Congenital Anomalies Of Spine And Spinal Cord
92
IMAGING OF CONGENITAL ANOMALIES OF SPINE AND SPINAL CORD Dr Roshan Valentine PG Resident Radiodiagnosis St Johns Medical College
-
Upload
roshan-valentine -
Category
Health & Medicine
-
view
682 -
download
0
Transcript of Congenital Anomalies Of Spine And Spinal Cord

IMAGING OF CONGENITAL
ANOMALIES OF SPINE AND SPINAL
CORDDr Roshan ValentinePG ResidentRadiodiagnosisSt Johns Medical College

In the spine, the most common congenital lesions presenting to medical attention are the diverse forms of spinal dysraphism diverse forms of caudal spinal anomalies

IMAGING MODALITIES
MRI :IOC PLAIN RADIOGRAPH: bony defects ,
widened spinal canal , scoliosis, segmentation anomalies like block vertebrae , butterfly vertebrae , bony spur (diastematomyelia)
USG: antenatal Dx – open widened neural arch , meningomyelocele sac , hydrocephalus , contents of sac
CT : bony spur

Spinal Cord Development Summarized in three basic embryologic stages
1. The first stage : Gastrulation (the 2 or 3 week) conversion of the embryonic disk from a bilaminar
disk to a trilaminar disk.2. The second stage : primary neurulation (weeks 3–
4) the notochord and overlying ectoderm interact to form the neural plate. The neural plate bends and folds to form the neural tube, which then closes bidirectional in a zipperlike manner
3. The final stage : secondary neurulation (weeks 5–6), a secondary neural tube is formed by the caudal cell mass. The secondary neural tube is initially solid and subsequently cavitation, eventually forming the tip of the conus medullaris and filum terminale by a process called retrogressive differentiation.

GASTRULATION

Primary neurulation.
Formation of the Neural Plate
Shaping of the Neural Plate
Bending of the Neural Plate
Fusion



Canalization and retrogressive differentiation (synonym: secondary neurulation). Diagrammatic representationof proposed embryogenesis.

Classification of spinal dysraphisms


OPEN SPINAL DYSRAPHISM
Open spinal dysraphism (OSD)characterized by exposure of nervous tissue/covering meninges through a congenital Defect
Almost 99% are myelomeningocelesVariable degree of sensorimotor
deficits,bowel and bladder dysfunctionAll patients with OSD have Chiari IIRole of MRI: anatomic
characterization;presurgical evaluation; identification of cord splitting when present

OPEN SPINAL DYSRAPHISM (OSD)
MYELOCELE AND MYELOMENINGOCELEEmbryological defect : Complete
nondisjunction of cutaneous ectoderm from neural ectoderm.
Neural folds do not fuse in the midline to form neural tube.
Remain in continuity with the cutaneous ectoderm.
This exposed part of the spinal cord is NEURAL PLACODE.

MC location : Lumbosacral region >thoraco-lumbar region
Imaging usually not done(clinically obvious)
Surgical emergencyMRI if indicated to look for
associated anomaliesHydromyeliaChiari II malformationhydrocephalus

The main differentiating
feature between a myelomeningocele and myelocele is the position of the neural placode relative to the skin surface
The neural placode protrudes above the skin surface with a myelomeningocele and is flush with the skin surface with a myelocele


OPEN SPINAL DYSRAPHISMSMYELOMENINGOCELE AND MYELOCELE
HEMIMYELOMENINGOCELE AND HEMIMYELOCELE
Myelomeningoceles and myeloceles are caused by defective closure of the primary neural tube
Exposure of the neural placode through a midline skin defect on the back.
Myelomeningoceles account for more than 98% of open spinal dysraphisms
Myeloceles are rare.
Hemimyelomeningoceles and hemimyeloceles can also occur but are extremely rare . These conditions occur when a myelomeningocele or myelocele is associated with diastematomyelia (cord splitting) and one hemicord fails to neurulate.


Myelomeningocele. Axial schematic of myelomeningocele shows neural placode (star) protruding above skin surface due to expansion of underlying subarachnoid space (arrow).
Myelomeningocele. Axial T2-weighted MR image Myelomeningocele. Sagittal
T2-weighted MR image).

Myelocele. Axial schematic of myelocele shows neural placode (arrow) flush with skin surface.
Myelocele. Axial T2-weighted MR image in 1-day-old girl shows exposed neural placode (arrow) that is flush with skin surface, consistent with myelocele. There is no expansion of underlying subarachnoid space

LUMBAR MENINGOCELE

Chiari Malformations


Sagittal T1-weighted image shows caudal tonsillar ectopia (arrow).The posterior fossa is small
Axial T1-weighed image shows crowding of the foramen magnum due to the presence ofthe tonsils (T) behind the medulla oblongata

Chiari II malformation with hydromyelia

Sagittal images very small posterior cranial fossa and the typical cascade of herniations constitutin the hallmark of the Chiari-II malformation.

CHIARI-III MALFORMATIONChiari II + cephalocele
CHIARI-IV MALFORMATION Severe cerebellar hypoplasia + myelomeningocele

CLOSED SPINAL DYSRAPHISMS

CLOSED SPINAL DYSRAPHISMS WITH A SUBCUTANEOUS MASS
Lipoma with dorsal defectsMyelocystocele(Temrinal or cervical)MeningoceleCervical myelomeningocele

CLOSED SPINAL DYSRAPHISMS WITH A SUBCUTANEOUS MASS
Lipomas with dural defect : Lipomyelocele and lipomyelomeningocele
Embryological defect: nondisjunction

CLOSED SPINAL DYSRAPHISMS WITH A SUBCUTANEOUS MASS
C/F : subcutaneous fatty mass above the gluteal crease
Diff both based on lipoma – placode interface
Lipomyelocele : placode-lipoma interface within spinal canal
Lipomyelomenigocele: Outside the spinal canal due to sub-arachnoid space expansion.



the hairy tuft overlying subcutaneous lipomas

MENINGOCELE : herniation of CSF filled sac lined by dura and arachnoid matter .Spinal cord not located within a
meningocele but may be tethered to the neck of the sac
Posterior meningocele : posterior spina bifida Lumbar/sacral
Anterior : Pre-sacral mostly


ANTERIOR MENINGOCELE

TERMINAL MYELOCYSTOCELE
MYELOCYSTOCELE(NON TERMINAL)
Herniation of large terminal syrinx (syringocele) into a posterior meningocele through a posterior spinal defect is referred to as a terminal .
The terminal syrinx and meningocele components do not usually communicate with each other
Dilated central canal herniates through a posterior spina bifida defect.
covered with skin MC -cervical or
cervicothoracic regions


NON TERMINAL MYELOCYSTOCELE

CLOSED SPINAL DYSRAPHISM

Closed Spinal Dysraphisms Without a Subcutaneous MassSIMPLE DYSRAPHIC STATES
COMPLEX DYSRAPHIC STATES
Intradural lipoma, Filar lipoma, Tight filum terminale,
persistent terminal ventricle
Dermal sinus.
A)Disorders of midline notochordal integrationDorsal neurentericfistula,Neurenteric cyst Diastematomyelia, B)Disorders of notochordal formation, Caudal agenesis Segmental spinal
dysgenesis.

LIPOMA2 Types : Intradural lipoma and Filar lipomaEmbryological defect : focal premature disjunction of
epidermal from neural ectoderm.
INTRADURAL LIPOMALipoma within the dural sacMC : Lumbosacral spinea/w tethered-cord syndrome
FILAR LIPOMAFibrolipomatous thickening of the filum terminale is referred
to as a filar lipoma. MR : T1 hyperintense signal + thickened filum terminale

.Sagittal T1-weighted (A) and sagittal T2-weighted fat-saturated (B) MR images show large intradural lipoma (arrows), which is hyperintense on T1-weighted image and hypointense on T2-weighted fat-saturated image. Lipoma is attached to conus medullaris, which is low lying.
Intradural lipoma
Filar lipoma
, Sagittal (A) and axial (B) T1-weighted MR images I with filar lipoma (arrows), which has characteristic T1 hyperintensity and marked thickening of filum terminale

Plain radiographs show posterior scalloping.Intraspinal lipomas may produce posterior scalloping of vertebral bodies and flattening of the pedicles

SIMPLE DYSRAPHIC STATESTIGHT FILUM TERMINALE
hypertrophy and shortening of the filum terminale .
EMBRYOLOGY : incomplete involution of the distal spinal cord during embryogenesis.
This condition causes tethering of the spinal cord and impaired ascent of the conus medullaris.
The conus medullaris is low lying relative to its normal position, which is usually above the L2–L3 disk level
Sagittal T2-weighted MR image in 12-month-old boy shows tight filum terminale, characterized by thickening and shortening of filum terminale (black arrow) with low-lying conus medullaris. Incidental cross-fused renal ectopia (white arrow) is also present.


Simple dysraphic statesPERSISTENT TERMINAL VENTRICLE Persistence of a small,
ependymal lined cavity within the conus medullaris.
It is the widest part of the central canal at the level of conus
point of union between the portion of the central canal made by neurulation and the portion made by canalization of the caudal cell mass
Imaging : Location – above the filum terminale and lack of contrast enhancment
Persistent terminal ventricle.A and B, Sagittal T2-weighted (A) and sagittal T1-weighted contrast-enhanced (B) MR images in 12-month-old boy show persistent terminal ventricle as cystic structure (arrows) at inferior aspect of conus medullaris, which does not enhanc

SIMPLE DYSRAPHIC STATES
DERMAL SINUS Epithelial lined fistula
that connects neural tissue or meninges to the skin surface.
If the superficial ectoderm fails to separate from the neural ectoderm at one point.
MC : Lumbo sacral region
C/F : midline dimple , hairy naevus , hyperpigmented patch /capillary hemangioma
Infectious complication if not surgically treated

DERMAL SINUS

COMPLEX DYSRAPHIC STATES
DISORDERS OF MIDLINE NOTOCHORDAL INTEGRATION
DISORDERS OF NOTOCHORDAL FORMATION
Dorsal enteric fistula,Neurenteric cystDiastematomyelia,
Caudal agenesis Segmental spinal dysgenesis.

DISORDERS OF MIDLINE NOTOCHORDAL INTEGRATION
DORSAL ENTERIC FISTULA Abnormal connection between the
skin surface and bowel.NEURENTERIC CYSTS Localized form of dorsal enteric
fistula Mucin-secreting epithelium (~GI
tract ) lined cystMC : cervico-thoracic spine anterior
to spinal cord

5—Neurenteric cyst in 3-year-old girl

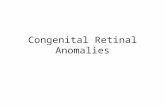
DISORDERS OF MIDLINE NOTOCHORDAL INTEGRATIONDIASTEMATOMYELIASeparation of the spinal cord into two hemicords The two hemicords are usually symmetric, although the
length of separation is variable. Type 1 : Dual Dural-Arachnoid Tubes (Pang Type I) :
the two hemicords are located within individual dural sacs separated by an osseous or cartilaginous septum
In Type 2 : Single Dural-Arachnoid Tube (Pang Type II) :Single dural tube containing two hemicords,
sometimes with an intervening fibrous septumC/F : Hairy tuft , scoliosis , tethered cord syndrome.

TYPE I DIASTEMATOMYELIA
Sagittal T2-weighted MR (A), axial T2-weighted MR (B), and axial CT with bone algorithm (C) images in 6-year-old boy show two dural tubes separated by osseous bridge (arrows), which is characteristic for type 1 diastematomyelia.

TYPE 2 DIASTEMATOMYELIA.
, Sagittal T1-weighted (A), coronal T1-weighted (B), and axial T2-weighted (C) MR images show splitting of distal cord into two hemicords (white arrows, B and C) within single dural tube, which is characteristic for type 2 diastematomyelia. Incidental filum lipoma (black arrows, A and B) is present as well.

DISORDERS OF NOTOCHORDAL FORMATION
CAUDAL AGENESISTotal or partial agenesis of the spinal
column A/w anal imperforation, genital anomalies,
renal dysplasia or aplasia, pulmonary hypoplasia, or limb abnormalities.
2 TypesType 1 : high position of conus + abrupt
termination of conus medullaris(D11/12)+ sig neuro deficit
Type II : low position(L1) + tethering of conus medullaris

CAUDAL AGENESIS
,

CAUDAL REGRESSION SYNDROME
Partial agenesis of the thoracolumbosacral spine
Imperforate anusMalformed genitaliaBilateral renal dysplasia or aplasiaPulmonary hypoplasiaExtreme external rotation and fusion of the
lower extremities (sirenomelia) Sacral agenesis arises early in gestation,
probably before the 10th week of gestation a/w diabetes mellitus,

CLASSIFICATION OF LUMBOSACRAL AGENESIS
Type I : Total sacral agenesis + some lumbar vertebrae missing
Type II: Total SA + lumbar vertebrae not involved
vertebra, severely shortening transverse pelvic diameter
Type III : Subtotal SA + at least S-1 is present.

Type IV: Hemisacrum IVA Total hemisacrum; all sacral segments
present on one side, but entire opposite side is missing IVB Subtotal hemisacrum, unilateral; all sacral
segments present on one side, only part of opposite side is missing
IVC Subtotal hemisacrum, bilateral; part of each side is missing but to different extentsType V: Coccygeal agenesis VA Total VB Subtotal

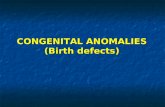
DISORDERS OF NOTOCHORDAL FORMATIONSEGMENTAL SPINAL DYSGENESISSegmental agenesis or
dysgenesis of the thoracic or lumbar spine + segmental abnormality of the spinal cord / nerve roots + congenital paraparesis / paraplegia, + congenital lower limb deformities.
Three-dimensional CT reconstructions can be helpful in showing various vertebral segmentation anomalies
Three-dimensional CT reconstruction image (A) in 4-year-old girl and schematic illustration (B) show multiple segmentation anomalies in lumbar spine (superior to inferior beginning at level of arrow): partial sagittal partition, butterfly vertebra, hemivertebra, tripedicular vertebra, and widely separated butterfly vertebra

DEVELOPMENT OF VERTEBRAL COLUMN




VERTEBRAL COLUMN
Formed form the sclerotome of somitesSclerotome converts to loose mesenchymeIt surrounds the notochord.Extend to either side of neural tube and
surrounds itLateral extension to form transverse processVentrally in the body wall to form ribsNotochord disappears in the region of
vertebral body. In the region of the vertebral discs , it
expands and forms nucleus pulposus

STAGE OF CHONDRIFICATION 6th week2 centers of chondrification in each Centrum appearFuse together at the end of embryonic
period (8th week) form cartilaginous centrum
– Centers of chondrification appear in neural arches and fuse with each other and centrum
– Chondrification spreads until a cartilaginous vertebral column formed

STAGES OF OSSIFICATION
Comprises of 2 stages:1. primary ossification center2. secondary ossification center
Primary ossification center at the end of 8th week.
3 ossification centers are present by the end of embryonic period
one in the centrum one for each neural arch

Bony halves of the vertebral arch fuse together
during the first 3 to 5 yearsThe arches articulate with the centrum at cartilaginous neurocentral jointsThese joints dissapear when vertebral arches fuses with the centrum during the 3rd to 6th years

Secondary ossification center
Time of development: after puberty
the 5 secondary ossification center appears at,
1. tip of spinous process2. tip of each transverse process3. superior rim of the vertebral body4. inferior rim of the vertebral body

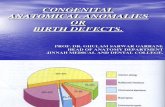
ANOMALIES OF THE VERTEBRAL COLUMN

Caused by anomalous vertebral development in the embryoThey may result in severe spinal deformity or
even cor pulmonale or paraplegia.

Schematic drawing depicting the development ofnormal and abnormal vertebral bodies

SPINA BIFIDACause: incomplete fusion of halves of the vertebral arches resulting in midline defect usually in lumbosacral regionFeature: It varies, but generally the small bones (vertebrae) that make up the spine don’t form fully and may have gaps between them.

VERTEBRAL BODY CONFIGURATIONSCONGENITALASOMIA(agenesis)• Complete absence of
body of vertebra• Posterior elements
present• FAILURE OF
OSSIFICATION CENTERES TO APPEAR

VERTEBRAL BODY CONFIGURATIONSCONGENITAL
HEMIVERTEBRAU/L Wedge Vertebrae
: lack of ossification of one half of body
Scoliosis resultsDorsal Or Ventral
Hemivertebrae: failure of ventral /dorsal half to ossify
Kyphosis results

VERTEBRAL BODY CONFIGURATIONSCONGENITAL
METAMERIC HEMIVERTEBARE• Due to hemi
metameric segmental displacement
• Hemivertebrae separated from each other in sagittal plane
• Fuses with the segment above or below

CORONAL CLEFTFailure of fusion of
anterior and posterior ossification centres
Seperated by a cartilage plate

BUTTERFLY VERTEBRAFailure of fusion of
lateral halves of the body
Due to persistent notochordal tissue
May be a/w spinabifida and anterior meningocele

BLOCK VERTEBRAFailure of
segmentationComplete(both the
anterior an dposteiror elemnts involved) or partial.
Differentiate fromacquired by the presence of WAIST at the level of intervertebral disc.

Result of vascular insufficiency during fetal life.
HYPOPLASTIC VERTEBRA

SACRALIZATION OF 5TH LUMBAR VERTEBRA
Cause: 5th lumbar is fused with the sacrum
Feature: number of lumbar vertebra is 4 and the sacrum is formed of 6 vertebra

LUMBRIZATION OF FIRST PIECE OF SACRUM TO FORM SEPARATE VERTEBRA
Cause: separation of first piece of sacrum to form separate vertebra
Feature: number of lumbar vertebra is 6 and the sacrum is only formed of 4 sacral vertebra

CONGENITAL KYPHOSIS
Two types of congenital kyphosis exist:
defects of segmentation defects of formation Defects of segmentation occur most
often in midthoracic or thoracolumbar regions and may involve 2-8 levels
Produce a round kyphosis

CONGENITAL KYPHOSIS

CONGENITAL SCOLIOSIS
lateral curvature of the spine that is caused by congenital anomalies of vertebral development classified according to the types of anomalies.
Failure of formation Partial failure of formation (wedge vertebra)Complete failure of formation (hemivertebra)

Failure of segmentation
Mixed (see image below)
Unilateral failure of segmentation (unilateral unsegmented bar)Bilateral failure of segmentation (block vertebra)

CONGENITAL SCOLIOSIS

CONGENITAL LORDOSIS
least common of the 3 major patterns of congenital spinal deformity
caused by a failure of posterior segmentation in the presence of anterior active growth
usually is progressiveTreatment of
congenital lordosis is purely surgical.