Congenital Anomalies of the Central Nervous System
77
Congenital Anomalies of the Central Nervous System
-
Upload
felix-combs -
Category
Documents
-
view
27 -
download
0
description
Congenital Anomalies of the Central Nervous System. Major Events in Human Brain Development and Peak Times of Occurrence (Menkes). Gestational Age in Months. Postnatal. 1. 2. 3. 5. 4. 6. 7. 8. 9. Neurulation (3 – 4 wks). Neural tube Brain & Spinal cord Neural crest PNS & - PowerPoint PPT Presentation
Transcript of Congenital Anomalies of the Central Nervous System

Congenital Anomalies of the Central Nervous
System
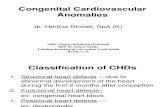
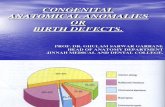
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neurulation(3 – 4 wks)
Prosencephalic(2 – 3 mos)
NeuronalProliferation(3 – 4 mos)
NeuronalMigration(3 – 5 mos)
Organization(5 – postnatal years)
Myelination(Birth – Postnatal yrs)
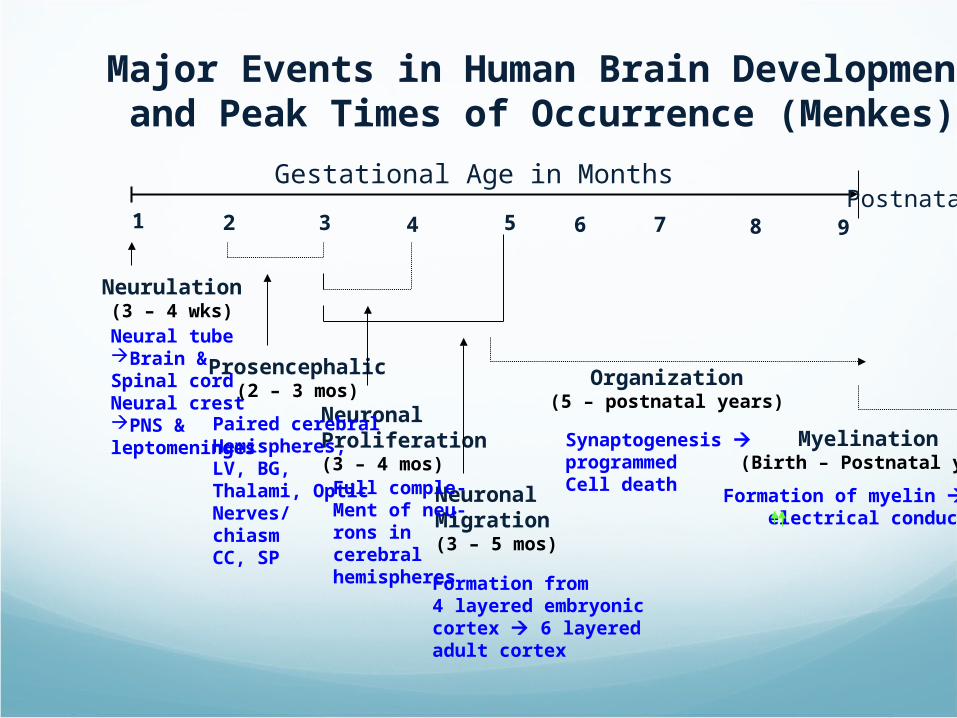
Major Events in Human Brain Developmentand Peak Times of Occurrence (Menkes)
Neural tubeBrain &Spinal cordNeural crestPNS &leptomeninges
Paired cerebralHemispheres,LV, BG,Thalami, OpticNerves/chiasmCC, SP
Full comple-Ment of neu-rons in cerebralhemispheres Formation from
4 layered embryoniccortex 6 layeredadult cortex
Synaptogenesis programmedCell death
Formation of myelin electrical conduction

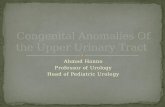
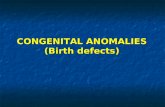
Transverse sections ofembryos at Different ages to show theDev’t ofthe spinal cord
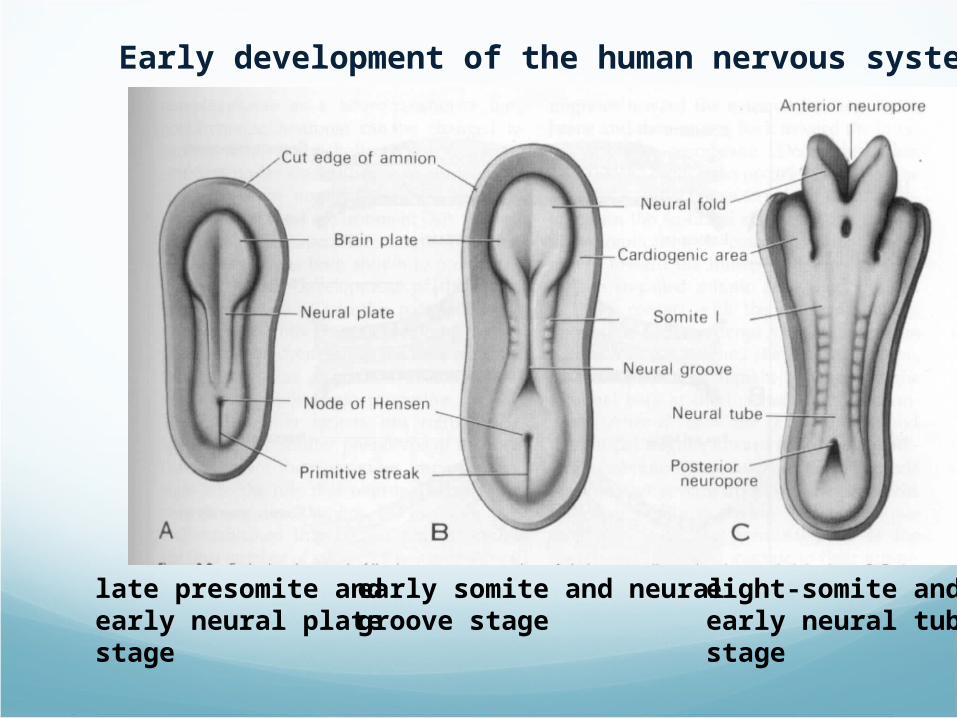
Early development of the human nervous system
late presomite andearly neural plate stage
early somite and neuralgroove stage
eight-somite andearly neural tubestage
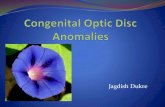
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neurulation(3 – 4 wks)
Prosencephalic(2 – 3 mos)
NeuronalProliferation(3 – 4 mos)
NeuronalMigration
(3 – 5 mos)
Organization(5 – postnatal years)
Myelination(Birth – Postnatal yrs)
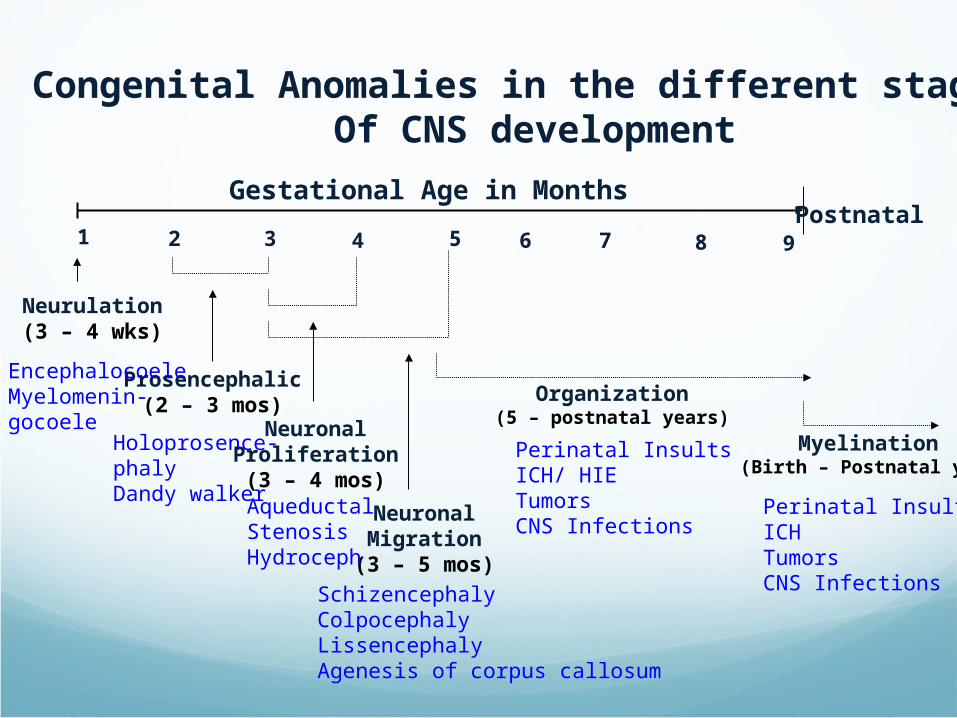
Congenital Anomalies in the different stages Of CNS development
EncephalocoeleMyelomenin-gocoele
Holoprosence-phalyDandy walker Aqueductal
StenosisHydroceph
SchizencephalyColpocephalyLissencephalyAgenesis of corpus callosum
Perinatal InsultsICH/ HIETumorsCNS Infections
Perinatal InsultsICHTumorsCNS Infections

Neural Tube Defects (Posterior Midline Defects/Dysraphism)
Results from failure of the neural tube to close spontaneously between the 3rd-4th week of in utero development
Possible etiologic factors:RadiationDrugsMalnutrition ChemicalsGenetic determinants (mutations in folate-
responsive and folate-dependent pathways)

Neural Tube Defects Spina bifida occulta
Meningocoele/ Myelomeningocoele
Encephalocoele
Anencephaly
Dermal sinus
Tethered cord
Syringomyelia
Diastematomyelia
Neural Tube DefectsDiagnostic tool:
Failure of closure of the neural tube allows excretion of fetal substances (AFP, acetylcholinesterase) into the amniotic fluid
Prenatal screening of maternal serum for AFP during 16-18 week AOG
AF AFP obtained between 15-20 weeks’ gestation is most specific
Rostral end of the NT closes on the 23rd day and the caudal neuropore closes by the 27th day of development
Neural Tube Defects and FA
Maternal periconceptional use of folic acid supplementation reduces the incidence of NT defects by at least 50%
US: recommends all women of childbearing age take 0.4 mg of folic acid daily, and women with previous pregnancy of NT defect should be treated with 4 mg of folic acid beginning one month before pregnancy is planned, until at least the 12th week AOG when neurulation is complete
Fortification of flour, pasta, rice and cornmeal with 0.15 mg of folic acid/100 g was mandated in the US and Canada in 1998



Spina Bifida OccultaMidline defect of the vertebral bodies without
protrusion of the SC or meninges
May be asymptomatic without neuro signs
In some, patches of hair, lipoma, discoloration of skin or dermal sinus may be present

Spina Bifida OccultaSpine x-ray: defect in closure of the posterior
vertebral arches and laminae, usually in L5 and S1
May be associated with syringomyelia, diastematomyelia, and tethered cord
Recurrent meningitis of occult origin should prompt careful exam for dermal sinus tract

1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neurulation Period
S. N., 2 mos old, female
Marked obstructive Hydrocephalussecondary to ARNOLD CHIARI II

Meningocoele
Formed when the meninges herniate through a defect in the posterior vertebral arches
SC may be normal, or may present with tethering, syringomyelia, or diastematomyelia
A fluctuant mass that may transilluminate along the vertebral column

MeningocoeleDxtic: plain x-ray, utz, MRI for the spine, CT of
the head to R/O HCP
Txtic: Asymptomatic children with N neuro findings and full-thickness skin may have surgery delayed.
Patients with leaking CSF or a thin skin covering should undergo immediate repair to prevent meningitis.

MeningocoeleAnterior meningocoele may project into the
pelvis through a defect in the sacrum causing symptoms of constipation and bladder dysfunction
Female patients may have associated anomalies of the genital tract (rectovaginal fistula, vaginal septa)
Dxtic: plain x-ray, CT, MRI
MyelomeningocoeleMost severe form of dysraphism involving the
vertebral column with an incidence of 1/4000 LB
Risk of recurrence after one affected child increases to 3-4% and increases to ~10% with 2 previous abnormal pregnancies
Certain drugs that antagonize folic acid (TMP, AEDs: CBZ, PHY, Pb, primidone) increase the risk of myelomeningocoele
Valproic acid cause NT defects in ~1-2% of pregnancies

MyelomeningocoeleMay be located anywhere along the
neuraxis but the LS region accounts for 75% of the cases
Extent and degree of the neuro deficit depend on the location
CM: flaccid paralysis, absent DTRs, sensory deficit below the affected level, postural abn of the LE (clubfeet, subluxation of the hips), constant urinary dribbling and a relaxed anal sphincter

Myelomeningocoele
HCP in association with a type II Chiari defect develops in at least 80% with myelomeningocoele
Infants with HCP and Chiari II develop symptoms of hindbrain dysfunction: difficulty feeding, choking, stridor, apnea, VC paralysis, pooling of secretions, spasticity of UEs
Chiari crisis is due to downward herniation of the medulla and cerebellar tonsils
MyelomeningocoeleRequires a multidisciplinary approach:
surgeon, therapist, pediatrician
Surgery: repair and shunting; orthopedic procedure, urologic evaluation
GUT: regular catheterization to prevent UTI and reflux leading to PN and hydronephrosis, urine cult, serum elec, creatinine, renal scan, IV pyelogram, Utz
Rehab: functional ambulation (sacral or LS lesion)
MyelomeningocoelePrognosis:
MR- 10-15% Most deaths occur before age 4 years70% have normal intelligence, but learning
problems and seizure disorders are commonHistory of meningitis or ventriculitis adversely
affect the ultimate IQ
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neurulation Period
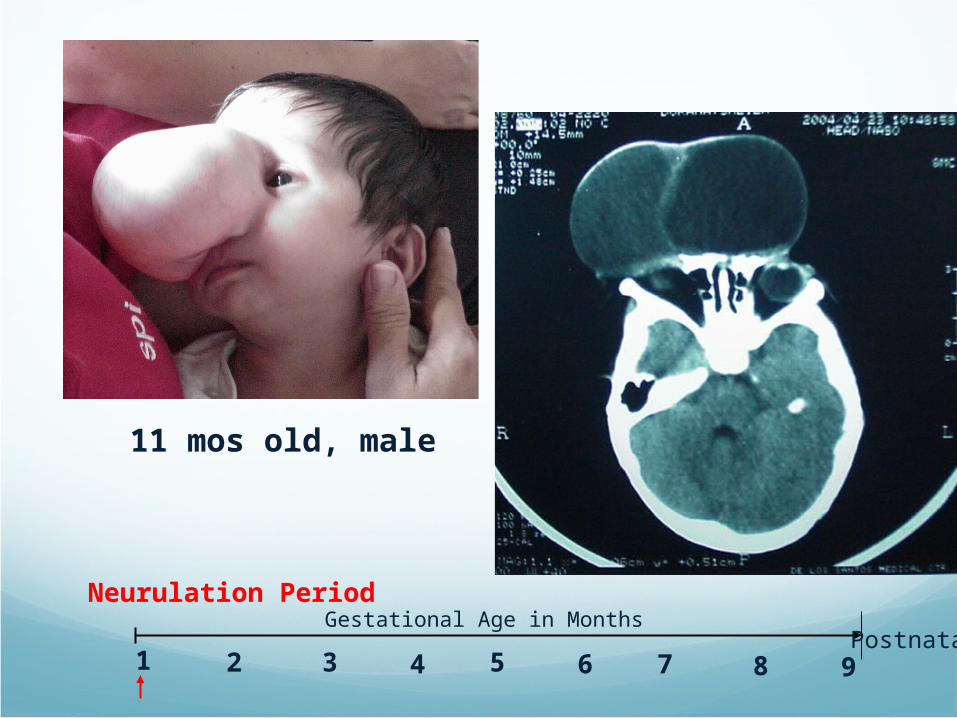
11 mos old, male
EncephalocoeleCranium meningocoele: CSF-filled
meningeal sac only
Cranial encephalocoele: contains the sac plus cerebral cortex, cerebellum or portions of the brainstem usually with abnormalities
Usually occurs in the occipital region or below the inion, although in some countries, frontal or nasofrontal encephalocoeles are more prominent

EncephalocoeleDxtic:
Plain x-ray of the skull and cervical spineCranial utzIn utero: AFP, biparietal diameter
Prognosis:Encephalocoele- at risk for visual problems,
microcephaly, MR, seizuresMeckel-Gruber syndrome: AR condition,
occipital encephalocoele, cleft lip or palate, microcephaly, microphthalmia, abnormal genitalia, polycystic kidneys, and polydactyly

AnencephalyLarge defect of the calvarium, meninges, and
scalp associated with a rudimentary brain which results from failure of closure of the rostral neuropore
Primitive brain consists of portions of connective tissue, vessels and neuroglia
The cerebral and cerebellar hemispheres are usually absent, and only a residue of the brainstem can be identified; the pituitary gland is hypoplastic, and the SC pyramidal tracts are absent
AnencephalyAssociated anomalies: folding of the ears, cleft
palate, congenital heart defects (10-20%)
Die within several days of birth
Frequency: 1/1000 LB
Recurrence risk: 4% and increases to 10% with 2 previously affected pregnancies
Monitoring of succeeding pregnancies: amniocentesis, AFP levels, Utz between 14-16th week of AOG
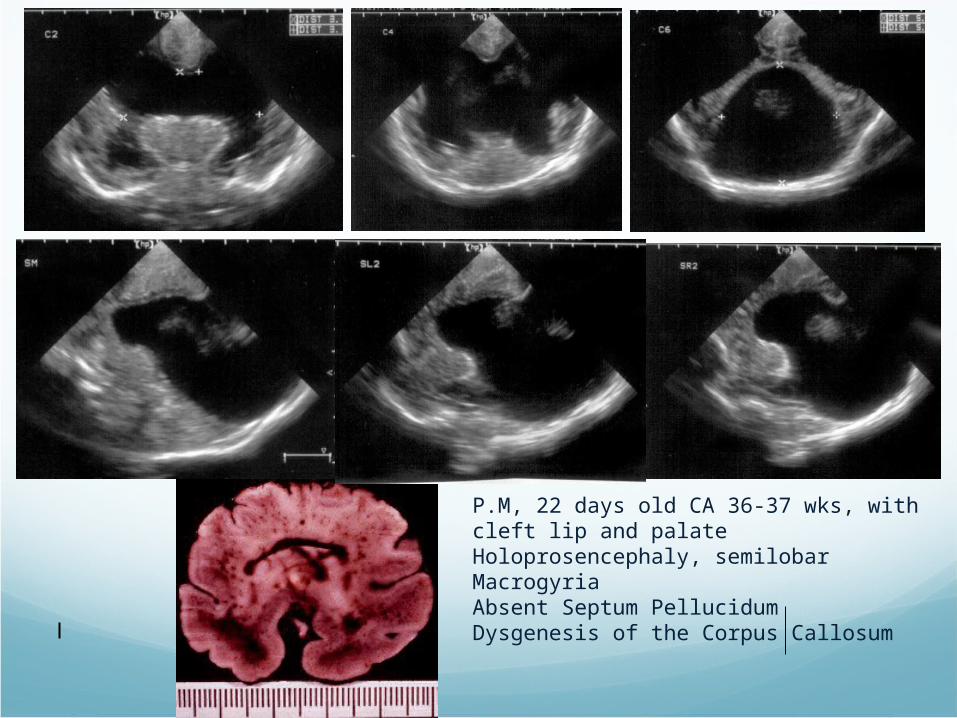
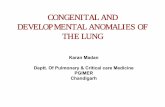
P.M, 22 days old CA 36-37 wks, with cleft lip and palateHoloprosencephaly, semilobarMacrogyriaAbsent Septum PellucidumDysgenesis of the Corpus Callosum
Anterior Midline Defects (Holoprosencephaly)
Alobar, semilobar, lobar, middle interhemispheric fusion variant
Alobar holoprosencephaly: single midline ventricular cavity, absent falx, inferior frontal and temporal regions are absent, only the primary motor and sensory cortex may be present
Failure of cleavage of the hemispheres which occur at 33 days AOG
Defective expression of the gene Sonic hedgehog (Shh) at 7q
Associated with maternal diabetes
HoloprosencephalyClinically, present with profound MR, Szs,
rigidity, apnea and temperature imbalance; HCP can develop with aqueductal obstruction; endocrine disorders can present with hypothalamic or pituitary malformations
Facial abnormalities include cyclopia, cebocephaly, and premaxillary agenesis
Dxtic: facial x-ray to show deformed anterior craniobasal bones, cytogenetics, MRI.
EEG, VER, ABR are generally abnormal.

Disorders of Neuronal Migration
Migrating neurons attach to the radial glial fiber and reach their predetermined sites to form the six-layered cerebral cortex
Small heterotopias- little or no CM
Lissencephaly
Schizencephaly severe MR

Lissencephaly(Agyria)Absence of the cerebral convolutions and a poorly
formed sylvian fissure (3-4 month fetal brain), numerous gray heterotopia
Present with failure to thrive, microcephaly, marked developmental delay, severe seizure disorder, hypoplasia of the optic nerve, microphthalmia
Miller-Dieker syndrome: prominent forehead, bitemporal hollowing, anteverted nostrils, prominent upper lip, micrognathia (90% with chromosomal deletions of 17p13.3- lissencephaly I gene)

Lissencephaly

SchizencephalyUnilateral or bilateral clefts within the
cerebral hemispheres due to an abnormality of morphogenesis
The cleft may be fused or unfused, and is usually surrounded by abnormal brain, microgyria
Present with severe MR, intractable Szs, microcephaly, spastic quadriplegia when clefts are bilateral
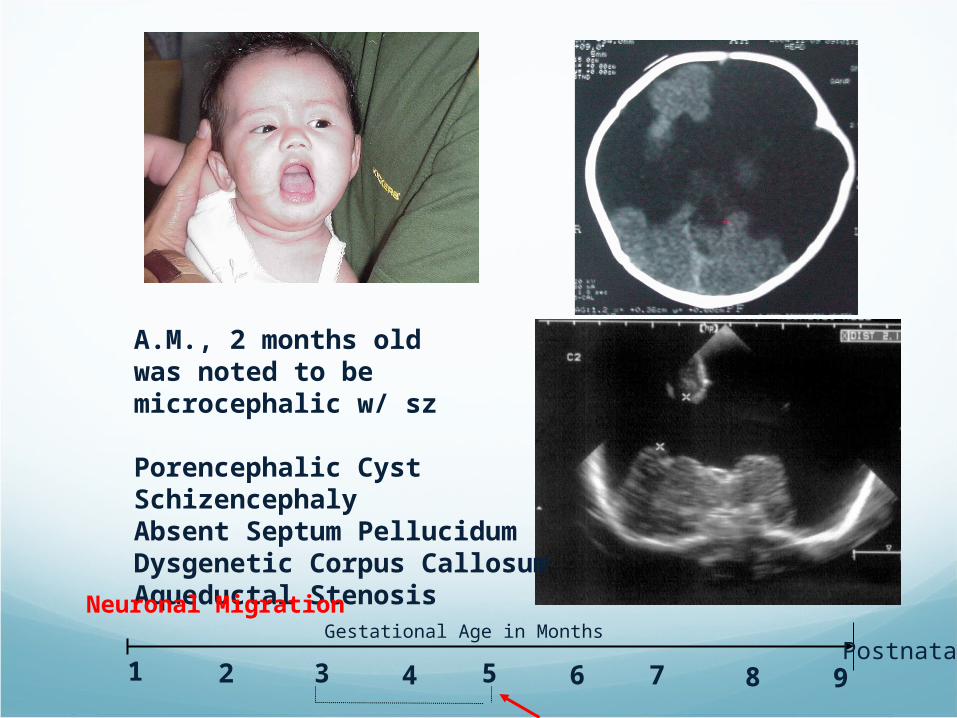
A.M., 2 months oldwas noted to be microcephalic w/ sz
Porencephalic CystSchizencephalyAbsent Septum PellucidumDysgenetic Corpus CallosumAqueductal Stenosis
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neuronal Migration

PorencephalyCysts or cavities within the brain that may or
may not communicate with the ventricular system, resulting from vascular or infectious results during late fetal or early infantile life
Usually present with hemiparesis and focal seizures during the 1st year of life

Porencephaly

Agenesis of the Corpus Callosum
Results from an insult to the commissural plate during embryogenesis
When it appears as an isolated phenomenon, the patient may be normal; but those with associated migration defects (heterotopia, microgyria, pachygyria) may present with MR, microcephaly, hemiparesis, diplegia and seizures
CT/MRI: widely separated frontal horns with an abnormally high position of the 3rd ventricle

Agenesis of the Corpus Callosum

Agenesis of the Corpus Callosum
Aicardi SyndromePatients are almost all females (may be lethal in
males)Characterized by severe MR, intractable seizures
with onset between birth and 4 mons of age, and chorioretinal lacunae. Hemivertebrae and costovertebral anomalies are common.
EEG: independent activity from both hemispheres as a result of the absence of the CC

Agenesis of the Cranial Nerves
II, III(Congenital ptosis), V, VIII, IX, X, XI, XII
Marcus Gunn phenomenon: sucking jaw movements causing simultaneous eyelid blinking
Mobius syndrome: absence of the VII nerve resulting in bilateral facial weakness, associated with abducens nerve paralysis. Result in feeding difficulties due to poor suck. Immobile or dull facies may be misinterpreted as MR.
MicrocephalyHC >3 SDs below the mean for age/sex
Primary (genetic) Microcephaly
Secondary (non-genetic) Microcephaly
Dxtic: mother’s serum phenylalanine, karyotype (abnormal facies, short stature, associated congenital abn), CT/MRI (TORCH), fasting plasma and urine amino acid analysis, serum NH4.

HydrocephalusCSF production: 20 ml/hr
Total CSF volume: 50 ml (infant)
150 ml (adult)
Normal IV pressure: 180 mm H2O
Communicating HydrocephalusNoncommunicating or obstructive hydrocephalus

HydrocephalusObstructive HCP
Aqueductal stenosis- x-linked recessive trait, associated with spina bifida occulta, NF
Aqueductal gliosis- 20 to neonatal meningitis or SAH in PT, intrauterine viral infections, mumps meningoencephalitis
Vein of Galen malformationSpace occupying lesions in the posterior fossa

C. V., 1 month oldAt 2 weeks of age wasnoted to have a fastenlarging head
Aqueductal Stenosis
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Neuronal Proliferation

R.C., 5 months oldcame in because ofenlarge head size
Vein of Galen Malformation

HydrocephalusInfant: increasing HC, open and bulging AF,
dilated scalp veins, broad forehead, setting-sun eye signs, hyperreflexia, spasticity, clonus, bilateral Babinski sign
Child: irritability, lethargy, poor appetite, vomiting, headache. Gradual personality change and deterioration in academic performance
Serial HC monitoring, Macewen sign
Papilledema
Causes of HydrocephalusChiari malformation
Type I: medulla is displaced caudally into the spinal canal, inferior cerebellar hemispheres is herniated through the foramen magnum
Type II: medulla, cerebellum and part or all of the 4th ventricle are displaced into the spinal canal, with associated obst hcp and LS spina bifida
Type III: features of type I or II plus the entire cerebellum is herniated through the foramen magnum with a cervical spina bifida cystica
Type IV: cerebellar hypoplasia with other malformations of the posterior fossa

Chiari Malformation
Type I Type II
HydrocephalusCause: Dandy-Walker malformation- cystic
expansion of the 4th ventricle in the posterior fossa
Dxtic: Plain skull x-ray: separation of sutures, erosion of the
post clinoids, beaten-silver appearanceUTZ/CT/MRI
DDx: thickened cranium, metabolic and degenerative disorders producing megalencephaly, gigantism, NF, familial megalencephaly
Management: depends on the cause
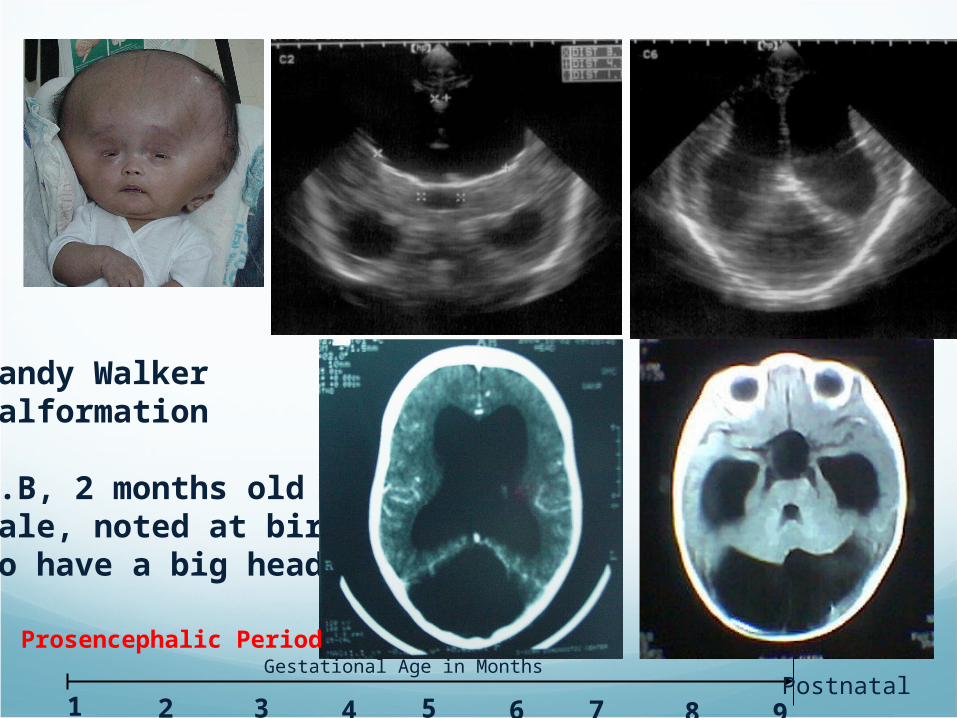
Dandy WalkerMalformation
R.B, 2 months oldmale, noted at birthto have a big head
1 2 3 4 5 6 7 8 9
Gestational Age in MonthsPostnatal
Prosencephalic Period
CraniosynostosisPremature closure of the cranial sutures
Primary craniosynostosis- closure of one or more sutures probably due to abnormal development of the base of the skull
Secondary caniosynostosis- results from failure of brain growth and expansion

CraniosynostosisScaphocephaly- premature closure of the
sagittal suture producing a long and narrow skull, broad forehead, prominent occiput and absent AF
Frontal plagiocephaly- premature fusion of a coronal and sphenofrontal suture resulting in unilateral flattening of the forehead, elevation of the ipsilateral orbit and eyebrow, and an ipsilateral prominent ear

CraniosynostosisType Suture with premature
closure
Occipital plagiocephaly Lambdoid suture
Trigonocephaly Metopic suture
Turricephaly Coronal and sphenofrontal and frontoethmoidal
Kleeblattschadel deformity
Cloverleaf shaped skull
CraniosynostosisCrouzon syndrome: due to bilateral closure of the
coronal sutures, char. by underdeveloped orbits, ocular proptosis, hypoplasia of the maxilla and orbital hypertelorism
Apert syndrome: Premature fusion of multiple sutures resulting in asymmetric facies, syndactyly, progressive calcification and fusion of the bones of the hands, feet and cervical spine
Carpenter syndrome
Chotzen syndrome
Pfeiffer syndrome
CraniosynostosisMutations of the fibroblast growth factor
receptor (FGFR) gene familyPfeiffer syndrome- FGFR1 on ch8Apert syndrome- FGFR2 geneIdentical mutations of FGFR2 gene may result in
both Pfeiffer and Crouzon phenotype
Involvement of one suture rarely causes neuro deficit. Surg is indicated for cosmetic purposes.
Craniectomy is mandatory for mgt of increased ICP
All of the following statements about spina bifida cystica are true except:
A. it is often associated with HCP
B. it is fatal if not treated within 24 hrs.
C. It may be diagnosed in utero with UTZ
D. It can cause urologic problems
E. It requires orthopedic management

NEUROMUSCULAR DISORDERS

Neuromuscular DisordersDisorder of the motor unit
Motor neuron in the brainstem or ventral horn of the spinal cord
Axon -- peripheral nerve
Neuromuscular junction
All muscle fibers innervated by a single motor neuron
Work-up of the child with a suspected muscular dystrophy or
myopathy
A. MRI
B. ECG
C. Nerve conduction velocity or NCV study
D. Sural nerve biopsy

Distinguishing Features of Disorders of the Motor System
LOCUS OF LOCUS OF LESSONLESSON
FACEFACE ARMS ARMS LEGSLEGS PROXIMALPROXIMAL-DISTAL-DISTAL
DEEP DEEP TENDON TENDON
REFLEXESREFLEXES
ELECTRO-ELECTRO-MYOGRAPHYMYOGRAPHY
MUSCLE BIOPSYMUSCLE BIOPSY OTHEROTHER
CENTRALCENTRAL 0 0 ++ ++ > OR => OR = NORMAL NORMAL OR UPOR UP
NORMALNORMAL NORMALNORMAL SEIZURES, SEIZURES, HEMIPARESIS, AND HEMIPARESIS, AND DELAYED DELAYED DEVELOPMENTDEVELOPMENT
ANTERIOR ANTERIOR HORN CELL HORN CELL
LATELATE ++++++++ ++++++++ > OR => OR = 00 FASCICULATIONS FASCICULATIONS AND FIBRILLATIONSAND FIBRILLATIONS
DENERVATION DENERVATION PATTERNPATTERN
FASICULATIONS FASICULATIONS (TONGUE)(TONGUE)
PERIPHERAL PERIPHERAL NERVENERVE
00 ++++++ ++++++ << DOWNDOWN FIBRILLATIONS FIBRILLATIONS DENERVATION DENERVATION PATTERNPATTERN
SENSORY DEFICIT, SENSORY DEFICIT, ELEVATED ELEVATED CEREBROSAL FLUID CEREBROSAL FLUID PROTEIN, DEPRESSED PROTEIN, DEPRESSED NERVE CONDUCTION NERVE CONDUCTION VELOCITY, ABNORMAL VELOCITY, ABNORMAL NERVE BIOPSYNERVE BIOPSY
NEURO-NEURO-
MUSCULAR MUSCULAR JUNCTIONJUNCTION
++++++ ++++++ ++++++ == NORMALNORMAL DECREMENTAL DECREMENTAL RESPONSE RESPONSE (MYATHENIA); (MYATHENIA); INCREMENTAL INCREMENTAL RESPONSE AND RESPONSE AND BSAP (BOTULISM)BSAP (BOTULISM)
NORMALNORMAL RESPONSE TO RESPONSE TO NEOSTIGMINE OR NEOSTIGMINE OR ENDOPHONIUM ENDOPHONIUM (MYASTHERIA); (MYASTHERIA); CONSTIPATION AND CONSTIPATION AND FIXED PUPILS FIXED PUPILS (BOTULISM)(BOTULISM)
MUSCLEMUSCLE VARIABLEVARIABLE
( + TO +++( + TO ++++)+)
++++ ++ >> DOWNDOWN SHORT SHORT DURATION,SMALL DURATION,SMALL AMPLITUDE MOTOR AMPLITUDE MOTOR UNIT POTENTIALS UNIT POTENTIALS AND MYOPATHIC AND MYOPATHIC POLYPHASIC POLYPHASIC POTENTIALS POTENTIALS
MYOPATHIC MYOPATHIC PATTERNPATTERN
ELEVATED MUSCLE ELEVATED MUSCLE ENZYME LEVELS ENZYME LEVELS (VARIABLE)(VARIABLE)
DEVELOPMENTAL DISORDERS OF MUSCLE
Myotubular Myopathy
Congenital Muscle Fiber–Type Disproportion (CMFTD)
Nemaline Rod Myopathy
Central Core Disease and Minicore Myopathy
Muscular Dystrophies
Primary Myopathy
Genetic Basis
Progressive Cause
Degeneration and death of muscle fibers

Duchenne and Becker Muscular Dystrophies
Most common hereditary
neuromuscular disease
Progressive weakness, hypertrophy of calves, intellectual impairment, proliferation of connective tissue in muscle
Incidence 1 : 3,600
X-linked recessive M trait
Xp21 gene locus
Duchene Muscular Dystrophy Clinical
Features
Progressive hip girdle weakness
Gowers sign
Hip waddle
Progressive weakness from early childhood
Pseudohypertrophy of calves and wasting of thigh muscles
Distal muscle function preserved
Intact extraocular muscle,anal and urethral sphincter
Intellectual impairment
Duchenne Muscular Dystrophy LABORATORY FINDINGS:
Electromyography – Myopathic features (no denervation)
Cardiac Evaluation – ECG, Echocardiography
Blood PCR
Muscle Biopsy – diagnostic
(Endomysial connective tissue proliferation, scattered degenerating and regenerating microfibers)
Most myofibers express no dystrophin.
Duchenne Muscular Dystrophy
TREATMENT:
No medical cure or way of slowing it’s progression
Improve quality of life
> good nutritional state
> treat pulmonary infections
> cardiac decompensation
> physiotherapy – may delay contractions
> steriods – may decrease rate of apoptosin

Disorders Of Neuromuscular Transmission and Of Motor Neurons
Myasthenia Gravis
2004 international Classification of Headache
Disorders MIGRAINE
Migraine without aura
Migraine with aura
Typical aura with migraine headache
Typical migraine with nonmigraine headache
Typical aura without headache
Familial hemiplegic migraine
Sporadic hemiplegic migraine
Basiliar-type migraine
Childhood periodic symptoms that are commonly precursors of migraine
Cyclic vomiting
Abdominal migraine
Benign paroxysmal vertigo of childhood
Retinal migraine
Complications of migraine
Chronic migraine
Status migraine
Persistent aura without infarction
Migrainous infarction
Probable migraine

Indications for Neuroimaging in a child with headaches
Abnormal neurologic signs
Recent school failure, behavioral change, fall-off linear growth rate
Headache awareness child during sleep, early morning headache, with increase in frequency and severity
Periodic headaches and seizures coincide, especially if seizure has a focal onset
Migraine and seizure occur in the same episode, and vascular symptoms precede the seizure (20-50 % of tumor or arteriovenous malformation)
Cluster headaches in child; any child < 5-6 yr whose principal complaint is a headache
Focal neurologic symptoms or signs developing during a headache (i.e. complicated migraine)
Focal neurologic symptoms or signs (except classic visual symptoms of migraine) develop during the aura, with fixed laterality; focal signs of the aura persisting or recurring in the headache phase.
Visual graying-out occuring at the peak of a headache instead of the aura
Brief cough headache in a child or adolescent

Paroxysmal Disorders of the Neonatal Period
PAROXYSMAL NONEPILEPTIFORM DISORDERS
Jitterness
Benign neonatal sleep myoclonus
ACUTE SYMPTOMATIC SEIZURES AND OCCASIONAL SEIZURES
Hypoxic-Ischemic encephalopathy
Intraventricular hemorrhage
Acute metabolic disorders
Sepsis-meningitis

Paroxysmal Disorders of the Neonatal Period
EPILEPTIC SYNDROMES
Benign idiopathic neonatal convulsions
Familial
Symptomatic focal epilepsy
Brain tumor
Malformations of cortical development
Inherited metabolic disease; mitochondrial disorders
Early-onset generalized epileptic syndromes with encephalopathy
Early myoclonic encephalopathy
Early infantile encephalopathic epilepsy

Nonepileptic Paroxysmal Disorders
NEONATE
Jitteriness
Benign neonatal sleep myoclonus
INFANT
Infantile syncope
Cyanotic breath-holding spells
Pallid syncope
Sleep disorders
head banging

Nonepileptic Paroxysmal Disorders
CHILDREN
Breath-holding spells
Migraine and migraine equivalents,recurrent abdominal pain, cyclic vomitting
Tic
Witholding, constipation
Daydreaming, staring spells
Sleep Disorders Head bangingSomnambulism

Nonepileptic Paroxysmal Disorders
ADOLESECENTS
Syncope
Migraine
Daydreaming
Sleep disordersNocturnal myoclonus, hypnic jerks NarcolepsySomnambulism