
Combinatorial Metabolism Notably Affects Human...
42
DMD #51391 Combinatorial Metabolism Notably Affects Human Systemic Exposure to Ginsenosides from Orally Administered Extract of Panax notoginseng Roots (Sanqi) Zheyi Hu, Junling Yang, Chen Cheng, Yuhong Huang, Feifei Du, Fengqing Wang, Wei Niu, Fang Xu, Rongrong Jiang, Xiumei Gao, Chuan Li Shanghai Institute of Materia Medica, Chinese Academy of Sciences, Shanghai, China (Z.H., J.Y., C.C., F.D., F.W., W.N., F.X., R.J., C.L.); Tianjin University of Traditional Chinese Medicine, Tianjin, China (Y.H., X.G.); Institute of Chinese Materia Medica, China Academy of Chinese Medical Sciences, Beijing, China (C.L.). DMD Fast Forward. Published on May 6, 2013 as doi:10.1124/dmd.113.051391 Copyright 2013 by the American Society for Pharmacology and Experimental Therapeutics. This article has not been copyedited and formatted. The final version may differ from this version. DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391 at ASPET Journals on July 29, 2018 dmd.aspetjournals.org Downloaded from
Transcript of Combinatorial Metabolism Notably Affects Human...
DMD #51391
1
Combinatorial Metabolism Notably Affects
Human Systemic Exposure to Ginsenosides
from Orally Administered Extract of Panax
notoginseng Roots (Sanqi)
Zheyi Hu, Junling Yang, Chen Cheng, Yuhong Huang,
Feifei Du, Fengqing Wang, Wei Niu, Fang Xu, Rongrong
Jiang, Xiumei Gao, Chuan Li
Shanghai Institute of Materia Medica, Chinese Academy of Sciences,
Shanghai, China (Z.H., J.Y., C.C., F.D., F.W., W.N., F.X., R.J., C.L.); Tianjin
University of Traditional Chinese Medicine, Tianjin, China (Y.H., X.G.);
Institute of Chinese Materia Medica, China Academy of Chinese Medical
Sciences, Beijing, China (C.L.).
DMD Fast Forward. Published on May 6, 2013 as doi:10.1124/dmd.113.051391
Copyright 2013 by the American Society for Pharmacology and Experimental Therapeutics.
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
2
Running Title: PHARMACOKINETICS AND METABOLISM OF GINSENOSIDES IN
HUMANS
Address correspondence to: Dr. Chuan Li, Laboratory for DMPK Research
of Herbal Medicines, Shanghai Institute of Materia Medica, Chinese Academy
of Sciences, 501 Haike Road, Zhangjiang Hi-Tech Park, Shanghai 201203,
China. E-mail: [email protected]
Number of Text Pages: 22
Number of Figures: 9
Number of References: 24
Number of Words in Abstract Section: 235
Number of Words in Introduction Section: 714
Number of Words in Discussion Section: 1499
ABBREVIATIONS: AUC0-t, area under concentration-time curve to the last measured
time point; CLR, renal clearance; CLtot,P, total plasma clearance; Cmax, maximum plasma
concentration; Cum.Ae, cumulative amount excreted; CYP, cytochrome P450; HLM,
human liver microsomes; MRT, mean residence time; ppd-type, 20(S)-protopanaxadiol
type; ppt-type, 20(S)-protopanaxatriol type; PK, pharmacokinetic; Tmax, time taken to
achieve the maximum concentration
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
3
ABSTRACT
Ginsenosides are medicinal ingredients of the cardiovascular herb Panax notoginseng
roots (Sanqi). Here, we implemented a human study (ChiCTR-ONC-09000603;
www.chictr.org) to characterize pharmacokinetics and metabolism of ginsenosides from
an orally ingested Sanqi extract (a 1:10 water extract of Sanqi) and the human plasma
and urine samples were analyzed by liquid chromatography-mass spectrometry. Plasma
and urinary compounds derived from ginsenosides included (1) intestinally absorbed
ginsenosides Ra3, Rb1, Rd, F2, Rg1, and notoginsenoside R1 and (2) the deglycosylated
products compound-K, 20(S)-protopanaxadiol, 20(S)-protopanaxatriol, and their oxidized
metabolites. The systemic exposure levels of the first group compounds increased as
the Sanqi extract dose increased, but those of the second group compounds were
dose-independent. The oxidized metabolites of 20(S)-protopanaxadiol and
20(S)-protopanaxatriol represented the major circulating forms of ginsenosides in the
bloodstream, despite their large interindividual differences in exposure level. The
metabolites were formed via combinatorial metabolism that consisted of a rate-limiting
step of ginsenoside deglycosylation by the colonic microflora and a subsequent step of
sapogenin oxidation by the enterohepatic cytochrome P450 enzymes. Significant
accumulation of plasma ginsenosides and the metabolites occurred in the human
subjects receiving three-week subchronic treatment with the Sanqi extract. Plasma
20(S)-protopanaxadiol and 20(S)-protopanaxatriol could be used as pharmacokinetic
markers to reflect the subject’s microbial activities, as well as the timely-changes and
interindividual differences in plasma levels of their respective oxidized metabolites. The
information gained from the current study is relevant to pharmacology and therapeutics
of Sanqi.
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
4
Introduction
In China, the tradition of herbal medicine has prospered over millennia and is
still accepted by the physicians, the patients, and the regulatory authority. However,
the scientific standards for accepting the value of an herbal product as a medicine
fall below the existing requirements for establishing the value of synthetic drugs.
China has announced an ambitious attempt to bring the practice of traditional
medicine into line with modern standards (Qiu, 2007).
Phytochemists traditionally work in concert with ethnopharmacologists in
herbal medicine research, where whole herb extracts, as well as the individual
compounds isolated and purified from the herbs, are applied to in vivo and/or in
vitro pharmacological assessments. However, the studies often fail to address which
chemical ingredients present are the medicinal principles responsible for the
pharmacological effects of the investigative herbal medicine. The most abundant
constituents present in an herbal medicine do not necessarily produce the highest in
vivo concentrations (such as the plasma concentrations, the tissue concentrations, or
the like) after dosing, while in vivo measured herbal metabolites are usually absent
in the dosed medicine (Lu et al., 2008; Liu et al., 2009; Li et al., 2012; Yan et al.,
2012; Li, 2012). In other words, there can be significant differences in nature and
relative levels between the chemical ingredients present in an herbal medicine and
the circulating botanical compounds after dosing. The accurate and complete
information of pharmacokinetics and metabolism is vital to the pharmacological
research for identification of the medicinal principles. Accordingly, pharmacokinetic
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
5
(PK) scientists are needed to participate in the herbal medicine research by working
with ethnopharmacologists and phytochemists in a manner similar to that for drug
discovery. Different from the early practice that was based only on pharmacological
assessment of a range of chemicals, the current drug discovery is normally achieved
by combining medicinal chemistry and pharmacology together with
pharmacokinetics, which has resulted in improved candidate selection for preclinical
and clinical development (Pritchard et al., 2003). PK and metabolism study of an
herbal medicine tells the ethnopharmacologists which herb-derived compounds are
worth further evaluation.
Sanqi (the dried root of Panax notoginseng, family Araliaceae) has been
commonly used in the Chinese traditional medicine to eliminate blood stasis, to
arrest bleeding, to cause subsidence of swelling, and to alleviate pain (Chinese
Pharmacopoeia Commission, 2010). The medicinal herb is usually administered
orally in such forms as powders, aqueous extracts, and teas, in daily dose ranging
from 2 g to 30 g of root but averaging 3–9 g. In addition, injections prepared from
Sanqi extract have also been approved for clinical use in China. The triterpene
saponins ginsenosides are believed to be the pharmacologically active ingredients of
Sanqi and can be classified according to their structures as 20(S)-protopanaxadiol
type (ppd-type) and 20(S)-protopanaxatriol type (ppt-type) (Christensen, 2009; Lv et
al., 2009). The major saponins present in Sanqi include the ppd-type ginsenosides
Ra3, Rb1, and Rd and the ppt-type ginsenosides Re, Rg1, and notoginsenoside R1.
Recently, we investigated intestinal absorption and disposition of ginsenosides in
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
6
rats receiving an orally (p.o.) administered Sanqi extract and found that poor
membrane permeability, rapid biliary excretion, and colonic microflora-induced
deglycosylation were the key factors affecting the rat systemic exposure to
ginsenosides (Liu et al., 2009). The major ginsenosides measured in rat plasma were
long-circulating ppd-type ginsenosides Ra3, Rb1, and Rd, which can be used as
pharmacokinetic markers (PK markers) to substantiate rat systemic exposure to the
Sanqi extract. Meanwhile, ppt-type ginsenosides Re, Rg1, and notoginsenoside R1, as
well as the deglycosylated products of both the types, were subject to rapid biliary
excretion that limited their systemic exposure levels. Interspecies differences in
biliary excretion (Mahmood and Sahajwalla, 2002; Lai, 2009) and colonic
microflora-induced metabolism (Nicholson et al., 2005; Sousa et al., 2008)
complicate the extrapolation of human absorption and disposition of ginsenosides
from the animal data. Accordingly, we implemented a human study to characterize
pharmacokinetics and metabolism of ginsenosides from an orally ingested Sanqi
extract. One of our important findings is that several metabolites derived from
ginsenosides were measured as major circulating compounds after dosing. These
metabolites, absent in the administered herbal extract, were formed via
combinatorial metabolism that consisted of a rate-limiting step of ginsenoside
deglycosylation induced by the colonic microflora and a subsequent step of
sapogenin oxidation mediated by the enterohepatic cytochrome P450 enzymes (CYP
enzymes).
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
7
Materials and Methods
A detailed description of materials and experimental procedures is provided in
the Supplemental Materials and Methods.
Materials. Sanqi-extract, for p.o. administration to human subjects, was a 1:10
water extract, i.e., 2 kg of dried roots of Panax notoginseng (Sanqi) was used to
make 20 l of the final extract. The prepared Sanqi-extract contained ginsenosides
Rg1 (2680 μM), Rb1 (1377 μM), Rd (366 μM), Re (254 μM), Rh1 (103 μM), Ra3 (76
μM), Rg2 (60 μM), F1 (48 μM), F2 (18 μM), Rg3 (17 μM), Rb2 (14 μM), Rf (13 μM),
Rc (3 μM), and Rh2 (1 μM), as well as notoginsenosides R1 (360 μM), R3/R6 (69
μM), and 20-gluco-ginsenoside Rf (33 μM). Only one batch of Sanqi-extract was
prepared and used for the whole study. The content levels of ginsenosides in
Sanqi-extract were measured immediately after preparation and after storage at 4ºC
for 1 and 3 months. Chemical stability was defined as the retention of ≥85% of the
initial levels. The herb extract was used after shaking well.
Purified ginsenosides, 20(S)-protopanaxadiol, and 20(S)-protopanaxatriol were
obtained from the National Institutes for Food and Drug Control (Beijing, China) or
other commercial sources, the purity of which exceeded 98%. Pooled human liver
microsomes (HLM) of Chinese origin were obtained from the Research Institute for
Liver Diseases (Shanghai, China). Single cDNA-expressed human cytochrome P450
(CYP) enzymes were obtained from BD Gentest (Woburn, MA).
Human Study. The protocol for human study was approved by the Ethics
Committee of Clinical Investigation at the Second Affiliated Hospital of Tianjin
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
8
University of Traditional Chinese Medicine (Tianjin, China). The study was
registered on Chinese Clinical Trials Registry (www.chictr.org) with a registration
number of ChiCTR-ONC-09000603. The informed consent was obtained from each
of twelve male and twelve female healthy volunteers (22–26 yr).
A two-period, open-label, single center study was performed at the National
Clinical Research Center of the hospital (Tianjin, China; Fig. 1). In period 1, all the
subjects were randomly assigned to one of three dosage groups, with four male and
four female subjects per group. Each subject was asked to fast overnight before
receiving a single p.o. dose of Sanqi-extract (90, 180, or 270 ml/subject) in the next
morning. The low dose level was derived from the dose level recommended by the
Pharmacopoeia of the People’s Republic of China. The intermediate and high dose
levels were also used clinically. Serial blood samples (~1 ml collected in heparinized
tubes) were taken from an antecubital vein catheter at 0, 0.5, 1.5, 3, 4.5, 8, 12, 15, 24,
30, 38, 48, and 56 h after dosing. The blood samples were then centrifuged at 3000×
g for 5 min, and the resulting plasma fractions were frozen at −70°C until analysis.
Meanwhile, serial urine samples were also collected predose and at 0–3, 3–6, 6–10,
10–14, 14–24, 24–32, 32–40, 40–48, and 48–72 h postdose, which were weighed
prior to storage at −70°C without use of any preservative. In period 2 (after three-day
wash-out period following the first acute p.o. treatment with Sanqi-extract), the four
male subjects of the low-dose group continued to receive a subchronic p.o. treatment
with Sanqi-extract at 90 ml/subject/day for three weeks. On days 11, 18, and 24 of
period 2, the blood and urine samples were collected according to the preceding time
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
9
schedules, except for the sampling only performed 0–24 h after the dosing on days
11 and 18. The hepatic and renal function of subjects was monitored before period 1
and 72 h after a single dose of Sanqi-extract, as well as on days 4, 12, 15, 19, 20, 21,
22, 23, and 25 (before the daily dose of Sanqi-extract) of period 2. Serum alanine
aminotransferase (ALT), aspartate aminotransferase (AST), total protein (TP),
albumin/globulin (A/G) ratio, total bilirubin (TBiL), and direct bilirubin (DBiL)
were monitored as liver function markers for the human subjects, while serum
creatinine (CRE) and blood urea nitrogen (BUN) were also assessed to monitor their
renal function. The reference ranges, indicating normal liver or kidney function, of
ALT, AST, TP, A/G ratio, TBiL, DBiL, CRE, and BUN were 0–40 U/l, 0–40 U/l,
64–87 g/l, 1–2.5, 0–17.1 μM, 0–8.0 μM, 22–106 μM, and 1.7–8.3 mM, respectively.
In Vitro Metabolism Studies. Pure 20(S)-protopanaxadiol,
20(S)-protopanaxatriol, and compound-K at 2 μM was incubated with HLM in
presence of the cofactor(s) NADPH, UDPGA, or the both to assess metabolic stability
and to support metabolite characterization. A variety of cDNA-expressed human CYP
enzymes (CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6,
CYP2E1, CYP3A4, and CYP3A5) were used for the enzyme identification. To
determine the enzyme kinetics, 20(S)-protopanaxadiol (1.56–200 μM) or
20(S)-protopanaxatriol (0.08–200 μM) was incubated with NADPH-fortified HLM
under linear metabolite formation conditions, which were performed in duplicate in
96-well plates.
Liquid Chromatography-Mass Spectrometry Analyses. An AB Sciex API
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
10
4000 Q Trap mass spectrometer (Toronto, Canada) interfaced via a Turbo V ion
source with a Waters Acquity UPLC separation module (Milford, MA, USA) was
used for metabolite profiling and quantification for study purposes. The human
plasma and urine samples (50 μl) were precipitated with 150 μl of methanol before
measurement. Meanwhile, in vitro metabolism study samples (100 μl) were treated
with an equal volume of methanol to stop the reaction before analysis. Validation of
the quantification assays with the reference standards available were implemented
according to the US Food and Drug Administration guide on bioanalytical method
validation (http://www.fda.gov/cder/guidance/index.htm) to demonstrate that their
performance characteristics were reliable for the intended use.
Data Analysis. PK parameters were determined by non-compartmental method
using the Kinetica 5.0 (Thermo Fisher Scientific; Philadelphia, PA), which were
shown as means ± standard deviation. Dose proportionality assessment was conducted
by the regression of log-transformed data (the Power Model) with the criterion that
was calculated according to the method by Smith et al. (2000). Michaelis constant (Km)
and maximum velocity (Vmax) values were determined by nonlinear regression
analysis using the Michaelis-Menten equation (rate of metabolite formation as a
function of substrate concentration) using GraFit software (version 5; Erithacus
Software Ltd., Surrey, UK). The ratio of Vmax and Km was used to calculate in vitro
intrinsic clearance (CLint). The Shapiro-Wilk test of normality was used to check the
distribution shape of systemic exposure levels of ginsenoside-derived compounds in
AUC0-t. The Kendall’s tau-b coefficients were calculated using PASW statistics 18
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
11
software (SPSS Inc., Chicago, IL) to estimate whether the systemic exposure levels of
a certain ginsenoside-derived compound were positively or negatively correlated to
those of another ginsenoside-derived compound. Correlation was statistically
significant at P < 0.01 level (two-tailed).
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
12
Results
Safety of Sanqi-extract. No serious adverse event was observed during the
human study. After a p.o. dose of Sanqi-extract at 90, 180, or 270 ml/subject, none
of liver or kidney function indicators exceeded the upper normal levels. During the
subsequent multiple dose treatment, the four male subjects (m1–m4; receiving
Sanqi-extract at 90 ml/subject/day) had the hepatic or renal function indicators
within the normal ranges during the study period, except for some transient elevation
of alanine aminotransferase (ALT) for subjects m2–m4. Subject m3 had elevated
ALT (54–79 U/l) on days 15–22. This subject withdrew from the study after day 18
to let his elevated ALT return to the normal level (<40 U/l).
Appearance of Plasma and Urine Ginsenosides and Metabolites after p.o.
Administration of Sanqi-extract. Ginsenosides and their deglycosylated products
occurred in human plasma and urine after a p.o. dose of Sanqi-extract (270
ml/subject), which were compared with the profiles of the control plasma and urine
samples before dosing. As shown in Fig. 2B, Ppd-type ginsenoside Rb1 was the most
abundant plasma Sanqi saponin absorbed, while other saponins measured in plasma
were ppd-type ginsenosides Ra3, Rd, F2, Rg3, and Rh2, as well as ppt-type
ginsenosides Re, Rg1, F1, Rh1, and notoginsenoside R1. These plasma ginsenosides
were also excreted into urine (Fig. 2C), except ginsenosides Rg3 and Rh2.
Meanwhile, 20-gluco-ginsenoside Rf and notoginsenoside R3/6 were measured in
urine but not in plasma. Although ppt-type ginsenoside Rg1 had a higher content
level in the administered Sanqi-extract than ginsenoside Rb1, its plasma abundance
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
13
was significantly lower than that of the ppd-type ginsenoside (Fig. 2B). However,
urinary ginsenoside Rg1 was the most abundant of all the ginsenosides excreted into
urine (Fig. 2C). Notably, the deglycosylated products compound-K,
20(S)-protopanaxadiol, and 20(S)-protopanaxatriol, absent in the ingested
Sanqi-extract (Fig. 2A), also occurred substantially in plasma with
20(S)-protopanaxatriol being ~3-times more abundant than plasma ginsenoside Rb1
(Fig. 2B).
Although 20(S)-protopanaxadiol and 20(S)-protopanaxatriol circulated
significantly in the bloodstream, they are not measured in the urine samples. To
understand the elimination of the deglycosylated products, their metabolism was
further assessed. A total of 29 metabolites of the deglycosylated products were
detected in the plasma samples (Fig. 2D). Plasma M8, M11, and M12 had their
abundances 1.2–11 times higher than 20(S)-protopanaxatriol, while the abundances of
plasma M3–M7, M9, M10, and M13–M22 were 7–72% of that of the sapogenin.
Meanwhile, a total of 29 urinary metabolites were measured (Fig. 2E). The plasma
metabolites M17–M22 were absent in urine, while the urinary metabolites M30 and
M31–M35 were not measured in plasma. The most abundant metabolites in urine
were M8 and M6, i.e., 131% and 90% of urinary ginsenoside Rg1, respectively, while
urinary M3, M5, M7, M11–M13, M23–M25, M27, M29, and M35 were only
10%–43%. It is worth mentioning that the preceding plasma and urine metabolites
(M1–M35) were absent in the administered Sanqi-extract. As to the ginsenosides
present in Sanqi-extract, their oxidized or conjugated metabolites were not measured
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
14
in the human samples.
In Vitro Metabolism of 20(S)-Protopanaxadiol, 20(S)-Protopanaxatriol,
and Compound-K. To help characterize the preceding in vivo metabolites
(M1–M35), in vitro metabolism studies were implemented with HLM.
20(S)-Protopanaxadiol or 20(S)-protopanaxatriol was labile when incubating with
NADPH-fortified HLM (in vitro t1/2, 6 and 4 min, respectively; Supplemental Table
1). Furthermore, both the sapogenins were quite stable with UDPGA-fortified HLM
(>120 min). These data suggested that the oxidation of the sapogenins was rapid in
the liver, while the glucuronidation was relatively slow. Compound-K was slowly
metabolized with the human microsomal enzymes (>120 min). According to the in
vitro data (Supplemental Table 1), M16–M22, M34, and M35 were characterized as
the oxidized metabolites of 20(S)-protopanaxadiol, while M3–M15, M23–M29, and
M31–M33 were derived from 20(S)-protopanaxatriol. M1, M2, and M30 were the
metabolites of compound-K. Figure 3 depicts the proposed metabolic pathways of
the deglycosylated products in the humans.
Human CYP3A4 and CYP3A5 were the major enzymes responsible for the
oxidation of 20(S)-protopanaxadiol or 20(S)-protopanaxatriol (Fig. 4). In addition,
CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and
CYP2E1 could also mediate the oxidation of 20(S)-protopanaxadiol. The Michaelis
constants of HLM towards the formation of M20/M21/M22 from
20(S)-protopanaxadiol and those for M8/M10/M11/M12 from 20(S)-protopanaxatriol
were 4.0–6.6 and 0.2–1.1 μM, respectively (Supplemental Table 2).
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
15
Plasma Pharmacokinetics and Urinary Excretion of Ginsenosides and their
Major Metabolites after p.o. Administration of Sanqi-extract. Figure 5 shows
plasma level-time profiles of the major ginsenosides after a p.o. dose of
Sanqi-extract to the human subjects, as well as those of the deglycosylated products
[compound-K, 20(S)-protopanaxadiol, and 20(S)-protopanaxatriol] and the oxidized
metabolites of the sapogenins, while the plasma PK parameters are summarized in
Supplemental Tables 3–5. After dosing at 270 ml/subject, the plasma concentrations
of ppd-type ginsenosides Ra3, Rb1, and Rd increased up to Cmax (3.1, 27.9, and 9.3
nM, respectively) with Tmax of 8–12 h and then slowly decreased with t1/2 of 33–57 h.
Their MRT values were 50–82 h. The Tmax and MRT of ppd-type ginsenoside F2
were 13 h and 22–29 h, respectively. The renal excretion of ginsenosides Ra3, Rb1,
Rd, and F2 was slow with CLR of 0.01–0.04 l/h and their urinary Cum.Ae(0→72h)
accounted for only ~0.01% of the compound doses from the p.o. ingested
Sanqi-extract. The AUC0-56h of ginsenosides Ra3, Rb1, Rd, and F2 increased in
Sanqi-extract dose-related manners (90–270 ml/subject), but the dose proportionality
was inconclusive (Fig. 6). Compound-K exhibited a significantly higher mean
AUC0-56h than ginsenoside Rb1, demonstrating 4749 versus 749 nM·h after dosing at
270 ml/subject, while the former’s interindividual difference in AUC0-56h was
significantly larger than that of the latter. Meanwhile, compound-K had a Tmax of
10–30 h and an MRT of 23–26 h. The average CLR value of compound-K was very
low (0.01 l/h). Significant interindividual difference in plasma occurrence was also
observed with 20(S)-protopanaxadiol. The AUC0-56h value of compound-K or
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
16
20(S)-protopanaxadiol correlated poorly with the dose of Sanqi-extract (Fig. 6). In
addition, compound-K or 20(S)-protopanaxadiol was correlated poorly with
ginsenosides Ra3, Rb1, Rd, and F2 in AUC0-56h for the individual subjects (Fig. 7).
Compound-K was also correlated poorly with 20(S)-protopanaxadiol.
At the Sanqi-extract dose 270 ml/subject, ppt-type ginsenoside Rg1 and
notoginsenoside R1 had Tmax of 6–7 h and Cmax values of 10.2 and 1.4 nM,
respectively. Their MRT values were 7–13 h. The renal excretion of these ppt-type
ginsenosides was rapid with CLR of 5.6 and 4.0 l/h, respectively, while their urinary
Cum.Ae(0-24h) accounted for ~0.06% of the compound doses from Sanqi-extract. The
AUC0-38h values of ginsenoside Rg1 and notoginsenoside R1 increased in Sanqi-extract
dose-related manners, but lack of proportionality was concluded (Fig. 6). Ppt-type
ginsenoside F1 had a Tmax of 14–19 h and a Cmax of 4.3 nM. Its CLR was 0.7 l/h.
Although 20(S)-protopanaxatriol had higher systemic exposure as compared with the
major Sanqi ginsenosides, the interindividual difference was larger. The AUC0-56h of
20(S)-protopanaxatriol was independent of the Sanqi-extract dose (Fig. 6), which was
also not correlated with AUC0-38h of ginsenosides Rg1, F1, or notoginsenoside R1 for
the individual subjects (Fig. 7). There appeared to be correlation between
20(S)-protopanaxatriol and 20(S)-protopanaxadiol in AUC0-56h (P < 0.01).
As shown in Fig. 5, the plasma concentrations of M16, M17, and M19–M22
increased and then decreased concurrently as the concentration of their precursor
20(S)-protopanaxadiol changed with time. In addition, there were significantly
positive correlations in AUC0-56h between 20(S)-protopanaxadiol and these
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
17
metabolites for the individual subjects (P < 0.01; Fig. 7). Meanwhile, the plasma
concentrations of M4–M8 and M10–M15 also changed concomitantly with that of
20(S)-protopanaxatriol and significant correlations existed between the sapogenin and
its oxidized metabolites (P < 0.01). Similar to the situations of their parent sapogenins,
the AUC0-56h value of the preceding oxidized metabolites appeared to be Sanqi-extract
dose-independent (Fig. 6). With respect to the renal excretion, the ppd-derived
metabolites were not or negligibly recovered in the human urine after oral
administration of San qi-extract. In contrast, many of the ppt-derived metabolites (in
the ranking order of M6>M7>M5≈M13>M8) were notably excreted into urine with
CLR of 0.1–1.3 l/h.
Figure 8 depicts AUC0-24h changes of ginsenosides and the metabolites for the
subjects m1, m2, and m4 who received Sanqi-extract for additional 21 days. The
AUC0-24h of ginsenosides Ra3, Rb1, and Rd increased significantly during the
multiple-dose treatment, indicative of 1.9–11.3-fold increases on day 11 as compared
with the data on day 1 and 1.3–10.3-fold increases on day 18. However, the AUC0-24h
values on day 24 tended to decrease for these subjects. The AUC0-24h values of
compound-K and ginsenosides F1 and F2 did not exhibit a clear initial increase and
eventual decrease. Subjects m1 and m2 had notable increases in AUC0-24h values of
ginsenoside Rg1 and notoginsenoside R1 on day 18 (3.5–7.4-fold of the day 1 data)
and decreases on day 24 (22%–55% of the day 18 data). 20(S)-Protopanaxadiol and
20(S)-protopanaxatriol had significantly increased AUC0-24h values on days 11, 18,
and 24 as compared with the data on day1. Notably, the AUC0-24h values of
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
18
ppd-derived M16, M17, and M19–M22 increased and decreased as the AUC0-24h
value of 20(S)-protopanaxadiol changed with time (Fig. 8). Similar situation occurred
with 20(S)-protopanaxatriol and its metabolites M4–M8 and M10–M15 (Fig. 8). In
addition, there were significantly positive correlations in AUC0-24h between
20(S)-protopanaxadiol and its metabolites M16, M17, and M19–M22 and between
20(S)-protopanaxatriol and the metabolites M4–M8 and M10–M15 (P < 0.01; Fig. 9).
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
19
Discussion
Unlike synthetic drugs, herbal medicines are complex chemical mixtures.
Benefits of herb therapy are normally based on a range of activities of compounds
working together. Accordingly, ADME/PK study of an herb medicine involves
investigation of multiple botanical compounds to link the medicine administration and
the medicinal benefits. An earlier systematic ADME/PK study of a Sanqi extract was
performed in rats (Liu et al., 2009), which provided the indispensable guidance for us
to implement strategically this follow-up multi-compound human PK study.
Similar to the situation in rats, the ppd-type ginsenosides Ra3, Rb1, and Rd from
p.o. dosed Sanqi-extract had long elimination half-lives (>30 h) in the human subjects
and significant accumulation in AUC0-24h during the multiple-dose treatment. Their
systemic exposure levels increased in a Sanqi-extract dose-dependent manner (90–270
ml/subject). These plasma ginsenosides were considered to be Sanqi-extract
dose-dependent PK markers to substantiate human systemic exposure to the oral herb
extract. Unlike the situation in rats, the human systemic exposure levels of the
ppt-type ginsenoside Rg1 and notoginsenoside R1 and the ppd-type ginsenoside F2
also increased in Sanqi-extract dose-related manners. Poorer biliary excretion in
humans than in rats (Mahmood and Sahajwalla, 2002; Lai, 2009) likely accounted for
the interspecies differences. Accordingly, plasma ginsenosides Rg1, F2 and
notoginsenoside R1 could also be used as Sanqi-extract dose-dependent PK markers in
humans.
The most important finding of this human study was the substantially measured
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
20
plasma metabolites that resulted from the combinatorial metabolism of ginsenosides
(consisting of the saponin deglycosylation by the colonic microflora and the
subsequent sapogenin oxidation by the enterohepatic CYP enzymes). Deglycosylation
of ginsenosides via action of the colonic microflora has been demonstrated in vitro
and in vivo for years (Hasegawa et al., 1996; Tawab et al., 2003; Yang et al., 2006)
and the human CYP-mediated oxidation of the sapogenins has also been assessed in
vitro recently (Kasai et al., 2000; Hao et al., 2010; Li et al., 2011). Unlike the situation
in humans, these metabolites were poorly detected in rat plasma after p.o. dose of
Sanqi extract (Liu et al., 2009). The human colon is heavily bacterial-colonized as
compared with the rat colon (Sousa et al., 2008), which likely accounts for the
observed metabolism interspecies difference. The amount of variation in the colonic
microflora is considerable between human individuals (Nicholson et al., 2005). In this
study, we observed marked interindividual differences in formation of the
deglycosylated compound-K, 20(S)-protopanaxadiol, and 20(S)-protopanaxatriol.
Notably, the systemic exposure levels of oxidized metabolites of the sapogenins,
regardless of the sex of subject or the Sanqi-extract dose level, were well correlated
with those of the sapogenins, rather than the levels of the ginsenosides absorbed (Fig.
7 and 9). The colonic microflora-mediated deglycosylation appeared to be the
rate-limiting step in the combinatorial metabolism of ginsenosides. As shown in Fig. 5,
although the Tmax values of compound-K, 20(S)-protopanaxadiol, and
20(S)-protopanaxatriol were delayed ~20 h as compared with those of the
ginsenosides, these deglycosylated products and their oxidized metabolites were
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
21
almost identical in Tmax. Even if the gastrointestinal transit time (normally 4–5 h) to
colon is taken into consideration, these data still suggested that the deglycosylations
were significantly slower than the enterohepatic oxidations. In addition, the
deglycosylation activities of the colonic microflora appeared to be induced by the
unabsorbed ginsenosides during the subchronic treatment with Sanqi-extract. Despite
the structural similarity, multiple CYP enzymes mediated the oxidation of
20(S)-protopanaxadiol, whereas only CYP3A4 and CYP3A5 were implicated in the
metabolism of 20(S)-protopanaxatriol. This finding suggests that the
20(S)-protopanaxadiol oxidation is relatively refractory to the effects of
CYP-inhibitors. The oxidized metabolites from the sapogenins were likely cleared via
renal excretion and/or glucuronidation-associated biliary excretion (Supplemental
Figure 1).
Besides the preceding dose-dependent PK markers, we further proposed two
other concepts of dose-independent PK markers for Sanqi-extract. The colonic
microflora mediating the ginsenoside deglycosylation played a key role in the
combinatorial metabolism. The plasma compound-K, 20(S)-protopanaxadiol, and
20(S)-protopanaxatriol could be used as PK markers to reflect the interindividual
differences in deglycosylation activities of the colonic microflora. This proposal is
also supported by in vitro formation of these deglycosylated products from
ginsenosides via action of the human fecal microflora under anaerobic conditions
(Hasegawa et al., 1996). In addition, the plasma concentration of
20(S)-protopanaxadiol and the plasma levels of oxidized metabolites (M16–M22)
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
22
concomitantly increased up to maxima and then decreased with almost the same Tmax
and MRT values. The same situation also occurred with 20(S)-protopanaxatriol and its
oxidized metabolites (M4–M8 and M10–M15). Significant correlations in AUC (Fig.
7 and 9) between 20(S)-protopanaxadiol and the ppd-derived metabolites and those
between 20(S)-protopanaxatriol and the ppt-derived metabolites suggested that the
plasma sapogenins could be used as PK markers to reflect the timely-changes and
interindividual differences in plasma levels of their respective oxidized metabolites. In
pharmacological studies of herbal medicines, the intensity of pharmacological
response was often found to be correlated poorly with the dose. Unlike the absorbed
ginsenosides, the plasma levels of the ppd-derived or ppt-derived metabolites were
dependent on the human individual’s deglycosylation activities of colonic microflora
rather than the Sanqi-extract dose. The information gained and the associated PK
markers identified may be implicated when the dose-response relationship is assessed
for Sanqi in humans.
Poor oral bioavailability of many herbal constituents is often associated with
their low levels of systemic exposure, which impedes translation of many in vitro
pharmacological activities of the compounds to the therapeutic effects of herbal
medicines (Zhang et al., 2012). However, we found that ppd-type ginsenosides Ra3,
Rb1, and Rd from a p.o. ingested Sanqi extract had considerably high plasma levels in
rats despite their <1% oral bioavailability (Liu et al., 2009). These ppd-type
ginsenosides were long-circulating because their elimination kinetics was associated
with high metabolic stability and slow biliary and urinary excretion. In this human
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
23
study, we found that the deglycosylated products compound-K, 20(S)-protopanaxadiol,
20(S)-protopanaxatriol, and their many oxidized metabolites had high plasma levels
and accumulated substantially with repeated doses of Sanqi-extract. Assessing the
pharmacological activities of these herbal compounds with significant exposure levels
after dosing is important for evaluation of oral Sanqi’s therapeutic values.
Accordingly, additional studies are planned to make pharmacological assessments of
the herbal metabolites found in this study.
Considerable hepatotoxicity and nephrotoxicity were observed in rats receiving
multiple p.o. doses of “notoginseng total saponin” (containing ginsenosides Rg1, Rb1,
Rd, Re, and notoginsenoside R1) at 1600 mg/day/kg for thirteen weeks (Ma and Dai,
2011). Our earlier rat Sanqi study indicated that the major ppt-type ginsenosides Rg1,
Re, and notoginsenoside R1, as well as the ppd-type compound-K, were subject to
rapid biliary excretion via an active transport mechanism and had high liver levels
(Liu et al., 2009). In this study, no significant hepatotoxicity and nephrotoxicity were
observed for the human subjects receiving oral Sanqi-extract, except for the subject
m3. Although this subject had obviously increased ALT during the multiple-dose
treatment, his plasma levels of ginsenosides and the metabolites were not high as
compared with the other subjects. According to dose normalization by body surface
area (Reagan-Shaw et al., 2007), the daily doses (800–1600 mg/kg) in the rat study by
Ma and Dai (2011) were about 20–40 times greater than the daily dose for our
subchronic treatment of the human subjects m1–m4 with Sanqi-extract (90
ml/subject). Although the potential effects of ginsenosides and their metabolites on
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
24
the hepatic and renal function need to be confirmed by more studies, it is nonetheless
wise to exercise caution when high dose levels of Sanqi extracts or the associated
pharmaceutical products are administered for a long period.
In pharmacological assessment of an herbal medicine, it is important to
understand not only its chemical content but also which herb-derived compounds
circulate considerably in the bloodstream after dosing. In this study, notable
differences were found between the circulating compounds derived from ginsenosides
after p.o. ingestion of Sanqi-extract and the ginsenosides present in the extract. Our
study provides information for the ethnopharmacologists on which Sanqi-derived
compounds are worth further evaluation, while it also tells the phytochemists which
Sanqi-derived compounds should be prepared for the pharmacological and safety
assessments. In summary, 20(S)-protopanaxadiol, 20(S)-protopanaxatriol, and their
oxidized metabolites, as well as compound-K, represent major circulating forms of
ginsenosides in the human bloodstream after p.o. ingestion of Sanqi-extract. However,
the systemic exposure levels of these metabolites are of large interindividual variance,
which depend on the deglycosylation activities of the colonic microflora of individual
subjects, rather than the Sanqi-extract dosage size. Compound-K,
20(S)-protopanaxadiol, and 20(S)-protopanaxatriol measured in human plasma can be
used as PK markers to reflect the microbial activities of human individuals. In
addition, plasma 20(S)-protopanaxadiol and 20(S)-protopanaxatriol can also serve as
PK markers to indicate the timely-changes and interindividual differences in plasma
levels of their respective oxidized metabolites. The ppd-type ginsenosides Ra3, Rb1
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
25
and Rd, as well as the ppt-type ginsenosides Rg1, F2, and notoginsenoside R1, can be
used as Sanqi-extract dose-dependent PK markers to substantiate human systemic
exposure to the orally ingested extract. Most plasma ginsenosides, as well as their
metabolites, accumulate substantially in the systemic circulation during multi-dose
treatment with oral Sanqi-extract.
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
26
Authorship Contributions
Participated in research design: Li, Yang, Huang, and Gao
Conducted experiments: Hu, Yang, Cheng, Du, Huang, Wang, Niu, and Xu
Performed data analysis: Li, Hu, Yang, Cheng, and Jiang
Wrote or contributed to the writing of the manuscript: Li, Hu, Yang, and Cheng
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
27
References
Chinese Pharmacopoeia Commission (2010) Pharmacopoeia of the People’s Republic of China,
volume 1, English 11th ed. (China Medical Science Press, Beijing)
Christensen LP (2009) Ginsenosides: chemistry, biosynthesis, analysis, and potential health effects.
Adv Food Nutr Res 55:1–99.
Hao H-P, Lai L, Zheng C-N, Wang Q, Yu G, Zhou X-Y, Wu L, Gong P, and Wang G-J (2010)
Microsomal cytochrome p450-mediated metabolism of protopanaxatriol ginsenosides:
metabolite profile, reaction phenotyping, and structure-metabolism relationship. Drug Metab
Dispos 38:1731–1739.
Hasegawa H, Sung J-H, Matsumiya S, Uchiyama M (1996) Main ginseng saponin metabolites
formed by intestinal bacteria. Planta Med 62:453–457.
Kasai R, Hara K, Dokan R, Suzuki N, Mizutare T, Yoshihara S, and Yamasaki K (2000) Major
metabolites of ginseng sapogenins formed by rat liver microsomes. Chem Pharm Bull
48:1226–1227.
Lai Y-R (2009) Identification of interspecies difference in hepatobiliary transporters to improve
extrapolation of human biliary secretion. Expert Opin Drug Metab Toxicol 5:1175–1187.
Li C (2012) Absorption, disposition, and pharmacokinetics of herbal medicines: what and how?
Curr Drug Metab 13:491–493.
Li L, Chen X-Y, Li D, and Zhong D-F (2011) Identification of 20(S)-protopanaxadiol metabolites
in human liver microsomes and human heptatocytes. Drug Metab Dispos 39:472–483.
Li L, Zhao Y-S, Du F-F, Yang J-L, Xu F, Niu W, Ren Y-H, and Li C (2012) Intestinal absorption
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
28
and presystemic elimination of various chemical constituents present in GBE50 extract, a
standardized extract of Ginkgo biloba leaves. Curr Drug Metab 13:494–509.
Liu H-F, Yang J-L, Du F-F, Gao X-M, Ma X-T, Huang Y-H, Xu F, Niu W, Wang F-Q, Mao Y,
Sun Y, Lu T, Liu C-X, Zhang B-L, and Li C (2009) Absorption and disposition of ginsenosides
after oral administration of Panax notoginseng extract to rats. Drug Metab Dispos
37:2290–2298.
Lu T, Yang J-L, Gao X-M, Chen P, Du F-F, Sun Y, Wang F-Q, Xu F, Shang H-C, Huang Y-H,
Wang Y, Wan R-Z, Liu C-X, Zhang B-L, and Li C (2008) Plasma and urinary tanshinol from
Salvia miltiorrhiza (Danshen) can be used as pharmacokinetic markers for cardiotonic pills, a
cardiovascular herbal medicine. Drug Metab Dispos 36:1578–1586.
Lv J-M, Yao Q-Z, and Chen C-Y (2009) Ginseng compounds: an update on their molecular
mechanisms and medical applications. Curr Vasc Pharmacol 7: 293–302.
Ma Y-K and Dai X-L (2011) Safety investigation of total saponins from Notoginseng Radix et
Rhizoma. Food and Drug 13: 408–411.
Mahmood I and Sahajwalla C (2002) Interspecies scaling of biliary excreted drugs. J Pharm Sci
91:1908–1914.
Nicholson JK, Holmes E, and Wilson ID (2005) Gut microorganisms, mammalian metabolism and
personalized health care. Nat Rev Microbiol 3:431–438.
Pritchard JF, Jurima-Romet M, Reimer ML, Mortimer E, Rolfe B, Cayen MN (2003). Making
better drugs: Decision gates in non-clinical drug development. Nat Rev Drug Discov 2:542–553.
Qiu J (2007) China plans to modernize traditional medicine. Nature 446:590–591.
Reagan-Shaw S, Nihal M, and Ahmad N (2007) Dose translation from animal to human studies
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
29
revisited. FASEB J 22: 659–661.
Smith BP, Vandenhende FR, DeSante KA, Farid NA, Welch PA, Callaghan JT, Forgue ST (2000)
Confidence interval criteria for assessment of dose proportionality. Pharm Res 17:1278–1283.
Sousa T, Paterson R, Moore V, Carlsson A, Abrahamsson B, and Basit AW (2008) The
gastrointestinal microbiota as a site for the biotransformation of drugs. Int J Pharm 363:1–25.
Tawab MA, Bahr U, Karas M, Wurglics M, and Schubert-Zsilavecz M (2003) Degradation of
ginsenosides in humans after oral administration. Drug Metab Dispos 31:1065–1071.
Yan R, Ko NL, Ma B, Tam YK, and Lin G (2012) Metabolic conversion from co-existing
ingredient leading to significant systemic exposure of Z-butylidenephthalide, a minor ingredient
in Chuanxiong Rhizoma in rats. Curr Drug Metab 13:524–534.
Yang L, Liu Y, and Liu C-X (2006) Metabolism and pharmacokinetics of ginsenosides. Asian J
Pharmacodyn Pharmacokinet 6:103–120.
Zhang J-W, Zhou F, Lu M, Ji W, Niu F, Zha W-B, Wu X-L, Ha H-P, and Wang G-J (2012)
Pharmacokinetic-pharmacology disconnection of herbal medicines and its potential solutions
with cellular pharmacokinetic-pharmacodynamic strategy. Curr Drug Metab 13:558–576.
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
30
Footnotes
Zheyi Hu, Junling Yang, and Chen Cheng contributed equally to the study. This work was
supported by the National Science Fund of China for Distinguished Young Scholars [Grant
30925044], the National Basic Research Program of China [Grant 2012CB518403], the National
Science and Technology Major Project of China “Key New Drug Creation and Manufacturing
Program” [Grants 2009ZX09304-002, 2012ZX09304007, and 2012ZX09303010], and the
Knowledge Innovation Program of the Chinese Academy of Sciences [Grant
KSCX2-YW-R-191].
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

DMD #51391
31
Legends for Figures
Fig. 1. Flowchart for the two-period, open-label, single center human study. Twenty four subjects
were randomly assigned to one of three dosage groups (four males and four females per group). After
the random assignment, the subjects were renumbered before receiving a p.o. dose of Sanqi-extract at
90 (the male subjects m1–m4 and the female subjects f1–f4), 180 (m5–m8 and f5–f8), or 270
ml/subject (m9–m12 and f9–f12). In addition, the subjects m1–m4, after three-day wash-out period
following the first acute p.o. treatment with Sanqi-extract, continued to receive multiple p.o. doses of
the herb extract at 90 ml/subject/day for three weeks. Their blood and urine samples were collected
on days 11, 18, and 24. “HF/RF” denotes hepatic function and renal function.
Fig. 2. Ginsenosides present in Sanqi-extract (panel A), as well as plasma (panels B and D) and
urinary ginsenosides and their metabolites measured (panels C and E) after p.o. administration of
Sanqi-extract (270 ml/subject). The blood was sampled from the human subjects 8 and 24 h after
dosing, which normally had high levels of the ginsenosides absorbed and those of the metabolites
formed, respectively. After centrifugation, all the plasma fractions (10 μl from each) were pooled
before analysis. Meanwhile, the urine samples (0–24 h after dosing) were also collected from these
subjects and the sample combining (20 μl from each) was also performed for analysis. Compound-K,
20(S)-protopanaxadiol, and 20(S)-protopanaxatriol were not present in Sanqi-extract; they were
ginsenosides’ metabolites measured in plasma. The symbol “×” (in red) denotes the ginsenoside or
metabolite not measured in human or urine. Blue, red, and black bars are used to show the content
levels of ginsenosides in Sanqi-extract, their plasma levels, and their urine levels, respectively, while
pink and grey bars exhibit the plasma and the urine levels of ginsenosides’ metabolites, respectively.
The response was determined as compound peak area corrected with the intensity ratio of the
fragment ion to the precursor ion. Relative abundance measures are expressed in percentile, with 100
being 20(S)-protopanaxatriol in the plasma data set and with 100 being ginsenoside Rg1 in the urinary
data set.
Fig. 3. Proposed metabolism pathways of compound-K, 20(S)-protopanaxadiol, and
20(S)-protopanaxatriol in humans. The metabolites in the brackets are proposed intermediates, which
were not measured in the samples of human plasma (HP) or human urine (HU). The metabolites M36,
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
32
M37, and M38 were the glucuronides of M20, M21, and M22, respectively, which were measured in
the samples of rat bile (RB) after i.v. administration of 20(S)-protopanaxadiol.
Fig. 4. Human CYP enzymes mediating the oxidation of 20(S)-protopanaxadiol or that of
20(S)-protopanaxatriol. The substrate and enzyme concentration used were 2 μM and 50 pmol
P450/ml, respectively, for all the test cDNA-expressed CYP enzymes and the incubation time was 5
min (panels A and B) or 30 min (panels C and D). The response was determined as compound peak
area corrected with the intensity ratio of the fragment ion to the precursor ion. The relative abundance
was expressed as percentile, with 100, in the data sets, being the most abundant M8 that was formed
after incubation with CYP3A4 for 30 min.
Fig. 5. Mean plasma concentration-time profiles of ginsenosides and their major metabolites after a
single p.o. dose of Sanqi-extract at 90 (green solid lines), 180 (blue solid lines), or 270 ml/subject (red
solid lines). The subject f12 (receiving Sanqi-extract at 270 ml/subject; red dashed lines) exhibited
marked extensive but delayed formation of 20(S)-protopanaxadiol and 20(S)-protopanaxatriol, and
their oxidized metabolites.
Fig. 6. AUC0-56h values of compound-K, 20(S)-protopanaxadiol, 20(S)-protopanaxatriol, the
ppd-derived metabolites (M16, M17, and M19–M22), and the ppt-derived metabolites (M4–M8 and
M10–M15) being Sanqi-extract dose-independent. The exposure values were measured in human
subjects (solid circles, the male subjects; open circles, the female subjects) receiving a p.o. dose of
Sanqi-extract at 90 (green circles), 180 (blue circles), or 270 ml/subject (red circles). Unlike the
metabolites’ situations, AUC0-56h values of ginsenoside Ra3, Rb1, Rd, F2, Rg1, and notoginsenoside R1
increased in Sanqi-extract dose-dependent manners. The term “r” denotes the correlation coefficient.
The ratio of dose-normalized geometric mean AUC values is given before the parentheses, while the
numbers in the parentheses are the statistically derived 90% confidence interval. The critical interval
was 0.797–1.203.
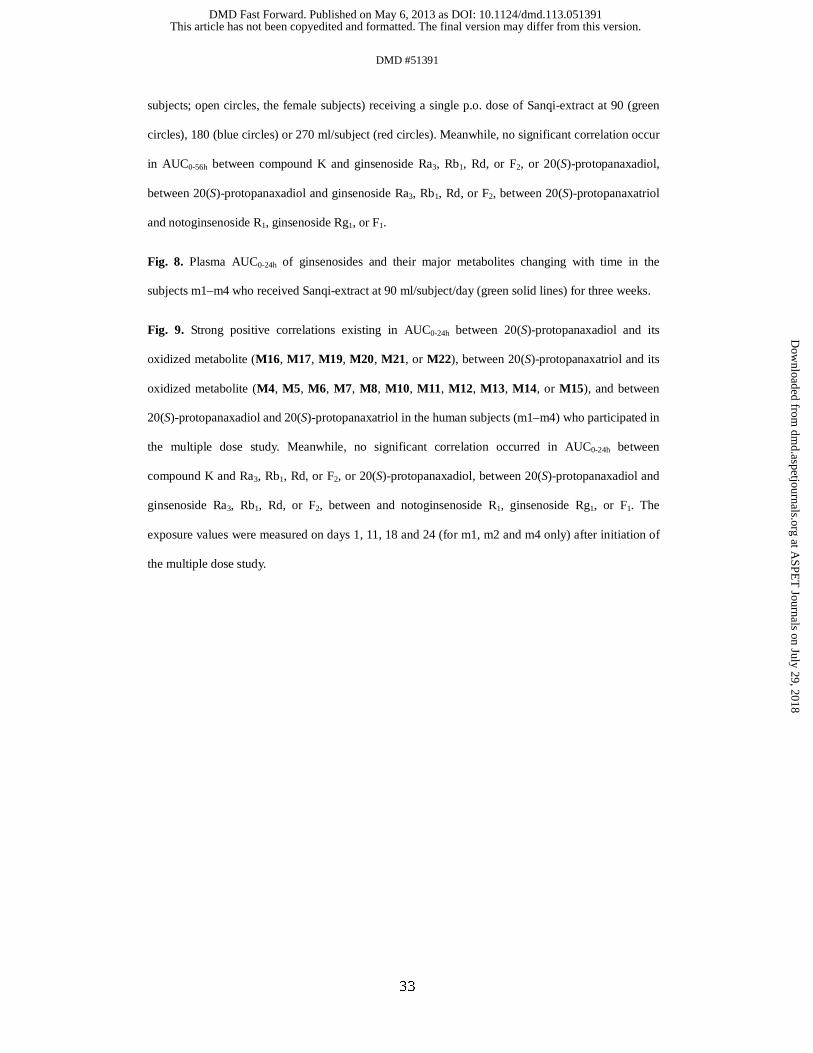
Fig. 7. Strong positive correlations existing in AUC0-56h between 20(S)-protopanaxadiol and its
oxidized metabolite (M16, M17, M19, M20, M21, or M22), between 20(S)-protopanaxatriol and its
oxidized metabolite (M4, M5, M6, M7, M8, M10, M11, M12, M13, M14, or M15), and between
20(S)-protopanaxadiol and 20(S)-protopanaxatriol in the human subjects (solid circles, the male
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
DMD #51391
33
subjects; open circles, the female subjects) receiving a single p.o. dose of Sanqi-extract at 90 (green
circles), 180 (blue circles) or 270 ml/subject (red circles). Meanwhile, no significant correlation occur
in AUC0-56h between compound K and ginsenoside Ra3, Rb1, Rd, or F2, or 20(S)-protopanaxadiol,
between 20(S)-protopanaxadiol and ginsenoside Ra3, Rb1, Rd, or F2, between 20(S)-protopanaxatriol
and notoginsenoside R1, ginsenoside Rg1, or F1.
Fig. 8. Plasma AUC0-24h of ginsenosides and their major metabolites changing with time in the
subjects m1–m4 who received Sanqi-extract at 90 ml/subject/day (green solid lines) for three weeks.
Fig. 9. Strong positive correlations existing in AUC0-24h between 20(S)-protopanaxadiol and its
oxidized metabolite (M16, M17, M19, M20, M21, or M22), between 20(S)-protopanaxatriol and its
oxidized metabolite (M4, M5, M6, M7, M8, M10, M11, M12, M13, M14, or M15), and between
20(S)-protopanaxadiol and 20(S)-protopanaxatriol in the human subjects (m1–m4) who participated in
the multiple dose study. Meanwhile, no significant correlation occurred in AUC0-24h between
compound K and Ra3, Rb1, Rd, or F2, or 20(S)-protopanaxadiol, between 20(S)-protopanaxadiol and
ginsenoside Ra3, Rb1, Rd, or F2, between and notoginsenoside R1, ginsenoside Rg1, or F1. The
exposure values were measured on days 1, 11, 18 and 24 (for m1, m2 and m4 only) after initiation of
the multiple dose study.
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
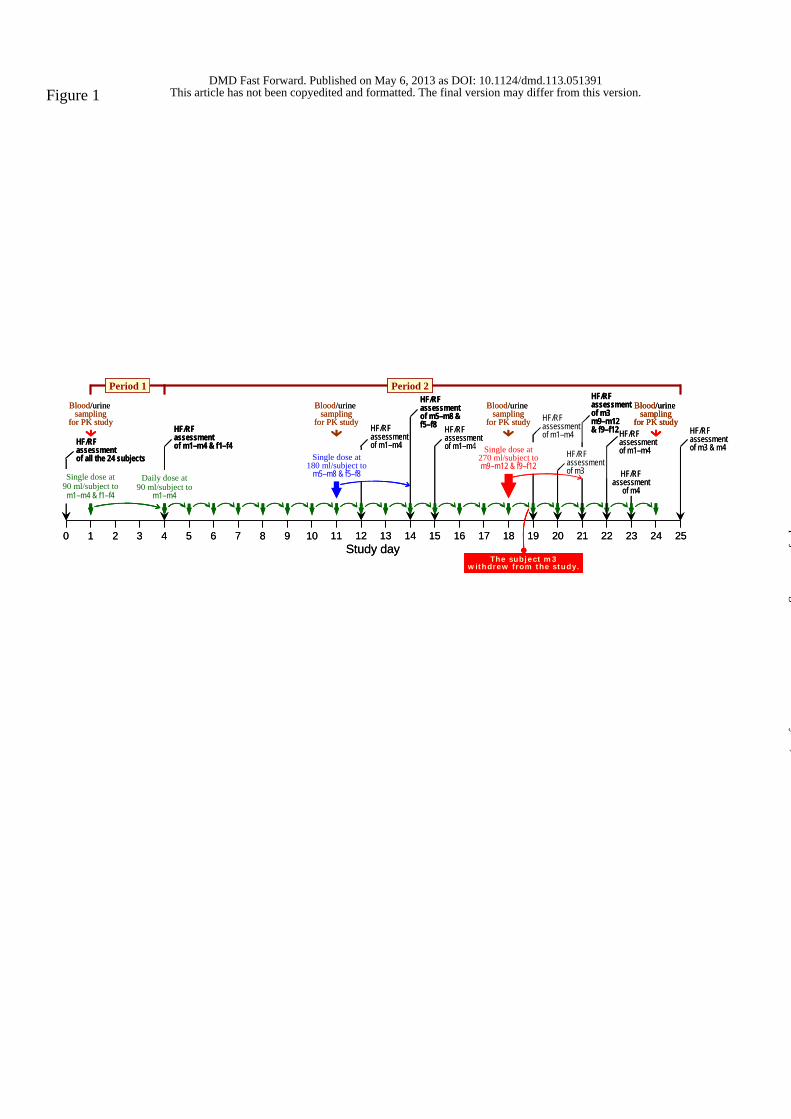
Figure 1
11 12 13 14
Blood/urinesampling
for PK study
HF/RFassessmentof all the 24 subjects
7 8 9 103 4 5 60 1 2 15 16 17 18 19 20 21 22 23 24 25
Period 1 Period 2
HF/RFassessmentof m1–m4 & f1–f4
HF/RFassessmentof m1–m4
HF/RFassessmentof m3 & m4
HF/RFassessmentof m1–m4
HF/RFassessment
of m4
Blood/urine sampling
for PK study
Blood/urinesampling
for PK study
Blood/urine sampling
for PK study
Daily dose at90 ml/subject to
m1–m4
The subject m3withdrew from the study.
Single dose at90 ml/subject to
m1–m4 & f1–f4
Single dose at180 ml/subject to
m5–m8 & f5–f8
Single dose at270 ml/subject tom9–m12 & f9–f12
HF/RFassessmentof m1–m4
Study day
HF/RFassessmentof m3m9–m12& f9–f12
HF/RFassessmentof m1–m4
HF/RFassessmentof m5–m8 &f5–f8
HF/RFassessmentof m3
11 12 13 14
Blood/urinesampling
for PK study
HF/RFassessmentof all the 24 subjects
7 8 9 103 4 5 60 1 2 15 16 17 18 19 20 21 22 23 24 25
Period 1 Period 2
HF/RFassessmentof m1–m4 & f1–f4
HF/RFassessmentof m1–m4
HF/RFassessmentof m3 & m4
HF/RFassessmentof m1–m4
HF/RFassessment
of m4
Blood/urine sampling
for PK study
Blood/urinesampling
for PK study
Blood/urinesampling
for PK study
Blood/urine sampling
for PK study
Daily dose at90 ml/subject to
m1–m4
Daily dose at90 ml/subject to
m1–m4
The subject m3withdrew from the study.
The subject m3withdrew from the study.
Single dose at90 ml/subject to
m1–m4 & f1–f4
Single dose at90 ml/subject to
m1–m4 & f1–f4
Single dose at180 ml/subject to
m5–m8 & f5–f8
Single dose at270 ml/subject tom9–m12 & f9–f12
HF/RFassessmentof m1–m4
Study day
HF/RFassessmentof m3m9–m12& f9–f12
HF/RFassessmentof m1–m4
HF/RFassessmentof m5–m8 &f5–f8
HF/RFassessmentof m3
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
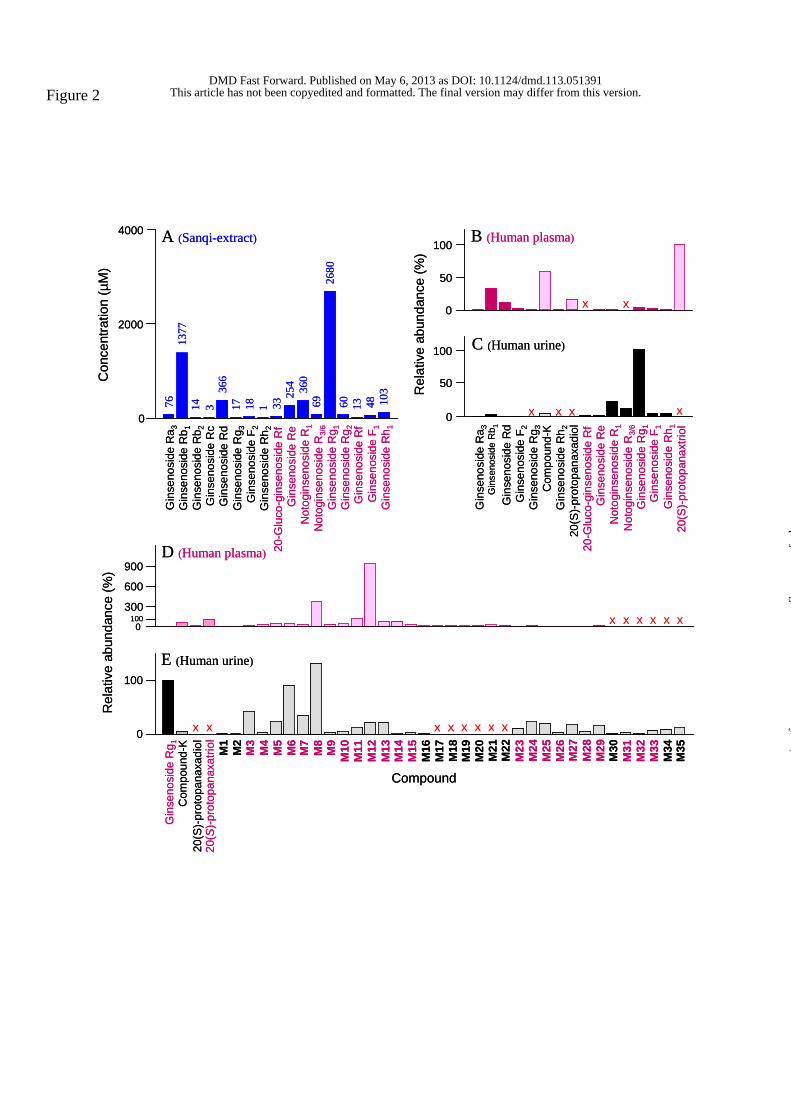
Figure 2
100
0
0
Rel
ativ
e ab
unda
nce
(%)
100300
600
900
X X X X X X
Com
poun
d-K
Gin
seno
side
Rg 1 M2
M3
M4
M5
M6
M7
M8
M9
M10
M11
M12
M13
M14
M15
M16
M17
M18
M19
M20
M21
M22
M23
M24
M25
M26
M27
M28
M29
M30
M31
M32
M33
M34
M35
X X X X X X
D (Human plasma)
E (Human urine)
M1
20(S
)-pro
topa
naxa
triol
X X
Compound
A (Sanqi-extract)
0
2000
4000
Con
cent
ratio
n (µ
M)
Gin
seno
side
Ra 3
Gin
seno
side
Rb 1
Gin
seno
side
Rb 2
Gin
seno
side
Rc
Gin
seno
side
Rd
Gin
seno
side
Rg 3
Gin
seno
side
F2
Gin
seno
side
Rh 2
20-G
luco
-gin
seno
side
Rf
Gin
seno
side
Re
Not
ogin
seno
side
R1
Not
ogin
seno
side
R3/
6G
inse
nosi
de R
g 1G
inse
nosi
de R
g 2G
inse
nosi
de R
fG
inse
nosi
de F
1G
inse
nosi
de R
h 1
7613
7714 3
366
17 18 1 3325
4 360
6926
8060 13 48 10
3
B (Human plasma)
C (Human urine)
50
0
50
100
Rel
ativ
e ab
unda
nce
(%)
100
0
Gin
seno
side
Ra 3
Gin
seno
side
Rb 1
Gin
seno
side
Rd
Gin
seno
side
F2
Gin
seno
side
Rg 3
Com
poun
d-K
Gin
seno
side
Rh 2
20(S
)-pro
topa
naxa
diol
20-G
luco
-gin
seno
side
Rf
Gin
seno
side
Re
Not
ogin
seno
side
R1
Not
ogin
seno
side
R3/
6G
inse
nosi
de R
g 1G
inse
nosi
de F
1G
inse
nosi
de R
h 120
(S)-p
roto
pana
xtrio
l
X X
X XXX
20(S
)-pr
otop
anax
adio
l
100
0
0
Rel
ativ
e ab
unda
nce
(%)
100300
600
900
X X X X X X
Com
poun
d-K
Gin
seno
side
Rg 1 M2
M3
M4
M5
M6
M7
M8
M9
M10
M11
M12
M13
M14
M15
M16
M17
M18
M19
M20
M21
M22
M23
M24
M25
M26
M27
M28
M29
M30
M31
M32
M33
M34
M35
X X X X X X
D (Human plasma)
E (Human urine)
M1
20(S
)-pro
topa
naxa
triol
X X
Compound
A (Sanqi-extract)
0
2000
4000
Con
cent
ratio
n (µ
M)
Gin
seno
side
Ra 3
Gin
seno
side
Rb 1
Gin
seno
side
Rb 2
Gin
seno
side
Rc
Gin
seno
side
Rd
Gin
seno
side
Rg 3
Gin
seno
side
F2
Gin
seno
side
Rh 2
20-G
luco
-gin
seno
side
Rf
Gin
seno
side
Re
Not
ogin
seno
side
R1
Not
ogin
seno
side
R3/
6G
inse
nosi
de R
g 1G
inse
nosi
de R
g 2G
inse
nosi
de R
fG
inse
nosi
de F
1G
inse
nosi
de R
h 1
7613
7714 3
366
17 18 1 3325
4 360
6926
8060 13 48 10
3
B (Human plasma)
C (Human urine)
50
0
50
100
Rel
ativ
e ab
unda
nce
(%)
100
0
Gin
seno
side
Ra 3
Gin
seno
side
Rb 1
Gin
seno
side
Rd
Gin
seno
side
F2
Gin
seno
side
Rg 3
Com
poun
d-K
Gin
seno
side
Rh 2
20(S
)-pro
topa
naxa
diol
20-G
luco
-gin
seno
side
Rf
Gin
seno
side
Re
Not
ogin
seno
side
R1
Not
ogin
seno
side
R3/
6G
inse
nosi
de R
g 1G
inse
nosi
de F
1G
inse
nosi
de R
h 120
(S)-p
roto
pana
xtrio
l
X X
X XXX
20(S
)-pr
otop
anax
adio
l
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
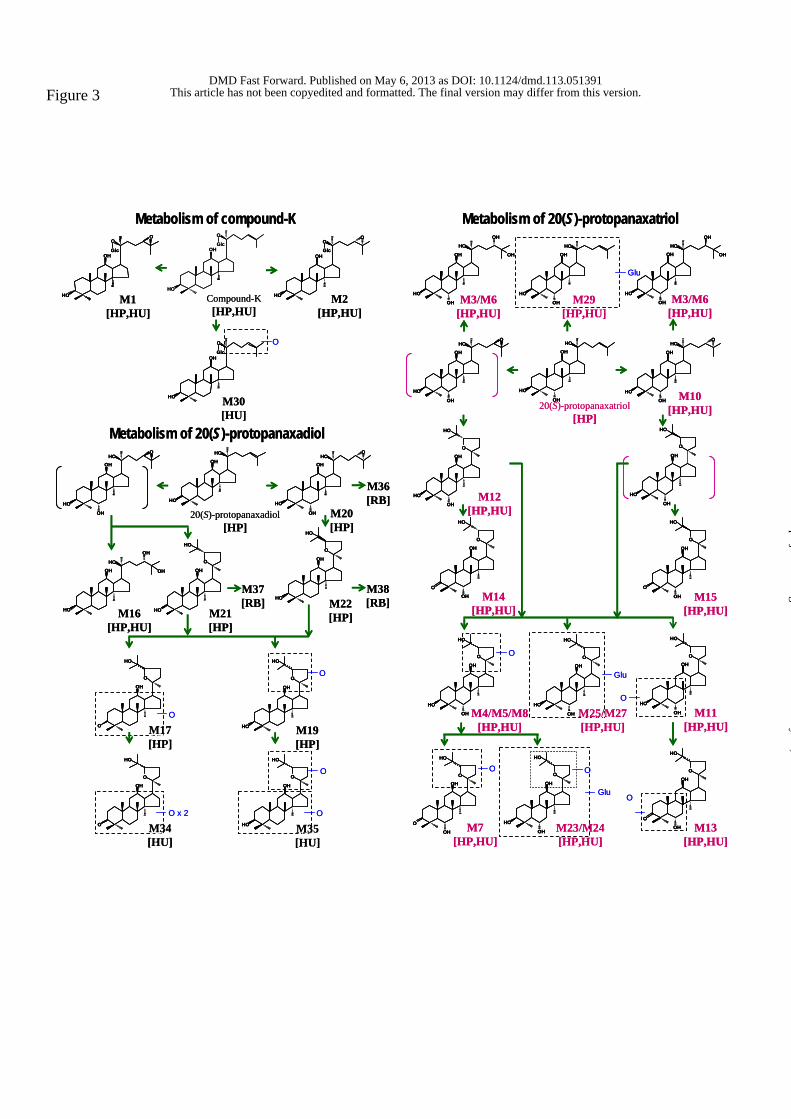
Figure 3
M1[HP,HU]
M2[HP,HU]
M3/M6[HP,HU]
M3/M6[HP,HU]
Glu
Metabolism of compound-K Metabolism of 20(S)-protopanaxatriol
HO
OH
O
Glc
O
HO
OH
O
Glc
HO
OH
O
Glc
O
HO
OH
OH
HO
OH
OH
HO
OH
OH
HO
HO
OH
OH
HO
OH
OH
M30[HU]
O
M10[HP,HU]
M21[HP]
O x 2
O
O
M19[HP]
O
O
M16[HP,HU]
M20[HP]
M22[HP]
Metabolism of 20(S)-protopanaxadiol
20(S)-protopanaxadiol[HP]
M38[RB]
M36[RB]
M37[RB]
HO
OH
O
Glc
HO
OH
OH
HOO
HO
OHHO
HO
OH
OH
HOO
HO
OHHO
OH
OH
HO
OH
O
HO
O
OH
O
HO
HO
OH
O
HO
O
OHO
HO
HO
OH
O
HO
HO
OH
OH
HOO
HO
OH
OH
HO
HO
OH
OH
HOO
M12[HP,HU]
M14[HP,HU]
M15[HP,HU]
M4/M5/M8[HP,HU]
M11[HP,HU]
M7[HP,HU]
M13[HP,HU]
O
Glu
O
O O
OGlu
20(S)-protopanaxatriol[HP]
O
OHO
HO
OH
HO
OH
O
HO
OH
HO
OH
O
HO
OH
O
OH
O
HO
OH
HO
OHO
HO
OH
HO
OHO
HO
OH
O
OHO
HO
OH
HO
OH
O
HO
OH
HO
OHO
HO
OH
O
OHO
HO
OH
Compound-K[HP,HU]
HO
OH
O
HO
M35[HU]M35[HU]
M34[HU]M34[HU]
M17[HP]M17[HP]
M29[HP,HU]
M29[HP,HU]
M25/M27[HP,HU]
M25/M27[HP,HU]
M23/M24[HP,HU]
M23/M24[HP,HU]
M1[HP,HU]
M2[HP,HU]
M3/M6[HP,HU]
M3/M6[HP,HU]
Glu
Metabolism of compound-K Metabolism of 20(S)-protopanaxatriol
HO
OH
O
Glc
O
HO
OH
O
Glc
O
HO
OH
O
Glc
HO
OH
O
Glc
O
HO
OH
O
Glc
O
HO
OH
OH
HO
OH
OH
HO
OH
OH
HO
OH
OH
HO
OH
OH
HO
HO
OH
OH
HO
HO
OH
OH
HO
OH
OH
HO
OH
OH
HO
OH
OH
M30[HU]
O
M10[HP,HU]
M21[HP]
O x 2
O
O
M19[HP]
O
O
M16[HP,HU]
M20[HP]
M22[HP]
Metabolism of 20(S)-protopanaxadiol
20(S)-protopanaxadiol[HP]
M38[RB]
M36[RB]
M37[RB]
HO
OH
O
Glc
HO
OH
O
Glc
HO
OH
OH
HOO
HO
OH
OH
HOO
HO
OHHO
HO
OHHO
HO
OH
OH
HOO
HO
OH
OH
HOO
HO
OHHO
OH
OH
HO
OHHO
OH
OH
HO
OH
O
HO
HO
OH
O
HO
O
OH
O
HO
O
OH
O
HO
HO
OH
O
HO
HO
OH
O
HO
O
OHO
HO
O
OHO
HO
HO
OH
O
HO
HO
OH
O
HO
HO
OH
OH
HOO
HO
OH
OH
HOO
HO
OH
OH
HO
HO
OH
OH
HO
HO
OH
OH
HOO
HO
OH
OH
HOO
M12[HP,HU]
M14[HP,HU]
M15[HP,HU]
M4/M5/M8[HP,HU]
M11[HP,HU]
M7[HP,HU]
M13[HP,HU]
O
Glu
O
O O
OGlu
20(S)-protopanaxatriol[HP]
O
OHO
HO
OH
O
OHO
HO
OH
HO
OH
O
HO
OH
HO
OH
O
HO
OH
HO
OH
O
HO
OH
HO
OH
O
HO
OH
O
OH
O
HO
OH
O
OH
O
HO
OH
HO
OHO
HO
OH
HO
OHO
HO
OH
HO
OHO
HO
OH
HO
OHO
HO
OH
O
OHO
HO
OH
O
OHO
HO
OH
HO
OH
O
HO
OH
HO
OH
O
HO
OH
HO
OHO
HO
OH
HO
OHO
HO
OH
O
OHO
HO
OH
O
OHO
HO
OH
Compound-K[HP,HU]
HO
OH
O
HO
HO
OH
O
HO
M35[HU]M35[HU]
M34[HU]M34[HU]
M17[HP]M17[HP]
M29[HP,HU]
M29[HP,HU]
M25/M27[HP,HU]
M25/M27[HP,HU]
M23/M24[HP,HU]
M23/M24[HP,HU]
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
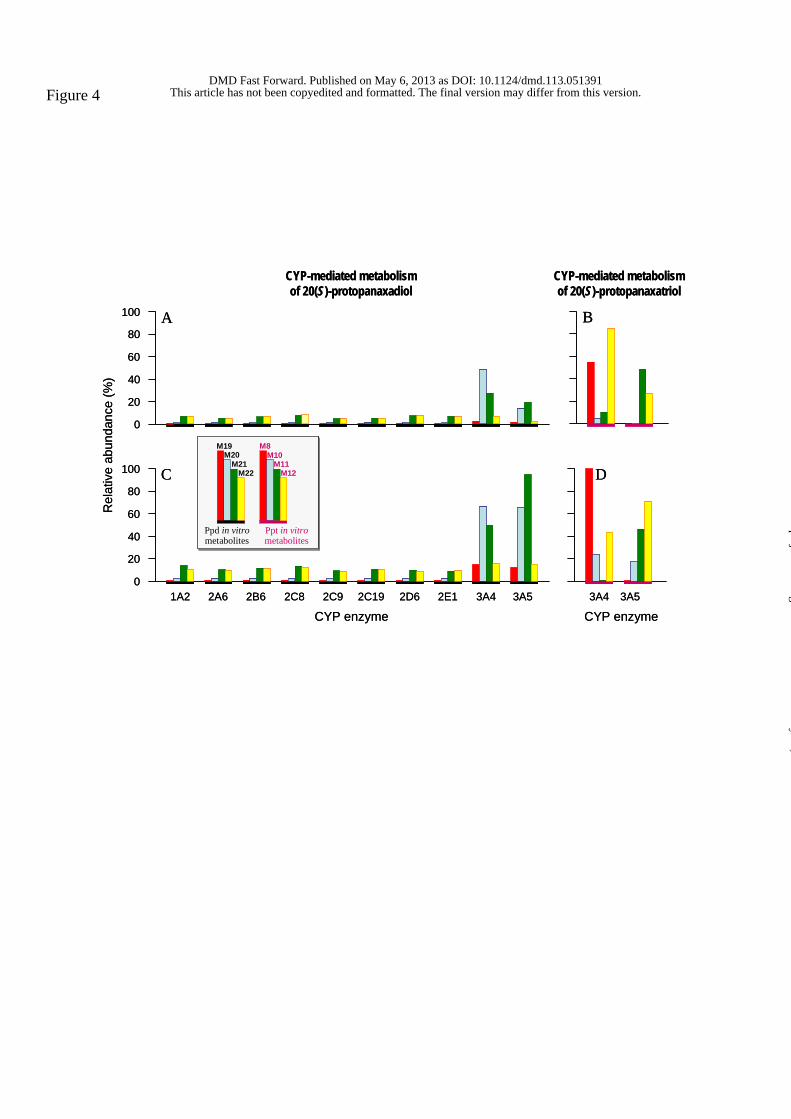
Figure 4
1A2 2A6 2C8 2C92B6 2C19 2E12D6 3A53A4
100
80
60
40
20
0
CYP-mediated metabolism of 20(S)-protopanaxadiol
CYP-mediated metabolism of 20(S)-protopanaxatriol
CYP enzyme
Rel
ativ
e ab
unda
nce
(%)
Ppd in vitrometabolites
M20M21
M22
Ppt in vitrometabolites
M8M10
M11M12
M19
3A53A4
CYP enzyme
100
80
60
40
20
0
A B
C D
1A2 2A6 2C8 2C92B6 2C19 2E12D6 3A53A4
100
80
60
40
20
0
CYP-mediated metabolism of 20(S)-protopanaxadiol
CYP-mediated metabolism of 20(S)-protopanaxatriol
CYP enzyme
Rel
ativ
e ab
unda
nce
(%)
Ppd in vitrometabolites
M20M21
M22
Ppt in vitrometabolites
M8M10
M11M12
M19
Ppd in vitrometabolites
M20M21
M22
Ppt in vitrometabolites
M8M10
M11M12
M19
3A53A4
CYP enzyme
100
80
60
40
20
0
A B
C D
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
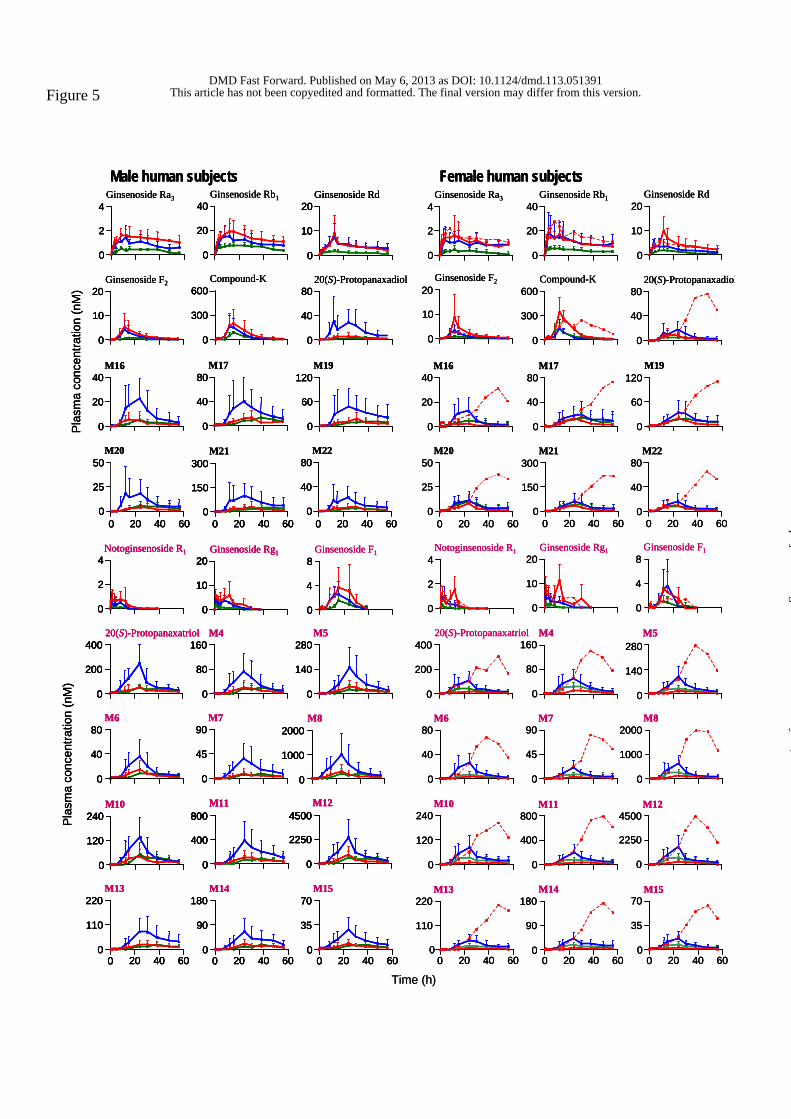
Figure 5
Time (h)
Ginsenoside Ra34
2
0
Ginsenoside Rd20
10
0
Ginsenoside Rb140
20
0
Ginsenoside F220
10
0
Compound-K600
300
0
20(S)-Protopanaxadiol80
40
0
40
20
0
M16 M1780
40
0
120
60
0
M19
0 20 40 60
M2050
25
0
M2280
40
0
M21300
150
0
Ginsenoside F18
4
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
M4160
80
0
20(S)-Protopanaxatriol400
200
0
M5280
140
0
M6 M7 M880
40
0
90
45
0
2000
1000
0
M10240
120
0
M11 M12800
400
0
4500
2250
0
M14M13 M15220
110
0
180
90
0
70
35
00 20 40 60 0 20 40 60 0 20 40 60
Female human subjects
0 20 40 60 0 20 40 60
Ginsenoside Ra34
2
0
Male human subjectsGinsenoside Rd
20
10
0
40
20
0
Ginsenoside Rb1
Ginsenoside F220
10
0
600
300
0
Compound-K80
40
0
20(S)-Protopanaxadiol
M16 M1740
20
0
80
40
0
M19120
60
0
50
25
0
M20 M2280
40
0
M21300
150
0
Ginsenoside F18
4
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
M4160
80
0
20(S)-Protopanaxatriol 400
200
0
280
140
0
M5
90
45
0
M6 M7 M82000
1000
0
80
40
0
M10240
120
0
M124500
2250
0
M11800
400
0
M13 M14 M1570
35
0
180
90
0
220
110
00 20 40 60 0 20 40 60 0 20 40 60
Pla
sma
conc
entra
tion
(nM
)
0 20 40 600 20 40 600 20 40 60
Pla
sma
conc
entra
tion
(nM
)
Time (h)
Ginsenoside Ra34
2
0
Ginsenoside Rd20
10
0
Ginsenoside Rb140
20
0
Ginsenoside F220
10
0
Compound-K600
300
0
20(S)-Protopanaxadiol80
40
0
40
20
0
M16 M1780
40
0
120
60
0
M19
0 20 40 60
M2050
25
0
M2280
40
0
M21300
150
0
Ginsenoside F18
4
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
M4160
80
0
20(S)-Protopanaxatriol400
200
0
M5280
140
0
M6 M7 M880
40
0
90
45
0
2000
1000
0
M10240
120
0
M11 M12800
400
0
4500
2250
0
M14M13 M15220
110
0
180
90
0
70
35
00 20 40 60 0 20 40 60 0 20 40 60
Female human subjects
0 20 40 60 0 20 40 60
Ginsenoside Ra34
2
0
Ginsenoside Rd20
10
0
Ginsenoside Rb140
20
0
Ginsenoside F220
10
0
Compound-K600
300
0
20(S)-Protopanaxadiol80
40
0
40
20
0
M16 M1780
40
0
120
60
0
M19
0 20 40 60
M2050
25
0
M2280
40
0
M21300
150
0
Ginsenoside F18
4
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
M4160
80
0
20(S)-Protopanaxatriol400
200
0
M5280
140
0
M6 M7 M880
40
0
90
45
0
2000
1000
0
M10240
120
0
M11 M12800
400
0
4500
2250
0
M14M13 M15220
110
0
180
90
0
70
35
00 20 40 60 0 20 40 60 0 20 40 60
Female human subjects
0 20 40 60 0 20 40 60
Ginsenoside Ra34
2
0
Male human subjectsGinsenoside Rd
20
10
0
40
20
0
Ginsenoside Rb1
Ginsenoside F220
10
0
600
300
0
Compound-K80
40
0
20(S)-Protopanaxadiol
M16 M1740
20
0
80
40
0
M19120
60
0
50
25
0
M20 M2280
40
0
M21300
150
0
Ginsenoside F18
4
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
M4160
80
0
20(S)-Protopanaxatriol 400
200
0
280
140
0
M5
90
45
0
M6 M7 M82000
1000
0
80
40
0
M10240
120
0
M124500
2250
0
M11800
400
0
M13 M14 M1570
35
0
180
90
0
220
110
00 20 40 60 0 20 40 60 0 20 40 60
Pla
sma
conc
entra
tion
(nM
)
0 20 40 600 20 40 600 20 40 60
Pla
sma
conc
entra
tion
(nM
)
Ginsenoside Ra34
2
0
4
2
0
Male human subjectsGinsenoside Rd
20
10
0
Ginsenoside Rd20
10
0
20
10
0
40
20
0
40
20
0
Ginsenoside Rb1
Ginsenoside F220
10
0
20
10
0
600
300
0
600
300
0
Compound-K80
40
0
80
40
0
20(S)-Protopanaxadiol
M16 M1740
20
0
40
20
0
80
40
0
80
40
0
M19120
60
0
120
60
0
50
25
0
50
25
0
M20 M2280
40
0
80
40
0
M21300
150
0
300
150
0
Ginsenoside F18
4
0
8
4
0
Notoginsenoside R14
2
0
Notoginsenoside R14
2
0
Ginsenoside Rg120
10
0
Ginsenoside Rg120
10
0
20
10
0
M4160
80
0
160
80
0
20(S)-Protopanaxatriol 400
200
0
20(S)-Protopanaxatriol 400
200
0
400
200
0
280
140
0
280
140
0
M5
90
45
0
90
45
0
M6 M7 M82000
1000
0
2000
1000
0
80
40
0
80
40
0
M10240
120
0
M10240
120
0
240
120
0
M124500
2250
0
M124500
2250
0
4500
2250
0
M11800
400
0
M11800
400
0
800
400
0
M13 M14 M1570
35
0
70
35
0
180
90
0
180
90
0
220
110
0
220
110
00 20 40 600 20 40 60 0 20 40 600 20 40 60 0 20 40 600 20 40 60
Pla
sma
conc
entra
tion
(nM
)
0 20 40 600 20 40 600 20 40 600 20 40 600 20 40 600 20 40 60
Pla
sma
conc
entra
tion
(nM
)This article has not been copyedited and formatted. The final version may differ from this version.
DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
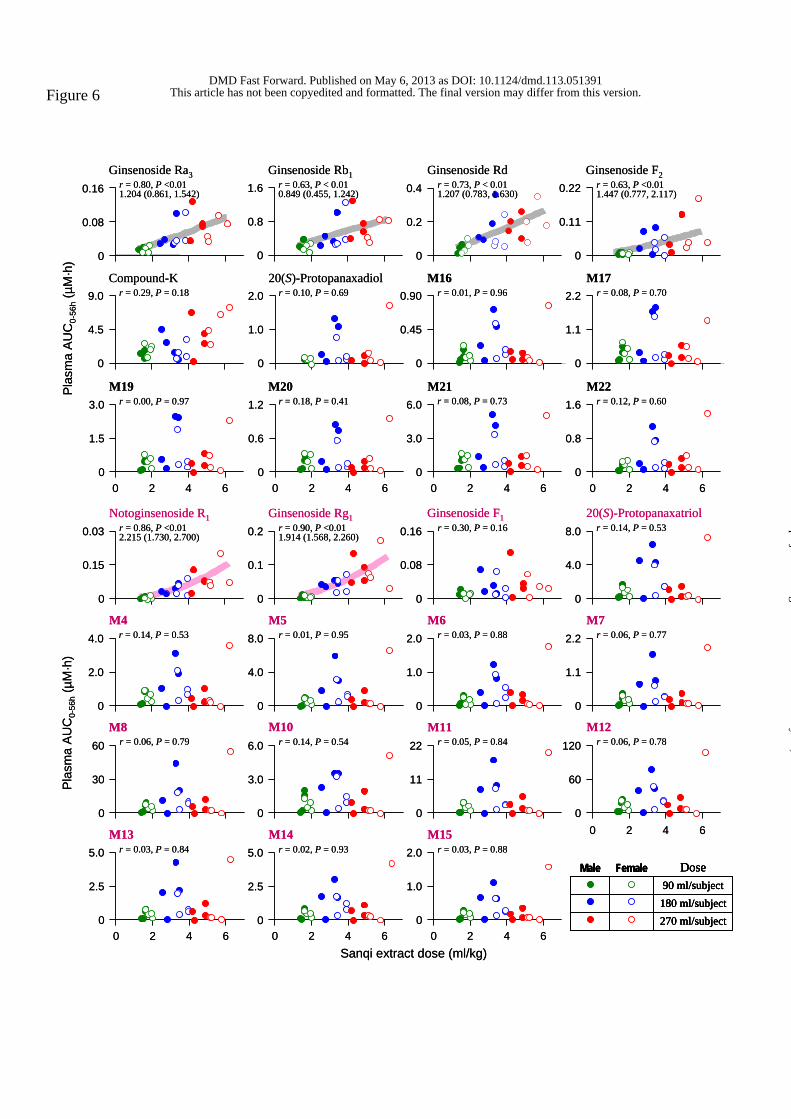
Figure 6
Pla
sma
AU
C0-
56h
(µM
·h)
Ginsenoside Ra3r = 0.80, P <0.011.204 (0.861, 1.542)
0
0.08
0.16
0
0.8
1.6 r = 0.63, P < 0.010.849 (0.455, 1.242)
Ginsenoside Rb1
0
0.2
0.4Ginsenoside Rd
0
0.11
0.22 r = 0.63, P <0.011.447 (0.777, 2.117)
Ginsenoside F2
r = 0.29, P = 0.18
0
4.5
9.0Compound-K
0
1.0
2.020(S)-Protopanaxadiol
r = 0.10, P = 0.69
0
0.45
0.90 r = 0.01, P = 0.96M16
0
1.1
2.2 r = 0.08, P = 0.70M17
0 2 4 60
1.5
3.0 r = 0.00, P = 0.97M19
0
0.6
1.2 r = 0.18, P = 0.41
0 2 4 6
M20
0
3.0
6.0 r = 0.08, P = 0.73
0 2 4 6
M21
0
0.8
1.6 r = 0.12, P = 0.60
0 2 4 6
M22
0
0.1
0.2 r = 0.90, P <0.011.914 (1.568, 2.260)
Ginsenoside Rg1
Sanqi extract dose (ml/kg)
0
0.15
0.03 r = 0.86, P <0.012.215 (1.730, 2.700)
Notoginsenoside R1
0
0.08
0.16 r = 0.30, P = 0.16Ginsenoside F1 20(S)-Protopanaxatriol
r = 0.14, P = 0.53
0
4.0
8.0
0
2.0
4.0 r = 0.14, P = 0.53M4
0
1.0
2.0 r = 0.03, P = 0.88M6
0
4.0
8.0 r = 0.01, P = 0.95M5
0
1.1
2.2 r = 0.06, P = 0.77M7
0
30
60 r = 0.06, P = 0.79M8
0
3.0
6.0 r = 0.14, P = 0.54M10
0
11
22 r = 0.05, P = 0.84M11
0
60
120 r = 0.06, P = 0.78
0 2 4 6
M12
r = 0.03, P = 0.84
0
2.5
5.0
0 2 4 6
M13
0
2.5
5.0 r = 0.02, P = 0.93
0 2 4 6
M14
0
1.0
2.0 r = 0.03, P = 0.88
0 2 4 6
M15
Plas
ma
AU
C0-
56h
(µM
·h)
r = 0.73, P < 0.011.207 (0.783, 1.630)
270 ml/subject180 ml/subject90 ml/subject
DoseFemaleMale
270 ml/subject180 ml/subject90 ml/subject
DoseFemaleMale
Pla
sma
AU
C0-
56h
(µM
·h)
Ginsenoside Ra3r = 0.80, P <0.011.204 (0.861, 1.542)
0
0.08
0.16
0
0.8
1.6 r = 0.63, P < 0.010.849 (0.455, 1.242)
Ginsenoside Rb1
0
0.2
0.4Ginsenoside Rd
0
0.11
0.22 r = 0.63, P <0.011.447 (0.777, 2.117)
Ginsenoside F2
r = 0.29, P = 0.18
0
4.5
9.0Compound-K
0
1.0
2.020(S)-Protopanaxadiol
r = 0.10, P = 0.69
0
0.45
0.90 r = 0.01, P = 0.96M16
0
1.1
2.2 r = 0.08, P = 0.70M17
0 2 4 60
1.5
3.0 r = 0.00, P = 0.97M19
0
0.6
1.2 r = 0.18, P = 0.41
0 2 4 6
M20
0
3.0
6.0 r = 0.08, P = 0.73
0 2 4 6
M21
0
0.8
1.6 r = 0.12, P = 0.60
0 2 4 6
M22
0
0.1
0.2 r = 0.90, P <0.011.914 (1.568, 2.260)
Ginsenoside Rg1
Sanqi extract dose (ml/kg)
0
0.15
0.03 r = 0.86, P <0.012.215 (1.730, 2.700)
Notoginsenoside R1
0
0.08
0.16 r = 0.30, P = 0.16Ginsenoside F1 20(S)-Protopanaxatriol
r = 0.14, P = 0.53
0
4.0
8.0
0
2.0
4.0 r = 0.14, P = 0.53M4
0
1.0
2.0 r = 0.03, P = 0.88M6
0
4.0
8.0 r = 0.01, P = 0.95M5
0
1.1
2.2 r = 0.06, P = 0.77M7
0
30
60 r = 0.06, P = 0.79M8
0
3.0
6.0 r = 0.14, P = 0.54M10
0
11
22 r = 0.05, P = 0.84M11
0
60
120 r = 0.06, P = 0.78
0 2 4 6
M12
r = 0.03, P = 0.84
0
2.5
5.0
0 2 4 6
M13
0
2.5
5.0 r = 0.02, P = 0.93
0 2 4 6
M14
0
1.0
2.0 r = 0.03, P = 0.88
0 2 4 6
M15
Plas
ma
AU
C0-
56h
(µM
·h)
r = 0.73, P < 0.011.207 (0.783, 1.630)
270 ml/subject180 ml/subject90 ml/subject
DoseFemaleMale
270 ml/subject180 ml/subject90 ml/subject
DoseFemaleMale
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
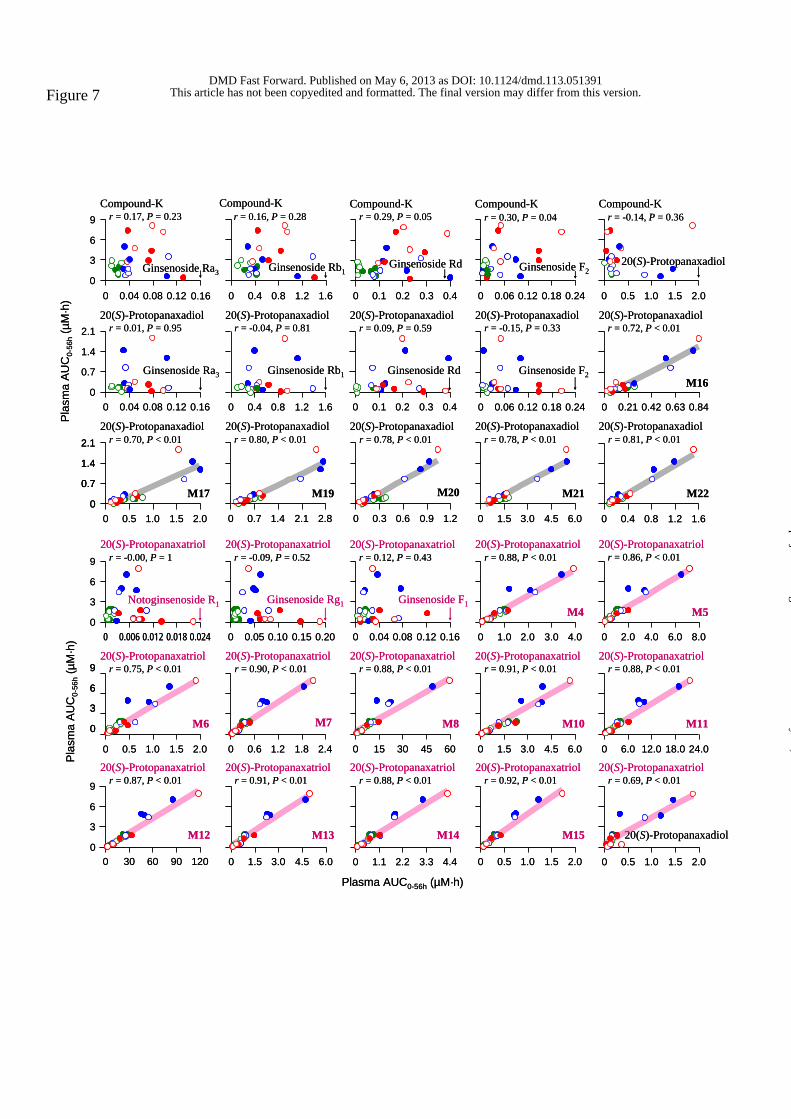
Figure 7
Ginsenoside Ra30
3
6
9
0 0.04 0.08 0.12 0.16
Compound-Kr = 0.17, P = 0.23
Pla
sma
AU
C0-
56h
(µM
·h)
0
0.7
1.4
2.1
0 0.5 1.0 1.5 2.0
r = 0.70, P < 0.0120(S)-Protopanaxadiol
M17
0 0.04 0.08 0.12 0.160
0.7
1.4
2.1 r = 0.01, P = 0.9520(S)-Protopanaxadiol
Ginsenoside Ra3
Ginsenoside Rb1
r = 0.16, P = 0.28Compound-K
0 0.4 0.8 1.2 1.6
0 0.7 1.4 2.1 2.8
r = 0.80, P < 0.0120(S)-Protopanaxadiol
M19
Ginsenoside Rd
0 0.1 0.2 0.3 0.4
r = 0.29, P = 0.05Compound-K
0 0.3 0.6 0.9 1.2
r = 0.78, P < 0.0120(S)-Protopanaxadiol
M20
0 0.1 0.2 0.3 0.4
r = 0.09, P = 0.5920(S)-Protopanaxadiol
Ginsenoside Rd
Ginsenoside F2
r = 0.30, P = 0.04
0 0.06 0.12 0.18 0.24
Compound-K
0 1.5 3.0 4.5 6.0
r = 0.78, P < 0.0120(S)-Protopanaxadiol
M21
r = -0.15, P = 0.33
0 0.06 0.12 0.18 0.24
20(S)-Protopanaxadiol
Ginsenoside F2
0 0.5 1.0 1.5 2.0
r = -0.14, P = 0.36Compound-K
20(S)-Protopanaxadiol
0 0.4 0.8 1.2 1.6
r = 0.81, P < 0.0120(S)-Protopanaxadiol
M22
0
3
6
9
0 30 60 90 120
r = 0.87, P < 0.01
M12
20(S)-Protopanaxatriol
0
3
6
9
0 0.5 1.0 1.5 2.0
r = 0.75, P < 0.01
M6
20(S)-Protopanaxatriol
r = -0.00, P = 1
0
3
6
9
0 0.006 0.012 0.018 0.024
Notoginsenoside R1
20(S)-Protopanaxatriol
0 1.5 3.0 4.5 6.0
r = 0.91, P < 0.01
M13
20(S)-Protopanaxatriol0 0.6 1.2 1.8 2.4
r = 0.90, P < 0.01
M7
20(S)-Protopanaxatriol
r = -0.09, P = 0.52
0 0.05 0.10 0.15 0.20
Ginsenoside Rg1
20(S)-Protopanaxatriol
0 1.1 2.2 3.3 4.4
r = 0.88, P < 0.01
M14
20(S)-Protopanaxatriol
Plasma AUC0-56h (µM·h)
0 15 30 45 60
r = 0.88, P < 0.01
M8
20(S)-Protopanaxatriol
r = 0.12, P = 0.43
0 0.04 0.08 0.12 0.16
Ginsenoside F1
20(S)-Protopanaxatriol
0 0.5 1.0 1.5 2.0
r = 0.92, P < 0.01
M15
20(S)-Protopanaxatriol0 1.5 3.0 4.5 6.0
r = 0.91, P < 0.01
M10
20(S)-Protopanaxatriol
0 1.0 2.0 3.0 4.0
r = 0.88, P < 0.01
M4
20(S)-Protopanaxatriol
0 0.5 1.0 1.5 2.0
r = 0.69, P < 0.01
20(S)-Protopanaxadiol
20(S)-Protopanaxatriol0 6.0 12.0 18.0 24.0
r = 0.88, P < 0.01
M11
20(S)-Protopanaxatriol
0 2.0 4.0 6.0 8.0
r = 0.86, P < 0.01
M5
20(S)-Protopanaxatriol
0 0.21 0.42 0.63 0.84
r = 0.72, P < 0.0120(S)-Protopanaxadiol
M16
0 0.4 0.8 1.2 1.6
r = -0.04, P = 0.8120(S)-Protopanaxadiol
Ginsenoside Rb1
Plas
ma
AU
C0-
56h
(µM
·h)
Ginsenoside Ra30
3
6
9
0 0.04 0.08 0.12 0.16
Compound-Kr = 0.17, P = 0.23
Pla
sma
AU
C0-
56h
(µM
·h)
0
0.7
1.4
2.1
0
0.7
1.4
2.1
0 0.5 1.0 1.5 2.0
r = 0.70, P < 0.0120(S)-Protopanaxadiol
M17
0 0.04 0.08 0.12 0.160
0.7
1.4
2.1 r = 0.01, P = 0.9520(S)-Protopanaxadiol
Ginsenoside Ra3
Ginsenoside Rb1
r = 0.16, P = 0.28Compound-K
0 0.4 0.8 1.2 1.6
0 0.7 1.4 2.1 2.8
r = 0.80, P < 0.0120(S)-Protopanaxadiol
M19
Ginsenoside Rd
0 0.1 0.2 0.3 0.4
r = 0.29, P = 0.05Compound-K
0 0.3 0.6 0.9 1.2
r = 0.78, P < 0.0120(S)-Protopanaxadiol
M20
0 0.1 0.2 0.3 0.4
r = 0.09, P = 0.5920(S)-Protopanaxadiol
Ginsenoside Rd
Ginsenoside F2
r = 0.30, P = 0.04
0 0.06 0.12 0.18 0.24
Compound-K
0 1.5 3.0 4.5 6.0
r = 0.78, P < 0.0120(S)-Protopanaxadiol
M21
r = -0.15, P = 0.33
0 0.06 0.12 0.18 0.24
20(S)-Protopanaxadiol
Ginsenoside F2
0 0.5 1.0 1.5 2.0
r = -0.14, P = 0.36Compound-K
20(S)-Protopanaxadiol
0 0.4 0.8 1.2 1.6
r = 0.81, P < 0.0120(S)-Protopanaxadiol
M22
0
3
6
9
0 30 60 90 120
r = 0.87, P < 0.01
M12
20(S)-Protopanaxatriol
0
3
6
9
0
3
6
9
0 0.5 1.0 1.5 2.0
r = 0.75, P < 0.01
M6
20(S)-Protopanaxatriol
r = -0.00, P = 1
0
3
6
9
0 0.006 0.012 0.018 0.024
Notoginsenoside R1
20(S)-Protopanaxatriol
0 1.5 3.0 4.5 6.0
r = 0.91, P < 0.01
M13
20(S)-Protopanaxatriol0 0.6 1.2 1.8 2.4
r = 0.90, P < 0.01
M7
20(S)-Protopanaxatriol
r = -0.09, P = 0.52
0 0.05 0.10 0.15 0.20
Ginsenoside Rg1
20(S)-Protopanaxatriol
0 1.1 2.2 3.3 4.4
r = 0.88, P < 0.01
M14
20(S)-Protopanaxatriol
Plasma AUC0-56h (µM·h)
0 15 30 45 60
r = 0.88, P < 0.01
M8
20(S)-Protopanaxatriol
r = 0.12, P = 0.43
0 0.04 0.08 0.12 0.16
Ginsenoside F1
20(S)-Protopanaxatriol
0 0.5 1.0 1.5 2.0
r = 0.92, P < 0.01
M15
20(S)-Protopanaxatriol0 1.5 3.0 4.5 6.0
r = 0.91, P < 0.01
M10
20(S)-Protopanaxatriol
0 1.0 2.0 3.0 4.0
r = 0.88, P < 0.01
M4
20(S)-Protopanaxatriol
0 0.5 1.0 1.5 2.0
r = 0.69, P < 0.01
20(S)-Protopanaxadiol
20(S)-Protopanaxatriol0 6.0 12.0 18.0 24.0
r = 0.88, P < 0.01
M11
20(S)-Protopanaxatriol
0 2.0 4.0 6.0 8.0
r = 0.86, P < 0.01
M5
20(S)-Protopanaxatriol
0 0.21 0.42 0.63 0.84
r = 0.72, P < 0.0120(S)-Protopanaxadiol
M16
0 0.4 0.8 1.2 1.6
r = -0.04, P = 0.8120(S)-Protopanaxadiol
Ginsenoside Rb1
Plas
ma
AU
C0-
56h
(µM
·h)
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from
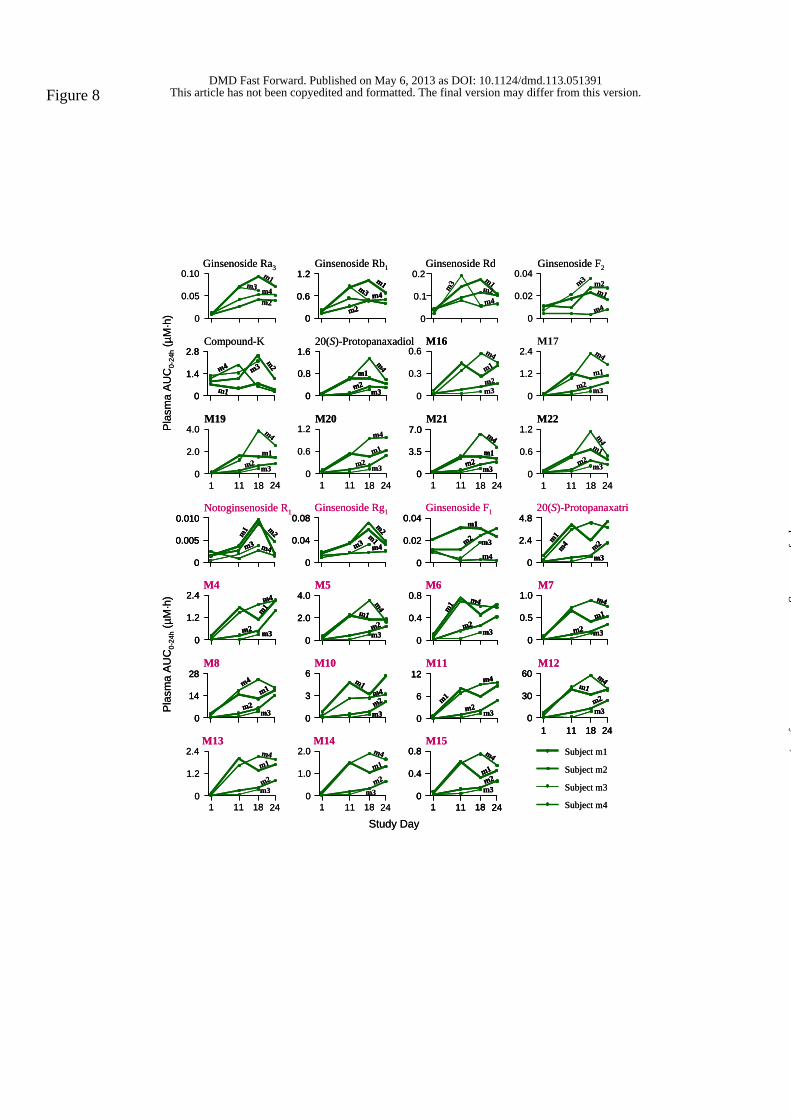
Figure 8
Study Day
M19
0.10
0.05
0
Compound-K
1.2
0.6
0
4.0
2.0
01 18 24
Ginsenoside Ra3
M132.0
1.0
0
2.4
1.2
011 18 24
M4
11
1
M20
Ginsenoside Rb10.2
0.1
0
M10
M5
0.6
0.3
0
1 18 24
M14
1 11 18 24
11
Ginsenoside Rd
M16
0.04
0
Ginsenoside F1
M6
2.4
1.2
0
1.2
0.6
0
M15
0.02
M22
Ginsenoside F2
M17
1 11 18 24
Subject m1
Subject m2
Subject m3
Subject m4
M7
Pla
sma
AU
C0-
24h
(µM
·h)
m1
m2
m4
m3
m1
m2
m4
m3
0.8
0.4
01 11 18 24
m1m2
m4
m3
6
3
0
m1
m2m4
m3
1.0
0.5
0
m1
m2
m4
m3
0.8
0.4
0
m1
m2
m4
m3
4.0
2.0
0
m1
m2
m4
m3
2.4
1.2
0
m1
m2
m4
m3
0.04
0.02
0
m2
m4
m1
m3
m1m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m4m2
m3m1m2m4
m3
m1m2
m4
m31.2
0.6
0
m1m4
m2
m3
2.8
1.4
0
m3
m2m4
m1
20(S)-Protopanaxadiol1.6
0.8
0
m1
m2
m4
m3
M217.0
3.5
0
m1m2
m4
m3
Notoginsenoside R10.010
0.005
0
m1
m4
m2
m3
Ginsenoside Rg10.08
0
0.04
m2
m1m4m3
20(S)-Protopanaxatrio4.8
2.4
0m1
m2m4m3
M828
14
0
m1
m2
m4
m3
M1112
6
0
m1m2
m4
m3
M1260
30
01 11 18 24
m1
m2
m4
m3
1 18 2411
Pla
sma
AU
C0-
24h
(µM
·h)
Study Day
M19
0.10
0.05
0
Compound-K
1.2
0.6
0
4.0
2.0
01 18 24
Ginsenoside Ra3
M132.0
1.0
0
2.4
1.2
011 18 24
M4
11
1
M20
Ginsenoside Rb10.2
0.1
0
M10
M5
0.6
0.3
0
1 18 24
M14
1 11 18 24
11
Ginsenoside Rd
M16
0.04
0
Ginsenoside F1
M6
2.4
1.2
0
1.2
0.6
0
M15
0.02
M22
Ginsenoside F2
M17
1 11 18 24
Subject m1
Subject m2
Subject m3
Subject m4
M7
Pla
sma
AU
C0-
24h
(µM
·h)
m1
m2
m4
m3
m1
m2
m4
m3
0.8
0.4
01 11 18 24
m1m2
m4
m3
0.8
0.4
01 11 18 24
m1m2
m4
m3
6
3
0
m1
m2m4
m3
6
3
0
m1
m2m4
m3
1.0
0.5
0
m1
m2
m4
m3
1.0
0.5
0
m1
m2
m4
m3
0.8
0.4
0
m1
m2
m4
m3
0.8
0.4
0
m1
m2
m4
m3
4.0
2.0
0
m1
m2
m4
m3
4.0
2.0
0
m1
m2
m4
m3
2.4
1.2
0
m1
m2
m4
m3
2.4
1.2
0
m1
m2
m4
m3
0.04
0.02
0
m2
m4
m1
m3
0.04
0.02
0
m2
m4
m1
m3
m1m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m2
m4
m3
m1
m4m2
m3m1m2m4
m3
m1m2
m4
m31.2
0.6
0
m1m4
m2
m3
1.2
0.6
0
m1m4
m2
m3
2.8
1.4
0
m3
m2m4
m1
2.8
1.4
0
m3
m2m4
m1
20(S)-Protopanaxadiol1.6
0.8
0
m1
m2
m4
m3
1.6
0.8
0
m1
m2
m4
m3
M217.0
3.5
0
m1m2
m4
m3
7.0
3.5
0
m1m2
m4
m3
Notoginsenoside R10.010
0.005
0
m1
m4
m2
m3
0.010
0.005
0
m1
m4
m2
m3
Ginsenoside Rg10.08
0
0.04
m2
m1m4m3
0.08
0
0.04
m2
m1m4m3
20(S)-Protopanaxatrio4.8
2.4
0m1
m2m4m3
4.8
2.4
0m1
m2m4m3
M828
14
0
m1
m2
m4
m3
28
14
0
m1
m2
m4
m3
M1112
6
0
m1m2
m4
m3
12
6
0
m1m2
m4
m3
M1260
30
01 11 18 24
m1
m2
m4
m3
60
30
01 11 18 24
m1
m2
m4
m3
1 18 2411
Pla
sma
AU
C0-
24h
(µM
·h)
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from

Figure 9
0
1.0
2.0
3.0
0 0.025 0.050 0.075 0.100
Compound-K
Plas
ma
AU
C0-
24h
(µM
·h)
r = -0.08, P = 0.69
Ginsenoside Ra3
0
0.5
1.0
1.5
0 0.6 1.2 1.8 2.4
r = 0.77, P < 0.0120(S)-Protopanaxadiol
M17
Ginsenoside Ra3
0
0.5
1.0
1.5
0 0.025 0.05 0.075 0.100
r = 0.45, P = 0.0320(S)-Protopanaxadiol
0 0.3 0.6 0.9 1.2
Compound-Kr = -0.07, P = 0.73
Ginsenoside Rb1
r = 0.03, P = 0.88
0 0.05 0.10 0.15 0.20
Compound-K
Ginsenoside Rd
0 0.01 0.02 0.03 0.04
Compound-Kr = 0.20, P = 0.30
Ginsenoside F2
0 1.0 2.0 3.0 4.0
r = 0.82, P < 0.0120(S)-Protopanaxadiol
M19
Ginsenoside Rb1
0 0.3 0.6 0.9 1.2
r = 0.44, P = 0.0420(S)-Protopanaxadiol
0 0.25 0.50 0.75 1.00
r = 0.69, P < 0.0120(S)-Protopanaxadiol
M20
0 0.05 0.10 0.15 0.20
r = 0.21, P = 0.3320(S)-Protopanaxadiol
Ginsenoside Rd
0 1.6 3.2 4.8 6.4
M21
r = 0.85, P < 0.0120(S)-Protopanaxadiol
0 0.01 0.02 0.03 0.04
r = -0.13, P = 0.5420(S)-Protopanaxadiol
Ginsenoside F2
0 0.4 0.8 1.2 1.6
Compound-Kr = -0.21, P = 0.33
20(S)-Protopanaxadiol
0 0.3 0.6 0.9 1.2
M22
r = 0.97, P < 0.0120(S)-Protopanaxadiol
0 0.15 0.30 0.45 0.60
M16
r = 0.74, P < 0.0120(S)-Protopanaxadiol
0 2.5 5.0 7.5 10
r = 0.83, P < 0.01
20(S)-Protopanaxatriol
M11
0 0.4 0.8 1.2 1.6
r = 0.64, P < 0.0120(S)-Protopanaxatriol
20(S)-Protopanaxadiol
0 1.0 2.0 3.0 4.0
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M5
0
1.6
3.2
4.8
0 0.2 0.4 0.6 0.8
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M6
0
1.6
3.2
4.8
0 15 30 45 60
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M12
0
1.6
3.2
4.8
0 0.0025 0.005 0.0075 0.01
r = 0.18, P = 0.3520(S)-Protopanaxatriol
Notoginsenoside R1
Plasma AUC0-24h (µM·h)
0 0.25 0.50 0.75 1.00
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M7
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.01
M13
20(S)-Protopanaxatriol
0 0.02 0.04 0.06 0.08
r = 0.21, P = 0.2820(S)-Protopanaxatriol
Ginsenoside Rg1
0 7 14 21 28
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M8
0 0.5 1.0 1.5 2.0
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M14
0 0.01 0.02 0.03 0.04
r = 0.26, P = 0.1820(S)-Protopanaxatriol
Ginsenoside F1
0 1.6 3.2 4.8 6.4
r = 0.89, P < 0.0120(S)-Protopanaxatriol
M10
0 0.2 0.4 0.6 0.8
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M15
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.0120(S)-Protopanaxatriol
M4
Plas
ma
AUC
0-24
h(µ
M·h
)
0
1.0
2.0
3.0
0 0.025 0.050 0.075 0.100
Compound-K
Plas
ma
AU
C0-
24h
(µM
·h)
r = -0.08, P = 0.69
Ginsenoside Ra3
0
0.5
1.0
1.5
0 0.6 1.2 1.8 2.4
r = 0.77, P < 0.0120(S)-Protopanaxadiol
M17
Ginsenoside Ra3
0
0.5
1.0
1.5
0 0.025 0.05 0.075 0.100
r = 0.45, P = 0.0320(S)-Protopanaxadiol
0 0.3 0.6 0.9 1.2
Compound-Kr = -0.07, P = 0.73
Ginsenoside Rb1
r = 0.03, P = 0.88
0 0.05 0.10 0.15 0.20
Compound-K
Ginsenoside Rd
0 0.01 0.02 0.03 0.04
Compound-Kr = 0.20, P = 0.30
Ginsenoside F2
0 1.0 2.0 3.0 4.0
r = 0.82, P < 0.0120(S)-Protopanaxadiol
M19
Ginsenoside Rb1
0 0.3 0.6 0.9 1.2
r = 0.44, P = 0.0420(S)-Protopanaxadiol
0 0.25 0.50 0.75 1.00
r = 0.69, P < 0.0120(S)-Protopanaxadiol
M20
0 0.05 0.10 0.15 0.20
r = 0.21, P = 0.3320(S)-Protopanaxadiol
Ginsenoside Rd
0 1.6 3.2 4.8 6.4
M21
r = 0.85, P < 0.0120(S)-Protopanaxadiol
0 0.01 0.02 0.03 0.04
r = -0.13, P = 0.5420(S)-Protopanaxadiol
Ginsenoside F2
0 0.4 0.8 1.2 1.6
Compound-Kr = -0.21, P = 0.33
20(S)-Protopanaxadiol
0 0.3 0.6 0.9 1.2
M22
r = 0.97, P < 0.0120(S)-Protopanaxadiol
0 0.15 0.30 0.45 0.60
M16
r = 0.74, P < 0.0120(S)-Protopanaxadiol
0 2.5 5.0 7.5 10
r = 0.83, P < 0.01
20(S)-Protopanaxatriol
M11
0 0.4 0.8 1.2 1.6
r = 0.64, P < 0.0120(S)-Protopanaxatriol
20(S)-Protopanaxadiol
0 1.0 2.0 3.0 4.0
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M5
0 2.5 5.0 7.5 10
r = 0.83, P < 0.01
20(S)-Protopanaxatriol
M11
0 0.4 0.8 1.2 1.6
r = 0.64, P < 0.0120(S)-Protopanaxatriol
20(S)-Protopanaxadiol
0 1.0 2.0 3.0 4.0
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M5
0
1.6
3.2
4.8
0 0.2 0.4 0.6 0.8
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M6
0
1.6
3.2
4.8
0 15 30 45 60
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M12
0
1.6
3.2
4.8
0 0.0025 0.005 0.0075 0.01
r = 0.18, P = 0.3520(S)-Protopanaxatriol
Notoginsenoside R1
Plasma AUC0-24h (µM·h)
0 0.25 0.50 0.75 1.00
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M7
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.01
M13
20(S)-Protopanaxatriol
0 0.02 0.04 0.06 0.08
r = 0.21, P = 0.2820(S)-Protopanaxatriol
Ginsenoside Rg1
0 7 14 21 28
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M8
0 0.5 1.0 1.5 2.0
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M14
0 0.01 0.02 0.03 0.04
r = 0.26, P = 0.1820(S)-Protopanaxatriol
Ginsenoside F1
0 1.6 3.2 4.8 6.4
r = 0.89, P < 0.0120(S)-Protopanaxatriol
M10
0 0.2 0.4 0.6 0.8
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M15
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.0120(S)-Protopanaxatriol
M4
0
1.6
3.2
4.8
0 0.2 0.4 0.6 0.8
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M6
0
1.6
3.2
4.8
0 15 30 45 60
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M12
0
1.6
3.2
4.8
0 0.0025 0.005 0.0075 0.01
r = 0.18, P = 0.3520(S)-Protopanaxatriol
Notoginsenoside R1
Plasma AUC0-24h (µM·h)
0 0.25 0.50 0.75 1.00
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M7
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.01
M13
20(S)-Protopanaxatriol
0 0.02 0.04 0.06 0.08
r = 0.21, P = 0.2820(S)-Protopanaxatriol
Ginsenoside Rg1
0 7 14 21 28
r = 0.85, P < 0.0120(S)-Protopanaxatriol
M8
0 0.5 1.0 1.5 2.0
r = 0.83, P < 0.0120(S)-Protopanaxatriol
M14
0 0.01 0.02 0.03 0.04
r = 0.26, P = 0.1820(S)-Protopanaxatriol
Ginsenoside F1
0 1.6 3.2 4.8 6.4
r = 0.89, P < 0.0120(S)-Protopanaxatriol
M10
0 0.2 0.4 0.6 0.8
r = 0.81, P < 0.0120(S)-Protopanaxatriol
M15
0 0.6 1.2 1.8 2.4
r = 0.87, P < 0.0120(S)-Protopanaxatriol
M4
Plas
ma
AUC
0-24
h(µ
M·h
)
This article has not been copyedited and formatted. The final version may differ from this version.DMD Fast Forward. Published on May 6, 2013 as DOI: 10.1124/dmd.113.051391
at ASPE
T Journals on July 29, 2018
dmd.aspetjournals.org
Dow
nloaded from


















