Critical Care Case Presentation 27th Nov,2013 case ppt.pdf · 2015-07-15 · Physical Examination:...
35
Critical Care Case Presentation 27 th Nov,2013 Done By: Sara AlArfaj
Transcript of Critical Care Case Presentation 27th Nov,2013 case ppt.pdf · 2015-07-15 · Physical Examination:...

Critical Care Case Presentation
27th Nov,2013
Done By:
Sara AlArfaj
Outlines:
• Topic Review.
1) Background
2) Etiology
3) Epidemiology
4) Diagnosis
5) Treatment
• Case Components.

Diabetic Foot Infections

Background:
• Diabetes mellitus is a disorder that primarily affects
the microvascular circulation.
• Worldwide, diabetic foot infections are the most
common skeletal and soft-tissue infections in
patients with diabetes.
• Diabetic foot ulcers in diabetics occur as a result of
various factors, such as peripheral neuropathy, and
atherosclerotic peripheral arterial disease, pressure,
and foot deformity.
"Diabetic Foot Infections ." Diabetic
Foot Infections. N.p., n.d. Web. 23
Nov. 2013
4

Diabetic foot infections typically take
one of the following forms:
Cellulitis
Deep-skin and soft-tissue infections
Acute osteomyelitis
Chronic osteomyelitis
"Diabetic Foot Infections ." Diabetic
Foot Infections. N.p., n.d. Web. 23
Nov. 2013
Etiology:
• Microvascular disease due to "sugar-coated capillaries" limits the blood supply to the superficial and deep structures.
• Diabetics are predisposed to foot infections because of this compromised vascular supply.
• Impaired microvascular circulation hinders WBC migration into site of infection, limits the ability of antibiotics to reach the site in a good concentration.
"Diabetic Foot Infections ." Diabetic Foot
Infections. N.p., n.d. Web. 23 Nov. 20136

Cont’d
• Superficial infections like Cellulitis can be caused by
Strept (group A and B).
Staph Aureus.
• Deep soft-tissue infections in diabetic patients can
be associated with gas-producing Gm-ve Bacilli.
• Chronic Osteomyelitis:
Strept (group A and B), Gm-ve Bacilli.
Bacteroids Fragilis, E.Coli, Proteus Marbilis and Klebsella
Pneumoniae.
"Diabetic Foot Infections ." Diabetic Foot
Infections. N.p., n.d. Web. 23 Nov. 20137

Epidemiology:
• More than 50% of lower limb
amputations are due to DM.
• Up to 80% of diabetic foot
amputations can be prevented.
• About 325 amputations are likely to
occur annually in Jeddah compared
to 741 in Riyadh and 3970 in KSA.
The rule of 15 *
15% of people with diabetes develop ulcers
15% of ulcers develop osteomyelitis
15% of ulcers result in amputation
* Armstrong, David G. and Lavery, Lawrence A. (2005).
Clinical Care of the Diabetic Foot. American Diabetes
Association. ISBN- 10: 1580402232
The Journal of Diabetic Foot
Complications, 2011; Volume 3, Issue
3, No. 3, Pages 55-61
8

www.smj.org.sa Saudi Med J 2006;
Vol. 27 (2)9

Diagnosis:
History, signs and symptoms
WBC,ESR Blood cultures
Gmstain/cultures for aspirated
samples
Radiography, CT, or MRI
NICE clinical guideline 119 –
Diabetic foot problems 201210

Treatment and Management:
IDSA Guideline for Diabetic Foot
Infections • CID 2012:54 (15 June)11
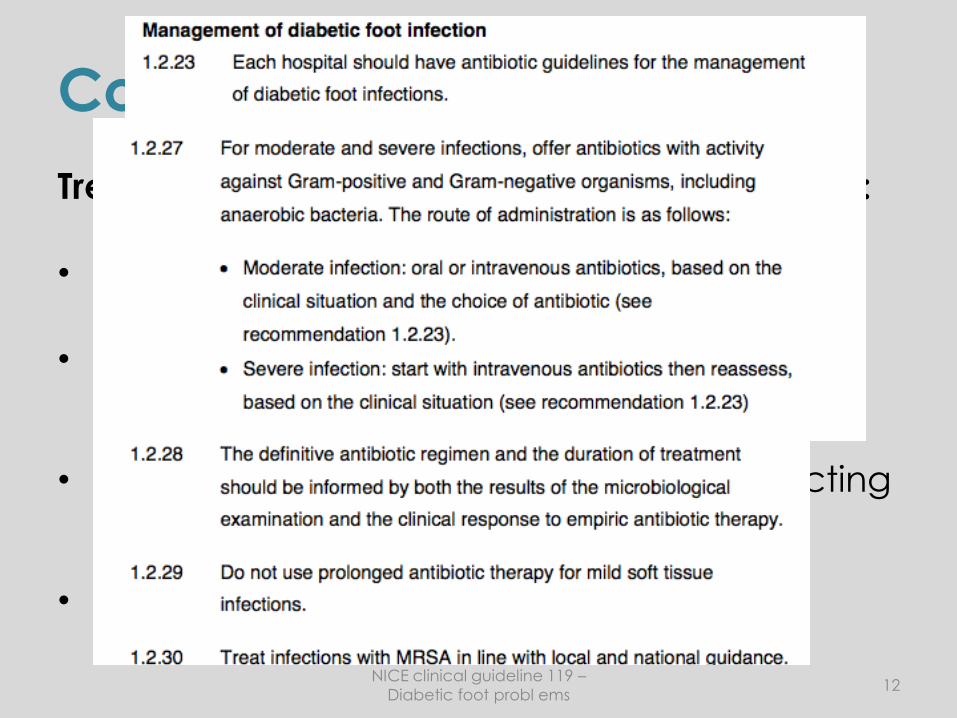
Cont’d
Treatment depends on the severity of infection:
• Cellulitis being the easiest.
• Deep skin and soft-tissue infections are curable.
• Acute osteomyelitis, depends on the infecting MO and the right antibiotic choice.
• Chronic osteomyelitis, the most difficult.
NICE clinical guideline 119 –
Diabetic foot probl ems12
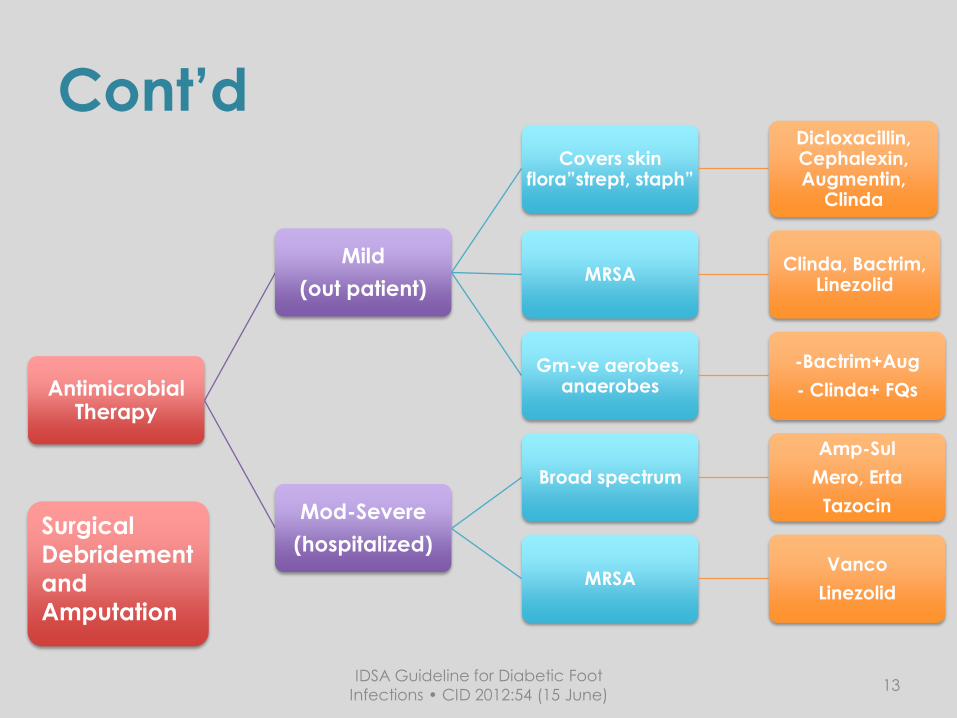
Cont’d
Antimicrobial Therapy
Mild
(out patient)
Covers skin flora”strept, staph”
Dicloxacillin, Cephalexin, Augmentin,
Clinda
MRSAClinda, Bactrim,
Linezolid
Gm-ve aerobes, anaerobes
-Bactrim+Aug
- Clinda+ FQs
Mod-Severe
(hospitalized)
Broad spectrum
Amp-Sul
Mero, Erta
Tazocin
MRSAVanco
Linezolid
Surgical
Debridement
and
Amputation
IDSA Guideline for Diabetic Foot
Infections • CID 2012:54 (15 June)13

Cont’d
Manage and control other
complications and comorbidities. (DM,
CKD, HTN)
KDOQI Diabetes Guideline: 2012 Update/ADA,
DIABETES CARE, VOLUME 36, SUPPLEMENT 1, JANUARY
2013
14

Case Components

Patient’s Information:
MA is a 50 yo Saudi female, came to the OPD
nursing clinic for a follow up.
Chief Compliant:
Came for a follow up for the diabetic foot, she
was fatigued with a LL swelling.

HPI:
• The patient came for a follow up, her primary physician found she had a rising Cr and Urea levels, she was suspecting a possible sepsis as well.
• So, the patient was admitted in 8th of Nov for more renal evaluation.
• In the 10th, She aspirated while she was eating.
• She was arrested, CPR lasted about 25 minutes, with two failed attempts of intubation.
• Admitted to the ICU.She was hypoxic 60-
70%
Cr= 195 (44-80 umol/L)
U= 33.5 (2.5-6.4 mmol/L)
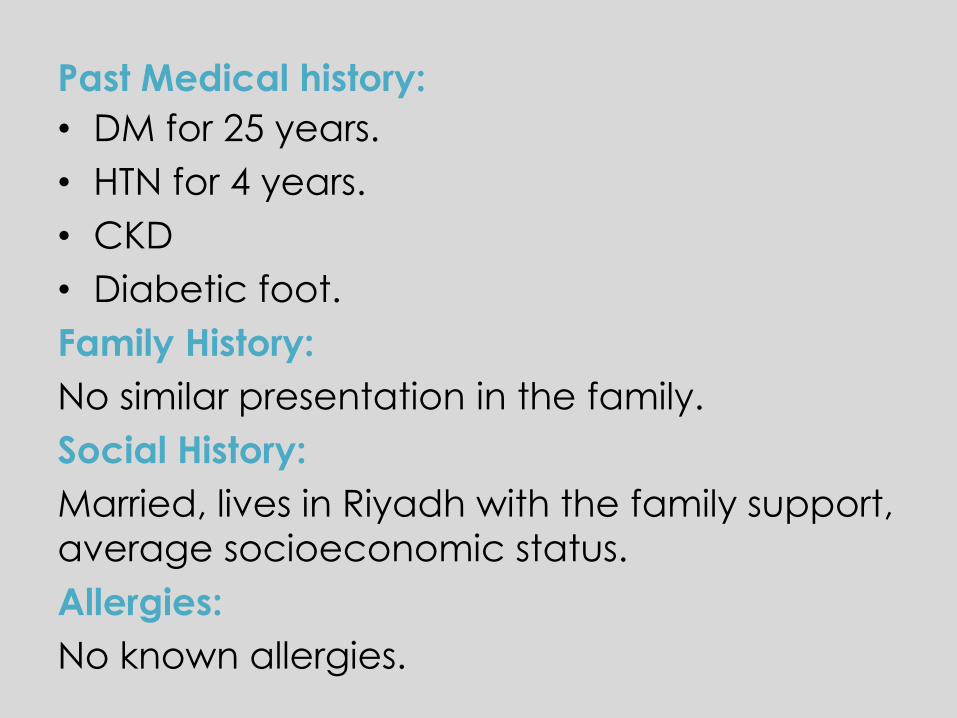
Past Medical history:
• DM for 25 years.
• HTN for 4 years.
• CKD
• Diabetic foot.
Family History:
No similar presentation in the family.
Social History:
Married, lives in Riyadh with the family support,
average socioeconomic status.
Allergies:
No known allergies.
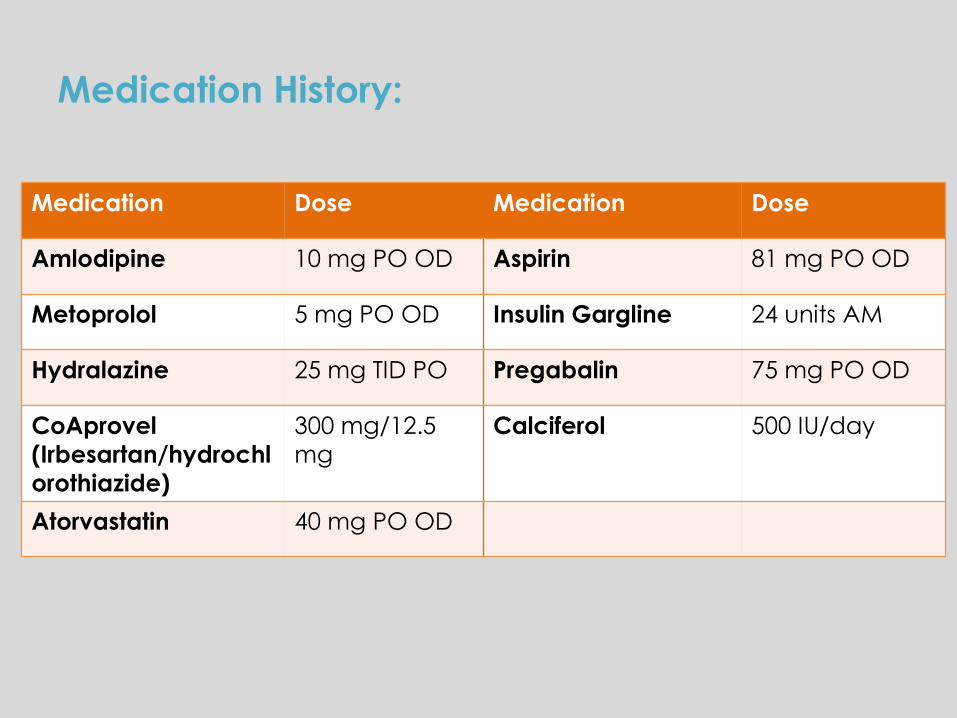
Medication History:
Medication Dose Medication Dose
Amlodipine 10 mg PO OD Aspirin 81 mg PO OD
Metoprolol 5 mg PO OD Insulin Gargline 24 units AM
Hydralazine 25 mg TID PO Pregabalin 75 mg PO OD
CoAprovel
(Irbesartan/hydrochl
orothiazide)
300 mg/12.5
mg
Calciferol 500 IU/day
Atorvastatin 40 mg PO OD

Vital signs:
T= 36.6 BP= 121/65 P=65
RR=20 HR=98 O2Sat= 96%
Wt= 60.9 kg Ht=157 cm

Physical Examination:
GEN Conscious, sleepy, responds to calling, looks unwell, fatigued
and pale.
Bilateral pitting edema.
Dressing over a wound in the left leg.
HEENT Not jaundiced, not cyanotic, JVP not raised.
CHEST Shallow breathing, not rapid. Equal chest expansion.
CVS S1+ S2 +O
ABD Soft not tender, no organomegaly, +ve bowel sounds.
CNS Conscious, drowsy, responds and opens eyes with loud
voices.

Laboratory Tests:
Electrolytes:
10 11 12 13 14 16 18 20 22 25
Na 145 144 143 145 141 143 147 150 145 148
K 4.8 4.2 4.0 3.6 3.6 4.4 4.4 5.1 5.1 4.6
Mg .92 .93 .95 .91 1.0 1.08 1.06 1.14 1.12 1.01
Ca 2.16 2.11 2.19 2.31 2.30 2.27 2.38 2.36 2.31 2.23
U 32.4 31.4 33 33 32 33 35 34 34.9 30
Cr 181 194 197 195 178 167 157 148 142 123

CBC:
Coagulation:
11 13 14 15 16 18 20 22
WBC
11.9 13.7 15.6 11.6 8.8 7.19 8.16 8.34
RBC 3.17 3.01 2.95 2.86 2.8
4
2.62 3.14 2.91
Hg 8.50 8.20 8.00 7.8 7.7
0
7.10 8.9 7.70
Hct 25.6 24.3 23.9 23.3 23 21 27.7 24
Plt 180 191 176 144 125 113 115 121
10 11 12 13 14 15 16 18 20 22
PT 19.8 18.8 19.3 18.9 17.3 17.5 17.3 16.
5
15.9 16.3
APTT 36.4 39.3 38.9 37.3 36.8 1.5 37.8 44 40.3 50
INR 1.7 1.6 1.7 1.6 1.5 41.3 1.5 1.4 1.3 1.3
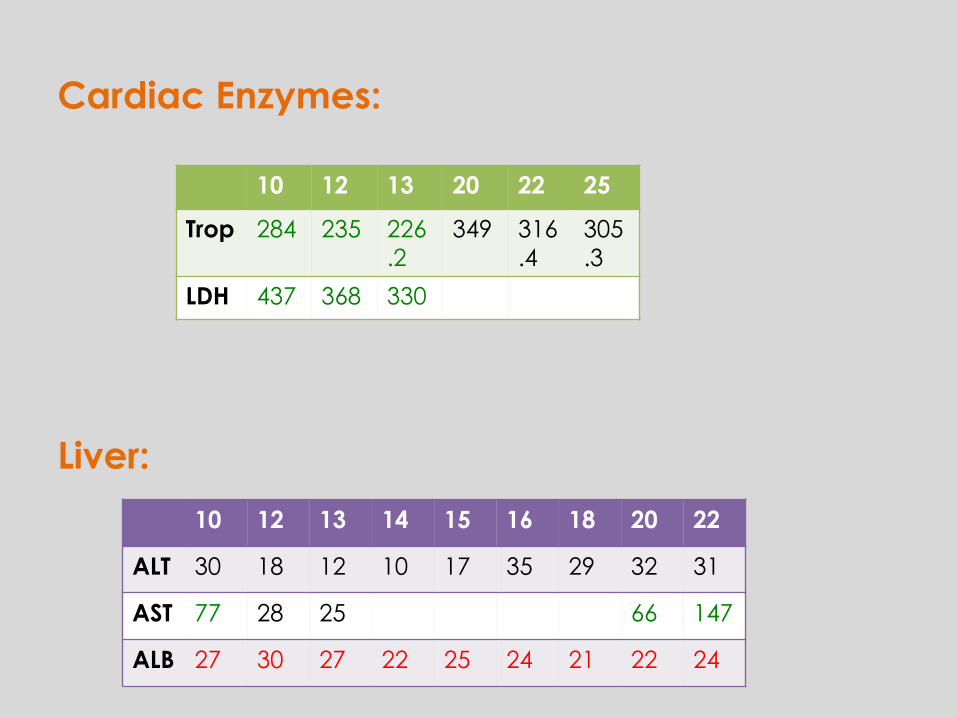
Cardiac Enzymes:
Liver:
10 12 13 20 22 25
Trop 284 235 226
.2
349 316
.4
305
.3
LDH 437 368 330
10 12 13 14 15 16 18 20 22
ALT 30 18 12 10 17 35 29 32 31
AST 77 28 25 66 147
ALB 27 30 27 22 25 24 21 22 24
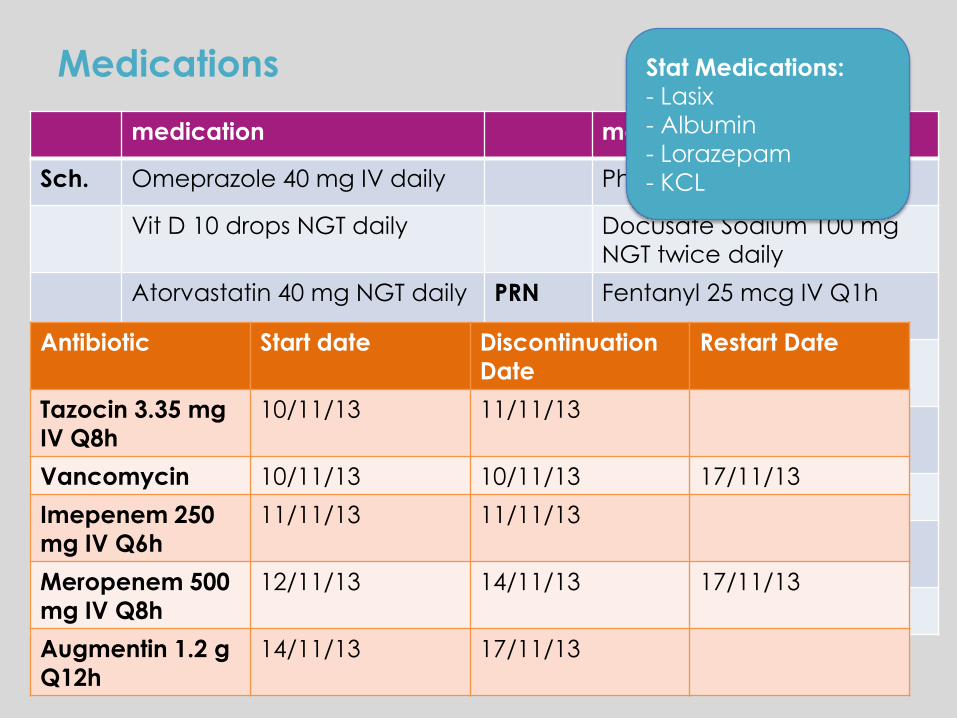
Medications
medication medication
Sch. Omeprazole 40 mg IV daily Phenytoin 100 mg IV Q8h
Vit D 10 drops NGT daily Docusate Sodium 100 mg
NGT twice daily
Atorvastatin 40 mg NGT daily PRN Fentanyl 25 mcg IV Q1h
Aspirin 81 mg NGT daily Hydralazine 10 mg IV Q1h
Sodium Carbonate 650 mg
NGT Q8
Infusion Insulin
Heparin 5000 unites SQ BID Midazolam 3 mg/hr
Levetiracetam 500 mg IV
daily
Norepinephrine .053
mcg/kg/min
Refresh eye drops
Stat Medications:
- Lasix
- Albumin
- Lorazepam
- KCL
Antibiotic Start date Discontinuation
Date
Restart Date
Tazocin 3.35 mg
IV Q8h
10/11/13 11/11/13
Vancomycin 10/11/13 10/11/13 17/11/13
Imepenem 250
mg IV Q6h
11/11/13 11/11/13
Meropenem 500
mg IV Q8h
12/11/13 14/11/13 17/11/13
Augmentin 1.2 g
Q12h
14/11/13 17/11/13

Problem List:
1) Post CPR ( cardiac arrest and
Respiratory failure).
2) Post Aspiration Pneumonia.
3) Diabetic Foot Ulcer, Osteomyelitis.
4) Worsening CKD.
5) DM.
6) HTN.

Day 1 (10th Nov)
S The patient was brought to the ICU after she aspirated and got
arrested (CPR 25 minutes).
O • T= 36 BP= 126/75 HR=70 O2Sat=95% HGT=4 Na= 145
alb=27
• High Cr and Urea levels (181, 32.4 respectively).
• High INR of 1.7
• On Inotropes.(Dopamine 20 mcg/kg/min)
A Possible sepsis (DF, Osteomyelitis)
P • For more cardiac, renal and liver work up.
• Tazocin 3.35 mg IV Q8h.
• Albumin 5% (500 ml) IV.
• Hold Aspirin.

11th Nov
S ICU day 2
O • T= 36.1 BP= 118/63 HR=80 O2Sat=97% HGT=8.2 Na= 144
alb=29 K=4.2 Cr=194 U=31.4 INR=1.6 WBC=11.98.
• Low HGB=8.50, RBCs= 3.17 and HCT= 25.60
• GCS 3/15, intubated, sedated on Midazolam, NGT feeding.
A Post CPR, DFU, seizure, AKI on top of Chronic
P • DC Levetiracetam.
• Start Phenytoin 20 mg/kg stat over 1 ½ hrs, then continue with
100 mg IV Q8hrs.
• Discontinue Imepenem and switch to Meropenem 500 mg
Q8hrs IV for 14 days.
• EEG: status epilepticus.
• CT: no hypoxic ischemic brain insult, no intracranial
hemorrhage or infarction.
• US: moderate ascites at the upper and lower
abdomen

12th/ 13th Nov
S ICU day 3 and 4
O • T= 36 BP= 137/66 HR=92 O2Sat=99% HGT=12.6 alb=23
Cr=195 U=33 INR= 1.6 WBC= 13.74
• Phenytoin level= 21.51
• Urine output 100-200 ml/hr
• Culture results.
A Hemodynamically stabel, no inotropic support, no siezures
P • Close observation for seizures.
• Meropenem frequency changed to Q12hrs. ( CL= 28.47
ml/min)
• If culture came ESBL –ve, deescalate duration from 14 days to
7 days.
- Blood: negative.
- Feet wound: heavy
growth of gm-ve bacilli,
not yet identified.
* She’s a known carrier of ESBL
If CrCl 26-50
ml/min: 0.5-1 g IV
Q12 hrs

14th-16th Nov
S ICU day 5,6 and 7.
O • T= 36.8 BP= 132/57 HR=77 O2Sat=99% HGT=10.1 alb=24
Cr= 174 U=33 WBC=8.2 INR= 1.5.
• Culture results.
• DDIM= 9.1 ug/ml (0.0-.5 μg/ml)
A Patient is stable.
P 14/11
• Stop Meropenem, Start Augmentin 1.2 g IV Q12hrs for 7 days.
• Heparin 5000 units SQ Q12hrs.
16/11
• Change Omeprazole 40 mg daily from IV to NGT.
Wound (14/11):
- Heavy growth of klebsiella Pneumoniae
- Heavy growth of Proteus Mirabilis
- Heavy growth of SA.
* All sensitive to Augmentin.
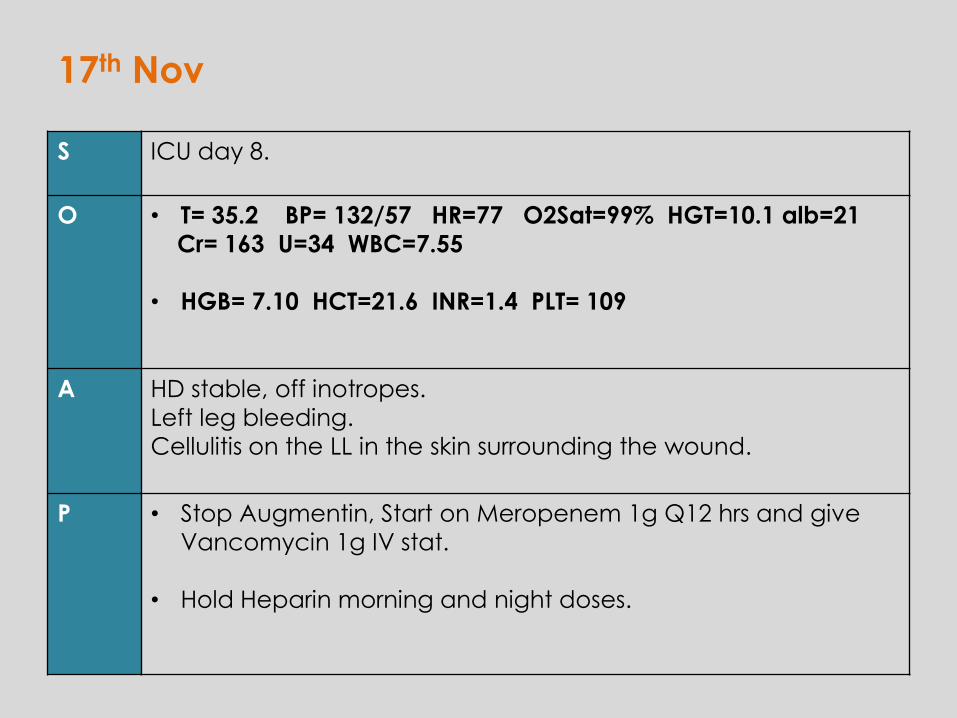
17th Nov
S ICU day 8.
O • T= 35.2 BP= 132/57 HR=77 O2Sat=99% HGT=10.1 alb=21
Cr= 163 U=34 WBC=7.55
• HGB= 7.10 HCT=21.6 INR=1.4 PLT= 109
A HD stable, off inotropes.
Left leg bleeding.
Cellulitis on the LL in the skin surrounding the wound.
P • Stop Augmentin, Start on Meropenem 1g Q12 hrs and give
Vancomycin 1g IV stat.
• Hold Heparin morning and night doses.
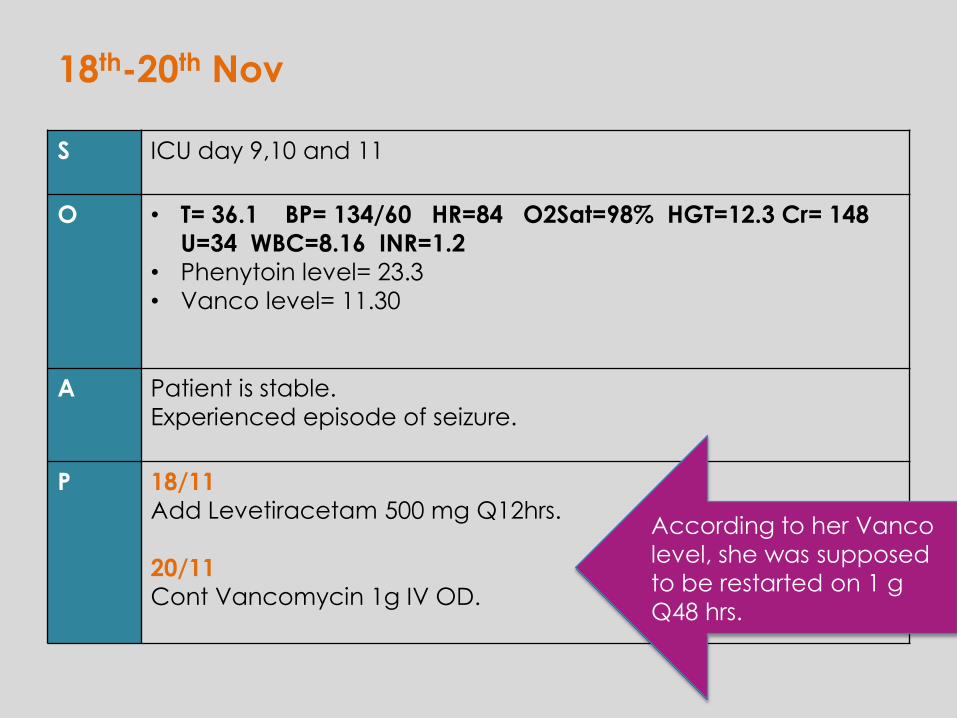
18th-20th Nov
S ICU day 9,10 and 11
O • T= 36.1 BP= 134/60 HR=84 O2Sat=98% HGT=12.3 Cr= 148
U=34 WBC=8.16 INR=1.2
• Phenytoin level= 23.3
• Vanco level= 11.30
A Patient is stable.
Experienced episode of seizure.
P 18/11
Add Levetiracetam 500 mg Q12hrs.
20/11
Cont Vancomycin 1g IV OD.
According to her Vanco
level, she was supposed
to be restarted on 1 g
Q48 hrs.
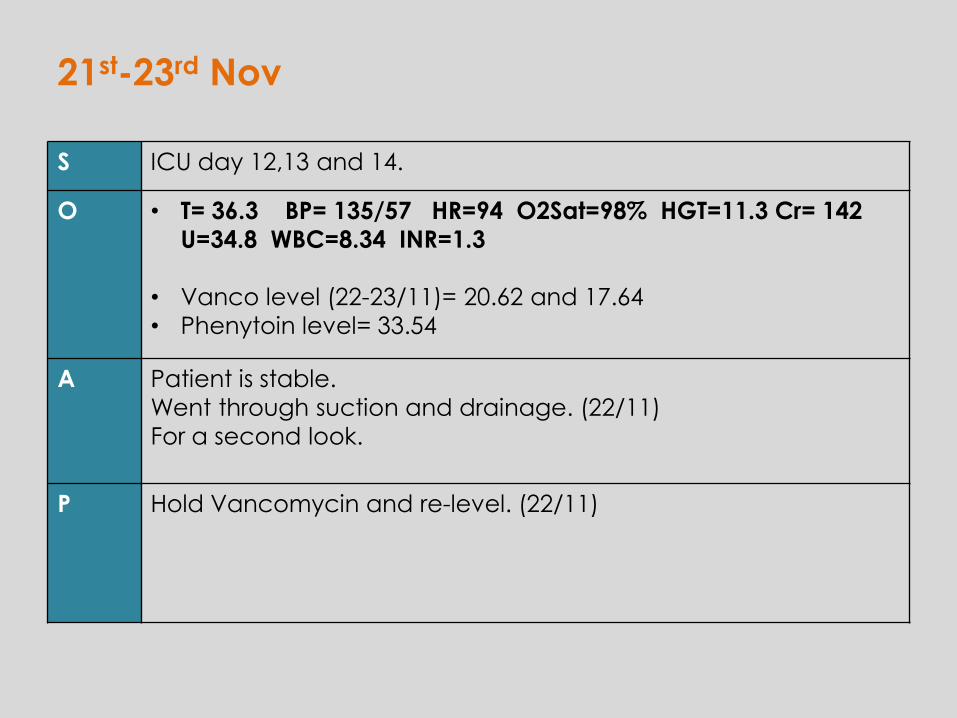
21st-23rd Nov
S ICU day 12,13 and 14.
O • T= 36.3 BP= 135/57 HR=94 O2Sat=98% HGT=11.3 Cr= 142
U=34.8 WBC=8.34 INR=1.3
• Vanco level (22-23/11)= 20.62 and 17.64
• Phenytoin level= 33.54
A Patient is stable.
Went through suction and drainage. (22/11)
For a second look.
P Hold Vancomycin and re-level. (22/11)

24th ,25th Nov
S ICU day 15 and 16
O • T= 36 BP= 141/57 HR=96 O2Sat=98% HGT=10 Cr= 123
U=30.1 WBC=6.12 INR=1.1
• Vanco levels= 13.79 and 11.92
A For OR.
P 24/11
Levetiracetam 750 mg IV BID
25/11
Vancomycin every 48 hours.
Phenytoin 100 mg NGT Q8hrs
Levetiracetam 750 NGT Q12hrs.
Thank You..Questions?