COMMERCIAL SERODIAGNOSTIC TESTS FOR DIAGNOSIS...
72
COMMERCIAL SERODIAGNOSTIC TESTS FOR DIAGNOSIS OF TUBERCULOSIS EXPERT GROUP MEETING REPORT 22 July 2010 This report contains the collective views of an international group of experts, and does not necessarily represent the decisions or the stated policy of the World Health Organization. Mention of a technology does not imply endorsement of any specific commercial product.
Transcript of COMMERCIAL SERODIAGNOSTIC TESTS FOR DIAGNOSIS...

COMMERCIAL SERODIAGNOSTIC TESTS
FOR DIAGNOSIS OF TUBERCULOSIS
EXPERT GROUP MEETING REPORT 22 July 2010
This report contains the collective views of an international group of experts, and does not
necessarily represent the decisions or the stated policy of the World Health Organization. Mention of a technology does not imply endorsement of any specific commercial product.

© World Health Organization 2011
All rights reserved. Publications of the World Health Organization are available on the WHO web site
(www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211
Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial
distribution – should be addressed to WHO Press through the WHO web site
(http://www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the
expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status
of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or
boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full
agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are
endorsed or recommended by the World Health Organization in preference to others of a similar nature that
are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by
initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information
contained in this publication. However, the published material is being distributed without warranty of any
kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the
reader. In no event shall the World Health Organization be liable for damages arising from its use.
Printed in Switzerland
WHO/HTM/TB/2011.14

Executive summary
Background: An antibody detection-based diagnostic test in a suitable format could potentially
replace microscopy and extend tuberculosis diagnosis to lower levels of health services. Dozens of
commercial serological tests for tuberculosis are being marketed in many parts of the world, despite
previous systematic reviews having reported variable sensitivity and specificity of these tests. Since
the publication of these reviews, the evidence base has grown, methods for meta-analyses of
diagnostic tests have evolved, and WHO Stop TB Department (STB) has implemented a systematic
approach to evidence synthesis for TB diagnostic policy development involving systematic reviews
and meta-analyses, assessment of the evidence base by Expert Group review, and implementation
of the GRADE process for evidence synthesis.
Methods: An updated systematic review was commissioned to synthesize the evidence on the
diagnostic accuracy of commercial serological tests for pulmonary and extrapulmonary tuberculosis.
Database searches for relevant studies in all languages were updated through May 2010 and a
bivariate meta-analysis that jointly models both sensitivity and specificity was performed. The
findings were presented to a WHO Expert Group and the evidence assessed using the GRADE
approach. This report reflects the outcomes of the Expert Group meeting and the consensus
recommendations.
Results: For pulmonary tuberculosis, 67 unique studies were identified, including 32 studies from
low- and middle-income countries. None of these studies evaluated the tests in children. The results
demonstrated that (1) for all commercial tests, sensitivity (0% to 100%) and specificity (31% to
100%) from individual studies were highly variable; (2) using bivariate meta-analysis, for Anda-TB IgG
(the most commonly evaluated test), the pooled sensitivity was 76% (95% CI 63% to 87%) in studies
of smear-positive and 59% (95% CI 10% to 96%) in studies of smear-negative patients, respectively;
the pooled specificity in these studies was similar: 92% (95% CI 74% to 98%) and 91% (95% CI 79% to
96%), respectively; (3) for Anda-TB IgG, sensitivity values in smear-positive (54% to 85%) and smear-
negative (35% to 73% ) patients from individual studies were highly variable; (4) for Anda-TB IgG,
specificity values from individual studies were variable (68% to 100%); (5) a TDR evaluation of 19
rapid commercial tests, in comparison with culture plus clinical follow-up, showed similar variability
with sensitivity values of 1% to 60% and specificity of 53% to 99%; (6) compared with ELISAs [60%
(95% CI 6% to 65%], immuno-chromatographic assays had lower sensitivity [53%, 95% CI 42% to
64%]; and (7) in a single study involving HIV-infected TB patients, the sensitivity of the SDHO test
was 16% (95% CI 5% to 34%).
For extrapulmonary tuberculosis, 25 unique studies were identified, including 10 studies from low-
and middle-income countries. None of these studies evaluated the tests in children. The results
demonstrated that (1) for all commercial tests, sensitivity (0% to 100%) and specificity (59% to
100%) values from individual studies were highly variable; (2) pooled sensitivity was 64% (95% CI
28% to 92%) for lymph node tuberculosis and 46% (95% CI 29% to 63%) for pleural tuberculosis; (3)
for Anda-TB IgG, although the pooled sensitivity and specificity were 81% (95% CI 49% to 97%) and
85% (95% CI 77% to 92%) respectively, sensitivity (26% to 100%) and specificity (59% to 100%) values
from individual studies were equally variable; and (5) in one study involving HIV-infected TB patients,
the sensitivity of the MycoDot test was 33% (95% CI 19% to 39%).
Conclusions: Commercial serological tests provide inconsistent and imprecise estimates of sensitivity
and specificity. There is no evidence that existing commercial serological assays improve patient-
important outcomes. Overall data quality was graded as very low and the Expert Group strongly
recommended that these tests not be used for the diagnosis of pulmonary and extra-pulmonary TB.

Contents
1. BACKGROUND ......................................................................................................................................... 1
2. EVIDENCE BASE ....................................................................................................................................... 2
2.1 EVIDENCE SYNTHESIS ................................................................................................................................... 2
2.1.1 Systematic review and meta-analyses .............................................................................................. 2
2.1.2 WHO/TDR laboratory-based evaluation of 19 commercially available rapid diagnostic tests for
tuberculosis .................................................................................................................................................... 3
2.2 CASE STUDY) OF ECONOMIC AND EPIDEMIOLOGICAL IMPACT OF SEROLOGIC TESTING FOR ACTIVE TUBERCULOSIS IN INDIA 3
2.3 GRADE EVALUATION.................................................................................................................................. 4
2.4 MEETING PROCEDURAL ISSUES ...................................................................................................................... 5
3. RESULTS .................................................................................................................................................. 7
3.1 COMMERCIAL DIAGNOSTICS IN PULMONARY TB: PERFORMANCE CHARACTERISTICS.................................................. 7
3.1.1 Studies included ................................................................................................................................ 7
3.1.2 Methodological quality ..................................................................................................................... 9
3.1.3 Test performance overall ................................................................................................................ 12
3.1.3 Individual test performance ............................................................................................................ 16
3.1.5 Results from meta-analysis ............................................................................................................. 20
3.1.6 Results in HIV-infected TB patients ................................................................................................. 23
3.2 FINDINGS FROM THE WHO/TDR LABORATORY-BASED EVALUATION .................................................................. 23
3.3 PERFORMANCE CHARACTERISTICS OF COMMERCIAL SERODIAGNOSTICS IN EXTRA-PULMONARY TB ........................... 25
3.3.1 Studies included .............................................................................................................................. 25
3.3.2 Methodological quality ................................................................................................................... 25
3.3.3 Test performance by site of disease ................................................................................................ 26
3.3.4 Individual test performance ............................................................................................................ 27
3.3.5 Results from meta-analysis ............................................................................................................. 28
3.3.6 Results in HIV-infected TB patients ................................................................................................. 29
3.4 ECONOMIC AND EPIDEMIOLOGICAL IMPACT OF TB SERODIAGNOSTICS IN INDIA ........................................................... 29
4. SUMMARY OF FINDINGS AND GRADE EVIDENCE PROFILES ................................................................... 31
4.1 PULMONARY TB ...................................................................................................................................... 31
4.2 EXTRA-PULMONARY TB ............................................................................................................................. 31
4.3 STRENGTHS AND LIMITATIONS OF THE EVIDENCE BASE ..................................................................................... 32
4.4 GRADE EVIDENCE PROFILES AND FINAL RECOMMENDATIONS ........................................................................... 33
5. RESEARCH GAPS .................................................................................................................................... 42
6. REFERENCES .......................................................................................................................................... 42

List of Tables TABLE 1. QUADAS TOOL ......................................................................................................................................... 5
TABLE 2. COMMERCIAL SEROLOGICAL TESTS INCLUDED IN THE SYSTEMATIC REVIEW .............................................................. 7
TABLE 3. BIVARIATE META-ANALYSES: POOLED SENSITIVITY AND SPECIFICITY ESTIMATES BY SUBGROUP; POSTERIOR MEANS WITH
95% CREDIBLE INTERVALS IN PARENTHESES ............................................................................................................ 21
TABLE 4. TDR EVALUATION: PERFORMANCE OF 19 RAPID TESTS FOR PULMONARY TUBERCULOSIS........................................ 24
TABLE 5. SHOULD COMMERCIAL SEROLOGICAL TESTS BE USED AS A REPLACEMENT TEST FOR CONVENTIONAL TESTS SUCH AS SMEAR
MICROSCOPY IN PATIENTS SUSPECTED OF HAVING PULMONARY TUBERCULOSIS? ............................................................ 34
TABLE 6. SHOULD COMMERCIAL SEROLOGICAL TESTS BE USED AS AN ADD-ON TO CONVENTIONAL TESTS SUCH AS SMEAR
MICROSCOPY IN PATIENTS SUSPECTED OF HAVING PULMONARY TUBERCULOSIS? ............................................................ 36
TABLE 7. DIAGNOSTIC ACCURACY OF ANDA-TB IGG .................................................................................................... 38
TABLE 8. DIAGNOSTIC ACCURACY OF ANDA-TB IGG IN STUDIES OF SMEAR-NEGATIVE PATIENTS (IE. AS AN ‘ADD ON’ TEST TO SMEAR
MICROSCOPY) ................................................................................................................................................... 40
List of Figures
FIGURE 1. SUMMARY OF METHODOLOGICAL QUALITY SUMMARY: STUDIES ON PULMONARY TB ........................................ 11
FIGURE 2. METHODOLOGICAL QUALITY BY AUTHOR, PULMONARY TB, ALL COMMERCIAL TESTS, STUDIES OF SMEAR-NEGATIVE
PATIENTS 12
FIGURE 3. FOREST PLOT OF SENSITIVITY, ALL INCLUDED STUDIES, ALL COMMERCIAL TESTS ................................................. 13
FIGURE 4. FOREST PLOT OF SPECIFICITY, ALL INCLUDED STUDIES, ALL COMMERCIAL TESTS ................................................. 14
FIGURE 5. FOREST PLOT OF SENSITIVITY, ALL COMMERCIAL TESTS, SMEAR-NEGATIVE PATIENTS .......................................... 15
FIGURE 6. FOREST PLOT OF SPECIFICITY, ALL COMMERCIAL TESTS, SMEAR-NEGATIVE PATIENTS ........................................... 15
FIGURE 7. METHODOLOGICAL QUALITY: ANDA-TB, IGG, SMEAR-POSITIVE PULMONARY TB ............................................. 16
FIGURE 8. METHODOLOGICAL QUALITY: ANDA-TB, IGG, SMEAR-NEGATIVE/CULTURE-POSITIVE PULMONARY TB ................. 17
FIGURE 9. FOREST PLOTS: ANDA-TB, IGG, SMEAR-POSITIVE PULMONARY TB ................................................................ 17
FIGURE 10. FOREST PLOTS: ANDA-TB, IGG, SMEAR-NEGATIVE/CULTURE-POSITIVE PULMONARY TB .................................... 18
FIGURE 11. METHODOLOGICAL QUALITY: PATHOZYME MYCO, IGG, IGM AND IGA. ......................................................... 18
FIGURE 12. FOREST PLOTS: PATHOZYME MYCO-G, M, AND A. G = IGG ........................................................................ 19
FIGURE 13. METHODOLOGICAL QUALITY GRAPH FOR DETERMINER TB GLYCOLIPID ASSAY .................................................. 20
FIGURE 14. FOREST PLOTS: DETERMINER TB GLYCOLIPID ASSAY .................................................................................. 20
FIGURE 15. SUMMARY ROC PLOTS OF SENSITIVITY AND SPECIFICITY FOR ANDA-TB IGG .................................................... 22
FIGURE 16. SUMMARY ROC PLOTS OF SENSITIVITY AND SPECIFICITY BY ASSAY TECHNIQUE .................................................. 23
FIGURE 17. METHODOLOGICAL QUALITY: EXTRAPULMONARY TB .................................................................................. 25
FIGURE 18. METHODOLOGICAL QUALITY: LYMPH NODE TB .......................................................................................... 26
FIGURE 19. FOREST PLOTS: ALL COMMERCIAL TESTS, LYMPH NODE TB ............................................................................ 26
FIGURE 20. METHODOLOGICAL QUALITY GRAPH, PLEURAL TB ....................................................................................... 27
FIGURE 21. FOREST PLOTS: ALL COMMERCIAL TESTS, PLEURAL TB ................................................................................. 27
FIGURE 22. METHODOLOGICAL QUALITY: ANDA-TB IGG, EXTRAPULMONARY TB, ALL SITES OF DISEASE ............................... 28
FIGURE 23. FOREST PLOTS: ANDA-TB IGG, EXTRAPULMONARY TB, ALL SITES OF DISEASE .................................................. 28
FIGURE 24. COST FOR 1.5 MILLION TB SUSPECTS UNDERGOING SEROLOGIC TESTING IN INDIA ............................................. 29
FIGURE 25. GAINS FROM INVESTMENT IN DIFFERENT DIAGNOSTIC TESTS IN INDIA ............................................................. 30

Annexes Annex 1: Meeting background and objectives Annex 2: Agenda Annex 3: Meeting participants Annex 4: Declarations of Interest Annex 5: Included studies Annex 6: Excluded studies

Page | 1
COMMERCIAL SERODIAGNOSTIC TESTS FOR DIAGNOSIS OF TUBERCULOSIS
1. BACKGROUND
Tuberculosis (TB) serological tests almost exclusively rely on antibody recognition of antigens of M.
tuberculosis by the humoral immune response, as opposed to antigen recognition by the cellular
immune response (e.g. interferon-gamma release assays). An accurate serological test could provide
rapid diagnosis of TB and in a suitable format (e.g. point-of-care) would be particularly useful both as
a replacement for laboratory-based tests and for extending TB diagnosis to lower levels of health
services, especially those without on-site laboratories. Although no serological TB test is
recommended by international guidelines for clinical use nor approved by the US Food and Drug
Administration, dozens of distinct commercial serological tests (also referred to as commercial
serodiagnostics in this document) are marketed in many parts of the world, especially in developing
countries with weak regulatory systems.
Several systematic reviews and one laboratory-based evaluation on this topic have been published.
Two reviews evaluating commercial tests for pulmonary TB (68 studies) and extrapulmonary TB (21
studies) found sensitivity and specificity of these tests to be highly variable.1-3 A meta-analysis of
non-commercial tests for pulmonary TB (254 datasets including 51 distinct single antigens and 30
distinct multiple-antigen combinations) identified potential candidate antigens for inclusion in an
antibody detection based TB test in HIV-uninfected and -infected individuals; however, no antigen or
antigen combination achieved sufficient sensitivity to replace smear microscopy.2 A previous
systematic review by Dinnes and colleagues of rapid TB diagnostic tests (literature search through
2003, seven datasets) reported pooled sensitivity and specificity values of 34% and 91%, respectively
in studies meeting at least two design-related criteria.4
In 2005, the UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in
Tropical Diseases (TDR) performed an evaluation of 19 commercially available rapid diagnostic TB
tests (‘rapid’ defined as having a test result available in less than 15 minutes).5 The evaluation
reported that, in comparison with culture plus clinical follow-up, commercial tests provided
sensitivity and specificity values of 1% to 60% and 53% to 99%, respectively.
Since the publication of previous reviews, the evidence base has grown and approaches to meta-
analyses of diagnostic tests have evolved. WHO-STB and TDR therefore commissioned an updated
systematic review to synthesize new evidence since 2006 on the diagnostic accuracy of commercial
tests for pulmonary and extrapulmonary TB. In addition, the findings from the previous TDR
evaluation are summarised below.
The systematic review and this document are limited to commercial serological tests only. In-house
tests are likely to be less standardised, have less quality assurance during manufacture, and are
prone to be more operator dependent. As a result, the quality issues of limitations, precision,
consistency, directness and probably publication bias are expected to be more severe.

Page | 2
2. EVIDENCE BASE
2.1 Evidence synthesis
The systematic, structured, evidence-based process for TB diagnostic policy generation developed by
WHO-STB was followed: The first step constituted a systematic review and meta-analysis of
available data (published and unpublished) using standard methods appropriate for diagnostic
accuracy studies. The second step involved the convening of an Expert Group to a) evaluate the
strength of the evidence base; b) recommend operational and logistical considerations for
mainstreaming such the methods/approaches into national TB control programmes; and c) identify
gaps to be addressed in future research. Based on the Expert Group findings, the third and final step
involves WHO policy guidance on the use of these tools/approaches, presented to the WHO
Strategic and Technical Advisory Group for TB (STAG-TB) for consideration, and eventual
dissemination to WHO Member States for implementation.
The Expert Group (Annex 1) consisted of researchers, clinicians, epidemiologists, end-users
(programme and laboratory representatives), community representatives and evidence synthesis
experts. The Expert Group meeting followed a structured agenda (Annex 1) and was co-chaired by
WHO and a clinical epidemiologist with expertise and extensive experience in evidence synthesis and
guideline development.
To comply with current standards for evidence assessment in formulation of policy
recommendations, the GRADE system (www.gradeworkinggroup.org), adopted by WHO for all policy
and guidelines development, was used. The GRADE approach, assessing both the quality of evidence
and strength of recommendations, aims to provide a comprehensive and transparent approach for
developing policy guidance. Started about 10 years ago to assess treatment interventions, the
GRADE approach has recently been refined for diagnostics; however, while the latter process shares
the fundamental logic of recommendations for other interventions (notably treatment), it also
presents unique challenges, most often due to study limitations related to a lack of data on patient-
important outcomes and impact (see below).
Recognising that test results may be surrogates for patient-important outcomes, the Expert Group
evaluated diagnostic accuracy while also drawing inferences on the likely impact of these
approaches on patient outcomes, as reflected by false-negatives (i.e. cases missed) or false-
positives. In addition, the Expert Group was presented with an epidemiological and economic model
on the cost-effectiveness and cost-benefit of commercial serodiagnostics using a case study from
India, where an estimated 1.5 million TB commercial (ELISA) tests are performed every year. These
tests are used mostly by the private sector (the primary source for TB care) in India, predominantly
using imported TB ELISA kits at an expenditure conservatively estimated at 15 million US dollars per
year (Dowdy and Pai, unpublished information).
2.1.1 Systematic review and meta-analyses
An updated systematic review was done following standard protocols and using predetermined
eligibility criteria for primary analyses of diagnostic accuracy of commercial serological tests, for
both pulmonary and extra-pulmonary TB. Detailed methodology is described in the systematic
review report available at www.who.int/tb/dots/laboratory/policy. In summary, database searches
for relevant studies from 1990 through May 2010 in all languages were updated and summarised,
and a bivariate meta-analysis was performed which jointly models sensitivity and specificity.
Hierarchical receiver operating characteristic (HSROC) curves from relevant meta-analyses were
done. The HSROC curve gives an idea of the overall performance of a test across different
thresholds. The closer the curve is to the upper left hand corner of the plot (sensitivity and
specificity both 100%), the better the performance of the test.

Page | 3
Studies were heterogeneous in many respects, particularly concerning the commercial test
evaluated, antibody (ies) detected, sputum smear status (pulmonary TB), site of extrapulmonary TB,
and assay technique. Therefore, in order to address heterogeneity and combine study results,
subgroups of comparable tests and extrapulmonary sites were pre-specified. When possible, studies
were stratified by smear and HIV status.
Studies using culture of M. tuberculosis from patient specimens as the reference standard were
included for pulmonary tuberculosis. For extra-pulmonary TB, studies using microscopy, culture or
histopathology as reference standard were included. The following studies were excluded: (1)
studies published before 1990; (2) animal studies; (3) conference abstracts and proceedings; (4)
studies on the detection of latent TB infection; (5) studies on nontuberculous mycobacterial
infection; (6) studies that used non-immunological methods for detection antibodies; and (7) basic
science literature that focused on detection/cloning of new antigens or their immunological
properties (i.e. early pre-clinical studies).
2.1.2 WHO/TDR laboratory-based evaluation of 19 commercially available
rapid diagnostic tests for tuberculosis
The TDR test data were synthesised separately since this evaluation was a head-to-head comparison
of rapid point of care tests whose performance was assessed with the same archived frozen
specimens. Because of this unique design, it was preferable not to pool data from the TDR
evaluation with data from the systematic review. The objective of the evaluation was two-fold: (1)
to compare the performance and reproducibility of rapid M. tuberculosis-specific antibody detection
tests using well-characterized serum samples from the WHO/TDR TB Specimen Bank and (2) to
assess the operational characteristics of rapid M. tuberculosis tests, including ease of use, technical
complexity, and inter-reader variability.
Details regarding the analyses can be found in the systematic review report available at
www.who.int/tb/dots/laboratory/policy.
The TDR report is available on http://apps.who.int/tdr/svc/publications/tdr-research-
publications/diagnostics-evaluation-2.
2.2 Case study) of economic and epidemiological impact of serologic testing for active tuberculosis in India
As no data were available on the cost implications of commercial serodiagnostics, a case study of
serologic testing for TB in India was performed, including construction of a decision-analytic model
to estimate the impact of such testing. India is the country with the greatest burden of TB, nearly 2
million incident cases per year. Conservatively, over 10 million TB suspects need diagnostic testing
for TB each year. Findings were presented from a recent in-country survey done for the Bill &
Melinda Gates Foundation (Pai M, personal communication). According to this survey, the market
for TB serology in India exceeds that for sputum smear and TB culture; six major private lab
networks (out of hundreds) perform >500,000 TB ELISA tests each year, at a cost of approximately
$10 per test or $30 per patient (for three simultaneous tests). Most serological tests on the market
in India have no published evidence to support their claims of sensitivity and specificity (usually in
excess of 95% each, according to package inserts). These tests are performed in an environment
with no external quality assurance, and tests from different labs on specimens from the same
patient often yield widely varying results.
Current approaches to modeling diagnostic tests for TB have several limitations. These include
treatment of the diagnostic process as a ‘once-only’ process, failure to fully account for the adverse
impact of false-positive diagnosis, and the implicit assumption that TB resources are unlimited. With

Page | 4
these limitations in mind, a decision analysis model was constructed (Dowdy, personal
communication) using the framework of a previously-published model designed to evaluate the
economic and epidemiological impact of novel diagnostic tests for TB.6 This model was adapted by
changing all country-specific parameters to those representative of India, using data from the 2009
WHO Global TB Report, and inserting pooled accuracy (sensitivity and specificity) values for Anda-TB
IgG, the most commonly used TB serologic test in India, from the systematic review described in
other sections of this report.
For the estimate of specificity, data from studies using a cross-sectional design only were used (ie.
where ‘controls’ were not deliberately selected by the authors. This model was used to project the
impact of serological testing (at $20/patient) in a population of 1.5 million TB suspects, a
conservative estimate of the market for TB serologics in India, assuming that one in seven TB
suspects actually has TB (Dowdy, personal communication). The impact of serological testing was
compared against that of other testing modalities (sputum smear, TB culture, conventional nucleic
acid amplification testing (NAAT) as well as improved NAATs, and sensitivity analysis was performed
around the accuracy of the test and the annual number of tests performed (results summarised
below).
2.3 GRADE evaluation
Evaluation followed the GRADE system for grading quality of evidence and strength of
recommendations for diagnostic tests. The quality of evidence was evaluated according to six
criteria:
Overall study design
Cross-sectional: Random or consecutive selection of patients/specimens at risk (preferred);
Case-control: Selection of patients/specimens according to reference standard.
Risk of bias (as reflected by the QUADAS tool) or limitations in study design and execution
Compliance of studies with a subset of 14 independent quality assessment criteria (Table 1).
Directness
Presence of direct evidence of impact on patient-important outcomes and generalisability in
relation to the population, the diagnostic tests used, the comparator of the test and whether
tests were directly or indirectly compared.
Inconsistency
Unexplained inconsistency in sensitivity or specificity estimates.
Imprecision
Wide confidence intervals for pooled sensitivity or specificity estimates.
Publication bias
Publications of research based on their nature and outcome, e.g. studies showing poor performance
not being published, language bias, etc.
Study limitations were assessed by using a subset (11/14 items) from QUADAS (Quality Assessment
of Diagnostic Accuracy Studies), a validated tool for diagnostic studies.

Page | 5
Table 1. QUADAS tool
Conflicts of interest are a known concern; therefore, the systematic reviews evaluated the
involvement of commercial test manufacturers in published studies.
As called for by GRADE, the Expert Group also considered for each method/approach the strength of
the recommendation (strong or conditional/weak), based on a balance of effects (benefits weighed
against downsides), patient values and preferences, and costs.
Given the absence of relevant data from the studies reviewed, assumed patient values and
preferences were assessed as a proxy measure, based on the relative importance/impact of false-
positive and false-negative results:
True positives: Benefit to patients from earliest diagnosis and treatment;
True negatives: Patients spared unnecessary treatment; benefit of reassurance and alternative
diagnosis;
False positives: Likely patient anxiety and morbidity from additional testing, unnecessary treatment;
may halt further diagnostic evaluation;
False negatives: Increased risk of patient morbidity and mortality, and continued risk of community
transmission of TB.
2.4 Meeting procedural issues
The systematic review report as well as the TDR report was made available to the Expert Group for
scrutiny before the meeting.
As agreed, interchange by Expert Group meeting participants was restricted to those who attended
the Expert Group meeting in person, both for the discussion and follow-up dialogue.
WHO is committed to ensuring that the highest standards of evidence are used in formulation of
recommendations and has therefore standardised the synthesis process based on the GRADE
approach. The first paper specifically addressing the GRADE approach to diagnostic tests and

Page | 6
strategies was published in 2008 (Schunemann. BMJ 2008; 336:1106-1110) and was made available
to the Expert Group in the background documentation for the meeting.
It was explained that individuals were selected to be members of the Expert Group to carefully
represent and balance important perspectives for the process of formulating recommendations.
Therefore the Expert Group included technical experts, end-users, patient representatives and
evidence synthesis methodologists.
Expert Group members were asked to submit completed Declaration of Interest (DOI) forms. These were reviewed by the WHO legal department prior to the Expert Group meeting. A summary is attached in Annex 2. DOI statements were summarized by the co-chair (WHO-STB) of the Expert Group meeting at the start of the meeting. Selected individuals with intellectual and/or research involvement in the methods were invited as observers to provide technical input and answer technical questions. These individuals did not participate in the GRADE evaluation process and were excluded from the Expert Group discussions when recommendations were developed. They were also not involved in the development of the final Expert Group meeting reports, nor in preparation of the STAG-TB documentation or preparation of the final WHO policy statements.

Page | 7
3. RESULTS
3.1 Commercial diagnostics in pulmonary TB: performance characteristics
3.1.1 Studies included
4,256 citations were identified and 160 full-text articles reviewed. Thirty-one publications including
67 studies (datasets) met the eligibility criteria. A list of included and excluded studies and the
reasons for exclusion are presented in Annex 3.
Of the 67 included studies, six (9%) were reported in languages other than English: Spanish (2),
Turkish (1), Chinese (1), Bosnian (1), Russian (1). Thirty-two (48%) studies were conducted in
low/middle-income countries. One study involved HIV-infected individuals and no studies involved
children. 31 (46%) studies involved smear–positive patients, 28 (42%) studies involved smear–
negative patients, and eight (12%) studies did not report smear status.
The median number of TB patients was 41 (range 33 to 54). Eighteen commercial tests were
evaluated (Table 2). The antigen composition for five (28%) of these tests was proprietary and
therefore not available. Of the tests with known antigens, all had unique antigenic compositions
except for Anda-TB and Hexagon which both include Ag60.
Fifty-four (81%) studies used ELISA, 12 (18%) studies used an immunochromatographic assay, and
one study used a kaolin precipitation test. The majority of studies detected only IgG antibody (44
studies) and used frozen serum (51 studies).
Table 2. Commercial serological tests included in the systematic review
Name of Manufacturer,a
City, Country
Name of Test
(No. of studies)
Antigenic Composition Antibodies
Detected
Laboratory
Technique
1 Adaltis – Advanced
Laboratory Diagnostics
Systems, Rome, Italy
Detect-TB
(2)
Proprietary, a cocktail of
3 M. TB recombinant
proteins and two
synthetic peptides from
5 different proteins
IgG ELISA
2 Anda Biologicals,
Strasbourg, France
Anda TB-ELISAb
(16)
A60 IgG, IgM,
IgA and
IgG plus M
ELISA
3 Chengdu Pharmaceutical,
Chengdu, China
Tuberculosis
Specific Antigen
(1)
Proprietary Unknown ELISA
4 Hitech Laboratories,
Bombay, India
Kaolin
Agglutination Test
(1)
Tuberculophosphatide IgG Agglutination
test
5 Human Geselschaft fur
Biochemica und
Diagnostica, Wiesbaden,
Germany
Hexagon TB
(1)
A60 IgG, IgA,
IgM
ICT

Page | 8
6 IBL, Hamburg, Germany Mycobacterium
tuberculosis IgG
(1)
18-, 36-, and 40-kDa
recombinant antigens
IgG, IgA,
IgM
ELISA
7 ICT Diagnostics, Sydney,
Australia
ICT TB
(3)
38 kDa and four
proprietary antigens; all
5 antigens are
recombinant
IgG ICT
8 InBios International,
Seattle, US
ActiveTBDetect
(1)
Mtb81, Mtb8, Mtb48,
DPEP (MPT32), 38-kDa
protein, and two
additional proprietary
antigens
IgG ELISA
9 Jamnalal Bajaj Tropical
Disease Research Centre,
Mahatma Gandhi
Institute of Medical
Sciences, Maharashtra,
India
SEVA
(1)
31 kDa, Native
glycoprotein antigen
from culture filtrate of
MTB H37Rv
IgG ELISA
10 Kreatech, Amsterdam,
The Netherlands
TB Enzyme
Immunoassay
(5)
Kp-90 antigenic
compound: LAM, 10
kDa, 16 kDa, 21 kDa, 30
kDa, 34 kDa, 65 kDa, and
95 kDa
IgG, IgA ELISA
11 Kyowa Medex Co, Ltd,
Tokyo, Japan
Determiner TB
Glycolipid Assay
(6)
Contains: trehalose 6,6’-
dimycolate and
trehalose
monomycolate,
diacyltrehalose, phenolic
glycolipid, 2,3,6,6-
tetraacyl-trehalose-2-
sulfate, and 2,3,6-
triacyl-trehalose
IgG ELISA
12 MedTek. Paranque
City,the Philippines; and
Genelabs Diagnostics,
Singapore
Assure TB
(2)
Proprietary; 2
recombinant antigens
IgG ICT
13 Mossman Associates,
Blackstone, MA, US
MycoDot
(3)
LAM IgG ICT
14 Omega Diagnostics, Alva,
Scotland
Pathozyme Mycoc
(11)
LAM, recombinant 38
kDa
IgG, IgA,
IgM
ELISA
15 Omega Diagnostics, Alva,
Scotland
Pathozyme TB
Complex
Recombinant 38 kDa IgG ELISA

Page | 9
(2)
16 Omega Diagnostics, Alva,
Scotland
Pathozyme TB
Complex Plusd
(9)
Recombinant 38kDa and
16 kDa
IgG ELISA
17 SDHO Laboratories Inc.,
Saint-Sauveur des Monts,
Canada
SDHO MTB
(1)
Proprietary IgG ICT
18 Zephyr Biomedicals,
Verna, Goa, India
Serocheck-MTB
(1)
Recombinant 14 kDa, 38
kDa, 16 kDa, and 6 kDa
Unknown ICT
ELISA=enzyme-linked immunosorbent assay; kDa=kilodalton; ICT, immunochromatographic test; LAM, lipoarabinomannan
aSome manufacturers may no longer provide the commercial tests listed above. It is also possible that the same test may
be marketed under various names by various companies.
bAnda-TB: IgG = 13 studies, IgM = 1 study; IgA = 2 studies
cPathozyme Myco: IgG = 3 studies, IgM = 2 studies; IgA = 2 studies; IgG plus IgM = 1 study; IgG plus IgA = 1 study; IgM plus
IgA = 1 study; IgG plus IgM plus IgA = 1 study
dPathozyme TB Complex Plus as a single test (3 studies) or in combination with Pathozyme Myco G (1 study); Pathozyme
Myco M (1 study); Pathozyme Myco A (1 study); Pathozyme Myco G and A (1 study); Pathozyme Myco M and A (1 study); Pathozyme Myco G, M, and A (1 study)
One study directly compared a commercial test to sputum microscopy. No studies evaluated the incremental value by multivariable analysis of adding a commercial test after smear examination for acid-fast bacilli. However, as noted, 28 (42%) studies involved smear–negative patients. These studies were considered to provide a proxy for accuracy of a diagnostic strategy using a serological test as an additional test after smear microscopy. No studies reported on patient-important outcomes or patient values and preferences concerning these tests.
Characteristics of included studies stratified by type of commercial test are presented in the
systematic review report available at www.who.int/tb/dots/laboratory/policy.
3.1.2 Methodological quality
Methodological quality was considered by paper (n=31) and by individual study/dataset (n=67), for
all patients and for smear-negative patients respectively.
Methodological quality of included studies is presented in Figure 1 (all patients) and Figure 2 (smear-
negative patients).
For all patients, study quality by paper suffered from lack of a representative patient spectrum, as
only 13% (4/31) of papers were considered to include a representative sample. Blinding of
commercial test results to culture was also rarely reported (11/31 papers).
When assessed by individual study, 37/67 (55%) studies used a cross-sectional design and 30/67
(45%) studies used a case-control design. Only 19/67 (28%) studies were considered to include a
representative sample. Ten of the 30 case-control studies involved healthy controls. These studies
were not considered as having a representative patient spectrum. 27/67 (40%) of studies recruited
patients in a consecutive manner. 29/67 (43%) studies were conducted in an outpatient setting.
Blinding of commercial test results was reported in 34/67 (51%) studies.

Page | 10
In studies involving smear-negative patients, overall study quality suffered from lack of a
representative patient spectrum as only 1/12 (8%) papers was considered to include a
representative sample. Blinding of commercial test results to culture was reported in 5/12 (42%)
papers. When considered by individual study, 21/28 (75%) studies used a cross-sectional design and
7/28 (25%) used a case-control design. 17/28 (61%) studies recruited patients in a consecutive
manner; 18/28 (64%) studies were conducted in an outpatient setting. Blinding of the commercial
test result was reported in 18/28 (64%) studies.
Studies involving smear-negative patients were taken as a proxy for studies of the strategy of using
commercial tests as an addition to sputum microscopy. The estimates of sensitivity and specificity
were therefore assumed to apply also to the use of commercial tests as an ‘add on’ test.

Page | 11
Figure 1. Summary of methodological quality summary: Studies on pulmonary TB

Page | 12
Figure 2. Methodological quality by author, pulmonary TB, all commercial tests, studies of
smear-negative patients
3.1.3 Test performance overall
Test performance was considered for all patients and for smear-negative patients respectively.
For all patients, sensitivity values ranged from 0% to 100% (Figure 3) and specificity values from 31%
to 100%, (Figure 4). Accuracy estimates were not pooled because of significant heterogeneity
among studies: sensitivity median = 64%, I-square = 89.6%; p = 0.0000; specificity median = 91%, I-
square = 93.8%; p = 0.0000. For the subset of studies conducted in low- and middle-income,
sensitivity (16% to 91%) and specificity (31% to 100%) values of commercial tests were similarly
inconsistent (data not shown).
For studies involving smear-negative patients, sensitivity values ranged from 29% to 77% (Figure 5)
and specificity values from 77% to 100% (Figure 6). Accuracy estimates were not pooled because of
the considerable heterogeneity among studies: sensitivity median = 61%, I -square = 72.5%; p =
0.0000; specificity median = 92% I-square = 72.1%; p = 0.0000. Hence, when used as an ‘add on’
test, commercial tests showed inconsistent sensitivity and specificity.
Calculating the number of false-positive and false-negative results under different scenarios of TB
prevalence showed that the false-positivity rate using commercial serodiagnostics increases as the
prevalence of TB decreases. Since TB prevalence is lower in smear-negative TB cases this suggests
that serologic tests used in this group would lead to an unacceptably high false-positive rate (data
not shown).

Page | 13
Figure 3. Forest plot of sensitivity, all included studies, all commercial tests
Sensitivity 0 0.2 0.4 0.6 0.8 1
Alifano 1994 0.83 (0.69 - 0.93) Alifano 1996a 0.85 (0.68 - 0.95) Alifano 1996b 0.82 (0.65 - 0.93) Alifano 1996c 0.64 (0.46 - 0.79) Alifano 1996d 0.64 (0.46 - 0.79) Alifano 1997a 0.75 (0.57 - 0.89) Alifano 1997b 0.68 (0.54 - 0.80) Amicosante1999a 0.83 (0.71 - 0.92) Amicosante 1999b 0.65 (0.50 - 0.79) Anderson 2008a 1.00 (0.72 - 1.00) Anderson 2008c 1.00 (0.72 - 1.00) Bukhary 2007 1.00 (0.93 - 1.00) Chandrasekaran 1990 0.55 (0.42 - 0.67) Conde 2004a 0.75 (0.59 - 0.87) Conde 2004b 0.83 (0.67 - 0.93) D'Alessandro 2008a 0.85 (0.55 - 0.98) D'Alessandro 2008b 0.54 (0.25 - 0.81) Erer 2001 0.47 (0.31 - 0.62) Gao 2007 0.75 (0.70 - 0.80) Imaz 2004a 0.49 (0.33 - 0.65) Imaz 2004b 0.32 (0.18 - 0.48) Imaz 2004c 0.34 (0.20 - 0.51) Imaz 2004d 0.63 (0.47 - 0.78) Imaz 2004e 0.59 (0.42 - 0.74) Imaz 2004f 0.49 (0.33 - 0.65) Imaz 2004g 0.68 (0.52 - 0.82) Imaz 2004h 0.29 (0.16 - 0.46) Imaz 2004i 0.59 (0.42 - 0.74) Imaz 2004j 0.51 (0.35 - 0.67) Imaz 2004k 0.49 (0.33 - 0.65) Imaz 2004l 0.66 (0.49 - 0.80) Imaz 2004m 0.61 (0.45 - 0.76) Imaz 2004n 0.76 (0.60 - 0.88) Julian 2000 0.74 (0.54 - 0.89) Julian 2004a 0.41 (0.24 - 0.61) Julian 2004b 0.10 (0.02 - 0.27) Julian 2004c 0.21 (0.08 - 0.40) Julian 2004d 0.31 (0.15 - 0.51) Kalantri 2005a 0.80 (0.71 - 0.87) Kalantri 2005b 0.29 (0.20 - 0.38) Kassa-Kelembho 2006a 0.16 (0.05 - 0.34) Kassa-Kelembho 2006b 0.32 (0.18 - 0.50) Luh 1996 0.71 (0.59 - 0.82) Maekura 2001a 0.90 (0.84 - 0.94) Maekura 2001b 0.69 (0.55 - 0.81) Maekura 2003 0.60 (0.48 - 0.72) McConkey 2002 0.87 (0.77 - 0.94) Mizusawa 2008 0.59 (0.49 - 0.69) Mukhopadhyay 2006a 0.72 (0.58 - 0.84) Mukhopadhyay 2006b 0.48 (0.27 - 0.69) Nurkic 2006 0.91 (0.81 - 0.97) Okuda 2004a 0.82 (0.65 - 0.93) Okuda 2004b 0.73 (0.52 - 0.88) Okuda 2004c 0.76 (0.59 - 0.89) Okuda 2004d 0.58 (0.37 - 0.77) Okuda 2004e 0.76 (0.59 - 0.89) Okuda 2004f 0.77 (0.56 - 0.91) Ongut 2006 0.40 (0.26 - 0.54) Platonova 2007 0.42 (0.15 - 0.72) Somi 1999 0.26 (0.13 - 0.42) Traunmuller 2005 0.84 (0.69 - 0.94) Wilkinson 1997a 0.78 (0.70 - 0.85) Wilkinson 1997b 0.76 (0.64 - 0.85) Wu 2004a 0.63 (0.52 - 0.73) Wu 2004b 0.35 (0.25 - 0.46) Wu 2005 0.54 (0.41 - 0.66)
Sensitivity (95% CI)
Chi-square = 618.64; df = 65 (p = 0.0000) Inconsistency (I-square) = 89.5 %

Page | 14
Figure 4. Forest plot of specificity, all included studies, all commercial tests
Specificity 0 0.2 0.4 0.6 0.8 1
Alifano 1994 0.98 (0.93 - 1.00) Alifano 1996a 0.93 (0.81 - 0.99) Alifano 1996b 0.89 (0.75 - 0.96) Alifano 1996c 0.93 (0.81 - 0.99) Alifano 1996d 0.89 (0.75 - 0.96) Alifano 1997a 0.86 (0.67 - 0.96) Alifano 1997b 0.86 (0.67 - 0.96) Amicosante1999a 0.97 (0.92 - 0.99) Amicosante 1999b 0.97 (0.92 - 0.99) Anderson 2008a 0.99 (0.94 - 1.00) Anderson 2008b 1.00 (0.96 - 1.00) Anderson 2008c 0.72 (0.60 - 0.82) Bukhary 2007 0.32 (0.14 - 0.55) Chandrasekaran 1990 0.86 (0.80 - 0.90) Conde 2004a 0.77 (0.59 - 0.90) Conde 2004b 0.48 (0.30 - 0.67) D'Alessandro 2008a 0.90 (0.68 - 0.99) D'Alessandro 2008b 0.95 (0.75 - 1.00) Erer 2001 1.00 (0.83 - 1.00) Gao 2007 0.31 (0.26 - 0.36) Imaz 2004a 1.00 (0.92 - 1.00) Imaz 2004b 0.93 (0.82 - 0.99) Imaz 2004c 0.98 (0.88 - 1.00) Imaz 2004d 0.93 (0.82 - 0.99) Imaz 2004e 0.98 (0.88 - 1.00) Imaz 2004f 0.91 (0.79 - 0.98) Imaz 2004g 0.91 (0.79 - 0.98) Imaz 2004h 1.00 (0.92 - 1.00) Imaz 2004i 1.00 (0.92 - 1.00) Imaz 2004j 0.93 (0.82 - 0.99) Imaz 2004k 0.98 (0.88 - 1.00) Imaz 2004l 0.98 (0.88 - 1.00) Imaz 2004m 0.91 (0.79 - 0.98) Imaz 2004n 0.91 (0.79 - 0.98) Julian 2000 0.47 (0.30 - 0.65) Julian 2004a 0.97 (0.85 - 1.00) Julian 2004b 0.97 (0.85 - 1.00) Julian 2004c 0.97 (0.85 - 1.00) Julian 2004d 0.86 (0.70 - 0.95) Kalantri 2005a 1.00 (0.91 - 1.00) Kalantri 2005b 1.00 (0.91 - 1.00) Kassa-Kelembho 2006a 0.90 (0.74 - 0.98) Kassa-Kelembho 2006b 0.90 (0.74 - 0.98) Luh 1996 0.89 (0.85 - 0.92) Maekura 2001a 0.85 (0.79 - 0.90) Maekura 2001b 0.85 (0.79 - 0.90) Maekura 2003 0.88 (0.77 - 0.96) McConkey 2002 0.82 (0.72 - 0.90) Mukhopadhyay 2006a 0.77 (0.69 - 0.84) Mukhopadhyay 2006b 0.77 (0.69 - 0.84) Nurkic 2006 0.78 (0.71 - 0.84) Okuda 2004a 0.91 (0.84 - 0.96) Okuda 2004b 0.91 (0.84 - 0.96) Okuda 2004c 0.97 (0.92 - 0.99) Okuda 2004d 0.97 (0.92 - 0.99) Okuda 2004e 0.89 (0.82 - 0.94) Okuda 2004f 0.89 (0.82 - 0.94) Ongut 2006 1.00 (0.93 - 1.00) Platonova 2007 0.90 (0.70 - 0.99) Somi 1999 0.84 (0.76 - 0.91) Traunmuller 2005 0.73 (0.62 - 0.83) Wilkinson 1997a 0.94 (0.80 - 0.99) Wilkinson 1997b 0.94 (0.80 - 0.99) Wu 2004a 0.88 (0.73 - 0.97) Wu 2004b 0.88 (0.73 - 0.97) Wu 2005 0.68 (0.54 - 0.79)
Specificity (95% CI)
Chi-square = 954.44; df = 65 (p = 0.0000) Inconsistency (I-square) = 93.2 %

Page | 15
Figure 5. Forest plot of sensitivity, all commercial tests, smear-negative patients
Figure 6. Forest plot of specificity, all commercial tests, smear-negative patients
Specificity
0 0.2 0.4 0.6 0.8 1
Alifano 1996c 0.93 (0.81 - 0.99) Alifano 1996d 0.89 (0.75 - 0.96) Alifano 1997b 0.86 (0.67 - 0.96) Amicosante 1999b 0.97 (0.92 - 0.99) Chandrasekaran 1990 0.86 (0.80 - 0.90) Imaz 2004a 1.00 (0.92 - 1.00) Imaz 2004b 0.93 (0.82 - 0.99) Imaz 2004c 0.98 (0.88 - 1.00) Imaz 2004d 0.93 (0.82 - 0.99) Imaz 2004e 0.98 (0.88 - 1.00) Imaz 2004f 0.91 (0.79 - 0.98) Imaz 2004g 0.91 (0.79 - 0.98) Imaz 2004h 1.00 (0.92 - 1.00) Imaz 2004i 1.00 (0.92 - 1.00) Imaz 2004j 0.93 (0.82 - 0.99) Imaz 2004k 0.98 (0.88 - 1.00) Imaz 2004l 0.98 (0.88 - 1.00) Imaz 2004m 0.91 (0.79 - 0.98) Imaz 2004n 0.91 (0.79 - 0.98) Luh 1996 0.89 (0.85 - 0.92) Maekura 2001b 0.85 (0.79 - 0.90) Maekura 2003 0.88 (0.77 - 0.96) Mukhopadhyay 2006b 0.77 (0.69 - 0.84) Okuda 2004b 0.91 (0.84 - 0.96) Okuda 2004d 0.97 (0.92 - 0.99) Okuda 2004f 0.89 (0.82 - 0.94) Wilkinson 1997b 0.94 (0.80 - 0.99) Wu 2004b 0.88 (0.73 - 0.97)
Specificity (95% CI)
Chi-square = 96.90; df = 27 (p = 0.0000) Inconsistency (I-square) = 72.1 %
Sensitivity 0 0.2 0.4 0.6 0.8 1
Alifano 1996c 0.64 (0.46 - 0.79) Alifano 1996d 0.64 (0.46 - 0.79) Alifano 1997b 0.68 (0.54 - 0.80) Amicosante 1999b 0.65 (0.50 - 0.79) Chandrasekaran 1990 0.55 (0.42 - 0.67) Imaz 2004a 0.49 (0.33 - 0.65) Imaz 2004b 0.32 (0.18 - 0.48) Imaz 2004c 0.34 (0.20 - 0.51) Imaz 2004d 0.63 (0.47 - 0.78) Imaz 2004e 0.59 (0.42 - 0.74) Imaz 2004f 0.49 (0.33 - 0.65) Imaz 2004g 0.68 (0.52 - 0.82) Imaz 2004h 0.29 (0.16 - 0.46) Imaz 2004i 0.59 (0.42 - 0.74) Imaz 2004j 0.51 (0.35 - 0.67) Imaz 2004k 0.49 (0.33 - 0.65) Imaz 2004l 0.66 (0.49 - 0.80) Imaz 2004m 0.61 (0.45 - 0.76) Imaz 2004n 0.76 (0.60 - 0.88) Luh 1996 0.71 (0.59 - 0.82) Maekura 2001b 0.69 (0.55 - 0.81) Maekura 2003 0.60 (0.48 - 0.72) Mukhopadhyay 2006b 0.48 (0.27 - 0.69) Okuda 2004b 0.73 (0.52 - 0.88) Okuda 2004d 0.58 (0.37 - 0.77) Okuda 2004f 0.77 (0.56 - 0.91) Wilkinson 1997b 0.76 (0.64 - 0.85) Wu 2004b 0.35 (0.25 - 0.46)
Sensitivity (95% CI)
Chi-square = 98.30; df = 27 (p = 0.0000) Inconsistency (I-square) = 72.5 %

Page | 16
3.1.3 Individual test performance
1) Anda-TB IgG
Anda-TB IgG was the most frequently evaluated commercial test accounting for 13/67 (19%) studies.
In seven studies, the test was evaluated in smear-positive patients, and in four studies in smear-
negative patients. In two studies, the smear status was not reported.
Methodological quality of included studies is presented in Figure 7 (smear-positive patients) and
Figure 8 (smear-negative/culture-positive patients).
Figure 7. Methodological quality: Anda-TB, IgG, smear-positive pulmonary TB

Page | 17
Figure 8. Methodological quality: Anda-TB, IgG, smear-negative/culture-positive pulmonary TB
In studies involving smear-positive patients, only 1/7 studies was conducted in a low/middle-income
country. None of the studies was considered to have a representative spectrum (only 2/7 studies
were conducted in an outpatient setting; 1/7 studies used a cross-sectional study design; and 1/7
studies reported selecting subjects in a consecutive manner). In 2/7 studies the index test was
blinded and in 5/7 studies differential verification was avoided. The sensitivity varied from 54% to
85% and the specificity from 68% to 100% (Figure 9).
Figure 9. Forest plots: Anda-TB, IgG, smear-positive pulmonary TB
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
In studies involving smear-negative/culture-positive patients, no studies were conducted in a
low/middle-income country. None of the studies was considered to have a representative spectrum
(only 1/4 studies was conducted in an outpatient setting; 2/4 studies used a cross-sectional study
design; and 0/4 studies reported selecting subjects in a consecutive manner). In 1/4 studies the
index test was blinded and in 1/4 studies differential verification was avoided. The sensitivity varied
from 35% to 73% and the specificity from 88% to 93% (Figure 10). Studies of smear-negative

Page | 18
patients provided lower pooled sensitivity estimates than studies of smear-positive patients (see
meta-analysis results below).
Figure 10. Forest plots: Anda-TB, IgG, smear-negative/culture-positive pulmonary TB
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
2) Pathozyme Myco-G, A and M
Pathozyme Myco (all three versions, G, A, and M) was the second most frequently evaluated
commercial test accounting for 11/67 (16%) studies. 8/11 studies were conducted in a low/middle-
income country.
Methodological quality of included studies is presented in Figure 11. 8/11 studies were considered
to have a representative spectrum (8/11 studies were conducted in an outpatient setting; 8/11
studies used a cross-sectional study design; and 8/11 reported selecting subjects in a consecutive
manner). In 7/11 studies the index test was blinded and in 8/11 studies differential verification was
avoided.
Figure 11. Methodological quality: Pathozyme Myco, IgG, IgM and IgA.
The sensitivity varied from 10% to 85% and the specificity from 90% to 100%. Some of the variability
in sensitivity could be accounted for by the immunoglobulin detected, with sensitivity values for
Myco-M (anti-IgM) tending to be lower than the values for Myco-G and Myco-A (Figure 12).

Page | 19
Figure 12. Forest plots: Pathozyme Myco-G, M, and A. G = IgG
M = IgM; A = IgA: TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
3) Determiner TB Glycolipid Assay
Determiner TB was the third most frequently evaluated commercial test accounting for 6/67 (9%)
studies. No studies were conducted in a low/middle-income country.
Methodological quality of included studies is presented in Figure 13. None of the studies was
considered to have a representative spectrum (2/6 studies were conducted in an outpatient setting;
4/6 studies used a cross-sectional study design, but only one study reported selecting subjects in a
consecutive manner). In 5/6 studies the index test was blinded and in 1/6 studies differential
verification was avoided.

Page | 20
Figure 13. Methodological quality graph for Determiner TB Glycolipid Assay
The sensitivity varied from 59% to 90% and the specificity from 85% to 89% (Figure 14). All studies
reported some industry involvement (donation of test kits 5 studies and work relationships or
manuscript production 4 studies).
Figure 14. Forest plots: Determiner TB Glycolipid Assay
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are
included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue
squares) and 95% CIs (black horizontal lines).
3.1.5 Results from meta-analysis
There were a sufficient number of studies to perform a meta-analysis for only one particular
commercial test, Anda-TB IgG, with results stratified by smear status (Table 3). In studies involving
smear-positive patients, Anda-TB IgG yielded a pooled sensitivity of 76% (95% CI 63% to 87%) and a
specificity of 92% (95% CI 74% to 98%). In studies with smear-negative patients, the pooled
sensitivity decreased to 59% (95% CI 10 to 96%); the specificity was 91% (95% CI 79 to 96%).

Page | 21
Meta-analyses were also performed grouping assays that used the same format (ELISA or immuno-
chromatographic) regardless of antigen and grouping studies on particular sites of extra-pulmonary
tuberculosis (Table 3).
Table 3. Bivariate meta-analyses: pooled sensitivity and specificity estimates by subgroup;
posterior means with 95% credible intervals in parentheses
Subgroup No. of studies
Sensitivity %
Specificity %
Pulmonary TB
Anda-TB IgG Smear Positive 7 76 (63 to 87)
92 (74 to 98)
Anda-TB IgG Smear Negative 4 59 (10 to 96)
91 (79 to 96)
ELISA 54 60 (6 to 65)
98 ( 96 to 99)
Immunochromatographic Assays*
12 53 (42 to 64)
98 (94 to 99)
Extrapulmonary TB
Lymph Node TB 6 64 (28 to 92)
90 (76 to 97)
Pleural TB 5 46 (29 to 63),
87 (51 to 99)
Anda-TB IgG 10 81 (49 to 97)
85 (77 to 92)
*Commercial tests included: ICT TB 3 studies; Assure TB 2 studies; MycoDot 3 studies; SDHO 2 studies; Hexagon 1 study; Serocheck MTB 1 study
IgG, immunoglobulin G
The HSROC curves show the decreased performance of the test in smear-negative patients
compared with smear-positive patients (Figure 15).

Page | 22
Figure 15. Summary ROC plots of sensitivity and specificity for Anda-TB IgG
Performance in (A and blank circles) smear-positive patients and (B and gray circles) smear-negative patients. The
diameter of the circles is proportional to the number of patients in each study. The red squares are the summary values
for sensitivity and specificity.
Exploring whether test technique had an impact on accuracy was done by comparing the
performance of the set of studies using ELISAs with those using immunochromatographic assays
(Table 3, Figure 16). Compared with ELISA [sensitivity = 60% (95% CI 6% to 65%); specificity = 98%
(95% CI 96% to 99%)], immunochromatographic assays yielded lower sensitivity (53%, 95% CI 42% to
64%) and identical specificity (98%, 95% CI 94% to 99%).

Page | 23
Figure 16. Summary ROC plots of sensitivity and specificity by assay technique
Performance in ELISA (A and blank circles) and ) immunochromatographic (B and gray circles assay. The width of the
circles is proportional to the number of patients in each study. The red squares are the summary values for sensitivity
and specificity.
3.1.6 Results in HIV-infected TB patients
Only one study included confirmed HIV-infected patients, comparing the performance of the SDHO
MTB test (SDHO Laboratories Inc., Canada) head-to-head with smear microscopy in 55 pulmonary TB
suspects residing in the Central African Republic. As with all studies in the review, the reference
standard was culture.
Compared with smear microscopy [sensitivity = 68% (95% CI 49% to 83%)], SDHO yielded a
sensitivity of only 16% (95% CI 5 to 34%). Specificity of SDHO was 90% (95% CI 74% to 98%), lower
than the specificity of smear microscopy [100% (95% CI 89% to 100%)].
3.2 Findings from the WHO/TDR laboratory-based evaluation
The WHO/TDR evaluation involved head-to-head comparison of 19 commercially available rapid
serodiagnostic tests. Overall, the sensitivity of the tests ranged from 1% to 60% and specificity from
53% to 99% (Table 4). Test performance was poorer in patients with sputum smear-negative TB
compared with patients with smear-positive TB and in HIV seropositive patients compared with
seronegative patients. The average difference in test sensitivity, HIV-uninfected (n=198) minus HIV-
infected population (n=157), was 22%.
When smear microscopy was added to most rapid tests, overall sensitivity increased from 75%
(smear alone) up to 89% (smear plus rapid test). This gain is equivalent to the detection of 57%
(29/51) of the smear-negative, culture-positive TB cases. However, there was a corresponding
decrease in specificity to 58% (86/149). Thus in a setting with a TB prevalence of 20%, for every 1000
TB suspects evaluated, one could expect 800 individuals without TB, of whom 336 would be false
positives (0.42 x 800).

Page | 24
Sixteen (84%) tests showed high reliability (kappa value ≥ 0.70). None of the tests received perfect
scores in any area (clarity of instructions, technical complexity, and ease of interpretation of results)
and all kits required equipment that was not provided. However, 12/19 (63%) tests were rated as
very easy to use and would therefore have been considered appropriate for use in primary care
settings in developing countries had their technical accuracy been adequate.
Table 4. TDR evaluation: Performance of 19 rapid tests for pulmonary tuberculosis
Manufacturer Rapid test Sensitivity %
(95% CI)
Specificity %
(95% CI)
1 ABP Diagnostics Focus Sure Check TB 8 (4-11) 95 (92-99)
2 Advanced Diagnostics Tuberculosis Rapid Test 40 (33-46) 53 (45-61)
3 American Bionostica Rapid Test for TB 20 (15-26) 80 (73-86)
4 Ameritek dBest One Step TB Test 34 (27-40) 68 (61-76)
5 BioMedical Products Corp TB Rapid Screen Test 49 (42-56) 57 (49-65)
6 Chembio TB Stat-Pak II 32 (25-38) 83 (76-89)
7 CTK Biotech TB Antibody Onsite Rapid Screening Test 27 (21-33) 69 (62-77)
8 Hema Diagnostic Rapid 1-2-3 TB Test 36 (29-42) 72 (65-80)
9 Laboratorio Silanes TB-Instantest 38 (31-44) 70 (62-77)
10 Millenium Biotechnology Immuno-Sure TB Plus 2 (0-5) 99 (97-100)
11 Minerva Biotech V Scan 21 (16-27) 89 (84-94)
12 Mossman Associates MycoDot 36 (30-42) 87 (81-92)
13 Pacific Biotech Bioline TB 19 (14-25) 95 (91-98)
14 Premier Medical Corporation First Response Rapid TB 21 (16-27) 95 (92-99)
15 Princeton BioMeditech BioSign M tuberculosis 1 (0-2) 99 (97-100)
16 Span Diagnostics TB Spot ver 2.0 38 (32-45) 78 (71-85)
17 Standard Diagnostics SD Rapid TB 21 (15-26) 96 (93-99)
18 UniMED International Inc FirstSign MTB Card Test 60 (53-66) 58 (50-66)
19 Veda Lab TB Rapid Test 13 (8-17) 98 (96-100)
Source: Laboratory-based evaluation of 19 commercially available rapid diagnostic tests for tuberculosis.5

Page | 25
3.3 Performance characteristics of commercial serodiagnostics in extra-pulmonary TB
3.3.1 Studies included
4,256 citations were identified and 160 full-text articles reviewed. Twelve publications with 25 studies (datasets) met the eligibility criteria. Of these, ten (40%) studies were conducted in low/middle-income countries. A list of included and excluded studies and the reasons for exclusion are presented in Annex 3. All studies were written in English. Only one study involved HIV-infected individuals and no studies predominantly involved children. Commercial tests were evaluated for diagnosis of the following forms of extrapulmonary TB: lymph node, 6 studies; pleural, 5 studies; multiple sites, 5 studies; genitourinary, 2 studies; disseminated, 4 studies; and meningeal, 1 study. In two studies, the site of extrapulmonary involvement was not reported. Six distinct commercial tests were evaluated, of which 17/25 (68%) studies used Anda-TB (IgG 10 studies; IgM 5 studies; IgA 1 study; IgM plus IgA 1 study). ELISA was used in 21 (84%) studies and immunochromatographic assays in four studies. The majority (72%) of studies detected IgG antibodies. The condition of the specimen was frozen in 6 (24%) studies and not reported in 19 studies. The median number of TB patients was 35 (range 30 to 56). No studies reported on patient-important outcomes or patient values and preferences concerning these tests.
3.3.2 Methodological quality
Methodological quality was considered by paper and by individual study/dataset. By paper, study
quality suffered from lack of a representative patient spectrum 2/12 (17%) papers were considered
to include a representative sample. Blinding of commercial test results to culture was rarely
reported (2/12 papers). No conflict of interest (absence of industry involvement) was explicitly
stated in 1/12 papers. When considered by study, 14 (56%) studies reported the findings from case-
control studies of which four studies involved healthy controls. QUADAS assessments of studies
included in subgroup analyses are presented in Figure 17.
Figure 17. Methodological quality: extrapulmonary TB

Page | 26
3.3.3 Test performance by site of disease
1) Lymph node TB
Six studies were identified (Anda-TB 3 studies, SEVA 1 study; MycoDot 2 studies). 4/6 studies were
conducted in a low/middle-income country. None of the studies (Figure 18) was considered to have
a representative spectrum (0/6 studies used a cross-sectional study design and 0/6 reported
selecting subjects in a consecutive manner). In 2/6 studies the index test was blinded and in 4/6
studies differential verification was avoided.
Figure 18. Methodological quality: lymph node TB
Sensitivity was highly variable ranging from 23% to 100%; specificity ranged from 59 to 97% (Figure
19).
Figure 19. Forest plots: all commercial tests, lymph node TB
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
2) Pleural TB
Five studies were identified (Anda-TB 4 studies; ICT 1 study). 4/5 studies were conducted in a
low/middle-income country. Figure 20 shows that one study was considered to have a
representative spectrum (5/5 studies used a cross-sectional study design and 1/5 studies reported
selecting subjects in a consecutive manner). In 1/5 studies the index test was blinded and in 2/5
studies differential verification was avoided.

Page | 27
Figure 20. Methodological quality graph, pleural TB
Sensitivity was highly variable ranging from 26% to 59%; specificity ranged from 60% to 100% (Figure
21).
Figure 21. Forest plots: all commercial tests, pleural TB
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
3.3.4 Individual test performance
1) Anda-TB, IgG
Anda-TB IgG was the most frequently evaluated commercial test accounting for 10/25 (40%)
studies. 2/10 studies were conducted in a low/middle-income country. As shown in Figure 22, none
of the studies was considered to have a representative spectrum (4/10 studies used a cross-sectional
study design and 0/10 studies reported selecting subjects in a consecutive manner). In 0/10 studies
the index test was blinded and in 2/10 studies differential verification was avoided.

Page | 28
Figure 22. Methodological quality: Anda-TB IgG, extrapulmonary TB, all sites of disease
Sensitivity was highly variable ranging from 26 to 100%; specificity ranged from 59 to 100% (Figure
23).
Figure 23. Forest plots: Anda-TB IgG, extrapulmonary TB, all sites of disease
TP = True Positive; FP = False Positive; FN = False Negative; TN = True Negative. 95% confidence intervals (CI) are included between the brackets. The figure shows the sensitivity and specificity estimates for individual studies (blue squares) and 95% CIs (black horizontal lines).
3.3.5 Results from meta-analysis
Pooled sensitivity and specificity estimates were calculated for studies evaluating any commercial
test for the diagnosis of lymph node or pleural TB. For lymph node TB, the sensitivity was 64% (95%
CI 28% to 92%) and specificity 90% (95% CI 76 to 97%). For pleural TB, the sensitivity was 46% (95%
CI 29% to 63%) and specificity 87% (95% CI 51% to 99%).
Pooled sensitivity and specificity estimates for Anda-TB IgG were done for: multiple sites, 3 studies;
lymph node, 2 studies; pleural TB, 2 studies; disseminated TB, 2 studies; and genitourinary, 1 study.

Page | 29
For Anda-TB IgG, the sensitivity was 81% (95% CI 49% to 97%) and specificity 85% (95% CI 77% to
92%), as reflected in Table 3 above.
3.3.6 Results in HIV-infected TB patients
One study evaluated the performance of the MycoDot test in a cross-sectional study of TB suspects
in Thailand. 142 HIV seropositive [mean CD4 count = 188 cells/mm (range 7 to 632)] and 144 HIV
seronegative newly diagnosed TB patients participated in the study, of whom 50 patients [40 HIV-
infected, 10 HIV-uninfected] were diagnosed by culture or histopathological examination with lymph
node TB.
Compared with the sensitivity of MycoDot in HIV seronegative TB patients, [80%, (95% CI 44 to
98%)], the sensitivity of the test in HIV seropositive TB patients was considerably lower [33% (95% CI
19 to 39%)]. The specificity in both groups was identical 97% (95% CI 93 to 99%).
3.4 Economic and epidemiological impact of TB serodiagnostics in India
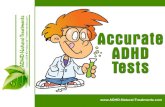
The total cost to the healthcare system (cost of diagnosis, treatment of TB cases, and treatment of false-positives) of testing 1.5 million Indian TB suspects with serology was USD62 million. Thus, the cost of testing 10-15% of India’s TB suspects is similar to the USD65 million annual budget of the Revised National TB Control Program (RNTCP). Of this USD62 million, USD30 million is for the diagnostic test itself, and USD19 million for treatment of false-positives, with only USD13 million spent on treatment of true TB cases, 66% of whom would have been treated in the absence of any TB-specific diagnostic testing based on clinical suspicion alone (Figure 24). Performing sputum smear microscopy alone on these patients would reduce total costs to USD26 million, with >50% reduction in costs for false-positive treatment and 85% reduction in costs for diagnosis. For every new case of TB diagnosed by serology, 2.82 false-positive cases would be diagnosed and treated (vs. 0.98 for sputum smear and 0.66 for smear plus TB culture) (Figure 24). In sensitivity analyses incorporating more realistic assumptions, serology performed even more poorly. Overall, compared to sputum smear microscopy or culture, serology was estimated to be more costly and less effective in all scenarios considered.
Figure 24. Cost for 1.5 million TB suspects undergoing serologic testing in India
$0
$20
$40
$60
$80
No Diagnostics Sputum Smear Smear + Culture
Serology
Mill
ions
of U
S D
olla
rs
Diagnosis (Cost of Diagnostic Test)
False-Positives (Wasted Money)
TB Treatment (Desirable Costs)

Page | 30
Figure 25. Gains from investment in different diagnostic tests in India
0
528
740
511
0
200
400
600
800
No Diagnostics Sputum Smear Smear + Culture Serology
DALYs Averted (x1,000)
Increasing Cost

Page | 31
4. Summary of findings and GRADE evidence profiles
4.1 Pulmonary TB
The updated systematic review of the diagnostic accuracy of commercial tests for pulmonary TB
identified 67 unique studies, including 32 studies from low- and middle-income countries. None of
these studies evaluated the tests in children. The results demonstrate that:
(1) for all commercial tests, sensitivity (0% to 100%) and specificity (31 to 100%) from individual
studies are highly variable;
(2) using bivariate meta-analysis, for Anda-TB IgG (the most commonly evaluated test), the pooled
sensitivity is 76% (95% CI 63 to 87%) in studies of smear-positive and 59% (95% CI 10 to 96%) in
studies of smear-negative patients, respectively; the pooled specificity in these studies was similar:
92% (95% CI 74 to 98%) and 91% (95% CI 79 to 96%), respectively;
(3) for Anda-TB IgG, sensitivity values in smear-positive (54% to 85%) and smear-negative (35% to
73% ) patients from individual studies are highly variable;
(4) for Anda-TB IgG, specificity values from individual studies are variable (68% to 100%);
(5) in the TDR evaluation of 19 rapid commercial tests, in comparison with culture plus clinical
follow-up, sensitivity (1% to 60%) and specificity (53% to 99%) values are highly variable;
(6) compared with ELISAs [60% (95% CI 6% to 65%], immuno-chromatographic assays have similar
sensitivity [53%, 95% CI 42% to 64%]; and
(7) in the single study involving HIV-infected TB patients, the sensitivity of the SDHO test is 16% (95%
CI 5% to 34%).
The only commercial test (Anda-TB) that could be included in sub-analyses provided poor
performance and the other commercial tests did not have enough data to analyse. None of the tests
reviewed could replace smear microscopy, a finding consistent with those reported in a previous
systematic review.2
The sensitivity and specificity estimates in this meta-analysis are likely to be overly optimistic for at
least two reasons: (1) as described earlier, study quality generally suffered from lack of a
representative patient spectrum which could result in exaggerated estimates of test accuracy48, 49
and (2) potential publication bias, where studies with poor performance were likely to be
unpublished. Subgroup analyses in a meta-analysis, like subgroup analyses in a clinical trial, are
vulnerable to bias; therefore, the findings of this meta-analysis should be interpreted with caution.50
4.2 Extra-pulmonary TB
The updated systematic review of the diagnostic accuracy of commercial tests for extrapulmonary
TB identified 25 unique studies, including 10 studies from low- and middle-income countries. None
of these studies evaluated the tests predominantly in children. The results demonstrate that:
(1) for all commercial tests, sensitivity (0% to 100%) and specificity (59% to 100%) values from
individual studies are highly variable;
(2) pooled sensitivity is 64% (95% CI 28% to 92%) for lymph node tuberculosis and 46% (95% CI 29%
to 63%) for pleural tuberculosis;

Page | 32
(3) for Anda-TB IgG, although the pooled sensitivity and specificity are 81% (95% CI 49% to 97%) and
85% (95% CI 77 to 92%) respectively, sensitivity (26% to 100%) and specificity (59% to 100%) values
from individual studies are highly variable;
(5) in the single study involving HIV-infected individuals, the sensitivity of MycoDot is 33% (95% CI
19% to 39%).
As discussed above for pulmonary TB, the only commercial test (Anda-TB) that could be included in
subgroup-analyses for extrapulmonary TB provided poor performance and the other commercial
tests did not have enough data to analyze. These findings are consistent with those reported in a
previous systematic review.3
The sensitivity and specificity estimates in this meta-analysis are likely to be overly optimistic for at
least two reasons: (1) as described earlier, study quality generally suffered from lack of a
representative patient spectrum which could result in exaggerated estimates of test accuracy48, 49
and (2) potential publication bias, where studies with poor performance were likely to be
unpublished. Subgroup analyses in a meta-analysis, like subgroup analyses in a clinical trial, are
vulnerable to bias; therefore, the findings of this meta-analysis should be interpreted with caution.50
4.3 Strengths and limitations of the evidence base
Strengths of the systematic reviews include the use of a standard protocol and comprehensive
search strategy, independent reviewers, a bivariate model for meta-analysis, and pre-specified
subgroups to account for heterogeneity.
Limitations related to the evidence base include the fact that the majority of studies was not
considered to have a representative patient spectrum and was not performed in a blinded manner
or blinding was not explicitly stated. Also, subgroup analyses were limited by the small number of
studies for a particular commercial test or form of extrapulmonary disease. Differing criteria for
patient selection and greater duration and severity of illness of the study populations may have
introduced variability in findings among studies. Finally, although statistical tests and graphical
methods are available to detect potential publication bias in meta-analyses of randomized
controlled trials, such techniques have not been adequately evaluated for diagnostic data.
Nevertheless, it was considered prudent to assume some degree of publication bias as studies
showing poor performance of commercial tests may be less likely to be published. This in turn may
have introduced ‘optimism bias’ in the pooled estimates of sensitivity and specificity.
Concerning the TDR evaluation, a few additional limitations were discussed:
Testing was done retrospectively using stored frozen sera that passed through two freeze-thaw
cycles. It is possible that the use of fresh serum may increase sensitivity;
There was limited geographic diversity amongst TB and HIV-positive patients whose specimens
were used for evaluating the commercial tests. It is possible that there may be variations in the
anti-mycobacterial antibody responses both due to patient genetic diversity and differential
antigen expression by different mycobacterial isolates that could have led to reduced sensitivity
with these specimens;
The duration of illness in patients was unknown. Greater duration or severity of illness may be
correlated with the likelihood of a positive diagnostic test;
It is possible that infections with nontuberculous mycobacteria or exposure to environmental
mycobacteria led to cross reactivity and decreased specificity;

Page | 33
The systematic review focused on test accuracy (ie. sensitivity and specificity). None of the papers
reviewed provided information on patient-important outcomes, ie. showing that commercial tests
used in a given situation resulted in a clinically relevant improvement in patient care and/or
outcomes. In addition, no information was available on the values and preferences of patients.
No studies were identified that directly assessed the value of serology over and above conventional
tests such as sputum smear microscopy. The TDR study did evaluate added value of smear plus
serology and reported a gain equivalent to the detection of 57% of the smear-negative, culture-
positive TB cases. However, there was a corresponding unacceptable decrease in specificity (58%).
4.4 GRADE evidence profiles and final recommendations
The GRADE evidence profiles are provided in Tables 5 to 8. Based on these assessments, the Expert
Group concluded that the quality of evidence for commercial serodiagnostic tests was very low and
recommended that these tests should not be used in individuals suspected of active pulmonary or
extra-pulmonary TB, irrespective of their HIV status.
This recommendation also applies to paediatric TB based on the generalisation of data from
adults (while acknowledging the limitations of microbiological diagnosis in children);
This recommendation also applies to the use of commercial serodiagnostic tests as add-on tests
in smear-negative individuals given the high risk of false-positives and the consequent adverse
effects.
OVERALL QUALITY OF EVIDENCE VERY LOW
STRENGTH OF RECOMMENDATION STRONG

Page | 34
Table 5. Should commercial serological tests be used as a replacement test for conventional tests such as smear microscopy in patients suspected of
having pulmonary tuberculosis?
Outcome No. studies
Study Design
Limitations Indirectness Inconsistency Imprecision Publication bias
Final Quality
1
Effect per 1000 Importance
True Positives
67 (8318)
A1
Cross-sectional and case-control
Very Serious
A2
(-2)
No Serious Indirectness
A3
Very Serious
A4
(-2)
SeriousA5
(-1)
LikelyA6
Very Low
Prev 10%: 64
Prev 30%: 192
Critical
True Negatives
67 (8318)
A1
Cross-sectional and case-control
Very Serious
A2
(-2)
No Serious Indirectness
A3
Very Serious
A4
(-2)
SeriousA5
(-1)
LikelyA6
Very Low
Prev 10%: 819
Prev 30%: 637
Critical
False Positives
67 (8318)
A1
Cross-sectional and case-control
Very Serious
A2
(-2)
No Serious Indirectness
A3
Very Serious
A4
(-2)
SeriousA5
(-1)
LikelyA6
Very Low
Prev 10%: 81
Prev 30%: 63
Critical
False Negatives
67 (8318)
A1
Cross-sectional and case-control
Very Serious
A2
(-2)
No Serious Indirectness
A3
Very Serious
A4
(-2)
SeriousA5
(-1)
LikelyA6
Very Low
Prev 10%: 36
Prev 30%: 108
Critical
Accuracy estimates were not pooled because of the considerable heterogeneity among studies. Based on sensitivity median = 64%, specificity median = 91%
1 Quality of evidence rated as high (no points subtracted), moderate (1 point subtracted), low (2 points subtracted), or very low (>2 points subtracted) based on five factors: study limitations,
indirectness of evidence, inconsistency in results across studies, imprecision in summary estimates, and likelihood of publication bias. For each outcome, the quality of evidence started at high
when there were randomized controlled trials or high quality observational studies (cross-sectional or cohort studies enrolling patients with diagnostic uncertainty) and at moderate when these
types of studies were absent. One point was then subtracted when there was a serious issue identified or two points when there was a very serious issue identified in any of the criteria used to
judge the quality of evidence.
A167 studies evaluated 18 commercial tests. 37/67 (55%) studies used a cross-sectional design and 30/67 (45%) studies used a case-control design.

Page | 35
A2 Study limitations were assessed using the QUADAS tool. Overall, study quality suffered from lack of a representative patient spectrum as only 19/67 (28%) studies were considered to include
a representative sample (scored as yes when ambulatory patients suspected of having active TB were consecutively selected). 27/67 (40%) of studies recruited patients in a consecutive
manner. 29/67 (43%) studies were conducted in an outpatient setting. Blinding of commercial test results was reported in 34/67 (51%) studies.
A3Diagnostic accuracy was considered a surrogate for patient-important outcomes; therefore this factor was not downgraded. Uncertainty about directness for false-negatives relates to possible
detrimental effects from delayed diagnosis and uncertain but likely deterioration of health status. Uncertainty about directness for false-positives relates to the following concerns: diagnosing
other respiratory diseases (such as pneumonia) as pulmonary TB may lead to delayed diagnosis or death from the other disease; false-positives unnecessarily consume health care and patient
resources through DOT administration and patient misclassification (resulting in potentially inappropriate treatment regimens); adverse drug reactions may increase. Only 32 (48%) studies were
conducted in low/middle-income countries limiting generalisability to these settings.
A4Heterogeneity was assessed visually and statistically. There was significant heterogeneity in accuracy estimates: sensitivity range 0% to 100%, I-square = 89.6%; p = 0.0000; specificity range
31% to 100%, I-square = 93.8%; p = 0.0000. In further analyses, subgroups were pre-specified by identity of commercial test, antibody detected, and smear status to decrease heterogeneity.
Differing criteria for patient selection and greater duration and severity of illness of the study populations may have introduced variability in findings among studies. The heterogeneity between
studies could also be explained by use of different cut-offs for positivity, a factor that could not be addressed.
A5Accuracy estimates were not pooled. The 95% confidence intervals were wide for many individual studies; however, this factor was not downgraded as there were a large number of studies
and 2 points had already been subtracted for inconsistency.
A6Data included in the systematic review did not allow for formal assessment of publication bias using methods such as funnel plots or regression tests. Therefore, publication bias cannot be
ruled out and it was considered prudent to assume a degree of publication bias as studies showing poor performance of commercial tests were probably less likely to be published. Industry
involvement was recorded in 40/67 studies(32/40 involved donation of test kits)

Page | 36
Table 6. Should commercial serological tests be used as an add-on to conventional tests such as smear microscopy in patients suspected of having
pulmonary tuberculosis?
Outcome No. studies
Study Design
Limitations Indirectness Inconsistency Imprecision Publication bias
Final Quality
Effect per 1000
Importance
True Positives
28 (3433)B1
Mainly cross-sectional
SeriousB2
(-1)
SeriousB3
(-1)
Very Serious
B4
(-2)
Serious
ImprecisionB5
(-1)
LikelyB6
Very Low
Prev 10%: 61
Critical
True Negatives
28 (3433) Mainly cross-sectional
SeriousB2
(-1)
SeriousB3
(-1)
Very Serious
B4
(-2)
Serious
ImprecisionB5
(-1)
LikelyB6
Very Low
Prev 10%: 828
Critical
False Positives
28 (3433) Mainly cross-sectional
SeriousB2
(-1)
SeriousB3
(-1)
Very Serious
B4
(-2)
Serious
ImprecisionB5
(-1)
LikelyB6
Very Low
Prev 10%: 72 Critical
False Negatives
28 (3433) Mainly cross-sectional
SeriousB2
(-1)
SeriousB3
(-1)
Very Serious
B4
(-2)
Serious
ImprecisionB5
(-1)
LikelyB6
Very Low
Prev 10%: 39
Critical
Accuracy estimates were not pooled because of the considerable heterogeneity among studies. Based on sensitivity median = 61%, specificity median = 92%
B128 studies involving smear-negative patients were included; 21/28 (75%) used a cross-sectional design and 7/28 (25%) used a case-control design.
B2Study limitations were assessed using the QUADAS tool. 17/28 (61%) studies recruited patients in a consecutive manner; 18/28 (64%) studies were conducted in an outpatient setting. Blinding
of the commercial test result was reported in 18/28 (64%) studies.
B3Diagnostic accuracy was considered a surrogate for patient-important outcomes (see
A3). Indirectness was regarded as a greater concern if a commercial serological test is used as an ‘add on’
test, therefore this was downgraded one point. 16 (57%) were conducted in low/middle-income countries limiting generalisability to these settings.
B4 Heterogeneity was assessed visually and statistically. There was significant heterogeneity in accuracy estimates: sensitivity range 29 to 77%, I-square = 72.5%; p = 0.0000; specificity range 77
to 100%, I-square = 72.1%; p = 0.0000. Subgroups were pre-specified by identity of commercial test, antibody detected, and smear status to decrease heterogeneity. Differing criteria for patient

Page | 37
selection and greater duration and severity of illness of the study populations may have introduced variability in findings among studies. The heterogeneity between studies could also be explained by use of different cut-offs for positivity, a factor that could not be addressed.
B5 Accuracy estimates were not pooled. The 95% confidence intervals were very wide for many individual studies; however, this factor was not downgraded as there were a large number of
studies and 2 points had already been subtracted for inconsistency.
B6Data included in the systematic review did not allow for formal assessment of publication bias using methods such as funnel plots or regression tests (see
A6). Therefore, publication bias
cannot be ruled out and it was considered prudent to assume a degree of publication bias as studies showing poor performance of commercial tests were probably less likely to be published.

Page | 38
Table 7. Diagnostic accuracy of Anda-TB IgG
Outcome No. studies
Study Design
Limitations Indirectness Inconsistency Imprecision Publication bias
Final Quality
Effect per 1000
Importance
True Positives
7 (870)C1
Mainly case-control
Very Serious
C2
(-2)
No Serious Indirectness
C3
No Serious Inconsistency
C4
SeriousC5
(-1) Likely
A6 Very Low
Prev 10%: 76
Prev 30%: 228
Critical
True Negatives
7 (870)C1
Mainly case-control
Very Serious
C2
(-2)
No Serious Indirectness
C3
No Serious Inconsistency
C4
SeriousC5
(-1) Likely
A6 Very Low
Prev 10%: 828
Prev 30%: 644
Critical
False Positives
7 (870)C1
Mainly case-control
Very Serious
C2
(-2)
No Serious Indirectness
C3
No Serious Inconsistency
C4
SeriousC5
(-1) Likely
A6 Very Low
Prev 10%: 72
Prev 30%: 56
Critical
False Negatives
7 (870)C1
Mainly case-control
Very Serious
C2
(-2)
No Serious Indirectness
C3
No Serious Inconsistency
C4
SeriousC5
(-1) Likely
A6 Very Low
Prev 10%: 24
Prev 30%: 72
Critical
Based on pooled sensitivity = 76% (95% CI 63 to 87%), pooled specificity = 92% (95% CI 74 to 98%)
C17 studies were included in smear-positive patients that evaluated Anda-TB IgG (Anda Biologicals, Strasbourg), an A60-based ELISA.
C2 Study limitations were assessed using the QUADAS tool.
None of the studies was considered to have a representative spectrum (only 2/7 studies were conducted in an outpatient setting; 1/7
studies used a cross-sectional study design; and 1/7 studies reported selecting subjects in a consecutive manner). In 2/7 studies the index test was blinded and in 5/7 studies differential verification was avoided.
C3Diagnostic accuracy was considered a surrogate for patient-important outcomes (see
A3); Only 1/7 studies was conducted in low/middle-income countries limiting generalisability to these
settings.
C4Heterogeneity was assessed by visual inspection of forest plots of sensitivity and specificity estimates. Sensitivity in the studies varied from 54% to 85% and specificity varied from 68% to
100%. However, except for two studies by the same author, the sensitivity estimates were consistent. Specificity estimates were more variable. Heterogeneity between studies could be explained by use of different cut-offs for positivity, a factor that could not be addressed.
C5Accuracy estimates were pooled by bivariate meta-analysis. Pooled sensitivity and specificity had relatively wide confidence intervals: sensitivity 76% (95% CI 63% to 87%); specificity 92% (95%
CI 74 to 98%).

Page | 39
C6Data included in the systematic review did not allow for formal assessment of publication bias using methods such as funnel plots or regression tests. Therefore, publication bias cannot be
ruled out and it was considered prudent to assume a degree of publication bias as studies showing poor performance of commercial tests were probably less likely to be published. This in turn may have introduced ‘optimism bias’ in the pooled estimates of sensitivity and specificity; nevertheless this factor was not downgraded.

Page | 40
Table 8. Diagnostic accuracy of Anda-TB IgG in studies of smear-negative patients (ie. as an ‘add on’ test to smear microscopy)
Outcome No. studies
Study Design
Limitations Indirectness Inconsistency Imprecision Publication bias
Final Quality
Effect per 1000
Importance
True Positives
4 (700)D1 Mainly case-control
Very SeriousD2 (-2)
SeriousD3 (-1)
No Serious InconsistencyD4
Very SeriousD5 (-2)
LikelyD6 Very Low
Prev 10%: 59
Critical
True Negatives
4 (700)D1 Mainly case-control
Very SeriousD2 (-2)
SeriousD3 (-1)
No Serious InconsistencyD4
Very SeriousD5 (-2)
LikelyD6 Very Low
Prev 10%: 819
Critical
False Positives
4 (700)D1 Mainly case-control
Very SeriousD2 (-2)
SeriousD3 (-1)
No Serious InconsistencyD4
Very SeriousD5 (-2)
LikelyD6 Very Low
Prev 10%: 81
Critical
False Negatives
4 (700)D1 Mainly case-control
Very SeriousD2 (-2)
SeriousD3 (-1)
No Serious InconsistencyD4
Very SeriousD5 (-2)
LikelyD6 Very Low
Prev 10%: 41
Critical
Based on pooled sensitivity = 59% (95% CI 10 to 96%), pooled specificity = 91% (95% CI 79 to 96%)
D1Four studies were included of smear-negative patients that evaluated Anda-TB IgG (Anda Biologicals, Strasbourg), an A60-based ELISA.
D2Study limitations were assessed using the QUADAS tool.
None of the studies was considered to have a representative spectrum (only one study was conducted in an outpatient setting; 2/4
studies used a cross-sectional study design; and 0/4 studies reported selecting subjects in a consecutive manner). In 1/4 studies the index test was blinded and in 1/4 studies differential verification was avoided.
D3Diagnostic accuracy was considered a surrogate for patient-important outcomes (see
A3). Indirectness was regarded as a greater concern if Anda-TB were used as an add-on test; this factor
was therefore downgraded by one point. No studies were conducted in low/middle-income countries limiting generalizability to these settings.

Page | 41
D4Heterogeneity was assessed by visual inspection of forest plots of accuracy estimates. The sensitivity varied from 35 to 73% and the specificity varied from 88 to 93%. However, except for one
study, sensitivity was consistent and this factor was therefore not downgraded.
D5Accuracy estimates were pooled by bivariate meta-analysis. Pooled sensitivity had very wide confidence intervals: sensitivity 59% (95% CI 10 to 96%); specificity 91% (95% CI 79 to 96%).
D6Data included did not allow for formal assessment of publication bias using methods such as funnel plots or regression tests. Therefore, publication bias cannot be ruled out and it was
considered prudent to assume a degree of publication bias as studies showing poor performance of commercial tests were probably less likely to be published. This in turn may have introduced ‘optimism bias’ in the pooled estimates of sensitivity and specificity; nevertheless, this factor was not downgraded.

Page | 42
5. RESEARCH GAPS
The Expert Group strongly encouraged further research to identify new/alternative serological tests with
improved accuracy. Such research should be based on adequate study design including QUADAS principles
such as representative suspect populations, prospective follow-up and adequate, explicit blinding.
Future studies should include children and HIV-infected individuals, with stratification by CD4 count.
Studies should also consider randomised approaches to investigate patient-relevant outcomes, while using
incremental designs and test strategies so as to not merely focus on performance of new assays.
Further research on accurate point-of-care tests for TB diagnosis is strongly recommended.
6. REFERENCES
1. Steingart K R, Henry M, Laal S, et al. Commercial serological antibody detection tests for the diagnosis of
pulmonary tuberculosis: a systematic review. PLoS Med. 2007 Jun;4(6):e202.
2. Steingart K R, Henry M, Laal S, et al. A systematic review of commercial serological antibody detection
tests for the diagnosis of extrapulmonary tuberculosis. Thorax. 2007 Oct;62(10):911-8.
3. Steingart K R, Dendukuri N, Henry M, et al. Performance of purified antigens for serodiagnosis of
pulmonary tuberculosis: a meta-analysis. Clin Vaccine Immunol. 2009 Feb;16(2):260-76.
4. Dinnes J, Deeks J, Kunst H et al. A systematic review of rapid diagnostic tests for the detection of
tuberculosis infection. Health Technol. Assess. 2007 Jan;11(3):1-196.
5. World Health Organization on behalf of the Special Programme for Research and Training in Tropical
Diseases 2008. Laboratory-based evaluation of 19 commercially available rapid diagnostic tests for
tuberculosis (Diagnostics evaluation series, 2). Available at:
http://apps.who.int/tdr/svc/publications/tdr-research-publications/diagnostics-evaluation-2
6. Dowdy D W, O'Brien M A, Bishai D. Cost-effectiveness of novel diagnostic tools for the diagnosis of
tuberculosis. IJTLD. 2008 Sept; 12(9):1021-1029.

Annexes
Page | 43
Annex 1: Meeting background and objectives
Use of commercial serological tests for the diagnosis of TB
- EXPERT GROUP MEETING -
Date and time: 22 July 2010, 09:00 – 1600 Venue: Salle B, WHO-HQ Main Building, Geneva, Switzerland
BACKGROUND
Commercial serological tests for diagnosis of TB have been used for many years, especially in the private
health sector. In 2008, a head-to-head comparison by TDR of 19 commercial tests showed clear deficiencies
in the performance characteristics of these tests, particularly in specimens from patients co-infected by
HIV, where the sensitivity was greatly affected1. It was concluded that none of the tested assays performed
well enough to replace conventional microbiological tests for TB. Nevertheless, aggressive marketing of
serodiagnostics continues in many parts of the world, with claims about accuracy often based on poor
quality and grossly insufficient data. WHO has therefore called for an update on the current evidence base
for commercial serodiagnostic tests, with the aim of developing global policy guidance on their relevance in
TB diagnosis.
WORLD HEALTH ORGANIZATION: EVIDENCE-BASED PROCESS FOR POLICY GUIDANCE In order to facilitate rapid policy guidance on the use of new diagnostic tools, new methods, and/or novel
approaches using existing tools, WHO has developed a systematic, structured, evidence-based process. The
first step involves a systematic review and meta-analysis of available data, using standard methods
appropriate for diagnostic accuracy studies. The second step involves the convening of an Expert Group to
evaluate the strength of the evidence base and recommend operational and logistical considerations for
mainstreaming such tools/approaches into national TB control programmes, and/or identify gaps to be
addressed in future research. The third and final step involves WHO policy guidance on the use of these
tools/approaches, presented to the WHO Strategic and Technical Advisory Group for TB (STAG-TB) for
endorsement and subsequent dissemination to member states for implementation.
MEETING OBJECTIVE
To review the evidence base and evaluate data from systematic reviews on the performance
characteristics of commercial serological diagnostic tests for the diagnosis of tuberculosis.
EXPECTED OUTCOME
Evidence-based recommendations on the use of commercial serological diagnostic tests for the
diagnosis of pulmonary and extra-pulmonary tuberculosis.
1 Laboratory-based evaluation of 19 commercially available rapid diagnostic tests for tuberculosis. Diagnostics
Evaluation Series No. 2 - WHO/TDR, 10 October 2008

Annexes
Page | 44
Annex 2: Agenda
AGENDA
Chair and co-chair: H. Schünemann and K. Weyer
Rapporteur: P Godfrey-Fausset
09:00 - 09:10 Welcome M. Raviglione, WHO R. Ridley, TDR
09:10 - 09:20 Meeting scope and objectives K. Weyer
09:20 - 09:30 Declaration of Interest by Expert Group members C. Lienhardt
09:30 - 10:15 Systematic review and meta-analysis: Commercial
serological antibody detection tests for the diagnosis
of TB
K. Steingart
10:15 - 10:45 Discussion All
10:45 - 11:15 BREAK
11:15 - 11:45 TB serological testing in India: an economic-
epidemiological model
D. Dowdy & M. Pai
11:45 - 12:00 Discussion All
12:00 - 13:00 LUNCH
13:00 - 14:00 Draft recommendations: Use of commercial
serological antibody detection tests for the diagnosis
of TB
All
14:00 - 14:30 GRADE summary K. Weyer
14:30 - 14:45 Next steps K. Weyer
14:45 - 15:00 Closing M. Raviglione

Annexes
Page | 45
Annex 3: Meeting participants Expert Group Dr Richard A Adegbola Senior Program Officer Infectious Diseases, Global Health Bill & Melinda Gates Foundation P O Box 23350 Seattle, WA 98102 USA [email protected] Dr Lakhbir Singh Chauhan Deputy Director General of Health Services Ministry of Health and Family Welfare 522 "C" Wing, 5th Floor Nirman Bhavan 110011 - New Delhi India [email protected] Dr Daniela Cirillo Head, Emerging Bacterial Pathogens Unit San Raffaele del Monte Tabor Foundation (HSR), Emerging bacterial pathogens Via Olgettina 60 20132- Milan Italy [email protected] Dr Peter Godfrey-Faussett Department of Infection & Tropical Diseases London School of Hygiene & Tropical Medicine Keppel Street WC1E 7HT - London United Kingdom [email protected] Dr Anneke C Hesseling Professor and Director: Paediatric TB Research Program, Desmond Tutu TB Centre Department of Paediatrics and Child Health, Faculty of Health Sciences Stellenbosch University Private Bag X1 Matieland, 7602 South Africa [email protected]

Annexes
Page | 46
Dr Phillip Hill McAuley Professor of International Health Director, Centre for International Health Department of preventive and Social Medicine Univeristy of Otago School of Medicine PO BOX 913, Dunedin 9054 New Zealand [email protected] Mr Oluwamayowa Joel Communication for Development Centre 73, Ikosi Road, Ketu, Lagos State Nigeria [email protected] Dr Philip LoBue Associate Director for Science, Division of Tuberculosis Elimination National Center for STD, HIV/AIDS, Viral Hepatitis, and TB Prevention Centers for Disease Control and Prevention 1600 Clifton Road Mailstop E-04 Atlanta , GA 30333 USA [email protected] Dr Holger Schünemann Department of Clinical Epidemiology & Biostatistics Michael Gent Chair in Healthcare Research Professor of Clinical Epidemiology Biostatistics and Medicine McMaster University Health Sciences Centre, Room 2C10B 1200 Main Street West Hamilton Canada [email protected] Systematic reviewers and observers Dr Adithya Cattamanchi San Francisco General Hospital Pulmonary Division – Room 5K1 1001 Potrero Ave San Francisco, CA 94110 USA [email protected] Dr Anand Date HIV/AIDS Care & Treatment Branch (HIV/TB) Global AIDS Program Centers for Disease Control & Prevention 1600 Clifton Road Mailstop E-04 Atlanta , GA 30333 USA [email protected]

Annexes
Page | 47
Dr Anne Detjen Technical Consultant The Union North America Office International Union Against Tuberculosis and Lung Disease 61 Broadway, Suite 1720 New York, NY 10006 USA [email protected] Dr Richard Menzies Montreal Chest Institute Room K1.24, 3650 St. Urbain St. Montreal, PQ Canada H2X 2P4 [email protected] Dr John Metcalfe Division of Pulmonary and Critical Care Medicine University of California, San Francisco Division of Epidemiology University of California, Berkeley 230 Santa Paula Ave. San Francisco, CA 94127 USA [email protected] Dr Richard J O'Brien Foundation for New Innovative New Diagnostics (FIND) 16 Avenue de Budé 1202 Geneva Switzerland [email protected] Dr Madhukar Pai McGill University Dept of Epidemiology & Biostatistics 1020 Pine Ave West Montreal, QC H3A 1A2 Canada [email protected] Dr Karen R Steingart Physician Consultant Curry International Tuberculosis Center University of California, San Francisco 3180 18th Street, Suite 101 San Francisco, CA 94110-2028 USA [email protected]

Annexes
Page | 48
Dr Alice Zwerling Montreal Chest Institute, Rm K3.09 3650 St Urbain, Montreal, Quebec H2X 2P4 Canada [email protected] Dr Molebogeng Rangaka Institute of Infectious Diseases and Molecular Medicine School of Health Sciences University of Cape Town Observatory, 7925 South Africa [email protected] [email protected] Dr Suman Laal Associate Professor of Pathology & Microbiology NYU Langone Medical Center c/o VA Medical Center 423 East 23rd Street, Room 18123N New York, NY 10010 USA [email protected]

Annexes
Page | 49
WHO HQ Staff Dr Chris Gilpin, TBL [email protected] Mr Jean Iragena, TBL [email protected] Dr Christian Lienhardt, TBP [email protected] Dr Fuad Mirzayev, TBL [email protected] Dr Mario Raviglione, Director, STB [email protected] Dr Diana Weil, Coordinator, STB [email protected] Dr Karin Weyer, Coordinator, TBL [email protected] Dr Matteo Zignol, TBS [email protected] WHO/TDR Dr Luis Cuevas [email protected] Dr Andy Ramsay [email protected]

Annexes
Page | 50
Annex 4: Declarations of Interest
None declared
R. Adegbola
A. Cattamanchi
L. Chauhan
D. Cirillo
P. Godfrey-Fausset
A. Hesseling
P. Hill
P. LoBue
H. Schüneman
J. Oluwamayowa
Declared, insignificant
C. Boehme (FIND support to academia to develop POC serodiagnostic test, FIND biomarker discovery
project
R. O’Brien (FIND support to academia to develop POC serodiagnostic test, FIND biomakarker discovery
project)
Declared, significant (observer status)
D. Dowdy (relevant research, participation in systematic review)
M. Pai (relevant research, participation in systematic reviews)
S. Laal (relevant research, participation in systematic reviews )
K. Steingart (principal systematic reviewer)
R. Menzies (principal systematic reviewer)
A. Detjen (principal systematic reviewer)

Annexes
Page | 51
Annex 5: Included studies
Pulmonary TB
1. Alifano M, Del Pezzo M, Lamberti C, Faraone S, Covelli I. ELISA method for evaluation of anti-A60 IgG in patients with pulmonary and extrapulmonary tuberculosis. New Microbiol. 1994 Jan;17(1):37-43.
2. Alifano M, Sofia M, Mormile M, et al. IgA immune response against the mycobacterial antigen A60 in patients with active pulmonary tuberculosis. Respiration. 1996;63(5):292-7.
3. Alifano M, De Pascalis R, Sofia M, Faraone S, Del Pezzo M, Covelli I. Evaluation of IgA-mediated humoral immune response against the mycobacterial antigen P-90 in diagnosis of pulmonary tuberculosis. Chest. 1997 Mar;111(3):601-5.
4. Amicosante M, Houde M, Guaraldi G, Saltini C. Sensitivity and specificity of a multi-antigen ELISA test for the serological diagnosis of tuberculosis. Int J Tuberc Lung Dis. 1999 Aug;3(8):736-40.
5. Anderson B L, Welch R J, Litwin C M. Assessment of three commercially available serologic assays for detection of antibodies to Mycobacterium tuberculosis and identification of active tuberculosis. Clin Vaccine Immunol. 2008 Nov;15(11):1644-9.
6. Bukhary Z A. Evaluation of anti-A60 antigen IgG enzyme-linked immunosorbent assay for serodiagnosis of pulmonary tuberculosis. Ann Thorac Med. 2007 Apr;2(2):47-51.
7. Chandrasekaran S, Gupta E V V, Chauhan M M, Baily G V J, Chaudhuri K. Serodiagnosis of pulmonary tuberculosis by kaolin agglutination test. Indian Journal of Tuberculosis. 1990;37(1):11-5.
8. Conde M B, Suffys P, Silva J, Kritski A L, Dorman S E. Immunoglobulin a (IgA) and IgG immune responses against P-90 antigen for diagnosis of pulmonary tuberculosis and screening for Mycobacterium tuberculosis infection. Clinical and Diagnostic Laboratory Immunology. 2004 Jan;11(1):94-7.
9. D'Alessandro A, de Waard J H. [Evaluation of two commercial tests for the serodiagnosis of pulmonary tuberculosis]. Rev Chilena Infectol. 2008 Feb;25(1):37-40.
10. Erer O F, Biçmen C, Kýraklý C, Aktoðu S, Florat N, Tibet G. Diagnostic Value of a Rapid Immunochromotographic Test (ICT) in Patients With Active Pulmonary Tuberculosis. Toraks Dergisi. 2001;2(1):80-4.
11. Gao M-q, Chu N-h, Wang H-y, et al. The clinical significance of serum tuberculosis specific antigen antibody in the diagnosis of tuberculosis. Zhonghua Jiehe He Huxi Zazhi. 2007 Dec;30(12):918-20.
12. Imaz M S, Comini M A, Zerbini E, et al. Evaluation of commercial enzyme-linked immunosorbent assay kits for detection of tuberculosis in Argentinean population. J Clin Microbiol. 2004 Feb;42(2):884-7.
13. Julian E, Matas L, Alcaide J, Luquin M. Comparison of antibody responses to a potential combination of specific glycolipids and proteins for test sensitivity improvement in tuberculosis serodiagnosis. Clin Diagn Lab Immunol. 2004 Jan;11(1):70-6.
14. Julian E, Matas L, Hernandez A, Alcaide J, Luquin M. Evaluation of a new serodiagnostic tuberculosis test based on immunoglobulin A detection against Kp-90 antigen. IntJTubercLung Dis. 2000;4:1082-5.

Annexes
Page | 52
15. Kalantri Y, Hemvani N, Bhatia G C, Chitnis D S. Elisa kit evaluation for IgG and IgM antibodies to A-60 tubercular protein antigen. Indian Journal of Medical Sciences. 2005;59(8):337-46.
16. Kassa-Kelembho E, Kassa E, Zandanga G, Service Y-B, Ignaleamoko A, Talarmin A. Poor performance of a novel serological test for diagnosis of pulmonary tuberculosis in Bangui, Central African Republic. Clinical and Vaccine Immunol. 2006;13(6):702-3.
17. Luh K T, Yu C J, Yang P C, Lee L N. Tuberculosis antigen A60 serodiagnosis in tuberculous infection: application in extrapulmonary and smear-negative pulmonary tuberculosis. Respirology. 1996 Jun;1(2):145-51.
18. Maekura R, Kohno H, Hirotani A, et al. Prospective clinical evaluation of the serologic tuberculous glycolipid test in combination with the nucleic acid amplification test. J Clin Microbiol. 2003 Mar;41(3):1322-5.
19. Maekura R, Okuda Y, Nakagawa M, et al. Clinical evaluation of anti-tuberculous glycolipid immunoglobulin G antibody assay for rapid serodiagnosis of pulmonary tuberculosis. J Clin Microbiol. 2001 Oct;39(10):3603-8.
20. McConkey S J, Youssef F G, Azem E, Frenck R W, Weil G J. Evaluation of a rapid-format antibody test and the tuberculin skin test for diagnosis of tuberculosis in two contrasting endemic settings. Int J Tuberc Lung Dis. 2002 Mar;6(3):246-52.
21. Mizusawa M, Kawamura M, Takamori M, et al. Increased synthesis of anti-tuberculous glycolipid immunoglobulin G (IgG) and IgA with cavity formation in patients with pulmonary tuberculosis. Clin Vaccine Immunol. 2008 Mar;15(3):544-8.
22. Mukhopadhyay A, Guan M, Chen H Y, Lu Y, Lim T K. Prospective study of a new serological test (ASSURE TB Rapid Test) for the diagnosis of pulmonary tuberculosis. Int J Tuberc Lung Dis. 2006 Jun;10(6):620-4.
23. Nurkic M, Imamovic A, Numanovic F, Gegic M, Osmic M, Hadzihafizbegovic S. [Diagnostical values of antibody on A60 antigen in diagnostic of tuberculosis]. Med Arh. 2006;60(3):166-70.
24. Okuda Y, Maekura R, Hirotani A, et al. Rapid serodiagnosis of active pulmonary Mycobacterium tuberculosis by analysis of results from multiple antigen-specific tests. J Clin Microbiol. 2004 Mar;42(3):1136-41.
25. Ongut G, Ogunc D, Gunseren F, et al. Evaluation of the ICT Tuberculosis test for the routine diagnosis of tuberculosis. BMC Infect Dis. 2006 Feb 27;6(1):37.
26. Platonova I L, Sakhelashvili M I. [Comparative evaluation of the informative value of the rapid serochek mbt test to determine mycobacterium tuberculosis antibodies and mantoux tuberculin test in adults]. Problemy tuberkuleza I boleznei legkikh. 2007;8:10-13.
27. Somi G R, O'Brien R J, Mfinanga G S, Ipuge Y A. Evaluation of the MycoDot (TM) test in patients with suspected tuberculosis in a field setting in Tanzania. Inter J TubercLung Dis. 1999 Mar;3(3):231-8.
28. Traunmuller F, Haslinger I, Lagler H, Wolfgang G, Zeitlinger M A, Abdel Salam H A. Influence of the washing buffer composition on the sensitivity of an enzyme-linked immunosorbent assay using mycobacterial glycolipids as capture antigens. J Immunoassay Immunochem. 2005;26(3):179-88.

Annexes
Page | 53
29. Wilkinson R J, Haslov K, Rappuoli R, et al. Evaluation of the recombinant 38-kilodalton antigen of
Mycobacterium tuberculosis as a potential immunodiagnostic reagent. J Clin Microbiol. 1997 Mar;35(3):553-7.
30. Wu H P, Hua C C, Yu C C, Wu S Y. Comparison of plasma interferon-gamma and antigen 60 immunoglobulin G in diagnosing pulmonary Mycobacterium tuberculosis infection. Chang Gung Medical Journal. 2005;28(11):779-85.
31. Wu H P, Shieh W B, Hsien F K, Hua C C. The significance of Mycobacterium tuberculosis antibody, antigen 60 IgG in patients with abnormal chest radiography. Chang Gung Med J. 2004 Dec;27(12):869-76.
Extrapulmonary TB
1. Alifano M, De Pascalis R, Sofia M, Faraone S, Del Pezzo M, Covelli I. Detection of IgG and IgA against the mycobacterial antigen A60 in patients with extrapulmonary tuberculosis. Thorax. 1998 May;53(5):377-80.
2. Banerjee S, Gupta S, Shende N, Kumar S, Harinath B C. Serodiagnosis of tuberculosis using two ELISA systems. Indian Journal of Clinical Biochemistry. 2003;18(2):48-53.
3. Caminero J A, Rodriguez de Castro F, Carrillo T, Diaz F, Rodriguez Bermejo J C, Cabrera P. Diagnosis of pleural tuberculosis by detection of specific IgG anti-antigen 60 in serum and pleural fluid. Respiration. 1993;60(1):58-62.
4. Caminero J A, Rodriguez de Castro F, Carrillo T, Lafarga B, Diaz F, Cabrera P. Value of ELISA using A60 antigen in the serodiagnosis of tuberculosis. Respiration. 1994;61:283-6.
5. Chierakul N, Damrongchokpipat P, Chaiprasert A, Arjratanakul W. Antibody detection for the diagnosis of tuberculous pleuritis. Int J Tuberc Lung Dis. 2001 Oct;5(10):968-72.
6. Gevaudan M J, Bollet C, Charpin D, Mallet M N, De Micco P. Serological response of tuberculosis patients to antigen 60 of BCG. Eur J Epidemiol. 1992 Sep;8(5):666-76.
7. Kunter E, Cerrahoglu K, Ilvan A, et al. The value of pleural fluid anti-A60 IgM in BCG-vaccinated tuberculous pleurisy patients. Clin Microbiol Infect. 2003 Mar;9(3):212-20.
8. Luh K T, Yu C J, Yang P C, Lee L N. Tuberculosis antigen A60 serodiagnosis in tuberculous infection: application in extrapulmonary and smear-negative pulmonary tuberculosis. Respirology. 1996 Jun;1(2):145-51.
9. McConkey S J, Youssef F G, Azem E, Frenck R W, Weil G J. Evaluation of a rapid-format antibody test and the tuberculin skin test for diagnosis of tuberculosis in two contrasting endemic settings. Int J Tuberc Lung Dis. 2002 Mar;6(3):246-52.
10. Nsanze H, Ameen A S, Fares E, Vargees L, Mustafa N. Serodiagnosis of tuberculosis and leprosy by enzyme immunoassay. Clinical Microbiology and Infection. 1997;3(2):236-9.

Annexes
Page | 54
11. Ratanasuwan W, Kreiss J K, Nolan C M, et al. Evaluation of the MycoDot test for the diagnosis of tuberculosis in HIV seropositive and seronegative patients. Int J Tuberc Lung Dis. 1997 Jun;1(3):259-64.
12. Senol G, Erer O F, Yalcin Y A, et al. Humoral immune response against 38-kDa and 16-kDa mycobacterial antigens in tuberculosis. Eur Respir J. 2007 Jan;29(1):143-8.

Annexes
Page | 55
Annex 6: Excluded studies
(Reasons for exclusion in parenthesis after reference)
1. Achkar JM, Dong Y, Holzman RS, Belisle J, Kourbeti IS, Sherpa T, et al. Mycobacterium tuberculosis malate synthase- and MPT51-based serodiagnostic assay as an adjunct to rapid identification of pulmonary tuberculosis. Clin Vaccine Immunol. 2006 Nov;13(11):1291-3. (Noncommercial)
2. Achkar JM, Jenny-Avital E, Yu X, Burger S, Leibert E, Bilder PW, et al. Antibodies against Immunodominant Antigens of Mycobacterium tuberculosis in Tuberculosis Suspects in the US: A Comparison by HIV Status. Clin Vaccine Immunol. 2010 Jan 13. (Noncommercial)
3. Ahmed S O, Kharal S A, Hasan S S, Shah E S, Rahat N, Begum B. Elisa method for evaluation of anti A60 IgG for the diagnosis of tuberculosis. Journal of the Liaquat University of Medical and Health Sciences. 2008;7(1):25-30. (Reference standard not satisfied)
4. Alavi-Naini R, Metanat M, Alijani E, Mozaffar H. Patho-TB test for the rapid diagnosis of pulmonary tuberculosis. Journal of Research in Medical Sciences. 2009 Sep-Oct;14(5):301-7. (Antigen detection)
5. 5 Almeida CM, Vasconcelos AC, Kipnis A, Andrade AL, Junqueira-Kipnis AP. Humoral immune responses of tuberculosis patients in Brazil indicate recognition of Mycobacterium tuberculosis MPT-51 and GlcB. Clinical and Vaccine Immunology. 2008 Mar;15(3):579-81. (Noncommercial)
6. Amor YB, Shashkina E, Johnson S, Bifani PJ, Kurepina N, Kreiswirth B, et al. Immunological characterization of novel secreted antigens of Mycobacterium tuberculosis. Scandinavian Journal of Immunology. 2005 Feb;61(2):139-46. (Noncommercial)
7. Araujo Z, Giampietro F, Cancado LC, Singh M, Wide A. Comparison of serological responses in two different populations with pulmonary tuberculosis. Mem Inst Oswaldo Cruz. 2008 Nov;103(7):661-7. (Noncommercial)
8. Asceric M, Nadarevic A, Avdic S, Vrabac-Mujcinagic M, Nukic S, Mujcinovic Z. Hexagon TB for the rapid diagnosis of lung TBC in praxis. Bosn J Basic Med Sci. 2007 Aug;7(3):218-21. (Fewer than 10)
9. Ashino J, Ashino Y, Guio H, Saitoh H, Mizusawa M, Hattori T. Low antibody response against tuberculous glycolipid (TBGL) in elderly gastrectomised tuberculosis patients. Int J Tuberc Lung Dis. 2005 Sep;9(9):1052-3. (Active TB, unspecified)
10. Azzurri A, Kanaujia GV, Sow OY, Bah B, Diallo A, Del Prete G, et al. Serological markers of pulmonary tuberculosis and of response to anti-tuberculosis treatment in a patient population in Guinea. International Journal of Immunopathology and Pharmacology. 2006 Jan-Mar;19(1):199-208. (Noncommercial)
11. Baassi L, El Fenniri L, Bourkkadi J, et al. [Diagnosis of pulmonary tuberculosis: evaluation of the TB IgA EIA assay in Morocco]. East Mediterr Health J. 2007 Jan-Feb;13(1):72-8. (Reference standard not satisfied)
12. Bahk YY, Kim SA, Kim JS, Euh HJ, Bai GH, Cho SN, et al. Antigens secreted from Mycobacterium tuberculosis: Identification by proteomics approach and test for diagnostic marker. Proteomics. 2004 Nov;4(11):3299-307. (Noncommercial)

Annexes
Page | 56
13. Bai X, Wei Q, Li J, Li G. [Recombinant phosphoenolpyruvate carboxykinase from Mycobacterium tuberculosis for sero diagnosis]. Wei Sheng Wu Xue Bao. 2008 Oct 4;48(10):1383-6. (Noncommercial)
14. Beck ST, Leite OM, Arruda RS, Ferreira AW. Combined use of Western Blot/ELISA to improve the serological diagnosis of human tuberculosis. Brazilian Journal of Infectious Diseases. 2005;9(1):35-43. (Noncommercial)
15. Beck ST, Leite OM, Arruda RS, Ferreira AW. Humoral response to low molecular weight antigens of Mycobacterium tuberculosis by tuberculosis patients and contacts. Brazilian Journal of Medical and Biological Research. 2005 Apr;38(4):587-96. (Noncommercial)
16. Benabdesselem C, Fathallah DM, Huard RC, Zhu H, Jarboui MA, Dellagi K, et al. Enhanced patient serum immunoreactivity to recombinant Mycobacterium tuberculosis CFP32 produced in the yeast Pichia pastoris compared to Escherichia coli and its potential for serodiagnosis of tuberculosis. J Clin Microbiol. 2006 Sep;44(9):3086-93. (Noncommercial)
17. Ben-Selma W, Ben-Kahla I, Marzouk M, Ferjeni A, Ghezal S, Ben-Said M, et al. Rapid detection of Mycobacterium tuberculosis in sputum by Patho-TB kit in comparison with direct microscopy and culture. Diagn Microbiol Infect Dis. 2009 Nov;65(3):232-5. (Antigen detection)
18. Bera S, Shende N, Kumar S, Harinath BC. Detection of antigen and antibody in childhood tuberculous meningitis. Indian J Pediatr. 2006 Aug;73(8):675-9. (Noncommercial)
19. Bethunaickan R, Baulard AR, Locht C, Raja A. Antibody response in pulmonary tuberculosis against recombinant 27kDa (MPT51, Rv3803c) protein of Mycobacterium tuberculosis. Scand J Infect Dis. 2007;39(10):867-74. (Noncommercial)
20. Beyene D, Lumc Franken K, Yamuah L, Aseffa A, Wiker HG, Kolk A, et al. Serodiagnosis of tuberculous lymphadenitis using a combination of antigens. J Infect Dev Ctries. 2010;4(2):96-102. (Noncommercial)
21. Bezerra JM, Beck ST, Kanunfre KA, Leite OM, Ferreira AW. A study of IgA antibody response to different mycobacterium tuberculosis antigens in the diagnosis and monitoring of pulmonary tuberculosis. Braz J Infect Dis. 2009 Feb;13(1):53-8. (Noncommercial)
22. Bhatia AS, Gupta S, Shende N, Kumar S, Harinath BC. Serodiagnosis of childhood tuberculosis by ELISA. Indian Journal of Pediatrics. 2005 May;72(5):383-7. (Noncommercial)
23. Bi A-x, Ding Y-s, Liu Z-h, Hu Z-y. [Expression and purification of CFP32 of Mycobacterium tuberculosis and its serodiagnostic analysis]. Zhonghua Yufang Yixue Zazhi. 2008 Feb 6;42(2):81-5. (Noncommercial)
24. Castro CM, Porras TB, Guerrero MI, Leon CI, Mojica MA, Lara M, et al. [Development of a multiantigenic serological test for tuberculosis diagnosis]. Biomedica. 2005 Mar;25(1):55-64. (Noncommercial)
25. Chaudhary VK, Kulshreshta A, Gupta G, Verma N, Kumari S, Sharma SK, et al. Expression and purification of recombinant 38-kDa and Mtb81 antigens of Mycobacterium tuberculosis for application in serodiagnosis. Protein Expression and Purification. 2005 Mar;40(1):169-76. (Noncommercial)
26. Chou CH, Huang YT, Hsu HL, Lai CC, Liao CH, Hsueh PR. Rapid identification of the Mycobacterium tuberculosis complex by an enzyme-linked immunosorbent assay. Int J Tuberc Lung Dis. 2009 Aug;13(8):996-1001. (Antigen detection)

Annexes
Page | 57
27. Corstjens PL, Chen Z, Zuiderwijk M, Bau HH, Abrams WR, Malamud D, et al. Rapid assay format for
multiplex detection of humoral immune responses to infectious disease pathogens (HIV, HCV, and TB). Ann N Y Acad Sci. 2007 Mar;1098:437-45. (Noncommercial)
28. Das AK, Harinath BC. Comparative analysis of ES-31 and ES-41 antigens in the detection of tubercular IgG antibodies and study on combine sensitivity of antibody-antigen. Biosciences Biotechnology Research Asia. 2008;5(1):359-62. (Noncommercial)
29. Davidow A, Kanaujia GV, Shi L, Kaviar J, Guo X, Sung N, et al. Antibody profiles characteristic of Mycobacterium tuberculosis infection state. Infection and Immunity. 2005;73(10):6846-51. (Noncommercial)
30. Dayal R, Singh A, Katoch VM, Joshi B, Chauhan DS, Singh P, et al. Serological diagnosis of tuberculosis. Indian J Pediatr. 2008 Dec;75(12):1219-21. (Noncommercial)
31. Dayal R, Sirohi G, Singh MK, Mathur PP, Agarwal BM, Katoch VM, et al. Diagnostic value of Elisa serological tests in childhood tuberculosis. J Trop Pediatr. 2006 Dec;52(6):433-7. (Noncommercial)
32. de Larrea CF, de Waard JH, Giampietro F, Araujo Z. The secretory immunoglobulin A response to Mycobacterium tuberculosis in a childhood population. Rev Soc Bras Med Trop. 2006 Sep-Oct;39(5):456-61. (Noncommercial)
33. Demissie A, Leyten EMS, Abebe M, Wassie L, Aseffa A, Abate G, et al. Recognition of stage-specific mycobacterial antigens differentiates between acute and latent infections with Mycobacterium tuberculosis. Clinical and Vaccine Immunology. 2006 Feb;13(2):179-86. (Noncommercial)
34. Demkow U, Filewska M, Michalowska-Mitczuk D, Kus J, Jagodzinski J, Zielonka T, et al. Heterogeneity of antibody response to myobacterial antigens in different clinical manifestations of pulmonary tuberculosis. J Physiol Pharmacol. 2007 Nov;58 Suppl 5(Pt 1):117-27. (Insufficient data)
35. Demkow U, Ziolkowski J, Bialas-Chromiec B, Filewska M, Zielonka T, Wasik M, et al. Humoral immune response against mycobacterial antigens in children with tuberculosis. J Physiol Pharmacol. 2006 Sep;57 Suppl 4:63-73. (Insufficient data)
36. Diaz FA, Martinez RA. Serological tests in the diagnosis of tuberculosis. Biomedica: revista del Instituto Nacional de Salud. 2005;25(3):422-3; author reply 3-4. (Insufficient data)
37. Dinnes J, Deeks J, Kunst H, et al. A systematic review of rapid diagnostic tests for the detection of tuberculosis infection. Health Technol Assess. 2007 Jan;11(3):1-196. (Systematic review; not a primary study)
38. Doveren RFC, Goudswaard J, Hendriks JCM, Bins MC, van Belzen C. Prognostic variables for high titres in a fluorescent antibody test to diagnose tuberculosis. Respiratory Medicine. 2005 Apr;99(4):477-84. (Noncommercial)
39. El-Shazly S, Mustafa AS, Ahmad S, Al-Attiyah R. Utility of three mammalian cell entry proteins of Mycobacterium tuberculosis in the serodiagnosis of tuberculosis. Int J Tuberc Lung Dis. 2007 Jun;11(6):676-82. (Noncommercial)

Annexes
Page | 58
40. Fabre M, Gerome P, Maslin J, Herve V, Vong R, Carpentier G, et al. Assessment of the Patho-TBTM kit for diagnosis of tuberculosis. Pathologie Biologie. 2007;55(10):482-5. (Antigen detection)
41. Fujita Y, Doi T, Maekura R, Ito M, Yano I. Differences in serological responses to specific glycopeptidolipid-core and common lipid antigens in patients with pulmonary disease due to Mycobacterium tuberculosis and Mycobacterium avium complex. Journal of Medical Microbiology. 2006;55(2):189-99. (Noncommercial)
42. Fujita Y, Doi T, Sato K, Yano I. Diverse humoral immune responses and changes in IgG antibody levels against mycobacterial lipid antigens in active tuberculosis. Microbiology-Sgm. 2005 Jun;151:2065-74. (Noncommercial)
43. Fujita Y, Ogata H, Yano I. Clinical evaluation of serodiagnosis of active tuberculosis by multiple-antigen ELISA using lipids from Mycobacterium bovis BCG Tokyo 172. Clinical Chemistry and Laboratory Medicine. 2005;43(11):1253-62. (Noncommercial)
44. Gennaro ML, Affouf M, Kanaujia GV, Brusasca PN, Mangura B, Reichman L. Antibody markers of incident tuberculosis among HIV-infected adults in the USA: a historical prospective study. Int J Tuberc Lung Dis. 2007 Jun;11(6):624-31. (Noncommercial)
45. Greenaway C, Lienhardt C, Adegbola R, Brusasca P, McAdam K, Menzies D. Humoral response to Mycobacterium tuberculosis antigens in patients with tuberculosis in the Gambia. International Journal of Tuberculosis and Lung Disease. 2005;9(10):1112-9. (Noncommercial)
46. Gupta S, Shende N, Bhatia AS, Kumar S, Harinath BC. IgG subclass antibody response to mycobacterial serine protease at different stages of pulmonary tuberculosis. Medical Science Monitor. 2005;11(12):CR585-CR8. (Noncommercial)
47. Gupta S, Shende N, Kumar S, Harinath BC. Detection of antibodies to a cocktail of mycobacterial excretory-secretory antigens in tuberculosis by ELISA and immunoblotting. Current Science. 2005 Jun;88(11):1825-7. (Noncommercial)
48. Harinath BC, Kumar S, Roy SS, Hirudkar S, Upadhye V, Shende N. A cocktail of affinity-purified antibodies reactive with diagnostically useful mycobacterial antigens ES-31, ES-43, and EST-6 for detecting the presence of Mycobacterium tuberculosis. Diagnostic Microbiology and Infectious Disease. 2006;55(1):65-8. (Noncommercial)
49. Hauer B, Diel R, Priwitzer M, Rusch-Gerdes S, Schaberg T, Loddenkemper R. [The new tuberculosis rapid assay from DiaVita - no improvement of diagnostic]. Pneumologie. 2008 Aug;62(8):480-1. (Editorial and commentary)
50. Hauer B, Mauch H, Loddenkemper R, Forssbohm M, Fruh J, Loytved G, et al. The tuberculosis rapid assay from DiaVita - No alternative to the tuberculin skin test. Pneumologie. 2005;59(10):681-4. (Editorial and commentary)
51. Hoff ST, Abebe M, Ravn P, Range N, Malenganisho W, Rodriques DS, et al. Evaluation of Mycobacterium tuberculosis--specific antibody responses in populations with different levels of exposure from Tanzania, Ethiopia, Brazil, and Denmark. Clin Infect Dis. 2007 Sep 1;45(5):575-82. (Noncommercial)

Annexes
Page | 59
52. Iacob G, Iacob S, Banica D, Cojocaru M. Diagnostic utility of Elisa method using mycobacterial antigen A60 in neurotuberculosis diagnosis. Archives of the Balkan Medical Union. 2007;42(2):75-9. (Could not obtain)
53. Imaz MS, Schmelling MF, Kaempfer S, Spallek R, Singh M. Serodiagnosis of tuberculosis: specific detection of free and complex-dissociated antibodies anti-mycobacterium tuberculosis recombinant antigens. Braz J Infect Dis. 2008 Jun;12(3):234-44. (Noncommercial)
54. Jackson M, Gicquel B. Desaturase antigen of mycobacterium tuberculosis. 2006 Jul 4 2006. (Noncommercial)
55. Jain AK, Jena SK, Singh M, Dhammi I, Ramachadran V, Dev G. Evaluation of clinico-radiological, bacteriological, serological, molecular and histological diagnosis of osteoarticular tuberculosis. Indian J Orthop. 2008 Apr;42(2):173-7. (Insufficient data)
56. Kaisermann MC, Sardella IG, Trajman A, Coelho LV, Kampfer S, Jonas F, et al. IgA antibody responses to Mycobacterium tuberculosis recombinant MPT-64 and MT-10.3 (Rv3019c) antigens in pleural fluid of patients with tuberculous pleurisy. International Journal of Tuberculosis and Lung Disease. 2005 Apr;9(4):461-6. (Noncommercial)
57. Kalra M, Khuller GK, Grover A, Behera D, Wanchu A, Verma I. Utility of a combination of RD1 and RD2 antigens as a diagnostic marker for tuberculosis. Diagn Microbiol Infect Dis. Feb;66(2):153-61. (Noncommercial)
58. Kanaujia GV, Lam PK, Perry S, Brusasca PN, Catanzaro A, Gennaro ML. Integration of microscopy and serodiagnostic tests to screen for active tuberculosis. International Journal of Tuberculosis and Lung Disease. 2005;9(10):1120-6. (Noncommercial)
59. Kashino SS, Pollock N, Napolitano DR, Rodrigues V, Jr., Campos-Neto A. Identification and characterization of Mycobacterium tuberculosis antigens in urine of patients with active pulmonary tuberculosis: an innovative and alternative approach of antigen discovery of useful microbial molecules. Clin Exp Immunol. 2008 Jul;153(1):56-62. (Antigen detection)
60. Katti MK, Azeem M. A novel erythrocyte-based immunoassay for simultaneous detection of both antimycobacterial antibody response and mycobacterial antigen in human serum samples of pulmonary tuberculosis and a control group of patients using 'a single probe'. Fems Immunology and Medical Microbiology. 2006 Jun;47(1):134-7. (Noncommercial)
61. Khan N, Alam K, Nair S, Valluri VL, Murthy KJ, Mukhopadhyay S. Association of strong immune responses to PPE protein Rv1168c with active tuberculosis. Clin Vaccine Immunol. 2008 Jun;15(6):974-80. (Noncommercial)
62. Khan N, Mian I, Zia U, Muhammad J. Performance of ICT-TB test in the detection of pulmonary and extra-pulmonary tuberculosis. J Ayub Med Coll Abbottabad. 2004 Apr-Jun;16(2):55-6. (Reference standard not satisfied)
63. Khosravi A D, Torabizadeh R, Landi A. Investigation of the level of IgG, IgM and IgA antibodies against A60 antigen in tuberculosis patients referred to PHLS, Ahvaz, Iran. Pakistan Journal of Medical Sciences. 2005;21(4):465-9. (Reference standard not satisfied)

Annexes
Page | 60
64. Kim SY, Shin AR, Kim HJ, Cho SN, Park JK, Shin SJ. Identification of Rv2041c, a Novel Immunogenic Antigen from Mycobacterium tuberculosis with Serodiagnostic Potential. Scandinavian Journal of Immunology. 2009;70(5):457-64. (Duplicate)
65. Kochak HE, Ahmad S, Alinaghi S, Zarghom O, Hekmat S, Jam S, et al. Evaluation of serological tests using A60 antigen for diagnosis of tuberculosis. Acta Medica Iranica. 2010;48(1):21-6. (Insufficient data)
66. Koh KW, Soh SE, Seah GT. Strong Antibody Responses to Mycobacterium tuberculosis PE-PGRS62 Protein Are Associated with Latent and Active Tuberculosis. Infection and Immunity. 2009 Aug;77(8):3337-43. (Noncommercial)
67. Kondo A, Oketani N, Maruyama M, et al. [Serological diagnosis of pulmonary tuberculosis and nontuberculous pulmonary mycobacteriosis]. Kekkaku. 2001 Sep;76(9):603-14. (Reference standard not satisfied)
68. Kozlowska I, Filewska M, Rozy A, Augustynowicz-Kopec E, Krawiecka D, Broniarek-Samson B, et al. [Evaluation of humoral immune response against mycobacterial antigens in bronchoalveolar lavage fluid from patients with pulmonary tuberculosis confirmed by genetic and culture methods]. Pneumonol Alergol Pol. 2007;75(4):355-62. (Evaluation of an antibody-based detection test in specimen other than serum)
69. Kulikovskaia NV, Vaneeva TV, Moroz IA, Nosova EI, Lazareva OL, Lovacheva OV, et al. Potentialities of laboratory diagnosis in tuberculous meningitis. Problemy tuberkuleza i boleznei legkikh. 2005(8):39-42. (Noncommercial)
70. Kulshrestha A, Gupta A, Verma N, Sharma SK, Tyagi AK, Chaudhary VK. Expression and purification of recombinant antigens of Mycobacterium tuberculosis for application in serodiagnosis. Protein Expression and Purification. 2005;44(1):75-85. (Noncommercial)
71. Kumar G, Dagur PK, Singh M, Yadav VS, Dayal R, Singh HB, et al. Diagnostic potential of Ag85C in comparison to various secretory antigens for childhood tuberculosis. Scand J Immunol. 2008 Aug;68(2):177-83. (Noncommercial)
72. Kumar G, Dagur PK, Singh PK, Shankar H, Yadav VS, Katoch VM, et al. Serodiagnostic Efficacy of Mycobacterium tuberculosis 30/32-kDa Mycolyl Transferase Complex, ESAT-6, and CFP-10 in Patients with Active Tuberculosis. Arch Immunol Ther Exp (Warsz). 2010 Feb;58(1):57-65. (Noncommercial)
73. Lawn SD, Edwards DJ, Kranzer K, Vogt M, Bekker LG, Wood R. Urine lipoarabinomannan assay for tuberculosis screening before antiretroviral therapy diagnostic yield and association with immune reconstitution disease. AIDS. 2009 Sep 10;23(14):1875-80. (Antigen detection)
74. Le Moigne V, Robreau G, Borot C, Guesdon JL, Mahana W. Expression, immunochemical characterization and localization of the Mycobacterium tuberculosis protein p27. Tuberculosis. 2005 Jul;85(4):213-9. (Noncommercial)
75. Lee JS, Jo EK, Noh YK, Shin AR, Shin DM, Son JW, et al. Diagnosis of pulmonary tuberculosis using MTB12 and 38-kDa antigens. Respirology. 2008 May;13(3):432-7. (Noncommercial)

Annexes
Page | 61
76. Liu ZH, Qin LH, Feng YH, Bi AX, Yang H, Ding YS, et al. [Identification of the Mycobacterium tuberculosis complex by detecting recombinant secretory protein MPT64.]. Zhonghua Jie He He Hu Xi Za Zhi. 2009 Aug;32(8):608-12. (Noncommercial)
77. Majumdar A, Upadhye V, Harinath BC. Peroxidase enzyme immunoassay for circulating SEVA TB ES-31 antigen in pulmonary tuberculosis sera. Biomedical Research. 2008;19(3):201-6. (Antigen detection)
78. Majumdar A, Upadhye V, Harinath BC. A prospective study of inhouse developed SEVA TB ELISA using cocktail of antigens and their immunoglobulins in the diagnosis of tuberculosis suspected patients in a tertiary care hospital located in rural area. Biomedical Research. 2009;20(1):59-63. (Noncommercial)
79. Malen H, Softeland T, Wiker HG. Antigen analysis of Mycobacterium tuberculosis H37Rv culture filtrate proteins. Scandinavian Journal of Immunology. 2008 Mar;67(3):245-52. (Noncommercial)
80. Mathur ML, LoBue PA, Catanzaro A. Evaluation of a serologic test for the diagnosis of tuberculosis. Int J Tuberc Lung Dis. 1999 Aug;3(8):732-5. (Active TB, unspecified; information requested from author)
81. Morimoto T, Takanashi S, Hasegawa Y, Fujimoto K, Okudera K, Hayashi A, et al. Level of antibodies against mycobacterial glycolipid in the effusion for diagnosis of tuberculous pleural effusion. Respiratory Medicine. 2006;100(10):1775-80. (Evaluation of an antibody-based detection test in specimen other than serum)
82. Mudaliar AV, Kashyap RS, Purohit HJ, Taori GM, Daginawala HF. Detection of 65 kD heat shock protein in cerebrospinal fluid of tuberculous meningitis patients. BMC Neurol. 2006;6:34. (Antigen detection)
83. Mukherjee P, Dutta M, Datta P, Dasgupta A, Pradhan R, Pradhan M, et al. The RD1-encoded antigen Rv3872 of Mycobacterium tuberculosis as a potential candidate for serodiagnosis of tuberculosis. Clin Microbiol Infect. 2007 Feb;13(2):146-52. (Noncommercial)
84. Muramira M N. Evaluation of TB-ST tuberculosis rapid test in adult pulmonary tuberculosis in Rwanda Universite Nationale du Rwanda; 2007. (Reference standard not satisfied)
85. Murthy MK, Parasa RR, Deenadayalan A, Sharma P, Raja A. Evaluation of the diagnostic potential of region of deletion-1-encoded antigen culture filtrate protein-10 in pulmonary tuberculosis. Diagn Microbiol Infect Dis. 2007 Nov;59(3):295-302. (Fewer than 10)
86. Nabeshima S, Murata M, Kashiwagi K, Fujita M, Furusyo N, Hayashi J. Serum antibody response to tuberculosis-associated glycolipid antigen after BCG vaccination in adults. Journal of Infection and Chemotherapy. 2005;11(5):256-8. (Fewer than 10)
87. Nagel T, Ehrentreich-Forster E, Singh M, Schmitt K, Brandenburg A, Berka A, et al. Direct detection of tuberculosis infection in blood serum using three optical label-free approaches. Sensors and Actuators B-Chemical. 2008 Feb;129(2):934-40. (Noncommercial)
88. Narayana Y, Joshi B, Katoch VA, Mishra KC, Balaji KN. Differential B-cell responses are induced by Mycobactelium tuberculosis PE antigens RV1169c, RV0978c, and RV1818c. Clinical and Vaccine Immunology. 2007 Oct;14(10):1334-41. (Noncommercial)

Annexes
Page | 62
89. Omrani M, Ansari MH, Agaverdizadae D. PCR and Elisa methods (IgG and IgM): their comparison with conventional techniques for diagnosis of Mycobacterium tuberculosis. Pak J Biol Sci. 2009 Feb 15;12(4):373-7. (Insufficient data)
90. Ongut G, Ogunc D, Gunseren F, et al. Evaluation of the ICT tuberculosis test for the routine diagnosis of tuberculosis. BMC Infectious Diseases. 2006;6. (Duplicate)
91. Platonova IL, Sakheloshvili MI. [Diagnostic efficiency of the rapid "SEROCHEK MBT" test for the determination of antibodies to mycobacterium tuberculosis]. Klin Lab Diagn. 2008 Apr(4):10-2. (Duplicate)
92. Poddubnaia LV, Romanov VV. [Implication of tuberculosis antibodies in the determination of tuberculous infection]. Probl Tuberk Bolezn Legk. 2006(3):37-40. (Noncommercial)
93. Quan C, Lu CZ, Qiao J, Xiao BG, Li X. Comparative evaluation of early diagnosis of tuberculous meningitis by different assays. J Clin Microbiol. 2006 Sep;44(9):3160-6. (Noncommercial)
94. Raja A, Devi KRU, Ramalingam B, Brennan PJ. Improved diagnosis of pulmonary tuberculosis by detection of free and immune complex-bound anti-30kDa antibodies. Diagnostic Microbiology and Infectious Disease. 2004 Dec;50(4):253-9. (Noncommercial)
95. Raja A, Ranganathan UD, Bethunaickan R. Improved diagnosis of pulmonary tuberculosis by detection of antibodies against multiple Mycobacterium tuberculosis antigens. Diagn Microbiol Infect Dis. 2008 Apr;60(4):361-8. (Noncommercial)
96. Rajan AN, Kashyap RS, Purohit HJ, Taori GM, Daginawala HF. Serodiagnosis of tuberculosis based on the analysis of the 65 kD heat shock protein of Mycobacterium tuberculosis. Int J Tuberc Lung Dis. 2007 Jul;11(7):792-7. (Antigen detection)
97. Rajavelu P, Madhumathi J, Das SD. Humoral immune responses of normals and tuberculosis patients to multiple sonicate antigens prepared from the most prevalent strains of Mycobacterium tuberculosis harbouring single copy of IS6110 from South India. Current Science. 2006 Oct;91(7):918-22. (Noncommercial)
98. Rao L, Padmavathy L. Utility of MycoDot test in the diagnosis of cutaneous tuberculosis [2]. Indian Journal of Dermatology, Venereology and Leprology. 2003;69(6):428-9. (Insufficient data)
99. Rao PV, Murthy MK, Basirudeen S, Sharma P, Swaminathan S, Raja A. Improved diagnosis of tuberculosis in HIV-positive patients using RD1-encoded antigen CFP-10. Int J Infect Dis. 2009 Sep;13(5):613-22. (Noncommercial)
100. Raqib R, Mondal D, Karim MA, Chowdhury F, Ahmed S, Luby S, et al. Detection of antibodies secreted from circulating Mycobacterium tuberculosis-specific plasma cells in the diagnosis of pediatric tuberculosis. Clin Vaccine Immunol. 2009 Apr;16(4):521-7. (Noncommercial)
101. Reither K, Saathoff E, Jung J, Minja LT, Machibya H, Maboko L, et al. Evaluation of Diagnos TB AG, a flow-through immunoassay for rapid detection of pulmonary tuberculosis. International Journal of Tuberculosis and Lung Disease. 2010 Feb;14(2):238-40. (Antigen detection)

Annexes
Page | 63
102. Restrepo BI, Pino PA, Volcy M, Franco AF, Kanaujia GV, Robledo J. Interpretation of mycobacterial antibodies in the cerebrospinal fluid of adults with tuberculous meningitis. Trop Med Int Health. 2008 May;13(5):653-8. (Noncommercial)
103. Rosenkrands I, Aagaard C, Weldingh K, Brock I, Dziegiel MH, Singh M, et al. Identification of Rv0222 from RD4 as a novel serodiagnostic target for tuberculosis. Tuberculosis (Edinb). 2008 Jul;88(4):335-43. (Noncommercial)
104. Sartain MJ, Slayden RA, Singh KK, Laal S, Belisle JT. Disease state differentiation and identification of tuberculosis biomarkers via native antigen array profiling. Mol Cell Proteomics. 2006 Nov;5(11):2102-13. (Noncommercial)
105. Savolainen L, Pusa L, Kim HJ, Sillanpaa H, Seppala I, Tuuminen T. Pilot study of diagnostic potential of the Mycobacterium tuberculosis recombinant HBHA protein in a vaccinated population in Finland. PLoS One. 2008;3(9):e3272. (Noncommercial)
106. Senol G, Ecevit C, Ozturk A. Humoral immune response against 38- and 16-kDa mycobacterial antigens in childhood tuberculosis. Pediatr Pulmonol. 2009 Sep;44(9):839-44. (Reference standard not satisfied)
107. Shah M, Variava E, Holmes CB, Coppin A, Golub JE, McCallum J, et al. Diagnostic accuracy of a urine lipoarabinomannan test for tuberculosis in hospitalized patients in a High HIV prevalence setting. J Acquir Immune Defic Syndr. 2009 Oct 1;52(2):145-51. (Antigen detection)
108. Shamsuzzaman A K, Akhter S, Shamsuzzaman S M, Siddique A. Comparison between ELISA and ICT- MycoDot in adult pulmonary tuberculosis. Mymensingh medical journal : MMJ. 2006;15(1):33-9. (Reference standard not satisfied)
109. Shen G, Behera D, Bhalla M, Nadas A, Laal S. Peptide-based antibody detection for tuberculosis diagnosis. Clin Vaccine Immunol. 2009 Jan;16(1):49-54. (Noncommercial)
110. Shende N, Gupt S, Upadhye V, Kumar S, Harinath BC. Detection of in vitro and in vivo released antigens of diagnostic interest in Mycobacterium tuberculosis by immunoblotting. Indian J Exp Biol. 2008 Jan;46(1):18-21. (Antigen detection)
111. Shende N, Gupta S, Bhatia AS, Kumar S, Harinath BC. Detection of free and immune-complexed serine protease and its antibody in TB patients with and without HIV co-infection. International Journal of Tuberculosis and Lung Disease. 2005 Aug;9(8):915-9. (Noncommercial)
112. Shende N, Gupta S, Upadhye V, Kumar S, Harinath BC. Isolation and analysis of circulating tuberculous antigens in Mycobacterium tuberculosis. Indian J Tuberc. 2007 Jul;54(3):125-9. (Antigen detection)
113. Shende N, Upadhye V, Kumar S, Gangane N, Harinath BC. Study of M. tuberculosis ES-31 and ES-20 antigen levels in different pathogenic grades of lymph node tuberculosis. Int J Tuberc Lung Dis. 2007 Feb;11(2):222-6. (Antigen detection)
114. Shende N, Upadhye V, Kumar S, Harinath BC. A low molecular weight ES-20 protein released in vivo and in vitro with diagnostic potential in lymph node tuberculosis. Indian J Med Microbiol. 2008 Jan-Mar;26(1):29-33. (Noncommercial)

Annexes
Page | 64
115. Shi KY, Hu ZY. [The application of enzyme-linked immunosorbent spot in the diagnosis of tuberculosis]. Zhonghua Jie He He Hu Xi Za Zhi. 2006 Jun;29(6):414-6. (Latent TB infection)
116. Shin AR, Lee KS, Lee JS, Kim SY, Song CH, Jung SB, et al. Mycobacterium tuberculosis HBHA protein reacts strongly with the serum immunoglobulin M of tuberculosis patients. Clin Vaccine Immunol. 2006 Aug;13(8):869-75. (Noncommercial)
117. Shin AR, Shin SJ, Lee KS, Eom SH, Lee SS, Lee BS, et al. Improved sensitivity of diagnosis of tuberculosis in patients in Korea via a cocktail enzyme-linked immunosorbent assay containing the abundantly expressed antigens of the K strain of Mycobacterium tuberculosis. Clin Vaccine Immunol. 2008 Dec;15(12):1788-95. (Noncommercial)
118. Shin SJ, Kim SY, Shin AR, Kim HJ, Cho SN, Park JK. Identification of Rv2041c, a novel immunogenic antigen from Mycobacterium tuberculosis with serodiagnostic potential. Scand J Immunol. 2009 Nov;70(5):457-64. (Noncommercial)
119. Silva VM, Sardella IG, Luiz RR, Cunha AJ, Cavalcanti AH, Mahavir S, et al. Immunoreactivity of five antigens of Mycobacterium tuberculosis in patients attending a public health care facility in an area with high endemicity for TB. Microbiol Immunol. 2008 Nov;52(11):544-50. (Noncommercial)
120. Simonney N, Chavanet P, Perronne C, Leportier M, Revol F, Herrmann JL, et al. B-cell immune responses in HIV positive and HIV negative patients with tuberculosis evaluated with an ELISA using a glycolipid antigen. Tuberculosis (Edinb). 2007 Mar;87(2):109-22. (Noncommercial)
121. Singh KK, Dong Y, Belisle JT, Harder J, Arora VK, Laal S. Antigens of Mycobacterium tuberculosis recognized by antibodies during incipient, subclinical tuberculosis. Clinical and Diagnostic Laboratory Immunology. 2005 Feb;12(2):354-8. (Noncommercial)
122. Singh KK, Sharma N, Vargas D, Liu Z, Belisle JT, Potharaju V, et al. Peptides of a novel Mycobacterium tuberculosis-specific cell wall protein for immunodiagnosis of tuberculosis. J Infect Dis. 2009 Aug 15;200(4):571-81. (Noncommercial)
123. Song HY, Kim YH, Kim CH, Min YK, Kim DJ, Ko KK. [The purification and immunogenicity of TB-14 recombinant Protein of Mycobacterium tuberculosis]. Tuberculosis and Respiratory Diseases. 2006;61(3):239-47. (Noncommercial)
124. Sumi S, Mathai A, Radhakrishnan VV. Dot-immunobinding assay. Methods Mol Biol. 2009;536:89-93. (Insufficient data)
125. Talat N, Shahid F, Dawood G, Hussain R. Dynamic changes in biomarker profiles associated with clinical and subclinical tuberculosis in a high transmission setting: A four-year follow-up study. Scandinavian Journal of Immunology. 2009;69(6):537-46. (Noncommercial)
126. Tat'kov SI, Nosareva ON, Boldyrev AN, Smirnova O, Tumanov Iu V, Lebedev LR, et al. [Use of recombinant species-specific proteins M. tuberculosis for the serological diagnosis of tuberculosis]. Klin Lab Diagn. 2006 Dec(12):23-4, 33-4. (Noncommercial)
127. Tavares RC, Salgado J, Moreira VB, Ferreira MA, Mello FC, Leung JA, et al. Cell proliferation and interferon-gamma response to recombinant MBP-3, NarL, MT-10.3, and 16 kDa Mycobacterium

Annexes
Page | 65
tuberculosis antigens in Brazilian tuberculosis patients. Mem Inst Oswaldo Cruz. 2006 Dec;101(8):857-61. (Noncommercial)
128. Thanyani ST, Roberts V, Siko DG, Vrey P, Verschoor JA. A novel application of affinity biosensor technology to detect antibodies to mycolic acid in tuberculosis patients. J Immunol Methods. 2008 Mar 20;332(1-2):61-72. (Noncommercial)
129. Tiwari RP, Tiwari D, Garg SK, Chandra R, Bisen PS. Glycolipids of Mycobacterium tuberculosis strain H37Rv are potential serological markers for diagnosis of active tuberculosis. Clinical and Diagnostic Laboratory Immunology. 2005 Mar;12(3):465-73. (Noncommercial)
130. Tong M, Jacobi CE, van de Rijke FM, Kuijper S, van de Werken S, Lowary TL, et al. A multiplexed and miniaturized serological tuberculosis assay identifies antigens that discriminate maximally between TB and non-TB sera. Journal of Immunological Methods. 2005 Jun;301(1-2):154-63. (Noncommercial)
131. Trajman A, Kaisermann C, Luiz RR, Sperhacke RD, Rossetti ML, Feres Saad MH, et al. Pleural fluid ADA, IgA-ELISA and PCR sensitivities for the diagnosis of pleural tuberculosis. Scand J Clin Lab Invest. 2007;67(8):877-84. (Noncommercial)
132. Tripathi DG, Sriram N, Naik VK, Smita P, Seema A, Shakila G, et al. Efficacy of immunochromatographic techniques for the serodiagnosis of tuberculosis. Indian J Med Microbiol. 2004 Apr-Jun;22(2):131-2. (Insufficient data)
133. Umadevi KR, Ramalingam B, Raja A. Qualitative and quantitative analysis of antibody response in childhood tuberculosis against antigens of mycobacterium tuberculosis. Indian J Med Microbiol. 2002 Jul-Sep;20(3):145-9. (Noncommercial)
134. Upadhye V, Saha-Roy S, Shende N, Kumar S, Harinath BC. Isolation of Mycobacterium tuberculosis protein antigens ES-3 1, ES-43 and EST-6 of diagnostic interest from tubercle bacilli by affinity chromatography. Indian J Exp Biol. 2007 Jul;45(7):599-602. (Antigen detection)
135. Voronkova QV, Novitsky VV, Urazova OI, Strelis AK, Khasanova RR, Serebryakova VA, et al. Characteristic of humoral immune response in patients with pulmonary tuberculosis before and during antituberculous therapy. Immunologiya. 2008 Sep-Oct;29(5):281-4. (Noncommercial)
136. Wanchu A, Dong Y, Sethi S, Myneedu VP, Nadas A, Liu Z, et al. Biomarkers for clinical and incipient tuberculosis: performance in a TB-endemic country. PLoS One. 2008;3(4):e2071. (Noncommercial)
137. Wang BL, Xu Y, Li ZM, Xu YM, Weng XH, Wang HH. Antibody response to four secretory proteins from Mycobacterium tuberculosis and their complex antigen in TB patients. International Journal of Tuberculosis and Lung Disease. 2005;9(12):1327-34. (Noncommercial)
138. Wang EL, Liu WT, Li T. [The serodiagnostic value of antigens secreted from Mycobacterium tuberculosis]. Zhonghua Jie He He Hu Xi Za Zhi. 2006 Jul;29(7):466-9. (Noncommercial)
139. Wang JY, Lee LN, Lai HC, Hsu HL, Jan IS, Yu CJ, et al. Performance assessment of the Capilia TB assay and the BD ProbeTec ET system for rapid culture confirmation of Mycobacterium tuberculosis. Diagn Microbiol Infect Dis. 2007 Dec;59(4):395-9. (Antigen detection)

Annexes
Page | 66
140. Weldingh K, Rosenkrands I, Okkels LM, Doherty TM, Andersen P. Assessing the serodiagnostic potential of 35 Mycobacterium tuberculosis proteins and identification of four novel serological antigens. Journal of Clinical Microbiology. 2005 Jan;43(1):57-65. (Noncommercial)
141. Wu X, Yang Y, Zhang J, Li B, Liang Y, Zhang C, et al. Humoral immune responses against M. tuberculosis 38-kDa, MTB48 and CFP-10/ESAT-6 antigens in tuberculosis. Clin Vaccine Immunol. 2010 Jan 6. (Noncommercial)
142. Xia JL, Zhu Y, Den JJ, Wan CM. The body fluid purified protein derivative antibody tests: Diagnosis value in pediatric tuberculosis. Chinese Journal of Evidence-Based Medicine. 2006;6(7):537-9. (Relevance)
143. Yanai M, Uehara Y, Takeuchi M, Nagura Y, Hoshino T, Hayashi K, et al. Evaluation of serological diagnosis tests for tuberculosis in hemodialysis patients. Ther Apher Dial. 2006 Jun;10(3):278-81. (Latent TB infection)
144. Zhang G, Zhang L, Zhang M, Pan L, Wang F, Huang J, et al. Screening and assessing 11 Mycobacterium tuberculosis proteins as potential serodiagnostical markers for discriminating TB patients from BCG vaccines. Genomics Proteomics Bioinformatics. 2009 Sep;7(3):107-15. (Noncommercial)
145. Zhang H, Wang J, Lei J, Zhang M, Yang Y, Chen Y, et al. PPE protein (Rv3425) from DNA segment RD11 of Mycobacterium tuberculosis: a potential B-cell antigen used for serological diagnosis to distinguish vaccinated controls from tuberculosis patients. Clin Microbiol Infect. 2007 Feb;13(2):139-45. (Noncommercial)
146. Zhang M, Yang Y, Xu Y, Qie Y, Wang J, Zhu B, et al. Trehalose-6-phosphate Phosphatase from Mycobacterium tuberculosis induces humoral and cellular immune responses. FEMS Immunology and Medical Microbiology. 2007 Feb;49(1):68-74. (Noncommercial)
147. Zhang SL, Zhao JW, Sun ZQ, Yang EZ, Yan JH, Zhao Q, et al. Development and evaluation of a novel multiple-antigen ELISA for serodiagnosis of tuberculosis. Tuberculosis (Edinb). 2009 Jul;89(4):278-84. (Noncommercial)


![Ultrasound versus liver function tests for diagnosis of ... · [Diagnostic Test Accuracy Review] Ultrasound versus liver function tests for diagnosis of common bile duct stones Kurinchi](https://static.fdocuments.us/doc/165x107/601bcce3144189465e124f14/ultrasound-versus-liver-function-tests-for-diagnosis-of-diagnostic-test-accuracy.jpg)