Current PTFE Grafts
8
Current PTFE Grafts A Biomechanical, Scanning Electron, and Light Microscopic Evaluation K. C. HANEL, M.D., C. McCABE, M.D., W. M. ABBOTT, M.D., J. FALLON, M.D., J. MEGERMAN, PH.D. Two currently available brands of PTFE grafts (Goretex® and Impras) were studied in a canine femoral artery model to de- termine whether changes in the manufacturing processes of the two grafts, which increased their strength, had altered the bio- physical properties and the histological reactivity of either graft. Both grafts were found to be similar except for differ- ences in their suturability. Their in vivo dynamic compliances were almost identical (1.2 ± 0.35 vs. 1.2 ± 0.45). Scanning electron microscopy showed endothelialization of the grafts only adjacent to the anastomoses, and light microscopy dem- onstrated similar degrees of histologic incorporation by the host tissues, though of slower tempo than that previously de- scribed. These results are examined and discussed with regard to the suitability of this model for characterizing new arterial prostheses of small to medium diameter. XPANDED POLYTETRAFLUOROETHYLENE GRAFTS are L the most popular of the synthetic alternatives to autologous vein, with over 200,000 grafts implanted in the last five years. Since they were first used experi- mentally as a venous substitute by Soyer in 19721 and as an arterial bypass by Matsumoto in 1973,2 they have been utilized for a number of clinical purposes including access for hemodialysis, peripheral arterial bypass, por- tasystemic shunting, venous replacement, aortopulmon- ary shunting, ureteral replacement, and coronary artery bypass grafting. Much information concerning the bio- physical properties of the available PTFE grafts (Goretex® and Impra®), such as strength, durability, porosity, and healing properties, was accrued between 1971 and 1976 from clinical and experimental studies. Indeed, many of the principles on which development Grafts were supplied by W. L. Gore & Associates, Flagstaff, Ar- izona and Impra Incorporated, Tempe, Arizona. Dr. Kevin C. Hanel is supported by an Applied Health Sciences Fellowship, N.H.M.R.C. (Australia). Reprint requests: W. M. Abbott, M.D., Massachusetts General Hospital, Department of Surgery, Boston, Massachusetts 02114. Submitted for publication: August 26, 1981. From the Massachusetts General Hospital, Department of Surgery, Boston, Massachusetts of new synthetic prostheses is based were derived from these studies. There has been little done, however, since 1975, when major structural changes were introduced by the man- ufacturers in an effort to increase graft strength and minimize the aneurysmal dilatation that characterized the early grafts. Gore added a tube of reinforcing mesh to their grafts, and the Impra grafts were thickened. There have been reports that the reinforcing mesh of Goretex grafts decreases their compliance and also in- terferes with fibroblastic infiltration. This present study was organized to examine these features and to char- acterize and compare the properties of these two grafts, particularly their handling qualities, viscoelasticity, mode of surface healing, and histologic maturation. Materials and Methods Grafts were interposed in the femoral arteries of mongrel dogs weighing 25-30 kg. Anesthesia was in- duced with intravenous pentobarbital (60 mg/kg) and maintained with intermittent injections of the drug as required. Animals were intubated, and respiration was maintained with a Harvard ventilator. All procedures were performed under a full sterile protocol, and intra- venous fluids were infused at the rate of 300 ml per hour. No heparin was employed. The femoral arteries were exposed from the level of the inguinal ligament to 2 inches above the knee, and flow in the arteries was measured with a Statham SP 2202® electromagnetic square wave flowmeter. The craniofemoral branch of the femoral arteries was ex- posed and cannulated with 2-mm polyethylene tubing, 0003-4932/82/0400/0456 $00.90 © J. B. Lippincott Company 456
Transcript of Current PTFE Grafts

Current PTFE Grafts
A Biomechanical, Scanning Electron, and Light Microscopic Evaluation
K. C. HANEL, M.D., C. McCABE, M.D., W. M. ABBOTT, M.D., J. FALLON, M.D., J. MEGERMAN, PH.D.
Two currently available brands of PTFE grafts (Goretex® andImpras) were studied in a canine femoral artery model to de-termine whether changes in the manufacturing processes of thetwo grafts, which increased their strength, had altered the bio-physical properties and the histological reactivity of eithergraft. Both grafts were found to be similar except for differ-ences in their suturability. Their in vivo dynamic complianceswere almost identical (1.2 ± 0.35 vs. 1.2 ± 0.45). Scanningelectron microscopy showed endothelialization of the graftsonly adjacent to the anastomoses, and light microscopy dem-onstrated similar degrees of histologic incorporation by thehost tissues, though of slower tempo than that previously de-scribed. These results are examined and discussed with regardto the suitability of this model for characterizing new arterialprostheses of small to medium diameter.
XPANDED POLYTETRAFLUOROETHYLENE GRAFTS areL the most popular of the synthetic alternatives toautologous vein, with over 200,000 grafts implanted inthe last five years. Since they were first used experi-mentally as a venous substitute by Soyer in 19721 andas an arterial bypass by Matsumoto in 1973,2 they havebeen utilized for a number of clinical purposes includingaccess for hemodialysis, peripheral arterial bypass, por-tasystemic shunting, venous replacement, aortopulmon-ary shunting, ureteral replacement, and coronary arterybypass grafting. Much information concerning the bio-physical properties of the available PTFE grafts(Goretex® and Impra®), such as strength, durability,porosity, and healing properties, was accrued between1971 and 1976 from clinical and experimental studies.Indeed, many of the principles on which development
Grafts were supplied by W. L. Gore & Associates, Flagstaff, Ar-izona and Impra Incorporated, Tempe, Arizona. Dr. Kevin C. Hanelis supported by an Applied Health Sciences Fellowship, N.H.M.R.C.(Australia).
Reprint requests: W. M. Abbott, M.D., Massachusetts GeneralHospital, Department of Surgery, Boston, Massachusetts 02114.Submitted for publication: August 26, 1981.
From the Massachusetts General Hospital, Department ofSurgery, Boston, Massachusetts
of new synthetic prostheses is based were derived fromthese studies.
There has been little done, however, since 1975, whenmajor structural changes were introduced by the man-ufacturers in an effort to increase graft strength andminimize the aneurysmal dilatation that characterizedthe early grafts. Gore added a tube of reinforcing meshto their grafts, and the Impra grafts were thickened.There have been reports that the reinforcing mesh ofGoretex grafts decreases their compliance and also in-terferes with fibroblastic infiltration. This present studywas organized to examine these features and to char-acterize and compare the properties of these two grafts,particularly their handling qualities, viscoelasticity,mode of surface healing, and histologic maturation.
Materials and Methods
Grafts were interposed in the femoral arteries ofmongrel dogs weighing 25-30 kg. Anesthesia was in-duced with intravenous pentobarbital (60 mg/kg) andmaintained with intermittent injections of the drug asrequired. Animals were intubated, and respiration wasmaintained with a Harvard ventilator. All procedureswere performed under a full sterile protocol, and intra-venous fluids were infused at the rate of 300 ml perhour. No heparin was employed.The femoral arteries were exposed from the level of
the inguinal ligament to 2 inches above the knee, andflow in the arteries was measured with a Statham SP2202® electromagnetic square wave flowmeter. Thecraniofemoral branch of the femoral arteries was ex-posed and cannulated with 2-mm polyethylene tubing,
0003-4932/82/0400/0456 $00.90 © J. B. Lippincott Company
456

CURRENT PTFE GRAFTS 457TABLE 1. Hemodynamic Parameters Obtained at Implantation
of PTFE Grafts
Goretex (Artery) Impra (Artery)
In vivo dynamiccompliance(%mmHgx lo-2) 1.2 ± 0.35 6.63 ± 3.0 1.2 ± 0.45 5.38 ± 2
External diameter(mm) 6.06 ± 0.15 4.94 ± 0.49 6.24 ± 0.4 4.94 ± 0.58
Flow (ml/min) 100 ± 40 91 ± 39
which was connected to a Statham SP 23dB® pressuretransducer to monitor and record the femoral pressure.The pulsatile radial displacement of the walls of thefemoral artery was measured with a cantilever trans-ducer, as previously described.3 The femoral artery di-ameter, change in diameter, and corresponding pulsepressure were used to calculate the dynamic in vivocompliance of the host artery. In vivo dynamic com-pliance is expressed by the equation:
C = AD/DAP (% mmHg X 10-)
where AD is the change in external diameter, D is thediastolic external diameter, and AP is the pulsatile pres-sure.
Goretex and Impra PTFE grafts, 5 mm in internaldiameter and 6-7 cm long, were inserted into the fem-oral arterial circulation by two experienced vascularsurgeons (K.C.H., C.McC) simultaneously. The typeof graft inserted by each was alternated in successiveexperiments. End-to-end anastomoses were performedwith continuous 6.0 prolene with the aid of loop mag-nification. Observations as to the ease of handling ofthe grafts and the amount of anastomotic hemorrhagewere noted at the time of graft insertion.
Circulation was reestablished and graft blood flowmeasurements made. The in vivo dynamic complianceof the grafts was determined using the cantilever andpressure data. The polyethylene tubes were left in situand placed subcutaneously so that they could be usedfor repeated angiography in the follow-up period. Thewounds were closed in layers.The animals were inspected postoperatively at reg-
ular intervals, and the status of the grafts assessed bypalpation, doppler ultrasound examination, and an-giography. The latter was performed routinely in allanimals at one, four, eight, and 12 weeks through theimplanted cannulae to detect any ongoing pathologicprocess in the grafts, such as anastomotic stenosis oraneurysmal dilation. Angiography was also performedat other times if there was any doubt as to graft patency.If these lines became nonfunctional, standard transbra-chial aortography was performed.
All occluded grafts were harvested at the time thatfailure was detected, while patent grafts were harvestedat three months. Occluded grafts were excised andplaced in formalin, while the patent grafts were per-fused and fixed at arterial pressure to maintain normalartery and graft diameters and to preserve the delicateintimal surface morphology in its in vivo state. Theprocess consisted of isolating the proximal and distalfemoral arteries, without disturbing the graft or its an-astomoses. Ringer's lactate was perfused through thegraft at arterial pressure, and when the perfusate wasfree of blood, 2.5% glutaraldehyde in sodium cacodylatebuffer was substituted for it. The grafts were perfusedwith this solution for 30 minutes at arterial pressure.The specimens were removed, divided longitudinally,
and placed in buffered cacodylate solution. Both an-astomoses and selected segments along the graft weresectioned and stained with hemotoxylin and eosin, elas-tic tissue, and Masson's trichrome stain and subjectedto microscopic examination. Corresponding sections ofthe specimen were critically point dried, sputter coatedwith gold palladium, and examined in an AMR 1400scanning electron microscope.
Results
Twenty-six grafts were implanted in 13 dogs. Onedog died on the first postoperative day, and one graftoccluded within the first week due to a technical prob-lem related to the angiography catheter. This resultedin 12 Goretex grafts and 11 Impra grafts remaining
TABLE 2. Life Table of Patency Rates for Goretex and Impra Grafts
Goretex Impra
Interval (weeks) OP 0-1 1-2 2-4 4-8 8-12 OP 0-1 1-2 2-4 4-8 8-12
Number 13 13 8 7 6 5 13 13 7 6 5 5Occluded 0 4 1 1 0 1 0 4 1 1 0 1Lost 0 1* 0 0 it 0 0 2*t 0 0 0 0Cumulative patency (%) 100 70 61.25 52.5 52.5 42 100 76.7 65.73 54.8 54.82 43.82
* Lost graft' death.t Lost graft, infected.
t Lost graft, technical error.
Vol. 195 - No. 4

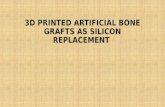
FIG. 1. Examples of SEM,typical of both grafts withendothelium growing fromthe host artery across theanastomosis for a variabledistance of 0.5 to 1.2 cm. a.Arterial spindle-shaped en-dothelium aligned in thedirection of blood flowstreaming towards the anas-tomosis. b. Endothelial cellslining the graft havechanged shape to a thinner,rounded configuration sim-ilar to venous endothelium.c. Advancing edge of en-dothelium merging with thefibrinous cellular lining inthe middle of the graft.Cells become irregular inshape and orientation. d.Lining of midgraft. e. Ar-tifactual disruption of en-dothelium in graft showinghow thin the new itima isand the configuration of thePTFE fibrils below. f. Nor-mal arterial endothelium.Cells aligned longitudinally.Transverse folds prominentdue to underlying collagenstrands, muscle contrac-tion, and corrugated inter-nal elastic lamina.
... ......

CURRENT PTFE GRAFTS
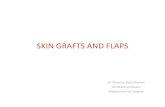
FIG. 2. H & E Impra.Showing absence of rein-forcing mesh, open mesh-work, and an acellular zonein the midwall. The lumenis at the top and the adven-titial surface below. Origi-nal magnification X 100.
available for study. A further Goretex graft was ex-cluded at five weeks because it became infected.
Both grafts were pliable and easy to insert. It wasnoted that the Impra grafts tended to tear longitudinallyat the needle holes, requiring that less tension be usedin tying the sutures; however, this was not a major tech-nical problem. A series of experiments on the sutureholding capacity of ten randomly selected samples ofthe two grafts using a tensionometer revealed that Gor-etex had approximately five times the suture holdingcapacity of the Impra grafts (810 ± 168 gm vs. 134± 17 gm). The in vivo dynamic compliance of the twografts was almost identical (1.2 ± 0.35 for Goretex and1.2 ± 0.45 for Impra). This was compared with an av-erage femoral artery compliance of 6.26 ± 2.8. Bloodflow in the grafted arteries was similar, and they wereisodiametric (see Table 1).The timing and nature of graft occlusion were iden-
tical for both grafts in each dog (Table 2). The three-month cumulative patency for Goretex was 42% (4/12)and for Impra 43.8% (4/1 1), as illustrated in Table 2.Five grafts in both groups failed within the first twoweeks due to acute thrombosis. There were two furtherfailures in both groups at four weeks and eight weeksdue to an accumulation of pale thrombus at the anas-tomoses. Two failed at ten weeks, again due to acutethrombosis. There was no difference between grafts that
occluded and those that remained patent with regardto graft and artery diameters or blood flow at implan-tation. Initial flow in occluded grafts was 101 ± 0.7, andin the patent grafts (123.5 ± 21.3 ml/min [NS]).Arteriography did not demonstrate any progressive
anastomotic stenosis or dilatation of any graft. Noneof the grafts that occluded demonstrated any progres-sive pathologic process that could have been implicatedin their failure. Two grafts exhibited narrowing of thedistal artery at two weeks; however, this did not persistin subsequent angiograms and was presumably due tospasm.
Scanning electron microscopy demonstrated identicalpatterns of intimal healing in both grafts. A thin pannusof endothelial cells extended across the anastomosesfrom the host artery into the grafts for distances thatvaried from 0.5 to 1.2 cms. The neointima in the middleof the grafts was devoid of endothelial cells and con-sisted of a red cell-fibrin coagulum (Fig. 1). The en-dothelial cells as they extended into the grafts lost theelongated spindle shape characteristic of arterial sur-faces and flattened out in a regular uniform manner.At their leading edge they became irregular in size,shape, and orientation. The cells separated and mergedwith the meshwork of fibrin and red cells. These findingsare illustrated in Fig. 1.
Examination by light microscopy again demonstrated
Vol. 195 * No. 4 459

Ann. Surg. * April 1982HANEL AND OTHERS
FIG. 3. Anastomotic regionof Goretex graft harvestedat three months showing in-timal hyperplasia. The lu-minal surface is at the top.Original magnification X46.
*
no difference in the amount or timing of cellular in-corporation between the two grafts. Both showed anaccumulation of inflammatory cells along the outsidesurface of the grafts, and there was an ingrowth ofmesenchymal cells into the internodal spaces from boththe outer and luminal surfaces. There was an innermidwall zone that was relatively acellular comparedwith the outer zones. This middle area was filled withan eosinophilic proteinaceous transudate (Fig. 2). Ma-ture collagen was recognizable in the interstices of bothgrafts, although its amount differed widely in differentareas. It seemed to be in greater concentration adjacentto the anastomoses. Neocapillary formation was notedonly at the outer surface of the grafts. Two patent grafts(one Goretex and one Impra) demonstrated a minimaldegree of intimal hyperplasia at their distal anastomoses(Fig. 3), although not enough to cause obstruction.None of the occluded grafts had these lesions, andthrombosis was the recognizable mode of failure in allcases.The reinforcing mesh was visible on the Goretex
grafts. It was noted, however, that there was fibroustissue infiltrating through small, regularly spaced per-forations in the mesh (see Fig. 4), and there was norecognizable difference in fibrous incorporation be-tween the two grafts.
Discussion
The experiments in this study were performed tocharacterize the biophysical properties of and the his-tological response to the two current models of ex-panded polytetrafluoroethylene (ePTFE) grafts thathave a prominent place in the vascular surgeon's ar-mamentarium for the reconstruction of diseased smallto medium-sized arteries. The physical properties ofePTFE are alleged to have many of the attributesthought necessary for a vascular prosthesis. The basematerial, polytetrafluoroethylene, is one of the mostchemically inert polymers known, and the graft engen-ders very little tissue or blood reaction. It is imperviousto blood due to its electrophobic nature and does notrequire preclotting. Because its surface is electronega-tive, it is purported to be "nonthrombogenic" by someinvestigators. It is easy to handle because of its sponge-like pliability, although there may be problems due toexcessive bleeding through the suture holes, as was ev-ident in this study. The stretching process used in themanufacture of PTFE results in a highly porous matrixof solid nodes of material, interconnected by multiplefine fibrils. The porosity allegedly allows complete in-corporation by the host tissue.The material does not undergo biological or chemical
460

CURRENT PTFE GRAFTS
FIG. 4. H & E Goretex.Shows reinforcing mesh on
the inferior (adventitial)surface of the graft but withcells passing into the graftfrom the surrounding tissuethrough perforations in themesh. Original magnifica-tion X160.
deterioration; however, the earlier models of both Impraand Goretex did have a high incidence of aneurysmaldilatation because they had insufficient radial strengthto resist the cold flow (creep) of the material at arterialpressure. This complication was reported in 5/25 pa-
tients with A.V. shunts by Owens and colleagues.4Campbell5 also reported four aneurysms in 50 patientswith femoropopliteal grafts. What is more disturbingabout this second report is that no aneurysms developedin 300 porcine and canine implants that had been stud-ied prior to the use of the grafts in humans. This raisesdoubts as to the appropriateness of applying some ex-
perimental results in animals to humans. The problemof dilatation was obviated by changes in the manufac-turing processes of both grafts. The Gore Company, in1975, added a thin circumferential hoop of PTFE tothe original tube to increase the radial strength of thegraft. A further modification has been the perforationsin the outer wrapping, which were evident in the graftsin this study. In 1977, the Impra Company increasedthe radial strength of their graft by increasing the wallthickness from 0.5 to 0.75 mm. The bursting strengthsof both grafts have been assessed by independent lab-oratories, and both have been found to be strong enoughto resist distension at arterial pressure, with Goretexbeing approximately three times as strong as Impra.6
Because of the changes, dilatation seems no longer tobe a problem with either type of graft.
It has been alleged that the reinforcing mesh that ispart of the current model Goretex is not conducive tocomplete graft healing, as it interferes with fibroblasticinfiltration into the interstices of the graft. Mohring andcolleagues,7 in a study of Impra and Goretex graftsharvested from dialysis patients, conclude that the twografts behaved differently. The open structure of theImpra allowed free ingrowth of connective tissue cells,resulting in an organized cellular neointimal lining. Incomparison, the ingrowth of fibroblasts into the Goretexgrafts was less pronounced, and they had an almost cell-free pseudointima. Similar observations were reportedby Morgan and his colleagues8 in a study of Goretexgrafts used in humans as arteriovenous shunts. Theyattributed a higher infection rate in these grafts to theconfiguration of the reinforcing mesh, which did notallow proper tissue ingrowth. These observations are notconfirmed in the present study, in which both grafts are
seen to have similar degrees of histologic incorporation,and the reinforcing mesh seems to have no effect on theamount of fibroblastic infiltration into the graft due tothe perforations in the wrapping. The susceptibility ofsynthetic grafts to infection and the correlation of thissusceptibility with the completeness of healing have
461Vol. 195.o NO. 4

HANEL AND OTHERS
been recently studied by Moore, who demonstrated thatboth Impra and Goretex have similar resistances tobacteremic infectability.9The pioneer work of Weslowski on prosthetic grafts
introduced the concept of graft porosity and its role ingraft healing.'0 The rate and degree of histologic mat-uration of PTFE grafts related to their porosity has alsobeen documented, but most of this work was in theearlier thin or nonreinforced tubes. Campbell reportedthat the porosity of PTFE was an important determi-nant of its patency."' Grafts that had a pore size lessthan 22,q had an 88% patency, compared with only 53%in those with pores greater than 34,t. He attributed thebetter results to the smaller pore size, which alloweda more controlled ingrowth of fibroblastic tissue. Themore porous grafts allowed more blood to enter theirinterstices; the blood became static, activated the co-
agulation system, and resulted in a more thrombogenicinterface. These results, however, were completely con-
tradictory to those of Matsumoto2 and Florien,'2 whoobtained patency rates of 100% in grafts with a poresize of 100,u. This discrepancy may be explained by theshort grafts used in the latter two studies, which were
only 2.5 to 4 cm long. In the present study the endo-thelial ingrowth across the anastomoses in the patentgrafts was up to 1.2 cm, and so some of the grafts inthe cited studies may have endothelialized from theproximal and distal host artery. The high patency ratesin such cases would not have been influenced by trans-mural healing. It would seem that the results obtainedby implanting short grafts, or from a high-flow exper-
imental model such as the canine aorta, have little rel-evance to the behavior of prosthetic grafts in the dis-eased human femoropopliteal site. This is supported bythe study of Walley et al.,'3 who demonstrated that longPTFE grafts (12 cm) implanted into the canine ilio-femoral region had a 0% patency rate irrespective ofpore size or type of anastomosis, while short grafts (4cm) had 45% patency in the carotid (high-flow) and22% in the femoral (low-flow) region at three months.The degrees of "healing" of both grafts in this study,
while very similar to each other, are not as rapid as hasbeen reported in previous studies. Shack'4 reportedmesenchymal cells within the walls of the graft by eightdays and complete incorporation by fibrous tissue by25 days. Campbell described neocapillary formation by35 days." In none of our patent 12-week grafts was
neocapillary formation evident in the interstices of thegrafts. Both of these authors described a thin, firmlyadherent, glistening neointima comprising endothelial-like cells. In none of our grafts did this type of neointimaform. Scanning electron microscopy confirmed that the
only endothelium that was present occurred adjacentto the proximal and distal anastomoses and that themiddle of the grafts was lined by a coagulum of fibri-nous and blood elements only.The importance of the viscoelastic properties of syn-
thetic and biological arterial grafts has been empha-sized by previous studies in our laboratory'3"5 and byothers.'6 These studies have suggested that matchingthe mechanical properties of prosthetic grafts to thoseof the host artery will diminish suture line stresses andallow more efficient propagation of pulsatile energy.Various anecdotal reports from surgeons that Impragrafts were more compliant than Goretex were one ofthe factors that inspired the present study. However,the grafts were found to have almost identical compli-ances, one sixth that of the normal canine femoral ar-tery. This implies that a similar problem of mismatchexists with both PTFE grafts. Such a mismatch, how-ever, may have played a role in graft thromboses, whichoccurred without other obvious cause.
One of the major objectives of this study, the char-acterization of the biological response to the grafts, hasproduced some results that are inconsistent with pre-
vious findings. This refers particularly to the slower rateof fibrous incorporation, the lack of capillaries withinthe graft interstices, the nature of the neointima, andthe rarity of subintimal hyperplasia as a mode of graftfailure. This latter entity has been implicated as themajor cause of occlusion in a number of studies.'6"17 Inthis study it was not responsible for any failures, al-though it did occur to a minimal degree in two patentgrafts. The short interval between occlusion and harvestof the grafts in this study may have resulted in theanastomotic pathology being recognized as thrombusrather than organized thrombus, which could possiblybe misinterpreted as intimal hyperplasia. Most of theinconsistencies with previous studies may be explainedby differences in graft length, site of implantation, typeof anastomosis, and blood flow. The low-flow, smalldiameter, long femoral artery graft would seem to bea much more appropriate model than others that havebeen used. The other aim of the study, that of com-
paring the two grafts, has produced less equivocal re-
sults. Both grafts were almost identical with regard totheir less than ideal mechanical properties and host in-corporation. It would seem that the choice betweenthem should be based on handling qualities, availability,and cost.
AcknowledgmentThe authors wish to acknowledge the significant contributions made
by Mr. Gilbert L'Italien and Ms. Bobbie Feldman in the executionof this work.
462 Ann. Surg. - April 1982

Vol. 195 * No. 4 CURRENT PTFE GRAFTS 463References
1. Soyer T, Lempinen M, Cooper B, et al. A new venous prosthesis.Surgery 1972; 72:864.
2. Matsumoto H, Hasegawa T, Fuse K, et al. A new vascular pros-thesis for a small caliber artery. Surgery 1973; 74:519.
3. Baird RN, Kidson IG, L'Italien GJ, Abbott WM. Dynamic com-pliance of arterial grafts. Am J. Physiol 1977; 233:568.
4. Owens ML, Shinaberger JH, Wilson SE, Wang SMS. Aneurys-mal enlargement of ePTFE AV fistulas. Dialysis Transplan-tation 1978; 7:692.
5. Campbell CD, Goldfarb D., Roe R. A small arterial substitute,expanded microporous polytetrafluoroethylene. Patency versusporosity. Ann Surg 1972; 182:138.
6. Bergen JJ, Harris JP, Rudo ND, Yao JST. In: Veith FJ, ed.Current Critical Problems in Vascular Surgery. New York:Appleton Century Crofts. (In press).
7. Mohring K, Asbach HW, Bersch HW, et al. Clinical implicationsof pathomorphological findings in vascular prostheses. In:Hawkins R, ed. Dialysis Transplantation Nephrology. GreatBritain: The Pitman Press, 1978; 582.
8. Morgan AP, Damin GJ, Lazarus JM. Failure modes in secondaryvascular access for hemodialysis. ASAIO 1978; 1:44.
9. Moore WS, Malone JM, Keown K. Prosthetic arterial graft ma-terial. Arch Surg 1980; 115:1379.
10. Weslowski SA, Golaski WM, Sauvage LR, et al. Considerationsin the development of small artery prostheses. 1968; ASAIO14:43.
11. Campbell CD, Brooks DS, Webster MW, Balinson HT. The useof expanded micro porous polytetrafluoroethylene for limb sal-vage: a preliminary report. Surgery 1976; 79:485.
12. Florian A, Cohn LH, Dammin GJ, Collins JJ. Small vessel re-placement with Goretex. Arch Surg 1976; 111:267.
13. Walley BD, James PM, Meredith JH, et al. Expanded micro-porous polytetrafluoroethylene as canine arterial bypass or re-placement graft. Arch Surg 1978; 113:863-866.
14. Shack RB, Neblett WW, Ritchie RE, Dean RH. Expanded poly-tetrafluoroethylene as dialysis access grafts: a serial study ofhistology and fibrinolytic activity. Am Surg 1977; 43:817.
15. Walden R, L'Italien GJ, Megerman J, Abbott WM. Matchedelastic properties and successful arterial grafting. Arch Surg1980; 115:1166.
16. Sieffert KB, Albo D, Knowlton H, Lyman DJ. Effect of elasticityof prosthetic wall on patency of small diameter arterial pros-thesis. Surg Forum 1979; 30:206.
17. Oblath RW, Buckley FO, Green RM, et al. Prevention of plateletaggregation and adherence to prosthetic vascular grafts byaspirin and dipyrimadole. Surgery 1978; 84:37.