Congenital Renal Anomalies
29
Congenital Renal Congenital Renal Anomalies Anomalies Andrew Phan Andrew Phan MS4 MS4 November 2005 November 2005
Transcript of Congenital Renal Anomalies

Congenital Renal Congenital Renal AnomaliesAnomaliesAndrew PhanAndrew Phan
MS4MS4
November 2005November 2005


Antenatal UltrasonographyAntenatal Ultrasonography
• Antenatal ultrasonography is a routine Antenatal ultrasonography is a routine procedure in the management of pregnant procedure in the management of pregnant patients. patients.
• 90% of fetal kidneys can be identified by 17 90% of fetal kidneys can be identified by 17 to 20 weeks of gestation, and 95% by 22 to 20 weeks of gestation, and 95% by 22 weeks weeks
• Antenatal detection of renal anomalies has Antenatal detection of renal anomalies has changed approach to anatomic renal changed approach to anatomic renal disease and has led to controversial disease and has led to controversial therapies for obstructive uropathies therapies for obstructive uropathies
• Allows for early diagnosis of congenital Allows for early diagnosis of congenital urine flow impairments.urine flow impairments.

UltrasonographyUltrasonography
Ultrasonography examines:
• the dilatation of the urinary tract
• the echostructure of the renal parenchyma
• the volume of amniotic fluid
• the visualization of the fetal bladder.

Accuracy of ScreeningAccuracy of Screening
• Study done by Livera et al. in 1998Study done by Livera et al. in 1998• 6292 pregnant women reaching 28 weeks' 6292 pregnant women reaching 28 weeks'
gestation within the study period gestation within the study period • Compared antenatal diagnosis to post-Compared antenatal diagnosis to post-
natal diagnosisnatal diagnosis– 92 babies had abnormal antenatal scans92 babies had abnormal antenatal scans– Of those 92, 42 had abnormalities confirmed Of those 92, 42 had abnormalities confirmed
on postnatal U/S. (4/42 died, 21/42 with on postnatal U/S. (4/42 died, 21/42 with surgery to correct at 18 months)surgery to correct at 18 months)
– 7 were missed on antenatal U/S.7 were missed on antenatal U/S.

Renal AnomaliesRenal Anomalies
• Renal dysplasiaRenal dysplasia
• Renal hypoplasiaRenal hypoplasia
• Renal aplasiaRenal aplasia
• Multicystic Multicystic Dysplastic KidneyDysplastic Kidney
• Ureteropelvic Ureteropelvic Junction ObstructionJunction Obstruction
• Vesicoureteral refluxVesicoureteral reflux
• Ectopic uretersEctopic ureters
• UreterocelesUreteroceles
• Polycystic kidney Polycystic kidney diseasedisease
• Posterior Urethral Posterior Urethral valvesvalves


Normal Kidney Normal Kidney DevelopmentDevelopment• Kidney derives from intermediate Kidney derives from intermediate
mesodermmesoderm
• Pronephros is rudimentary kidney that Pronephros is rudimentary kidney that appears in third week of gestation, appears in third week of gestation, regresses, and has no known functionregresses, and has no known function
• Mesonephros is second transient kidney, Mesonephros is second transient kidney, from fifth to twelfth week of gestation. from fifth to twelfth week of gestation. Degenerates in cephalocaudal direction. Degenerates in cephalocaudal direction. Mesonephric duct gives rise to portions Mesonephric duct gives rise to portions of epididymis and ductus deferens in of epididymis and ductus deferens in boys (forms vestigial structure in girls)boys (forms vestigial structure in girls)
• Metanephros (definitive kidney) appears Metanephros (definitive kidney) appears during fifth week of gestation. Initiated during fifth week of gestation. Initiated by interaction between ureteric bud, a by interaction between ureteric bud, a branch of mesonephric ductbranch of mesonephric duct
• Ureteric bud is responsible form Ureteric bud is responsible form formation of kidney and urinary formation of kidney and urinary collecting system.collecting system.
• Nephrogenesis involves differentiation Nephrogenesis involves differentiation of mesenchyme into tubular and of mesenchyme into tubular and glomerular epitheliumglomerular epithelium

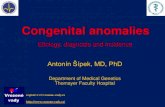
Pyramid
Collecting system
Lower pole
Cortex
CapsuleUpper pole
Normal Ultrasound Renal AnatomyNormal Ultrasound Renal Anatomy

Normal Renal Normal Renal MeasurementsMeasurements
Han BK, Babcock DS. Sonographic measurements and appearance of normal kidneys in children. AJR 1985; 145(3):611-616.

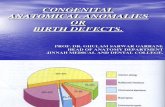
Fusion of right and left kidneys

Horseshoe KidneyHorseshoe Kidney• Fusion of the lower poles of the kidneys Fusion of the lower poles of the kidneys
midlinemidline
• 1/500 births. Seen in 7% of patients with 1/500 births. Seen in 7% of patients with Turner syndrome. Turner syndrome.
• Wilms tumors are 4x more frequent than in Wilms tumors are 4x more frequent than in general population. Other complications general population. Other complications include obstructive uropathy, related to include obstructive uropathy, related to ureteropelvic junction obstruction, calculi ureteropelvic junction obstruction, calculi and urinary tract infections. and urinary tract infections.
• Renal function is generally normal. Renal function is generally normal.

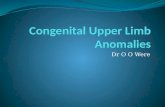
Dilation of renal pelvis, consistent with hydronephrosis

CT of separate patient with hydronephrosis.
Note the diilation of the pelvis with substance
that has similar echogenicity of water.

©2005 UpToDate®

HydronephrosisHydronephrosis• Often a transient findingOften a transient finding• Multiple etioligies, including urinary tract Multiple etioligies, including urinary tract
obstruction and vesicoureteral reflux. May obstruction and vesicoureteral reflux. May result in abnormal renal development and result in abnormal renal development and injury. injury.
• If found antenatally, requires evaluation after If found antenatally, requires evaluation after birth. birth.
• Bilateral hydronephrosis seen in 20 to 40% of Bilateral hydronephrosis seen in 20 to 40% of cases.cases.
• 5% of individuals who have antenatal 5% of individuals who have antenatal hydronephrosis will require surgical hydronephrosis will require surgical intervention intervention

Etiologies of HydronephrosisEtiologies of HydronephrosisTransient Transient 48%48%
PhysiologicPhysiologic 15%15%
Ureteropelvic junction (UPJ) obstructionUreteropelvic junction (UPJ) obstruction 11%11%
Vesicoureteral reflux (VUR)Vesicoureteral reflux (VUR) 9%9%
Megaureter (obstructed or unobstructed)Megaureter (obstructed or unobstructed) 4%4%
Multicystic dysplastic kidneyMulticystic dysplastic kidney 2%2%
Ureterocoele Ureterocoele 2%2%
Posterior urethral valvesPosterior urethral valves 1%1%
Other ( ectopic ureter, prune belly, urachal Other ( ectopic ureter, prune belly, urachal cyst, and urethral atresia)cyst, and urethral atresia)
8%8%
Woodward, M and Frank, D. Postnatal management of antenatal hydronephrosis. BJU International 2002; 89(2): 149-156.

RefluxReflux
• An etiology in 9% of individuals with hydronephrosis. An etiology in 9% of individuals with hydronephrosis. Predisposes individuals to chronic renal failure. Predisposes individuals to chronic renal failure.
• Best evaluated by voiding cysturethrogram (VCUG). Best evaluated by voiding cysturethrogram (VCUG). • Grade I- Ureter only Grade I- Ureter only • Grade II - Ureter, renal pelvis, calyces without dilatation Grade II - Ureter, renal pelvis, calyces without dilatation • Grade III - Dilatation or tortuosity of ureter and/or dilated pelvis Grade III - Dilatation or tortuosity of ureter and/or dilated pelvis • Grade IV - Shape of calyces maintained but dilated Grade IV - Shape of calyces maintained but dilated • Grade V - Gross dilation of collecting system Grade V - Gross dilation of collecting system • Management may include prophylactic antibiotics or surgical Management may include prophylactic antibiotics or surgical
interventionintervention


Cystic structures with no parenchymal development

Multicystic Dysplastic Multicystic Dysplastic KidneysKidneys• Kidney consists of groups of cysts with Kidney consists of groups of cysts with
connective tissue. Minimal or no renal connective tissue. Minimal or no renal parenchyma. parenchyma.
• 1:2,400 live births1:2,400 live births• Multicystic dysplastic kidney is often Multicystic dysplastic kidney is often
unilateral. unilateral. • Vesicoureteral reflux is common (20%) in Vesicoureteral reflux is common (20%) in
the contralateral kidneythe contralateral kidney• Current reccomendation is to evaluate for Current reccomendation is to evaluate for
reflux with serial ultrasounds reflux with serial ultrasounds • Increased risk of hypertension. Increased risk of hypertension.

Enlarged kidney with increased echogenicity. Poorly
differentiated parenchyma with no evidence of
macroscopic cysts.

Pulmonary hypoplasia secondary to
enlarged kidneys

Autosomal Recessive Polycystic Kidney Autosomal Recessive Polycystic Kidney DiseaseDisease
• Kidneys increased in size with microcysts. Increased Kidneys increased in size with microcysts. Increased echogenicity with poor parenchymal differentiation. echogenicity with poor parenchymal differentiation.
• Lungs may be hypoplastic secondary to kidney Lungs may be hypoplastic secondary to kidney enlargement. enlargement.
• Liver may be involved with cysts, congenital hepatic Liver may be involved with cysts, congenital hepatic fibrosis, and portal hypertension fibrosis, and portal hypertension
• ~1:25,000~1:25,000
• Wide spectrum of disease manifestation, even within Wide spectrum of disease manifestation, even within families. Most severe manifestations die in utero. Most families. Most severe manifestations die in utero. Most cases, however present by 1 year of age with renal cases, however present by 1 year of age with renal impairment and hypertension. impairment and hypertension.
• Treatment at this time is symptomatic and aimed at Treatment at this time is symptomatic and aimed at managing complications of disease. managing complications of disease.

Enlarged kidney with macroscopic cystic
structures in kidney. Kidney parenchyma is
evident. The kidney has increased echogenicity.

Bilateral enlargement of both kidneys. Increased echogenicity with cystic
structures seen. In 1/3 of cases hepatic cysts also
seen.

Autosomal Dominant Polycystic Kidney Autosomal Dominant Polycystic Kidney DiseaseDisease
• Usually not clinically apparent in young children Usually not clinically apparent in young children with onset usually during the fourth decadewith onset usually during the fourth decade
• Often bilateral involvement of kidneys with large Often bilateral involvement of kidneys with large cystic structures seencystic structures seen
• Cysts may also be present in liver, pancreas, Cysts may also be present in liver, pancreas, cerebral vessels and other organscerebral vessels and other organs
• ~1:700~1:700• Unlike ARPKD, congenital hepatic fibrosis is rareUnlike ARPKD, congenital hepatic fibrosis is rare• Presents with gross or microscopic hematuria, Presents with gross or microscopic hematuria,
hypertension, proteinuria, cyst infection and renal hypertension, proteinuria, cyst infection and renal insufficiencyinsufficiency
• Progresses to end stage renal failureProgresses to end stage renal failure


Works CitedWorks Cited
Behrman: Nelson Textbook of Pediatrics, 17th ed. 2004. Saunders, an Imprint of Elsevier.
Han BK, Babcock DS. Sonographic measurements and appearance of normal kidneys in children. AJR 1985; 145(3):611-616
Livera, LN, Brookfield, DS, Egginton, JA, Hawnaur, JM. Antenatal ultrasonography to detect fetal renal abnormalities: A prospective screening program. BMJ 1989; 298:1421.
Lonergan GJ, Rice RR, Suarez ES. Autosomal recessive polycystic kidney disease: radiologic-pathologic correlation. Radiographics. 2000. 20(3):837-55.
Mouriquand, PD, Wilcox, TD, and Troisfontaines, E. Antenatal and perinatal uro-nephrology:current questions and dilemmas. Pediatr Nephrol (1999) 13:938–944
Up To Date Online. www.utdol.com. 2005. Woodward, M and Frank, D. Postnatal management of antenatal hydronephrosis. BJU
International 2002; 89(2): 149-156.