Complications of TMJ Surgery - Elseviersecure-ecsd.elsevier.com/us/pdf/SampleContent/Oral-and... ·...
16
Complications of TMJ Surgery David Hoffman, DDS a , Leann Puig, DMD b Complications from temporomandibular joint (TMJ) surgery can be divided in true complications and untoward outcomes. The purpose of this article was to look at complications directly related to TMJ surgery and not dwell on the outcomes or the success of TMJ surgery. Needless to say, complications clearly affect surgical outcomes; however, there are many other factors that affect the success rate of TMJ surgery. The 3 main surgi- cal procedures that could lead to complications are: Arthroscopic surgery Open arthroplasty; and Total joint reconstruction. Although these 3 groups are general or broad categories, they each have their own specific sur- gical techniques and therefore their own potential complication rates. They are all done differently, and each one in successive order has an increasing rate of complications. In general, complications can be divided into the following categories: 1. Anatomic 2. Neurovascular 3. Infectious 4. Autoimmune, and 5. Biomechanical. Damage to adjacent anatomic structures can become a major concern when doing TMJ sur- gery of all kinds. Infections are a second impor- tant group of complications, and although rare (about 2% in all 3 categories), when they occur they have devastating effects on the patient. Infection rates can also be looked at as a compar- ison in what the overall infection rate is in other orthopedic joint-related procedures. There are so few publications on TMJ infections and the numbers are so low that, for any given group, the orthopedic literature has become the bench- mark for comparisons. Hypersensitivity reactions a Oral & Maxillofacial Surgery, Staten Island University Hospital, 256-C Mason Avenue, 3rd Floor, Staten Island, NY 10305, USA; b Kings County Hospital, Brooklyn, 451 Clarkson Ave, NY 11203, USA E-mail address: [email protected] KEYWORDS TMJ surgery TMJ surgical complications TMJ surgical infections Maxillary artery bleeds TMJ nerve damage KEY POINTS The complications of temporomandibular joint (TMJ) surgery are a known event and, even in the best surgical hands and surgical intentions, complications can develop. There are no indications to suggest that a complication such as bleeding, infection, or failure of the prosthesis is necessarily the fault of the surgeon or the patient. For the most part, complications are rare and TMJ surgery can be done in a very successful manner. The advent of arthroscopic surgery has minimized untoward events and has been a major help to many surgical patients. Simplifying many of the arthroplasty procedures can be of benefit to patients and be performed in predictable and successful fashion with minimal complication rate. Oral Maxillofacial Surg Clin N Am 27 (2015) 109–124 http://dx.doi.org/10.1016/j.coms.2014.09.008 1042-3699/15/$ – see front matter Ó 2015 Elsevier Inc. All rights reserved. oralmaxsurgery.theclinics.com
Transcript of Complications of TMJ Surgery - Elseviersecure-ecsd.elsevier.com/us/pdf/SampleContent/Oral-and... ·...

Complications of TMJSurgery
David Hoffman, DDSa, Leann Puig, DMDbKEYWORDS
� TMJ surgery � TMJ surgical complications � TMJ surgical infections � Maxillary artery bleeds� TMJ nerve damage
KEY POINTS
� The complications of temporomandibular joint (TMJ) surgery are a known event and, even in thebest surgical hands and surgical intentions, complications can develop.
� There are no indications to suggest that a complication such as bleeding, infection, or failure of theprosthesis is necessarily the fault of the surgeon or the patient.
� For the most part, complications are rare and TMJ surgery can be done in a very successfulmanner.
� The advent of arthroscopic surgery has minimized untoward events and has been a major help tomany surgical patients.
� Simplifying many of the arthroplasty procedures can be of benefit to patients and be performed inpredictable and successful fashion with minimal complication rate.
inics.com
Complications from temporomandibular joint(TMJ) surgery can be divided in true complicationsand untoward outcomes. The purpose of thisarticle was to look at complications directly relatedto TMJ surgery and not dwell on the outcomes orthe success of TMJ surgery. Needless to say,complications clearly affect surgical outcomes;however, there are many other factors that affectthe success rate of TMJ surgery. The 3 main surgi-cal procedures that could lead to complicationsare:
� Arthroscopic surgery� Open arthroplasty; and� Total joint reconstruction.
Although these 3 groups are general or broadcategories, they each have their own specific sur-gical techniques and therefore their own potentialcomplication rates. They are all done differently,and each one in successive order has anincreasing rate of complications.
a Oral & Maxillofacial Surgery, Staten Island University HoNY 10305, USA; b Kings County Hospital, Brooklyn, 451E-mail address: [email protected]
Oral Maxillofacial Surg Clin N Am 27 (2015) 109–124http://dx.doi.org/10.1016/j.coms.2014.09.0081042-3699/15/$ – see front matter � 2015 Elsevier Inc. All
In general, complications can be divided into thefollowing categories:
1. Anatomic2. Neurovascular3. Infectious4. Autoimmune, and5. Biomechanical.
Damage to adjacent anatomic structures canbecome a major concern when doing TMJ sur-gery of all kinds. Infections are a second impor-tant group of complications, and although rare(about 2% in all 3 categories), when they occurthey have devastating effects on the patient.Infection rates can also be looked at as a compar-ison in what the overall infection rate is in otherorthopedic joint-related procedures. There areso few publications on TMJ infections and thenumbers are so low that, for any given group,the orthopedic literature has become the bench-mark for comparisons. Hypersensitivity reactions
spital, 256-C Mason Avenue, 3rd Floor, Staten Island,Clarkson Ave, NY 11203, USA
rights reserved. oralmaxsurgery.thecl

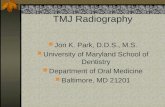
Fig. 2. Blood vessels in the field of the temporoman-dibular joint condyle. (From Quinn PD. Color atlas oftemporomandibular joint surgery. Philadelphia:Mosby; 1998; with permission.)
Hoffman & Puig110
or hardware failures are rare, but also potentiallyincapacitating.A basic understanding of the TMJ anatomy is
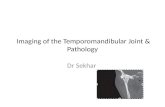
inherent in understanding potential complications.The joint itself is surrounded by neurologic struc-tures primarily derived from cranial nerves V andVII, and blood vessels branches of the internalmaxillary and superficial temporal artery predo-minantly (Figs. 1 and 2). Additionally, the joint isintimately involved with the base of the skull,sharing the roof of the glenoid fossa with the mid-dle cranial fossa, so that any damage to the bonystructures of the joint has the potential to cause anintracranial hematoma or cerebrospinal fluid fis-tula. One of the problems associated with someof the vasculature surrounding the joint, in partic-ular the maxillary artery, is that it is located medialto the joint and any damage to it during a surgicalprocedure runs the risk of having a bleed that isnot approachable for routine tying off of the vessel.For most surgeons who have experienced a maxil-lary artery bleed, isolation and ligation is ideal;but, if not possible, packing and embolizationshould be considered. The close proximity of theear potentiates damage to the external auditorycanal, the tympanic membrane, and the middleear. Additionally, the parotid gland is inferior butadjacent to the joint.Certainly, the best approach to minimizing
the complication rate of TMJ surgery is carefulsurgical planning, delicate technique, and
Fig. 1. Diagram of the facial nerve (VIIth cranialnerve) around the temporomandibular joint. (FromQuinn PD. Color atlas of temporomandibular jointsurgery. Philadelphia: Mosby; 1998; with permission.)
preparedness to identify and treat a complicationbefore it occurs or immediately upon its expres-sion. With the advent of 3-dimensional modeling,computed tomography (CT) arteriograms, andMRI, the surgeon can anticipate many of the prob-lems that might potentially occur and plan to avoidthem, or treat them if they do occur. For example,when the CT arteriogram illustrates an arterydirectly in the field of an ankylosed joint, the useof interventional radiology either before or duringsurgery, can minimize or eliminate intraoperativebleeding with the use of selective embolization.This is just one of many examples of how the useof technology and imaging can help to plan andperform a safe TMJ surgery.Another technology that lends itself to complex
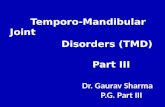
TMJ surgical procedures such as ankylosis isimage-guided surgery. This technology, althoughdeveloped either for intracranial surgery or ear,nose, and throat surgery, is directly applicable toTMJ surgery. In this instance, a surgical wandthat allows the surgeon to identify their positionon a computed axial tomography (CAT) during sur-gery can be very helpful. Currently, there are 3companies that support this type of technology,each one having the maxillofacial component.They are Brain Lab, Stryker, and Medtronics(Fig. 3).Another complication applicable to any type of
TMJ surgical procedure is the effect of the TMJon function and occlusion. Although arthroscopyhas a minimal and temporary effect on mandibularocclusion, it does have significant effects on itsfunction. The 2 other surgical procedures—arthro-plasty and total joint reconstruction—directly

Fig. 3. Image-guided surgery in a case of temporomandibular joint ankylosis. Surgical wand shows the position ofthe wand in the bone.
Complications of TMJ Surgery 111
affect occlusion because the joint becomes one ofthe stable structures in establishing a bite. There-fore, a surgical malocclusion as a result of TMJsurgery could easily be construed as a complica-tion. For example, a malpositioned total jointreplacement would be unforgiving if the bite werenot exactly set right. Furthermore, failure to main-tain the occlusion after ablative surgery of the TMJcan easily result in a malocclusion.
In some instances, surgical complications aredirectly related to the craniofacial structures andhave similar comparisons to other skeletal joints.Occlusion and joint function are specific to theTMJ and cannot necessarily be compared withother orthopedic models. On the other hand, infec-tions become similar to other orthopedic replace-ment systems and a comparison of the givenTMJ surgical procedures can be extrapolated tosee how they would fair against the orthopedicliterature. Vallerand and Dolwick1 reviewed TMJsurgical complications in 1990. At that time, TMJarthroscopy had recently become popular, andalloplastic joint replacements were in a holdingpattern owing to problems with proplast. Kieth2
published a similar review in 2003 with a substan-tial amount of data on arthroscopy, and a growingbody of data on the latest generation of total jointreplacement systems.
ARTHROSCOPIC SURGERY
Arthroscopic surgery is probably among the safestprocedures performed by maxillofacial surgeons.In its simplest form, a 1.9 or smaller arthroscopeis placed in the TMJ either through a posteriorpuncture or an anterior puncture or portal. Scopesas long as 2.3 have been used, and even workinginstruments as large as almost 3 mm can be uti-lized with or without the protective casing. Arthros-copy can be as simple as a single puncture in theTMJ with an outflow system created with an 18-gauge needle to a more complex procedure usingmultiport or triangulation techniques involving theuse of 1 portal for the arthroscope and the secondportal for instrumentation. Instrumentation canrange from forceps to graspers, spinal needles toinject, shavers, electrocauteries, and lasers. Inlight of this multiport or triangular operative

Hoffman & Puig112
arthroscopic surgery, the complication potentialof a broken instrument always exists. Instrumentsshould be checked carefully before they areinserted, and if there is any question of work hard-ening or potential fractures, they should bechanged for a newer version. If an instrumentdoes break, the surgeon should be prepared toeither retrieve it through the arthroscope orperform an open procedure at that time. Fortu-nately, broken instruments in the TMJ rarely occur,and there are virtually no reported instrumentbreaks in the literature.The number 1 complication in terms of severity is
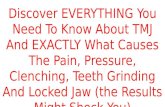
damage to the ear by an inadvertent misplacementof the arthroscope. Routinely, the arthroscope isplaced through a portal at approximately 10 mmanterior of the tragus along the tragal canthal line.Surgical placement of the trocar is the key to avoid-ing damage to the external or middle ear struc-tures. The trocar for the posterior portal shouldalways be angled anterior away from the ear.With the patient in a supine position and the headturn 90� and the side of face parallel to the floor,the potential of inadvertently placing the trocar orthe scope into the ear canal is minimized (Fig. 4).Even though the markings of 10, 20, and 30 mmare good indicators of the position and contour ofthe glenoid fossa, it is important for the surgeonto take his finger and palpate the rim of the glenoidfossa to find the actual indentation and make apuncture wound along that line. To avoid compli-cations of placement of the instrument inadver-tently into the ear structures, the surgeon mustfirst ensure that the scope is in the joint afterplacing the trocar in the joint itself. This is doneby a combination of both feel, when the scopehas free movement inside the joint space, and
Fig. 4. Position of the arthroscopic cannula enteringthe posterior puncture site. Note that the scope is inthe depression under the rim of the glenoid fossa,and is pointe forward.
visual sighting. If both these parameters are notmet, the surgeon has to regroup and ensure thatthe cannula or arthroscope is inserted in the appro-priate position. Once inside the joint, an inflow andoutflow system can be established and furtherexamination can occur. Several studies havebeen reported on related ear damage with arthros-copy and they vary from virtually none to minor ortemporary issues; hearing was affected in fewerthan 1% of cases.3,4
NERVE DAMAGE
The facial nerve could be considered the secondmost important structure at risk during arthros-copy of the TMJ. Understanding the anatomy ofthe facial nerve as it passes over the TMJ is keyto all TMJ surgeries. Classical literature has des-cribed a safe zone approximately 0.8 to 1.8 mmin front of the tragus and approximately 10 mminferior to the root of the glenoid fossa The conceptof arthroscopic surgery with placement of a scopealong the posterior portal at approximately 10 mmseems to be very safe and blunt dissection of atrocar has minimal chance of damaging the nerve.The second cannula, if we are using a multiporttechnique, is placed approximately 25 to 35 mmanterior to the tragus and usually is in front of thefacial nerve. Accordingly, placement of the instru-ments into the TMJ has minimal potential to dam-age to the facial nerve. However, inadvertentbleeding, scarring, or aberrant moves can run therisk of facial nerve injury.Cranial nerve V, particularly its third division, can
also be damaged during arthroscopy. Patientsreport some numbness to their lip or teeth accord-ingly. This seems to be more the result of swelling,because the nerve itself is not in the surgical field.Fluid extravasation with into the surround tissuesmay cause a transient nerve injury to either cranialnerve V or VII.Neuropraxia around the joint usually is related
to temporary edema and is usually short lived.Should there be permanent nerve damage, itwould potentially be to the frontal zygomaticbranches and this can be treated appropriatelywith either the use of botulinum toxin on thecontralateral side of the forehead or a gold weightinto upper lid if it is permanent in nature. Thisauthor has had 2 patients with masseter nervedamage and secondary weakness. One of thepatients went on to achieve full recovery, and theother had permanent dysfunction and atrophy ofthe muscle.Arthroscopy also runs the risk of damaging the
base of the skull by inadvertently putting the scopeinto a weak portion of the roof of the glenoid fossa.

Fig. 5. Maxillary artery medial to the condyle (arrow).(From Quinn PD. Color atlas of temporomandibularjoint surgery. Philadelphia: Mosby; 1998; withpermission.)
Fig. 6. Computed tomography arteriogram showingblood vessels around the ankylosis.
Complications of TMJ Surgery 113
Careful introduction of the trocar and appropriatesiting of the joint space avoids this pitfall. Damageto medial structures is particularly uncommon ifthe surgeon knows the parameters of the jointitself. Most joints are within the 25 mm of width,and careful attention to the depth of the trocarcan almost make this an unlikely possibility. Theskin is of variable thickness, but McCain describesthe medial wall at about 50 mm forms the skin.4–6
The literature has not reported any significantdamage to the middle cranial fossa, and certainlycareful technique and staying with in the jointspace are paramount.
Damage to joint structures is a potential compli-cation. If the surgeon is just doing a simple lysisand lavage or injecting medications, the complica-tion rate for the most part is negligible. The use ofsteroids inside the joint is somewhat controversial,and there has been some suggestion that a singleunit of steroid injection may facilitate degenerativejoint disease. On the other hand, steroids in thejoints are commonly used in orthopedics for otherassociated joints and the literature does not sub-stantiate that a 1-time use of a steroid in the jointis problematic. One can even suggest that thepatient’s joint is damaged to begin with and thatthe steroid is given for the purposes of improvingjoint function. For the most part, damage to relatedstructures inside the joint such as the synovium,the disc, or the medial draping are minimal, andthe joint has quite a bit of reparative effect. Mostof the time, surgeons find damaged joints as aresult of the disease process. The literature hasno reported incidents of the surgeon doing perma-nent iatrogenic damage to a TMJ through manipu-lation or placement of an instrument into the discor synovial tissue.
On certain occasions, the joint space is so oblit-erated that the joint cannot be well visualized andthe surgeon is not sure the instruments are in thejoint. In this instance, the discretion of the surgeoncould be discontinuing the case or take instru-ments such as shavers or lasers and create a jointspace. In doing so, the surgeon must be careful toalways have the instrument in sight, and that theyare comfortable with the performed procedure.
Potentially, when there is no joint space visi-ble, the surgeon could become disoriented andeasily slip into an area anterior to the joint suchas the sigmoid notch and hit the maxillary arterywith a maxillary artery bleed (Figs. 5 and 6).This could be problematic. During arthroscopicsurgery, on lysis and lavage, there can be onoccasion bleeding that is more than just simpleooze. However, placing the patient into occlusionoften stops any eventual bleeding, and it has notbeen reported that bleeding is a known risk of
arthroscopic surgery. Hemarthrosis can be a pro-blem jeopardizing postoperative function.Bleeding from the puncture site can occur andthis can easily be controlled with oversuturingthe area. Misdiagnosis of a potential ankylosiscould occur without the use of appropriate imag-ing, and an attempt to arthroscope the joint thathas no true space could easily put the surgeonin a situation where the scope is misguided andsome of the above complications could occur.
Patient selection is important for many reasons,some of which beyond the scope of this article.However, the heavier the patient is, the more diffi-cult the procedure will be.
There has been a case report of an arteriove-nous fistula and cardiac arrhythmias.7–9

Hoffman & Puig114
Overall, TMJ arthroscopic surgery can be con-sidered a very safe and low-risk procedure. Theincidence of nerve damage complications is al-most negligible.10 During a 10-year period, atone of the institutions of the author, we looked atthe overall rate of infections in arthroscopic sur-gery, and it was approximately 1%. When furtherdelineating the use, this was an operative arthros-copy where sutures were placed in a multiporttechnique. During this procedure, the few patientswho have had infections were examined very care-fully, and of the 6 patients who have had postoper-ative infections, 1 or 2 were stitch abscesses andthe others were all immunodeficient patients.This is in line with the known incidence of infec-tions in orthopedic literature, which is about1%.11–13 Obviously, careful selection of patientsis paramount in any surgical procedure and thepotential of infections in immunocompromisedpatients is always there.Postoperative pain can occur in many patients
and is beyond the scope of this discussion as aknown complication. However, selection whendealing with chronic pain patients is importantand should be taken into consideration beforethe decision to operate is made.Distention of the joint can occur during an
arthroscopic procedure. This is a result of con-stantly having more fluid flushed into the jointand not having an appropriate outflow. Surgeonswho rely on a pump are more prone to havingthis problem. In addition, the surgeon who hasan assistant pumping water through the inflowand outflow system and is not watching the appro-priate outflow can also have this problem. Disten-sion of the surrounding tissues can collapse thejoint space and limit the ability to complete theoperation. The swelling can be so severe that itcan cause a shift medial to the joint and create apotential airway occlusion. Although this compli-cation has been reported, it is not commonlyseen and it is not among the known risks, otherthan that the surgeon should avoid distendingthe joint. Once the surrounding joint space is dis-tended, the arthroscopic surgery is over and thesurgeon has to stop the procedure with no benefitto the patient.14,15
TEMPOROMANDIBULAR JOINTARTHROPLASTY
TMJ arthroplasties encompass surgical incisionsinto the TMJ through an external approach. Themost common incision is the preauricular, althoughothers have been discussed. Regardless of thediagnosis, the surgical procedure has a group ofcommon potential complications, including
damage to adjacent structures including nerves,vessels, the ear, parotid gland, base of the skull,and middle cranial fossa. In addition, infectionsand secondary issues such as ankylosis, functionaldisorders, and increase postoperative pain shouldbe considered. Common surgical treatments forinternal derangements, degenerative joint disease,tumors ankylosis, or part of total joint placement forthe most part entail the same complication issues.
Nerve Injuries
Nerve injuries can occur to cranial nerves V andVII. The surgical approach stays within the safezone and has been described elsewhere. Damageto the facial nerve is a known risk in this procedureand intuitively increases in the patient who hasundergone previous operations. Damage caneither be permanent or temporary, and can bethe result of stretching to gain access to the jointor severing in the dissection. Nerve stimulatorsare helpful to avoid this problem.
Treatment of nerve injuriesIn this instance, it is the same as from arthroscopy,and if weakness in the frontal branches is ob-served, cosmetic treatment of the injury can bedone with either a forehead lift, or botulinum toxinto the adjacent side to give symmetry. An inabilityto close the eyelid is difficult to fix anatomically,but the use of a gold weight in the upper lid seemsto resolve the problem.Damage to the fifth mandibular division of
cranial nerve V is not likely. However, patients doreport having some numbness to that area,although it seems to be transient. It seems that itis either from swelling or retraction that has gonebeyond that level of the capsule and causingsome pressure on the mandibular nerve as ittravels parallel to the joint and enters the inferioralveolar canal.2,16
InfectionsInfections from arthroplasty of the joint are in the1% to 2% range, as indicated by these authorsand as compared with the orthopedic literature.Infections can be of 3 distinct routes in theory:Contamination during the operative procedureowing to some type of flora from the adjacentstructures, for example, the external ear, or scalp;immunodeficient patients; and opportunistic in-fections. Patients with a localized infection maycontaminate the wound and this may occurbefore surgery or postoperatively. For example,the patient in Fig. 7 developed a secondary infec-tion to an allergic reaction to tape and had aStaphylococcus infection surrounding the joint.Owing to the increased concentration of the

Fig. 7. Skin infection from an allergic reaction to tapein a total joint patient that spread to the joint itself.
Complications of TMJ Surgery 115
bacterial flora in and around the joint, the jointbecame secondarily infected. These infectionsare known as acute infections and can often betreated with appropriate antibiotics and lavagingof the joint. Because there are no foreign bodies,in an arthroplasty per se, with the exception of aMitek bone anchor or a suture, joints can oftenbe treated with aggressive postoperative care.There have been reported instances where thepatients themselves would seed the infectionfor some unforeseen psychological gain. Thesecases are difficult to treat and can have unlikelyflora on culture. Drug addicts also have a propen-sity to infections in a joint and they often grow aserration-type infection. Indications of an occultjoint infection start out with signs of pain, swelling,and inflammation around the joint. It may takeseveral weeks before the joint opens up andstarts to ooze. Certainly, arthroplasty patientswho have an abnormal postoperative presen-tation with signs of swelling, lymphadenopathy,and edema should be considered for infection.This may include testing beyond the clinicalexamination, including bone scans and bloodchemistry looking at C-reactive protein and sedi-mentation rates.
Surgical infections in general in joints can bedivided into acute, subacute, and chronic infec-tions. Acute infections lend themselves to aggres-sive wound care and antibiotics. Subacuteinfections are defined as one that occurs withinthe first year. Chronic infections often developlater and can be persistent. Chronic infectionscan come from a biofilm if an alloplastic materialis used, although with no foreign body in the joint,a biofilm is an unlikely culprit. In either case, if therehas been an autogenous grafting in the joint,then one must consider that the material that has
been grafted is contaminated and may need tobe removed. Chronic infections of the joint couldlead to chronic osteomyelitis in the joint or spreadthe infection beyond the joint and into the adjacentstructures, such as osteomyelitis of the base ofskull and the glenoid fossa. Infection in the jointalso may present through a fistula into the externalauditory canal; the primary source may be thecanal itself or the joint. Without foreign body, thiscircumstance is difficult to determine. With theforeign body, one would assume that the jointwas the source of infection.
The use of Mitek bone anchors is the mostcommon foreign body placed in the joint. Therehas been nothing in the literature to suggest thatMitek bone anchors have an higher incidence ofinfection fat grafting in the joint; other autogenousgrafts bring along with them the potential site ofcontamination on the operating table or from thecontamination of the donor site. When periumbili-cal fat is used, it should be carefully managedbecause it is proximal to the umbilicus, which isconsidered part of the dirty field and should becopiously given a sterile preparation.2,12,13
Damage to Adjacent Structures
Damage to adjacent structures of the joint canoccur either through direct trauma during thetime of surgery or secondary as a result of a bleedor infection. The ear is probably the most trouble-some structure that could have severe effects ifthere is a hearing impairment that is related tothe joint. Care should be taken so that the surgeonstays in front of the auditory canal and there is nobleeding or heavy instrumentation in that area thatwould potentially damage the middle ear or theossicles per se.
The base of the skull again can be damaged ifsurgery extends too far medially. On either sideof the joint, there is a capsule. Scar tissue andbony ankylosis can also penetrate the medialaspect and damage can occur there. Medial tothe joint below the level of the condyle lies themaxillary artery, and this could be a significant vitalstructure that is discussed elsewhere.
Damage to Vessels
Bleeding and nerve damage often run hand inhand. In the attempt to stop bleeding with acautery, the burn can propagate to a nearby nerve.Most bleeding in TMJ surgery occurs during thedissection and can be controlled with surgicaltechnique. Damage to the maxillary artery ismore ominous and is discussed under total jointreplacements.

Hoffman & Puig116
Frey Syndrome
Frey syndrome or gustatory sweating is a knowncomplication of both parotid gland surgery andTMJ surgery. It is a mix up of the sympatheticand parasympathetic nerves around the face.Treatment includes the use of botulinum toxin,and or placement of a graft material under theskin in the effected area.
Diskectomy
Removal of the disk with or without a graft hasbecome a standard procedure in TMJ surgery;the major complication is disease progression.This author presented a paper at an AmericanAssociation of Oral and Maxillofacial Surgeonsmeeting on the outcome of diskectomy patientswith or without fat grafts. Of note was the factthat at least 50% of patients went on to potentiallyrequire a total joint replacement.
Patients Undergoing Multiple Operations
One concern over arthroplasty patients is the needfor serial operative procedures. This may be owingto disease progression or ectopic bone formation.Whether this scenario is a complication is debat-able. The surgeon must consider in the surgicalalgorithm at least a stopgap measure to avoidmultiple procedures and having their patientsbecome chronically ill pain patients.
Alloplastic Implant
Historically, there have been several types of diskimplants or substitutes, including Teflon/proplastimplants and silicone sheeting. The problem withthese materials is that they tend to break apartand cause foreign body cell reactions. Metal fossaimplants were used for a time and avoided thisproblem, but have not been widely accepted andmay not be available currently. All insertable mate-rials run the risk of infections, instability, and hostresponse problems.17,18
TMJ surgery is a technique-sensitive procedure.Attention to detail, preoperative planning, a patientexpectations should all be part of the decision-making process. Intraoperative problems are realand can occur, even in the best of hands. Thinkingahead and surgical preparation become keyfactors.
TOTAL JOINT REPLACEMENTS
Of the 3 surgical procedures discussed herein,total joint replacements are probably the mostcomplex and demanding. Whether the surgeon isusing a custom-made or stock joint, the surgicalprocedures are for the most part the same and
the complications are nearly identical. It is notthe intent of this paper to compare different pros-theses. Because total joint replacements add theelement of a foreign body into the equation, surgi-cal sterility becomes paramount. Replacement ofa total joint requires 2 surgical incisions. The firstincision is identical to the arthroplasty incisionand incorporates a preauricular incision in frontof the ear. The second incision has some variation,but is either a retromandibular or submandibularincision; either one has its proximity to the facialnerve and related vasculature, facial artery, andvein. The incisions for this procedure are well-described in these clinics as well as other surgicalapproaches to the facial skeleton. It is probablyimportant that both incisions are made with carefulattention to cranial nerve VII and that either a nervestimulator or a nerve locator be used.It is important that surgeons spend a reasonable
amount of time in planning the surgical procedurewhen it comes to total joint replacements. Usually,detailed computed axial tomography scans areobtained and a surgical plan is developed wellbefore the time in the operating room. Particularlyin the case of ankylosis patients, there are manyprocedures that could be done preoperatively todelineate the extent of the ankylosis and thevascularity surrounding the ankylosis. The use ofCT, especially in conjunction with arteriograms,can clearly define the surgical anatomy as wellas the abnormal surgical structures.
Nerve Damage
As described in the discussion on an arthroplasty,cranial nerve VII lies directly over the surgical fieldof entry. In this instance, not only does the preaur-icular incision involve part of the facial nerve, butso does the retromandibular or submandibularapproach. Damage to any one of these branchescan result in either a true severing of the nerve orpurely a stretching of the nerve. In a case of nervestretching, nerve function generally returns, whe-reas if there is inadvertent severing of the nerve,it is unlikely that function will return to normal. Un-like a TMJ arthroplasty, it is possible to damageisolated branches of the facial nerve in the re-tromandibular or submandibular incision whileleaving the main trunk alone. The preauricular inci-sion alternatively can have either the frontal orzygomatic branch damage and/or potentiallydamage in severe cases the entire trunk of thefacial nerve, including all 5 branches involved. Itis unlikely for complete facial nerve paralysis tooccur, but in theory it is possible. Again, carefulsurgical technique and either a nerve stimulatoror a nerve locator will help to avoid this problem.

Complications of TMJ Surgery 117
It is important to instruct the anesthesiologist notuse muscle relaxants if possible so that this testingcan be done.16
Potentially, a nerve can be damaged through theuse of electrocautery. In this instance, in anattempt to stop bleeding, a nerve injury can occurwhere the radiation of the electrical chargespreads in a circular fashion around the point.The use of a Colorado tip or bipolar cautery mini-mizes this problem. In addition, when bleedingoccurs, especially at the root of the incision ofthe preauricular approach, it may be safer to tryto correct the problem with the use of local anes-thetic and oversew the area with an absorbablesuture in lieu of trying to cauterize the minor bleedthat could potentially spread to a nerve injury.
In general, complications related to TMJ or totaljoint replacements can be classified as immediateintraoperative complications or postoperativecomplications. Bleeding is be an intraoperativecomplication, as is nerve damage. Often, the at-tempt to stop a continuous bleed or ooze withthe use of a cautery leads to nerve injury.
Damage to cranial nerve V is possible in both theplacement of the joint with the screws leading intothe inferior alveolar canal, or exceeding the medialaspect of the joint and entering into the base of theskull. Cranial nerve V can be damaged, becauseits foramen lies medial to the medial draping ofthe glenoid fossa. In this instance, the damagemay be permanent or transient. In this author’sseries of approximately 250 joint replacements,inferior alveolar nerve damage has been minimal,and it if occurs, it is most likely the result of thean unavoidable screw placed into the nerve canalas a result of abnormal or compromised mandib-ular anatomy. In the case of big counterclockwiserotations were the mandible is repositioned anteri-orly, traction to the inferior alveolar nerve occur,causing temporary or potentially permanentdamage to the nerve.
Custom and stock joints are designed so thatthe screw fixation should lie posterior to the inferioralveolar canal and that minimal damage wouldoccur as a result of fixation of the condylarcomponent.
Bleeding Issues
Intraoperative bleeding in total joint replacementscan occur from some of the major vessels locatedin the surgical field, including the maxillary artery,temporal artery, masseteric artery, and facialartery. In addition, the associated veins can alsobe injured. Furthermore, because there is musclestripping and cutting, especially of the masseterand both pterygoid muscles, there can be a
significant amount of oozing of that musculature.Inadvertent damage to the masseteric artery canoccur when the area underlying the sigmoid notchis not protected in an attempt to remove sufficientbone to place the joint, during ankylosis, or inattempts to remove the coronoid process. Knowl-edge of the vascular anatomy and adherence togood surgical technique of isolating the soft tissueaway from the bone can minimize intraoperativebleeding. Several surgeons favor the use of aPiezo saw when they get close to the adjacentsoft tissue next to bone and find this as anotherform of safety to minimize bleeding.
The most clinically important vessel that couldbe damaged in TMJ surgery is the maxillary artery,which runs behind the neck of the condyle and atthe level just above the sigmoid notch (seeFig. 5). In most instances, this area can be pro-tected with the use of instrumentation that isposterior and medial to the bony cuts of thecondyle. Should the maxillary artery bleed, itposes a significant intraoperative threat becauseof the lack of accessibility to tie it off, especiallyin ankylosis. There are discussions in the literaturethat suggest that tying off the branch of the maxil-lary artery as it comes off the external carotid willnot suffice because there will be retro-flow andthe bleed will continue. However, surgeons whohave been in this situation have reported thateither tying off the visible artery or tying off thebranch can help in stopping the bleeding. Carefulpreoperative planning in cases of ankylosis canallow the surgeon to embolize the artery 1 or2 days before surgery. An alternative to that pro-cedure can be exposure of the branches of theexternal carotid during the surgery and immediateembolization, if a bleed occurs, can be undertaken(Figs. 8 and 9).
Adjunctive therapies to stop bleeding shouldalways be available such as thrombin-soakedSurgicel or the use of some of the fibrin products.Often packing in the area and allowing a sufficientamount of time stops most oozing or minor jointbleeds.
Damage to Adjacent Structures
Intraoperative damage to adjacent structures isalways a concern as an intraoperative complica-tion. Most relevant structures related to jointreplacement TMJ surgery are the 3 areas sur-rounding the condylar component, including theexternal and internal structures of the ear, theanatomic areas medial to the joint (specificallythe base of the skull), and damage to the superioraspect of the glenoid fossa into the intracranialspace. All these potential areas of damage require

Fig. 8. Embolization of a maxillary artery bleed during temporomandibular joint surgery.
Hoffman & Puig118
careful surgical dissection to minimize the po-tential hazard. Careful presurgical workup withcomputed axial tomography can identify areasthat would be of concern in situations such as tu-mors or ankylosis. Again, the use of image-guidedsurgery and careful dissection can help to
Fig. 9. Branches of the external carotid artery and themaxillary artery exposed in case of a maxillary arterybleed.
minimize this problem. The literature does notreport any significant complications to the baseof the skull, although in an ankylosis case thereis potential to go beyond the medial envelope ofthe joint. Certainly, in an attempt to remove suffi-cient tissue for placement of prosthesis, the sur-geon can enter the base of the skull and damagesome of the structures located in that area,because their foramens are just medial (see Fig. 2).Damage to the ear can happen if the surgeon is
misguided or the ankylosis extends into the earcanal. In addition, aggressive use of instrumenta-tion such as a chisel and a hammer can causetrauma to the related areas. The surgeon shouldhave some type of anatomic guide when ap-proaching ankylosis that extends adjacent to theear canal. Damage to the ear canal itself can occurduring the surgery, but again this is a rarelydescribed event.Perforation of the roof of the glenoid fossa will
lead into the intracranial exposure the parietallobe of the brain. In this event, if the dura is intact,it is probably not going to be a considerable prob-lem. Should there be a cerebrospinal fluid leak or

Complications of TMJ Surgery 119
perforation that seems sufficiently large, it needsto be addressed with both a neurosurgical consul-tation and the potential for sealing off the space. Abone graft, dural patch, or use of the prosthesisitself may suffice as a safeguard. Potentially, abone graft can be placed and the surgery can beaborted and returned at a later date. One concernis that a foreign body, such as prosthesis, be-comes infected; it could lead to an intracranialinfection. However, it is not uncommon to use aforeign body to seal the bony structure of the cra-nial cavity during routine neurosurgical proce-dures, and the TMJ could be considered as anyother intracranial approach. A neurosurgical con-sultation would be required. The literature doesnot discuss this problem, but this author hasseen a few clinical cases and presentations byothers on this topic. This complication is alwaysa concern in the event that the roof of the glenoidfossa is violated.
Malposition of the Prosthesis
Malpositioning of the prosthesis can occur inseveral different clinical manifestations. The dentalocclusion must be set appropriately before thecondylar and fossa components are set. It is advis-able to double check this surgical step in the oper-ating room, because a mistake will lead to redoingthe surgery. Many times, attempts are made toreposition the mandible during surgery, and thereis a significant amount of pulling and an inabilityto release some of the scarring from previoussurgical endeavors. Passive stable occlusionshould be obtained. The surgeon should alwayshave some system of checking the occlusiononce the patient is taken out of intermaxillary fixa-tion during the surgical procedure before all thescrews are placed. A second possibility is thatthe condyle is poorly situated, and even thoughthe occlusion is stable as soon as the intermaxil-lary fixation is released, the condyles returnsback to an unfavorable spot. Again, surgical tech-nique requires that the condyle be seated appro-priately during fixation of the components. The
Fig. 10. Displaced fossa on the left joint.
fossa itself has to be positioned appropriately,and if it is not secured into good bone stock, thepotential for the fossa to slip postoperatively canoccur (Fig. 10).
Additionally, postoperative dislocations canoccur. These can occur inadvertently during thetime of surgery, upon extubation, or in the immedi-ate postoperative period when the patient may besuffering from severe nausea or vomiting and putsabnormal stretch on the joint. It can occur in thepostoperative period during the healing phase aswell, but is not a common event any time afterthe first few weeks postoperative. The most com-mon time for dislocations to occur is when boththe medial and lateral pterygoid muscles are strip-ped so that there are no constraining muscles(Fig. 11). It is helpful for the surgeon to check thecondyle at the time of fixation of the components,after fixation, and before closing the incisions,confirming that the condyles are visible and inthe most posterosuperior position. Last but notleast, the surgeon should check the mobility ofthe condyle, and if it easily dislocates while theyare visualizing the joint, then the patient shouldbe considered a candidate for some type of fixa-tion with interarch wiring or elastics.
Dislocation of the condyle is easily detectableowing to malocclusion and can be addressedeither with an attempt at repositioning the condylewith sedation and then placement in a short periodof intermaxillary fixation or, in the worst casescenario, the incision sites have to be openedand the condyle has to be manipulated into itsproper position.
INFECTIONS OF THE TEMPOROMANDIBULARJOINT
The most ominous of all problems of a total jointreplacement are postoperative infections. Infec-tions can be divided into acute, subacute, orchronic. In the acute phase, it is conceivable totreat the patient with antibiotics and/or open thejoint, wash it out, and reseal it. In the chronicphase, it is almost imperative that the components

Fig. 11. Dislocated condyle in the Hoffman Pappasjoint.
Hoffman & Puig120
be removed, especially the fossa. The probabilitythat there is a biofilm is likely. The subacute phaseis somewhat less clear, and can have a mixedresponse. This author has treated several totaljoint infections by removing the fossa in the acutephase and then aggressively trying to sterilize thecondylar component intraoperatively. The factthat it is smooth and can be washed especiallywith a sterilizing agent such as Betadine hasseemingly worked in many patients. However,clinical examination and appropriate imagingshould be able to determine if the infection hasspread along the ramus area. CT to see a collec-tion of purulent material or a bone scan to see ifanything lights up other than in the joint spacealone helps to make the diagnosis. If in doubt,the surgeon needs to remove both componentsand place some type of temporary spacer in thejoint. This author has treated infections with methylmethacrylate mixed with tobramycin in removal ofboth joint components and in many instancesjust the fossa alone. There is an higher incidenceof infections after secondary surgeries on totaljoints and placement of a new fat graft. Therefore,this author has abandoned the placement of fatgrafts as a secondary procedure for this purpose.As a primary procedure, there has not been anyindication that there is any further incidence ofinfection.19–22
In a study done at Staten Island University Hos-pital and presented in an abstract at the AmericanAssociation of Oral and Maxillofacial Surgeonsmeeting, our infection rate was approximately
2% to 3%, which is even lower than the publishedpercentage unit in the orthopedic literature, whichis anywhere from 3% to 5%. The questions aroundinfections often required the decision to removeeither part or the entire prosthesis. In either case,the use of a 6-week course of intravenous antibi-otics and an infectious disease consultation areimportant. The literature on biofilms in joint re-placements has been established and it seemsto be the significant cause of infection23; othercauses are immunosuppressed patients and intra-venous drug usage. The use of prophylactic antibi-otics for dental procedures is debatable, but owingto the proximity of the condyle to any type ofdental infection, it would be prudent to take thesame precautions that orthopedics does in havingno obvious dental or skin infections in the areabefore placement and to treat them aggressivelyif an infection occurs.Replacement of the total join or fossa compo-
nent can be performed when the patent is deemedto be infection free. Following the sedimentationrate, white blood cell count, and the C-reactiveprotein levels are all helpful indicators.This author has had 2 patients with a fistula
between the external auditory canal and the jointspace with secondary infections. Both requiredremoval of the fossa, and one the entire joint.The etiology is unclear, but both have been treatedwith revisions.
LOOSENING OF PROSTHESIS
The joints are generally very secure. Most totaljoint systems involve at least 6 to 8 screws. Therehas been some debate in the biomedical engineer-ing as to the total number of screws needed tosecure the condylar component to the ramus. Itseems that fewer than 5 screws would suffice,and some form of microlocking helps to avoid mi-cromovement, which can lead to screw failure. Anattempt to have the ramus component stay asclose as possible to the existing bone is seeminglyimportant. In the use of stock joint, we wouldrequire re-contouring of the bone to get a flatsurface against a flat surface. Custom joints canavoid this problem, but at the same time, if theydo not get an exact fit, there can be an irregularsurface against an irregular surface. In anyrespect, it seems that there have been no indica-tions in the literature that a small gap in the inter-face is of any significance as long as the jointhas what is termed as 3-point stabilization andhas no wobbling per se. The fossa runs the riskof being displaced postoperatively when screwscan loosen and bone stock is not strong enoughto hold the joint in place. Displacement of the fossa

Complications of TMJ Surgery 121
runs hand in hand with screw loosening and it isdifficult to determine the cause. The cause forthe displacements or screw loosening should beidentified. Infections, trauma, or misplacement allshould be considered. Screws can loosen espe-cially when the bone is thin and there is somemicromovement associated. The concept againis that a custom joint would have a better fit anda non-custom joint would have at least 3-pointstabilization in trying to maintain a flat surfaceagainst the flat surface. In any respect, the patientshould be followed on routinely with appropriateimaging. Because the polyethylene is often notvisible on imaging, surgeons who have less expe-rience with total joint replacements can be fooledinto thinking that there is an abnormal positionowing to a shadow or space between the condylarcomponent and the metal fossa.
In the use of the Biomet joint with no metal-backed fossa, screw fixation is directly into thepolyethylene. A theoretic problem associatedwith polyethylene would be that there is micro-movement and migration of particles along thescrew fixation of the polyethylene head withoutmetal backing. This has been shown to occur inthe hip literature with propagation of a screw inthe polyethylene. This has not been a known prob-lem with the Biomet joint, and it seems that thedata available now, which are starting to becomelong term, show that these joints are not moreprone to a dislodgement in any other joint than ametal-backed fossa.
In the same vein of discussion, the use of a high-ly polished metal condyle against a polyethylenefossa has a potential problem of wear debris,although this has not been shown to occur.
In addition to displacement of a prosthetic joint,the possibility of a component fracture exists.Chromium cobalt, when used as a condylarstem, can fatigue and fracture. Fractured compo-nents are rare and the current group of jointsapproved by the US Food and Drug Administration
Fig. 12. Fracture of the condyle (right) and the fossa on (
have only isolated cases that some manufacturershave shared (Fig. 12).
Allergy to Materials
Reaction to foreign bodies, especially nickel ortitanium, can occur. Patients who are known tobe allergic to metals can be tested for metal allergyboth by an allergist and also by getting some of themetal that these joints are made of from thecompany to give them a skin test. The area ofmetal allergy seems to be controversial. However,a patient with a known history of sensitivity tometals may not be a candidate for a jointreplacement.
Recurrent Bone Formation
Recurrent ankylosis is always a concern when thepatients have had previous ankylosis whether itis fibrous, fibro-osseous, or bony ankylosis. Thegeneral surgical rule is to try and create as largegap as possible so that if bone does form, it willhave trouble connecting from the mandible to thebase of the skull. The use of fat grafts has seem-ingly minimized this event, as well as the use ofvery wide resections. There have been nocontrolled studies suggesting that fat grafts aremandatory, but several leading surgeons in thisfield routinely use fat grafts; however, others donot. It does seem prudent that, if one is concernedwith an ankylosis, patients have wide resection ofbone to minimize the ability of the bone to reap-proximate itself. Additionally, reducing the boneto levels of clean periosteum may very well helpand avoid a fibro-osseous union.
The use of postoperative low-dose radiation andmedications such as indomethacin and Didrinalcan help with this problem.
In addition to considerations that minimizerecurrent ankylosing, the ability to get good rangeof motion is important. In this instance, removal ofthe coronoid process may be helpful in improving
left).

Hoffman & Puig122
postoperative range of motion. The use of post-operative physical therapy, especially with thepatient continuing with it themselves over thelong run, would be seemingly helpful.Should ankylosis recur, it sometimes can be
approached with a rearthroplasty, but in many in-stances the joint has to be removed because thebone has grown medial to the joint and could notbe visualized. Many times the patient will formbone completely around the joint itself encapsu-lating the entire condyle in casing of bone.
Postoperative Pain
Postoperative pain can be considered a potentialcomplication. It is not uncommon for a patientwho has had bilateral joints to complain that 1side feels perfectly well and the other side is pain-ful. It is unclear exactly what the mechanism ofpain is. Intuitively, one would think that the moresurgical procedures the patient has had leadingup to surgery, the higher index of suspicion ofpostoperative chronic pain may exist. However,the discussion of pain related to TMJ surgery isbeyond the scope of this discussion. It would befair to say that pain, as a postoperative problem,is a real factor and should be addressed with thepatient both preoperatively as well as treated post-operatively with appropriate pain management.One source of postoperative pain, especially
at the 1-year mark, may be scarring inside the jointwith tissue growing in the interface of the condyleand the fossa. If this is the case, it is difficult to tellclinically that this is occurring, other than that thepatient was doing fine and then begins to havepain on motion of the joint. This can be remediedrelatively easily, with a simple arthroplasty andremoval of scar tissue. It is unclear as to why anytissue that slowly evolves as the interface betweenthe movable parts would be a problem; however, itis easy to understand that a tissue that has beensqueezed on a persistent basis could becomepainful.
Range of Motion
Poor range of motion after surgery can be anotherpostoperative problem. Most patients have losttheir pterygoid muscular function and thereforecannot translate or go side to side, although rarelya patient can. However, rotation movement shouldallow the patient to open at least 30 mm, andin many cases reportedly upwards of 40 mm.Aggressive physical therapy after surgery can behelpful. Some surgeons prefer to send their pa-tients for several months to physical therapist,whereas others feel that the use of home physicaltherapy with a device such as a TheraBite may
allow the patient to do this on a more regular basis.Two of the main objectives related to surgery in to-tal joint replacement include reduction of pain andimprovement of movement. It is inherent to pro-vide some type of therapy to improve the rangeof motion that has been obtained from the surgicalprocedure. It seems that patients tend to form afibrous scarring around the joint and this needsto be reduced with postoperative physical therapy.From time to time, the patient may have joint reop-erated on to reduce some of the scarring.There are other postoperative complications
related to TMJ surgery, but are general surgicalproblems associated with any type of facial sur-gery. Patients who have an allergy to the postoper-ative dressing can often develop a skin reactionand in case of a total joint replacement, owing tothe high concentration of bacteria adjacent to thejoint, can develop a joint infection. Wound carevaries from surgeon to surgeon from some biolog-ical dressings. Overall, it does not seem that thesurgical dressing plays a significant role in postop-erative infection. Unfavorable scarring in some ofthe areas would be more related to surgical tech-nique than the procedure itself. In general, thesurgical scars created by the TMJ surgeon areusually minimal and are not any more specificthan any other surgical procedure of the face.In summary, for complications related to TMJ
infections, it is clear that, in going from arthros-copy to arthroplasty to total joint replacements,the infections and complications become moreinvolved and more troublesome. Overall, surgeonscan separate arthroscopy and arthroplasty fromtotal joint replacements with regard to complica-tions. The latter group has to be monitored forissues related to the prosthesis itself on long-term basis.Overall, the prostheses used today, which are
highly polished metal (either titanium andchrome-cobalt or combinations of the 2 against apolyethylene surface), seem to be the standard.There have been joints using metal-on-metal andthere have been some discussion of the materials’interface. However, there seem to be no hard datasuggesting that a metal-on-metal joint in the TMJwould be a problem. On the other hand, the ortho-pedic industry has subsequently stopped usingmetal-on-metal joints. A discussion on choice ofmaterials is beyond the scope of this article ofcomplications TMJ surgical complications. How-ever, there are concerns along the lines of pros-thetic joints in terms of fatiguing of the joint withsubsequent fractures of the prosthesis. Originallyin the pure chromium-cobalt joints made by Chris-tensen, Inc, there was fracturing of the condylarcomponent. Fracturing of the condylar component

Complications of TMJ Surgery 123
now in any of the joint seems to be a rare event.Certainly, it is not advisable for any surgeon tobend or try to reconfigure these joints becausethis maneuver may cause fatigue in the metaland make it subject to a fracture. However,breaking of the prosthesis at this junction doesnot seem to be a reported problem. Furthermore,wearing out of the polyethylene has not beenreported, and does not seem to be problematic.In summary, with regard to problems associatedwith wear debris, joint fracture or choice of themetals, the 2 or 3 joints that are made todayseem to be safe. With regard to the longevity ofthese joints, they have all been established forgreater than 10 years. However, there are noindications that they should not last a lifetimeof a patient, although the data are yet to becollected. Retrieval of a joint for any reason cansometimes be a problem if the screws are coveredin bone, stripped, or metals have integrated withthe bone. This type of surgery can be verydemanding.
Total joint replacements in a growing individualhave relative contraindications, although thereare cases where they may be indicated if noother alternatives exist. Again, this is not neces-sarily a complication, but potentially a problem ifjoint replacement is needed in a growing patientand then needs to be replaced again at a laterdate.
Overall, the complications of TMJ surgery areknown and, even in the best surgical hands, com-plications can develop. There are no indicationsto suggest that a complication such as bleeding,infection, or failure of the prosthesis is necessarilythe fault of the surgeon or the patient. In manypatients, these are complex surgical proceduresand placed in a very difficult anatomic location.For the most part, complications are rare andTMJ surgery can be done in a very successfulmanner. The advent of arthroscopic surgery hasminimized untoward events and has been a majorhelp to many surgical patients. Furthermore,simplifying many of the arthroplasty procedurescan be of benefit to patients and be performedin predictable and successful fashion with mini-mal complication rate. With regard to total jointreplacements, as more time passes and despitetheir potential complications, they have clearlybecome a predictable procedure that has minimalcomplications and a well-trained surgeon canperform in a very satisfying manner for both pa-tient and doctor. Clearly, as generations of sur-geons place prosthetic joints, the confidencelevel will build and they will hopefully find theirplace in treating the patients in a similar fashionfor surgical placement of hips and knees.
REFERENCES
1. Vallerand WP, Dolwick MF. Complications of TMJ
surgery. Oral Maxillofac Surg Clin North Am 1990;
3:481.
2. Kieth DA. Complications of temporomandibular joint
surgery. Oral Maxillofac Surg Clin North Am 2003;
15:187.
3. Van Sickels JE, Nishioka GJ, Hegewald MD, et al.
Middle ear injury resulting from temporomandibular
joint arthroscopy. JOralMaxillofac Surg 1987;45:962.
4. Westesson PL, Erickson L, Liedberg L. The risk of
damage to facial nerve, superficial temporal
vessels, discs, and articular surfaces during arthro-
scopic examination of the temporomandibular joint.
Oral Surg Oral Med Oral Pathol 1986;62:124.
5. McCain JP. Complication of TMJ arthroscopy. J Oral
Maxillofac Surg 1998;46:256.
6. Sugisaki M, Ikai A, Tanabe H. Dangerous angles and
depth for cranial fossa injury during arthroscopy of
the temporomandibular joint. J Oral Maxillofac
Surg 1995;53:803.
7. Sacho RH, Kryshtalskyj B, Krings T. Arteriovenous
fistula of the middle meningeal artery- A rare compli-
cation after arthroscopic temporomandibular joint
surgery readily amenable to endovascular treat-
ment. J Oral Maxillofac Surg 2014;72:1258.
8. Martın-Granizo R, Caniego JL, de Pedro M, et al.
Arteriovenous fistula after temporomandibular joint
arthroscopy successfully treated with embolization.
Int J Oral Maxillofac Surg 2004;33:301–3.
9. Roberts RS, Best JA, Shapiro RD. Trigeminocar-
diac reflex during temporomandibular joint arthros-
copy: report of a case. J Oral Maxillofac Surg
1999;57:854.
10. Gonzalez-Garcıa R, Rodrıguez-Campo FJ, Escorial-
Hernandez V, et al. Complications of temporoman-
dibular joint arthroscopy: a retrospective analytic
study of 670 arthroscopic procedures. J Oral Maxil-
lofac Surg 2006;64:11.
11. Chossegros C, Cheynet F, Conrath J. Infratemporal
space infection after temporomandibular arthros-
copy: an unusual complication. J Oral Maxillofac
Surg 1995;53:949.
12. Norden C, Gillespie WJ, Nade S. Infections in bones
and joints. Boston: Blackwell Scientific Publications;
1994. p. 291–319.
13. KruegerK,HoffmanD, StracherM, et al. Abstract pre-
sentation: “Infection of the temporomandibular joint
after surgery”, American Association of Oral and
Maxillofacial Surgeons 1996 Annual Meeting. The
Fountainbleau, Miami, Florida, September 20, 1996.
14. Tsuyama M, Kondoh T, Seto K, et al. Complications
of temporomandibular joint arthroscopy: a retro-
spective analysis of 301 lysis and lavage proce-
dures performed using the triangulation technique.
J Oral Maxillofac Surg 2000;58:500.

Hoffman & Puig124
15. Carter JB, Testa L. Complications of TMJ arthros-
copy: a review of 2225 cases. Review of the 1988
Annual Scientific Sessions Abstract. J Oral Maxillo-
fac Surg 1988;46:M14.
16. Gokkulakrishnan S, Singh S, Sharma A, et al. Facial
nerve injury following surgery for temporomandib-
ular joint ankylosis: a prospective clinical study.
Indian J Dent Res 2013;24:521.
17. US Food and Drug Administration. Serious problems
with proplast coated TMJ Implant. Rockville (MD):
Department of Health and Human Services; 1990.
18. Kearans GJ, Perrott DH, Kaban LB. A protocol for
the management of failed alloplastic temporoman-
dibular joint disc implants. J Oral Maxillofac Surg
1995;53:1240–7.
19. Sidebottom AJ, Speculand B, Hensher R. Foreign
body response around total prosthetic metal-on-
metal replacements of the temporomandibular
joint in the UK. Br J Oral Maxillofac Surg 2008;
46:288–92.
20. Mercuri LG, Psutka D. Perioperative, postoperative,
and prophylactic use of antibiotics in alloplastic total
joint temporomandibular joint replacement surgery:
a survey and preliminary guidelines. JOral Maxillofac
Surg 2011;69:2106.
21. Sidebottom AJ, Gruber E. One-year prospective
outcome analysis and complicationsfollowing total
replacement of the temporomandibular joint with
the TMJ Concepts system. Br J Oral Maxillofac
Surg 2013;51:620–4.
22. Lidgren L, Knutson K, Stefansdottir A. Infection of
prosthetic joints. Best Pract Res Clin Rheumatol
2003;17:209.
23. Mercuri L. Microbial biofilms: a potential source for
alloplastic device failure. J Oral Maxillofac Surg
2006;64:1303–9.