Critical evaluation of plasma and LDL oxidant-trapping potential in hemodialysis patients
7
Kidney International, Vol. 56 (1999), pp. 747–753 Critical evaluation of plasma and LDL oxidant-trapping potential in hemodialysis patients THAO NGUYEN-KHOA,ZIAD A. MASSY,VE ´ RONIQUE WITKO-SARSAT,MARC THE ´ VENIN, MALIK TOUAM,GUY LAMBREY,BERNARD LACOUR,TILMAN B. DRU ¨ EKE, and BE ´ ATRICE DESCAMPS-LATSCHA INSERM U507, Divisions of Nephrology and Biochemistry, Necker Hospital, Paris, and Nephrology Division, Beauvais Hospital, Beauvais, France Critical evaluation of plasma and LDL oxidant-trapping poten- Chronic renal failure (CRF) is associated with an in- tial in hemodialysis patients. creased risk of atherosclerotic cardiovascular disease [1, 2], Background. We investigated whether the total peroxyl rad- which represents the major cause of mortality in patients ical-trapping antioxidant potential (TRAP) assay, which has on long-term hemodialysis (HD) [3–5]. Oxidative stress, recently been proposed as a gauge of oxidative stress, could defined as a rupture in the pro-oxidant–antioxidant bal- serve to evaluate plasma and low density lipoprotein (LDL) ance in favor of the former, largely participates in the antioxidant state in hemodialysis (HD) patients. Methods. TRAP was determined by the lag time of the chemi- pathogenesis of atherosclerosis [4, 5]. Interestingly, oxi- luminescence reaction induced by azo-initiator-catalyzed lino- dative stress has recently been incriminated in the pro- leic acid peroxidation in the plasma and corresponding LDL gression of renal diseases [6, 7], and culminates in dialysis preparations of 23 HD patients and 22 healthy subjects. Antiox- patients who combine a massive generation of reactive idant systems, including glutathione peroxidase (GSH-Px), oxygen species at each dialysis session [8–12] with a chronic ascorbate, vitamin E, and uric acid, oxidative stress markers deficiency in the major antioxidant systems [13–16]. In- including malondialdehyde (MDA), carbonyls, and advanced creased serum concentrations of lipid peroxidation by- oxidation protein products (AOPP), and lipids, including cho- lesterol and triglycerides, were also determined in the plasma. products such as malondialdehyde (MDA) have been Results. Both plasma and LDL-TRAP were significantly in- reported in HD patients, although with conflicting results creased in HD patients despite decreased GSH-Px and ascor- [17, 18]. More recently, we reported the presence of bate and increased MDA, carbonyl, and AOPP plasma levels. advanced oxidation protein products (AOPPs) as novel Plasma TRAP values were closely related to both uric acid markers of oxidative stress and proinflammatory media- and AOPP levels, and LDL-TRAP values were related to tri- tors in both dialyzed [19] and nondialyzed CRF patients glycerides and AOPP levels. In vitro studies showed that: (a) plasma TRAP of control plasma increased regularly with sup- [20]. Interestingly, Miyata et al suggested that oxidative plementation of uric acid, although not reaching that of HD stress could also participate in the formation of advanced plasma with similar uric acid levels; (b) the addition of human glycation end-products (AGEs) [21, 22] in HD patients, serum albumin-AOPP also regularly increased control plasma and we reported the accumulation of the AGE pentosi- TRAP, but was close to that of HD plasma with similar AOPP dine with the progression of CRF [23]. levels; and (c) LDL-TRAP was increased following LDL en- The total peroxyl radical-trapping antioxidant poten- richment with triglycerides. Conclusion. Our study demonstrates that TRAP is not a tial (TRAP), measured by the ability of a biological fluid relevant parameter for evaluating plasma or LDL antioxidant to resist 2,29-azobis [2-amidinopropane] hydrochloride capacity in HD patients, due to the high plasma levels of uric (ABAP)-induced linoleic acid peroxidation, has recently acid, triglycerides and AOPP, which by themselves do not exert been proposed as a useful tool for determining the global efficient antioxidant activity in vivo, but in vitro are able to antioxidant capacity of plasma in patients with oxidative scavenge the peroxyl radicals involved in the TRAP assay. stress-associated diseases such as diabetes [24], sickle cell disease [25], schizophrenia [26], and cystic fibrosis [27]. Jackson et al have reported an increased plasma Key words: total peroxyl radical-trapping antioxidant potential, antiox- idant, low density lipoprotein, carbonyls, malondialdehyde. TRAP in HD patients and related this finding to the presence of high circulating levels of uric acid, which Received for publication October 9, 1998 because of the profound ascorbate deficiency in these and in revised form March 15, 1999 Accepted for publication March 22, 1999 patients, has no efficient antioxidant activity in vivo [28]. The generation of oxidized low-density lipoprotein 1999 by the International Society of Nephrology 747
Transcript of Critical evaluation of plasma and LDL oxidant-trapping potential in hemodialysis patients

Kidney International, Vol. 56 (1999), pp. 747–753
Critical evaluation of plasma and LDL oxidant-trappingpotential in hemodialysis patients
THAO NGUYEN-KHOA, ZIAD A. MASSY, VERONIQUE WITKO-SARSAT, MARC THEVENIN,MALIK TOUAM, GUY LAMBREY, BERNARD LACOUR, TILMAN B. DRUEKE,and BEATRICE DESCAMPS-LATSCHA
INSERM U507, Divisions of Nephrology and Biochemistry, Necker Hospital, Paris, and Nephrology Division,Beauvais Hospital, Beauvais, France
Critical evaluation of plasma and LDL oxidant-trapping poten- Chronic renal failure (CRF) is associated with an in-tial in hemodialysis patients. creased risk of atherosclerotic cardiovascular disease [1, 2],
Background. We investigated whether the total peroxyl rad- which represents the major cause of mortality in patientsical-trapping antioxidant potential (TRAP) assay, which has on long-term hemodialysis (HD) [3–5]. Oxidative stress,recently been proposed as a gauge of oxidative stress, could
defined as a rupture in the pro-oxidant–antioxidant bal-serve to evaluate plasma and low density lipoprotein (LDL)ance in favor of the former, largely participates in theantioxidant state in hemodialysis (HD) patients.
Methods. TRAP was determined by the lag time of the chemi- pathogenesis of atherosclerosis [4, 5]. Interestingly, oxi-luminescence reaction induced by azo-initiator-catalyzed lino- dative stress has recently been incriminated in the pro-leic acid peroxidation in the plasma and corresponding LDL gression of renal diseases [6, 7], and culminates in dialysispreparations of 23 HD patients and 22 healthy subjects. Antiox- patients who combine a massive generation of reactiveidant systems, including glutathione peroxidase (GSH-Px),
oxygen species at each dialysis session [8–12] with a chronicascorbate, vitamin E, and uric acid, oxidative stress markersdeficiency in the major antioxidant systems [13–16]. In-including malondialdehyde (MDA), carbonyls, and advancedcreased serum concentrations of lipid peroxidation by-oxidation protein products (AOPP), and lipids, including cho-
lesterol and triglycerides, were also determined in the plasma. products such as malondialdehyde (MDA) have beenResults. Both plasma and LDL-TRAP were significantly in- reported in HD patients, although with conflicting results
creased in HD patients despite decreased GSH-Px and ascor- [17, 18]. More recently, we reported the presence ofbate and increased MDA, carbonyl, and AOPP plasma levels.
advanced oxidation protein products (AOPPs) as novelPlasma TRAP values were closely related to both uric acidmarkers of oxidative stress and proinflammatory media-and AOPP levels, and LDL-TRAP values were related to tri-tors in both dialyzed [19] and nondialyzed CRF patientsglycerides and AOPP levels. In vitro studies showed that: (a)
plasma TRAP of control plasma increased regularly with sup- [20]. Interestingly, Miyata et al suggested that oxidativeplementation of uric acid, although not reaching that of HD stress could also participate in the formation of advancedplasma with similar uric acid levels; (b) the addition of human glycation end-products (AGEs) [21, 22] in HD patients,serum albumin-AOPP also regularly increased control plasma
and we reported the accumulation of the AGE pentosi-TRAP, but was close to that of HD plasma with similar AOPPdine with the progression of CRF [23].levels; and (c) LDL-TRAP was increased following LDL en-
The total peroxyl radical-trapping antioxidant poten-richment with triglycerides.Conclusion. Our study demonstrates that TRAP is not a tial (TRAP), measured by the ability of a biological fluid
relevant parameter for evaluating plasma or LDL antioxidant to resist 2,29-azobis [2-amidinopropane] hydrochloridecapacity in HD patients, due to the high plasma levels of uric (ABAP)-induced linoleic acid peroxidation, has recentlyacid, triglycerides and AOPP, which by themselves do not exert
been proposed as a useful tool for determining the globalefficient antioxidant activity in vivo, but in vitro are able toantioxidant capacity of plasma in patients with oxidativescavenge the peroxyl radicals involved in the TRAP assay.stress-associated diseases such as diabetes [24], sicklecell disease [25], schizophrenia [26], and cystic fibrosis[27]. Jackson et al have reported an increased plasmaKey words: total peroxyl radical-trapping antioxidant potential, antiox-
idant, low density lipoprotein, carbonyls, malondialdehyde. TRAP in HD patients and related this finding to thepresence of high circulating levels of uric acid, whichReceived for publication October 9, 1998because of the profound ascorbate deficiency in theseand in revised form March 15, 1999
Accepted for publication March 22, 1999 patients, has no efficient antioxidant activity in vivo [28].The generation of oxidized low-density lipoprotein 1999 by the International Society of Nephrology
747

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential748
(ox-LDL) is a common feature of oxidative stress, andhigh levels of ox-LDL have been reported in HD patients[29, 30]. However, by their triglyceride content and theircapacity to retain liposoluble antioxidants such as vita-min E, LDLs also contribute to the antioxidant status[31]. LDL-TRAP has been studied in normal subjects[32] but has not yet been investigated in HD patients.
This study was aimed at evaluating whether or not theTRAP assay could be used to quantitate the redox stateof both plasma and LDL of HD patients assessed bycirculating plasma levels of antioxidants including gluta-thione peroxidase (GSH-Px), ascorbate, vitamin E, anduric acid and oxidative stress markers, including MDA,carbonyls, and AOPP.
METHODS
Patients
Twenty-three nonsmoking HD patients (11 males and12 females; mean age 6 sd, 63 6 15 years) enteredthis study after giving informed consent. Patients with
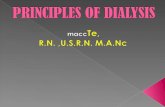
Fig. 1. Time course of luminol-amplified chemiluminescence (CL) ofchronic hepatitis, hematological and inflammatory disor-2,29-azobis [2-amidinopropane] hydrochloride (ABAP)-catalyzed lino-ders, cancer, and immunosuppressive therapy were ex-leic acid peroxidation in the presence of normal plasma (a representative
cluded. End-stage renal disease was secondary to inter- experiment). The CL reaction proceeds through the sequence of initia-tion, propagation, and termination phases and is characterized by itsstitial nephropathy (7 patients), polycystic kidney diseaselag time (t lag), rate, and peak.(4 patients), glomerulonephritis (3 patients), diabetic ne-
phropathy (2 patients), nephroangiosclerosis (1 patient),or unknown origin (6 patients). All patients were dia-lyzed for more than three months for 210 to 270 minutes Total peroxyl radical-trapping antioxidantthree times per week with diacetate or triacetate mem- potential assaybrane filters using bicarbonate dialysate. All patients had
Plasma and LDL-TRAP were measured by the delaya serum intact parathyroid hormone level below 250 pg/ml.in the luminol-amplified chemiluminescence (CL) pro-Twenty-two nonsmoking healthy subjects (9 males andduction induced by linoleic acid peroxidation initiated13 females, aged 41 6 13 years) were recruited amongby ABAP [32]. Briefly, the generation of peroxyl radicalsthe laboratory staff and served as controls.was induced by the injection of 100 ml of 250 mm ABAP(Polysciences Inc., Warrington, PA, USA) in the lumino-Materialsmeter (AutoLumat LB 953; Berthold, Wildbad, Ger-If not otherwise indicated, chemicals were purchasedmany) cuvette containing the reaction mixture, that is,from Sigma Chemical Co. (St. Louis, MO, USA).20 ml of 120 mm linoleic acid, 50 ml of 3 mm luminol(5-amino-2,3-dihydro-1,4-phtalazinedione), and 30 ml ofBlood collection, plasma and low-densityplasma in 470 ml of PBS or 100 ml of LDL in 400 ml oflipoprotein isolationPBS. The CL reaction proceeds through the sequence
Venous blood (10 ml) from HD patients and controlsof initiation, propagation, and termination phases and
was collected in standard tubes containing 5 mm ethyl-is characterized by its lag time (t lag), rate, and peak
enediaminetetraacetic acid (EDTA). In HD patients,(Fig. 1). The CL t lag is lengthened by the presence of
blood was drawn from the arteriovenous fistula just be-antioxidants such as Troloxt (6-hydroxy-2,5,7,8-tetra-
fore the dialysis session. Following centrifugation (600methylchroman 2-carboxylic acid; Aldrich, Milwaukee,
g 3 10 min, 48C), plasma was stored at 2808C. LDLsWI, USA), a water-soluble tocopherol that is used as
from 10 HD patients and 10 control subjects were iso-a standard for quantitating TRAP measurement [34].
lated by precipitation of 1 ml of plasma with 7 ml of 64Assuming that each Troloxt molecule neutralizes two
mm citrate buffer, pH 5.05, containing 50,000 IU/literperoxyl radicals, TRAP is expressed as follows:
sodium heparinate [33]. After centrifugation, the pelletwas resuspended in 1 ml 100 mm phosphate-buffered TRAP (lmol/liter) 5
[t lagSample/t lagTrolox] 3 Trolox (lmol/liter) 3 2saline (PBS), pH 7.4, containing 0.15 m sodium chloride.

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential 749
Lipid and protein oxidative stress markers specifically determining ascorbate, the reduced form ofvitamin C using ascorbate oxidase [37]. Briefly, two ali-Plasma levels of MDA were measured by a highlyquots of 100 ml of plasma were prepared, one with 40sensitive, synchronous fluorescence technique [35].ml of 4 UI/ml ascorbate oxydase and the other with 40Briefly, 100 ml of plasma were mixed to 750 ml of thiobar-ml of PBS. The reaction mixture consisted of 10 ml ofbituric acid reagent (Sobioda, Montbonnot, France) insample with 30 ml of PBS and 300 ml of reagent preparedacidic condition and boiled for one hour. After extractionwith 10 ml of 300 mm acetate buffer, pH 3.6, 1 ml of 10with 3 ml of N-butanol, the spectrum of the organic layermm 2,4,6-tripyridyl-s-triazine (TPTZ) in 0.04 n HCl, andwas recorded on a spectrophotometer (Shimadzu RF540,1 ml of 20 mm ferric chloride. The reduction of Fe31-Roucaire, Courtaboeuf, France) between 500 and 600TPTZ in the Fe21-TPTZ blue form was measured atnm keeping a constant interval, that is, Dl of 14 nm593 nm after an incubation of 45 seconds at 378C. Thebetween excitation and emission wavelengths. The MDAascorbate plasma level was calculated by the differenceconcentration was calculated by the fluorescence peakbetween absorption of sample with and without ascor-intensity at 553 nm using tetramethoxypropane, whichbate oxidase. Ascorbate (0 to 250 mm) (Merck, Darm-produces MDA, as the standard.stadt, Germany) was used as the standard.Plasma levels of carbonyls were measured by a spec-
Plasma levels of vitamin E were determined by a re-trophotometric procedure using 2,4-dinitrophenylhy-verse high-performance liquid chromatography (HPLC)drazine (DNPH) [36]. Briefly, plasma was treated withprocedure as described in [38], after deproteinization of10 mm DNPH in 2.5 mm HCl. After incubation for one200 ml of plasma with 200 ml of anhydrous HPLC-gradehour at room temperature in the dark, deproteinizationethanol. Briefly, after vitamin E extraction with 400 ml ofwith 20% (wt/vol) trichloracetic acid was realized at 48C.HPLC-grade heptane, the organic layer was evaporatedThe pellet was washed three times in ethanol/ethyl ace-under a nitrogen stream and the dry extract was redis-tate (1:1, vol/vol) and then solubilized at 378C for 30solved in 400 ml of HPLC-grade methanol. One hundredminutes in 6 m guanidine hydrochloride, pH 2.3. Carbonylsmicroliters of the sample were injected in a 250 3 4.6 mm,were measured using molar absorption coefficient e of5 mm ODS-C18 column (Satisfaction RP18AB; Cluzeau,22,000 m21cm21 at 370 nm and expressed in nmol/mg ofSte Foy La Grande, France), and eluted with HPLC-protein measured at 280 nm by referring to bovine serumgrade methanol at a flow rate of 2 ml/min. Detection wasalbumin.by ultraviolet absorbance at 292 nm. Internal and externalPlasma levels of AOPP were measured as previouslystandards consisted in a-tocopherol and a-tocopheroldescribed in our laboratory [19] by a spectrophotometricacetate, respectively.assay using a microplate reader MR5000 (Dynatech,
Plasma levels of uric acid were determined using aParis, France) at 340 nm. Briefly, 200 ml of a fivefoldHitachi 917 analyzer (Boehringer Mannheim, Meylan,dilution of plasma in 10 mm PBS were placed in a 96-wellFrance) with commercially available kits.plate (Nunc-immuno plate; Nunc, Roskilde, Denmark)
and mixed with 20 ml acetic acid. AOPP concentrationsLipid determinationswere expressed in mmol/liter by referring to standard
Cholesterol and triglycerides were determined in thewells, containing 200 ml of chloramine-T solution (0 toplasma and/or LDL preparations (for triglycerides) using100 mm), 10 ml of 1.16 m potassium iodide, and 20 ml ofa Hitachi 917 analyzer.acetic acid.
Advanced oxidation protein productsAntioxidant systems in plasmain vitro preparationSeleno-dependent GSH-Px activity was measured in
Human serum albumin (HSA; fraction V; CalBio-plasma using tert-butyl hydroperoxide as described previ-chem, Mendon, France) was oxidized with hypochlorousously [6]. Briefly, the reaction mixture consisting of 1 mmacid (HOCl) as described by Witko-Sarsat et al [19].reduced glutathione, 1 mm tert-butyl hydroperoxide, 230Briefly, HSA (100 mg/ml) was incubated at room temper-IU/liter of yeast glutathione reductase, 0.143 mm nicotin-ature for 15 minutes with 100 mm HOCl (HOCl:proteinamide adenine dinucleotide phosphate (NADPH), andmolar ratio of 60:1) and then dialyzed overnight against1.5 mm potassium cyanide in 100 mm PBS. The assay10 mm PBS, pH 7.4.kinetics were calculated using molar absorption coeffi-
cient e for NADPH of 6.22 3 1023 m21 cm21. GSH-PxStatistical analysisactivity was expressed in millimoles of NADPH oxidized
Data were expressed as means 6 sd. Statistical analy-per milliliter (IU/liter).sis was performed using the Mann–Whitney U-test forPlasma levels of vitamin C were measured by an auto-nonparametric data. Simple regression analysis and Spear-mated enzyme-linked ferric-tripyridyltriazine spectro-
photometric assay (Cobas Fara, Roche, Meylan, France) man’s rank correlation coefficients were calculated to

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential750
Table 2. Plasma levels of antioxidant systems, oxidative stressTable 1. Chemiluminescence (CL) reaction parameters and totalperoxyl radical-trapping antioxidant potential (TRAP) values of markers and lipids in hemodialysis (HD) patients as compared
to healthy control subjectsplasma and low density lipoprotein (LDL) preparation fromhemodialysis (HD) patients as compared to healthy control subjects
HD patients Control subjects(N523) (N522)HD patients Control subjects
Number 23 22 Antioxidant systemsGSH-Px IU/liter 2369b 72614CL lag time min 39.367.8c 23.264.7
CL rate /10 7 cpm 2.961.3c 7.362.5 Ascorbate lmol /liter 16615b 61619Vitamin E lmol /liter 28.066.4 28.5 67.2CL peak /10 7 cpm 6.162.3c 14.564.0
Plasma TRAP lmol /liter 13286255b 7836159 Uric acid lmol /liter 396685b 262661Lipid and protein oxidation products
Number 10 10 MDA lmol /liter 3.260.7b 2.460.2CL lag time min 7.862.7a 4.361.5 Carbonyls nmol/mg protein 0.7360.32a 0.3160.09CL rate /10 7 cpm 5.862.4 6.962.4 AOPP lmol /liter 147647b 38617CL peak /10 7 cpm 9.261.8 9.061.1 LipidsLDL-TRAP mmol /liter 108638a 60621 Cholesterol mmol /liter 5.361.2 5.3 60.9
Triglycerides mmol /liter 2.060.9b 1.060.5Values are expressed as mean 6 sd. P values, as determined by Mann-WhitneyU test are: a P , 0.05, b P , 0.001, c P , 0.0001
Values are expressed as mean 6 sd. P values were determined by the Mann-Whitney U test. Abbreviations are: AOPP, advanced oxidation protein products;MDA, malondialdehyde; GSH-Px, glutathione peroxidase.
a P , 0.001, a P , 0.0001
assess the relationship between the various parameters.The threshold of statistical significance was P , 0.05.
were not correlated with these antioxidants but wereRESULTS positively correlated with plasma levels of vitamin E (r 5
0.62, P , 0.01).Plasma and LDL-TRAP in hemodialysis patients andIn contrast to other antioxidants, uric acid was signifi-control subjects
cantly higher in the plasma of HD patients than of controlPlasma from HD patients significantly increased lagsubjects, and its level was positively correlated withtime and reduced both the rate and peak of the CLplasma TRAP (r 5 0.70, P , 0.0001) but not with LDL-reaction as compared with control plasma (Table 1). LDLTRAP values.preparations from HD patients also significantly increased
CL lag time but had no effect on the CL rate or peak. Relationship between TRAP and plasma levels ofTherefore TRAP, which only accounts for CL lag time, lipid and protein oxidation productswas significantly higher in HD patients than in controls
Malondialdehyde, carbonyl, and AOPP concentra-and for both plasma (P , 0.001) and LDL (P , 0.05;tions were significantly increased in the plasma of HDTable 1). Moreover, a positive correlation was observedpatients as compared with controls (Table 2).between plasma TRAP and LDL-TRAP values (r 5
Plasma TRAP values were positively correlated with0.54, P , 0.05).plasma levels of carbonyls (r 5 0.42, P , 0.02) andBecause previous studies have reported profoundAOPP (r 5 0.59, P , 0.0001) but not MDA. In contrast,changes in antioxidant systems with aging [39, 40], weLDL-TRAP values were correlated with both MDA (r 5compared plasma TRAP values in HD patients aged less0.60, P , 0.01) and AOPP (r 5 0.60, P , 0.01) but notthan 50 years (N 5 7) or $50 years (N 5 16) to thosewith carbonyl plasma levels.in healthy controls aged less than 50 years (N 5 18).
Plasma TRAP values (mean 6 sd) were similar in HDRelationship between TRAP and plasma lipid levelspatients ,50 years or $50 years (1364 6 227 and 1290 6
Whereas plasma cholesterol levels were similar in HD264 mmol/liter, respectively) and were significantly higherpatients and control subjects, plasma triglyceride levelsin HD patients ,50 years than in controls ,50 yearswere significantly higher in the former (Table 2).(1364 6 227 vs. 775 6 161 mmol/liter, P , 0.01).
Although no correlation was found between plasmaRelationship between TRAP and plasma levels of TRAP and triglyceride levels, a positive correlation wasantioxidant systems observed between LDL-TRAP values and plasma tri-
glyceride levels (r 5 0.64, P , 0.01).Plasma levels of GSH-Px and ascorbate were signifi-cantly decreased in HD patients as compared with con-
In vitro effect of compounds correlating with thetrols (Table 2). In contrast, plasma levels of vitamin ETRAP in vivowere similar in HD patients and in control subjects.
The positive correlations observed between, on thePlasma TRAP values were inversely correlated withone hand, plasma TRAP and uric acid or AOPP plasmaGSH-Px (r 5 20.59, P , 0.01) and ascorbate (r 5 20.54,
P , 0.01) plasma levels. In contrast, LDL-TRAP values levels and, on the other hand, LDL-TRAP and triglycer-

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential 751
HD [5, 6, 14–16]. Recently, TRAP has been proposed asa relevant parameter to determine the total antioxidantcapacity of plasma from patients with oxidative stress-associated diseases [24–27]. In contrast, the antioxidantpotential of LDL has not yet been investigated, althoughit could be of great interest in the evaluation of the roleof ox-LDL in the atherosclerosis process.
This study aimed at determining the potential clinicalrelevance of the TRAP parameter to gauge the redoxstate of HD patients showed that in fact both plasmaand LDL-TRAP were significantly increased in thesepatients as compared with controls (Table 1). This wasfound despite high circulating levels of oxidative stressmarkers, including MDA, carbonyls, and AOPP, anda profound deficiency of major antioxidants, includingGSH-Px and ascorbate but not vitamin E (Table 2), theactivity of which, however, is known to be consistentlyFig. 2. Effect of in vitro supplementation, respectively, 100 mM (a)impaired when the ascorbate level is reduced [41]. Theand 200 mM (b) uric acid and 100 mM (c) and 200 mM (d ) HSA-AOPP
preparation to a normal plasma (heavy line) on the CL reaction as inverse relationship found between plasma TRAP andcompared with a hemodialysis patient plasma (dashed line; results of plasma levels of GSH-Px or ascorbate further demon-a typical experiment).
strated that the capacity to scavenge peroxyl radicals invitro did not reflect the activity of the major plasmaantioxidant systems. Rather, it suggested the presenceof other substances in the plasma of uremic patients thatides or AOPP led us to perform an in vitro study of theare not necessarily efficient chain-breaking antioxidantseffect of these plasma compounds on the TRAP assay.in vivo, but are able to exert a peroxyl radical-scavengingThe addition of uric acid to control plasma did noteffect in vitro. Among these, uric acid is a good candidate.influence the CL rate and peak, but significantly in-Uric acid is usually an efficient antioxidant in vitro. How-creased the CL lag time in a dose-dependent mannerever, this is less the case in vivo in the presence of de-(Fig. 2). Thus, normal plasma TRAP regularly increasedcreased ascorbate levels [42]. In addition, it has beenwith uric acid supplementation, although it did not reachshown that uric acid is not efficient against oxidant-medi-that of HD patients having similar circulating uric acidated protein damage [43].levels (Table 3).
Interestingly, Jackson et al also found that plasmaThe addition of HSA-AOPP preparations to normalTRAP was higher in HD patients than in controls andplasma significantly increased the CL time lag and de-that it was significantly decreased by the end of a singlecreased both the CL rate and peak (Fig. 2). The CLdialysis session [28]. They attributed these observationsreaction pattern of control plasma supplemented withto uric acid, which is present at high plasma levels before150 mm HSA-AOPP was close to that given by HD plasmathe dialysis session and dramatically decreases at the endcontaining a mean AOPP level of 174 6 14 mmol/literof the session. Our in vitro study showed that the addition(Table 3).of uric acid to normal plasma increased its TRAP in aFinally, we investigated the effect of triglycerides ondose-dependent manner and thus further supported theLDL-TRAP by adding to a normal plasma LDL prepa-major influence of uric acid on TRAP assay. However,ration (containing 0.43 mmol/liter triglycerides), a tri-our observation that the control plasma TRAP obtainedglyceride-rich LDL preparation (containing 0.71 mmol/after uric acid supplementation was still lower than thatliter triglycerides), or triolein (3 mmol/liter), a triglycer-of an HD plasma with a similar uric acid level (Table 3)ide that is not integrated in LDL particles. Althoughstrongly suggested that other uremia-related substancestriolein had no effect on LDL-TRAP, a moderate in-contributed to the increase in plasma TRAP of HD pa-crease in the CL time lag (from 2.8 6 0.5 to 4.5 6 0.8 min)tients.was observed following the addition of the triglyceride-
Among these, AOPP, which we have recently pro-enriched LDL preparation.posed as novel uremic toxins and molecular basis of oxida-tive stress [44, 45], should be considered despite the fact
DISCUSSION that they do not exert proper antioxidant activity. In-Several groups, including ours, have highlighted the deed, Hawkins and Davies have previously reported that
role of antioxidant depletion in the progression of CRF oxidized proteins become more avid than native proteinsfor trapping radicals [43]. It is thus tempting to proposeand the complications associated with its treatment by

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential752
Table 3. Effect of uric acid and HSA-AOPP on plasma CL reaction and TRAP
Control plasma Control plasma supplemented with uric acid or AOPP HD plasma
Uric acid lmol /liter 245615 1100 1200 No No 432618AOPP lmol /liter 31610 No No 1100 1150 174614
CL reactionlag time min 19.762.0 23.061.6a 31.562.0b 23.861.1a 29.562.8b 37.661.0b
rate /10 7 cpm 5.961.3 5.761.0 5.860.9 3.360.8b 2.860.6b 2.761.0b
peak /10 7 cpm 11.961.4 11.560.5 10.961.0 6.260.8b 5.160.5b 5.560.4b
TRAP lmol /liter 624629 691626a 1005637b 745630a 1019645b 1223659c
Results of 5 experiments are shown (mean 6 sd). P values were by the Mann-Whitney U-test versus control plasma before supplementation.a P , 0.05, b P , 0.01, c P , 0.001
Reprint requests to Beatrice Descamps-Latscha, M.D., Ph.D.,that AOPPs, which are present at high concentration inINSERM U507, Hopital Necker, 161, rue de Sevres, 75743 Paris Cedex
the plasma of HD patients, could exert a scavenging 15, France.E-mail: [email protected] in vitro on the ABAP-catalyzed peroxyl radicals
involved in the assay. Our results showing that (a) invivo plasma TRAP values were correlated with AOPP
APPENDIXlevels but not with MDA levels, and (b) in vitro supple-Abbreviations used in this article are: ABAP, 2,29-azobis [2-amidi-mentation of normal plasma with HSA-AOPP prepara-
nopropane] hydrochloride; AGEs, advanced glycation end-products;tions significantly increased TRAP values (Table 3) sup- AOPPs, advanced oxidation protein products; CL, chemiluminescence;port this hypothesis. CRF, chronic renal failure; DNPH, 2,4-dinitrophenylhydrazine; GSH-
Px, glutathione peroxidase; HD, hemodialysis; HOCl, hypochlorousOur finding that LDL-TRAP of HD patients was, likeacid; HSA, human serum albumin; LDL, low-density lipoprotein;plasma, significantly increased allows the following com- MDA, malondialdehyde; NADPH, nicotinamide adenine dinucleotide
ments. The presence of ox-LDL, as a consequence of phosphate; ox-LDL, oxidized low-density lipoprotein; t lag, lag time;TPTZ, 2,4,6-tripyridyl-s-triazine; TRAP, total peroxyl radical-trappingoxidative stress, has been well documented in HD pa-antioxidant potential.tients [29]. The oxidation process may affect lipid and/
or protein moieties of LDL [46, 47], and interestingly,REFERENCESLDL-TRAP values were closely related with both MDA
and AOPP plasma levels. Because dialysis triggers a 1. Lindner A, Charra B, Sherrard DJ, Scribner BH: Acceleratedatherosclerosis in prolonged maintenance hemodialysis. N Engl Jmassive generation of chlorinated oxidants [8, 9, 11, 12],Med 290:697–701, 1974which represent the major source of oxidized proteins 2. Jungers P, Massy ZA, Nguyen-Khoa T, Fumeron C, Labrunie
[48, 49], it is tempting to propose that, as discussed earlier M, Lacour B, Descamps-Latscha B, Man NK: Incidence and riskfactors of atherosclerotic cardiovascular accidents in predialysisin this article for plasma, the ox-LDL protein moietychronic renal failure patients: A prospective study. Nephrol Dial(LDL-AOPP) may delay the CL reaction by scavenging Transplant 12:2597–2602, 1997
the peroxyl radicals generated in TRAP assay. However, 3. London GM, Drueke TB: Atherosclerosis and arteriosclerosis inchronic renal failure. Kidney Int 51:1678–1695, 1997the ox-LDL lipid moiety could also participate to such
4. Ritz E, Deppisch R, Stier E, Hansch G: Atherogenesis and cardiacan increased LDL-TRAP through their enriched-triglyc-death: Are they related to dialysis procedure and biocompatibility?
eride content [50], and our in vitro experiments con- Nephrol Dial Transplant 9(Suppl 2):165–172, 19945. Becker BN, Himmelfarb J, Henrich WL, Hakim RM: Reassessingfirmed that the addition of triglyceride-enriched LDL
the cardiac risk profile in chronic hemodialysis patients: A hypothe-preparations significantly increased LDL-TRAP. Thesis on the role of oxidant stress and other non-traditional cardiac
presence of elevated circulating levels of triglycerides is risk factors. J Am Soc Nephrol 8:475–486, 19976. Ceballos-Picot I, Witko-Sarsat V, Merad-Boudia M, Nguyena common feature of HD patients [51], but here again,
AT, Thevenin M, Jaudon MC, Zingraff J, Verger C, Jungerstriglycerides by themselves have no antioxidant effect.P, Descamps-Latscha B: Glutathione antioxidant system as aIt is therefore highly probable that when incorporated marker of oxidative stress in chronic renal failure. Free Radic Biol
into LDL particles triglycerides become an additional Med 21:845–853, 19967. Klahr S: Oxygen radicals and renal diseases. Miner Electrolytetarget of the peroxyl radicals involved in linoleic acid
Metab 23:140–143, 1997oxidation and in this manner delay the CL reaction. 8. Nguyen AT, Lethias C, Zingraff J, Herbelin A, Naret C, Des-It therefore appears obvious that TRAP is not a reli- camps-Latscha B: Hemodialysis membrane-induced activation of
phagocyte oxidative metabolism detected in vivo and in vitro withinable parameter for assessing the TRAP of plasma ormicro amounts of whole blood. Kidney Int 28:158–167, 1985LDL in HD patients. The evaluation of TRAP in this
9. Market M, Heierli C, Kuwahara T, Frei J, Wauters JP: Dialyzedclinical setting, which combines major oxidative stress polymorphonuclear neutrophil oxidative metabolism during dial-
ysis: A comparative study with 5 new and reused membranes. Clinwith profound uremia-related biochemical disturbances,Nephrol 29:129–136, 1988has nevertheless allowed us to highlight the potential
10. Vanholder R, Ringoir S, Dhondt A, Hakim RM: Phagocytosiseffects of uric acid, triglycerides, and AOPP on peroxyl in uremic and hemodialysis patients: A prospective and cross sec-
tional study. Kidney Int 39:320–327, 1991radical-mediated reactions.

Nguyen-Khoa et al: Plasma and LDL oxidant-trapping potential 753
11. Himmelfarb J, Lazarus JM, Hakim R: Reactive oxygen species 30. Holvoet P, Donck J, Landeloos M, Brouwers E, Luijtens K,production by monocytes and polymorphonuclear leukocytes dur- Arnout J, Lesaffre E, Vanrenterghem Y, Collen D: Correlationing dialysis. Am J Kidney Dis 17:271–276, 1991 between oxidized low density lipoproteins and von Willebrand
12. Cristol JP, Canaud B, Rabesandratana H, Gaillard I, Serre factor in chronic renal failure. Thromb Haemost 76:663–669, 1996A, Mion C: Enhancement of reactive oxygen species production 31. Esterbauer H, Gebicki J, Puhl H, Jurgens G: The role of lipidand cell surface markers expression due to haemodialysis. Nephrol peroxidation and antioxidants in oxidative modification of LDL.Dial Transplant 9:389–394, 1994 Free Radic Biol Med 13:341–390, 1992
13. Paul JL, Sall ND, Soni T, Poignet JL, Lindenbaum A, Man 32. Ahotupa M, Ruutu M, Mantyla E: Simple methods of quantifyingNK, Moatti N, Raichvarg D: Lipid peroxidation abnormalities oxidation products and antioxidant potential of low density lipo-in hemodialyzed patients. Nephron 64:106–109, 1993 proteins. Clin Biochem 29:139–144, 1996
14. Richard MJ, Arnaud J, Jurkovitz C, Hachache T, Meftahi H, 33. Wieland H, Seidel D: A simple specific method for precipitationLaporte F, Foret F, Favier A, Cordonnier D: Trace elements of low-density lipoproteins. J Lipid Res 24:904–909, 1983and lipid peroxidation abnormalities in patients with chronic renal 34. Wayner DD, Burton GW, Ingold KU, Locke S: Quantitativefailure. Nephron 57:10–15, 1991 measurement of total peroxyl radical trapping antioxidant capabil-
15. Ross EA, Koo LC, Moberly JB: Low whole blood and erythrocyte ity of human blood plasma by controlled peroxidation. FEBS Lettlevels of glutathione in hemodialysis and peritoneal dialysis. Am 187:33–37, 1985J Kidney Dis 30:489–494, 1997
35. Conti M, Morand PC, Levillain P, Lemonnier A: Improved16. Galli F, Buoncristiani U, Rovidati S, Albertini MC, Carobi C,fluorometric determination of malonaldehyde. Clin Chem 37:1273–Canestrari F: Lipoperoxidation and glutathione-dependent en-1275, 1991zymes in uremic anemia of CAPD patients. (letter) Nephron
36. Reznick AZ, Han D, Packer L: Cigarette smoke induced oxida-76:363, 1997tion of human plasma proteins, lipids, and antioxidants: Selective17. Taccone-Gallucci M, Lubrano R, Belli A, Citti G, Morosettiprotection by the biothiols dihydrolipoic acid and glutathione. Re-M, Meloni C, Elli C, Mazzarella V, Tozzo C, Meschini L,dox Rep 3:169–174, 1997Giardini O, Casciani CU: Lack of oxidative damage in serum
37. Benzie IFF: An automated, specific, spectrophotometric methodpolyunsaturated fatty acids before and after dialysis in chronicfor measuring ascorbic acid in plasma (EFTSA). Clin Biochemuremic patients. Int J Artif Organs 12:515–518, 198929:111–116, 199618. Schulz T, Schiffl H: Preserved antioxidative defense of lipopro-
38. Milne D, Botnen J: Retinol, a-tocopherol, lycopene, and a- andteins in renal failure and during hemodialysis. Am J Kidney Disb-carotene simultaneously determined in plasma by isocratic liquid25:564–571, 1995chromatography. Clin Chem 32:874–876, 198619. Witko-Sarsat V, Friedlander M, Capeillere-Blandin C, Ngu-
39. Olivieri O, Stanzial AM, Girelli D, Trevisan MT, Guarini P,yen-Khoa T, Nguyen AT, Zingraff J, Jungers P, Descamps-Latscha B: Advanced oxidation protein products as a novel Terzi M, Caffi S, Fontana F, Casaril M, Ferrari S, Corrochermarker of oxidative stress in uremia. Kidney Int 49:1304–1313, R: Selenium status, fatty acids, vitamins A and E, and aging: The1996 Nove Study. Am J Clin Nutr 60:510–517, 1994
20. Witko-Sarsat V, Friedlander M, Nguyen-Khoa T, Capeillere- 40. Schafer L, Thorling EB: Lipid peroxidation and antioxidant sup-Blandin C, Nguyen AT, Canteloup S, Dayer JM, Jungers P, plementation in old age. Scand J Clin Lab Invest 50:69–75, 1990Drueke T, Descamps-Latscha B: Advanced oxidation protein 41. Frei B, Keaney JF, Retsky KL, Chen K: Vitamins C and E andproducts as novel mediators of inflammation and monocyte activa- LDL oxidation. Vit Horm 52:1–34, 1996tion in chronic renal failure. J Immunol 161:2524–2532, 1998 42. Whitehead TP, Jungner I, Robinson D, Kolar W, Pearl A, Hale
21. Miyata T, Wada Y, Cai Z, Iida Y, Horie K, Yasuda Y, Maeda A: Serum urate, serum glucose and diabetes. Ann Clin BiochemK, Kurokawa K, van Ypersele de Strihou C: Implication of an 29:159–161, 1992increased oxidative stress in the formation of advanced glycation 43. Hawkins CL, Davies MJ: Hypochlorite-induced damage to pro-end products in patients with end-stage renal failure. Kidney Int teins: Formation of nitrogen-centred radicals from lysine residues51:1170–1181, 1997 and their role in protein fragmentation. Biochem J 332:617–625,
22. Miyata T, Maeda K, Kurokawa K, van Ypersele de Strihou C: 1998Oxidation conspires with glycation to generate noxious advanced 44. Witko-Sarsat V, Descamps-Latscha B: Advanced oxidation pro-glycation end products in renal failure. Nephrol Dial Transplant tein products: Novel uraemic toxins and pro-inflammatory media-12:255–258, 1997 tors in chronic renal failure? Nephrol Dial Transplant 12:1310–
23. Friedlander MA, Witko-Sarsat V, Nguyen AT, Wu YC, Labru- 1312, 1997nie M, Verger C, Jungers P, Descamps-Latscha B: The advanced45. Witko-Sarsat V, Nguyen-Khoa T, Jungers P, Drueke TB, Des-glycation endproduct pentosidine and monocyte activation in ure-
camps-Latscha B: Advanced oxidation protein products as novelmia. Clin Nephrol 45:379–382, 1996molecular basis of oxidative stress in uremia. Nephrol Dial Trans-24. Ceriello A, Bortolotti N, Pirisi M, Crescentini A, Tonutti L,plant 14:76–78, 1999Motz E, Russo A, Giacomello R, Stel G, Taboga C: Total plasma
46. Hazell LJ, van den Berg JJM, Stocker R: Oxidation of low-antioxidant capacity predicts thrombosis-prone status in NIDDMdensity lipoprotein by hypochlorite causes aggregation that is medi-patients. Diabetes Care 20:1589–1593, 1997ated by modification of lysine residues rather than lipid oxidation.25. Dailly E, Urien S, Barre J, Reinert P, Tillement JP: Role ofBiochem J 302:297–304, 1994bilirubin in the regulation of the total peroxyl radical trapping
47. Fu S, Davies MJ, Stocker R, Dean RT: Evidence for roles ofantioxidant activity of plasma in sickle cell disease. Biochem Bio-radicals in protein oxidation in advanced human atheroscleroticphys Res Commun 248:303–306, 1998plaque. Biochem J 333:519–525, 199826. Yao JK, Reddy R, McElhinny LG, van Kammen DP: Reduced
48. Daugherty A, Dunn JL, Rateri DL, Heinecke JW: Myeloperoxi-status of plasma total antioxidant capacity in schizophrenia.dase, a catalyst for lipoprotein oxidation, is expressed in humanSchizophr Res 32:1–8, 1998atherosclerotic lesions. J Clin Invest 94:437–444, 199427. Langley SC, Brown RK, Kelly FJ: Reduced free-radical-trapping
49. Leeuwenburgh C, Hansen P, Shaish A, Holloszy JO, Heineckecapacity and altered plasma antioxidant status in cystic fibrosis.JW: Markers of protein oxidation by hydroxyl radical and reactivePediatr Res 33:247–250, 1993nitrogen species in tissues of aging rats. Am J Physiol 43:R453–28. Jackson P, Loughrey CM, Lightbody JH, McNamee PT, YoungR461, 1998IS: Effect of hemodialysis on total antioxidant capacity and serum
50. Westhuyzen J, Saltissi D, Healy H: Oxidation of low densityantioxidants in patients with chronic renal failure. Clin Chemlipoprotein in hemodialysis patients: Effect of dialysis and compari-41:1135–1138, 1995son with matched controls. Atherosclerosis 129:199–205, 199729. Maggi E, Bellazzi R, Gazo A, Seccia M, Bellomo G: Autoanti-
51. Massy ZA, Ma JZ, Louis TA, Kasiske BL: Lipid-lowering therapybodies against oxidatively-modified LDL in uremic patients under-going dialysis. Kidney Int 46:869–876, 1994 in patients with renal disease. Kidney Int 48:188–198, 1995