CONGENITAL HEART DISEASES
221
PRESENTED BY DONA MATHEW MSC(N) GOVT.COLLEGE OF NURSING KOTTAYAM 1
-
Upload
dona-mathew -
Category
Health & Medicine
-
view
364 -
download
3
Transcript of CONGENITAL HEART DISEASES

PRESENTED BY DONA MATHEW
MSC(N)GOVT.COLLEGE OF NURSING
KOTTAYAM1

Congenital heart defect (CHD)
Anatomic malformation of the heart or greatvessels which occurs during intrauterinedevelopment, irrespective of the age atpresentation.
Congenital heart disease occurs inapproximately 0.8% of live births.
The incidence is higher in stillborns (3-4%),spontaneous abortuses (10-25%), andpremature infants (about 2% excludingpatent ductusarteriosus [PDA]
2
Causes of congenital heart defects
Environmental factors
Viral Infections
rubella during the first three months of pregnancy
Medication
lithium (used to manage bipolor disorder), Accutane(acne medication), some anti-seizure medications
Alcohol
with fetal alcohol syndrome (FAS)
Smoking
Cocaine
Maternal chronic illnesses –diabetes, phenylketonuria(PKU) and a deficiency in the B vitamin folic acid.
3

Genetic factors
Heredity –occur in siblings or offspring ofindividuals with heart defects than thosewithout.
Mutations –can affect the formation of theheart and lead to congenital heartmalformations
Linked with other birth defects – More thanone-third of children born with Downsyndrome have heart defects. About 25% ofgirls with Turner syndrome have heart defects
4

Classification of congenital heart disease
• Acyanotic
• Cyanotic
5

ACYANOTIC
INCREASED PULMONARY BLOOD FLOW
ASD,VSD,PDA,
ATRIOVENTRICULAR
CANAL MALFORMATOION
OBSTRUCTION TO BLOOD
FLOW FROM VENTRICLES
COARCTATION OF AORTA,AORTIC
STENOSIS, PULMONARY
STENOSIS
6

CYANOTIC
DECRESED
PULMONARY BLODD FLOW
TETRALOGY OF FALLOT. TRICUSPID ATRESIA
MIXED BLOOD FLOW
TRANS POSITION OF GREAT
ARTERIES,TOTAL ANOMOLOUS
PULMONARY VENOUS RETURN,TRUNCUS
ARTERIOSUS,
HYPOLPLASTIC LEFT HEART SYNDROME
7

RELATIVE FREQUENCY OF MAJOR CONGENITAL HEART LESIONS
LESION % OF ALL LESIONS
Ventricular septal defect 35-30
Atrial septal defect (secundum) 6-8
Patent ductus arteriosus 6-8
Coarctation of aorta 5-7
Tetralogy of Fallot 5-7
Pulmonary valve stenosis 5-7
Aortic valve stenosis 4-7
d-Transposition of great arteries 3-5
Hypoplastic left ventricle 1-3
Hypoplastic right ventricle 1-3
Truncus arteriosus 1-2
Total anomalous pulmonary venous return
1-2
Tricuspid atresia 1-2
Single ventricle 1-2
Double-outlet right ventricle 1-2
Others 5-10 8

ACYANOTIC CONGENITAL HEART DISEASE
9

DEFECTS WITH INCREASED PULMONARY BLOOD FLOW
10

Atrial Septal Defect (ASD)
An opening in the atrial septum
An atrial septal defect allows oxygenated (red) blood to pass from the left atrium, through the opening in the septum, and then mix with unoxygenated (blue) blood in the right atrium
During fetal heart devt. The partitioning process does not occur completely, leaving an opening in the atrial septum
Occur in 4-10% of all infants w/ CHD
Effects: when blood passes through the ASD from the left atrium to the right atrium a larger volume of blood than normal must be handled by the right side of the heart extra blood then passes through the pulmonary artery into the lungs pulmonary hypertension and pulmonary congestion
11

If the ASD is left uncorrected-->pulmonaryhypertension progresses -->pressure in the rightside of the heart will become greater than theleft side of the heart.
This reversal of the pressure gradient across theASD causes the shunt to reverse --> a right-to-left shunt will exist. This phenomenon is knownas Eisenmenger's syndrome
Once right-to-left shunting occurs, a portion ofthe oxygen-poor blood will get shunted to theleft side of the heart and ejected to theperipheral vascular system.
This will cause signs of cyanosis12
Atrial Septal Defect (ASD)
13

14

Types of atrial septaldefects
Ostium secundum atrial septal defect most common type of atrial septal defect comprises 6–10% of all congenital heart
diseases. Opening near the center of the septum The secundum atrial septal defect usually arises
from an enlarged foramen ovale, inadequategrowth of the septum secundum, or excessiveabsorption of the septum primum.
If the ostium secundum ASD is accompanied byan acquired mitral valve stenosis, that is calledLutembacher's syndrome.
15

Patent foramen ovale
A small channel that has some hemodynamic consequence
It is a remnant of the fetal foramen ovale.
On echocardiography, there may not be any shunting of blood noted except when the patient coughs.
16

Ostium primum atrial septal defect
Opening at the lower end of the septum
A defect in the ostium primum is occasionallyclassified as an atrial septal defect but it ismore commonly classified an atrioventricularseptal defect. Ostium primum defects are lesscommon than ostium secundum defects
17

Sinus venosus atrial septal defect
Opening near the junction of superior venacava and right atrium, may be associatedwith partial anomalous pulmonary venousconnection
Common or single atrium
It is a failure of development of theembryologic components that contribute tothe atrial septal complex. It is frequentlyassociated with heterotaxy syndrome.
18

19

CLINICAL MANIFESTATIONS
History.
Infants and children with ASDs are usuallyasymptomatic
Physical Examination
A relatively slender body build is typical.
A widely split and fixed S2 and a systolic ejectionmurmur are characteristic findings of ASD in olderinfants and children. .
Classic auscultatory findings of ASD are notpresent unless the shunt is reasonably large
20
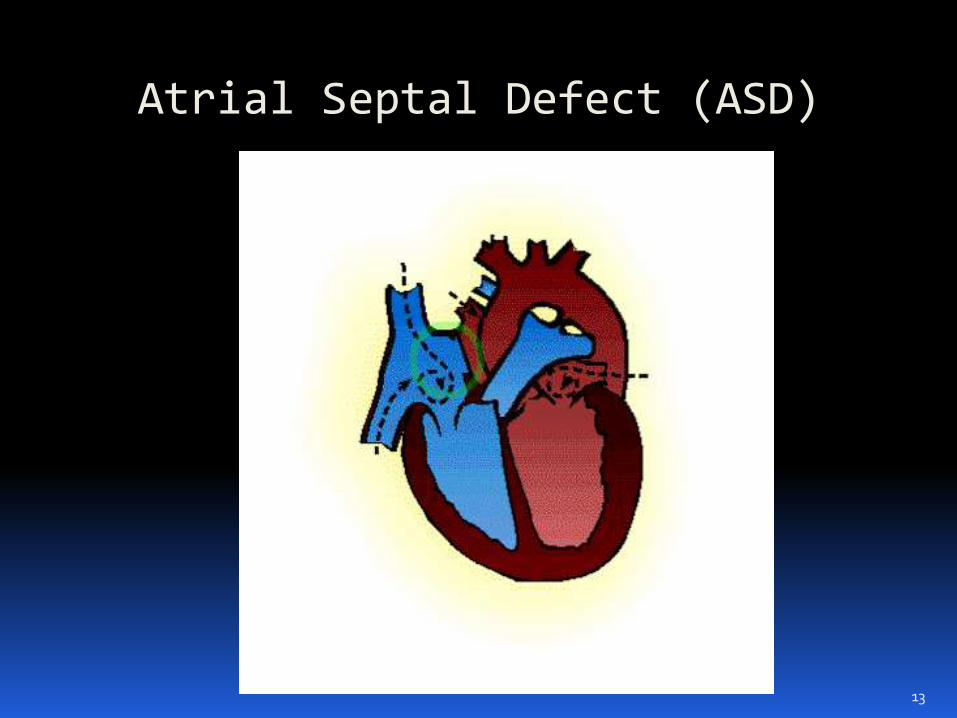
Electrocardiography
Right axis deviation of +90 to +180 degreesand mild right ventricular hypertrophy (RVH)or right bundle branch block (RBBB) with anrsR' pattern in V1 are typical findings
21

X-ray Studies
Cardiomegaly with enlargement of the RA andright ventricle (RV) may be present.
A prominent pulmonary artery (PA) segment andincreased pulmonary vascular markings are seenwhen the shunt is significant
22

Echocardiography
A two-dimensional echo study is diagnostic.
shows the position as well as the size of thedefect,
In secundum ASD, a dropout can be seen in themidatrial septum.
The primum type shows a defect in the lower atrialseptum
Indirect signs of a significant left-to-right atrialshunt include RV enlargement and RAenlargement, as well as dilated PA
M-mode echo may show increased RV dimensionand paradoxical motion of the interventricularseptum, which are signs of RV volume overload.
23

ASD on 2D echo
24

ASD flow by colour Doppler
25

Echocardiogram in apical four chamber view of primum
ASD
26

CONTRAST ECHO
If agitated saline is injected into aperipheral vein during echocardiography,small air bubbles can be seen onechocardiographic imaging.
It may be possible to see bubbles travelacross an ASD either at rest or during acough. (Bubbles will only flow from rightatrium to left atrium if the RA pressure isgreater than LA).
27

28

NATURAL HISTORY OF ASD spontaneous closure of the secundum defect
occurs in about 40% of patients in the first 4years of life
Most children with an ASD remain active andasymptomatic.
Rarely, congestive heart failure (CHF) candevelop in infancy.
If a large defect is untreated, CHF andpulmonary hypertension develop in adults whoare in their 20s and 30s
With or without surgery, atrial arrhythmias(flutter or fibrillation) may occur in adults.
29

MANAGEMENT
Medical
Exercise restriction is unnecessary.
Prophylaxis for infective endocarditis indicatedin patients with primum ASD.
In infants with CHF, medical management isrecommended because of its high success rateand the possibility of spontaneous closure ofthe defect.
30

Nonsurgical Closure of ASD
catheter-delivered closure device has becomea preferred method
Devices available for clinical use haveincluded the Sideris buttoned device, theAngel Wings device, the CardioSEAL device,and the Amplatzer ASD Occlusion Device.
The amplatzer septal occluder has thewidespread use.
31

Use of the closure device may be indicated In
To close a secundum ASD, measuring 5 mmor more in diameter (but less than 32 mm),
A significant left-to-right shunt with clinicalevidence of right ventricular volume overload
There must be enough rim (4 mm) of septaltissue around the defect for appropriateplacement of the device.
The timing of the device- because of thepossibility of spontaneous closure, it is notused in infancy unless the patient issymptomatic with heart failure.
32

33

Advantages of nonsurgical closure
Complete avoidance of cardiopulmonarybypass
Avoidance of pain and residual thoracotomyscars
A less than 24-hour hospital stay
Rapid recovery
All these devices are associated with a higherrate of small residual leak than is operativeclosure.
34

Post-device closure follow-up
The patients are administered aspirin 81mg/day for 6 months.
Postprocedure echo studies
35

Surgical ClosureIndications and Timing
A left-to-right shunt with a pulmonary-to-systemic blood flow ratio ( p/ s) of ≥1.5:1 .
Surgery is usually delayed until 2 to 4 years ofage because the possibility of spontaneousclosure.
Surgery is performed during infancy-if CHFdoes not respond to medical managementinfancy,.
36

Infants with associated bronchopulmonarydysplasia and the device closure is notconsidered appropriate, surgery is performedduring infancy.
High pulmonary vascular resistance may be acontraindication for surgery
37

Procedure.
For secundum ASD, the defect is traditionallyrepairedwith a simple suture or a pericardialor Teflon patch through a midsternal incisionunder cardiopulmonary bypass by either
For sinus venosus defect without associatedanomalous pulmonary venous return, thedefect is closed using an autologouspericardial patch.
38

When it is associated with a pulmonaryvenous anomaly, a tunnel is created betweenthe anomalous pulmonary vein and the ASDby using a Teflon or pericardial patch
For coronary sinus ASD, the ostium of thecoronary sinus is closed with an autologouspericardium
39

40

Mortality. Fewer than 0.5% of patients die
Complications. Cerebrovascular accident postoperative arrhythmias
Postoperative Follow-up 1. Cardiomegaly on x-ray film and enlarged RV
dimension on echo as well as the wide splitting ofthe S2 may persist for 1 or 2 years postoperatively.
The ECG typically demonstrates RBBB (or RVconduction disturbance).
2. Atrial or nodal arrhythmias occur in 7% to 20%of postoperative patients.
3. Rarely, patients with residual shunt may beadministered aspirin 81 mg to prevent paradoxicalembolization 41

Ventricular Septal Defect (VSD)
an opening in the ventricular septum
allows oxygenated blood to pass from the leftventricle, through the opening in the septum, andthen mix with unoxygenated blood in the rightventricle.
VSDs are the most commonly occurring type ofcongenital heart defect, occurring in 14-17 % ofbabies born each year.
occur when the partitioning process does not occurcompletely, leaving an opening in the ventricularseptum.
42

43

EFFECTS:
When blood passes through the VSD from theleft ventricle to the right ventricle a largervolume of blood than normal must be handledby the right side of the heart extra blood thenpasses through the pulmonary artery into thelungs pulmonary hypertension and pulmonarycongestion pulmonary arteries becomethickened and obstructed due to increasedpressure
.
Ventricular Septal Defect (VSD)
44

If VSD is not repaired, and lung disease begins to occur pressure in the right side of the heart will eventually exceed pressure in the left R to L shunt cyanosis
Due to high pressure --- tissue damage may eventually occur in the right ventricle bacteria in the bloodstream can easily infect this injured area bacterial endocarditis
45

CLINICAL MANIFESTATIONS History
With a small VSD, the patient is asymptomaticwith normal growth and development.
With a moderate to large VSD, delayedgrowth and development, decreased exercisetolerance, repeated pulmonary infections, andCHF are relatively common during infancy.
With long-standing pulmonary hypertension,a history of cyanosis and a decreased level ofactivity may be present.
46

Physical Examination Infants with small VSDs are well developed and
acyanotic. Before 2 or 3 months of age, infants with large
VSDs may have poor weight gain or show signsof CHF.
Cyanosis and clubbing may be present inpatients with Eisenmenger's syndrome
A systolic thrill may be present at the lower leftsternal border.
Precordial bulge and hyperactivity are presentwith a large-shunt VSD.
The S2 is loud and single in patients withpulmonary hypertension or pulmonary vascularobstructive disease.
47

A grade 2 systolic murmur is audible at thelower left sternal border .It may beholosystolic or early systolic.
An apical diastolic rumble is present with amoderate to large shunt because of increasedflow through the mitral valve during diastole.
48

Electrocardiography
With a small VSD, the ECG is normal.
With a moderate VSD, left ventricularhypertrophy (LVH) and occasional left atrialhypertrophy (LAH) may be seen.
With a large defect, the ECG showsbiventricular hypertrophy (BVH) with orwithout LAH
If pulmonary vascular obstructive diseasedevelops, the ECG shows RVH only
49

VSD (6 month old child)
50

X-ray Studies Cardiomegaly of varying degrees is present and
involves the LA, left ventricle (LV), and sometimes RV.
Pulmonary vascular markings increase.
The degree of cardiomegaly and the increase inpulmonary vascular markings directly relate to the
magnitude of the left-to-right shunt.
51

Echocardiography
52

NATURAL HISTORY Spontaneous closure occurs in 30% to 40% of
patients with membranous VSDs and muscularVSDs during the first 6 months of life.
CHF develops in infants with large VSDs butusually not until 6 to 8 weeks of age.
Pulmonary vascular obstructive disease maybegin to develop as early as 6 to 12 months ofage in patients with large VSDs, but the resultingright-to-left shunt usually does not develop untilthe teenage years.
Infective endocarditis rarely occurs.
53

Medical Management
Treatment of CHF if it develops, (digoxinand diuretics for 2 to 4 months )
Addition of spironolactone may be helpfulto minimize potassium loss.
Concomitant use of an afterload-reducingagent, such as captopril,
Frequent feedings of high-calorieformulas, by either nasogastric tube ororal feeding, may help.
54
Anemia, if present, should be corrected by oraliron therapy..
No exercise restriction is required in the absenceof pulmonary hypertension.
Maintenance of good dental hygiene andantibiotic prophylaxis against infectiveendocarditis are important
Nonsurgical closure of selected muscular VSDs ispossible using the “umbrella” device, but this isstill in the experimental stage.
55

Surgical-Indications and Timing
Small infants who have large VSDs and developCHF and growth retardation - If growth failurecannot be improved by medical therapy, the VSDshould be operated on within the first 6 monthsof life.
if the PA pressure is greater than 50% ofsystemic pressure, surgical closure should bedone by the end of the first year.
After 1 year of age, a significant left-to-rightshunt with p/ s of at least 2:1 indicates thatsurgical closure is needed, regardless of PApressure.
56

Surgical treatment
Palliative – pulmonary artery banding
Placing a band around the pulmonary arteryto decrease the pulmonary blood flow
It increases the resistance to blood flowthrough the pulmonary artery. Pressureincreases in the right ventricle and preventsexcess shunting from left to right
57

Complete repair-small defects are repairedwith a purse-string approach.
Large defects usually require a KnittedDacron patch sewn over the opening
Both procedures require CPB
The repair is generally approached throughthe right atrium and tricuspid valve
Post operative complications include residualVSD and conduction disturbances
58

Mortality.
Surgical mortality is less than 1%. Mortality ishigher for small infants younger than 2months of age, infants with associateddefects, or infants with multiple VSDs
59

Postoperative Follow-up Activity should not be restricted unless complications
have resulted from surgery.
The ECG shows RBBB in 50% to 90% of patients who hadVSD repair through right ventriculotomy and up to 40%of the patients who had repair through a right atrialapproach.
Bacterial endocarditis prophylaxis may be discontinued6 months after surgery. If a residual shunt is present,endocarditis prophylaxis should be continued indefinitelywhen the indications arise.
A patient with a postoperative history of transient heartblock with or without pacemaker therapy requires long-term follow-up.
60

Patent Ductus Arteriosus (PDA)
characterized by a connection between the aorta and the pulmonary artery
All babies are born with a ductus arteriosus.
As the baby takes the first breath, the blood vessels in the lungs open up, and blood begins to flow the ductus arteriosus is not needed to bypass the lungs
Most babies have a closed ductus arteriosus by 72 hours after birth.
In some babies, however, the ductus arteriosus remains open (patent) .
The opening between the aorta and the pulmonary artery allows oxygenated blood to pass back through the blood vessels in the lungs.
PDA occurs in 6-11 % of all children with CHD61

62

In many children, there is no known reason for the ductusarteriosus remaining open. However, PDA is seen more often in the following:
premature infants
infants born to a mother who had rubella during the first trimester of pregnancy
EFFECTS:
PDA oxygenated blood passes from the aorta to the pulmonary artery & mixes w/ the unoxygenated blood w/c goes to the lungs blood volume to the lungs pulmonary hypertension & congestion
Further, because blood is pumped at high pressure through the PDA, the lining of the pulmonary artery will become irritated and inflamed. Bacteria in the bloodstream can easily infect this injured area bacterial endocarditis.
Patent Ductus Arteriosus (PDA)
63

CLINICAL MANIFESTATIONS
History
Patients are usually asymptomatic when theductus is small.
A large-shunt PDA may cause a lowerrespiratory tract infection, atelectasis, andCHF (accompanied by tachypnea and poorweight gain).
Exertional dyspnea may be present inchildren with a large-shunt PDA
64

Physical Examination
Tachycardia and tachypnea may be present ininfants with CHF.
Bounding peripheral pulses with wide pulsepressure are characteristic findings.
A systolic thrill may be present at the upper leftsternal border.
A grade 1 to 4/6 continuous (“machinery”)murmur is best audible at the leftinfraclavicular area or upper left sternalborder..
If pulmonary vascular obstructive diseasedevelops, a right-to-left ductal shunt results incyanosis only in the lower half of the body
65

Electrocardiography. The ECG findings in PDA are similar to those in
VSD. A normal ECG or LVH is seen with small to
moderate PDA. BVH is seen with large PDA. If pulmonary vascular obstructive disease
develops, RVH is present.X-ray Studies.
X-ray findings are also similar to those of VSD. Chest x-ray films may be normal with a small-
shunt PDA. Cardiomegaly of varying degrees occurs in
moderate- to large-shunt PDA with enlargementof the LA, LV, and ascending aorta. Pulmonaryvascular markings are increased.
66
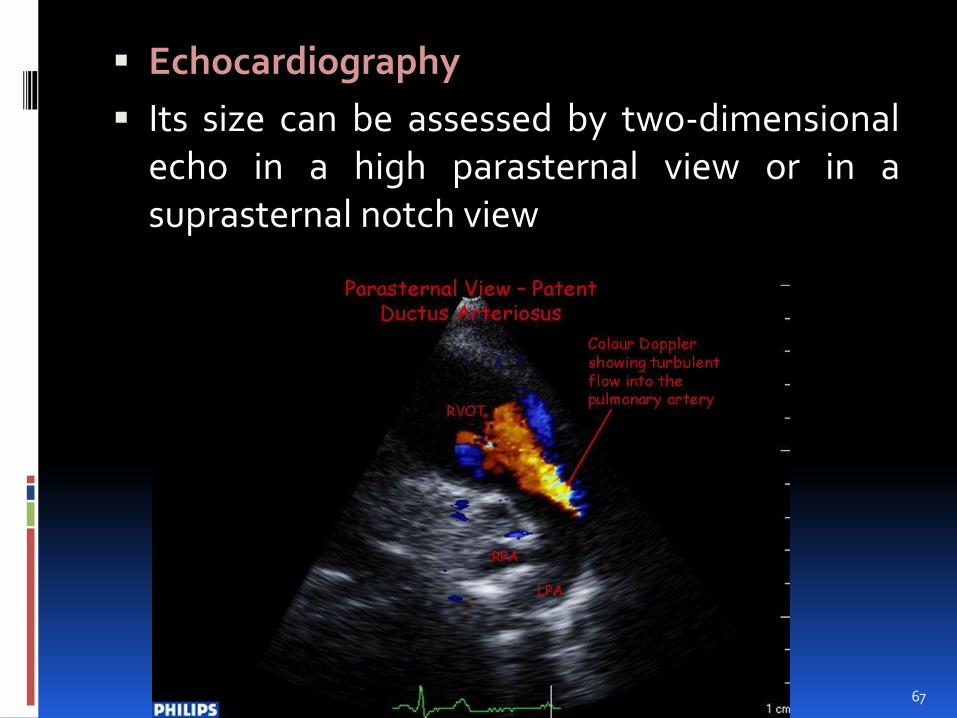
Echocardiography
Its size can be assessed by two-dimensionalecho in a high parasternal view or in asuprasternal notch view
67
NATURAL HISTORY
Spontaneous closure of a PDA does notusually occur in full-term infants andchildren. This is because the PDA in terminfants results from a structural abnormalityof the ductal smooth muscle
CHF or recurrent pneumonia or bothdevelop if the shunt is large.
Pulmonary vascular obstructive disease maydevelop if a large PDA with pulmonaryhypertension is left untreated.
Infective endocarditis may occur. Although rare, an aneurysm of PDA may
develop and possibly rupture in adult life.
68

MANAGEMENT- IN TERM NEONATES
Medical
Indomethacin is ineffective in term infantswith PDA and should not be used.
Standard anticongestive measures withdigoxin and diuretics are indicated when CHFdevelops.
No exercise restriction is needed in theabsence of pulmonary hypertension.
Prophylaxis for subacute bacterialendocarditis (SBE) is indicated whenindications arise.
69

Nonsurgical Closure. Small ductus less than 4 mm in diameter are
closed by coils
Larger ones by an amplatzer PDA device.
70

71

72
SURGICAL CLOSURE Surgical closure is reserved for patients in whom
a nonsurgical closure technique is not consideredapplicable
Procedure
Ligation and division through left posterolateralthoracotomy without cardiopulmonary bypass isthe standard procedure.
The technique of video-assisted thoracoscopicclip ligation has become the standard of care forsurgical management of a ductus with adequatelength
73

74

Patent Ductus Arteriosus in Preterm Neonates
Clinical evidence of PDA appears in 45% ofinfants with birth weight less than 1750 g andin about 80% of infants with birth weight lessthan 1200 g.
Significant PDA with CHF occurs in 15% ofpremature infants with birth weight less than1750 g and in 40% to 50% of those with birthweight less than 1500 g
75

MANAGEMENT- IN PRE TERM NEONATES
Medical
Fluid restriction to 120 mL/kg per day and adiuretic (e.g., furosemide, 1 mg/kg, two to threetimes a day) may be tried for 24 to 48 hours
Pharmacologic closure of the PDA can heachieved with indomethacin (a prostaglandinsynthetase inhibitor).
The dose is given intravenously every 12 hoursfor a total of three doses. For infants less than 48hours old, 0.2 mg/kg is followed by 0.1 mg/kg2 times .
76

For those 2 to 7 days old, 0.2 mg/kg times 3, andfor infants older than 7 days, 0.2 mg/kg followedby 0.25 mg/kg times 2
Contraindications to the use of indomethacin High blood urea nitrogen (>25 mg/dl) or creatinine
(>1.8 mg/dl) levels Low platelet count (<80,000/mm3) Bleeding tendency (including intracranial hemorrhage) Necrotizing enterocolitis, and hyperbilirubinemia.
A multicenter prospective study from Europeshowed that intravenous ibuprofen (10 mg/kg,followed at 24-hour intervals by two doses of 5mg/kg) starting on the third day of life was aseffective as indomethacin in closing the ductus inpreterm newborns..
77

ATRIOVENTRICULAR CANAL DEFECT
Also known as endocardial cushion defects
They account for about 5 percent of all congenital heart disease, and are most common in infants with down syndrome.
(About 15 percent to 20 percent of newborns with down syndrome have atrioventricularseptal defects).
78

79

Complete atrioventricularcanal (CAVC)
Complete atrioventricular canal (CAVC) is asevere defect in which there is a large hole inthe the septum that separates the left andright sides of the heart.
The hole is in the center of the heart, wherethe upper chambers and the lower chambersmeet.
In a child with a complete atrioventricularcanal defect, there is one large valve, and itmay not close correctly.
80

Partial atrioventricularcanal defects The hole does not extend between the lower
chambers of the heart and the valves arebetter formed.
Partial atrioventricular canal is also calledatrioventricular septal defect, or AVSD.
81

82

PATHOPHYSIOLOGY defect in the septum
blood to travel from the left side of the heart to the right side of the heart, or the other way around.
The oxygenated and unoxygenated blood being mixed up
The extra blood being pumped into the lung arteries makes the heart and lungs work harder and the lungs can become congested.
83

CLINICAL MANIFESTATION
Dyspnea
MILD CYANOSIS
A newborn baby will show signs of heart failure such as edema, fatigue, wheezing, sweating and irregular heartbeat
CHARACTERSTIC MURMUR
84

85

MANAGEMENT
Palliative-pulmonary artery banding
Complete repair –
Patch closure of septal defect
Reconstruction of AV valve tissue
86
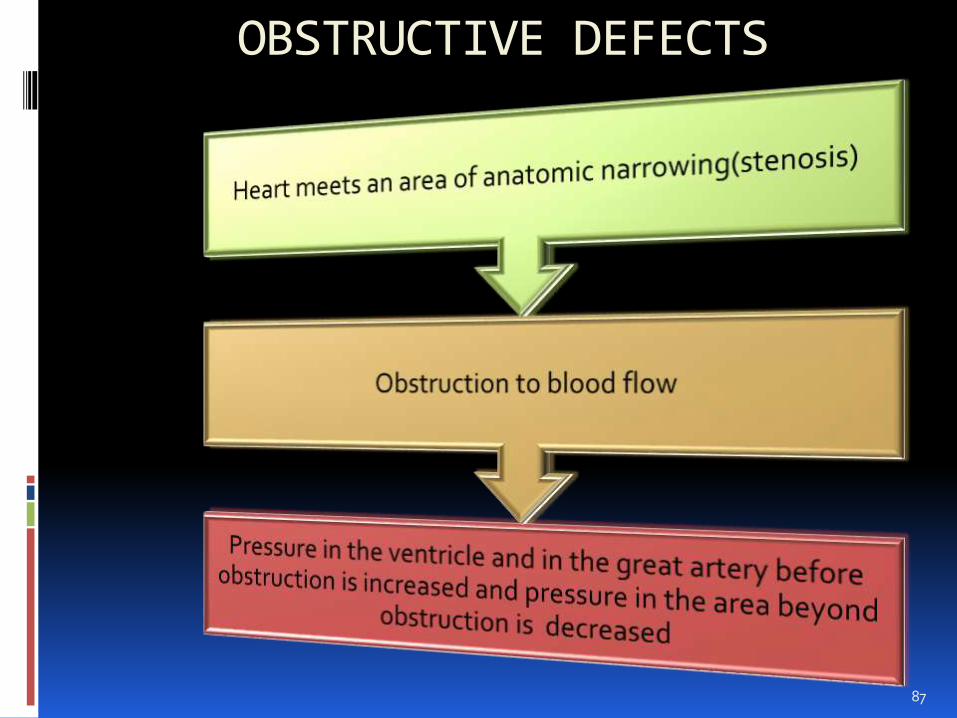
OBSTRUCTIVE DEFECTS
87

Coarctation of the Aorta
Narrowing of the aorta
can occur anywhere, but is most likely to happen in the segment just after the aortic arch.
This narrowing restricts the amount of blood to the lower part of the body
occurs in about 8-11 % of all children with CHD
88

EFFECTS:
The left ventricle has to work harder to try to move blood through the narrowing in the aorta left-sided heart failure
BP is higher above the narrowing, and lower below the narrowing.
Older children may have headaches from too much pressure in the vessels in the head, or cramps in the legs or abdomen from too little blood flow in that region.
The walls of the arteries may become weakened by high pressure spontaneous tears cause a stroke or uncontrollable bleeding.
risk for bacterial endocarditis.
89

90

91

SYMPTOMATIC INFANTS History.
Poor feeding, dyspnea, and poor weight gainor signs of acute circulatory shock maydevelop in the first 6 weeks of life.
Physical Examination
Infants with COA are pale and experiencevarying degrees of respiratory distress.
Oliguria or anuria, general circulatory shock,and severe acidemia are common.).
Peripheral pulses may be weak and threadyas a result of CHF.
92
A blood pressure differential may becomeapparent only after improvement of cardiacfunction with administration of rapidly actinginotropic agents.
The S2 is single and loud; a loud S3 gallop isusually present.
No heart murmur is present in 50% of sickinfants.
A nonspecific ejection systolic murmur isaudible over the precordium.
93

Electrocardiography.
A normal or rightward QRS axis and RVH orright bundle branch block (RBBB) are present
X-ray Studies.
Marked cardiomegaly and pulmonary edemaor pulmonary venous congestion are usuallypresent
94

The blue arrow to the actual coarctationand the green arrow to the post-stenotic dilation of the
descending aorta.
95

Echocardiography
Two-dimensional echo and color flowDoppler studies usually show the site andextent of the coarctation.
In the suprasternal notch view, a thin wedge-shaped “posterior shelf” is imaged in theposterolateral aspect of the upperdescending aorta
96

97

Natural History
About 20% to 30% of all patients with COA develop CHF by 3 months of age.
If it is undetected or untreated, early death may result from CHF and renal shutdown in symptomatic infants
98

Management
Medical
In symptomatic neonates, PGE1 infusion shouldbe started to reopen the ductus arteriosus andestablish flow to the descending aorta and thekidneys during the first weeks of life.
Intensive anticongestive measures with short-acting inotropic agents (e.g., dopamine,dobutamine), diuretics, and oxygen should bestarted.
Balloon angioplasty can be a useful procedurefor sick infants in whom standard surgicalmanagement carries a high risk.
99

Surgical
Indications and Timing
If CHF or circulatory shock develops early in life,surgery should be performed on an urgent basis.
Procedures
Resection and end-to-end anastomosis consistsof resecting the coarctation segment andanastomosing the proximal and distal aortas .
Subclavian flap aortoplasty consists of dividingthe distal subclavian artery and inserting a flap ofthe proximal portion of this vessel between thetwo sides of the longitudinally split aortathroughout the coarctation segment.
100

With patch aortoplasty, the aorta is openedlongitudinally through the coarctationsegment and extending to the left subclavianartery, and the fibrous shelf and any existingmembrane are excised. An elliptic wovenDacron patch is inserted to expand thediameter of the lumen.
101

102

ASYMPTOMATIC INFANTS AND CHILDREN
Management
Medical
Children with mild COA should be watchedclosely for hypertension in the arm or forincreasing pressure differences between thearm and leg.
Balloon angioplasty
A balloon-expandable stainless-steel stentimplanted concurrently with balloonangioplasty
An absorbable metal stent is in theexperimental stage
103

Surgical
Indications and Timing
COA with hypertension in the upperextremities or with a large systolic pressuregradient equal to or greater than 20 mm Hgbetween the arms and the legs indicates thatelective surgical correction is necessarybetween the ages of 2 and 4 years.
Reduction of aortic diameter by 50% at thelevel of COA is also an indication for surgery.
Older children are operated on soon after thediagnosis is made.
104
In asymptomatic children, surgery isperformed by age 4 to 5; late surgery mayincrease the risk of developing early essentialhypertension.
If severe hypertension, CHF, or cardiomegalyis present, surgery is performed at an earlierage.
105

Surgical Procedures
Resection of the coarctation segment andend-to-end anastomosis
Occasionally, subclavian artery aortoplasty orcircular or patch grafts may be performed.
106

AORTIC STENOSIS
Narrowing or stricture o the aortic valve
Resistance to blood flow in the left ventricle,decreased cardiac out put, left ventricularhypertrophy and pulmonary vascularcongestion
Valvular stenosis is the most common typeand is usually caused by malformed cusps
Sub valvular stenosis is a stricture caused bya fibrous ring below the normal valve
Supra valvular stenosis occurs infrequently
107

108

Pathophysiology
A stricture in the aortic outflow tract -->resistance to ejection of blood from leftventricle -> extra work load of the leftventricle -> hypertrophy -> left ventricularfailure -> left atrial pressure increases ->increased pressure in the pulmonary veins ->pulmonary edema
109

CLINICAL MANIFESTATIONS
History
Neonates with critical or severe stenosis of theaortic valve may develop signs of hypoperfusionor respiratory distress related to pulmonaryedema within days to weeks after birth.
Most children with mild to moderate AS areasymptomatic. Occasionally, exerciseintolerance may be present.
Exertional chest pain, easy fatigability, orsyncope may occur in a child with a severedegree of obstruction
110

Physical Examination
Infants and children with AS are acyanoticand are normally developed.
blood pressure is normal in most patients, buta narrow pulse pressure is present in severeAS.
A systolic thrill may be palpable at the upperright sternal border, in the suprasternalnotch, or over the carotid arteries.
An ejection click may be heard with valvularAS.
111

Newborns with critical AS may develop signsof reduced peripheral perfusion (with weakand thready pulses, pale cool skin, and slowcapillary refill)
112

Electrocardiography.
In mild cases the ECG is normal. LVH with orwithout strain pattern may be present insevere cases
X-ray Studies
The heart size is usually normal in children,but a dilated ascending aorta or a prominentaortic knob may be seen occasionally invalvular AS, resulting from poststenoticdilatation.
Significant cardiomegaly does not developunless CHF occurs later
113

Echocardiography
114

NATURAL HISTORY
Chest pain, syncope, and even sudden death(1% to 2% of cases) may occur in childrenwith severe AS.
Heart failure occurs with severe AS during thenewborn period or later in adult life.
Mild stenosis becomes more severe with timein a significant number of patients
115
MANAGEMENT
Medical
For critically ill newborns with CHF patients are stabilized before surgery
balloon valvuloplasty
use of rapidly acting inotropic agents and diureticsto treat CHF
intravenous infusion of PGE1 to reopen theductus.
Percutaneous balloon valvuloplasty is nowregarded as the first step in the managementof symptomatic neonates
116

Surgical
Valvular AS
Closed aortic valvotomy, using calibrateddilators or balloon catheters withoutcardiopulmonary bypass, may be performedin sick infants if balloon valvuloplasty hasbeen unsuccessful or if it is not available
Aortic valve commissurotomy is usually triedif stenosis is the predominant lesion
Aortic valve replacement may be necessary ifAR is the predominant lesion
117

Subvalvular AS- Excision of the membrane isdone for discrete subvalvular AS
Supravalvular AS- a reconstructive surgery isdone using aY-shaped patch
118

Postballoon and Postoperative Follow-up
An annual follow-up examination is necessary for allpatients who have the aortic valve balloon procedure orsurgery in order to detect development of stenosis orregurgitation.
Anticoagulation is needed after a prosthetic mechanicalvalve replacement.
The International Normalized Ratio (INR) should bemaintained between 2.5 and 3.5 for the first 3 monthsand 2.0 to 3.0 beyond that time.
Low-dose aspirin (75 to 100 mg/day for adolescents) isindicated in addition to warfarin (American College ofCardiology, 2006).
After aortic valve replacement with a bioprosthesis andno risk factors, aspirin (75 to 100 mg), but not warfarin, isindicated.
Restriction from competitive, strenuous sports may benecessary for children with moderate residual AS or AR,or both 119

PULMONARY VALVE STENOSIS
Narrowing at the entrance of pulmonary artery
Resistance to blood flow causes right ventricular hypertrophy
Pulmonary atresia is the extreme form – total fusion of commissures and no blood flows to the lungs
rt . Ventricle may be hypoplastic
120

121

Pathophysiology
PS--> Resistance to blood flow-->RVH
If Rt . Ventricular failure develops-->increase in rt, atrial pressure -->re-openingof foramen ovale-->shunting of un oxy. bloodin to the Lt.atrium--> systemic cyanosis
122

Clinical manifestations
May be asymptomatic
Some had mild cyanosis
Newborn with severe narrowig- cyanotic
Characteristic murmur
Cardiomegaly on chest radiograph
Pt are at risk for infective endocarditis
123

Management
Surgical
In infants trans ventricular valvotomy (brockprocedure)
In children pulmonary valvotomy with CPB
Non surgical treatment
Balloon angioplasty
124

125
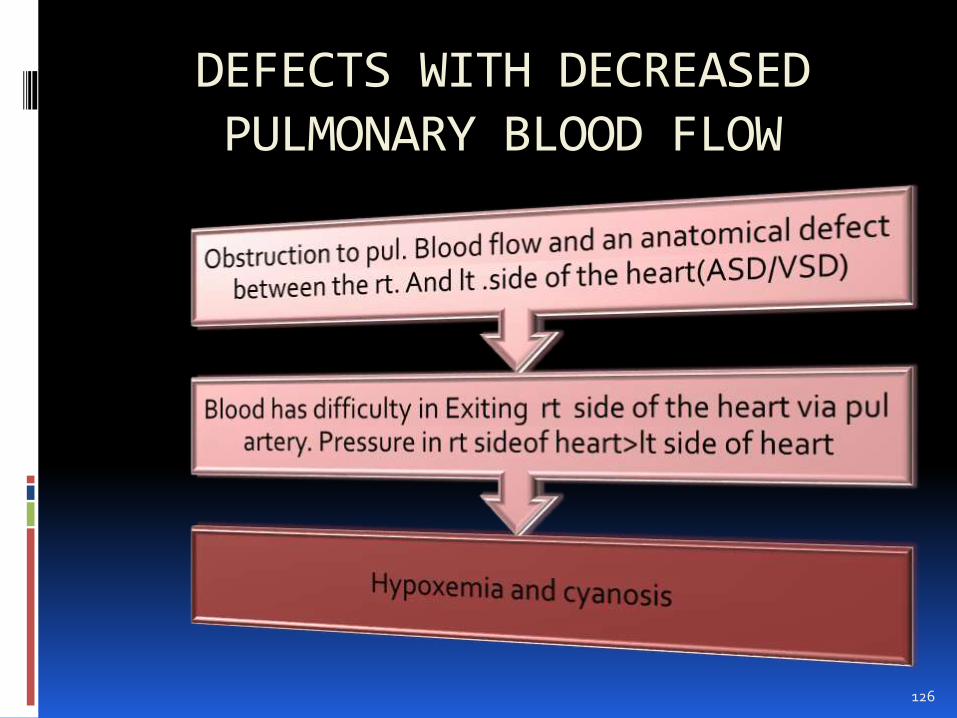
DEFECTS WITH DECREASED PULMONARY BLOOD FLOW
126

Tetralogy of Fallot (TOF)
a complex condition of several congenital defects that occurdue to abnormal devt. of the fetal heart during the first 8weeks of pregnancy. These problems include the following:
1. ventricular septal defect (VSD)
2. Pulmonary valve stenosis
3. overriding aorta - The aorta sits above both the left andright ventricles over the VSD, rather than just over the leftventricle. As a result, oxygen poor blood from the rightventricle can flow directly into the aorta instead of into thepulmonary artery to the lungs.
4. Right ventricular hypertrophy - The muscle of the rightventricle is thicker than usual because of having to workharder than normal.
127

128

EFFECTS:
If the right ventricle obstruction is severe, or if thepressure in the lungs is high a large amount ofoxygen-poor (blue) blood passes through the VSD, mixeswith the oxygen-rich (red) blood in the left ventricle, andis pumped to the body cyanosis
The more blood that goes through the VSD, the lessblood that goes through the pulmonary artery to thelungs oxygenated blood to the left side of theheart.
Soon, nearly all the blood in the left ventricle is oxygen-poor (blue). This is an emergency situation, as the bodywill not have enough oxygen to meet its needs.
Tetralogy of Fallot (TOF)
129
CLINICAL MANIFESTATIONS
History
A heart murmur is audible at birth.
Most patients are symptomatic with cyanosisat birth or shortly thereafter. Dyspnea onexertion or hypoxic spells develop later, evenin mildly cyanotic infants.
Immediately after birth, severe cyanosis isseen in patients with TOF and pulmonaryatresia.
130

Physical Examination
Varying degrees of cyanosis, tachypnea, andclubbing (in older infants and children) arepresent.
An RV tap along the left sternal border and asystolic thrill at the upper and mid-left sternalborders are commonly present (50%).
An ejection click that originates in the aortamay be audible
131

Electrocardiography
Right axis deviation (RAD) (+120 to +150 degrees) is present in cyanotic TOF.
RVH is usually present
BVH may be seen in the acyanotic form. RAH is occasionally present.
132

X- ray
Decreased pulmonary markings
Black lung fields
Boot shaped heart
133

NATURAL HISTORY
Infants with acyanotic TOF gradually becomecyanotic.
Patients who are already cyanotic become morecyanotic as a result of the worsening condition ofthe infundibular stenosis and polycythemia.
Polycythemia develops secondary to cyanosis.
Hypoxic spells may develop in infants.
Growth retardation may be present if cyanosis issevere.
134
HYPOXIC SPELL
Hypoxic spells are characterized by aparoxysm of hyperpnea (i.e., rapid and deeprespiration), irritability and prolonged crying,increasing cyanosis, and decreasing intensityof the heart murmur.
Hypoxic spells occur in infants, with a peakincidence between 2 and 4 months of age.
These spells usually occur in the morningafter crying, feeding, or defecation.
A severe spell may lead to limpness,convulsion, cerebrovascular accident, or evendeath.
135

136

137

Treatment of the hypoxic spell
The infant should be picked up and held in aknee-chest position.
Morphine sulfate, 0.2 mg/kg administeredsubcutaneously or intramuscularly, suppressesthe respiratory center and abolishes hyperpnea
Oxygen is usually administered, but it has littledemonstrable effect on arterial oxygensaturation.
Acidosis should be treated with sodiumbicarbonate (NaHCO3), 1 mEq/kg administeredintravenously. The same dose can be repeated in10 to 15 minutes..
138

P
139

MANAGEMENT OF TOF Medical educate parents to recognize the spell and know
what to do. Oral propranolol therapy, 0.5 to 1.5 mg/kg every
6 hours, is occasionally used to prevent hypoxicspells while waiting for an optimal time forcorrective surgery
Balloon dilatation of the right ventricular outflowtract and pulmonary valve, it is not widelypracticed,
Maintenance of good dental hygiene andpractice of antibiotic prophylaxis against SBE areimportant .
A relative iron deficiency state should bedetected and treated
140

Surgical
Palliative Shunt Procedures
Classic Blalock-Taussig shunt, anastomosedbetween the subclavian artery and the ipsilateralPA, is usually performed for infants older than 3months because the shunt is often thrombosedin younger infants with smaller arteries
141

142
Modified Blalock-Taussig (BT) shunt. AGore-Tex interposition shunt is placedbetween the subclavian artery and theipsilateral PA. This is the most popularprocedure for any age, especially for smallinfants younger than 3 months of age
143

144
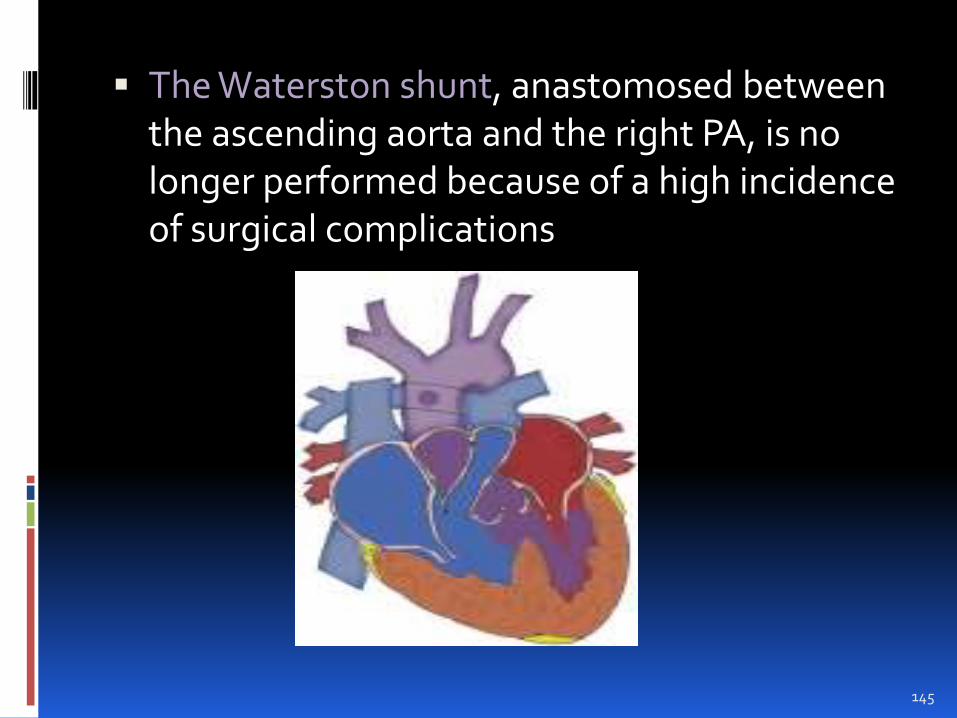
The Waterston shunt, anastomosed between the ascending aorta and the right PA, is no longer performed because of a high incidence of surgical complications
145

The Potts operation
Anastomosed between the descending aortaand the left PA, is no longer performed
146

Complete Repair Surgery
Usually done in the first year of life
Total repair of the defect is carried out undercardiopulmonary bypass
The procedure includes patch closure of theVSD, preferably through a transatrial andtranspulmonary artery approach
widening of the RVOT by division and/orresection of the infundibular tissue; andpulmonary valvotomy,).
The operative mortality for total correction ofTOF is 5%
147

148

Tricuspid Atresia
In this condition, there is no tricuspid valve, therefore, no blood flows from the right atrium to the right ventricle.
Blood in right atrium foramen ovale left atrium and left ventricle aorta
There is complete mixing of the oxy. Blood and un oxy. blood
Tricuspid atresia defect is characterized by the following:
a small right ventricle
a large left ventricle
Small VSD and PDA
diminished pulmonary circulation
cyanosis - bluish color of the skin and mucous membranes caused from a lack of oxygen.
149

150

CLINICAL MANIFESTATIONS History
Cyanosis is usually severe from birth. Tachypnea and poor feeding usually manifest. History of hypoxic spells may be present in infants
with this condition. Physical Examination
Cyanosis, either with or without clubbing, is always present.
A systolic thrill is rarely palpable when associated with PS.
A grade 2 to 3/6 holosystolic (or early systolic) murmur of VSD is usually present at the lower left sternal border
151

Electrocardiography
LVH is usually present;
RAH or biatrial hypertrophy (BAH) iscommon.
X-ray Studies.
The heart size is normal or slightly increased,with enlargement of the RA and LV
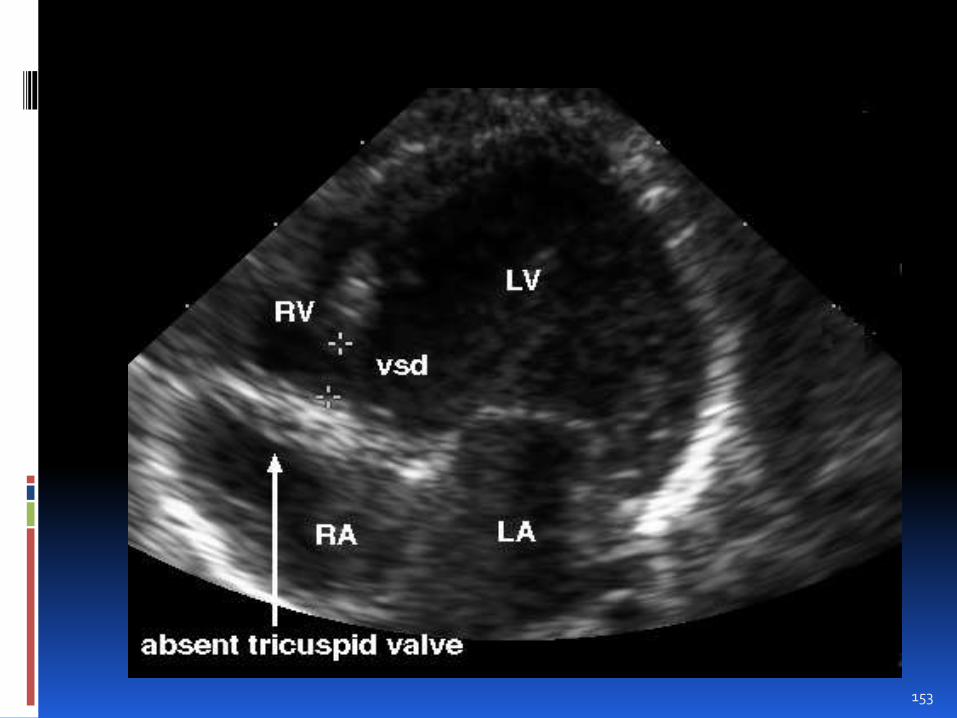
Echocardiography.
Absence of the tricuspid orifice, markedhypoplasia of the RV, and a large LV can beimaged in the apical four-chamber view.
152
153

MANAGEMENT
Initial Medical Management
PGE1 should be started in neonates with severecyanosis to maintain the patency of the ductusbefore planned cardiac catheterization orcardiac surgery.
The Rashkind procedure (balloon atrialseptostomy) may be performed as part of theinitial catheterization to improve the RA-to-LAshunt, especially when the interatrialcommunication is considered inadequate byecho studies.
154

Surgical.
Most infants with tricuspid atresia requireone or more palliative procedures before aFontan-type operation
Ideal candidates for a Fontan-type operationare those who have normal LV function andlow pulmonary resistance
Stage I
Blalock-Taussig shunt, when PBF is small
This procedure results in the volume load onthe LV because the LV supplies blood to boththe systemic and pulmonary circulations.
155

Damus-Kaye-Stansel and shunt operation
the aorta and pulmonary artery are joined using a patch (pink). The blue tube is known as a Modified Blalock-Taussig Shunt.
156

Pulmonary artery banding. PA banding is rarely necessary for infants with CHF resulting from increased PBF. PA banding protects the pulmonary vasculature from developing pulmonary hypertension
Medical follow-up after stage I. Watch for:
Cyanosis (O2 saturation <75%)—cardiac catheterization or MRI to find out its cause.
Poor weight gain (CHF from too much PBF)—tightening of PA band may be necessary.
157

Stage II (at 3 months or by 6 months).
Bidirectional Glenn operation (BDG).
also called bidirectional superiorcavopulmonary shunt
An end-to-side SVC-to-RPA shunt (alsocalled bidirectional superior cavopulmonaryshunt) can be performed by 2.5 to 3 monthsof age
This procedure satisfactorily increasesoxygen saturation
158

159
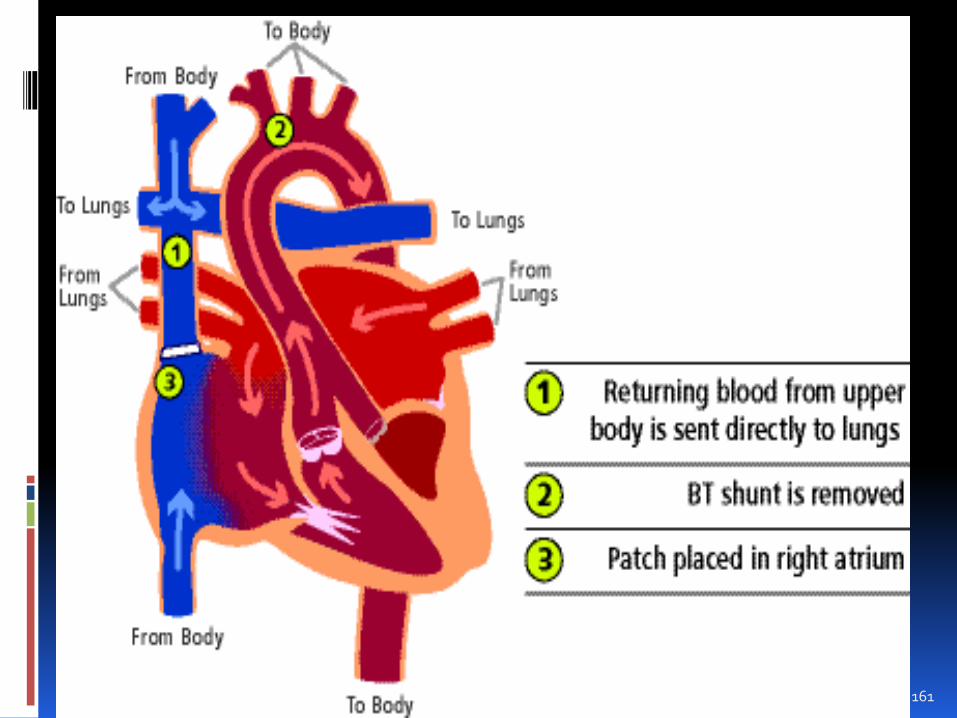
The hemi-Fontan operation.
SVC is connected to PA.
Blood coming back from the upper body nowflows directly to the lungs without going throughthe heart
The Blalock-Taussig (BT) shunt is removed.
A patch is placed over the top part of the heart'sright upper chamber . This prevents blood fromthe upper body from entering the heart andblood from the lower body from entering thelungs. It also maintains a connection that is usedfor the final stage of the repair and greatlysimplifies the last operation.
160
161
Medical follow-up after stage II. Watch for the following:
A gradual decrease in O2 saturation (<75%) may be caused by: .
Opening of venous collaterals
Pulmonary AV fistula (due to the absence of hepatic inhibitory factor)
Transient hypertension—1 to 2 weeks postoperatively—may use ACE inhibitors
162

Stage III ( Fontan operation)—within 1 to 2 years after stage II operation
The whole premise of the Fontan operation isdirecting the entire systemic venous blood tothe pulmonary arteries without anintervening pumping chamber.
The Fontan operation is usually completedwhen the child is around 2 years of age. Thisprocedure can even be performed on infants.
163

164

Postoperative Medical Follow-up
Patients should maintain a low-salt diet. Medications: Some patients need continued digoxin and diuretic
therapy. An angiotensin-converting enzyme (ACE) inhibitor is
generally recommended. Aspirin (or even warfarin) is used to prevent
thrombus formation in the RA. Patients should not participate in competitive,
strenuous sports. Antibiotic prophylaxis against SBE should be
observed when indications arise.165
MIXED BLOOD FLOW
Difference in the PA pressure and aortic pressure--> pulmonary congestion
Volume load in ventricles -->decresed cardiac out put
Relative desaturation of systemic blood,
Mixing of blood from pulmonary and systemic circulation within the heart chambers
166

Transposition of the Great Arteries (TGA)
the aorta is connected to the right ventricle, and the pulmonary artery isconnected to the left ventricle
Oxygen-poor (blue) blood returns to the right atrium from the body passes through the right atrium and ventricle, into the misconnectedaorta back to the body.
Oxygen-rich (red) blood returns to the left atrium from the lungs passes through the left atrium and ventricle, into the pulmonary arteryand back to the lungs.
Other heart defects are often associated with TGA
- atrial or ventricular septal defect
- may be necessary in order for the infant with TGA to survive
- Allow mixing of blood – providing at least smaller amounts of oxygento the body
167

168

CLINICAL MANIFESTATIONS
History
History of cyanosis from birth is alwayspresent.
Signs of congestive heart failure (CHF) withdyspnea and feeding difficulties developduring the newborn period.
169

Physical Examination
Moderate to severe cyanosis is present,
The S2 is single and loud..
If CHF supervenes, hepatomegaly anddyspnea develop.
170

Electrocardiography
There is a rightward QRS axis (i.e., +90 to+200 degrees).
Right ventricular hypertrophy (RVH) isusually present
Biventricular hypertrophy (BVH) may bepresent
Occasionally right atrial hypertrophy (RAH) ispresent.
171

Echocardiography.
In the parasternal short-axis view, the “circleand sausage” appearance of the normal greatarteries is not visible. Instead, the greatarteries appear as “double circles”
3. In the apical and subcostal five-chamberviews, the PA arises from the LV, and theaorta arises from the RV.
172

173

X-ray Studies
Cardiomegaly
An egg-shaped cardiac silhouette
174

NATURAL HISTORY
Without surgical intervention, death occurs in 90% of patients before they reach 6 months
of age.
175

MANAGEMENT Medical
Arterial blood gases and pH should beobtained and metabolic acidosis should becorrected
PGE1 infusion should be started to improvearterial oxygen saturation by reopening theductus.
Oxygen administration
A balloon atrial septotomy (Rashkindprocedure) may be performed to increase themixing by opening the atrial septum
176

Surgical
An arterial switch procedure- performed infirst week of life
Transecting the great arteries andanastomosing the main pulmonary artery tothe proximal aorta and anastomosing theascending aorta to the proximal pulmonaryartery
The coronary arteries are switched fromproximal aorta to the proximal pulmonaryartery to create a new aorta
177

178

Intra atrial baffle repairs –An intraatrial baffle is created to divert the venous blood to the mitral valve and pulmonary venous blood to the tricuspid valve using using patients atrialseptum or a prosthetic valve.
179

Rastelli procedure-operative choice in patients with TGA,VSD, and severe pulmonicstenosis.
It involves closure of VSD with baffle->LV blood directed through VSD in to aorta
Pulmonic valve is then closed , and a conduit is placed from RV to PA
180

Total Anomalous Pulmonary Venous Return
No direct communication between the pulmonary
veins and the left atrium
Drain anomalously into the systemic venous
tributeries or into right atrium
4 types
Supracardiac:( 50% of TAPVR ). The commonpulmonary venous sinus drains into the right SVC
Cardiac: (20% of TAPVR) .The commonpulmonary venous sinus drains into the coronarysinus
181

Infracardiac:( 20% of TAPVR patients) Thecommon pulmonary venous sinus drains tothe portal vein, ductus venosus, hepatic vein,or inferior vena cava (IVC).
Mixed type: This type, which is acombination of the other types, accounts for10% of TAPVR patients
182

183

TOTAL ANOMALOUS PULMONARY VENOUS
RETURN –Clinical ManifestationsHistory
CHF with gowth retardation
Frequent pulmonary infection
Mild cyanosis
Physical examination
Undernourished
Signs of CHF
Precordial bulge
ECG
RVH and occational RAH
184

TOTAL ANOMALOUS PULMONARY VENOUS
RETURN –Clinical Manifestations
X- ray studies
Cardiomegaly
Kerley B lines
Snowmans sign/ figure of 8
Echo
A large RA and a small LA, with deviation of the atrial septum to the left and dilated PAs, are also present.
185

186

MANAGEMENT
medical
Intensive anticongestive measures
Metabolic acidosis should be corrected,
Infants with severe pulmonary edema-shouldbe intubated and receive ventilator support
In some patients with pulmonaryhypertension, PGE1 can increase systemicflow by keeping the ductus open
187

Surgical treatment
Supracardiac Type.
A large, side-to-side anastomosis is madebetween the common pulmonary venoussinus and the LA. The ASD is closed with acloth patch.
TAPVR to the Right Atrium.
The atrial septum is excised and a patch issewn in such a way that the pulmonaryvenous return is diverted to the LA . TheASD may have to be enlarged.
188

TAPVR to the Coronary Sinus.
An incision is made in the anterior wall of thecoronary sinus (“unroofing”) to make acommunication between the coronary sinusand the LA. A single patch closes the originalASD and the ostium of the coronary sinus. Thisresults in the drainage of coronary sinus bloodwith low oxygen saturation into the LA
Infracardiac Type.
A large vertical anastomosis is made betweenthe common pulmonary venous sinus and theLA. The common pulmonary vein, whichdescends vertically to the abdominal cavity, isligated above the diaphragm
189

Truncus Arteriosus The aorta and pulmonary artery start as a single blood vessel, which
eventually divides and becomes two separate arteries.
Truncus arteriosus occurs when the single great vessel fails to separate completely, leaving a connection between the aorta and pulmonary artery.
Usually accompanied by a ventricular septal defect
EFFECTS:
oxygen-poor (blue) and oxygen-rich (red) blood mix back and forth through the ventricular septal defect.
This mixed blood then flows through the common truncal vessel. Some of it will flow to pulmonary artery and on to the lungs, and some of the mixed blood will go into the aortic branch and to the body.
The mixed blood that goes to the body does not have as much oxygen as normal, and will cause varying degrees of cyanosis
190

191

CLINICAL MANIFESTATIONS
History
Cyanosis may be seen immediately afterbirth.
Signs of CHF develop within several days toweeks after birth.
History of dyspnea with feeding, failure tothrive, and frequent respiratory infections isusually present in infants.
192

Physical Examination
Varying degrees of cyanosis and signs of CHFwith tachypnea and dyspnea are usuallypresent.
The peripheral pulses are bounding, with awide pulse pressure.
A systolic click is frequently audible at theapex and upper left sternal border.
193

Electrocardiography.
BVH is present in 70% of cases
X-ray Studies.
Cardiomegaly is usually present
Echocardiography.
A large, single great artery arises from theheart .The type of persistent truncusarteriosus can be identified, and the size ofthe PAs can be determined.
194
Medical
Vigorous anticongestive measures withdigitalis and diuretics
surgical
Corrective repair
Closing the VSD
Excising the pul. Arteries from aorta , andattaching them to the RV by means ofhomograft
Prognosis
Mortality greater than 10%
195

Hypoplastic Left Heart Syndrome
HLHS occurs in 1% of all congenital heartdefects or 9% of such defects in critically illnewborns
Underdevelopment of the left side of the heartresulting in a hypoplastic left ventricle andaortic atresia
Most of the blood from LA Flows across PFOto RARVPA
The descending aorta receives blood from pdasupplying systemic blood flow
196

197

Effects
PFO allows saturated blood from LA to mixwith desaturated blood from RA-->RV -->PA
from PA blood flows to lung and thenthrough ductus arteriosus in to the aorta andout f the body
The coronary and cerebral vessels receiveblood by retrograde flowthrough thehypoplastic ascending aorta
198

CLINICAL MANIFESTATIONS
A neonate with HLHS becomes critically ill withinthe first few hours to the first few days of life.
Tachycardia, dyspnea, pulmonary crackles, weakperipheral pulses, and vasoconstrictedextremities are characteristic.
The patient may not have severe cyanosis buthas a grayish blue color of the skin with poorperfusion.
The S2 is loud and single.. The ECG almost always shows RVH. Chest x-ray films characteristically show
pulmonary venous congestion or pulmonaryedema
Arterial blood gas levels reveal a slightlydecreased Po2 and a normal Pco2.
199
Therapeutic management
PGE1 infusion to maintain ductal patency
Surgical procedure
Several staged approach
1st stage- Norwood procedure
Anastomosis of main PA to the aorta to create anew aorta, placement of a shunt or inserting aconduit from the RV to PA to provide pulmonaryblood flow , and creation of a large ASD.
2nd stage-Bidirectional Glenn Shunt
Done at 6-9 months of age to relieve cyanosis and reduce overload in RV
200

201

Final repair-Modified Fontan Procedure
Transplantation
202

Ebstein's Anomaly
Ebstein anomaly is a congenital heartdefect in which the septal leaflet ofthe tricuspid valve is displaced towards theapex of theright ventricle of the heart.
The valve leaflets, however, are to a varyingdegree, attached to the walls and septum ofthe right ventricle.
There is subsequent 'atrialization' of a portionof the morphologic right ventricle
203

204
Pathophysiology
The right ventricle is thus divided into 2 parts by the abnormal tricuspid valve
the 1st, a thin-walled “atrialized” portion, is continuous with the cavity of the right atrium;
the 2nd, often smaller portion consists of normal ventricular myocardium.
The right atrium is enlarged as a result of tricuspid valve regurgitation,
205
In more severe forms of Ebstein anomaly, theeffective output from the right side of theheart is decreased due to a combination ofthe poorly functioning small right ventricle,tricuspid valve regurgitation, and obstructionof the right ventricular outflow tractproduced by the large, sail-like, anteriortricuspid valve leaflet.
The increased volume of right atrial bloodshunts through the foramen ovale (orthrough an associated atrial septal defect) tothe left atrium and produces cyanosis
206

CLINICAL MANIFESTATIONS
History
In severe cases, cyanosis and CHF developduring the first few days of life.
Children with milder cases may complain ofdyspnea, fatigue, cyanosis, or palpitation onexertion.
207

Physical Examination
Mild to severe cyanosis is present, as well asclubbing of the fingers and toes in older infantsand children.
Characteristic triple or quadruple rhythm isaudible.
Electrocardiography
1. Characteristic ECG findings of RBBB and RAHare present in most patients with this condition
x-ray Studies.
. In severe cases, an extreme cardiomegaly witha balloon-shaped heart and decreasedpulmonary vascular markings are present
208

Echocardiography
The tricuspid valve leaflets are elongated, redundant, and dysplastic
A large RA, including the atrialized RV, and a small functional RV represent anatomic severity
209

MANAGEMENT
Medical
In severely cyanotic newborns, intensivetreatment with mechanical ventilation,
PGE1 infusion
inotropic agents
correction of metabolic acidosis
210

Surgical
Palliative procedures
Blalock-Taussig shunt
Starnes operation- a procedure to reduce the RV or RA
Classic Glenn anastomosis or its modification may be considered in severely cyanotic infants
211

Definitive procedures
Two-ventricular repair
Danielson technique: For repair of thetricuspid valve
Carpentier technique: This repair alsoplicates the atrialized portion of the RV andthe tricuspid annulus
One-ventricular repair:
For patients with inadequate size of the RV,a Fontan-type operation is usuallyperformed in stages following the initialpalliative procedures such as bidirectionalGlenn operation
212

Nursing diagnosis
Impaired gas exchange related to altered pulmonary blood flow or oxygen deprivation
Altered cardiac output related to specific anatomic defect
Activity intolerance related to decreased oxygenation in blood and tissues
Altered Nutrition: less than body requirements related to the excessive energy demands required by increased cardiac workload
Increased potential for infection related to poor nutritional status
Anxiety related to diagnostic procedures and hospitalization
Developmental delay related to decreased energy, inadequate nutrition, physical limitations and social isolation
Alteration in parenting related to parental perception of the child as vulnerable
213

NURSING INTERVENTIONS
214

Relieve the respiratory distress associated with increased pulmonary blood flow or oxygen deprivation Determine degree of respiratory distress Position child at 45 degree angle to decrease pressure of the
viscera on the diaphragm and increase lung volume Pin diapers loosely and provide loose-fitting pajamas for older
children Feed slowly Tilt infant’s head slightly Suction the nose and throat if unable to cough out secretions Provide oxygen therapy as needed Improve oxygenation o that the body functions may be
maintained Provide effective oxygen environment Observe response to oxygen therapy Observe response to oxygen weaning therapy
Relieve Hypoxic spells associated with cyanotic types of Congenital heart disease
Observe for “tet” spells Encourage fluid intake Obtain vital signs
215

Nursing interventions
A. Provide adequate nutritional and fluidintake to maintain the growth anddevelopmental needs of the child
Feed in semi-erect position
Provide small frequent feedings
Provide foods with high nutritional value
Determine child’s likes and dislikes
Strict input and output
Daily weight
216

B. Prevent infection
Prevent exposure to communicable diseases
Immunizations should be up-to-date
Handwashing should be observed
Be certain that the child receives prophylactic medication for infective endocarditis
217

C. Reduce the workload of the heart since decreased activity and expenditure of energy will decrease oxygen requirements
Uninterrupted rest
Avoid unnecessary activities
Prevent excessive crying
Provide diversional activities
Prevent constipation
218

D. Observe child for symptoms of CongestiveHeart Failure that occur frequently as acomplication of Congenital Heart Disease
E. Observe for the development of symptoms ofinfective endocarditis that may occur as acomplication of congenital heart disease
F. Observe for the development of thrombosisthat may occur as a complication of congenitalheart disease
G. Prepare the child for diagnostic and treatmentprocedures
H. Explain cardiac problems to child and parents
219

Health Education
A. Instruct the family in necessary measures to maintain the child’s health
B. Teach the family about the defect and its treatment
C. Encourage the parents and other persons to treat child in a normal manner as possible
220

221