Congenital anomalies of the pulmonary arteries: Spectrum of … · 2018. 8. 20. · Congenital...
9
Radiología. 2017;59(3):209---217 www.elsevier.es/rx RADIOLOGY THROUGH IMAGES Congenital anomalies of the pulmonary arteries: Spectrum of findings on computed tomography J. Bueno a,* , L. Flors a , M. Mejía b a Imagen Cardiotorácica, Departamento de Radiología e Imagen Médica, Universidad de Virginia, Charlottesville, VA, United States b Departamento de Radiología, Fundación Valle del Lili, Cali, Valle del Cauca, Colombia Received 25 April 2016; accepted 16 September 2016 KEYWORDS Pulmonary arteries; Congenital anomalies; Pulmonary agenesis; Anomalous origin of the pulmonary artery; Tetralogy of Fallot; Computed tomography Abstract Objective: Congenital anomalies of the pulmonary arteries are uncommon. They can occur in isolation or in association with congenital heart defects. Isolated congenital anomalies remain undiscovered until they are reported as incidental findings on imaging tests, usually not until adolescence. We review the embryological development and normal anatomy of the pulmonary arteries as well as the spectrum of computed tomography findings for various con- genital anomalies: unilateral interruption of the pulmonary artery, anomalous origin of the left pulmonary artery (pulmonary artery sling), idiopathic aneurysm of the pulmonary artery, and other anomalies associated with congenital heart defects. Conclusion: Congenital anomalies of the pulmonary arteries represent a diagnostic challenge for clinicians and radiologists. Computed tomography is useful for their diagnosis, and gen- eral radiologists need to be familiar with their imaging appearance because they are often discovered incidentally. © 2016 SERAM. Published by Elsevier Espa˜ na, S.L.U. All rights reserved. PALABRAS CLAVE Arterias pulmonares; Anomalías congénitas; Anomalías congénitas de las arterias pulmonares: espectro de hallazgos en tomografía computarizada Resumen Las anomalías congénitas de las arterias pulmonares (AP) son poco frecuentes y pueden presentarse aisladas o asociadas a defectos cardiacos congénitos. En general, si son Please cite this article as: Bueno J, Flors L, Mejía M. Anomalías congénitas de las arterias pulmonares: espectro de hallazgos en tomografía computarizada. Radiología. 2017;59:209---217. * Corresponding author. E-mail address: [email protected] (J. Bueno). 2173-5107/© 2016 SERAM. Published by Elsevier Espa˜ na, S.L.U. All rights reserved. Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited. Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Transcript of Congenital anomalies of the pulmonary arteries: Spectrum of … · 2018. 8. 20. · Congenital...

Radiología. 2017;59(3):209---217
www.elsevier.es/rx
RADIOLOGY THROUGH IMAGES
Congenital anomalies of the pulmonary arteries:
Spectrum of findings on computed tomography�
J. Bueno a,∗, L. Flors a, M. Mejíab
a Imagen Cardiotorácica, Departamento de Radiología e Imagen Médica, Universidad de Virginia, Charlottesville, VA,
United Statesb Departamento de Radiología, Fundación Valle del Lili, Cali, Valle del Cauca, Colombia
Received 25 April 2016; accepted 16 September 2016
KEYWORDSPulmonary arteries;Congenitalanomalies;Pulmonary agenesis;Anomalous origin ofthe pulmonary artery;Tetralogy of Fallot;Computedtomography
Abstract
Objective: Congenital anomalies of the pulmonary arteries are uncommon. They can occur
in isolation or in association with congenital heart defects. Isolated congenital anomalies
remain undiscovered until they are reported as incidental findings on imaging tests, usually
not until adolescence. We review the embryological development and normal anatomy of the
pulmonary arteries as well as the spectrum of computed tomography findings for various con-
genital anomalies: unilateral interruption of the pulmonary artery, anomalous origin of the left
pulmonary artery (pulmonary artery sling), idiopathic aneurysm of the pulmonary artery, and
other anomalies associated with congenital heart defects.
Conclusion: Congenital anomalies of the pulmonary arteries represent a diagnostic challenge
for clinicians and radiologists. Computed tomography is useful for their diagnosis, and gen-
eral radiologists need to be familiar with their imaging appearance because they are often
discovered incidentally.
© 2016 SERAM. Published by Elsevier Espana, S.L.U. All rights reserved.
PALABRAS CLAVEArterias pulmonares;Anomalíascongénitas;
Anomalías congénitas de las arterias pulmonares: espectro de hallazgos
en tomografía computarizada
Resumen Las anomalías congénitas de las arterias pulmonares (AP) son poco frecuentes y
pueden presentarse aisladas o asociadas a defectos cardiacos congénitos. En general, si son
� Please cite this article as: Bueno J, Flors L, Mejía M. Anomalías congénitas de las arterias pulmonares: espectro de hallazgos en tomografía
computarizada. Radiología. 2017;59:209---217.∗ Corresponding author.
E-mail address: [email protected] (J. Bueno).
2173-5107/© 2016 SERAM. Published by Elsevier Espana, S.L.U. All rights reserved.
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

210 J. Bueno et al.
Agenesia pulmonar;Origen anómalo de laarteria pulmonar;Tetralogía de Fallot;Tomografíacomputarizada
aisladas, suelen pasar clínicamente inadvertidas hasta la adolescencia y ser un hallazgo inci-
dental en exploraciones radiológicas. Nuestro objetivo es revisar las bases embriológicas del
desarrollo de las AP, su anatomía normal y el espectro de hallazgos por tomografía com-
putarizada (TC) de sus anomalías congénitas, en concreto la interrupción unilateral de la AP,
el origen anómalo de la AP izquierda (sling pulmonar), el aneurisma idiopático de la AP y
otras anomalías asociadas a defectos cardiacos congénitos. Las anomalías congénitas de las AP
representan un reto diagnóstico, tanto clínico como radiológico. La TC es una herramienta útil
en su diagnóstico y el radiólogo general debe estar familiarizado con su apariencia, ya que
pueden ser un hallazgo incidental.
© 2016 SERAM. Publicado por Elsevier Espana, S.L.U. Todos los derechos reservados.
Introduction
Congenital anomalies of pulmonary arteries (PA) are usuallyassociated to other congenital heart defects and they do notusually occur in isolation. Although they can result in symp-toms during childhood, the PA isolated anomalies usually gounnoticed until adolescence or early adult age.1,2
The imaging diagnosis of PA anomalies are challengingboth for the clinician and the radiologist since conventionalimage modalities like X-rays and ultrasounds have a limitedvalue when it comes to detection and characterization,while the pulmonary angiography is an invasive method usu-ally reserved for cases that require treatment. This is thereason why both the computed tomography (CT) and mag-netic resonance imaging (MRI) play an essential role in thestudy of PA. In part thanks to the possibility of generat-ing particular multiplanar and volumetric reconstructionsthe angio-CT offers great advantages in the diagnosis andfollow-up of these anomalies making the characterization ofthe vascular and valvular anatomies possible as well as anyother associated findings in other organs. Also these recons-tructions facilitate the communication of findings and theunderstanding of the anatomy for an optimal surgical plan.
The goal of this paper is to review the embyological basisfor the development of PA, the PA normal anatomy and imagefindings of PA congenital anomalies----especially the unilat-eral interruption of PA, the anomalous origin of the leftPA (pulmonary sling), the main PA idiopathic aneurysm andother anomalies associated with congenital heart anomalies.
Embryological basis
After the formation of the cardiac tube and its differen-tiation into primitive segments that give rise to cardiacstructures the arterial trunk gives rise to the aorta andthe proximal section of the PA.3 During the fifth week ofembryonic life the aortopulmonary septum is created in aspiral-like shape that splits the truncus arteriosus into aortaand PAs (Fig. 1).
Thus the trunk of the pulmonary artery is derived intothe truncus arteriosus. The proximal sections of the sixthbilateral aortic arches make up the right and left Pas.4 Thedistal sections of the PAs are derived from primitive buds
Aortic
valve
Pulmonary
valve
TSVI
TSVD
Aorta
Pulmonary artery
Figure 1 Embryonic development of pulmonary artery.
Schematic illustration of the arterial trunk (left). The aortopul-
monary septum (arrow) shows a spiral disposition and divides
the arterial trunk into aorta and pulmonary aorta as well as the
aortic and pulmonary valves while dividing the outflow track of
both ventricles inferiorly. RVOT: right ventricle outflow track;
LVOT: left ventricle outflow track.
that come from these arches and grow toward the insideof lung buds (the origin of lungs) to later anastomose withthem.
We should remember that: since the embryonic lungmorphogenesis is a process parallel to the airway branch-ing morphogenesis,4 it is not rare to find a combination ofvascular and bronchial tree anomalies.
The anatomy of pulmonary arteries
The PA trunk stems from the right ventricle and bifurcatesinto the main right and left PAs. The pulmonary valve is madeup of three valvular sinuses and can be found in the proximalsection of the pulmonary trunk----the pulmonary root.5
The maximum diameter of the adult pulmonary trunkis 28 mm.6 The right and left PAs show an intrapericar-dial trajectory before bifurcating into the lobar arteries inevery side. Because of the special location of the pulmonarytrunk----left to the middle line, the intrapericardial segmentof the right PA is longer ant its bifurcation occurs at pul-monary root level. The right PA is located under the right
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Congenital anomalies of the pulmonary arteries: findings on computed tomography 211
Figure 2 Normal anatomy of pulmonary arteries. The right pulmonary artery (marker in a and b) has an inferior location with
respect to the main right bronchus. The left pulmonary artery (marker in c and d) has a superior location with respect to the main
left bronchus (arrowhead in d) and is the culprit of the higher position of the left pulmonary hilum in the normal thoracic X-ray
(arrow in e).
upper lobar bronchus (hypobronchial) laterally following theintermediate bronchus (Fig. 2a and b). The distal left PAresides in an epibronchial location (superior to the left mainbronchus) and keeps a posterior location to the bronchusuntil it bifurcates into the left lobar arteries (Fig. 2c---e).Both PAs should be of a similar caliber.
The central axial interstice area----a network of connec-tive tissue supporting the pulmonary structures reaches outfrom the pulmonary hila while surrounding the PAs and themain bronchi----reaching out distally as they originate lobar,segmental and sub-segmental branches. Both the arteriesand the bronchi are therefore one single bronchovascularpackage and have a similar diameter.
Congenital anomalies of pulmonary arteries
The congenital anomalies of PAs are usually associated withother congenital heart defects such as Fallot’s tetralogy.The isolated anomalies of PAs are a very select less commongroup made up of four main anomalies each and everyoneof them with defined anatomic characteristics.
Unilateral absence of pulmonary artery
Also known as proximal interruption of the PA since the distalsection of the artery inside the pulmonary parenchyma is
usually intact due to its different embryonic origin.3,6 Thecongenital interruption of PA is uncommon (reported in oneof every 200,000 individuals7) and it is thought to be due toan abnormal involution of the proximal section of the sixthprimitive aortic arch with a higher frequency in the rightside.3,8,9
We should remember that: when the homolaterallung is present----at times formed partially or rudimen-tary the pulmonary perfusion is provided by systemiccollaterals mainly bronchial arteries and intercostal arter-ies through transpleural branches, the internal mammaryartery, the subclavian artery or the brachiocephalic trunk(Figs. 3 and 4). The affected PA can be totally absent or end1 cm away from its origin, while the aortic arch is usuallycontralateral to the affected artery (Fig. 4).
Anomalous origin of the left pulmonary artery(pulmonary artery sling)
The aberrant disposition of the left pulmonary artery is dueto its abnormal origin from the right pulmonary artery and iscalled pulmonary sling due to its abnormal trajectory acrossthe tracheoesophageal space (Fig. 5). This anomaly is due toan abnormal process of involution of the sixth left proximalaortic arch.7,10,11 It usually occurs with respiratory distressor repetitive pulmonary infections.12,13
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

212 J. Bueno et al.
Figure 3 Eighteen-year-old female with suspicion of pneumonia. Thoracic X-ray; posterior-anterior (a) and lateral projections of
PA (b) showing deviation of the mediastinum to the left accompanied by a reduced left pulmonary volume (a). In the lateral X-ray
(b) we can see what looks like an abnormal looking left pulmonary hilum (arrow) without any circular lucency so typical of the main
left lobe bronchus due to a partial congenital absence of the pulmonary artery on this side. The X-ray does not show pneumonic
consolidation.
Figure 4 Fifty year old asymptomatic female. Posterior-anterior thoracic X-ray (a) showing loss of left pulmonary volume and
mediastinic deviation to the left as well as right aortic arch (arrow). The angio-CT axial images (b---d) confirm the congenital absence
of the left pulmonary artery (arrowhead) from its origin (b). The descending thoracic aorta is located to the right (arrow in b).
Pulmonary perfusion is provided by bronchial and intercostal dilated arteries (arrows in c). In the pulmonary window (d) we can
see left lung hyperplasia showing diffuse attenuation in polished glass and interlobular septal thickening. Subpleural reticulation is
due to perfusion provided by transpleural branches from intercostal arteries (arrow).
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Congenital anomalies of the pulmonary arteries: findings on computed tomography 213
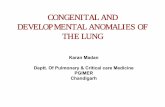
Figure 5 Five-year-old male with stress dyspnea. Angio-CT, maximum intensity projection (MIP) reconstruction, axial (a) and
sagittal (b) images showing the abnormal origin of the left PA from the right PA (a), and an abnormal retrotracheal trajectory toward
the left pulmonary hilum (arrowhead). The sagittal MIP reconstruction (b) shows the abnormal position of the left pulmonary artery,
posterior to the main left bronchus (arrow).
Figure 6 Five-year-old male (same patient from Fig. 5) with
anomalous origin of left pulmonary artery or pulmonary sling.
Coronal reconstruction in minimum intensity projection (MinIP)
showing abnormal segmentation of the tracheobronchial tree.
The bronchus for the right upper lobe stems directly from the
trachea (tracheal bronchus) (arrow). In this case there are no
stenosed areas.
We should remember that: the abnormal associated tra-cheal or bronchial segmentation (supernumerary bronchus,tracheal bronchus, tracheobronchial stenosis) subcatego-rizes these patients into a group with higher rates ofmortality or morbidity6 (Fig. 6).
Aneurysm of the idiopathic pulmonary artery
The idiopathic dilation of the trunk of the PA is a rare condi-tion that usually affects the pulmonary trunk in isolation(Fig. 7), but can reach out the left or right pulmonary arter-ies. Even though it can occur in isolation, the aneurysms of
the PA are usually associated with other congenital heartanomalies.17
The exact etiology is not fully established but it is thoughtto be due to the weakness of the middle elastic layers ofthe arterial wall14----suggestive of a similar physiopathologyto that of aortic aneurysms.
The diagnosis is achieved when there is dilation of thetrunk of the pulmonary artery (>30 mm) and intracardiac orextracardiac shunts, pulmonary disease or chronic heart dis-ease, vascular disease and pulmonary artery hypertension.15
We should remember that: the pulmonary valve diseaseis a finding associated with the idiopathic aneurysm of thePA16,17----usually accompanied by valve heart failure. Eventhough the development of symptoms due to pulmonaryvalve failure can lead to an early diagnosis, most thesepatients are usually asymptomatic until old age and can bediagnosed incidentally.
Other anomalies associated to congenital heart defects
Other congenital anomalies like pulmonary valve stenosis(Fig. 8), atresia, hypoplasia or segmental stenosis of the PA,or the anomalous origin of the PAs from the aorta are morecommon than the isolated cases and they are associated withother congenital heart defects like the double outflow tractof the right ventricle and Fallot’s tetralogy.
The combination of an abnormal position (cephalic andanterior) of the aortopulmonary septum and hypertrophy ofthe septo-parietal trabeculations of the right ventricle arethe cause for the outflow tract obstruction of the right ven-tricle that is so characteristic of Fallot’s tetralogy.18 This ischaracteristically associated with variable degrees of out-flow tract obstruction of the right ventricle with infundibularstenosis or pulmonary valve stenosis (or both). Pulmonaryatresia in extreme cases of Fallot’s tetralogy and trunkstenosis of the pulmonary artery (Fig. 9) or its branches areassociated findings too.19 The seriousness of the patient’ssymptoms and the surgical plan are initially determined bythe degree of obstruction to pulmonary flow. In serious casesof Fallot’s tetralogy there is pulmonary atresia (extremeFallot or arterious pseudo trunk) with a complete absence
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

214 J. Bueno et al.
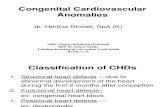
Figure 7 Asymptomatic sixteen-year-old male. Axial image (a) and CT sagittal reconstruction (b) with contrast showing massive
dilation of the main left pulmonary artery (asterisk) that measures 45 mm. Right and left pulmonary arteries of normal caliber. In
this case the pulmonary valve was competent.
Figure 8 Thirty-two-year old male with serious stenosis of his pulmonary valve and moderate failure. Angio-CT images --- axial
images (a---c) and oblique sagittal reconstruction (d) showing pulmonary valve thickening (arrows in a) and dilation typical of the
pulmonary trunk and left pulmonary artery (asterisk in b) showing post-stenotic dilation. Right ventricle in the borderline threshold
of normalcy with marked hypertrophy (arrowheads). We can also see infundibular hypertrophy (hollow arrow) conditioning the
added subvalvular stenosis.
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Congenital anomalies of the pulmonary arteries: findings on computed tomography 215
Figure 9 Six year-old-male with a history of Fallot’s tetralogy.
The arrow shows the proximal segmental stenosis of the pul-
monary artery trunk as an associated finding of the pulmonary
stenosis so typical of this condition.
of the main pulmonary artery and pulmonary circulationreplaced by aortopulmonary collateral circulation or tho-racic arteries stemming directly from the descending aorta(Fig. 10).
Angio-CT is an excellent tool for both preoperativeand postoperative assessments since it allows us to diag-nose complications such as stenoses or pulmonary residualobstructions (that can affect the outflow tract of the rightventricle all the way to the pulmonary branches----surgicalducts included (Fig. 11), outflow tract aneurysms of the rightventricle and defects at residual interventricular septumlevel (Fig. 12).
Figure 10 Eleven-year-old female with a history of Fal-
lot’s tetralogy and pulmonary atresia (arterious pseudo-trunk).
Coronal reconstruction with MIP showing one aortopulmonary
collateral of large caliber (arrow) that provided arterial flow to
the right lung due to complete obstruction of the right ventricle
outflow tract so typical of this condition.
Dilation and right ventricular dysfunction --- usually dueto pulmonary valve failure as the result of transannularpatch can also be assessed through cardiac CT with elec-trocardiographic synchronization which is considered analternative to cardiac magnetic resonance imaging (MRI) incases where it is not recommended such as in patients withpacemakers.20,21
Figure 11 Seventeen-year-old male with a history of Fallot’s tetralogy and pulmonary stenosis corrected through angioplasty.
Volumetric (a) and multiplanar reconstructions in oblique planes showing calcification and serious stenosis also affecting the right
ventricle outflow tract and the pulmonary trunk (arrows in b). Also stenosis is evident in the proximal section of both main pulmonary
arteries above all the left one where one intimal flap of skin (hollow arrow) can be seen probably due to dissection secondary to a
prior angioplasty (c). Dilation of the right ventricle (asterisk) can be seen too.
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

216 J. Bueno et al.
Figure 12 Sixteen-year-old male with a history of Fallot’s tetralogy corrected through transannular patch during his infancy and
further stenosis of left pulmonary artery corrected through stent implantation. The patient was asymptomatic yet the ultrasound
showed serious pulmonary failure. Angio-CT axial images showing calcification (arrow in a) of dilated transannular ring and left
pulmonary artery with patent stent (hollow arrow) of normal caliber (b). We can also see a significant dilation of the left ventricle
(asterisk in c) and residual interventricular septum defects (black arrow).
Conclusions
The congenital anomalies of the PAs can be asymptomaticuntil old age and be challenging when it comes to a correctdiagnosis. Finding them and characterizing them throughtransthoracic echocardiography (TTE) or X-ray is complexand this is the reason why the angio-CT is an essential modal-ity that allows us to characterize the vascular and valvularanatomies of these conditions as well as any associated find-ings in other organs. It is important for the radiologist toknow this spectrum of anomalies since incidental diagnosesare not uncommon.
Ethical responsibilities
Protection of people and animals. The authors declare thatno experiments with human beings or animals have beenperformed while conducting this investigation.
Confidentiality of data. The authors confirm that in thisarticle there are no data from patients.
Right to privacy and informed consent. The authors con-firm that in this article there are no data from patients.
Authors
1. Manager of the integrity of the study: JB, LF, MM.2. Study Idea JB, LF, MM.3. Study Design: JB, LF, MM.4. Data Mining: JB, LF, MM.5. Data Analysis and Interpretation: JB, LF, MM.6. Statistical Analysis: N/A.7. Reference: JB, LF.8. Writing: JB, LF, MM.9. Critical review of the manuscript with intellectually rel-
evant remarks: JB, LF, MM.10. Approval of final version: JB, LF, MM.
Conflicts of interests
The authors declare no conflict of interests associated withthis article whatsoever.
References
1. Catala FJ, Marti-Bonmati L, Morales-Marin P. Proximal absence
of the right pulmonary artery in the adult: computed tomo-
graphy and magnetic resonance findings. J Thorac Imaging.
1993;8:244---7.
2. Espinosa L, Agarwal P. Adult presentation of right lung agenesis
and left pulmonary artery sling. Acta Radiol. 2008;49:41---4.
3. Davies M, Guest PJ. Developmental abnormalities of the great
vessels of the thorax and their embryological basis. Br J Radiol.
2003;76:491---502.
4. Zylak CJ, Eyler WR, Spizarny DL, Stone CH. Developmental
lung anomalies in the adult: radiologic---pathologic correlation.
Radiographics. 2002;22:S25---43.
5. Saremi F, Gera A, Ho SY, Hijazi ZM, Sanchez-Quintana D.
CT and MR imaging of the pulmonary valve. Radiographics.
2014;34:51---71.
6. Castaner E, Gallardo X, Rimola J, Pallardo Y, Mata JM, Perendreu
J, et al. Congenital and acquired pulmonary artery anomalies in
the adult: radiologic overview. Radiographics. 2006;26:349---71.
7. Carter BW, Lichtenberger JP 3rd, Wu CC. Congenital abnor-
malities of the pulmonary arteries in adults. Am J Roentgenol.
2014;202:W308---13.
8. Ho PH, Shiau EL. Proximal interruption of the pulmonary artery.
QJM. 2013;106:957---8.
9. Krishnan AS, Babar JL, Gopalan D. Imaging of congenital and
acquired disorders of the pulmonary artery. Curr Probl Diagn
Radiol. 2012;41:165---78.
10. Kir M, Saylam GS, Karadas U, Yilmaz N, Cakmakci H, Uzuner N,
et al. Vascular rings: presentation, imaging strategies, treat-
ment, and outcome. Pediatr Cardiol. 2012;33:607---17.
11. Garrote Molpeceres R, Rellan Rodriguez S, Urbaneja Rodriguez
E, Pino Vazquez MA, Fuertes Alija JJ. Pulmonary artery sling as
a casual diagnosis. An Pediatr. 2014;80:267---8.
12. Leonardi B, Secinaro A, Cutrera R, Albanese S, Trozzi M, Frances-
chini A, et al. Imaging modalities in children with vascular ring
and pulmonary artery sling. Pediatr Pulmonol. 2015;50:781---8.
13. Li Y, Zhou G, Zhang M. Pulmonary artery sling causing tracheal
stenosis in a neonate. Tex Heart Inst J. 2015;42:504---5.
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Congenital anomalies of the pulmonary arteries: findings on computed tomography 217
14. Singh U, Singh K, Aditi Singh P, Aneja P. Idiopathic pul-
monary artery aneursym. Indian J Chest Dis Allied Sci. 2014;56:
45---7.
15. Martinez-Quintana E, Rodriguez-Gonzalez F, Gomez-Guindal JA,
Junquera-Rionda P. Idiopathic pulmonary artery aneurysm in a
young woman. Radiologia. 2010;52:255---7.
16. Holzinger C, Podesser BK, Lomoschitz F, Kassal H. Idiopathic
pulmonary artery aneurysm. J Card Surg. 2011;26:154---6.
17. Kastler B, Livolsi A, Germain P, Bernard Y, Michalakis D, Rodiere
E, et al. Value of MRI in the evaluation of congenital anomalies
of the heart and great vessels. J Radiol. 2004;85:1821---50.
18. Bailliard FAR. Tetralogy of Fallot. Orphanet J Rare Dis.
2009;4:1---10.
19. Allen H, Clark E, Gutgessell H. Moss and Adam’s Heart disease
in infants, children and adolescents. Philadelphia: Lippincott
Williams & Wilkins; 2001.
20. Ahmed S, Johnson PT, Fishman EK, Zimmerman SL. Role of mul-
tidetector CT in assessment of repaired tetralogy of Fallot.
Radiographics. 2013;33:1023---36.
21. Norton KI, Tong C, Glass RB, Nielsen JC. Cardiac MR imaging
assessment following tetralogy of fallot repair. Radiographics.
2006;26:197---211.
Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from http://www.elsevier.es, day 09/03/2018. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.