Congenital Heart Diseasecircinterventions.ahajournals.org/content/circcvint/8/2/... · often...
11
1 A cquired right ventricular (RV) outflow tract stenosis and pulmonary regurgitation after conduit replacement often complicate the long-term course of the congenital heart disease patient. As such, patients with conduit dysfunction require repeat open-heart surgery for pulmonary valve replace- ment. In this regard, several series have demonstrated favor- able short-term outcomes after percutaneous pulmonary valve implantation (PPVI) in the pediatric population. 1–6 Whether the timing of valve replacement affects RV remodeling is an unanswered question, with some units advocating early inter- vention even in the asymptomatic individual to maximize the effects on RV form and function. 7–9 This study examines the intermediate-term effect of PPVI on RV size, function, and aerobic exercise capacity and the influence of age at interven- tion on these variables. See Editorial by Aboulhosn and Levi Methods Patient Population and Data Collection All patients who underwent Melody valve (Medtronic Inc, Minneapolis, MN) PPVI at the Hospital for Sick Children and Toronto General Hospital, Toronto, Ontario, between October 2005 and October 2011 were enrolled. Research Ethics Board approval was obtained at both institutions and informed consent obtained. Information gathered retrospectively from the medical charts in- cluded echocardiographic, radiographic, exercise testing, and car- diac MRI (cMRI) findings. Investigations were obtained within 3 months before the index procedure and after implant: echocardiog- raphy on 1 day, 3 and 6 months, and yearly thereafter, an exercise test and chest x-ray after 3 months and biyearly, and cMRI within Background—Percutaneous pulmonary valve implantation (PPVI) is a safe, less invasive alternative to surgical valve replacement for the congenital heart disease patient with right ventricular (RV) outflow tract dysfunction. The aim of this study was to determine whether reverse RV remodeling after PPVI was persistent in the longer term and whether timing of PPVI influenced outcomes. Methods and Results—Consecutive patients from the pediatric and adult congenital heart disease programs were enrolled. Cardiac MRI, echocardiography, metabolic exercise testing, chest radiography, and hemodynamics before intervention were compared with repeated follow-up measurements to assess changes over time. Fifty-one patients (including 23 patients <16 years old) were followed for a mean 4.5±1.9 (0.9–6.9) years after implantation, 59% of patients having available comparative cardiac MRI data. Freedom from any reintervention was 87% and 68% at 3 and 5 years, and freedom from surgery was 90% at 5 years. For every decade younger at implantation, there was an increase of 3.9%±1.0% in cardiac MRI left ventricular ejection fraction (P<0.001) and 2.4±0.9 mL/kg/min in maxVO 2 (P=0.005) and a decrease of 0.7±0.2 cm in RV end-diastolic dimension (P<0.001) after intervention. Younger patients displayed an additional decline in the RV/left ventricular end-diastolic volume ratio (P=0.05) and trended toward improved RV ejection fraction in late follow-up (50%±7% versus 41%±12%, P=0.07). Conclusions—This is the largest series to show that PPVI at a younger age yields incremental improvements in RV size and maximum oxygen consumption. Early valve implantation is associated with better RV function and should be considered in management planning for this population. (Circ Cardiovasc Interv. 2015;8:e001745. DOI: 10.1161/ CIRCINTERVENTIONS.114.001745.) Key Words: catheterization ◼ congenital ◼ heart defects ◼ tetralogy of Fallot © 2015 American Heart Association, Inc. Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.114.001745 Received September 20, 2013; accepted December 3, 2014. From the Department of Pediatrics, Division of Cardiology, Labatt Family Heart Center, The Hospital for Sick Children and Division of Cardiology (S.B., K.-J.L., R.C., M.K.F., B.W.M., C.M., L.B.), and University Health Network Toronto General Division (A.C., E.H., M.O.), University of Toronto School of Medicine, Toronto, Canada. Correspondence to Lee Benson, MD, The Hospital for Sick Children, 555 University Ave, Toronto, Ontario, Canada M5G 1X8. E-mail [email protected] Percutaneous Pulmonary Valve Implantation: 5 Years of Follow-Up Does Age Influence Outcomes? Sharon Borik, MD; Andrew Crean, MD, FRCPC; Eric Horlick, MDCM, FRCPC; Mark Osten, MD, FRCPC; Kyong-Jin Lee, MD, FRCPC; Rajiv Chaturvedi, MD, PhD, MRCP(UK); Mark K. Friedberg, MD; Brian W. McCrindle, MD, FRCPC; Cedric Manlhiot, BSc; Lee Benson, MD, FRCPC Congenital Heart Disease by guest on July 16, 2018 http://circinterventions.ahajournals.org/ Downloaded from
Transcript of Congenital Heart Diseasecircinterventions.ahajournals.org/content/circcvint/8/2/... · often...

1
Acquired right ventricular (RV) outflow tract stenosis and pulmonary regurgitation after conduit replacement
often complicate the long-term course of the congenital heart disease patient. As such, patients with conduit dysfunction require repeat open-heart surgery for pulmonary valve replace-ment. In this regard, several series have demonstrated favor-able short-term outcomes after percutaneous pulmonary valve implantation (PPVI) in the pediatric population.1–6 Whether the timing of valve replacement affects RV remodeling is an unanswered question, with some units advocating early inter-vention even in the asymptomatic individual to maximize the effects on RV form and function.7–9 This study examines the intermediate-term effect of PPVI on RV size, function, and aerobic exercise capacity and the influence of age at interven-tion on these variables.
See Editorial by Aboulhosn and Levi
Methods
Patient Population and Data CollectionAll patients who underwent Melody valve (Medtronic Inc, Minneapolis, MN) PPVI at the Hospital for Sick Children and Toronto General Hospital, Toronto, Ontario, between October 2005 and October 2011 were enrolled. Research Ethics Board approval was obtained at both institutions and informed consent obtained. Information gathered retrospectively from the medical charts in-cluded echocardiographic, radiographic, exercise testing, and car-diac MRI (cMRI) findings. Investigations were obtained within 3 months before the index procedure and after implant: echocardiog-raphy on 1 day, 3 and 6 months, and yearly thereafter, an exercise test and chest x-ray after 3 months and biyearly, and cMRI within
Background—Percutaneous pulmonary valve implantation (PPVI) is a safe, less invasive alternative to surgical valve replacement for the congenital heart disease patient with right ventricular (RV) outflow tract dysfunction. The aim of this study was to determine whether reverse RV remodeling after PPVI was persistent in the longer term and whether timing of PPVI influenced outcomes.
Methods and Results—Consecutive patients from the pediatric and adult congenital heart disease programs were enrolled. Cardiac MRI, echocardiography, metabolic exercise testing, chest radiography, and hemodynamics before intervention were compared with repeated follow-up measurements to assess changes over time. Fifty-one patients (including 23 patients <16 years old) were followed for a mean 4.5±1.9 (0.9–6.9) years after implantation, 59% of patients having available comparative cardiac MRI data. Freedom from any reintervention was 87% and 68% at 3 and 5 years, and freedom from surgery was 90% at 5 years. For every decade younger at implantation, there was an increase of 3.9%±1.0% in cardiac MRI left ventricular ejection fraction (P<0.001) and 2.4±0.9 mL/kg/min in maxVO
2 (P=0.005) and a decrease
of 0.7±0.2 cm in RV end-diastolic dimension (P<0.001) after intervention. Younger patients displayed an additional decline in the RV/left ventricular end-diastolic volume ratio (P=0.05) and trended toward improved RV ejection fraction in late follow-up (50%±7% versus 41%±12%, P=0.07).
Conclusions—This is the largest series to show that PPVI at a younger age yields incremental improvements in RV size and maximum oxygen consumption. Early valve implantation is associated with better RV function and should be considered in management planning for this population. (Circ Cardiovasc Interv. 2015;8:e001745. DOI: 10.1161/CIRCINTERVENTIONS.114.001745.)
Key Words: catheterization ◼ congenital ◼ heart defects ◼ tetralogy of Fallot
© 2015 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.114.001745
Received September 20, 2013; accepted December 3, 2014.From the Department of Pediatrics, Division of Cardiology, Labatt Family Heart Center, The Hospital for Sick Children and Division of Cardiology
(S.B., K.-J.L., R.C., M.K.F., B.W.M., C.M., L.B.), and University Health Network Toronto General Division (A.C., E.H., M.O.), University of Toronto School of Medicine, Toronto, Canada.
Correspondence to Lee Benson, MD, The Hospital for Sick Children, 555 University Ave, Toronto, Ontario, Canada M5G 1X8. E-mail [email protected]
Percutaneous Pulmonary Valve Implantation: 5 Years of Follow-Up
Does Age Influence Outcomes?
Sharon Borik, MD; Andrew Crean, MD, FRCPC; Eric Horlick, MDCM, FRCPC; Mark Osten, MD, FRCPC; Kyong-Jin Lee, MD, FRCPC; Rajiv Chaturvedi, MD, PhD, MRCP(UK);
Mark K. Friedberg, MD; Brian W. McCrindle, MD, FRCPC; Cedric Manlhiot, BSc; Lee Benson, MD, FRCPC
Congenital Heart Disease
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

2 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
1 year and then every 2 to 3 years. Hemodynamic data were mea-sured at the index procedure. All available clinical data points were analyzed. Late outcomes assessed included exercise and aerobic capacity, ventricular function and size, degree of pulmonary re-gurgitation, and RV to pulmonary artery (PA) pressure gradients. Out-of-province patients were contacted (n=6) and their reports req-uisitioned from referral centers.
EchocardiographyTwo-dimensional transthoracic echocardiography was performed on a Phillips IE-33 (Andover, Massachusetts) machine using accepted meth-ods,2,10 with a standardized clinical protocol performed by a research sonographer. Data were retrieved from clinical reports with missing or outlying data points reviewed by 1 of the authors (S. Borik). RV end-diastolic (RVED) dimension and left ventricular (LV) ejection fraction were measured using m-mode in the parasternal short axis cut of the ventricles2 and RV systolic pressure (RVSp) estimated using continuous wave Doppler from the tricuspid regurgitation jet velocity plus 5 mm Hg. Z-scores were calculated using accepted pediatric values.11 RV outflow tract gradient was calculated using continuous wave Doppler on paraster-nal views. RV function was evaluated as a qualitative measure integrating all echocardiographic views and scored: 1, moderate to severely reduced function; 2, mildly reduced function; or 3, good function.12 The degree of pulmonary insufficiency (PI) was evaluated by comparing the regurgitant jet width in the parasternal long and short axis views to the pulmonary valve annulus diameter and scored: 0, none; 1, trivial (jet width ≤1/3 of the pulmonary valve annulus); 2, mild (≥1/3 but ≤1/2 of the pulmonary valve annulus); 3, moderate (≥1/2 but less than the pulmonary valve annulus and regurgitation beginning in the pulmonary trunk), or 4, severe insuffi-ciency (jet width equal to the pulmonary valve annulus with regurgitation seen in the branch pulmonary arteries).2
MRICardiac MRI was performed on a 1.5 Tesla Avanto MRI system (Siemens Medical Solutions, Erlangen, Germany)2 using a standard protocol and was reviewed by a cMRI specialist (A. Crean) blinded to the study objectives. ECG-gated anatomic imaging of the heart was acquired using static and cine steady state free procession in the 2-, 3-, and 4-chamber views, short and long axis planes, and the RV out-flow tract. Cine phase contrast velocity mapping of the ascending and descending aorta, main and branch pulmonary arteries, and superior caval and pulmonary veins were obtained for blood flow assessment.2 Pulmonary regurgitant fraction was calculated as percent backward flow over forward flow in the right outflow tract and main pulmonary artery. RV and LV volumes were assessed manually at end-diastole and systole (Mass Analysis and CV Flow, Medis Medical Imaging Systems, Leiden, the Netherlands) and ventricular ejection fraction calculated using standard formula.
Table 1. Demographic and Clinical Characteristics
Cohort (n=51)
Age at index procedure, y 20.2±10.8
Weight, kg 58.3±16.0
Female:Male 23:28
Follow-up, y 4.5±1.9
Diagnoses
TOF or DORV with PS 17
TOF with PA 14
PA with intact ventricular septum 2
TOF with absent pulmonary valve 2
Common arterial trunk 8
Ross procedure for aortic valve disease 5
Aortic atresia 1
Congenitally corrected transposition 2
Years from last cardiac surgery 12.2±7.1
RVOT dysfunction (n=49)
Predominantly PI 2
Predominantly PS 16
Both PI and PS 31
RVOT morphology
Homograft 17
Bioprosthetic conduit or valve 31
Miscellaneous* 3
Number of previous surgeries
1 10
2 19
3 14
4 8
Number of previous interventions (n=42)
None 8
1 13
2 16
≥3 5
DORV indicates double outlet right ventricle; PA, pulmonary atresia; PI, pulmonary insufficiency; PS, pulmonary stenosis; RVOT, right ventricular outflow tract; and TOF, tetralogy of fallot.
*Included 2 REV (réparation à l’ètage ventriculaire) patients and 1 implant into a single pulmonary artery.
WHAT IS KNOWN
• Percutaneous pulmonary valve implantation is an ef-fective alternative to open heart surgery in the con-genital heart disease patient with right ventricular outflow tract dysfunction.
• Several published series have shown acute reduc-tions in the outflow tract gradients and right ven-tricular pressures after percutaneous pulmonary valve implantation, along with favorable effects on ventricular volume, degree of pulmonary insuf-ficiency, and exercise capacity, maintained at the 1-year mark.
WHAT THE STUDY ADDS
• Our large cohort of children and adults displays persis-tent hemodynamic and functional improvements after percutaneous pulmonary valve implantation, well into intermediate-term follow up (mean 4.5 years).
• Younger patients (≤16 years of age), implanted at lower right ventricular volumes, exhibit incremental improvements in ventricular size and function and maximal oxygen consumption.
• With a low reoperation rate of 10% at 5 years and the expanding possibilities of percutaneous reinterven-tion, our study findings suggest considering percu-taneous pulmonary valve implantation at a younger age and smaller right ventricular volumes.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

3 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
Cardiopulmonary Exercise Testing and Chest RadiographsMetabolic exercise testing was performed on a programmable ramp ergometer (Ergometrics-800S, Ergoline, Bitz, Germany), recording endurance time, heart rate, blood pressure, and maximal workload.2 Respiratory data were analyzed for maximal oxygen consumption and anaerobic threshold as an average over 20 s (Max-1, Physio-Dyne Instrument Corporation, Quogue, New York). Raw exercise and met-abolic data are presented with predicted values13 for weight and body surface area. Digital chest radiograms were reviewed by one author (S. Borik) and graded for the presence of stent fracture(s) according to a previously accepted classification.14
Statistical AnalysisStatistical analysis was performed using SAS Statistical Software version 9.1 (SAS Institute, Cary, NC). Data were described as mean±standard deviation, medians with a range, and frequency as
appropriate. Analysis was performed using paired t-tests for com-parative data sets before and after PPVI and Fisher exact test for descriptive data. Changes over time after PPVI were assessed using linear regression models (general estimating equations for parameter estimation), adjusted for repeated measures through an autoregres-sive covariance structure with measured parameters as the dependent variable and time since implantation as the independent variable. Differences in rate of change over time were assessed using the in-teraction with time term in the regression models. All sequential data were recorded and annualized changes calculated, correcting for the number of data points per patient. Freedom from reintervention is presented using Kaplan–Meier curves with log-rank test to compare freedom from reintervention between eras (before and after 2008). All analyses were adjusted for repeated measures to account for the number of examinations per patient. A P value of ≤0.05 was consid-ered statistically significant. Analysis was performed on the full co-hort as well as 2 subgroups based on median age, above and below 16 years of age. For change over time, early outcomes were designated
Table 2. Pre- and Postprocedural Results
n Prior to n Early N Late* P1† P2‡
Hemodynamics
RV to PA pressure gradient, mm Hg 49 35±17 47 11±7 … … <0.001 …
RV systolic pressure, mm Hg 49 61±18 48 41±11 … … <0.001 …
RV/Ao systolic pressure ratio 47 0.68±0.20 44 0.45±0.24 … … <0.001 …
Echocardiographic data
Median time from PPVI (IQR), y … … … 0.008 (0.001–0.11) … 1.9 (1.0–3.3) … …
RV-to-PA pressure gradient, mm Hg 48 64±23 77 38±17 173 35±15 <0.001 <0.001
Estimated RVSp, mm Hg 41 79±18 68 57±15 144 52±16 <0.001 <0.001
RV systolic/systemic blood pressure 40 0.76±0.19 66 0.52±0.13 143 0.47±0.15 <0.001 <0.001
RVED dimension z-score 43 3.8±2.4 57 3.2±1.2 159 3.4±1.2 0.07 0.07
Exercise testing data
Median time from PPVI (IQR), y … … … 0.41 (0.25–0.57) … 3.2 (2.2–4.1) … …
Maximum VO2, mL/min/m2 40 23.2±6.8 33 26.0±6.2 50 26.4±7.1 0.07 0.03
% predicted maximum VO2
40 56±14 33 61±14 50 63±15 0.16 0.04
% predicted VO2 at anaerobic
threshold31 54±16 33 59±15 46 54±23 0.24 0.97
Work performed, watts 39 88±27 33 93±28 49 111±35 0.44 0.001
% predicted work performed 34 56±14 31 58±12 47 57±13 0.60 0.72
Peak heart rate, bpm 38 158±27 34 162±27 51 168±19 0.53 0.04
cMRI data
Median time from PPVI (IQR), y … … … 0.53 (0.37–0.63) … 3.4 (1.4–4.6) … …
RVEDVi, mL/m2 29 136±43 20 115±29 22 117±37 0.06 0.07
RVESVi, mL/m2 25 79±41 20 65±25 21 71±38 0.18 0.43
RV stroke volume, mL/min/m2 22 57±16 18 50±10 18 51±12 0.10 0.12
RVEF, % 28 43±12 20 44±10 21 44±10 0.76 0.74
LVEDVi, mL/m2 27 92±18 20 98±20 22 99±18 0.25 0.17
LVESVi, mL/m2 24 41±15 20 42±11 20 47±12 0.86 0.12
LV stroke volume, mL/min/m2 21 53±15 18 57±12 16 56±12 0.36 0.56
LVEF, % 27 57±9 20 57±6 21 53±7 1.00 0.07
RVEDVi/LVEDVi ratio 25 1.51±0.44 20 1.18±0.23 21 1.21±0.37 0.004 0.01
Ao indicates aortic; cMRI, cardiac MRI; IQR, interquartile range; LV, left ventricle; LVEDVi, LV end-diastolic volume index; LVEF, left ventricular ejection fraction; LVESVi, LV end-systolic volume index; PA, pulmonary artery; PPVI, percutaneous pulmonary valve implantation; RV, right ventricle; RVED, RV end-diastolic; RVEDVi, RVED volume index; RVEF, RV ejection fraction; RVESVi, RV end-systolic volume index; RVSp, RV systolic pressure; and VO
2, oxygen consumption.
*Hemodynamic data obtained during the PPVI procedure; late after the procedure was defined as >3 months for echocardiographic data; >12 months for exercise testing and cMRI data.
†P1, before procedure vs early after the procedure.‡P2, before procedure vs late after the procedure.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

4 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
as occurring within the first 3 months after PPVI for hemodynamic and echo results and 1 year for cMRI and exercise data, based on the clinical protocol at our institutions. Ninety-six percent of patients had serial echocardiograms in follow-up, 75% had exercise testing and chest radiography, and 59% had cMRIs before and after the proce-dure (71% had cMRI in follow up).
ResultsPatient PopulationAll 51 patients who underwent PPVI between October 2005 and October 2011 were reviewed and followed for a mean of 4.5±1.9 years (range 0.9–6.9 years, median 4.2 years; Table 1). Twenty-eight were male and mean age was 20.2±10.8 (median 16.2 [10.8–68.7]) years, with 23 patients <16 years of age (mean 13.3±1.6 years) and 28 patients >16 years (mean 25.9±11.8 years). Thirty-two patients had
conduit stenting before valve implantation, 15 at a previ-ous procedure (4.0±2.6 [0.1–7.6] years before PPVI, one of which was placed in preparation for PPVI).15 Balloon diam-eters used for the Melody valve implantations averaged 21±1 mm, and procedure time was 147±54 (65–309) minutes. Patients underwent an average of 5 echocardiograms (0–13, higher for earlier patients), 0.01 to 6.5 years after PPVI; and averaged 2 exercise tests (0–5), 0.2 to 6.4 years after implantation; 2 chest x-rays (0–6), 0.01 to 6.5 years after PPVI; and 1 cMRI (0–3), 0.01 to 6.2 years after the index procedure. One out-of-province patient was lost to follow-up and did not have a postprocedural echocardiogram but was clinically well. The mean time interval between the index procedure and the first cMRI was 0.9 years (range 0.4–1.2 years, median 0.6 years).
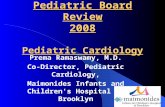
Figure 1. Change over time in right ventricular variables before and after percutaneous pulmonary valve implan-tation (PPVI). Red circles represent assessments before PPVI (black squares represent averages, black horizontal bars standard deviation), gray circles for assessments after PPVI (black solid line is the line of best fit and dotted lines 95% confidence intervals). PA indicates pulmo-nary artery; RV, right ventricle; RVEDVi, RV end-diastolic volume index; RVESVi, RV end-systolic volume index; and RVSp, RV systolic pressure.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
BeforePPVI
(n=46)
A�er PPVI(n=41)
6 months(n=40)
1 year(n=28)
2 years(n=37)
3 years(n=28)
4 years(n=23)
5 years(n=15)
6 years(n=9)
Perc
enta
ge o
f Pa�
ents
Time from PPVI
Severe
Moderate
Mild
Trivial
None
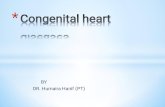
Degree of Pulmonary Insufficiency
Figure 2. Degree of echocardiographic pulmonary insufficiency before and sequentially after valve implantation. n indicates number of patients in each time period; and PPVI, percutaneous pulmo-nary valve implantation.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

5 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
Early ResultsAll patients exhibited immediate hemodynamic improve-ment after PPVI, including significant decreases in RV to PA pressure gradient, RVSp, and RV to systemic pressure ratio (Table 2). There was no statistical improvement in exer-cise variables early after implantation. From cMRI data, the indexed RV end-diastolic volumes (RVEDVi; P=0.06) and the ratio between RV and LV indexed volumes (P=0.004) decreased on the first postprocedural cMRI, whereas there was no change in LV functional parameters.
Late ResultsRV functional parameters did not change significantly in later follow-up (Table 2; Figure 1), with the reduction of the RVEDVi (cMRI) persistent (117±37 mL/m2; P=0.07). The RV to PA pressure gradient and the RVSp remained lower than before the procedure (P<0.001) and persisted in late follow-up, with no patient developing severe PI (Figure 2).
Early improvements seen in RV volumes and function were less pronounced through late follow-up, although overall they remained improved from values before PPVI (Figure 1). Assessment of annualized changes after the index procedure did not disclose any clinically significant differences. Absolute maximal and percent-predicted oxygen consumption was sig-nificantly improved in late follow up (Table 2; Figure 3), as were exercise duration and peak heart rate. Total work per-formed improved in follow-up; however, there was not a sta-tistically significant increase in percent-predicted values.
Outcomes by Age at Index ProcedureA younger age at the index procedure was associated with a smaller RVED dimension (−0.71±0.21 cm per decade of age and z-score, −1.29±0.36 per decade age), both P<0.001 at the first assessment after PPVI. Other variables such as the RVSp to systemic pressure ratio (−0.02±0.01 lower per decade, P=0.04), echocardiographic RV function (0.25±0.09 points higher per decade, P=0.008), and cMRI LV ejection
fraction (3.86±1.02% higher per decade, P<0.001) were noted to be better statistically, but of unclear clinical significance. Younger patients at intervention also exhibited improved exercise capacity on the first cardiopulmonary stress test after PPVI, with higher maximal oxygen consumption by 2.40±0.85 mL/kg/min per decade of age (P=0.005), a relation-ship that was not significant before the procedure (Table 3). Percent-predicted exercise values were also higher in younger patients, including percent-predicted VO
2 at anaerobic thresh-
old (higher by 13.6±6.0% per decade of age [P=0.02]) and percent-predicted maximal VO
2 (3.8±1.9% per decade of age
[P=0.05]).In an attempt to determine whether there was a favorable
age for valve implantation, serial post-PPVI measures were compared in patients above and below the median cohort age of 16 years (Table 4). The 2 age groups did not differ significantly in demographic parameters, criteria for inter-vention, or RV volumes (Table 3). After the procedure, the younger aged group displayed a smaller RV size and bet-ter biventricular function on sequential echocardiograms and cMRI. Additionally, RV size was smaller in follow-up in the younger group with a gradual, but nonsignificant decrease in RVEDVi and a statistically significant decline in the ratio of RVEDV/LVEDV compared with a gradual increase in these parameters in the older group (P=0.10 and 0.05, respectively). Furthermore, the younger patients dis-played a trend toward better RV function on cMRI in late follow up (RVEF 50±7% in those ≤16 years versus 41±12% in the older group, P=0.07; Table 4) and statistically signifi-cant better RV function on echo (2.8±0.5 or good to mildly reduced RV function for those ≤16 years versus 1.9±0.9, mildly to moderately reduced RV function in those >16 years; P<0.001).
Time to ReinterventionFreedom from reintervention (percutaneous or surgical) was 87% and 68% at 3 and 5 years, and freedom from reoperation was 90%
Figure 3. Change over time in left ven-tricular and exercise parameters before and after percutaneous pulmonary valve implantation (PPVI; legend as in Figure 2). LV indicates left ventricle; LVEDVi, LV end-diastolic volume index; and VO2, oxygen consumption.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

6 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
at 5 years (Figure 4). These included 2 RV to PA conduit replace-ments, 1 pulmonary valve replacement, 1 aortic valve and root replacement and pulmonary homograft implantation for infec-tious endocarditis, and an arterial switch operation and occurred in the first 14 patients who underwent valve implantation. The patient with endocarditis had a common arterial trunk and pre-sented 5 years after PPVI with multiple aortic root vegetations and vegetation on the implanted valve (Gram-positive cocci).
Freedom from reintervention was 100% at 2 years for all patients since 2008 (Figure 4). Seven patients (14%) under-went percutaneous reintervention at 3.6±2.1 (0.3–6.0) years after the index procedure, including 3 revalving (Melody-within-Melody), 2 Sapien (Edwards Lifesciences Corp, Irvine Ca) valve implantations within the Melody valve, and 2 bal-loon dilations of the Melody valve. In most of these cases, reintervention was caused by restenosis and RV hypertension.
Eighteen percent of patients had evidence of minor (type 1) stent fractures on digital chest radiography, and 3% exhib-ited stent facture with loss of stent integrity. Of these patients, 63% required reintervention during the study period versus 23% without a stent fracture (P=0.05). Eighty-eight percent of fractures were in patients implanted (before 2008), with
only a quarter of these having been prestented. However, the correlation between prestenting and the absence of stent fracture was not statistically significant (P=0.06), nor was there a correlation between age and the presence of a stent fracture.
Factors Associated With Improved OutcomesImproved maximal VO
2 and percent-predicted maximal
VO2 were significantly associated with a younger age at the
index procedure, lower preimplantation right-sided pressures, and better ventricular function and aerobic capacity before implantation (Table 5). Melody implantation within a pre-existing stent was also associated with an improved aerobic result and with better biventricular ejection fractions by cMRI after the procedure (Tables 5 and 6). Preparing the conduit for implantation was associated with a higher LV ejection fraction (5%±2%, P=0.006), better RV function (0.6%±0.2 points, P<0.001), a smaller RV (−0.8±0.3 cm, P=0.007), and lower RVSp (−9±3 mm Hg, P=0.01, echocardiographic), early after implantation, compared with those not stented. However, prestenting was not associated with a lower RV to PA pres-sure gradient. Interestingly, implantation within a homograft
Table 3. Patient Characteristics by Age Before PPVI
Characteristic n Age, y (≤16 y) n Age,y (>16 y) P Value
Age at catheterization, y 23 13.3±1.6 28 25.9±11.8 …
Follow-up duration, y 23 4.8±1.8 28 4.2±2.0 0.27
Years from previous operation, y 23 6.3±1.6 28 13.6±7.2 0.002
Diagnosis, n 23 … 28 … 0.22
Right sided obstruction … 15 … 22 …
Left sided obstruction … 3 … 3 …
Common arterial trunk … 5 … 3 …
RVOT dysfunction, n 22 … 27 … 0.41
Predominant PI … 0 … 2 …
Predominant PS … 8 … 8 …
PI and PS … 14 … 17 …
RVOT morphology, n 23 … 28 … 0.73
Homograft … 8 … 9 …
Stent … 13 … 18 …
Miscellaneous* … 2 … 1 …
RV systolic pressure, mm Hg 23 62±15 26 60±20 0.69
Systolic aortic pressure, mm Hg 23 85±8 25 96±20 0.02
RV-PA gradient, mm Hg (cath) 23 39±13 26 32±19 0.10
RVED dimension z-score (echo) 20 2.53±1.6 23 4.97±2.3 0.001
Maximal VO2, mL/min/m2 18 25.1±5.7 22 21.7±7.4 0.11
% predicted VO2 at anaerobic threshold 13 62±16 18 49±15 0.04
RVEDVi, mL/m2 11 128±41 18 142±45 0.39
RVESVi, mL/m2 10 67±34 15 87±44 0.21
Pre RVEF, % 14 47±12 17 40±12 0.20
Pre LVEF (MRI), % 10 60±7 17 55±10 0.16
LVEF indicates left ventricular ejection fraction; PA, pulmonary artery; PI, pulmonary insufficiency; PPVI, percutaneous pulmonary valve implantation; PS, pulmonary stenosis; RV, right ventricle; RVED, RV end-diastolic; RVEDVi, RVED volume index; RVEF, RV ejection fraction; RVESVi, RV end-systolic volume index; RVOT, right ventricular outflow tract; and VO
2, oxygen
consumption.*Included 2 REV (réparation à l’ètage ventriculaire) patients and 1 implant into a single pulmonary artery.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

7 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
showed considerable advantage in aerobic capacity to that in a bioprosthetic valve. Furthermore, younger patients who had higher aerobic capacity, smaller ventricular volumes, and preserved function before implantation had better functional results for RV and LV ejection fractions (cMRI) after implan-tation (Table 6).
DiscussionPPVI has become an accepted, less invasive alternative to open heart surgery for the congenital heart disease patient with RV outflow tract dysfunction in both pediatric and adult populations. Several groups, including our own, have shown favorable short-term results after PPVI with the Melody valve.1,2,16–19 Bonhoeffer and colleagues, pioneers in the use of this technology, reported a series of 155 patients followed echocardiographically for a median 28.4 months (2.4 years) after valve implantation,5 documenting a significant initial reduction in RVSp, pressure gradient across the pulmonary valve, improved valvar competence, and a 70% freedom from reintervention at 70 months. Our series further details the trajectory of these outcomes in the intermediate term (mean 4.5±1.9 years, median 4.2 years) from a large cohort with a wide age range at time of implantation. With a longer mean follow-up than previous series, we also document low rein-tervention rates and, importantly, low reoperation rates (10% over 5 years).
Our cohort also displayed a low (<2%) incidence of Melody valve-related infective endocarditis, in keeping with the expe-rience of other large centers.20 Additionally, the freedom from reintervention rate improved after 2008, due in part to better patient selection and enhanced technical improvements, such as valve implantation within a previously stented outflow tract. Earlier patients were also more likely to exhibit radiographic stent fracture, which was also associated with an increased rate of reintervention, in correlation with previous findings of the US Melody Valve Trial.14 Although prestenting was asso-ciated with various functional advantages in our patients, there was no associated statistically significant reduction in the RV to PA gradient observed compared with those not stented. That there were a significant proportion of patients with biopros-thetic valves, and thus a limited internal hemodynamic office, may have influenced this finding. Prestenting did, however, show a trend for fewer radiographic stent fractures, and this, in turn, likely translated into lower rates of reintervention.
As noted by our group2 and other investigators,1,16 the present patient cohort showed an immediate hemodynamic improve-ment with a significant decrease in RVSp and the RV to PA pressure gradient invasively and by echocardiography. Unlike the US Melody Trial,16 we noted an overall improvement in aerobic capacity, mainly late after implantation. However, when examining the results over time, an increase only in phys-ical working capacity continued throughout the study period, whereas aerobic capacity reached a plateau in the longer term.
Table 4. Serial Findings After PPVI: According to Age
N ≤16 y Change/Year n >16 y Change/Year P1 P2
Echocardiographic
RV to PA gradient, mm Hg 153 39±15 1.1 (0.8) 114 33±16 0.2 (0.6) 0.21 0.88
Estimated RVSp, mm Hg 131 54±15 −1.1 (1.1) 97 54±16 −0.3 (1.0) 0.24 0.87
RVED dimension, cm 137 3.0±1.2 0.1 (0.1) 103 3.8±1.1 0.3 (0.1) <0.001 0.45
RVED dimension z-score 137 2.4±2.5 0.1 (0.1) 103 4.1±2.1 0.5 (0.1) <0.001 0.53
LVEF, % 135 65±8 −0.7 (0.5) 101 61±10 −1.8 (0.4) 0.009 0.68
RV function (3-point scale) 137 2.8±0.5 0.1 (0.0) 114 1.9±0.9 −0.1 (0.0) <0.001 0.67
Exercise test
Maximal VO2, mL/min/m2 43 24.8±6.1 −0.2 (0.4) 45 27.6±7.0 −1.2 (1.2) 0.27 0.18
Work performed, watts 43 87±22 +4.1 (1.9) 43 121±35 +5.1 (1.5) 0.09 0.20
Exercise duration, min 45 8.2±2.2 +0.2 (0.1) 42 10.2±3.0 +0.8 (0.2) 0.36 0.11
cMRI
RVEDVi, mL/m2 25 110±23 −1.6 (1.6) 24 123±42 5.5 (3.3) 0.64 0.10
RVESVi, mL/m2 24 62±17 1.5 (1.9) 24 76±42 9.2 (5.0) 0.55 0.27
RVSVi, mL/min/m2 24 52±12 −1.1 (0.8) 18 48±10 0. 9 (0.5) 0.13 0.05
RVEF, % 24 50±7 −0.3 (0.6) 24 41±12 −1.9 (1.1) 0.07 0.78
LVEDVi, mL/m2 25 103±18 −0.2 (1.2) 24 94±18 −0.9 (1.0) 0.30 0.98
LVESVi, mL/m2 24 45±10 0.2 (0.6) 23 45±13 1.6 (1.7) 0.61 0.31
LVSVi, mL/min/m2 24 59±12 0.3 (0.3) 16 53±12 2.2 (1.8) 0.48 0.29
LVEF, % 24 57±6 −0.5 (0.8) 24 52±8 −2.5 (0.9) 0.12 0.46
RVEDVi/LVEDVi 25 1.1±0.2 −0.0 (0.0) 22 1.3±0.4 0.1 (0.0) 0.21 0.05
Values adjusted for repeated measures. P1, difference between age groups for values; P2, difference between groups for change/year from the interaction term between years and age group in the regression models. Ao indicates aortic; cMRI, cardiac MRI; LV, left ventricle; LVEDVi, LV end-diastolic volume index; LVEF, left ventricular ejection fraction; LVESVi, LV end-systolic volume index; LVSVi, LV stroke volume index; PA, pulmonary artery; PPVI, percutaneous pulmonary valve implantation; RV, right ventricle; RVED, RV end-diastolic; RVEDVi, RVED volume index; RVEF, RV ejection fraction; RVESVi, RV end-systolic volume index; RVSp, RV systolic pressure; RVSVi, RV stroke volume index; and VO
2, oxygen consumption.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

8 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
This may be partly a result of the nature of this study popu-lation, which included all consecutive patients undergoing Melody valve implantation, most of whom had mixed disease
with a significant degree of PI before the procedure. This ele-ment has been previously shown to be associated with a lack of improvement in exercise capacity after PPVI.21,22 The lack of aerobic improvement in follow-up may also be manifest because of later timing of valve implantation in RVs, which have lost their ability for persistent reverse remodeling, such that the initial positive effects gradually declined in follow-up.
Immediately after the procedure, confirming observations by other series,6,16 there was a decrease in RVEDVi and the ratio between RVEDV and LVEDV and a relative increase in LVEDVi. In this regard, the Lurz et al study from Great Ormond Street, London, examined the functional outcomes before, 1 month after, and 1 year after PPVI.6 They showed favorable physiological changes at 1 month, which persisted at 1 year, but with no additional RV remodeling or func-tional improvement thereafter. To explore further changes over time, we assessed serial echocardiographic, exercise testing, and cMRI findings after the procedure. Our obser-vations support those from Lurz’s group, suggesting that most early changes seen after PPVI plateau in the following months and years after the procedure. Furthermore, follow-up in our cohort beyond the 1-year timeframe showed no further increase in aerobic capacity and biventricular func-tion, accompanied by a gradual rise in RV volume, yet with a continued decrease in RVSp and RV to PA pressure gra-dient and an increase in physical work capacity. These late changes may reflect a modified unnatural history influenced predominately by the outflow diameter achieved, underlying cardiac anatomy, and the patient’s age at the time of inter-vention. Despite this reduction or reversal in the slope of improvement, the functional and volumetric findings of the cohort at 5 years were for the most part significantly better in comparison with their status before the procedure. In addi-tion, the low reoperation rate and high interventional success suggest that PPVI favorably influences the interventional history of this patient group and postpones the requirements for repeat surgery, whereas improving functional capacity, at least for the intermediate-term.
From observations in the pediatric cohort (at a younger age than most previous series), we noted that younger age at implantation was associated with improved biven-tricular function and aerobic capacity and a lower RV size after implantation compared with those intervened on at an older age. Although most functional and demographic characteristics were not different between the 2 cohorts, RVED dimension z-score and RVEDVi were lower in the younger patients before valve implantation (although nonsignificantly in the MRI data), suggesting that age at the procedure may be a surrogate for RV volume and for the duration of adverse loading conditions before valve implantation. In this regard, studies assessing the timing of surgical pulmonary valve replacement have suggested an improved ventricular recovery if valve competence is achieved at a younger age, at a RVEDVi ≈150 to 160 mL/m2 and before the development of RV dysfunction.7–9 In a recent clinical assessment, Lee and colleagues from South Korea9 analyzed a large group undergoing surgical pulmo-nary valve replacement for chronic PI and found that the optimal indexed RV volumes before surgery that lead to
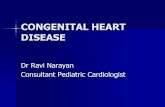
Figure 4. Freedom from reintervention after percutaneous pulmo-nary valve implantation (PPVI). A, Freedom from any surgical or percutaneous reintervention (dotted line=95% confidence inter-val). B, Comparison of surgical vs percutaneous freedom from reintervention. C, Freedom from reintervention by time period.
Table 5. Factors Associated With Maximal VO2 After PPVI (First Postimplant Study)
EST (SE) P Value
Age at catheterization −0.24 (0.09) 0.005
Pre RA pressure −0.66 (0.24) 0.007
Pre systolic RVSp (cath) −0.25 (0.08) 0.004
Pre maximal VO2
0.95 (0.14) <0.001
Pre RV cardiac index 8.28 (4.06) 0.04
Pre RVEF (MRI) 0.14 (0.08) 0.08
Pre LVESVi −0.20 (0.09) 0.02
Previous stenting 3.79 (1.90) 0.05
Homograft 6.68 (2.30) 0.004
Bioprosthetic valve −5.01 (2.14) 0.02
EST (SE) indicates parameter estimate from the regression model (standard error); LVESVi, LV end-systolic volume index; PPVI, percutaneous pulmonary valve implantation; PRE, preimplant variable; RA, right atrial; RV, right ventricle; RVEF, RV ejection fraction; RVSp, RV systolic pressure; and VO
2, oxygen consumption.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

9 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
normalization of RV volumes and function after surgery were a RVEDVi of ≤163 mL/m2 and end-systolic volume of ≤80 mL/m2. Previous groups have reported similar ranges of indexed end-diastolic RV volumes (150–170 mL/m2) and RVESVi (80–90 mL/m2) before surgery for opti-mal ventricular rehabilitation.7,8,23 Our results support these observations in part, suggesting younger patients whose RVs have not dilated to the extreme fare better than older patients with larger chamber dimensions and may have an enhanced potential for improvement in dimensions and function. Time will tell whether earlier and more aggres-sive rehabilitation of the right ventricle will be associated with more favorable clinical outcomes.
Improved aerobic capacity and biventricular function after PPVI were not solely associated with younger age, but also with a favorable hemodynamic profile before valve implantation, including a better aerobic capacity and ventricular function, pre-vious stenting of the outflow tract, and a homograft rather than a bioprosthetic valve in the outflow tract. Although these fac-tors did not significantly correlate with improved freedom from reintervention, they do suggest a patient profile, which may pre-dict enhanced benefit from valve implantation. Additionally, the expanding possibilities of reintervention after PPVI, including revalving with a second percutaneous valve5,18 further deferring surgical intervention, provides a rationale for percutaneous valve implantation at younger ages and smaller RV volumes.
LimitationsThe study is a retrospective observational study and suffers the drawbacks of retrospective data collection. The study group was small and only 59% of patients had a cMRI before and after implantation, limiting the power to assess events after
intervention and perform a multivariate analysis. Additionally, although attempts were made to have a uniform follow-up pro-tocol, it was variable such that the timing of functional changes had to be described arbitrarily into early and late and the num-ber of follow up examinations per patient required statistical adjustment for repeat measures. Z-scores used for echocardio-graphic data were used for the entire cohort and have not been validated in adult patients and as such may be overestimated in larger patients. Finally, the study group was anatomically and physiologically heterogeneous, such that the indications for intervention were mixed, with too few pure PI or PS patients to separate into respective groups. However, all patients met the clinically accepted indications for intervention. Thus, we think our conjecture of the effect of RV volumes remains valid.
ConclusionsPPVI with the Melody valve has favorable intermediate-term results with low reoperation rates. The degree of some early improvements decreases in later follow up, yet the patients dis-play significantly better functional and volumetric findings at 5 years, in comparison with their status before the procedure. Somewhat improved functional outcomes and RV dimensions were found in younger patients implanted at smaller RV volumes.
DisclosuresNone.
References 1. Khambadkone S, Coats L, Taylor A, Boudjemline Y, Derrick G, Tsang
V, Cooper J, Muthurangu V, Hegde SR, Razavi RS, Pellerin D, Deanfield J, Bonhoeffer P. Percutaneous pulmonary valve implantation in humans: results in 59 consecutive patients. Circulation. 2005;112:1189–1197. doi: 10.1161/CIRCULATIONAHA.104.523266.
Table 6. Factors Associated With Ventricular Function After PPVI (Univariable Models Early After PPVI)
RVEF LVEF
EST (SE) P Value EST (SE) P Value
Age ≤16 y 5.78 (3.31) 0.08 4.87 (2.13) 0.02
Pre RV-PA gradient (cath) 0.24 (0.09) 0.009 0.14 (0.06) 0.03
Pre % predicted maximal VO2
0.31 (0.15) 0.04 0.23 (0.09) 0.01
Pre RVEDVi −0.13 (0.02) <0.001 −0.05 (0.02) 0.01
Pre RVESVi −0.18 (0.03) <0.001 −0.07 (0.02) <0.001
Pre RV cardiac index 6.26 (2.64) 0.02 7.33 (1.41) <0.001
Pre RVEF 0.58 (0.08) <0.001 0.33 (0.05) <0.001
Pre RV/LV volumes −13.94 (2.35) <0.001 −5.55 (1.96) 0.005
Pre LVEDVi 0.03 (0.09) 0.73 0.05 (0.05) 0.24
Pre LVESVi −0.19 (0.14) 0.17 −0.14 (0.05) 0.01
Pre LVSVi 0.25 (0.10) 0.02 0.17 (0.05) 0.001
Pre LVEF (MRI) 0.62 (0.15) <0.001 0.48 (0.08) <0.001
Pre LVEF (echo) 0.20 (0.15) 0.20 0.31 (0.09) 0.001
Pre RV function (echo) −1.45 (0.80) 0.07 3.54 (1.59) 0.03
Pre RV z-score 5.36 (2.13) 0.01 −1.54 (0.56) 0.006
Prior stenting 10.41 (3.64) 0.004 6.70 (2.55) 0.009
EST (SE) indicates parameter estimate from the regression model (standard error); LV, left ventricle; LVEDVi, LV end-diastolic volume index; LVEF, left ventricular ejection fraction; LVESVi, LV end-systolic volume index; LVSVi, LV stroke volume index; PA, pulmonary artery; PPVI, percutaneous pulmonary valve implantation; RV, right ventricle; RVED, RV end-diastolic; RVEDVi, RVED volume index; RVEF, RV ejection fraction; RVESVi, RV end-systolic volume index; and VO
2, oxygen consumption.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

10 Borik et al Pulmonary Valve Implants: Time-Related Outcomes
2. Vezmar M, Chaturvedi R, Lee KJ, Almeida C, Manlhiot C, McCrindle BW, Horlick EM, Benson LN. Percutaneous pulmonary valve implanta-tion in the young 2-year follow-up. JACC Cardiovasc Interv. 2010;3:439–448. doi: 10.1016/j.jcin.2010.02.003.
3. Coats L, Khambadkone S, Derrick G, Hughes M, Jones R, Mist B, Pellerin D, Marek J, Deanfield JE, Bonhoeffer P, Taylor AM. Physiological con-sequences of percutaneous pulmonary valve implantation: the different behaviour of volume- and pressure-overloaded ventricles. Eur Heart J. 2007;28:1886–1893. doi: 10.1093/eurheartj/ehm181.
4. Coats L, Khambadkone S, Derrick G, Sridharan S, Schievano S, Mist B, Jones R, Deanfield JE, Pellerin D, Bonhoeffer P, Taylor AM. Physiological and clinical consequences of relief of right ventricular outflow tract obstruction late after repair of congenital heart defects. Circulation. 2006;113:2037–2044. doi: 10.1161/CIRCULATIONAHA.105.591438.
5. Lurz P, Coats L, Khambadkone S, Nordmeyer J, Boudjemline Y, Schievano S, Muthurangu V, Lee TY, Parenzan G, Derrick G, Cullen S, Walker F, Tsang V, Deanfield J, Taylor AM, Bonhoeffer P. Percutaneous pulmonary valve implantation: impact of evolving technology and learning curve on clinical outcome. Circulation. 2008;117:1964–1972. doi: 10.1161/CIRCULATIONAHA.107.735779.
6. Lurz P, Nordmeyer J, Giardini A, Khambadkone S, Muthurangu V, Schievano S, Thambo JB, Walker F, Cullen S, Derrick G, Taylor AM, Bonhoeffer P. Early versus late functional outcome after successful percutaneous pulmonary valve implantation: are the acute effects of altered right ventricular loading all we can expect? J Am Coll Cardiol. 2011;57:724–731. doi: 10.1016/j.jacc.2010.07.056.
7. Frigiola A, Tsang V, Bull C, Coats L, Khambadkone S, Derrick G, Mist B, Walker F, van Doorn C, Bonhoeffer P, Taylor AM. Biventricular re-sponse after pulmonary valve replacement for right ventricular outflow tract dysfunction: is age a predictor of outcome? Circulation. 2008;118(14 suppl):S182–S190. doi: 10.1161/CIRCULATIONAHA.107.756825.
8. Therrien J, Siu SC, McLaughlin PR, Liu PP, Williams WG, Webb GD. Pulmonary valve replacement in adults late after repair of tetralogy of fal-lot: are we operating too late? J Am Coll Cardiol. 2000;36:1670–1675.
9. Lee C, Kim YM, Lee CH, Kwak JG, Park CS, Song JY, Shim WS, Choi EY, Lee SY, Baek JS. Outcomes of pulmonary valve replacement in 170 patients with chronic pulmonary regurgitation after relief of right ven-tricular outflow tract obstruction: implications for optimal timing of pul-monary valve replacement. J Am Coll Cardiol. 2012;60:1005–1014. doi: 10.1016/j.jacc.2012.03.077.
10. Lopez L, Colan SD, Frommelt PC, Ensing GJ, Kendall K, Younoszai AK, Lai WW, Geva T. Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr. 2010;23:465–495, quiz 576. doi: 10.1016/j.echo.2010.03.019.
11. Chubb H, Simpson JM. The use of Z-scores in paediatric cardiology. Ann Pediatr Cardiol. 2012;5:179–184. doi: 10.4103/0974-2069.99622.
12. Mangion JR. Right ventricular imaging by two-dimensional and three-di-mensional echocardiography. Curr Opin Cardiol. 2010;25:423–429. doi: 10.1097/HCO.0b013e32833b55c4.
13. Mezzani A, Agostoni P, Cohen-Solal A, Corrà U, Jegier A, Kouidi E, Mazic S, Meurin P, Piepoli M, Simon A, Laethem CV, Vanhees L. Standards for the use of cardiopulmonary exercise testing for the func-tional evaluation of cardiac patients: a report from the Exercise Physiology
Section of the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil. 2009;16:249–267. doi: 10.1097/HJR.0b013e32832914c8.
14. McElhinney DB, Cheatham JP, Jones TK, Lock JE, Vincent JA, Zahn EM, Hellenbrand WE. Stent fracture, valve dysfunction, and right ven-tricular outflow tract reintervention after transcatheter pulmonary valve implantation: patient-related and procedural risk factors in the US Melody Valve Trial. Circ Cardiovasc Interv. 2011;4:602–614. doi: 10.1161/CIRCINTERVENTIONS.111.965616.
15. Asoh K, Walsh M, Hickey E, Nagiub M, Chaturvedi R, Lee KJ, Benson LN. Percutaneous pulmonary valve implantation within bioprosthet-ic valves. Eur Heart J. 2010;31:1404–1409. doi: 10.1093/eurheartj/ehq056.
16. McElhinney DB, Hellenbrand WE, Zahn EM, Jones TK, Cheatham JP, Lock JE, Vincent JA. Short- and medium-term outcomes after trans-catheter pulmonary valve placement in the expanded multicenter US melody valve trial. Circulation. 2010;122:507–516. doi: 10.1161/CIRCULATIONAHA.109.921692.
17. Moiduddin N, Asoh K, Slorach C, Benson LN, Friedberg MK. Effect of transcatheter pulmonary valve implantation on short-term right ventricular function as determined by two-dimensional speckle tracking strain and strain rate imaging. Am J Cardiol. 2009;104:862–867. doi: 10.1016/j.amjcard.2009.05.018.
18. Zahn EM, Hellenbrand WE, Lock JE, McElhinney DB. Implantation of the melody transcatheter pulmonary valve in patients with a dysfunc-tional right ventricular outflow tract conduit early results from the u.s. Clinical trial. J Am Coll Cardiol. 2009;54:1722–1729. doi: 10.1016/j.jacc.2009.06.034.
19. Eicken A, Ewert P, Hager A, Peters B, Fratz S, Kuehne T, Busch R, Hess J, Berger F. Percutaneous pulmonary valve implantation: two-centre experi-ence with more than 100 patients. Eur Heart J. 2011;32:1260–1265. doi: 10.1093/eurheartj/ehq520.
20. McElhinney DB, Benson LN, Eicken A, Kreutzer J, Padera RF, Zahn EM. Infective endocarditis after transcatheter pulmonary valve replacement us-ing the Melody valve: combined results of 3 prospective North American and European studies. Circ Cardiovasc Interv. 2013;6:292–300. doi: 10.1161/CIRCINTERVENTIONS.112.000087.
21. Lurz P, Muthurangu V, Schuler PK, Giardini A, Schievano S, Nordmeyer J, Khambadkone S, Cappeli C, Derrick G, Bonhoeffer P, Taylor AM. Impact of reduction in right ventricular pressure and/or volume over-load by percutaneous pulmonary valve implantation on biventricular re-sponse to exercise: an exercise stress real-time CMR study. Eur Heart J. 2012;33:2434–2441. doi: 10.1093/eurheartj/ehs200.
22. Lurz P, Giardini A, Taylor AM, Nordmeyer J, Muthurangu V, Odendaal D, Mist B, Khambadkone S, Schievano S, Bonhoeffer P, Derrick G. Effect of altering pathologic right ventricular loading conditions by percutane-ous pulmonary valve implantation on exercise capacity. Am J Cardiol. 2010;105:721–726. doi: 10.1016/j.amjcard.2009.10.054.
23. Geva T, Gauvreau K, Powell AJ, Cecchin F, Rhodes J, Geva J, del Nido P. Randomized trial of pulmonary valve replacement with and without right ventricular remodeling surgery. Circulation. 2010;122(11 suppl):S201–S208. doi: 10.1161/CIRCULATIONAHA.110.951178.
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Mark K. Friedberg, Brian W. McCrindle, Cedric Manlhiot and Lee BensonSharon Borik, Andrew Crean, Eric Horlick, Mark Osten, Kyong-Jin Lee, Rajiv Chaturvedi,
Outcomes?Percutaneous Pulmonary Valve Implantation: 5 Years of Follow-Up: Does Age Influence
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.114.0017452015;8:Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/8/2/e001745World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 16, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from