Consumerism and Actuarial Science in A 21 st Century Intelligent Health System Healthcare Visions,...
50
Consumerism and Actuarial Science in A 21 st Century Intelligent Health System Healthcare Visions, Inc. Creating the Possible… Ronald E. Bachman FSA. MAAA President & CEO Healthcare Visions, Inc. 404-697-7376 [email protected] www.healthcarevisions.net Sr. Fellow - Center for Health Transformati Sr. Fellow - Georgia Public Policy Foundati Fellow - Wye River Group on Health
-
Upload
alison-sherman -
Category
Documents
-
view
218 -
download
3
Transcript of Consumerism and Actuarial Science in A 21 st Century Intelligent Health System Healthcare Visions,...

Consumerism and
Actuarial Science in
A 21st Century Intelligent Health System
Healthcare Visions, Inc. Creating the Possible…
Ronald E. Bachman FSA. MAAAPresident & CEO
Healthcare Visions, Inc.404-697-7376
Sr. Fellow - Center for Health TransformationSr. Fellow - Georgia Public Policy Foundation
Fellow - Wye River Group on Health

What Is a 21st Century Intelligent Health System?
• In a 21st Century Intelligent Health System, the individual has:
– Accurate, timely knowledge of personal health needs,
– Access to the best information about how to maintain personal health,
– Knowledge of whom to see and where to go for health services,
– And confidence that health providers are practicing medicine using best practices based on the most up-to-date understanding of outcomes-based medicine.
• In a 21st Century Intelligent Health System, the individual has the right to know the price and quality information about health services in the most accurate, least expensive, and most convenient manner possible.
• In a 21st Century Intelligent Health System, the individual is the center of knowledge and decision-making and has responsibility for his or her own health.

Consumer-directed or Consumerism?
Consumer-directed health plans (CDHPs) utilizing an HRA or HSA are the newest weapon in the arsenal to reduce healthcare cost.
But will this approach really lower your cost?
CDHPs are a good start and can developing experience shows they can lower costs.
CDHPs are a good 1st generation attempt. The market is moving rapidly to 2nd generation and beyond.
The transformation is NOT to CDHP but to Consumerism.
Actuaries must go beyond traditional models to reflect the behavioral change component of a consumerism design.

Healthcare Consumerism
Healthcare Consumerism is about transforming a health benefit plan into one that puts economic purchasing power—and decision-making—in the hands of participants.
It’s about supplying the information and decision support tools they need, along with financial incentives, rewards, and other benefits that encourage personal involvement in altering health and healthcare purchasing behaviors.

Elements of Healthcare Consumerism
1. Budgeting – monthly versus annual
2. Risk Sharing – pooled claims for large groups
3. Savings – NEW with advent of HRAs and HSAs

The Core of Consumerism
The Unifying Theme for a
Health and Healthcare Strategy is:
“Implement only if it supports behavioral change consistent with the
strategy”
Behavioral ChangeBehavioral Change

Two Basic Principles for Successful Consumerism
1. Must work for the Sickest Members, as well as the healthy
2. Must work for those not wanting to get involved in decision-making, as well as the “techies”

Mega Trends
1.Personal Responsibility
2.Self-Help, Self-Care
3.Individual Ownership
4.Portability
5.Transparency (the Right to Know)
6.Consumerism (Empowerment)

The Evolution of Healthcare and Consumerism
Future Generations of Consumer Directed Healthcare
Behavioral Change and Cost Management Potential
Low Impact ---- ---- ---- ---- ---- ---- ---- ---- ---- High Impact
Traditional Planswith
ConsumerInformation
2nd Generation CDHC
Focus onBehaviorChanges
TraditionalPlans
3rd Generation CDHC
IntegratedHealth &
Performance
1st Generation CDHC
Focus on Discretionary
Spending
4th Generation CDHC
Personalized Health & Healthcare
mjthompson001

Major Building Blocks of Consumerism
•
Personal AccountsPersonal Accounts
Incentives & Incentives & RewardsRewards
Wellness/PreventionWellness/Prevention
Early InterventionEarly Intervention
Disease ManagementDisease Management
InformationInformation
Decision SupportDecision Support
It is the creative development, efficient delivery, efficacy, and successful integration of these elements that will prove the success or failure of consumerism.
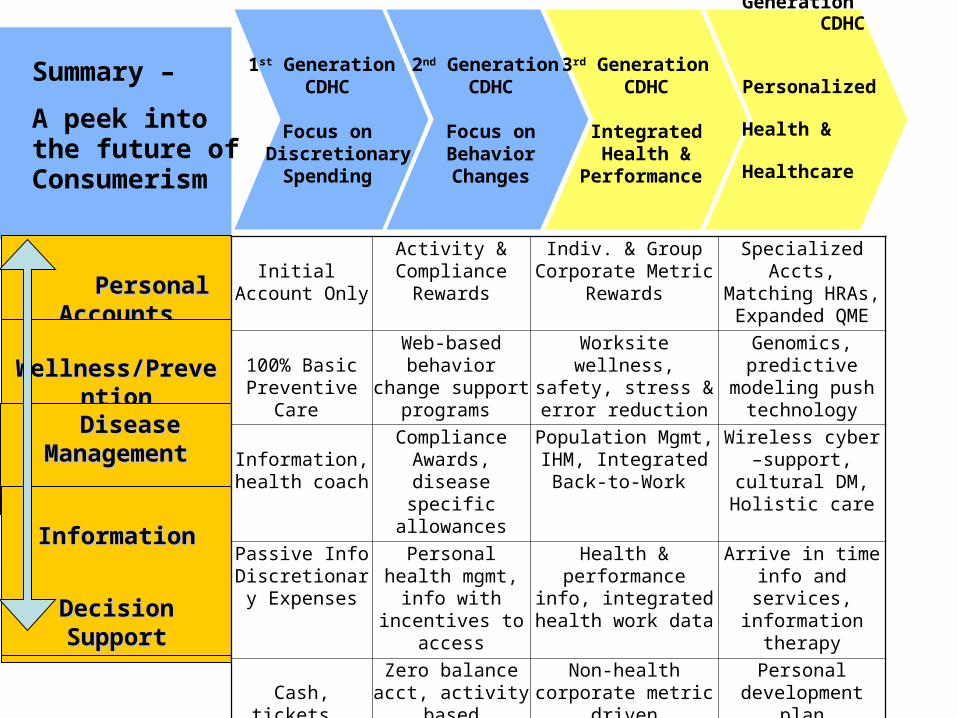
2nd Generation CDHC
Focus onBehaviorChanges
3rd Generation CDHC
IntegratedHealth &
Performance
1st Generation CDHC
Focus on Discretionary
Spending
4th Generation CDHC
Personalized Health & Healthcare
Personal AccountsPersonal Accounts
Incentives & Incentives & RewardsRewards
Wellness/PreventionWellness/Prevention
Early InterventionEarly Intervention
Disease ManagementDisease Management
InformationInformation
Decision SupportDecision Support
Initial Account Only
Activity & Compliance
Rewards
Indiv. & Group Corporate Metric
Rewards
Specialized Accts,Matching HRAs,Expanded QME
100% Basic Preventive Care
Web-based behavior change support
programs
Worksite wellness,safety, stress & error
reduction
Genomics, predictive modeling push
technology
Information, health coach
Compliance Awards, disease specific
allowances
Population Mgmt, IHM, Integrated Back-to-
Work
Wireless cyber –support, cultural DM,
Holistic care
Passive Info Discretionary
Expenses
Personal health mgmt, info with
incentives to access
Health & performance info, integrated health
work data
Arrive in time info and services,
information therapy
Cash, tickets, Trinkets
Zero balance acct, activity based
incentives
Non-health corporate metric driven incentives
Personal development plan incentives,
health status related
Summary –
A peek into the future of Consumerism

Using Information & Incentives To Change Behaviors
Low Users Medium Users
High Users
Very High Users
No Claims
Generally Healthy
Acute Episodic Conditions
O/P, Low In/P, High Maternity
Chronic & Persistent . Conditions . O/P, Low In/P, High
Catastrophic
% Mem 15% 48% 14% 3% 3% 12% 4% 1%
% Dollars 0% 12% 15%
12% 5% 21%
20%
15%
% Mem 63% 32% 17%
% Dollars 12% 32% 56%
PreventionPrevention Wellness - LifestyleWellness - Lifestyle
Minimize
Early InterventionEarly Intervention
Wellness - ClinicalWellness - Clinical
Maximize
Minimize
Maximize
Wellness - LifestyleWellness - Lifestyle
Wellness - ClinicalWellness - Clinical

Low Users Medium Users High Users Very High Users
No Claim
s
Generally
Healthy
Acute EpisodicConditions
Chronic & Persistent Conditions Catastrop
hicO/P, Low
In/P, High
Maternity
O/P, Low
In/P, High
% Ee
% Dollars
% Ee
% Dollars
PatientSafety
Centers of Excellence
PatientAdvocacy/
Case Management
Pre-Natal Care
Reduce Variation in Evidence-Based
Medicine
DiseaseManagement
Reduce Variation in Evidence-Based
Medicine
Discretionary Expenses
Psycho-Social Factors / Integrated Absence Management
Personal Health ManagementDecision Support & Information

Health Promotion
Health Risk Management
Chronic Disease Management
High Cost Case Management
Website Health Risk Assessment
Patient Identification and enrollment
Targeted Behavior Modification
Care Coordination
Practice Guidelines
HealthyLifestyle Promotion
Physical Activity Campaign
Address Comorbid Conditions
Integrated Services, Communications, Measurement and EvaluationIntegrated Services, Communications, Measurement and Evaluation
Care Continuum and Tools for Changing Behaviors
Acute Conditionse.g., Infections, Respiratory, Lacerations
Navigational Support
Patient Advocacy
Care Coordination
Address Comorbid Conditions
At Risk
e.g., Inactivity, High Stress, Overweight, High Blood Pressure
Chronic Conditions
e.g., Depression, Heart Disease
Catastrophic Conditions
e.g., Cancer, Hepatitis C
Well
e.g., Low Risk, Good Nutrition, Active
Lifestyle

Wellness
Communication
Acute Case Mgmt
Utilization and Case Management
NETWORK A / TPA A NETWORK B / TPA B
Education
Prevention
Demand Management
Disease Mgmt Programs
Integrated Absence Mgmt The secret is cooperation and synergy between
components supporting the corporate strategies
Integrated Health Management ProgramAn Implementation Option for Multiple Generations
General ManagerPersonal Care Accts.
FSAs, HRAs, HSAs
Process Integration &
Disciplined Im
provement
Com
pany
Dat
a W
areh
ouse
& M
etri
cs

Potential Savings from Full Implementation of Consumerism
Achievement of savings and improved outcomes is dependent upon both the Type and Effectiveness of the programs implemented.
Gross* Savings as % of Total Plan Costs
(Programs Applicable to All Members)
EffectivePrograms
Implemented
Traditional plans
Consumerism Plans Passive 1st Generation 2nd Generation 3rd Gen & Future
Basic 2% 3% 7% 10%
Expanded 3-4% 5-8% 12-15.0% 20.0+%
Complete 4% 7% 17% 25%
Comprehensive (Future) 5% 10% 20% 30%
*Excludes Carry-over HRAs/HSAs and any added Administrative Costs of Specialized Programs

Major Actuarial Issues
• Anti-selection, • Value of wellness, • Disease management ROI, • Actuarial credits for behavioral change

ModerateAdverseSelection
HighAdverseSelection
HighPositiveSelection
ModeratePositiveSelection
LowBenefit
HighBenefit
Higher Cost
Lower Cost
e.g., CorePlan
e.g., Age-RatedHMO
e.g., PPOor POS
e.g., Not typicallyseen
ModerateAdverseSelection
HighAdverseSelection
HighPositiveSelection
ModeratePositiveSelection
LowBenefit
HighBenefit
Higher Cost
Lower Cost
e.g., CorePlan
e.g., Age-RatedHMO
e.g., PPOor POS
e.g., Not typicallyseen
ModerateAdverseSelection
HighAdverseSelection
HighPositiveSelection
ModeratePositiveSelection
LowBenefit
HighBenefit
Higher Cost
Lower Cost
e.g., CorePlan
e.g., Age-RatedHMO
e.g., PPOor POS
e.g., Not typicallyseen
Understanding Risk Selection and Anti-selection
The primary drivers of risk selection are employee cost and the relative benefit richness of the competing options.
Employees will tend to choose the option expected to provide the best economic benefit for their situation.
For healthy individuals the selection is usually low cost/low benefit options.For less healthy individuals the selection is usually high cost/high benefit options.
Selection effect is at least directionally predictable in most cases.
Mitigating factors tend to reduce the magnitude of selection. Health care costs are not fully predictable. Plan choices are usually made at a family unit level versus the individual level..

Potential Anti-Selection from CDHC on an Optional Basis
• Introduction of CDHC on an optional basis will limit the cost reduction because fewer members will be impacted and because the members that do select CDHC are likely to have an existing favorable health status (anti-selection). Adopting companies and its members can benefit most by introducing consumerism with both a CDHC option and consumerism for all other plans.
Example - Selection in An Option Environment
OPTION # 1 – Current Plan OPTION # 2 - CDHC
% MembersParticipating
Clms/Part.Mbr. Vs Clms/All Mbrs.
RemainingMembers
Clms/Part.Mbr. Vs Clms/All Mbrs.
90% 101% 10% 87%
70% 103% 30% 92%
50% 103% 50% 97%

Consumerism Choices involve Options for Behavioral Change rather than
Optional Plan Designs
• Consumerism Choices:
• Wellness• Preventive care• Early Intervention• Lifestyle Options (diet, exercise, smoking, safety)• Self-help, self care• Discretionary Expenses (e.g. OV, ER, Rx)• Value purchasing (e.g. DXL, o/p vs. in/p)• Participation in Disease Management Programs• Compliance with Evidence Based Medicine Treatment
Plans

Survey ResultsWellness Assessment Risk Factors
Risk Factors for Health Conditions
27%
77%
60%
81%
8%
1%
30%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Stress
Overweight/Underweight
Physical Inactivity
Poor Diet
Tobacco Use
Alcohol Use
Overdue Preventive Visits

Value of Wellness – What is it?
How Much Physical Activity Do the Experts Recommend? 30? 60? 90? Minutes of What?
The Centers for Disease Control and Prevention and the American College of Sports Medicine recommend the following:
• 20 minutes of vigorous-intensity physical activity 3 times a week or
• 30 minutes of moderate-intensity physical activity 5 or more times a week.
What is moderate-intensity physical activity? Any activity that burns 3.5 to 7 calories per minute (e.g., walking briskly).
What is vigorous-intensity physical activity? Any activity that burns 7 or more calories per minute (e.g.,
climbing up and down stairs).

National Business Group on HealthComments on Wellness
Recent studies indicate that moderate increases in employees’ physical activity levels can result in significant decreases in company costs. Although existing research is limited, employers may use calculation tools and internal data to calculate the potential savings of an effective physical activity promotion program.
To reach a rough estimate of the cost of its employees’ physical inactivity, a company could turn to www.activelivingleadership.org for a new online tool.
This Physical Inactivity Cost Calculator was developed by, among others, the Active Living Leadership Initiative, Fifty Plus Lifelong Fitness and the National Coalition for Promoting Physical Activity and Health.

Examples of Corporate Wellness & ROI
Motorola’s wellness programs which saves the company
$3.93 for every $1 invested.
Northeast Utilities WellAware Program which in its first 24 months reduced lifestyle and behavioral claims by $1,400,000.
Caterpillar’s Healthy Balance program which is projected to result in long term savings of $700 million by 2015.
Johnson & Johnson’s Health and Wellness Program which has produced average annual health care savings of $224.66 per employee.

Wellness ROI Studies
Many studies have focused specifically on the return on investment (ROI) from worksite health promotion and disease prevention programs.
Findings on the return on investment for health promotion and disease management programs were reported for nine employers: Canada & North America Life; Chevron.; City of Mesa, AZ; General Mills; General Motors; Johnson & Johnson; Pacific Bell; Procter & Gamble; and Tenneco. These programs provide health education to their employees to promote behaviors that will improve health or prevent disease, and typically include exercise programs, health-risk appraisal, weight control, nutrition information, stress management, disease screening, and smoking cessation.
The review found significant return on investment for the programs provided by these nine employers, with the range of benefit-to-cost ratios, ranging from $1.49 to $4.91 in benefits per dollar spent on the program, and a median of $3.14.

Savings from National Wellness Program
Savings estimates revealed that participation in the National Wellness Program was associated with significant savings in dollars per employee from 1991 to 1995, with the highest dollar savings achieved in 1995 ($16 per employee per month).
Evaluation of the program showed that health risk assessment was associated with significant and substantial reductions in healthcare costs.
Employees who completed one, two, or three health risk assessments on average had lower 1997 health care costs of $112.89, $134.22, and $152.29, respectively. Employees who had completed at least one health risk assessment and participated in an additional wellness activity had an average cost savings of $200.35 per year.

CIGNA Wellness Savings
The Working Well Moms Program has decreased pharmacy costs – 62% fewer prescriptions for breast-fed children. The program has also contributed to decreased medical costs – a savings of $240,000 in healthcare expenses. In addition, program participants have 74 fewer absences per 100 mothers, a savings of $60,000 in lost time annually.
The Working Well Triumph Program has resulted in healthcare costs savings of more than $900 per program participant.
The Working Well Flu Shots Program participants have 29% less absenteeism as compared to employees not getting a shot. This
produced a savings of $33 per employee participant. The overall return on investment for the program was 3 to 1.
CIGNA’s smoking cessation program helped 67 percent of its participants quit smoking after 12 months, a quit rate up to three times higher than comparable smoking cessation programs. CIGNA estimates saving $949 in health care costs for each successful participant, a return on investment of 9.5 to 1.

Disease Management for Chronic and Persistent Conditions
The Agriculture and Health and Human Services Departments’ Dietary Guidelines for Americans 2005 recommend the following:
• To reduce the risk of chronic disease—at least 30 minutes of moderate-intensity physical activity on most, preferably all days of the week;
• To prevent the gradual accumulation of excess weight in adulthood, up to 30 additional minutes per day may be required over the 30 minutes for reduction of chronic disease risk and other health benefits; and
• To sustain weight loss for previously overweight/obese people, about 60 to 90 minutes of moderate-intensity physical activity per day is recommended.

Passive Assertive Aggressive Program Type: Phone and mail
out- reach, no incentives
Incentives (i.e., waiving Rx copays)
Incentives (i.e, waiving Rx copays,
premium differential
DM vendor pricing method
Per employee per month, all
employees
Low PEPM on all ees plus hourly or per
case rate on participants only (rate
varies based on participant risk
status)
Low PEPM on all ees plus hourly or per case rate on participants only (rate varies based on participant risk
status)
Percentage of chronic diseased participating in program
10% 50% 75%
Return on investment of disease management programs
0 - .5 1.5 - 2 1.5 - 3
Disease Management Program ROI

Medical Claims % Change
2003 Study
(13.5K members)3.7% increase in medical cost
2004 Study
(9 mos.)
(49K members)
Early indicators 6% increase in medical cost over 2003
Continuously Enrolled Members: Allowed claims
Change in Utilization (# of Units)
2003 Study(12 months of data)
2004 Study(9 months of data)
Inpatient Admissions -5.2% -6.7%
ER Visits -2.6% -15.9%
Outpatient Events -14.4% -4.6%
ALL Office Visits -3.3% -3.4%
PCP Visits -10.9% -12.3%
Specialists visits +3.4% +3.6%
First Year Aetna HealthFund Members2004 results (9 mos.) show low medical cost increase
Note: 12 month continuously enrolled results due in August

What Happens in the Second Year to Allowed Claims?
1Q ’03 2Q ’03 3Q ’03 4Q ’03 1Q ’04 2Q ‘04 3Q ’04 4Q ’04
AHF**
PPO
* Allowed Claims are total claims, eligible for payment before benefit plan is applied
** Based on all AHF members from 18 of 19 plan sponsors in 2003 study; one plan sponsor removed due to large increase in AHF enrollment.
Allo
wed
Cla
ims
PM
PM
$140
$160
$180
$200
$220
$240
$260
+10.3%
+8.7%
• Utilization in AHF increased at a lower rate than PPO, based on allowed* claims
• Reinforces assumption that AHF trend will be 1% below PPO
• Studies will continue to evaluate AHF trend into the third year

Highlights of the 2003 Aetna HealthFund 12-Month Study
• Lower medical cost increase, applicable to first-year AHF members - 3.7 % compared to double digit PPO plans
• Diabetics continue to seek necessary care, relative to comparative populations
• Increases in certain preventive care services • Reduction in pharmacy scripts and increased generic
usage• Increased use of online tools, information, and satisfied
members

2004 United Health Plan Experience
The iPlan study found:
• A drop in the number of claims per 1,000 enrollees compared to the year before enrollment;
• A decrease in total emergency room visits, illustrating more selective, responsible use of emergency services;
• Significantly less-than-expected medical cost trends (per member/per month) than for traditional health plans; when iPlan was the only option, the annual cost trend was less than 1 percent;
• Reductions in specialist visits, outpatient surgeries and radiology and lab services; and
• Higher utilization of preventive services among iPlan participants.

• 15% reduction in pharmacy costs
• 92% generic substitution rate (open formulary, 100% of rebates go back to employer)
• 5% increase in preventive care expenditures
• 18% reduction in outpatient visits
• 85% graduation rate (Health Coach Program)
• 42% HRA completion with incentive; 28% opt-in to Health Coach
• 60% of clients offer integrated health improvement incentives.
LumenosKey Results – Utilization Impact

Are HSAs the right vehicle for large employer groups?
Yes, If………..
Or
No, Because…….
Need to Understand the Consumer Movement & the Transformation
that is Underway

HSAs and HRAs Very Different
HSA – A law, with specific requirements and benefit design requirements.
Most TAX ADVANTAGED vehicle ever created*******************************************************HRAs – No Law, this is a regulatory creation based upon
an IRS ruling. Most FLEXIBLE vehicle ever created

Incentive Awards - Three Very Different Personal Care Accounts
• FSAs – Traditional Group Plans
• Health Reimbursements Arrangements (HRAs) – Employers’ choice for cash flow flexible incentive based medical plan benefit designs (best suited for self-insured groups)
• Health Savings Accounts (HSAs) – Employees’ choice for funded portable triple tax advantaged with “High Deductible Health Plans” (best suited for individuals and small groups)
• Combination Accounts – creative but confusing

Important Differences between Use of HRAs and HSAs for Supporting
Behavioral Change
Generation 1
Initial Account Only
Generation 2
Activity & Compliance Rewards
Generation 3
Indiv. & Group Corporate Metric Rewards
Generation 4Specialized Accts,Matching HRAs,Expanded QME
1. Any Amount 2. Notional Acct 3. Employer Determined 4. Employer Only Contributions
1. Flexible Activity & Compliance Rewards 2. Employer Determined 3. Can not be cashed out 4. Must be used for healthcare
1. Flexible Indiv & Group Rewards 2. Employer Determined 3. Can not be cashed out 4. Must be used for healthcare
1. Specialized Notional Accts, 2. Can terminate by employer rules 3. Potential IRS Expanded QME
Health Savings Health Savings AccountsAccounts
1. Amounts Set by law 2. Real Dollars in Acct 3. Er or Ee Contrib 4. Contributions up to
plan deductible of $1000-2650 Single
$2000-5250 Family
1. Ltd Potential 2. Must give Cash Option 3. Awards must be same $ amt or same % of deductible 3. HSA can be used (with 10% penalty) for non- healthcare expenses
1. Ltd Potential 2. All participants must receive same amount or same % of deductible 3. Difficult to use for Group Incentives
1. Ltd Potential 2. 100% Vested & Portable 3. Can use matching HRAs, 4. Potential IRS Expanded QME
Health Health Reimbursement Reimbursement ArrangementsArrangements
Personal Care
Accounts

The Evolution of Personal Care Accounts
• Current State
HRAs HSAs
Employer-based Healthcare with Individual Accountability
Individual-based Healthcare
Employer-based
Defined Contribution Developments
FSAs
Employer-based Healthcare
Traditional (Use it or Lose it)
Special Purpose Non-Plan
Combination Accounts
Employer-based healthcare
Special Purpose Accounts
Incentive Matching

Are HSAs the Wave of the Future?Which Point of View Direction will We Take?
Yes, if….1. we recognize the HSA legislation and regulations as a good start and another
building block for consumerism and behavioral change.2. there is additional legislation/regulation to support large Er interests in providing
HSAs (use for healthcare only, Rx coverage problem, combination accounts).3. there is legislative support for the common use of FSAs for targeted needs, HSAs
as “Health Savings Accounts” and HRAs as “Health Reimbursement Arrangements.
No, because….1. they were not legislated/regulated with large employers in mind.2. of a desire to promote individual insurance over individual ownership (under
employer and individual policies)3. they are just a tool to cost shift to employees, they can not reward behavior change4. they are only desirable to the young, healthy, and wealthy

Are HSAs the right vehicle for large employer groups?
Yes, If………..
Or
No, Because…….
Need to Understand the Consumer Movement & the Transformation
that is Underway

The Fundamental Policy Question
Will Legislation/Regulation Use HSAs to:
… mainly promote portable Individual & Small Group Insurance,
OR
… expand Personal Care Account ownership through in both an employer-based and individual-based healthcare system thru HSAs, HRAs, and FSAs.

Growth of Personal Care Accounts
HRAs HSAs2000* None None2001* 19,000 None2002* 53,000 None2003* 394,000 None2004(est) 1-1.5M 400,0002005(est) 3.2 M 1.0M+2006(est) 6.0+M ???2007(est) 12-15M ???
* Deliotte Consulting

The Answer – Flexible Health Savings Accounts (FHSAs)
FHSAs would have the tax advantages of HSAs and the key flexibilities of HRAs.
Basic Principles:1. Retain personal responsibility goal of HSA/HDHPs2. Focus on Behavior Change3. Recognize value of Pay for Compliance as a driver for
behavior change and shared savings with personal responsibility
4. Expand adoption and funding of HSAs by large employers

Flexible Health Savings Accounts (FHSAs)The Next Generation
Four needs that would allow FHSAs the flexibility to:
1. Provide financial Rewards and Incentives for Behavioral Change.
2. Encourage Employer/Carrier FHSA contributions towards healthcare
3. Be provided with plan designs other than HDHPs
4. Address FHSA/HSA Technical Issues

FHSA Flexibilty to Provide Financial Rewards and Incentives for Behavioral
Change
1. Allow for compliance incentives under disease management programs (e.g. diabetes, asthma, CHF) and wellness initiatives (e.g. wellness assessments, smoking cessation, etc.).
2. Change Comparability Rule to mean all members under a given program of care or treatment, such as, a disease management or wellness program.
3. Rewards and/or incentives should not be limited by the deductible limit, but should be consistent with expected savings from programs for which participation is being rewarded.
FHSA Flexibility to Encourage Employer Contributions to Healthcare
1. Allow employers/carriers to voluntarily contract with employees to require employer/carrier funded FHSAs to be used only for healthcare expenses while employed and covered under the plan.
2. Remove cap on employer/carrier funded FHSA contributions or expand to at least the plan’s Maximum Out-Of-Pocket total exposure in a given calendar year.

FHSAs Flexibility to be Provided with Plan Designs Other than HDHPs
1. Preventive drugs include maintenance drugs. Drugs now defined as preventive by the Treasury Dept. can be covered below the deductible, while the cost of maintenance drugs is now included in the deductible.
2. Allow Rx to exist as carve out benefits at least for prescription drugs associated with chronic and persistent disease states
3. Allow “incentive only based” FHSAs for employer/carrier only funding under non-HDHPs (i.e. no initial FHSA funding or employee funding)
4. Allow some mental health and substance abuse benefits (besides EAPs) to be included under preventive care.

FHSA Flexibility - Technical Issues
1. Allow FHSA/HSAs to go into effect on the first day of coverage is effective.
2. Allow FHSA/HSA contributions for a full calendar year regardless of when a plan is effective.
3. Allow FHSA/HSAs to be used to pay for health coverage premiums (other than current limited use for (1) Premiums for coverage under the Consolidated Omnibus Budget Reconciliation Act (COBRA), and (2) premiums for HDHP coverage for those who receive federal or state unemployment compensation).
4. Allow Flexibility to "post-date" the FHSA/HSA effective date so that FHSA/HSA dollars can cover expenses incurred before the account was established. Allow the account to be opened under a "provisional status" until the necessary paperwork is filed, at which time the account becomes active.

The Ultimate Successful The Ultimate Successful Implementation of ConsumerismImplementation of Consumerism
It’s about moving from a It’s about moving from a
““benefitbenefit” ”
to anto an
““accumulating assetaccumulating asset.”.”