Control of breathing during mechanical ventilation
41
Control of breathing during mechanical ventilation D. Georgopoulos, Professor of Medicine, Intensive Care Medicine Department, University Hospital of Heraklion, University of Crete, Heraklion, Crete, Greece
Transcript of Control of breathing during mechanical ventilation

Control of breathing during
mechanical ventilation
D. Georgopoulos, Professor of Medicine,
Intensive Care Medicine Department,
University Hospital of Heraklion,
University of Crete,
Heraklion, Crete, Greece

Disclosures
Covidien
Draeger
Research grants

Basic principles of control of
breathing

Multi-sources
Medullary respiratory controller
Spinal motor neurons
Pmus = V’xR + ΔVxE
Volume-time profile
VentilationPaO2, PaCO2, pH
Diseases
Therapy
Pres Pel
Chem
ical
fee
dbac
k
Ref
lex a
nd M
echan
ical
feed
bac
k
Behavioral
feedback

Multi-sources
Medullary respiratory controller
Spinal motor neurons
Paw +Pmus = V’xR + ΔVxE
Volume-time profile
VentilationPaO2, PaCO2, pH
Diseases
Therapy

+ Paw = Prs + Pel
Volume-time profile
Mechanical
Chemical
Reflex
Behavioral
Feedback
Response of Pmus
to ventilator delivered
breath
Response of
ventilator to Pmus
Pmus
Ventilator and Patient
factors
Georgopoulos D: Principles and Practice of Mechanical Ventilation
(ed. Tobin) 2013: pp 805-820

Response of ventilator to Pmus
1) The mode of mechanical ventilation
2) The mechanics of the respiratory system
3) The characteristics of Pmus waveform
OutputInput

Μodes of assisted mechanical
ventilation
• Assist volume control (AVC, VT constant)
• Pressure support or control (PS, Pressure constant)
• Proportional modes (PAV, NAVA. Neither pressure
nor volume are pre-set but the patient effort drives
ventilator pressure)
Proportional modes will help us to clarify the issue of control of
breathing in mechanically ventilated patients

0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
0 2 4 6 8 10 12
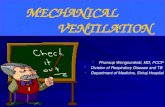
VT
(L)
Patient effort [PTPPmus (cmH2O.sec)]
PAV, NAVA
PS
AVC
Interaction between ventilator delivered volume
and patient effort with
different modes of support at high assist levels
Figure based on Data from: 1) Mitrouska et al. Eur Respir J 1999
2) Colombo et al. Intensive Care Med 2008
3) Meric et al. Respir Physiol Neurobiol 2014

Response of ventilator to Pmus
1) The mode of mechanical ventilation
2) The mechanics of the respiratory system
3) The characteristics of Pmus waveform
OutputInput
How do these factors affect the response of the ventilator?
(i.e. output)

-0,8
-0,6
-0,4
-0,2
0
0,2
0,4
0,6
0,8
-2 3 8 13 18
-5
0
5
10
15
20
25
30
35
-2 3 8 13 18
-5
0
5
10
15
20
-2 3 8 13 18
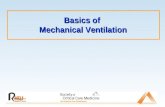
Time (sec)
Flo
w (
l/se
c)P
aw (
cmH
2O
)P
es (
cmH
2O
)
5 sec
Fr = 33 b/min
Georgopoulos et al. Intensive Care Med 2006;32:34
A patient with dynamic hyperinflation due to COPD on PSV
Ventilator rate = 12 b/min

Kondili et al. Br J Anaesth 2003;91:106
Double triggering due to expiratory asynchrony
between patient and ventilator
Ventilator rate = 2 x patient’s rate

Response of ventilator to Pmus
MessageDirect extrapolation of the ventilator output to the
patient’s control of breathing system (i.e. input) may be
misleading, guiding inappropriate therapeutic decisions
OutputInput

+ Paw = V’xR + VxE
Volume-time profile
Mechanical
Chemical
Reflex
Behavioral
Feedback
Response of Pmus
to ventilator delivered
breath
Response of
ventilator to Pmus
Pmus
Ventilator and Patient
factors
Georgopoulos D: Principles and Practice of Mechanical Ventilation
(ed. Tobin) 2013: pp 805-820

Chemical – Reflex
feedback
Chemical feedback
Prevents derangement
in arterial blood gasses
and acid-base balance
(hypoxia, hypercapnia,
hypocapnia)
Reflex feedback
Mainly prevents over-distention
(Hering-Breuer reflex)
VV
Pmus
ChemicalReflex
Polacheck et al. J Appl Physiol 1980;49:609
Cunningham et al. Handbook of Physiology. The Respiratory
system. Vol. 2. 1986; pp. 475–528.

Does mechanical ventilation
affect the operation (effectiveness)
of these feedback systems?
ChemicalReflex
Wakefulness
Sleep (and sedation)

Respiratory response to CO2 during
mechanical ventilation in awake humans
0
50
100
150
200
250
300
350
20 25 30 35 40 45 50 55
% o
f b
ase
lin
e
PaCO2
Pmus
Fr
Data from Georgopoulos et al. Am J Respir Crit Care Med 1997;156:146
f is relatively insensitive to CO2
over a wide range of PCO2
the ventilatory response to CO2 is expressed
mainly by the intensity of respiratory effort

VT/effort per breath
(neuroventilatory coupling per
breath) and not per min is the main
determinant of the respiratory
response to chemical feedback
0
100
200
300
400
20 30 40 50 60
% o
f b
ase
lin
e
PaCO2

• Consequences?
Chemical feedback during mechanical
ventilation - Wakefulness
VT/effort per breath is important

0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
PAV PS AVC
VT/P
TP
-Pm
us
I
(l/c
mH
2O
. sec)
* *
+
+
VT/effort per breath (neuroventilatory coupling) with low and
high respiratory drive at various modes of support (at high assist)
Data from Mitrouska et al. Eur Respir J 1999; 13:873
Low drive
High drive (CO2 challenge)
Hypocapnia
Hypercapnia
and/or distress
PETCO2
22 mmHg
PETCO2
21 mmHg
PETCO2
31 mmHg

Independent on assist level: RR constant on both modes
VT increased ≈ 500 ml VT constant
PtCO2 decreased
by ≈ 10 mmHg
(severe hypocapnia)
PtCO2 constant
Meric et al. Respir Physiol Neurobiology 2014;195:11
PS NAVA

Chemical feedback during mechanical
ventilation - Wakefulness
Consequences
• Modes of support that permit the
intensity of patient effort to be expressed
on the VT delivered by the ventilator
increase the effectiveness of chemical
feedback to regulate PaCO2
ChemicalReflex
Meric et al. Respir Physiol Neurobiology 2014;195:11
Mitrouska et al. Eur Respir J 1999; 13:873
Effective

Chemical feedback during mechanical
ventilation - Wakefulness
Consequences
• Modes of ventilation that impair the
neuroventilatory coupling (VT/effort)
may cause either hypocapnia or
hypercapnia and/or distress.
ChemicalReflex
Meric et al. Respir Physiol Neurobiology 2014;195:11
Mitrouska et al. Eur Respir J 1999; 13:873
Ineffective

Chemical feedback during mechanical
ventilation -Sleep
Observations
• The respiratory rhythm is critically depended on PaCO2
• A drop in PaCO2 by 3-4 mmHg causes apnea
(Datta et al. J Physiol 1991; 440:17, Mezza et al. J Appl Physiol 1998; 84:3)

0
2
4
6
8
10
12
14
16
18
20
10 15 20 25 30 35 40 45 50 55 60 65 70
Ventila
tion (
l/m
in)
PaCO2 (mmHg)
Wakefulness
Sleep
Apnea (Apneic threshold)
During sleep breathing frequency changes minimally
with decreasing PaCO2 up to a point (apneic threshold)
0
2
4
6
8
10
43 44 45 46 47 48
0
5
10
15
20
25
43 44 45 46 47 48
f
Pm
us
PaCO2
Meza et al. J Appl Physiol 1998;85:1928
Meza et al. J Appl Physiol 1998;84:3
16 14 14
Apnea Apnea Apnea
0 3 6
8
During sleep the chemical feedback
controls ventilation exclusively by
changing the respiratory effort per
breath (and not by changing
frequency)

Even during sleep VT/effort per breath
(neuroventilatory coupling per breath) and not
per min is the main determinant of the
respiratory response to chemical feedback
0
2
4
6
8
10
43 44 45 46 47 48
0
5
10
15
20
25
43 44 45 46 47 48
f
Pm
us
PaCO2
16 14 14
Apnea Apnea Apnea
0 3 6
8

Chemical feedback during mechanical
ventilation -Sleep
Consequences
• Modes of support that decrease the VT in
response to any reduction in Pmus
promote ventilatory stability
ChemicalReflex
Meza et al. J Appl Physiol 1998;85:1928
Meza et al. J Appl Physiol 1998;84:3

Chemical feedback during mechanical
ventilation -Sleep
Consequences
• At high assist, modes of ventilation that
impair the neuroventilatory coupling
(VT/effort) may cause apnoeas and trigger
periodic breathing
ChemicalReflex
Meza et al. J Appl Physiol 1998;85:1928
Meza et al. J Appl Physiol 1998;84:3

MESSAGE
The operation (effectiveness) of chemical
feedback during mechanical ventilation depends
mainly on the mode of mechanical ventilatory
support

+ Paw = V’xR + VxE
Volume-time profile
Mechanical
Chemical
Reflex
Behavioral
Feedback
Response of Pmus
to ventilator delivered
breath
Response of
ventilator to Pmus
Pmus
Ventilator and Patient
factors
Georgopoulos D: Principles and Practice of Mechanical Ventilation
(ed. Tobin) 2013: pp 805-820

Reflex feedback
Prevents over-distention
(i.e. Hering-Breuer)
VV
Pmus
ChemicalReflex
If effort drives the ventilator
(PAV, NAVA) this feedback
may control VT
↓Tineural with increasing volume
Polacheck et al. J Appl Physiol 1980;49:609

Paw
EAdi
Volume
Pes
↑↑ assist No assist
(for one breath)
ChemicalReflex
Grasselli et al. Intensive Care Med 2012;38:1224
Rabbits ventilated with NAVA

Theoretically
• Mechanically ventilated patients who express the feedback systems of control of breathing (CHEMICAL and REFLEX feedback) may choose a breathing pattern that limit the risks of lung damage.
ChemicalReflex

Animal data
Allowing animals with acute lung
injury to “control” their ventilatory
pattern (using NAVA) is at least as
protective (and probably more)
as a low VT strategy
(i.e. protective strategy)
Rabbit brain does a good job
Brander et al. Intensive Care Med. 2009;35:1979
Mirabella et al. Crit Care 2014;18:R22

Human brain?

108 patients mechanically ventilated on controlled modes andrecovering from acute respiratory failure were permitted to select theirown breathing pattern by placing them on PAV+ for a maximum periodof 48 hours
2016 Mar 17;228:69-75`
Individual driving pressure (ΔP) were calculated in these patients andexamined how it related to ΔP when the same patients were ventilatedpassively using the currently accepted lung-protective strategy
Studies in passively ventilated ARDS patients have shown that drivingpressure (but not VT) is associated with adverse outcomes
Amato MB et al. N Engl J Med 2015
Laffey et al. Intensive Care Medicine 2016
Sherpa Neto et al. Intensive Care Med. 2016

Human brain?
2016 Mar 17;228:69-75
Main results:
Critically ill patients control the driving pressure to low levels [10
cmH20 (8-12), median (IQR)] bybsizing VT to individual respiratory
system compliance using appropriate feedback mechanisms aimed at
limiting the degree of lung stress

-13
-11
-9
-7
-5
-3
-1
1
3
5
7
9
11
4 6 8 10 12 14 16 18 20 22
Ch
ang
e in
ΔP
(cm
H2O
)
ΔP
PA
V+
-Δ
PC
MV
ΔP during CMV (cmH2O)
87% (58/67)
91% (59/65)
Georgopoulos et al. Respir Physiol Neurobiology 2016 Mar 17;228:69-75
When the lung protective strategy results in high driving pressure (≥15 cmH2O),
the patients’ control of breathing system decreased the driving pressure in the
majority (87%) of measurements.

Message
The patients’ control of breathing system is adept
at protecting the lungs by preventing high driving
pressure, while not unnecessarily restricting tidal
volume when this has no protective value.
-13
-11
-9
-7
-5
-3
-1
1
3
5
7
9
11
4 6 8 10 12 14 16 18 20 22

ChemicalReflex
Provided that:
1) The mode of support does not interfere
with their operation
Doorduin et al. Am J Respir Crit Care Med 2016; Oct 17
Brochard et al. Am J Respir Crit Care Med. 2016 Sep 14
2) Load-independent high respiratory drive
that may override the protective mechanisms,
IS NOT AN ISSUE
Patients selection is crucial
(be very careful in patients with severe
metabolic acidosis, delirium, ongoing
sepsis, etc)

Response of
ventilator to Pmus
Response of Pmus
to ventilator delivered
breath
Direct extrapolation of the ventilator
output to the patient’s control of
breathing system (i.e. input) may be
misleading, guiding inappropriate
therapeutic decisions
OutputInput
Commands
ChemicalReflex
The control of breathing
system is damaged by the
ventilator