s. ida tmj
33
Transcript of s. ida tmj


INTRODUCTIONINTRODUCTIONThis joint is a typical sliding "ball and socket" that
has a disc sandwiched between it.The TMJ is used throughout the day to move the
jaw, especially in biting and chewing, talking,laughing and yawning.
It is one of the most frequently used joints of the body

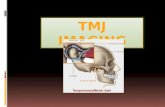
Radiographic lines and landmarks are important to skull positioning

Radiographic LandmarksGlabella: Triangular area
between and slightly superior to the eyebrows and above the bridge of the nose
Nasion: Depression at the bridge of the noseJunction of the two
nasal bones and the frontal bone

Radiographic LandmarksGonion: Angle of the mandible (Jaw)
Mental Point: A triangular area projects forward as the chin (mentum). The center of the mentum is the mental point

Radiographic LandmarksInner Canthus: Where
the eyelids meet near the nose
Outer Canthus: Lateral junction of the eyelids
Acanthion: Midline point at the junction of the upper lip and the nasal septum. Point where the nose and the upper lip meet

Radiographic LinesOrbitomeatal Line (OML):
Located between the outer canthus (midlateral orbital margin) and the EAM
Infraorbitomeatal Line (IOML): Formed by connecting the middle of the infraorbital margin to the EAM
Acanthiomeatal line
extending from the external acoustic meatus to the acanthion.

Radiographic PlanesInterpupillary Line
(IPL): A line connecting
either the pupils or the outer canthi of the patient’s eyes
The IPL must be exactly perpendicular to the IR in a TRUE LATERAL position

ArthrologyTemporomandibular Joint:
Only movable joints in the cranium
Formed by the mandibular fossa on each temporal bone with corresponding condyle of the mandible



TMJ Causes
can be caused by trauma, disease, wear and tear due to aging, or habits.

TMJ disordersTMJ disorders are also sometimes referred to as
myofacial pain dysfunction and Costen's syndrome. Because muscles and joints work together, a problem with either one can lead to stiffness, headaches, ear pain, bite problems (malocclusion), clicking sounds, or locked jaws.

TMJ Projection
AP Axial/TowneAxiolateral/ SchullersOrthopantogram (OPG)TMJ using an OPG machine

TECHNICAL FACTOR
PROJECTION TOWNE
PROJECTION AXIOLATERAL
SID 100cm 100cm
CASSETTE 24 X 30 24 X 30 (split)
FOCAL SPOT small small
TUBE ANGLE 35° caudad 25-30° caudad
EXPOSURE: KV 70-80 65-75
mAs 30-40 20-30
GRID yes yes
PROTECTION yes yes

TownesPatient Position
Patient supine.
All metal or plastic removable from head.
Part Position Patient supine.The chin is tucked into the
chest until the orbitomeatal line is perpendicular to cassette.
MSP of head perpendicular to the cassette.
Centre cassette to projected CR.
Collimation all sides to TMJ region
Central Ray CR pass through level of TMJs
1” or 2.5cm anterior EAMs



AXIOLATERAL PROJECTION

Part Position
i.MSP of head parallel to the cassette, affected side close to film
ii.InterPupillary line perpendicular to cassette
iii.Immobilise the head as necessary
Patient Positioni.Patient seated upright or semiprone
i.Adjust rotation of body so that the median sagittal of the head is parallel to the cassette
ii.Place the arms in a comfortable position

Central Rayi.Angle CR 25° -30° caudad. Centered to ½” anterior and 2” superior to upside EAM.
ii.Center cassette to projected TMJ
Collimation
Collimation on all sides approximately 10cm square.
AXIOLATERAL PROJECTION

Close mouthOpen mouth

IMAGE EVALUATION CRITERIA• Towne• Condyloid processes of mandible and temporomandibular fossae are shown.
• Condyloid processes visualization symmetrically lateral to the cervical spine.
• Collimation field includes the condyloid process of the mandible and the temporomandibular fossa.

IMAGE EVALUATION CRITERIA
Axiolateral
TMJ nearest the image receptor is visible.
TMJ anterior to EAM• close mouth - Condyle lying in mandibular fossa • open mouth – Condyle will move to anterior margin of fossa



With OPG

With OPG

TREATMENT
The mainstay of treatment for acute TMJ pain is heat and ice, soft diet, and anti-inflammatory medications.

TREATMENT1.Jaw rest: Patients are advised to avoid chewing
gum or eating hard crunchy foods such as raw vegetables, candy, or nuts. Foods that require opening the mouth widely, such as a big mac are also not recommended.
2.Heat and ice therapy: These assist in reducing muscle tension and spasm.
3.Medications: Anti-inflammatory medications, muscle relaxants such as aspirin, ibuprofen or steroids.

4.Physical therapy: Passively opening and closing the jaw, massage, and electrical stimulation help to decrease pain and increase the range of motion and strength of the joint. can help control inflammation.
5.Stress management: stress support groups, psychological counseling can also assist reducing muscle tension.
6.Occlusal therapy: A custom-made acrylic appliance which fits it acts to balance the bite and reduce or eliminate teeth grinding or clenching.

7.Correction of bite abnormalities: corrective dental therapy, such as orthodontics. Adjustments of bridges or crowns act to ensure proper alignment of the teeth.
8.Surgery: It is done as a last resort. TMJ arthroscopy, ligament tightening, joint restructuring, and joint replacement are considered in the most severe cases of joint damage or deterioration.