done with cataract surgery
Relatively low risk glaucoma treatment
× Uveitis - quite severe after ECP
Laser Treatment Ab-Interno CW Cyclophotocoagulation EndoCycloPhotocoagulation (ECP)
Presenter
Presentation Notes
Ab-Interno Continuous Wave Cyclophotocoagulation – EndoCycloPhotocoagulation (ECP) Then there’s the Ab-Interno – the newer version, the EndoCycloPhotocoagulation (ECP) and the most exciting (I think) is the newest iteration of this is Micropulse® Cyclophotocoagulation (MP3). So the Ab-Externo which is from the outside of the eye, continuous-wave cyclophotocoagulation— we just talked about that. It was pretty uncomfortable. Nope, it was downright painful. You actually had to block the eye or put somebody under anesthesia. And then not only— this is the other thing—not only could you get hypotony but there was even the possibility that you could get sympathetic ophthalmia from the severe inflammatory response. So you treat one eye and the other eye would go blind. Not ideal. So this is why we didn’t see much of this but because it did have its use it stayed around for a while. And eventually people figured out how to use this technology in a safer way that was still effective. And so EndoCycloPhotocoagulation was developed. This can be used for mild to moderate glaucoma it has to be done at the time of or after cataract surgery and it’s relatively low-risk glaucoma but it’s also you know relatively modest in its effect. And it does, as with anything you do with the iris or the ciliary body, it’s going to result in some inflammation.

Laser Treatment EndoCycloPhotocoagulation (ECP)
Presenter
Presentation Notes
So here is an animation of the ECP. A viscoelastic is placed in the in the eye a probe is then inserted and the individual ciliary body processes are then lasered and the trick is to shrink them. You have to shrink them enough that the epithelium stops producing aqueous. But you don’t want to actually pop them. And what happens is you see them shrink and if you go beyond the shrinking they pop like popcorn. And unfortunately that pop is so incredibly pro-inflammatory that this procedure is very much surgeon-dependent. So if the surgeon understands the nuances of the procedure you can get a nice effect without too much inflammation. If they’ve got a heavy hand or heavy foot, as the case may be it, it can actually result in a lot of inflammation.
Laser Treatment Micropulse Cyclophotocoagulation (MP3) • A “gentler” form of
cyclophotocoagulation
• Appears to work very much
like the eye drop Pilocarpine
• No restrictions on one’s
activities after
• Low risk profile
Presenter
Presentation Notes
Micropulse® Cyclophotocoagulation (MP3) This is, I think, as I said the one of the most exciting laser treatments that’s available. This uses, as we talked about before, micropulses. You’ve got tiny little pulses followed by a pause allowing for the thermal relaxation. So this was thought of as a gentler form of Cyclophotocoagulation. Nobody really knew how it worked. I mean if you’re not destroying the ciliary body process how in the world are you getting any reduction in aqueous. Well turns out you’re not. It doesn’t work by reducing aqueous. It works by pulling on—on the posterior trabecular meshwork and essentially enhancing outflow just like pilocarpine. Nice thing about this is although it is uncomfortable and you still have to either block or put some of the– quick five minutes of IV sedation, it’s generally comfortable afterwards, very low risk, and it works— works well as we’ll see in a moment.

Laser Treatment Micropulse Cyclophotocoagulation (MP3) • Uses a slow application of laser energy that is
“chopped” into micropulses (or, bursts).
• Does not burn or destroy eye tissue
Presenter
Presentation Notes
So this is the slow application. The lasers chopped in the micropulses.

Laser Treatment Micropulse Cyclophotocoagulation (MP3) NUHS Prospective Clinical Study1
• 33% IOP reduction at 18 months, (N = 38 patients)
• 61% med reduction (2.1±1.1 to 1.3±1.0)
Presenter
Presentation Notes
Laser Treatments of Glaucoma Micropulse® Cyclophotocoagulation (MP3) Glaucoma Treatment at Earlier Stages of Glaucoma The early studies looked at patients who just like with Transscleral, continuous wave Cyclophotocoagulation were kind of end-stage patients —you can see these are patients with pressures in the 40’s. And they come down in the mid 20’s. Since that time, they’ve also studied patients who have more reasonable pressures and the studies seem to indicate that they do (about) as well, in terms of the percent reduction. And this is the procedure it’s an external procedure… There’s no incision it does not have to be done under sterile conditions, and essentially you make about nine passes superiorly, nine passes inferiorly of this laser. And it’s not technically challenging although it can be somewhat challenging in patients who have small palpebral fissure because if you don’t get the laser posterior enough you can end up with a change in the pupil size and potential inflammation. And that’s probably the reason why pupil dilation is relatively common.

Laser Treatment Micropulse Cyclophotocoagulation (MP3)
Video Credit: Robert Noecker, MD
Presenter
Presentation Notes
And this is the procedure it’s an external procedure… There’s no incision it does not have to be done under sterile conditions, and essentially you make about nine passes superiorly, nine passes inferiorly of this laser. And it’s not technically challenging although it can be somewhat challenging in patients who have small palpebral fissure because if you don’t get the laser posterior enough you can end up with a change in the pupil size and potential inflammation. And that’s probably the reason why pupil dilation is relatively common.
Laser Treatment Micropulse Cyclophotocoagulation (MP3) • Common complications:
– pupil dilation (11%),
– corneal surface drying (7%),
– significant inflammation (3%),
– swelling of the macula (2%), and
– decreased near vision (2%).
Presenter
Presentation Notes
Laser Treatments of Glaucoma Micropulse® Cyclophotocoagulation (MP3) Glaucoma Treatment at Earlier Stages of Glaucoma And it’s not technically challenging although it can be somewhat challenging in patients who have small palpebral fissure because if you don’t get the laser posterior enough you can end up with a change in the pupil size and potential inflammation. And that’s probably the reason why pupil dilation is relatively common.

Incisional Surgery Traditional “Penetrating” Surgical Methods | Lower Risk Surgeries
Presenter
Presentation Notes
Currently Available Incisional Treatments for Glaucoma (Traditional “Penetrating” Surgical Methods) Incisional surgery These are what we can basically split into Penetrating (the more traditional ones) and the Lower Risk Surgeries, which are called “minimally invasive glaucoma surgeries” or “Micro Invasive Glaucoma Surgeries”—basically MIGS. And we’ll go over how well MIGS go, in a second, because you may have heard the tongue- in-cheek term, MEGS— M-E-G-S for Minimally Effective Glaucoma Surgery and we’ll see whether or not that’s case.

Traditional “Penetrating” Surgical Methods
Trabeculectomy | Glaucoma drainage devices
Presenter
Presentation Notes
Currently Available Incisional Treatments for Glaucoma (Traditional “Penetrating” Surgical Methods) Incisional surgery And we’ll go over how well MIGS go, in a second, because you may have heard the tongue- in-cheek term, MEGS— M-E-G-S for Minimally Effective Glaucoma Surgery and we’ll see whether or not that’s case.

Traditional “Penetrating” Trabeculectomy
Fistula
Bleb dependent
Bleb failure
Lifetime risk of infection
Lifestyle Limitation
Presenter
Presentation Notes
Trabeculectomy We all know about trabeculectomy— you create a fistula, so a shunt creates a bleb, the issues of bleb failure, lifetime risk of infection and lifestyle limitation. You can’t wear contact lenses; in general, you can’t go snorkelling or scuba diving— things like that. For our active baby boomer patients, this can be an issue.
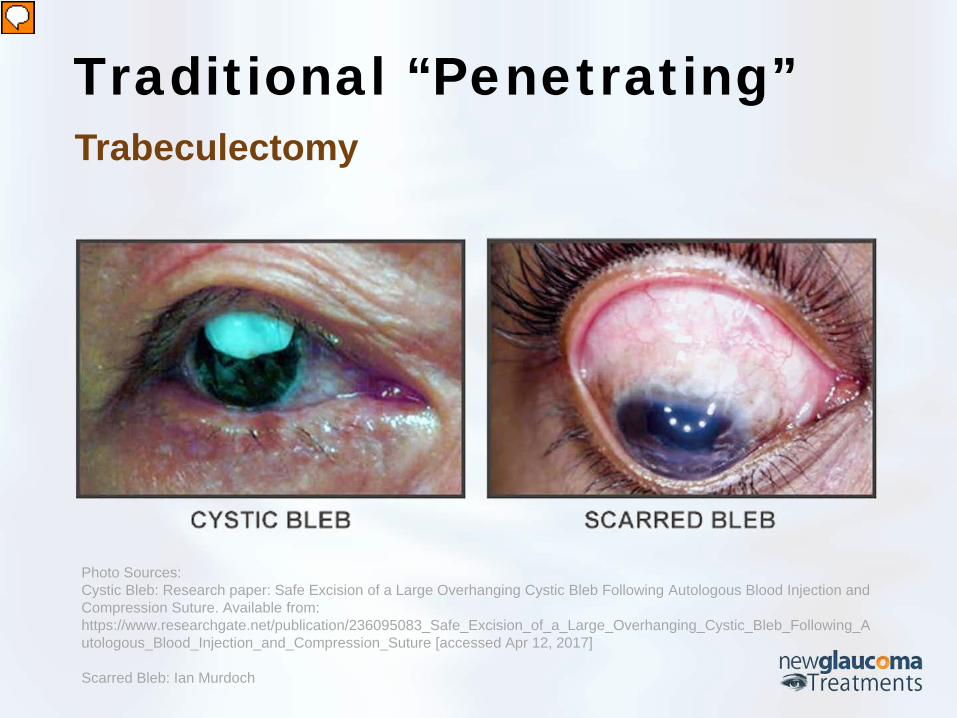
Traditional “Penetrating” Trabeculectomy
Photo Sources: Cystic Bleb: Research paper: Safe Excision of a Large Overhanging Cystic Bleb Following Autologous Blood Injection and Compression Suture. Available from: https://www.researchgate.net/publication/236095083_Safe_Excision_of_a_Large_Overhanging_Cystic_Bleb_Following_Autologous_Blood_Injection_and_Compression_Suture [accessed Apr 12, 2017] Scarred Bleb: Ian Murdoch
Presenter
Presentation Notes
There’s also other issues—you can have cystic blebs, resulting in ocular surface disease, you have scarred bleb, which is quite (you know) in five years after trabeculectomy, its more likely to have a cataract from the trabeculectomy than you are to have a working bleb. You know, they’ve been around since 1968 and they’ve really not changed much in that time so I think that we can all agree it’s time to move on. And we’re going to be talking about the potential methods by which we can move on.

Traditional “Penetrating” Glaucoma Drainage Devices Non-Valved vs. Valved
Movement of the implant
Infection
Scarring
Double Vision
Presenter
Presentation Notes
Glaucoma Drainage Devices Traditional penetrating surgeries also include the Glaucoma Drainage Devices. Essentially there are two that are commonly used here in the in the US — the non-valve, which is the Baerveldt® versus the valve, which is the Ahmed™ and these have a number of issues along with — that are shared as well as somewhat unique from Trabeculectomy.

Traditional “Penetrating” Glaucoma Drainage Devices
Presenter
Presentation Notes
And in the case of the Trabeculectomy and Glaucoma Drainage Devices the main risks are pressure elevation and hypotony—so both extremes there. In the case of the Glaucoma Drainage Devices, you’ve put an implant on the surface of the eye, underneath the conjunctiva, so not surprisingly the implant can sometimes move, you can give them the trouble with that, you can get an infection — if you get an infection on an implant, whether it’s an implant in the eye or anywhere else, that’s a big issue. You generally have to remove the implant. It’s very hard to eliminate an infection on any non-biologic tissue. Scarring can cause double vision. And then there are other things — the implant itself — the tube can erode. With Glaucoma Drainage Devices as well as Trabeculectomy, if you end up with a sudden drop in pressure, you can end up with a suprachoroidal hemorrhage— a bleed in the back of the eye that can lead to a total loss of vision or at least put you at great risk of that. So essentially after incisional glaucoma surgery that’s the only time I will ever tell my patients that not only can they use a laxative or stool softener but I want them to. Because I want them to avoid any Valsalva maneuver, anything that could cause an increase in venous pressure resulting in back flow into a hypotenuse eye. So given those risks and given the fact that with glaucoma, we’ve got patients that generally can see and we’re trying to keep them from losing vision. I don’t like offering surgical treatments that have a high risk of loss of vision.

Lower Risk Surgeries Ab-Externo (Canaloplasty) | Ab-Interno aka MIGS
Presenter
Presentation Notes
Currently Available Incisional Treatments for Glaucoma (Lower Risk Surgeries) So this is where the newer, lower risk surgeries are really exciting. The question is, are the lower risk surgeries as effective as the higher risk, older penetrating surgeries? so we’re going to look at the Ab-Externo (from the outside) and the Ab-Interno.
“Non-Penetrating”
No Hole. No Bleb
Lower IOP. Fewer Drops
Safer than traditional surgeries
Pro-Active Lifestyle
Photo credit: ellex.com
Lower Risk Surgeries Ab-Externo Canaloplasty
Presenter
Presentation Notes
Ab-Externo Canaloplasty Of the Ab-Externo, the main one is Canaloplasty. This is a develop— this is essentially a modification of a surgery that’s very commonly done in Europe, which is called Deep Sclerectomy or ViscoCanalostomy (this is another version of that). And they use it in Europe because it’s safer than Trabeculectomy. Well in the case of—when we’re talking of ViscoCanalostomy or Canaloplasty, these are non-penetrating. So you’re not actually creating a fistula from the anterior chamber into the subconjunctival space. So there’s no hole, no bleb… but they work well. So, you do lower the pressure, you have fewer drops in general, they’re safer than traditional surgeries, and this is key for our patients who like to be active: you, generally, do not have to adjust your lifestyle.
Lower Risk Surgeries Ab-Externo Canaloplasty
Video Credit: Ellex.com
Presenter
Presentation Notes
And so, showing you what Canaloplasty looks like here. You do—and this is just going to go through (sorry) the normal pathway of aqueous being produced by the axillary epithelium, going out through the trabecular meshwork but in the case of glaucoma patients there’s a blockage in either on the Trabecular Meshwork or the Schlemm’s canal…So with canaloplasty, you do create a partial thickness scleral flap; so it’s not a full thickness scleral flap. It’s a partial thickness. And a catheter-the world’s smallest catheter, it’s incredible little 250 micrometer diameter catheter is threaded through the canal, which is pretty neat to see. Once it’s through, you tie a suture to it and pull the suture back through the canal. Now why would you do that? The idea is as you’re pulling it back through the canal you’re actually injecting viscoelastic to dilate the canal. So it’s kind of like angioplasty for the eye. Now once you’ve pulled the suture back through you tie it to tighten the inner wall of the canal kind of like you tie a hoodie to bring it down and you can see that pulling down on the inner wall. Now what happens is you dilate the canal and you stent it open so you get better flow into the Schlemm’s canal and then out through the collector channel systems. Aha! But you have to have an open collector channel system, which there’s unfortunately no way to detect beforehand and this is going to be a theme through the rest of this talk.
Lower Risk Surgeries Ab-Externo Canaloplasty
Presenter
Presentation Notes
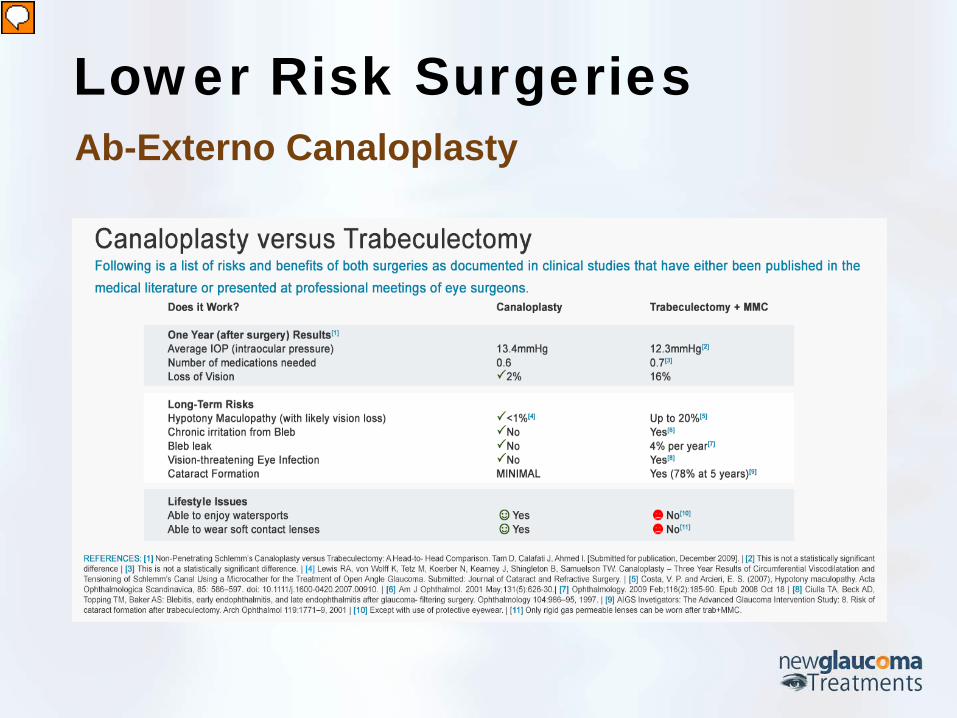
So how does it work? Well it turns out it works pretty well, okay. And one study that looked at the two surgeries Trabeculectomy versus Canaloplasty there was not a significant difference between the final pressures: 13.4 with Trabeculectomy (and this is one year out) versus 12.3 (sorry) 13.4 with Canaloplasty (I correct myself) versus 12.3 with Trabeculectomy and mitomycin. So yes Trabeculectomy had a tendency to be lower but it wasn’t a statistically significant difference.

Lower Risk Surgeries Ab-Externo Canaloplasty
Presenter
Presentation Notes
What was different importantly is the risks. Patients had better vision with Canaloplasty, they had lower risk of hypotony, they had no issues with blebs… I could go on. Anyway the three year results are quite good in terms of the reduction. So if Canaloplasty only there was a 34% mean IOP reduction from baseline and a 53% reduction in drop use. So not only did the pressure drop, but the number of drops that were required to keep that pressure dropped as well. If you combine Canaloplasty with phacoemulsification (so cataract surgery) it gets even better 42% mean intraocular pressure reduction. 81% mean reduction in drops and 90% (eighty-eight% of patients) were drop- free three years after surgery today without the risks of Trabeculectomy. So this is a really, really exciting procedure.
Lower Risk Surgeries Ab-Externo Canaloplasty
Presenter
Presentation Notes
The doctor who developed Canaloplasty, Dr. Robert Stegmann in South Africa, is an absolute genius. I think this quote pretty much sums it up, “it’s vital to find a safer more predictable operation with preferably no complications at all (and he felt that) canaloplasty is the closest that (he) has ever come to that”. And that’s another point that I didn’t make earlier; with Trabeculectomy/Glaucoma Drainage Devices it there’s no coupling between surgeon skill and the outcome. You speak to experience glaucoma surgeons, they will tell you “I will finish what I think is a perfect Trabeculectomy and have no idea how this patients going to do because it’s so dependent upon the body’s healing response.” And that’s not the case with Canaloplasty.

Lower Risk Surgeries Ab-Interno aka Minimally Invasive Glaucoma Surgery (MIGS) • Ab-Interno Canaloplasty (ABiC)
• Trabeculotomy
• iStent
• CyPass
• Xen Gel Stent
• Cataract Surgery
Presenter
Presentation Notes
Currently Available Incisional Treatments for Glaucoma (Lower Risk Surgeries) Ab-Interno or Minimally Invasive Glaucoma Surgery (MIGS) So moving on to the minimally invasive glaucoma surgeries, which is really an exciting area right now—but the question is, “are they also minimally effective?” So the ones we’re going to go over are the ones that are FDA-approved: Ab-interno Canaloplasty (ABiC)—so this is Canaloplasty from the inside of the eye, Trabeculotomy, iStent®, Cypass®, Xen Gel Stent, and Cataract Surgery. And you may say, “well, why’s cataract surgery up there?” We will get to that.
Exam n Mean IOP (mm Hg) ± SD
Mean Medications (n) ± SD
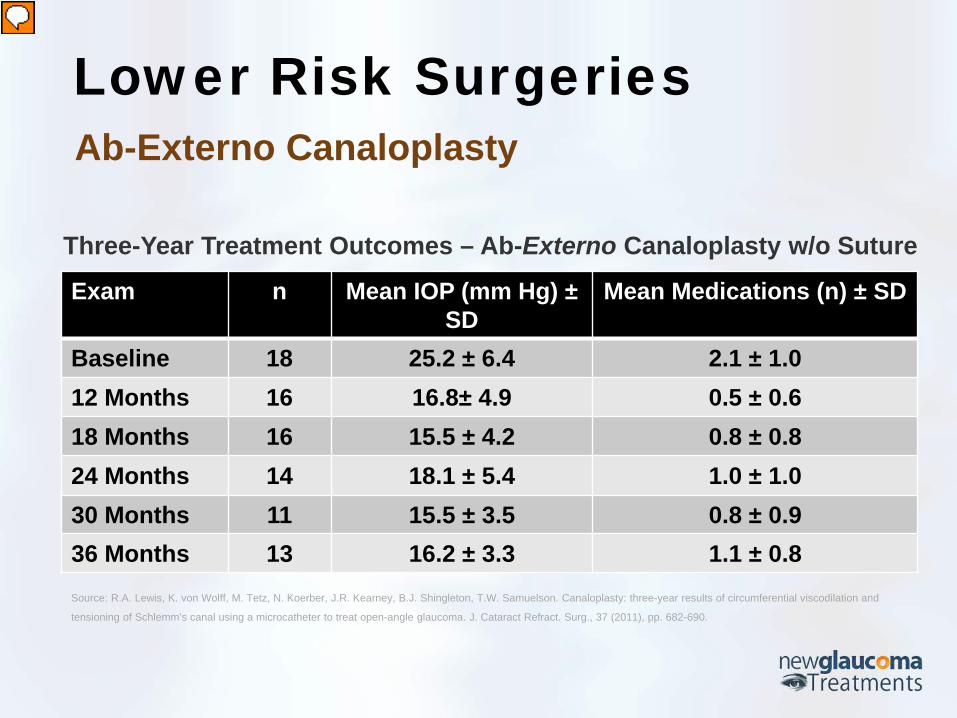
Baseline 18 25.2 ± 6.4 2.1 ± 1.0 12 Months 16 16.8± 4.9 0.5 ± 0.6 18 Months 16 15.5 ± 4.2 0.8 ± 0.8 24 Months 14 18.1 ± 5.4 1.0 ± 1.0 30 Months 11 15.5 ± 3.5 0.8 ± 0.9 36 Months 13 16.2 ± 3.3 1.1 ± 0.8 Source: R.A. Lewis, K. von Wolff, M. Tetz, N. Koerber, J.R. Kearney, B.J. Shingleton, T.W. Samuelson. Canaloplasty: three-year results of circumferential viscodilation and
tensioning of Schlemm’s canal using a microcatheter to treat open-angle glaucoma. J. Cataract Refract. Surg., 37 (2011), pp. 682-690.
Three-Year Treatment Outcomes – Ab-Externo Canaloplasty w/o Suture
Lower Risk Surgeries Ab-Externo Canaloplasty
Presenter
Presentation Notes
Ab-Interno Canaloplasty So interestingly enough, with the Ab-Externo Canaloplasty (coming from the outside) they separated the results in those that had the stent and those that didn’t have the stent. And what they saw was that, although they generally did better with the stent (even if you couldn’t get the stent in) the pressure is still dropped. And you can see in this here three-year results of those with Ab-Externo Canaloplasty but without the suture the average pressure dropped from 25.2 mmHg to 16.2 mmHg. This is a pretty decent reduction and the mean number of medications from 2.1 to 1.1— so by one medication on average. .

Lower Risk Surgeries Ab-Interno Canaloplasty
Comprehensive: treats trabecular meshwork,
Schlemm’s canal and collector channels
Better aqueous outflow
No permanent implant or stent
Presenter
Presentation Notes
So, Dr. Mark Gallardo in El Paso Texas thought, “well this is interesting. Is there a way that we could do this from the inside of the eye without making the incision from the outside the eye, which would make it much less complex of a surgery and also a much faster surgery. And it turns out you can and the neat thing about it is that by doing this you treat the trabecular meshwork—because you create an opening in the trabecular meshwork, you open Schlemm’s canal, you potentially dilate the collector channels— so you get better aqueous outflow, and there’s no permanent stent or implant. And that’s the key point of the Ab-Interno Canaloplasty— no permanent stent or implant.

Lower Risk Surgeries Ab-Interno Canaloplasty
Video Credit: Ellex.com
Presenter
Presentation Notes
What we’ll do here is I’m going to take us through—this here, so essentially this is after cataract surgery. So, what’s going to be done is— you can see over here that…here’s—the catheter is being inserted into the anterior chamber and it’s basically being rested against the angle here. Then what happens is a gonio lens is placed on the eye—and here again you can see that the catheter is resting there so you’re looking at the angle of the eye—and either a blade or Cystitome is used to actually pierce the trabecular meshwork, opening up into Schlemm’s canal, which also—which often results in a little blood reflux—so you can see a little blood there. And then this is what is so cool about this procedure—micro forceps are used to thread this catheter through and you can see the tip of the catheter (it’s a blinking red catheter), you’re going to see it coming around here in a moment—so these—he’s threading it around to the Schlemm’s canal. So he’ll thread it all the way around and then place another instrument in the eye to essentially hold the catheter up against the angle and he pulls it back through. As it’s being pulled back through, viscoelastic is being injected into the canal—dilating the canal.
Exam n Mean IOP (mm Hg) ± SD
Mean Medications (n) ± SD
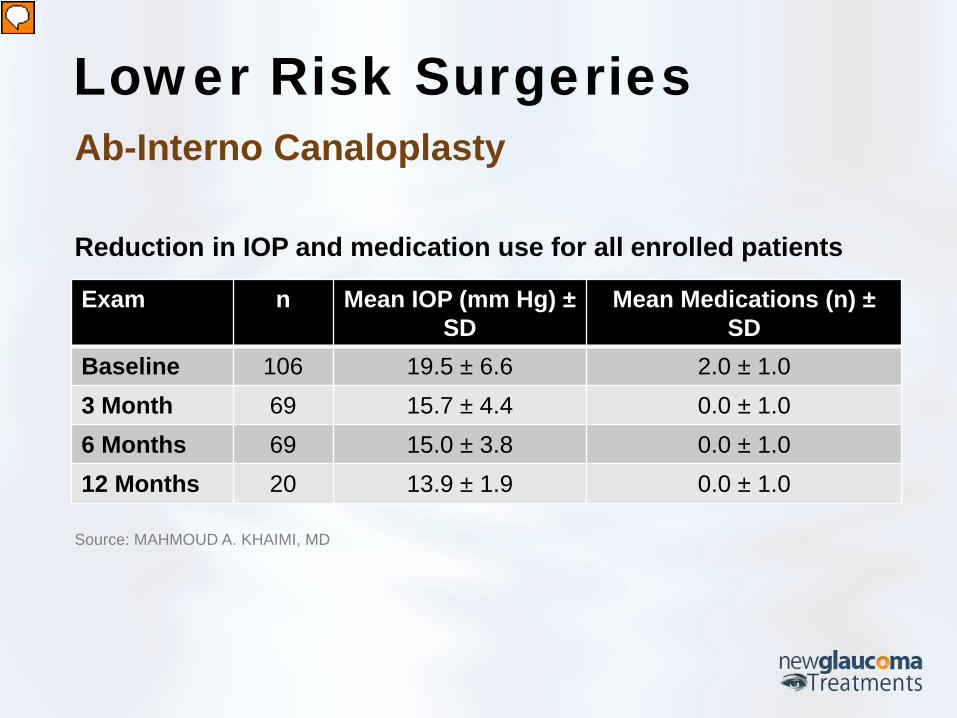
Baseline 106 19.5 ± 6.6 2.0 ± 1.0 3 Month 69 15.7 ± 4.4 0.0 ± 1.0 6 Months 69 15.0 ± 3.8 0.0 ± 1.0 12 Months 20 13.9 ± 1.9 0.0 ± 1.0
Source: MAHMOUD A. KHAIMI, MD
Reduction in IOP and medication use for all enrolled patients
Lower Risk Surgeries Ab-Interno Canaloplasty
Presenter
Presentation Notes
So how does it work? Well, the initial studies, looking one year out basically showed—there’s two: one was by Dr. Khiami, showed a reduction of from 19.5mmHg to 13.9mmHg. The reduction of average medications from 2 to 0.

Exam n Mean IOP (mm Hg) ± SD
Mean Medications (n) ± SD
Baseline 122 18.6 ± 6.4 2.0 ± 1.0 3 Month 88 14.0 ± 3.4 1.0 ± 1.0 6 Months 65 14.1 ± 3.7 1.0 ± 1.0 12 Months 38 12.9 ± 2.0 1.0 ± 1.0
Source: MARK J. GALLARDO, MD
Reduction in IOP and medication use for all enrolled patients
Lower Risk Surgeries Ab-Interno Canaloplasty
Presenter
Presentation Notes
Dr. Gallardo, showed a reduction of 18.6mmHg to 12.9 mmHg. You get 12.9 mmHg! I mean, that is in the range of what the Trabeculectomy studies are showing, right? And mean reduction from 2 medications to 1.
Exam n Mean IOP (mm Hg) ± SD
Mean Medications (n) ± SD
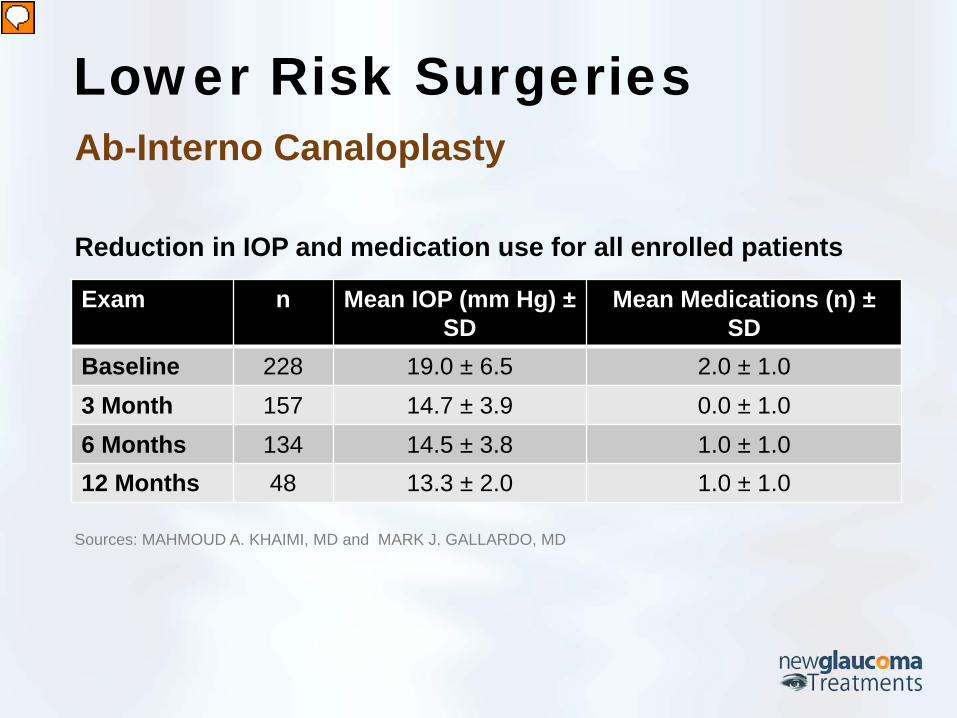
Baseline 228 19.0 ± 6.5 2.0 ± 1.0 3 Month 157 14.7 ± 3.9 0.0 ± 1.0 6 Months 134 14.5 ± 3.8 1.0 ± 1.0 12 Months 48 13.3 ± 2.0 1.0 ± 1.0
Sources: MAHMOUD A. KHAIMI, MD and MARK J. GALLARDO, MD
Reduction in IOP and medication use for all enrolled patients
Lower Risk Surgeries Ab-Interno Canaloplasty
Presenter
Presentation Notes
And if you actually combine the studies—mean IOP from 19 mmHg to 13.3 mmHg, 2 meds to 1. You know these are very impressive results for very safe and very fast surgery.

Trabeculotomy
MIST • GATT • Trabectome • Kahook Dual Blade Trabeculotomy
Presenter
Presentation Notes
Currently Available Incisional Treatments for Glaucoma (Lower Risk Surgeries) Trabeculotomy Micro-invasive Suture Trabeculotomy (MIST)

• 45% Average IOP reduction (2 Years Study)
Low risk procedure
After canaloplasty (with stent)
Lower Risk Surgeries Micro-invasive Suture Trabeculotomy (MIST)
Presenter
Presentation Notes
What else can we do? Well one thing we can do is dilate the canal, the other thing we can do is say, “well, if trabecular meshwork is the primary area of restriction, why don’t we just rip it out or tear it open?” And so, we can do that. It turns out that if you’ve had a patient who’s had Ab-externo Canaloplasty and at some point the pressure is no longer controlled— if they’ve had the Stent — so, if they’ve had the suture placed in the canal, you can go in with micro-forceps or another instrument and pull the suture through. Pulling the suture through rips open the Trabecular meshwork— that’s called Micro-invasive Suture Trabeculotomy. And in a two year study it showed a 45% reduction in intraocular pressure. So, low-risk procedure. Basically, the main risk you have is hyphema (system bleeding in the front of the eye as you open up the trabecular meshwork). That generally goes away on its own. There’s very low risk with any of these angle procedures of cyclodialysis, which can result in hypotony. That’s pretty low risk. So you know the nice thing about canaloplasty is that you can potentially get a double benefit: you can get the initial opening of the canal and then if you need to you can you know pull the suture through the trabecular meshwork.
Gonioscopy-Assisted Transluminal Trabeculotomy (GATT)
• 37.3% mean IOP reduction (2 Yrs Study)
conjunctival-preserving
after failed trabeculectomy or GDD implants
hyphema complication
IOP Spike
Lower Risk Surgeries
Presenter
Presentation Notes
Gonioscopy-Assisted Transluminal Trabeculotomy (GATT) So, there’s also if you’ve got somebody who has not had Canaloplasty you can perform what’s called Gonioscopy-Assisted Transluminal Trabeculotomy. That’s essentially taking that catheter we saw before but instead of just dilating the canal you move the catheter or some people will use a aid…a suture if you want to (you know) get really cheap you don’t want to use an instrument that’s been designed for this it can be done it’s a bit more challenging but in any case you move the suture around the canal and then you take the two end of the suture and you pull through and you rip through the trabecular meshwork. And it also shows a pressure reduction around 40% at two years.

For ocular hypertension or mild open angle
glaucoma
Done with cataract surgery
Limits future surgeries
Expensive
Ab-Interno Trabeculotomy: Trabectome™
Lower Risk Surgeries
Presenter
Presentation Notes
Ab-Interno Trabeculotomy You can get more sophisticated and a whole lot more expensive; Ab-Interno Trabeculotomy has been done using a device called a Trabectome, which has to be done with or after cataract surgery. As with all of the Trabeculotomies, they do limit the potential for future canal-based surgeries but the most—the biggest issue with Trabectome is it’s just—it’s darn expensive.

Lower Risk Surgeries Ab-Interno Trabeculotomy: Trabectome™
Presenter
Presentation Notes
This is the instrument here. And it’s a pretty cool looking instrument… it has a foot plate to protect the posterior wall of the canal and essentially it’s got these electrodes that produce plasma and then it sucks up the trabecular meshwork tissue as it opens up the canal there. So it’s about a fifty-thousand-dollar instrument and then they make you purchase each of the hand pieces so it’s not been that popular when you’ve got these other less expensive options.

Trabeculotomy – Kahook Dual Blade • Incises TM via clear corneal micro incision
• Paired with cataract surgery or alone
• No bleb and no implant left behind
Lower Risk Surgeries
Presenter
Presentation Notes
Kahook Dual Blade Trabeculotomy And one of the more interesting, less expensive options is the Kahook Dual Blade. Basically, it’s like a poor man’s Trabectome. But instead of using a plasma blade, it’s got this neat (I’ll show you) this really neat, design of this blade. There we go… that allows you to safely remove the trabecular meshwork as kind of a strip. So it strips it off. And here you can see the tip of the blade there and it’s got a kind of foot plate and then these two side blades, so you get a sharp tip to get into the trabecular meshwork. And boy, don’t I wish the trabecular meshwork looked that clear and easy to find. Angle base surgery is technically challenging. There’s a high learning curve but once you’ve got it, it can be quite fast and really gentle in terms of the patient experience.

Trabeculotomy – Kahook Dual Blade
Lower Risk Surgeries
Video Credit: Leonard Seibold, MD
Presenter
Presentation Notes
So this is a video of the Trabeculotomy using the Kahook dual blade. And you can see the blades in the angle—It’s getting in the trabecular meshwork. Now is going to come around from the other way and it’s pretty you actually end up with this little strip of trabecular meshwork that if you were interested in it for research or other purpose you can actually take it and send it to pathology. So you can see there’s a little strip on the edge of it. They’ll actually remove that in second.

For ocular hypertension or mild open angle
glaucoma
Done with cataract surgery
Limits future surgeries
Expensive
iStent
Lower Risk Surgeries
Presenter
Presentation Notes
So other angle based surgeries… iStent® The first micro invasive surgical implant to be FDA-approved is the IStent®. For use with ocular hypertension, mild Open Angle Glaucoma—to be done with cataract surgery. And you can see, it’s pretty neat device— it’s this snorkel that is meant to be implanted through the trabecular meshwork, into the canal. The problem is that it limits future surgeries. If you do this you can’t do canaloplasty or other procedures that require access to that area of the canal. And it’s damn expensive! I mean this device is the smallest FDA-approved surgical implant – ever. It’s made of titanium and per ounce this is the most valuable expensive thing you could ever purchase. I think that you know some rare man-made elements that you have to create in the Hadron Collider, maybe more expensive than this—but per ounce. But this is well-reimbursed. The implant itself is a thousand dollars and that’s about what the surgeon is paid for implanting one of these. So they become quite popular.
iStent
Lower Risk Surgeries
Video Credit: Ike Ahmed, MD
Presenter
Presentation Notes
The question is do they work and here’s a video from Ike Ahmed, who is just a truly expert, expert surgeon and has had the ability to be involved in a lot of these new surgical procedures. Have done a lot in terms of, you know, figuring out how best to do these things and this is him performing the surgery and as with all of his surgeries it’s just elegant to watch. You can see him implant the stent and he makes everything look so easy but one of the things about this particular video which underscores the issue with the iStent® is – you’re going to see in this video, that he does not implant one. He does not implant two. He implants three of these in the eye. Now if you implant three of these in the eye you should get an effect. The problem here in the US (separate from Canada) is you’re only going to get paid for one and at a thousand dollars each good luck finding a surgery center that’s going eat the extra two thousand or patient who’s going to be willing to pay for the extra two thousand. You can see how this goes into the canal through the trabecular meshwork and I just love watching his videos. I can’t think of too many too many eye surgeons who don’t. His work is so nice. Anyway, so… his surgical technique—absolutely fantastic!

• One Year Results (IOP < 22mmHg):
– Cataract surgery alone: 50%
– iStent plus CE/IOL: 72%
iStent
Lower Risk Surgeries
Presenter
Presentation Notes
How about the results of the iStent®? Do they match his surgical technique? No they don’t. The one year result of the iStent®—cataract surgery alone is done the pressure is reduced by…. the percentage of patients who achieved a pressure lower than 22 mmHg? 50% – so half of the patients, just from cataract surgery alone, will achieve that pressure under 22 mmHg. How about if you put the iStent® in with cataract surgery? 72%. Okay— so yeah you do get more but the majority of the reduction there is from the cataract surgery. Say, “okay well you know that some of these drops can be pretty expensive right?” I mean we’ve all got patients who are saying, “doctor that drop that you prescribed me the Simbrinza, it’s $250 a month.” Well a year of Simbrinza®—and you know this is paid for itself.
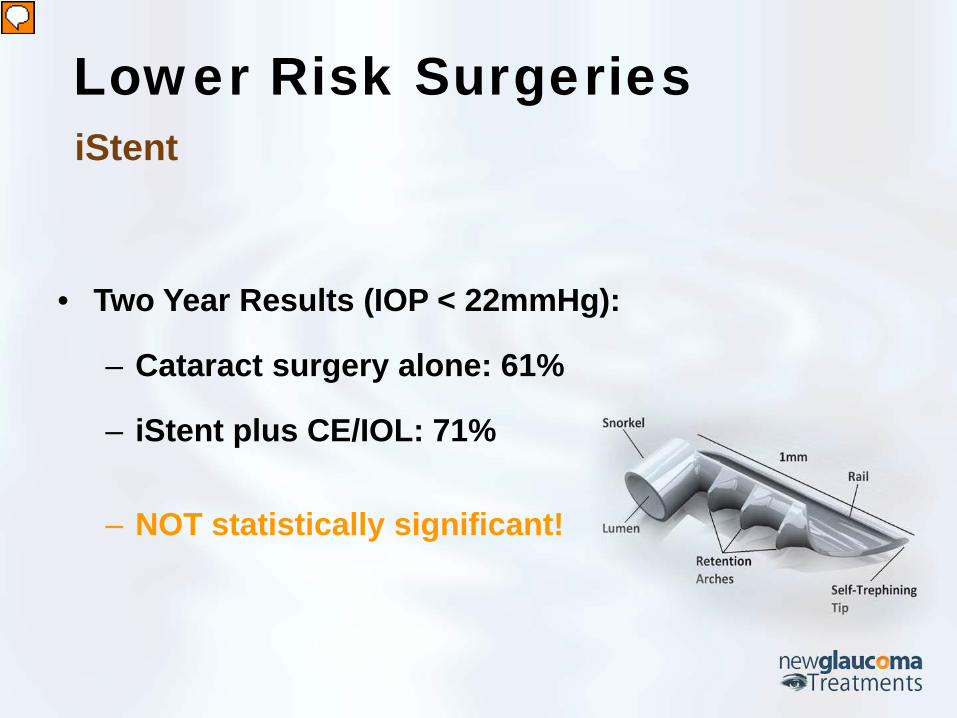
• Two Year Results (IOP < 22mmHg):
– Cataract surgery alone: 61%
– iStent plus CE/IOL: 71%
– NOT statistically significant!
iStent
Lower Risk Surgeries
Presenter
Presentation Notes
So maybe not so impressive when you’re looking at the difference between cataract surgery alone and cataract surgery plus the iStent® but taking a bigger picture it can be a useful option. But two years after surgery there’s no statistically significant difference between those who had cataract surgery alone and those who had cataract surgery plus the iStent®. So it’s easy to put in, it’s currently paid for by insurance, but is it really going to give us a long-term benefit? Probably not.

• For cataract patients with mild to moderate POAG
• Implanted during cataract surgery
• Placed in the supraciliary space
• Can be placed prior to or after most other
glaucoma surgeries
CyPass Micro-Stent® Lower Risk Surgeries
Presenter
Presentation Notes
Cypass® Microstent So what other options are there, well just recently at the end of 2016, the FDA approved the Cypass® Microstent. Now this is exciting because this is using an outflow shunting method that has not been available to us before. That is, it’s also like with the iStent®, only approved for those who are also having cataract surgery. The nice thing about this is because it uses a separate outflow it can be used even in patients who have had or may need to have other glaucoma surgeries.

CyPass Micro-Stent® Lower Risk Surgeries
Presenter
Presentation Notes
I want to show you this this video here…so this is showing the outflow pathway, showing essentially both the pathway through the trabecular meshwork as well as through the through the uvea scleral outflow. You can see that this is an essentially a tube. But it’s a tube is designed in such a way that it can atraumatically sit in the supraciliary space. So you can see that right in the angle, above the ciliary body and shunt fluid into that space. And it’s a very quick procedure. Basically you make an incision, just like you would with cataract surgery. You fill the eye with viscoelastic … (I’m sure we don’t need to see all the details of this) and you have this injector. It’s placed into the angle and then simply inserted into the supraciliary space. And there it is…

• Two Years Results
– 61.2% of patients with CyPass maintained this (vs.
43.5% with cataract surgery alone)
– 32% more effective than cataract surgery alone
(7.0 mmHg vs 5.3 mmHg)
CyPass Micro-Stent® Lower Risk Surgeries
Presenter
Presentation Notes
So the question of course is how well does it work? So if we look at 2-year results (and we do have two year results on this), they looked at patients whose diurnal curve was between (i think it was) 18 mmHg or 6 mmHg. That’s right – 6 mmHg and 18 mmHg and 61.2% patients of the Cypass® maintained this range versus 43.5% with cataract surgery alone. So again, what you see here is that, cataract surgery alone does have a beneficial effect in treating glaucoma. So more however experience this range of diurnal curve with combined cataract surgery and Cypass®. if we look at the absolute pressure reduction 7 mmHg with a Cypass® versus 5.3 mmHg on average which cataract surgery – really doesn’t look that impressive, alright. Less than 2 mmHg but if you look at the percentage difference it was 32% and again what we’re going to find is that with all of these lower risk micro invasive surgeries we don’t necessarily have to think of just one. We could potentially think of building up on different surgeries using different outflow pathways in order to achieve a reduction that could potentially end up in the same range as trabeculectomy or glaucoma drainage devices but without the vision threatening complications.
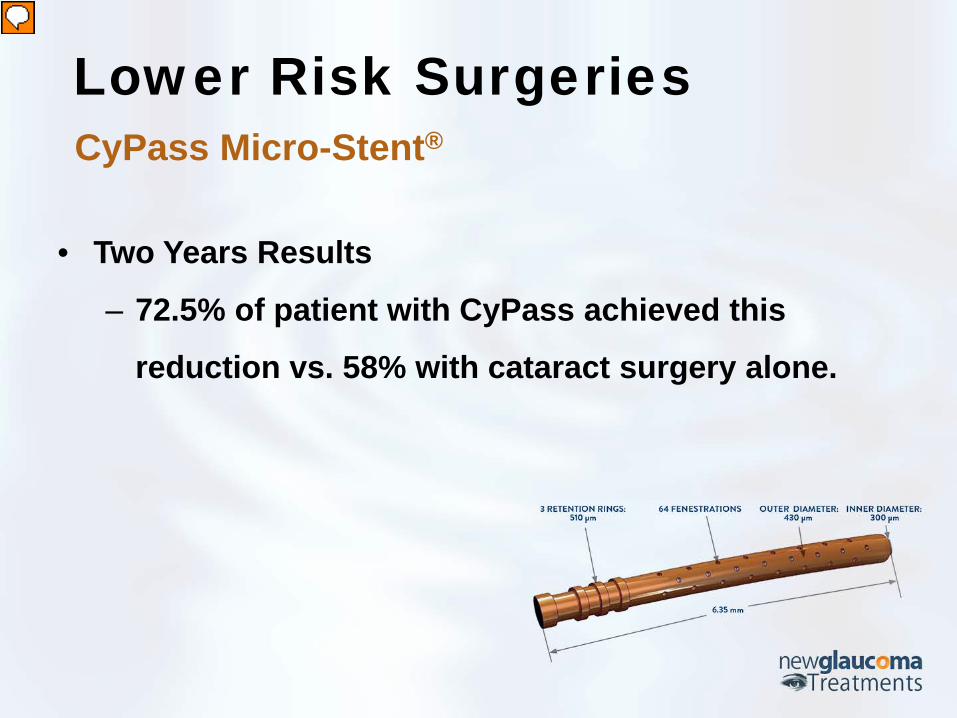
• Two Years Results
– 72.5% of patient with CyPass achieved this
reduction vs. 58% with cataract surgery alone.
CyPass Micro-Stent® Lower Risk Surgeries
Presenter
Presentation Notes
And if we look at the two-year results in terms of the percentage of patients who achieved a non-medicated pressure of 20mmHg or less… so 20mmHg or less without drops, 72.5% of patients for Cypass® achieve this versus almost 60% with cataract surgery alone.

CyPass Micro-Stent® Lower Risk Surgeries
Adverse Event Cataract Surgery
with CyPass (N = 374) n (%)
Cataract Surgery Only (N = 131) n (%)
Subjects with Any Adverse Event 147 (39.3%) 47 (35.9%)
BCVA loss => 10 letters read at/after 3 month postoperative visit 33 (8.8% 20 (15.3%)
AC cell and flare requiring steroid treatment at/after 30 days postoperative3 32 (8.6%) 5 (3.8%)
Worsening in visual field MD by => 2.5 dB as compared with preoperative 25 (6.7%) 13 (9.9%)
IOP => 10 mmHg over baseline at/after 30 days postoperative^ 16 (4.3%) 3 (2.3%)
Corneal edema at/after 30 days postoperative, or severe in nature 13 (3.5% 2 (1.5%)
Presenter
Presentation Notes
In terms of adverse events, there really weren’t that many when you look at the comparison of the combined Cypass® with cataract surgery versus cataract surgery alone, overall, quite similar. So it seems to be a pretty safe, safe device.
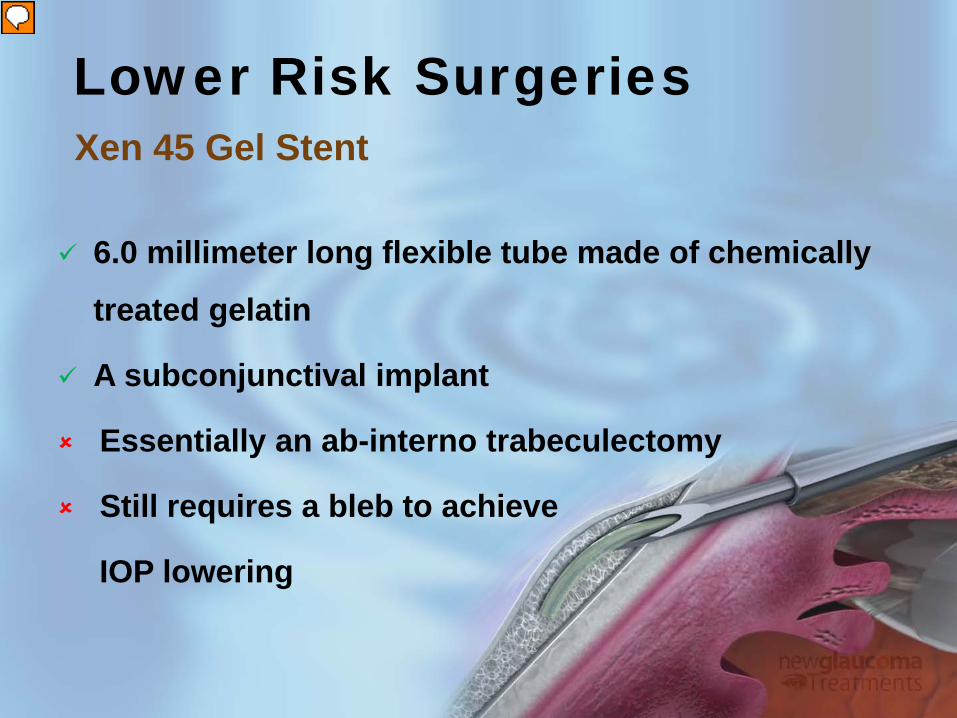
6.0 millimeter long flexible tube made of chemically
treated gelatin
A subconjunctival implant
Essentially an ab-interno trabeculectomy
Still requires a bleb to achieve
IOP lowering
Xen 45 Gel Stent
Lower Risk Surgeries
Presenter
Presentation Notes
Xen® 45 Gel Stent Also approved— at the end of 2016 by the FDA, the Xen® 45 Gel Stent. This is a chemically treated gelatin tube. It’s basically what it is – it’s a tube but it’s been designed so that the aqueous flow through it is restricted in such a way that it reduces the risk of hypotony. So, this is essentially an Ab-Interno method of trabeculectomy. You’re shunting the fluid into the subconjunctival space. So it still requires a bleb to achieve intraocular pressure lowering and as such it still has all of the potential complications or most if not all, that trabeculectomy would.
Xen 45 Gel Stent
Lower Risk Surgeries
• One Year Results (with Cataract Surgery)
– ~ 30% IOP reduction
(average drop from 20.8mmHg to 14.4mmHg)
– ~60% Medication reduction
(average decrease from 2.7 to 1.1)
Xen 45 Gel Stent
Lower Risk Surgeries
Presenter
Presentation Notes
The issue with this is that although it shares many of the complications with Trabeculectomy and although it’s much faster and in some ways easier to do, it doesn’t seem to do quite as well as Trabeculectomy in terms of pressure reduction. So the average drop of 30% from 20.8% to 14.4% at 1 year – not quite as impressive as trabeculectomy.

• Three Year Results (w & w/o Cataract Surgery)
– ~ 40% IOP reduction
– ~ 75% Medication reduction
– 5% of participants required additional
glaucoma surgery to
achieve IOP control.
Xen 45 Gel Stent
Lower Risk Surgeries
Presenter
Presentation Notes
Three year results looked pretty good 40% reduction, 75% medication reduction, and about 5% of participants needed to go on to additional surgery, which is pretty typical for glaucoma surgeries.
Hyphema
Short- or long-term hypotony
(IOP that is too low)
loss of vision (6.2% long-term
loss)
Xen 45 Gel Stent
Lower Risk Surgeries
Presenter
Presentation Notes
But as I said (was saying) earlier you have these issues of short and long term hypotony, potential for loss of vision—that’s not insignificant, right? 6.2 % long-term loss. So that’s on par with, really, trabeculectomy.

Cataract Surgery
Lower Risk Surgeries
• Cataract surgery alone on an eye with glaucoma will
sometimes lower the pressure in the eye.
Presenter
Presentation Notes
Cataract Surgery Cataract surgery – I’m not going to belabour on this point. You’ve seen already from the studies I showed earlier that cataract surgery alone can be effective with glaucoma. So for many of our patients who are kind of doing pretty well with their glaucoma – we’d like the pressure to be a little bit lower, they may be having some progression. If they’ve got cataracts or cataracts that are ready for surgery, and they’re not maxed out on medications, then cataract surgery alone, for many of these patients, is perfectly reasonable. The issue though is, if they are maxed out on medications and you perform cataract surgery and they have a pressure spike, which is not uncommon among glaucoma patients of cataract surgery, then what are you going to do? Then your only option is Diamox. So patients who are on max-tolerated medical therapy and need cataract surgery, we will generally consider combining the cataract surgery with one of these MIGS procedures. But if they’re not maxed out it’s perfectly reasonable to consider just cataract surgery alone in those who have mild to moderate glaucoma.

Next Generation Plumbing
What’s “In the Pipeline”?
MEDICATIONS | SURGERY
Presenter
Presentation Notes
Next Generation Plumbing | What’s “In the Pipeline” of Medications and Surgery So what’s in the pipeline? Next-generation medications and surgeries in the pipe line.

Next Generation Plumbing
ROCK & NET Inhibitors | Adenosine Receptor Agonists | Modified Prostaglandin Analogs
MEDICATIONS
Presenter
Presentation Notes
Medications Quickly, the medications that are—that you’re going to see—some of these are already available say in Japan and elsewhere but hopefully we’ll see these in the US. There’s essentially three new classes of medications:

Medications Rho-Kinase “ROCK” Inhibitors
“Opens the drain” – ‘Relaxes’ the Trabecular
Meshwork
Presenter
Presentation Notes
ROCK & NET Inhibitors The Rho-Kinase or the ROCK inhibitors—they open the drain by relaxing the trabecular meshwork. The Norepinephrine Transporter Inhibitors or the NET Medications—they “turn on the faucet”.

Medications Norepinephrine Transporter (“NET”) Inhibitors
“Turns down the faucet” – Reduces aqueous fluid
Presenter
Presentation Notes
There’s one an FDA trials right now, which is a ROCK/NET. So it uses both of these. Just like the alpha-2 agonists, you could potentially get both a reduction in the flow (reduction in the production of fluid) as well as an improvement in the outflow—so that’s very exciting.

Medications Adenosine Receptor Agonists
• Work by increasing outflow
through Trabecular
Meshwork (TM)
Presenter
Presentation Notes
Adenosine Receptor Agonists They work by increasing the outflow through the trabecular meshwork.
Medications Modified Prostaglandin Analogs
• PG plus Nitric Oxide
– Nitric Oxide relaxes the TM
and Schlemm’s Canal
Presenter
Presentation Notes
Modified Prostaglandin Analogs Now, these are basically Prostaglandin Analogue plus a Nitric Oxide. So they’re generally (you can think of some of these as) Prodrugs. They enter the anterior chamber, they’re split up into the prostaglandin and a nitric oxide. Nitric oxide relaxes the trabecular meshwork and Schlemm’s canal increasing outflow.

Next Generation Plumbing
iStent Supra | Hydrus™ Microstent | InnFocus MicroShunt | Stegmann Canal Expander
SURGERY
Presenter
Presentation Notes
Next Generation Plumbing | What’s “In the Pipeline” of Medications and Surgery Glaucoma Surgeries But what’s really exciting and what I’m going to end on here is the next generation of plumbing – the surgeries.

• Implanted alone or at the
time of cataract surgery
• IOP reduction of at least
– 20% (12 mos.)
Surgery iStent Supra
Presenter
Presentation Notes
iStent® Supra® The iStent Supra® is basically the the Glauko’s version of the Cypass® and it’s exciting but we’ve seen Cypass®—this isn’t that different. I’m sure there’s some nuances and one may end up working better than the other—have fewer complications—but what interests me is what follows.

Video Credit: Dr. Jose I. Belda
Surgery iStent Supra
Presenter
Presentation Notes
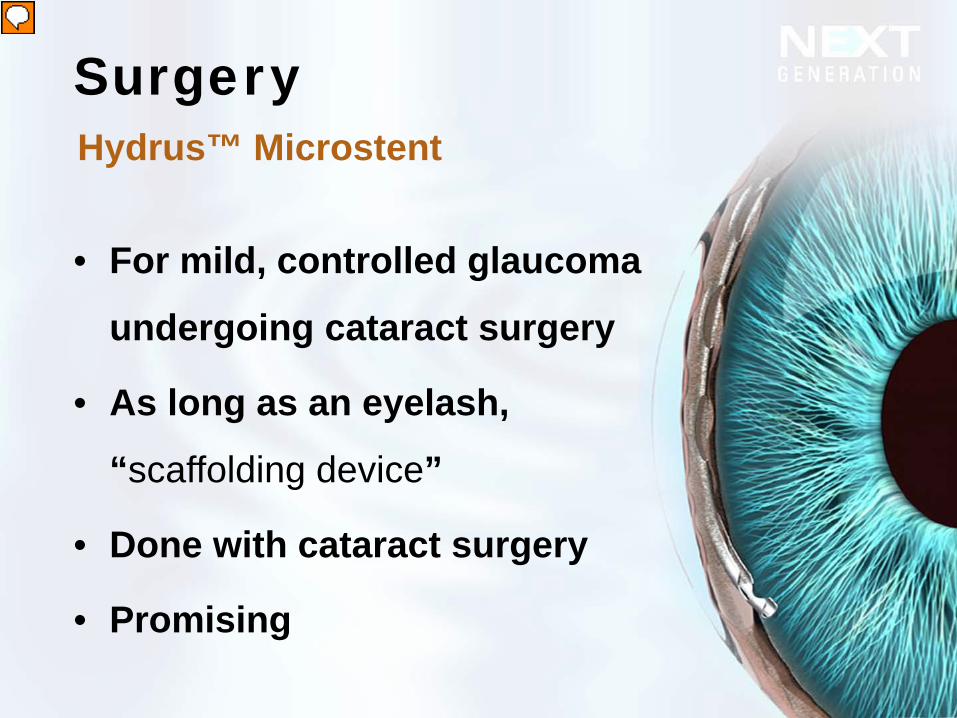
• For mild, controlled glaucoma
undergoing cataract surgery
• As long as an eyelash,
“scaffolding device”
• Done with cataract surgery
• Promising
Surgery Hydrus™ Microstent
Presenter
Presentation Notes
Hydrus™ Microstent The Hydrus™ Microstent – this is actually a way of stenting the canal. So we’ve seen with the Ab-interno Canaloplasty (ABiC) how we could dilate the canal but the problem is: you’ve dilated—that’s nice—angioplasty of the heart remember, many times the vessels would scar back down. So then they started putting stents in the vessels in the heart. Well, the same thing (we hope) we’ll be able to do with the Schlemm’s canal: dilate the canal and leave a stent. So, in this case, it’s a small little stent, only as long as an eyelash. It’s done with cataract surgery, seems quite promising. Another Ike Ahmed video, which is again fun to watch but given the time I think that we’ll hold off unless somebody wants to see it after the talk. I’m willing to stay around and do some theatre here.

Surgery Hydrus™ Microstent
Video Credit: Dr. Ike Ahmed
Presenter
Presentation Notes
Ike Ahmed Channel on YouTube Published on May 2, 2013 “The hydrus micro-stent by Ivantis is a microinvasive glaucoma surgery (MIGS) procedure designed to bypass resistance and scaffold Schlemm's canal to enhance aqueous flow through the conventional outflow system. It is designed with an inlet and three windows to provide direct flow into the canal as well through the stretched inner wall, thereby enhancing the effective filtration area, and scaffold the canal open to provide flow in collector channels and aqueous veins.” Source: https://youtu.be/qebLSny_nHY
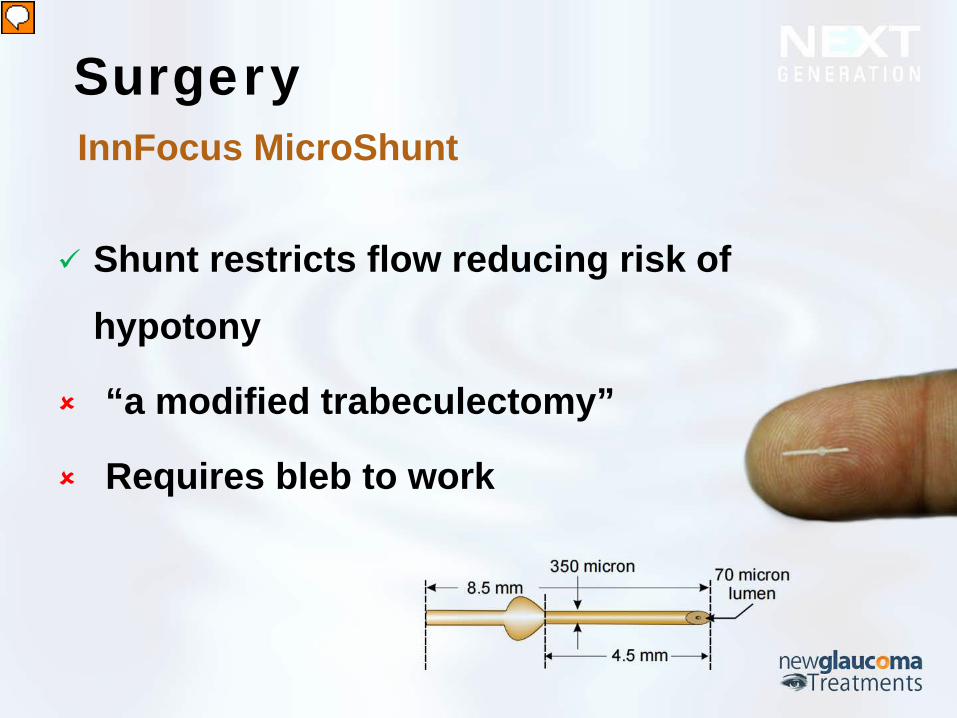
Shunt restricts flow reducing risk of
hypotony
“a modified trabeculectomy”
Requires bleb to work
Surgery InnFocus MicroShunt
Presenter
Presentation Notes
InnFocus MicroShunt® The other is the InnFocus MicroShunt®—These things are not yet FDA-approved but they’re in trials and then maybe. The InnFocus MicroShunt® is essentially— it’s an Ab-externo, unfortunately. It’s essentially a controlled trabeculectomy. So instead of creating a flap and punching a hole, you essentially place this device that limits flow. So very much like the XEN® Gel Stent, which you could do from inside the eye. This is similar but requires that you come from the outside of the eyes. Now, personally, now that the XEN® Gel Stent has been approved, I can’t imagine why anybody would want to take the trouble to use this but it might have… it might have a following—we’ll see. The Xen® Gel has the advantage of both being an Ab-interno – so quick and easy to do, as well as the fact that it’s already FDA-approved. So it’s kind of you know first one the market. So, if I was an investor I would not be investing on the InnFocus but I’m not.

• Tube-shaped “scaffolding device”
• Placed into Schlemm’s canal
• Keeps up to half of the canal open –
permanently.
Surgery Stegmann Canal Expander
Presenter
Presentation Notes
Canaloplasty with Stegmann Canal Expander This is the one I’m most excited about and I think you’ll see why. We’ve been talking about minimally invasive glaucoma surgery and the problem with it; potentially, being minimally effective specially when you compare it to cataract surgery. So Dr. Stegmann, who created Canaloplasty thought, “this is great stuff but can we make it better?” And so, in terms of what we just talked about—with the Hydrus as a scaffold from the inside—If that will…“can I create a scaffold that can be used with canaloplasty?” So he created this tube-shaped scaffolding device that’s placed in Schlemm’s canal and can keep —and this is the key: the Hydrus and these other scaffolds are very, very small (only a few clock hours). In the case of this device, it can keep—up to half the canal open permanently. And this video (I think) is worth seeing.

Surgery Stegmann Canal Expander
Video Credit: Matthias C. Grieshaber, MD
Presenter
Presentation Notes
Video: Stegmann Canal Expander by Dr. Matthias Grieshaber And this is by Dr. Matthias Grieshaber, who is an outstanding glaucoma surgeon (overseas). And you can see, this is actually—he’s already done the canaloplasty. He’s pulled the catheter back and you saw the viscoelastic gel at the end of it. So he’s dilated the canal. Now here is this stent. You can see it’s a pretty long stent. What he’s going to stent is on… it’s essentially a guide wire. So what he’s going to do is he’s going to thread this guide wire back through the dilated canal and now you can see at the end of this guide wire is this stent – he’s going to place this stent, again using the guide wire to help it move along. He’s going to move this into the canal. Now this is such a long stent that he wouldn’t be able to do this without the guide wire. And now he’ll pull the guide wire out, holding on to the stent, and then once this is done he’ll then do the same thing on the other side but then close up as he would any canaloplasty.

• Success Rate
Surgery Stegmann Canal Expander
Presenter
Presentation Notes
Success Rate So is it successful? It certainly looks like it should be. Well, we now have two year results and if we look at the success—recall earlier, I was talking about success rates with the different minimally invasive glaucoma surgeries in terms of the percentage of patients who had pressures at or below 20-21mmHg—the problem with these studies, of value is kind of a different outcome but if you recall those compare that to this: For those had a final intraocular pressure of less than or equal to 21mmHg, there is a 98% success rate. Almost a 100% of those who had the surgery had a final pressure of <= to 21 mmHg. That is absolutely outstanding! And if you you want to lower the threshold make it more challenging, <=18 mmHg almost 90% … so, 88%. And if you dropped it even further, <=16 mmHg, it did an 86% success rate. That is unheard of for a procedure with the safety profile of Canaloplasty. And the Stegmann Canal Expander did not significantly increase the risk over and above what one would expect from Canaloplasty.
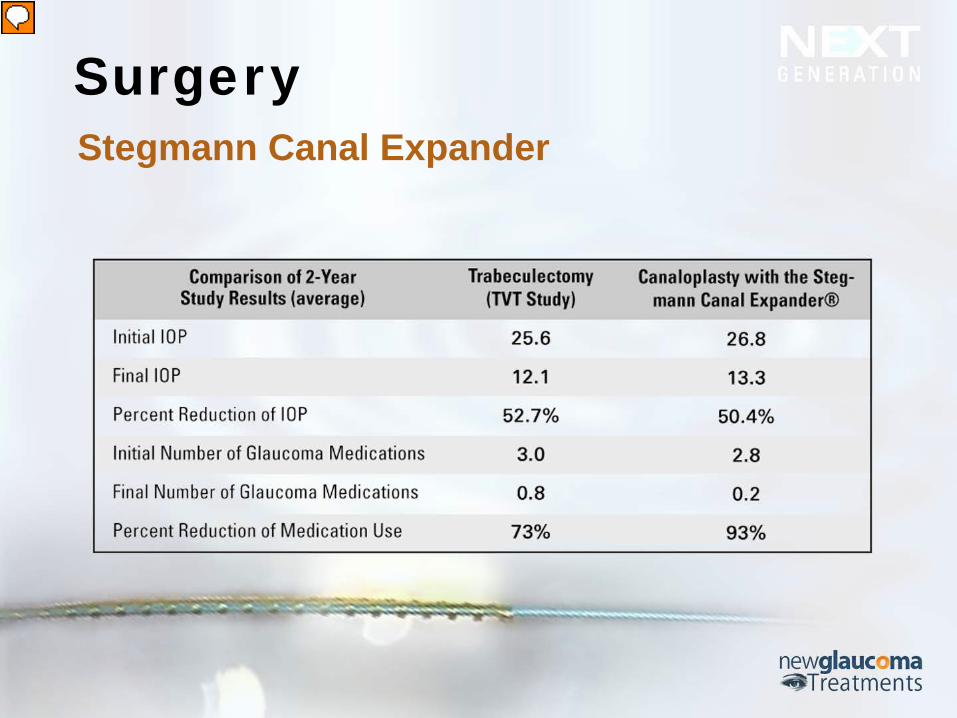
Surgery Stegmann Canal Expander
Presenter
Presentation Notes
How does the “gold standard” of trabeculectomy compare? And here’s the key slide I want to show you because we’ve started out talking about medications and the fact that all of these medications have risks and side effects and issues that bother our patients. We moved into surgery—the penetrating surgeries that have been around for over 50 years (a half a century) with all of the risks. And we said, “well the problem is nothing’s as good as Trabeculectomy”. The Holy Grail is to get a safer procedure that is as effective as Trabeculectomy. And if we look at the two-year study result of the “Trabeculectomy Versus Tube Study”, which is the one of the most commonly referenced studies looking at the outcome of Trabeculectomy and we compare that with a two-year results of the Canaloplasty with Stegmann Canal Expander… Let’s take a look at this. Initial IOP in this two studies (the TVT studies again). Trabeculectomy 25.6, the Canaloplasty 26.8 (so similar starting). Final IOP – 12.1mmHg in the TVT for Trabeculectomy, 13.3 for this Stegmann Canal Expander with Canaloplasty – 1mmHg of difference. We can also look at Percent Reduction (of IOP) – 52.7 in the Trabeculectomy, 50.4 with Canaloplasty with Stegmann Canal Expander. Initial glaucoma medications – 3 in Trabeculectomy, 2.8 on Canaloplasty with Stegmann Expander (again, very similar). Final number of glaucoma medications – 0.8 with Trabeculectomy and 0.2 with Canaloplasty with Stegmann Expander. And if we look at the percent reduction of medication use – 73% with Trabeculectomy, 93% with Canaloplasty with Stegmann. So it is—at least based on this comparison (one can feel pretty confident that this is), not inferior. Not significantly inferior to Trabeculectomy in terms of pressure reduction. But in terms of safety profile and the limitations that one would have to place on the patient, there’s no question that Trabeculectomy is the loser here and Canaloplasty with Stegmann Canal Expander is the winner. Now the only issue here is that unlike the other things I’ve shown you in the pipeline, this Stegmann Canal Expander is much further out. So the best we can get today with this is that Canaloplasty alone. We don’t yet have (and will probably not have for quite a few years if ever—depending on the FDA and what they decide) have this (Stegmann Canal Expander) but i am so incredibly hopeful that we will get that because i think that is the minimally invasive glaucoma surgery that is also maximally effective.
Presenter
Presentation Notes
Presentation Closing Remark So, a lot of interesting stuff coming down the pipeline. Of course, what we get and what we can just kind of look overseas and wish we had is something that we won’t know and it’s out of our control. (But you know) hopefully I’ve at least introduced a couple of new things to those of you and refresh your memory on some old things.

THANK YOU
(626) 289 7856 [email protected]
Presenter
Presentation Notes
And I’m going to open it up for questions and any questions that don’t get answered today this afternoon, please feel free to give me a call or an email. I’ve put—that’s my office number there and my email, but I’m also willing to give out my cell phone number to anybody who would like to call me personally. Alright, thank you.