Colon, Anus, Rectum
102
Colon, Anus, Rectum
description
Colon, Anus, Rectum. Random animal/human evacuating bowels. Embryology and Anatomy. Embryology Starts the fourth week of gestation derived from the endoderm three segments: foregut, midgut, and hindgut midgut and hindgut contribute to the colon, rectum, and anus - PowerPoint PPT Presentation
Transcript of Colon, Anus, Rectum

Colon, Anus, Rectum

Random animal/human Random animal/human evacuating bowelsevacuating bowels

Embryology and Embryology and AnatomyAnatomy
EmbryologyEmbryology Starts the fourth week of gestation Starts the fourth week of gestation derived from the endoderm derived from the endoderm three segments: foregut, midgut, and hindgutthree segments: foregut, midgut, and hindgut midgut and hindgut contribute to the colon, rectum, and midgut and hindgut contribute to the colon, rectum, and
anusanus Hindgut - distal transverse colon, descending colon, rectum, Hindgut - distal transverse colon, descending colon, rectum,
and proximal anus all blood supply from IMAand proximal anus all blood supply from IMA
AnatomyAnatomy anatomically and functionally divided into the colon, anatomically and functionally divided into the colon,
rectum, and anal canalrectum, and anal canal five distinct layers: mucosa, submucosa, inner circular five distinct layers: mucosa, submucosa, inner circular
muscle, outer longitudinal muscle (tenea coli), and serosa muscle, outer longitudinal muscle (tenea coli), and serosa (not present in mid and lower rectum)(not present in mid and lower rectum)

ColonColon Terminal ileum 3 to 5 ft to the rectumTerminal ileum 3 to 5 ft to the rectum Rectosigmoid junction (level of the sacral Rectosigmoid junction (level of the sacral
promontory) point at which the three promontory) point at which the three teniae coli coalesce teniae coli coalesce
Cecum is the widest diameter (normally Cecum is the widest diameter (normally 7.5 to 8.5 cm) and thinnest muscular wall 7.5 to 8.5 cm) and thinnest muscular wall (set up to perf) (set up to perf)
Sigmoid colon has a narrow caliber, Sigmoid colon has a narrow caliber, making it the most vulnerable to making it the most vulnerable to obstructionobstruction

Arterial SupplyArterial Supply
SMASMA - - Ileocolic artery (absent in up to 20% of people), Ileocolic artery (absent in up to 20% of people),
terminal ileum and proximal ascending colonterminal ileum and proximal ascending colon Right colic artery - ascending colon Right colic artery - ascending colon Middle colic artery - transverse colon Middle colic artery - transverse colon
IMAIMA - - Left colic artery - descending colon Left colic artery - descending colon Sigmoidal branches - sigmoid colon Sigmoidal branches - sigmoid colon Superior rectal artery - proximal rectum Superior rectal artery - proximal rectum Communicate via the marginal artery of Communicate via the marginal artery of
Drummond, complete in only 15 to 20% of Drummond, complete in only 15 to 20% of peoplepeople


Veins, Lymphatics, and Veins, Lymphatics, and InnervationInnervation
VeinsVeins Veins of the colon parallel their corresponding arteries (except IMV) and Veins of the colon parallel their corresponding arteries (except IMV) and
bear the same terminology bear the same terminology Inferior mesenteric vein ascends in the retroperitoneal plane over the Inferior mesenteric vein ascends in the retroperitoneal plane over the
psoas muscle, posterior to the pancreas to join the splenic vein. (During a psoas muscle, posterior to the pancreas to join the splenic vein. (During a colectomy, mobilized independently and ligated at the inferior edge of the colectomy, mobilized independently and ligated at the inferior edge of the pancreas)pancreas)
Lymphatic DrainageLymphatic Drainage Muscularis mucosa -> follow the regional arteries. Lymph nodes are found Muscularis mucosa -> follow the regional arteries. Lymph nodes are found
on the bowel wall (epicolic), along the inner margin of the bowel adjacent on the bowel wall (epicolic), along the inner margin of the bowel adjacent to the arterial arcades (paracolic), around the named mesenteric vessels to the arterial arcades (paracolic), around the named mesenteric vessels (intermediate), and at the origin of the superior and inferior mesenteric (intermediate), and at the origin of the superior and inferior mesenteric arteries (main). arteries (main).
Nerve SupplyNerve Supply Sympathetic (inhibitory) and parasympathetic (stimulatory) nerves, which Sympathetic (inhibitory) and parasympathetic (stimulatory) nerves, which
parallel the course of the arteries. Sympathetic nerves arise from T6–T12 parallel the course of the arteries. Sympathetic nerves arise from T6–T12 and L1–L3. Vagus nerve ->parasympathetic innervation to the right and and L1–L3. Vagus nerve ->parasympathetic innervation to the right and transverse colon; parasympathetic nerves to the left colon arise from transverse colon; parasympathetic nerves to the left colon arise from sacral nerves S2–S4 to form the nervi erigentes.sacral nerves S2–S4 to form the nervi erigentes.

AnorectalAnorectal
Rectum -12 to 15 cm in lengthRectum -12 to 15 cm in length Valves of Houston - three distinct submucosal folds Valves of Houston - three distinct submucosal folds Posteriorly -presacral fascia, Posteriorly -presacral fascia, Anteriorly - Denonvilliers' fascia Anteriorly - Denonvilliers' fascia Lateral ligaments support the lower rectumLateral ligaments support the lower rectum Surgical anal canal measures 2 to 4 cm (anorectal junction to anal Surgical anal canal measures 2 to 4 cm (anorectal junction to anal
verge) verge) Dentate or pectinate line transition columnar rectal mucosa and Dentate or pectinate line transition columnar rectal mucosa and
squamous anoderm, surrounded by longitudinal mucosal folds, squamous anoderm, surrounded by longitudinal mucosal folds, known as the columns of Morgagni, (anal crypts empty here, source known as the columns of Morgagni, (anal crypts empty here, source of cryptoglandular abscesses) of cryptoglandular abscesses)
Inner smooth muscle is thickened and comprises the internal anal Inner smooth muscle is thickened and comprises the internal anal sphincter sphincter
Deep external anal sphincter is an extension of the puborectalis Deep external anal sphincter is an extension of the puborectalis muscle muscle
Puborectalis, iliococcygeus, and pubococcygeusmuscles form the Puborectalis, iliococcygeus, and pubococcygeusmuscles form the levator ani musclelevator ani muscle


Anorectal Vascular SupplyAnorectal Vascular Supply
Superior rectal artery <- inferior Superior rectal artery <- inferior mesenteric artery (upper rectum) mesenteric artery (upper rectum)
Middle rectal artery <- internal iliacMiddle rectal artery <- internal iliac Inferior rectal artery <- internal Inferior rectal artery <- internal
pudendal <- internal iliac artery. pudendal <- internal iliac artery. Rich collaterals Rich collaterals

Veins and LymphaticsVeins and Lymphatics
VenousVenous Superior rectal vein -> inferior mesenteric -> portal system Superior rectal vein -> inferior mesenteric -> portal system Middle rectal vein -> internal iliac vein Middle rectal vein -> internal iliac vein Inferior rectal vein -> internal pudendal vein -> internal iliac veinInferior rectal vein -> internal pudendal vein -> internal iliac vein Submucosal plexus deep to the columns of Morgagni forms the Submucosal plexus deep to the columns of Morgagni forms the
hemorrhoidal plexus and drains into all three veins.hemorrhoidal plexus and drains into all three veins.Anorectal Lymphatic DrainageAnorectal Lymphatic Drainage Parallels the vascular supplyParallels the vascular supply Upper and middle rectum -> inferior mesenteric nodes Upper and middle rectum -> inferior mesenteric nodes Lower rectum -> inferior mesenteric Lower rectum -> inferior mesenteric andand internal iliac nodes internal iliac nodesAnal canal Anal canal Proximal to the dentate line -> inferior mesenteric and internal Proximal to the dentate line -> inferior mesenteric and internal
iliac nodes iliac nodes Distal -> inguinal nodes, inferior mesenteric and internal iliac Distal -> inguinal nodes, inferior mesenteric and internal iliac
nodesnodes


Anorectal Nerve SupplyAnorectal Nerve Supply
Sympathetic - L1–L3 -> preaortic plexus -> Sympathetic - L1–L3 -> preaortic plexus -> hypogastric plexus combine with ->hypogastric plexus combine with ->
Parasympathetic (nervi erigentes) S2–S4 to form the Parasympathetic (nervi erigentes) S2–S4 to form the pelvic plexus. pelvic plexus.
Sympathetic and parasympathetic fibers then supply Sympathetic and parasympathetic fibers then supply the anorectum and adjacent urogenital organs.the anorectum and adjacent urogenital organs.
The internal anal sphincter is innervated by The internal anal sphincter is innervated by sympathetic and parasympathetic nerve fibers; both sympathetic and parasympathetic nerve fibers; both inhibit sphincter contraction. inhibit sphincter contraction.
The external anal sphincter and puborectalis The external anal sphincter and puborectalis muscles are innervated by the inferior rectal branch muscles are innervated by the inferior rectal branch of the internal pudendal nerve. of the internal pudendal nerve.

Normal Physiology Normal Physiology
Fluid and Electrolyte ExchangesFluid and Electrolyte Exchanges The colon is a major site for water absorption and electrolyte The colon is a major site for water absorption and electrolyte
exchange. exchange. 90% of the water contained in ileal fluid is absorbed in the 90% of the water contained in ileal fluid is absorbed in the
colon (1000 to 2000 mL/d), and up to 5000 mL of fluid can be colon (1000 to 2000 mL/d), and up to 5000 mL of fluid can be absorbed daily absorbed daily
Sodium is absorbed actively via a Na-K ATPase. The colon can Sodium is absorbed actively via a Na-K ATPase. The colon can absorb up to 400 mEq of sodium per day. absorb up to 400 mEq of sodium per day.
Water accompanies the transported sodium and is absorbed Water accompanies the transported sodium and is absorbed passively along an osmotic gradient. passively along an osmotic gradient.
Potassium is actively secreted Potassium is actively secreted Chloride is absorbed actively via a chloride–bicarbonate Chloride is absorbed actively via a chloride–bicarbonate
exchange.exchange. Bacterial degradation of protein and urea produces ammonia. Bacterial degradation of protein and urea produces ammonia.
Ammonia is subsequently absorbed and transported to the Ammonia is subsequently absorbed and transported to the liver. liver.

Colonic Microflora and Colonic Microflora and Intestinal GasIntestinal Gas
Approximately 30% of fecal dry weight is composed of Approximately 30% of fecal dry weight is composed of bacteria (1011 to 102 bacteria/g of feces). bacteria (1011 to 102 bacteria/g of feces).
Anaerobes predominant Anaerobes predominant Bacteroides species are the most common (1011 to 1012 Bacteroides species are the most common (1011 to 1012
organisms/mL) > Escherichia coli are the most numerous organisms/mL) > Escherichia coli are the most numerous aerobes (108 to 1010 organisms/mL). Breakdown of carbs, aerobes (108 to 1010 organisms/mL). Breakdown of carbs, bilirubin, etc. bilirubin, etc.
Short-chain fatty acids (acetate, butyrate, and propionate) Short-chain fatty acids (acetate, butyrate, and propionate) are produced by bacterial fermentation of dietary are produced by bacterial fermentation of dietary carbohydrates, lack may result in mucosal atrophy and carbohydrates, lack may result in mucosal atrophy and "diversion colitis.""diversion colitis."
Produce vitamin K.Produce vitamin K. Hold off Clostridium difficile and other invadersHold off Clostridium difficile and other invaders Intestinal gas arises from swallowed air, diffusion from the Intestinal gas arises from swallowed air, diffusion from the
blood, and intraluminal production. blood, and intraluminal production.


MotilityMotility No cyclic motor activity characteristic of the migratory motor complex. Instead, the No cyclic motor activity characteristic of the migratory motor complex. Instead, the
colon displays intermittent contractions of either low (delay colonic transit) or high colon displays intermittent contractions of either low (delay colonic transit) or high amplitude (move contents). amplitude (move contents).
DefecationDefecation Distention of the rectum causes a reflex relaxation of the internal anal sphincter (the Distention of the rectum causes a reflex relaxation of the internal anal sphincter (the
rectoanal inhibitory reflex) that allows the contents to make contact with the anal rectoanal inhibitory reflex) that allows the contents to make contact with the anal canal. This "sampling reflex" allows the sensory epithelium to distinguish solid stool canal. This "sampling reflex" allows the sensory epithelium to distinguish solid stool from liquid stool and gas. from liquid stool and gas.
Coordination of increasing intra-abdominal pressure via the Valsalva maneuver, Coordination of increasing intra-abdominal pressure via the Valsalva maneuver, increased rectal contraction, relaxation of the puborectalis muscle, and opening of increased rectal contraction, relaxation of the puborectalis muscle, and opening of the anal canal.the anal canal.
ContinenceContinence At rest, the puborectalis muscle creates a "sling" around the distal rectum, forming a At rest, the puborectalis muscle creates a "sling" around the distal rectum, forming a
relatively acute angle that distributes intra-abdominal forces onto the pelvic floor. relatively acute angle that distributes intra-abdominal forces onto the pelvic floor. With defecation, this angle straightens, allowing downward force to be applied along With defecation, this angle straightens, allowing downward force to be applied along the axis of the rectum and anal canal. the axis of the rectum and anal canal.
Internal sphincter is responsible for most of the resting, involuntary sphincter tone Internal sphincter is responsible for most of the resting, involuntary sphincter tone (resting pressure). (resting pressure).
External sphincter is responsible for most of the voluntary sphincter tone (squeeze External sphincter is responsible for most of the voluntary sphincter tone (squeeze pressure). pressure).
Branches of the pudendal nerve innervate both the internal and external sphincter. Branches of the pudendal nerve innervate both the internal and external sphincter.

Tools of the TradeTools of the Trade
AnoscopyAnoscopy Anal canal. Anal canal. 8cm but variable 8cm but variable Anal procedures such as rubber band ligation or sclerotherapy of hemorrhoidsAnal procedures such as rubber band ligation or sclerotherapy of hemorrhoidsProctoscopyProctoscopy Rectum and distal sigmoid colon Rectum and distal sigmoid colon 25 cm in length. 25 cm in length. Polypectomy, electrocoagulation, or detorsion of a sigmoid volvulusPolypectomy, electrocoagulation, or detorsion of a sigmoid volvulusFlexible Sigmoidoscopy Flexible Sigmoidoscopy Colon and rectum (to splenic flexure)Colon and rectum (to splenic flexure) 60 cm in length 60 cm in length Colonoscopes Colonoscopes 100 to 160 cm in length 100 to 160 cm in length Entire colon and terminal ileumEntire colon and terminal ileum Bowel preparation, conscious sedationBowel preparation, conscious sedationCapsule EndoscopyCapsule Endoscopy Images transmitted by radiofrequencyImages transmitted by radiofrequency Primarily small bowel lesions Primarily small bowel lesions

ImagingImaging
Plain X-Rays and Contrast StudiesPlain X-Rays and Contrast Studies Free intra-abdominal air, bowel gas patterns suggestive of small or large bowel Free intra-abdominal air, bowel gas patterns suggestive of small or large bowel
obstruction, and volvulus. obstruction, and volvulus. Contrast studies are useful for evaluating obstructive symptoms, delineating fistulous Contrast studies are useful for evaluating obstructive symptoms, delineating fistulous
tracts, and diagnosing small perforations or anastomotic leaks. tracts, and diagnosing small perforations or anastomotic leaks. Gastrografin –less detail, water soluble, use if perforation Gastrografin –less detail, water soluble, use if perforation Double-contrast barium enema 70 to 90% sensitive for the detection of mass lesions Double-contrast barium enema 70 to 90% sensitive for the detection of mass lesions
greater than 1 cm in diameter. (back-up examination if colonoscopy is incomplete)greater than 1 cm in diameter. (back-up examination if colonoscopy is incomplete)Computed TomographyComputed Tomography Good for extraluminal diseaseGood for extraluminal disease Perforation or anastomotic leak, nonspecific findings such as bowel wall thickening or Perforation or anastomotic leak, nonspecific findings such as bowel wall thickening or
mesenteric stranding may suggest inflammatory bowel disease, enteritis/colitis, or mesenteric stranding may suggest inflammatory bowel disease, enteritis/colitis, or ischemia..ischemia..
Not good for intraluminal pathologyNot good for intraluminal pathologyVirtual Colonoscopy/Computed Tomography ColographyVirtual Colonoscopy/Computed Tomography Colography Helical CT and three-dimensional reconstruction to detect intraluminal colonic lesions. Oral Helical CT and three-dimensional reconstruction to detect intraluminal colonic lesions. Oral
bowel preparation, oral and rectal contrast, and colon insufflation bowel preparation, oral and rectal contrast, and colon insufflation Approaches colonoscopy’s sensitivityApproaches colonoscopy’s sensitivityMagnetic Resonance ImagingMagnetic Resonance Imaging Detecting bony involvement or pelvic sidewall extension of rectal tumors, determines the Detecting bony involvement or pelvic sidewall extension of rectal tumors, determines the
extent of spread of rectal cancer into adjacent structuresextent of spread of rectal cancer into adjacent structures Detection and delineation of complex fistulas in anoDetection and delineation of complex fistulas in ano


ImagingImaging
Positron Emission TomographyPositron Emission Tomography Imaging tissues with high levels of anaerobic glycolysis Imaging tissues with high levels of anaerobic glycolysis
(malignant tumors)(malignant tumors) F-fluorodeoxyglucose F-fluorodeoxyglucose Adjunct to CT in the staging of colorectal Adjunct to CT in the staging of colorectal AngiographyAngiography Detection of bleeding within the colon or small bowel. Detection of bleeding within the colon or small bowel. Must be relatively brisk (approximately 0.5 to 1.0 mL per Must be relatively brisk (approximately 0.5 to 1.0 mL per
minute)minute) If identified, infusion of vasopressin or angiographic If identified, infusion of vasopressin or angiographic
embolization can be therapeutic. embolization can be therapeutic. Endorectal UltrasoundEndorectal Ultrasound Evaluate the depth of invasion of neoplastic lesions in the Evaluate the depth of invasion of neoplastic lesions in the
rectum. rectum. Can detect enlarged perirectal lymph nodesCan detect enlarged perirectal lymph nodes

Laboratory StudiesLaboratory Studies
Fecal Occult Blood TestingFecal Occult Blood Testing Screening test for colonic neoplasms in asymptomatic, average-risk Screening test for colonic neoplasms in asymptomatic, average-risk
individuals. individuals. Serial testing, colorectal malignancies will bleed intermittentlySerial testing, colorectal malignancies will bleed intermittently Red meat, some fruits and vegetables, and vitamin C will produce a Red meat, some fruits and vegetables, and vitamin C will produce a
false-positive resultfalse-positive result Any positive FOBT mandates further investigation, usually by Any positive FOBT mandates further investigation, usually by
colonoscopy.colonoscopy.Stool StudiesStool Studies Stool studies often are helpful in evaluating the etiology of diarrhea. Stool studies often are helpful in evaluating the etiology of diarrhea. Wet-mount - fecal leukocytes <- colonic inflammation or the Wet-mount - fecal leukocytes <- colonic inflammation or the
presence of an invasive organism such as invasive E. coli or Shigella. presence of an invasive organism such as invasive E. coli or Shigella. Stool cultures can detect pathogenic bacteria, ova, and parasites. Stool cultures can detect pathogenic bacteria, ova, and parasites. C. difficile colitis is diagnosed by detecting bacterial toxin or PCRC. difficile colitis is diagnosed by detecting bacterial toxin or PCR Steatorrhea may be diagnosed by adding Sudan red stain to a stool Steatorrhea may be diagnosed by adding Sudan red stain to a stool
sample.sample.

Tumor MarkersTumor Markers
Carcinoembryonic antigen (CEA) 60 Carcinoembryonic antigen (CEA) 60 to 90% with colorectal cancerto 90% with colorectal cancer
Not an effective screening tool Not an effective screening tool Follow to detect early recurrence of Follow to detect early recurrence of
colorectal cancercolorectal cancer No survival benefit has yet been No survival benefit has yet been
proven. proven.

Pain!!!!!!!!!!Pain!!!!!!!!!!Abdominal painAbdominal pain Differential: obstruction (either inflammatory or neoplastic), inflammation, Differential: obstruction (either inflammatory or neoplastic), inflammation,
perforation, or ischemia. perforation, or ischemia. Plain x-rays and judicious use of contrast studies and/or a CT Plain x-rays and judicious use of contrast studies and/or a CT Gentle retrograde contrast studies (barium or Gastrografin enema) Gentle retrograde contrast studies (barium or Gastrografin enema)
sigmoidoscopy and/or colonoscopy (ischemic colitis, infectious colitis, and sigmoidoscopy and/or colonoscopy (ischemic colitis, infectious colitis, and inflammatory bowel disease) inflammatory bowel disease)
Pelvic pain Pelvic pain Distal colon and rectum or from adjacent urogenital structures. Distal colon and rectum or from adjacent urogenital structures. Tenesmus may result from proctitis or from a rectal or retrorectal mass. Tenesmus may result from proctitis or from a rectal or retrorectal mass. Cyclical pain associated with menses= endometriosis. Cyclical pain associated with menses= endometriosis. Pelvic inflammatory peridiverticular abscess or periappendiceal abscess Pelvic inflammatory peridiverticular abscess or periappendiceal abscess
into the pelvis may also cause pain. into the pelvis may also cause pain. CT scan and/or MRI, proctoscopy, laparoscopyCT scan and/or MRI, proctoscopy, laparoscopyAnorectal pain Anorectal pain Most often anal fissure, perirectal abscess and/or fistula, or a thrombosed Most often anal fissure, perirectal abscess and/or fistula, or a thrombosed
hemorrhoid >> anal canal neoplasms, perianal skin infection. hemorrhoid >> anal canal neoplasms, perianal skin infection. Proctalgia fugax results from levator spasm Proctalgia fugax results from levator spasm Physical examination is key, (DRE)Physical examination is key, (DRE)

Lower Gastrointestinal Lower Gastrointestinal BleedingBleeding
ABCs and adequate resuscitation. ABCs and adequate resuscitation. Correct coagulopathy and/or thrombocytopenia Correct coagulopathy and/or thrombocytopenia Most common source of GI hemorrhage is upper GI: esophageal, gastric, Most common source of GI hemorrhage is upper GI: esophageal, gastric,
or duodenal, so or duodenal, so nasogastric aspirationnasogastric aspiration should always be performed should always be performed Not negative unless return of bileNot negative unless return of bile suggests that the source of suggests that the source of
bleeding is distal to the ligament of Treitz.bleeding is distal to the ligament of Treitz. EGD if not negative EGD if not negative Anoscopy and/or limited proctoscopy for hemorrhoidal bleeding. Anoscopy and/or limited proctoscopy for hemorrhoidal bleeding. Technetium-99–tagged red blood cell scan is extremely sensitive and is Technetium-99–tagged red blood cell scan is extremely sensitive and is
able to detect as little as 0.1 mL/h of bleeding but imprecise.able to detect as little as 0.1 mL/h of bleeding but imprecise. Angiography, vasopressin or angioembolization may be Angiography, vasopressin or angioembolization may be
therapeutic, catheter can be left in the bleeding vessel to allow therapeutic, catheter can be left in the bleeding vessel to allow localization at the time of laparotomy. localization at the time of laparotomy.
Colonoscopy if stable, cautery or injection of epinephrine Colonoscopy if stable, cautery or injection of epinephrine Colectomy may be required if bleeding persists, segmental resection is Colectomy may be required if bleeding persists, segmental resection is
preferred if the bleeding source can be localized. preferred if the bleeding source can be localized. "Blind" subtotal colectomy may very rarely be required, must r/o rectal "Blind" subtotal colectomy may very rarely be required, must r/o rectal
sourcesource

Occult Blood Loss Occult Blood Loss
Presents as iron-deficiency anemia or + Presents as iron-deficiency anemia or + FOBT, if positive do colonoscopyFOBT, if positive do colonoscopy
Neoplasms bleed intermittentlyNeoplasms bleed intermittently Hematochezia -> hemorrhoids (painless Hematochezia -> hemorrhoids (painless
(internal), bright-red rectal bleeding with (internal), bright-red rectal bleeding with bowel movements) or fissure (sharp, knife-bowel movements) or fissure (sharp, knife-like pain and bright-red rectal bleeding like pain and bright-red rectal bleeding with bowel movements) with bowel movements)
Digital rectal examination, anoscopy, and Digital rectal examination, anoscopy, and proctosigmoidoscopy, if nothing found, do proctosigmoidoscopy, if nothing found, do colonoscopy. colonoscopy.


Constipation and Obstructed Constipation and Obstructed DefecationDefecation
Extremely common (4 million in U.S.A.) Extremely common (4 million in U.S.A.) Metabolic, pharmacologic, endocrine, psychological, and Metabolic, pharmacologic, endocrine, psychological, and
neurologic contribute neurologic contribute Exclude stricture or mass lesion by colonoscopy or barium enemaExclude stricture or mass lesion by colonoscopy or barium enema Evaluation focuses on differentiating slow-transit constipation Evaluation focuses on differentiating slow-transit constipation
(radiopaque markers) from outlet obstruction (anorectal (radiopaque markers) from outlet obstruction (anorectal manometry and EMG of the puborectalis) manometry and EMG of the puborectalis)
Defecography can identify rectal prolapse, intussusception, Defecography can identify rectal prolapse, intussusception, rectocele, or enterocele.rectocele, or enterocele.
Medical management is the mainstay: fiber, increased fluid Medical management is the mainstay: fiber, increased fluid intake, and laxativesintake, and laxatives
Outlet obstruction -> biofeedbackOutlet obstruction -> biofeedback Subtotal colectomy is considered only for patients with severe Subtotal colectomy is considered only for patients with severe
slow-transit constipation (colonic inertia) refractory to maximal slow-transit constipation (colonic inertia) refractory to maximal medical interventions -> complaints of diarrhea, incontinence, medical interventions -> complaints of diarrhea, incontinence, and abdominal pain.and abdominal pain.

DiarrheaDiarrhea
Further investigation is warranted if diarrhea is Further investigation is warranted if diarrhea is chronic or is accompanied by bleeding (colitis) chronic or is accompanied by bleeding (colitis) or abdominal pain or abdominal pain
Infection (invasive E. coli, Shigella, Salmonella, Infection (invasive E. coli, Shigella, Salmonella, Campylobacter, Entamoeba histolytica, or C. Campylobacter, Entamoeba histolytica, or C. difficile) ->stool wet-mount and culture difficile) ->stool wet-mount and culture
Inflammatory bowel disease (ulcerative colitis Inflammatory bowel disease (ulcerative colitis or Crohn's colitis) -> scopeor Crohn's colitis) -> scope
Ischemia -> scope (if stable)Ischemia -> scope (if stable)

Chronic diarrhea Chronic diarrhea
Chronic ulcerative colitis, Crohn's colitis, Chronic ulcerative colitis, Crohn's colitis, infection, malabsorption, and short-gut infection, malabsorption, and short-gut syndrome can cause chronic diarrhea. syndrome can cause chronic diarrhea.
Carcinoid syndrome and islet cell Carcinoid syndrome and islet cell tumors (VIP, somatostatinoma, tumors (VIP, somatostatinoma, gastrinoma), large villous lesionsgastrinoma), large villous lesions
Biopsies should be taken even if the Biopsies should be taken even if the colonic mucosa appears grossly normal.colonic mucosa appears grossly normal.

Irritable bowel syndrome Irritable bowel syndrome
Crampy abdominal pain, bloating, Crampy abdominal pain, bloating, constipation, and urgent diarrhea. constipation, and urgent diarrhea.
No underlying anatomic or physiologic No underlying anatomic or physiologic abnormality.abnormality.
Diagnosis of exclusionDiagnosis of exclusion Dietary restrictions and avoidance of Dietary restrictions and avoidance of
caffeine, alcohol, and tobacco may help to caffeine, alcohol, and tobacco may help to alleviate symptoms. alleviate symptoms.
Antispasmodics and bulking agents may helpAntispasmodics and bulking agents may help


Emergency ResectionEmergency Resection Obstruction, perforation, or hemorrhage. Obstruction, perforation, or hemorrhage. Bowel is almost always unprepared and the patient may be Bowel is almost always unprepared and the patient may be
unstable. unstable. Attempt should be made to resect the involved segment along Attempt should be made to resect the involved segment along
with its lymphovascular supply. with its lymphovascular supply. Right colon or proximal transverse colon, a primary ileocolonic Right colon or proximal transverse colon, a primary ileocolonic
anastomosis usually can be performed safely as long as the anastomosis usually can be performed safely as long as the remaining bowel appears healthy and the patient is stable. remaining bowel appears healthy and the patient is stable.
Left-sided tumors-resection and end colostomy, with or without a Left-sided tumors-resection and end colostomy, with or without a mucus fistula. mucus fistula.
Increasing data for primary anastomosis without a bowel Increasing data for primary anastomosis without a bowel preparation or with an on-table lavage, w/w/o diverting ileostomy, preparation or with an on-table lavage, w/w/o diverting ileostomy, may be equally safe in this setting. may be equally safe in this setting.
Subtotal colectomy with a small bowel to rectosigmoid Subtotal colectomy with a small bowel to rectosigmoid anastomosis if the proximal colon looks unhealthyanastomosis if the proximal colon looks unhealthy
Resection and diversion (ileostomy or colostomy) remains safe Resection and diversion (ileostomy or colostomy) remains safe and appropriate if the bowel looks compromised or if the patient is and appropriate if the bowel looks compromised or if the patient is unstable, malnourished, or immunosuppressedunstable, malnourished, or immunosuppressed

Minimally Invasive Techniques Minimally Invasive Techniques of Resectionof Resection
Laparoscopically or with hand-assisted Laparoscopically or with hand-assisted laparoscopy. laparoscopy.
Improved cosmetic result, decreased postoperative Improved cosmetic result, decreased postoperative pain, earlier return of bowel function, and pain, earlier return of bowel function, and possible decrease in immunosuppressive impact possible decrease in immunosuppressive impact
Most studies have demonstrated equivalence Most studies have demonstrated equivalence between laparoscopic and open resection in terms between laparoscopic and open resection in terms of extent of resection. of extent of resection.
Pequire longer operative time than do open Pequire longer operative time than do open procedures. procedures.
Return of bowel function and length of hospital Return of bowel function and length of hospital stay are highly variable, but appear to be better. stay are highly variable, but appear to be better.

ProceduresProcedures
Ileocolic ResectionIleocolic Resection Resection of terminal ileum, cecum, and appendix Resection of terminal ileum, cecum, and appendix Benign lesions or incurable cancers arising in the terminal ileum, cecum, and, Benign lesions or incurable cancers arising in the terminal ileum, cecum, and,
occasionally, the appendixoccasionally, the appendix Ileocolic vessels are ligated and divided. Ileocolic vessels are ligated and divided. Primary anastomosis distal small bowel to ascending colon Primary anastomosis distal small bowel to ascending colon Most distal ileum needs to be resectedMost distal ileum needs to be resectedRight ColectomyRight Colectomy Most appropriate operation for curative intent resection of proximal colon Most appropriate operation for curative intent resection of proximal colon
carcinoma. carcinoma. Ileocolic vessels, right colic vessels, and right branches of the middle colic 10 cm Ileocolic vessels, right colic vessels, and right branches of the middle colic 10 cm
of terminal ileum included of terminal ileum included Ileal-transverse colon anastomosisIleal-transverse colon anastomosis Extended right colectomy for curative for lesions at the hepatic flexure or Extended right colectomy for curative for lesions at the hepatic flexure or
proximal transverse colon proximal transverse colon Transverse ColectomyTransverse Colectomy Ligating the middle colic vessels Ligating the middle colic vessels Colocolonic anastomosisColocolonic anastomosis Extended right colectomy safer Extended right colectomy safer

ProceduresProceduresLeft ColectomyLeft Colectomy For lesions in distal transverse colon, splenic flexure, or descending colonFor lesions in distal transverse colon, splenic flexure, or descending colon Left branches of the middle colic vessels, the left colic vessels, and the first branches of Left branches of the middle colic vessels, the left colic vessels, and the first branches of
the sigmoid vessels are ligated. the sigmoid vessels are ligated. Colocolonic anastomosis usually can be performed.Colocolonic anastomosis usually can be performed.Sigmoid ColectomySigmoid Colectomy Divide sigmoid branches of the inferior mesenteric arteryDivide sigmoid branches of the inferior mesenteric artery Entire sigmoid colon should be resected to the level of the peritoneal reflection Entire sigmoid colon should be resected to the level of the peritoneal reflection Descending colon to upper rectumDescending colon to upper rectum Full mobilization of the splenic flexure for tension-free anastomosisFull mobilization of the splenic flexure for tension-free anastomosisTotal and Subtotal ColectomyTotal and Subtotal Colectomy Fulminant colitis, attenuated FAP (AFAP), or synchronous colon carcinomasFulminant colitis, attenuated FAP (AFAP), or synchronous colon carcinomas Divide ileocolic vessels, right colic vessels, middle colic vessels, and left colic vessels Divide ileocolic vessels, right colic vessels, middle colic vessels, and left colic vessels
leave superior rectal vessels leave superior rectal vessels Subtotal colectomy with ileosigmoid anastomosis – distal sigmoid leftSubtotal colectomy with ileosigmoid anastomosis – distal sigmoid left Sigmoid completely removed- total abdominal colectomy with ileorectal anastomosis Sigmoid completely removed- total abdominal colectomy with ileorectal anastomosis End-ileostomy - remaining sigmoid or rectum made into mucus fistula or Hartmann End-ileostomy - remaining sigmoid or rectum made into mucus fistula or Hartmann
pouch.pouch.Total ProctocolectomyTotal Proctocolectomy Colon, rectum, and anus are removed and the ileum is brought to the skin as a Brooke Colon, rectum, and anus are removed and the ileum is brought to the skin as a Brooke
ileostomy. ileostomy. Restorative Proctocolectomy (Ileal Pouch Anal Anastomosis)Restorative Proctocolectomy (Ileal Pouch Anal Anastomosis) Colon and rectum resected, but the anal sphincter muscles portion of the distal anal Colon and rectum resected, but the anal sphincter muscles portion of the distal anal
canal are preserved. canal are preserved.

ProceduresProcedures
High Anterior ResectionHigh Anterior Resection Distal sigmoid colon and upper rectum for benign lesions and disease Distal sigmoid colon and upper rectum for benign lesions and disease
at the rectosigmoid junction such as diverticulitis. at the rectosigmoid junction such as diverticulitis. Primary anastomosis (usually end-to-end) between the colon and Primary anastomosis (usually end-to-end) between the colon and
rectal stump with a short cuff of peritoneum surrounding its anterior rectal stump with a short cuff of peritoneum surrounding its anterior two thirds two thirds
Low Anterior ResectionLow Anterior Resection Lesions in the upper and midrectum. Lesions in the upper and midrectum. The rectosigmoid is mobilized, the pelvic peritoneum is openedThe rectosigmoid is mobilized, the pelvic peritoneum is opened Dissection to the anorectal ring Dissection to the anorectal ring Requires mobilization of the splenic flexure Requires mobilization of the splenic flexure Extended Low Anterior ResectionExtended Low Anterior Resection For distal rectum lesions but several centimeters above the sphincter For distal rectum lesions but several centimeters above the sphincter Coloanal anastomosis Coloanal anastomosis Creation of a temporary ileostomy Creation of a temporary ileostomy Can create colon J-pouch if no sphincter damage Can create colon J-pouch if no sphincter damage

ProceduresProcedures
Hartmann's Procedure and Mucus FistulaHartmann's Procedure and Mucus Fistula colostomy or ileostomy is created and the distal colon or rectum is left as a colostomy or ileostomy is created and the distal colon or rectum is left as a
blind pouchblind pouch mucus fistula if enough bowel presentmucus fistula if enough bowel presentAbdominoperineal ResectionAbdominoperineal Resection entire rectum, anal canal, and anus with construction of a permanent entire rectum, anal canal, and anus with construction of a permanent
colostomy from the descending or sigmoid coloncolostomy from the descending or sigmoid colon AnastomosesAnastomoses end-to-end (roughly the same caliber), end-to-side (one limb of bowel is larger end-to-end (roughly the same caliber), end-to-side (one limb of bowel is larger
than the other), side-to-end (proximal bowel is of smaller caliber than the distal than the other), side-to-end (proximal bowel is of smaller caliber than the distal bowel, ileorectal), or side-to-side (ileocolic and small bowel anastomoses) bowel, ileorectal), or side-to-side (ileocolic and small bowel anastomoses)
handsewn (single or double layer(continuous inner layer and an interrupted handsewn (single or double layer(continuous inner layer and an interrupted outer layer)) or stapled (particularly useful for creating low rectal or anal canal outer layer)) or stapled (particularly useful for creating low rectal or anal canal anastomoses)anastomoses)
none has been proven to be superiornone has been proven to be superior submucosal layer of the intestine provides the strength of the bowel wall submucosal layer of the intestine provides the strength of the bowel wall NO tension in a normotensiveNO tension in a normotensive Highest risk - distal rectal or anal canal, involve irradiated or diseased intestine, Highest risk - distal rectal or anal canal, involve irradiated or diseased intestine,
or are performed in malnourished, ill patients. or are performed in malnourished, ill patients.

OstomiesOstomies
Temporary or permanent, end-on or a loop Temporary or permanent, end-on or a loop Placement and construction are crucial for Placement and construction are crucial for
functionfunction Located within the rectus muscle to Located within the rectus muscle to
minimize the risk of a postoperative minimize the risk of a postoperative parastomal hernia parastomal hernia
Must be in plain sight Must be in plain sight Preoperative evaluation by ostomy nurse Preoperative evaluation by ostomy nurse
(sight and teaching) (sight and teaching)

More OstomyMore Ostomy
Temporary Ileostomy - loop ileostomy Temporary Ileostomy - loop ileostomy Subsequent closure often can be accomplished without a formal laparotomySubsequent closure often can be accomplished without a formal laparotomy Flexible endoscopy exam and a contrast enema (Gastrografin) are Flexible endoscopy exam and a contrast enema (Gastrografin) are
recommended before closure recommended before closure Permanent IleostomyPermanent Ileostomy After total proctocolectomy or in patients with obstruction. After total proctocolectomy or in patients with obstruction. End ileostomy is the preferred configuration End ileostomy is the preferred configuration Stitches often are used to secure the bowel to the posterior fascia.Stitches often are used to secure the bowel to the posterior fascia.Complications of IleostomyComplications of Ileostomy Stoma necrosis - skeletonizing or tight fascial defectStoma necrosis - skeletonizing or tight fascial defect Necrosis below the level of the fascia requires surgical revision Necrosis below the level of the fascia requires surgical revision Stoma retraction may occur early or lateStoma retraction may occur early or late Dehydration fluid and electrolyte abnormalities, keep at less than 1500 mL/dDehydration fluid and electrolyte abnormalities, keep at less than 1500 mL/d Bulk agents and opioids (Lomotil, Imodium, tincture of opium) are useful. Bulk agents and opioids (Lomotil, Imodium, tincture of opium) are useful.
Obstruction Obstruction Parastomal hernia - symptomatic should be repaired, re-siting the stoma to the Parastomal hernia - symptomatic should be repaired, re-siting the stoma to the
contralateral side of the abdomen. contralateral side of the abdomen. Prolapse (rare)Prolapse (rare)

ColostomyColostomy
Most end colostomies >> loop colostomies (too bulky and prolapse Most end colostomies >> loop colostomies (too bulky and prolapse is more likely) is more likely)
Should be matured in a Brooke fashionShould be matured in a Brooke fashion Mucus fistula or Hartmann's pouch Mucus fistula or Hartmann's pouch Closure generally requires laparotomyClosure generally requires laparotomyComplications of ColostomyComplications of Colostomy Necrosis management similar to ileostomy Necrosis management similar to ileostomy Retraction less problematic with a colostomy Retraction less problematic with a colostomy Obstruction is unusualObstruction is unusual Parastomal hernia is the most common late complication of a Parastomal hernia is the most common late complication of a
colostomy (repair if it is symptomatic)colostomy (repair if it is symptomatic) Prolapse occurs rarelyProlapse occurs rarely Dehydration is rare Dehydration is rare Functional ResultsFunctional Results Usually excellentUsually excellent Uncommon diarrhea and bowel frequency. Uncommon diarrhea and bowel frequency.

PositioningPositioning Most abdominal colectomies can be performed in the supine position. Most abdominal colectomies can be performed in the supine position.
Anterior and APRs require lithotomy positioning. Anterior and APRs require lithotomy positioning. Bowel PreparationBowel Preparation Decreasing the bacterial load in the colon and rectum (not proven)Decreasing the bacterial load in the colon and rectum (not proven) Most commonly used regimens include polyethylene glycol (PEG) solutions Most commonly used regimens include polyethylene glycol (PEG) solutions
or sodium phosphate, equally efficacious in bowel cleansing. or sodium phosphate, equally efficacious in bowel cleansing. Oral antibiotics to decreasing the bacterial load of the colon. never been Oral antibiotics to decreasing the bacterial load of the colon. never been
proven to decrease postoperative infectious complications. proven to decrease postoperative infectious complications. Ideally, a stoma should be placed in a location that the patient can easily Ideally, a stoma should be placed in a location that the patient can easily
see and manipulate, within the rectus muscle, and below the belt line (see see and manipulate, within the rectus muscle, and below the belt line (see Fig. 29-15). In emergencies, placement high on the abdominal wall is Fig. 29-15). In emergencies, placement high on the abdominal wall is preferred to a low-lying site.preferred to a low-lying site.
Ureteral StentsUreteral Stents Useful for identifying the ureters intraoperatively Useful for identifying the ureters intraoperatively Invaluable in reoperative pelvic surgery or when there is significant Invaluable in reoperative pelvic surgery or when there is significant
retroperitoneal inflammation retroperitoneal inflammation Lighted stents may be helpful in laparoscopic resections Lighted stents may be helpful in laparoscopic resections

Inflammatory Bowel DiseaseInflammatory Bowel Disease
Epidemiology Epidemiology Ulcerative colitis to 15 people per 100,000 Ulcerative colitis to 15 people per 100,000 Crohn's disease is slightly lower, one to five people per 100,000 population. Both have bimodal incidence, 15 to 30 years and Crohn's disease is slightly lower, one to five people per 100,000 population. Both have bimodal incidence, 15 to 30 years and
ages 55 to 60 years. ages 55 to 60 years. 15% indeterminate colitis.15% indeterminate colitis.EtiologyEtiology none are proven. none are proven. Family history 10 to 30% have a family member with the same diseaseFamily history 10 to 30% have a family member with the same disease Autoimmune vs infectiousAutoimmune vs infectious Pathology and Differential DiagnosisPathology and Differential DiagnosisUlcerative colitis is a mucosal process Ulcerative colitis is a mucosal process mucosa atrophic and friable, crypt abscesses friable, inflammatory pseudopolyps. Proctitis (just rectum) to pancolitis. mucosa atrophic and friable, crypt abscesses friable, inflammatory pseudopolyps. Proctitis (just rectum) to pancolitis. does not involve the small intestine, but "backwash ileitisdoes not involve the small intestine, but "backwash ileitis continuous involvement of the rectum and bloody diarrhea and crampy abdominal pain, tenesmus. Severe abdominal pain continuous involvement of the rectum and bloody diarrhea and crampy abdominal pain, tenesmus. Severe abdominal pain
and fever = fulminant colitis or toxic megacolon. Dx with colonoscopy and mucosal biopsy.and fever = fulminant colitis or toxic megacolon. Dx with colonoscopy and mucosal biopsy.Crohns disease Crohns disease transmural and can affect any part of the GI tract from mouth to anus. Mucosal ulcerations, noncaseating granulomas transmural and can affect any part of the GI tract from mouth to anus. Mucosal ulcerations, noncaseating granulomas
Chronic inflammation may ultimately result in fibrosis, strictures, and fistulas in either the colon or small intestine. Chronic inflammation may ultimately result in fibrosis, strictures, and fistulas in either the colon or small intestine. Colonoscopy deep serpiginous ulcers and a "cobblestone" appearance. Skip lesions and rectal sparing are common. Colonoscopy deep serpiginous ulcers and a "cobblestone" appearance. Skip lesions and rectal sparing are common.
diarrhea, crampy abdominal pain, and fever. Strictures may produce symptoms of obstruction. Perianal Crohn's disease may diarrhea, crampy abdominal pain, and fever. Strictures may produce symptoms of obstruction. Perianal Crohn's disease may present with pain, swelling, and drainage from fistulas or abscesses. present with pain, swelling, and drainage from fistulas or abscesses.
Extraintestinal ManifestationsExtraintestinal Manifestations Fatty infiltration of the liver is present in 40 to 50% cirrhosis is found in 2 to 5%. Fatty infiltration of the liver is present in 40 to 50% cirrhosis is found in 2 to 5%. 40 to 60% with primary sclerosing cholangitis have ulcerative colitis. Biliary carcinoma fromlong standing disease40 to 60% with primary sclerosing cholangitis have ulcerative colitis. Biliary carcinoma fromlong standing disease Arthritis 20 times greater than in the general population. Arthritis 20 times greater than in the general population. Sacroiliitis and ankylosing spondylitis are associated with inflammatory bowel diseaseSacroiliitis and ankylosing spondylitis are associated with inflammatory bowel disease Erythema nodosum is seen in 5 to 15%Erythema nodosum is seen in 5 to 15% Women are affected three to four times more frequently than men. Pyoderma gangrenosum is an uncommon but serious.Women are affected three to four times more frequently than men. Pyoderma gangrenosum is an uncommon but serious. Up to 10% will develop ocular lesions. Up to 10% will develop ocular lesions.

Principles of Nonoperative ManagementPrinciples of Nonoperative Management Ulcerative proctitis and proctosigmoiditis salicylate and/or corticosteroid suppositories and enemas Ulcerative proctitis and proctosigmoiditis salicylate and/or corticosteroid suppositories and enemas SalicylatesSalicylates Sulfasalazine (Azulfidine), 5-ASA, and related compounds are first-line agents in the medical treatment of Sulfasalazine (Azulfidine), 5-ASA, and related compounds are first-line agents in the medical treatment of
mild to moderate inflammatory bowel disease. cyclooxygenase and 5-lipoxygenase mild to moderate inflammatory bowel disease. cyclooxygenase and 5-lipoxygenase AntibioticsAntibiotics Metronidazole possibly helps with Crohn's colitis but Abx reserved for fulminant colitis or toxic megacolonMetronidazole possibly helps with Crohn's colitis but Abx reserved for fulminant colitis or toxic megacolonCorticosteroidsCorticosteroids Corticosteroids are a key component Corticosteroids are a key component 75 to 90% of patients will improve 75 to 90% of patients will improve Failure to wean corticosteroids is a relative indication for surgery.Failure to wean corticosteroids is a relative indication for surgery. Corticosteroid enemas provide effective local therapy for proctitis Corticosteroid enemas provide effective local therapy for proctitis Other Immunosuppressive AgentsOther Immunosuppressive Agents Azathioprine and 6-mercaptopurine are antimetabolite drugs ulcerative colitis and Crohn's disease in patients Azathioprine and 6-mercaptopurine are antimetabolite drugs ulcerative colitis and Crohn's disease in patients
who have failed salicylate therapy or who are dependent upon or refractory to corticosteroids. who have failed salicylate therapy or who are dependent upon or refractory to corticosteroids. Onset of action of these drugs takes 6 to 12 weeks taken with steriodsOnset of action of these drugs takes 6 to 12 weeks taken with steriods Cyclosporine interferes with T-cell function. Cyclosporine interferes with T-cell function. Not routinely used to treat inflammatory bowel disease, helps with refractory UC and CrohnsNot routinely used to treat inflammatory bowel disease, helps with refractory UC and Crohns Methotrexate is a folate antagonist efficacy of this agent is unprovenMethotrexate is a folate antagonist efficacy of this agent is unproven Infliximab (Remicade) is a monoclonal antibody against tumor necrosis factor alpha. moderate to severe Infliximab (Remicade) is a monoclonal antibody against tumor necrosis factor alpha. moderate to severe
Crohn's disease Recurrence is commonCrohn's disease Recurrence is commonNutritionNutrition Patients with inflammatory bowel disease often are malnourished. Pain, obstruction, diarrhea inflammatory Patients with inflammatory bowel disease often are malnourished. Pain, obstruction, diarrhea inflammatory
catabolic state catabolic state TPN suggestedTPN suggested

Ulcerative ColitisUlcerative Colitis
Characterized by remissions and exacerbations. Characterized by remissions and exacerbations. Insidious, with minimal bloody stools, or the onset can be abrupt, with severe Insidious, with minimal bloody stools, or the onset can be abrupt, with severe
diarrhea and bleeding, tenesmus, abdominal pain, and fever. diarrhea and bleeding, tenesmus, abdominal pain, and fever. Dx endoscopically with bx, chronic phase better, don’t perf (acute phase)Dx endoscopically with bx, chronic phase better, don’t perf (acute phase) RectumRectum invariably involved invariably involved Pus and mucus also may be present. Pus and mucus also may be present. Barium enema "lead pipe" colonBarium enema "lead pipe" colon Emergent surgery - hemorrhage, toxic megacolon, or fulminant colitis who fail to Emergent surgery - hemorrhage, toxic megacolon, or fulminant colitis who fail to
respond rapidly to medical therapy. respond rapidly to medical therapy. Fulminant colitis should be treated aggressively with bowel rest, hydration, broad-Fulminant colitis should be treated aggressively with bowel rest, hydration, broad-
spectrum antibiotics, and parenteral corticosteroids. No colonoscopy, barium spectrum antibiotics, and parenteral corticosteroids. No colonoscopy, barium enema, and antidiarrheal agents are contraindicated. Deteriation or failure to enema, and antidiarrheal agents are contraindicated. Deteriation or failure to improve within 24 to 48 hours mandates surgery.improve within 24 to 48 hours mandates surgery.
Elective surgery - intractability despite maximal medical therapy, side effects not Elective surgery - intractability despite maximal medical therapy, side effects not tolerated, significant risk of developing colorectal carcinoma. tolerated, significant risk of developing colorectal carcinoma.
Risk of malignancy increases with pancolonic disease and the duration of Risk of malignancy increases with pancolonic disease and the duration of symptoms is approximately 2% after 10 years, 8% after 20 years, and 18% after symptoms is approximately 2% after 10 years, 8% after 20 years, and 18% after 30 years. 30 years.
Long-standing ulcerative colitis undergo colonoscopic surveillance with multiple Long-standing ulcerative colitis undergo colonoscopic surveillance with multiple (40 to 50), random biopsies to identify dysplasia before invasive malignancy (40 to 50), random biopsies to identify dysplasia before invasive malignancy develops (flat polyps)develops (flat polyps)

Ulcerative ColitisUlcerative Colitis
Annual surveillance after: Annual surveillance after: 8 years in patients with pancolitis 8 years in patients with pancolitis 15 years in patients with left-sided colitis15 years in patients with left-sided colitis dysplasia - should be advised to undergo proctocolectomydysplasia - should be advised to undergo proctocolectomy controversy prophylactic proctocolectomy for chronic UC for >10 years controversy prophylactic proctocolectomy for chronic UC for >10 years
Emergent OperationEmergent Operation Fulminant colitis or toxic megacolon Fulminant colitis or toxic megacolon Total abdominal colectomy with end ileostomy>>>total Total abdominal colectomy with end ileostomy>>>total
proctocolectomy proctocolectomy Elective OperationElective Operation Include resection of the rectumInclude resection of the rectum Indeterminate -> abdominal colectomy with ileorectal anastomosis Indeterminate -> abdominal colectomy with ileorectal anastomosis Total proctocolectomy with end ileostomy has been the "gold Total proctocolectomy with end ileostomy has been the "gold
standard" for patients with chronic ulcerative colitis. standard" for patients with chronic ulcerative colitis. restorative proctocolectomy with ileal pouch–anal anastomosis has restorative proctocolectomy with ileal pouch–anal anastomosis has
become the procedure of choice become the procedure of choice

Crohn's DiseaseCrohn's Disease
Exacerbations and remissions. Exacerbations and remissions. Any portion of the intestinal tract, from mouth to anus, impossible to remove all of Any portion of the intestinal tract, from mouth to anus, impossible to remove all of
the at-risk intestinethe at-risk intestine Rectal sparing occurs in 40% Rectal sparing occurs in 40% Terminal ileum and cecum (ileocolic Crohn's disease) involved 41%Terminal ileum and cecum (ileocolic Crohn's disease) involved 41% Internal fistulas (require resection of the segment of bowel), chronic strictures Internal fistulas (require resection of the segment of bowel), chronic strictures
(resection or stricturoplasty) (resection or stricturoplasty) Length of bowel removed should be minimized. Length of bowel removed should be minimized. Bowel should be resected to an area with grossly normal margins ONLYBowel should be resected to an area with grossly normal margins ONLY Stoma should be strongly considered in any patient who is hemodynamically Stoma should be strongly considered in any patient who is hemodynamically
unstable, septic, malnourished, or receiving high-dose immunosuppressive therapy unstable, septic, malnourished, or receiving high-dose immunosuppressive therapy and in patients with extensive intra-abdominal contamination.and in patients with extensive intra-abdominal contamination.
Ileocolic and Small Bowel Crohn's DiseaseIleocolic and Small Bowel Crohn's Disease Most common indications for surgery are internal fistula or abscess (30 to 38% of Most common indications for surgery are internal fistula or abscess (30 to 38% of
patients) and obstruction (35 to 37% of patients). patients) and obstruction (35 to 37% of patients). Drainage of abscess(es) and antibiotics, Drainage of abscess(es) and antibiotics, Isolated chronic strictures also should be resected. In patients with multiple fibrotic Isolated chronic strictures also should be resected. In patients with multiple fibrotic
strictures that would require extensive small bowel resection, stricturoplasty is a safe strictures that would require extensive small bowel resection, stricturoplasty is a safe and effective alternative to resection.and effective alternative to resection.
Recurrence 50% in 10 yrsRecurrence 50% in 10 yrs

Crohn's colitis (especially pancolitis) carries nearly the same Crohn's colitis (especially pancolitis) carries nearly the same risk for cancer as ulcerative colitis. risk for cancer as ulcerative colitis.
Ileal pouch–anal reconstruction is not recommended Ileal pouch–anal reconstruction is not recommended perianal disease occurs in 35% of all patients with Crohn's perianal disease occurs in 35% of all patients with Crohn's
disease disease fissure from Crohn's disease is particularly deep more like an fissure from Crohn's disease is particularly deep more like an
ulcer. They often are multiple and located in a ulcer. They often are multiple and located in a lateral lateral positionposition
Treatment of anal and perianal Crohn's disease focuses on Treatment of anal and perianal Crohn's disease focuses on alleviation of symptoms. should not do surgery unless forced, alleviation of symptoms. should not do surgery unless forced, risk of creating chronic, nonhealing wounds. risk of creating chronic, nonhealing wounds.
Drain abscesses, mushroom catheters and liberal use of Drain abscesses, mushroom catheters and liberal use of setons, advancement flaps if minimal disease, intractable setons, advancement flaps if minimal disease, intractable perianal sepsis requires proctectomy.perianal sepsis requires proctectomy.
Infliximab and others have shown some efficacy in healing Infliximab and others have shown some efficacy in healing chronic fistulas (drain any and all abscesses before starting) chronic fistulas (drain any and all abscesses before starting)

Indeterminate ColitisIndeterminate Colitis
15% of patients with IBD 15% of patients with IBD characteristics of both diseasescharacteristics of both diseases
Indications for surgery are the same, Indications for surgery are the same, treat like Crohns treat like Crohns


Diverticular DiseaseDiverticular Disease
Majority false diverticula, mucosa and Majority false diverticula, mucosa and muscularis mucosa has herniated muscularis mucosa has herniated through the colonic wall, between the through the colonic wall, between the taeniae coli, where the main blood taeniae coli, where the main blood vessels penetrate the colonic wall vessels penetrate the colonic wall
Extremely common in US (50% over 50 Extremely common in US (50% over 50 years) years)
Sigmoid colon is the most common site Sigmoid colon is the most common site Lack of dietary fiber Lack of dietary fiber

Inflammatory Complications Inflammatory Complications (Diverticulitis)(Diverticulitis)
Left-sided abdominal pain, with or Left-sided abdominal pain, with or without fever, and leukocytosiswithout fever, and leukocytosis
Occurs in 10 to 25% of people with Occurs in 10 to 25% of people with diverticulosis. diverticulosis.
Broad spectrum of disease (out pt tx vs Broad spectrum of disease (out pt tx vs emergent OR)emergent OR)
Free air on films, CT scan pericolic Free air on films, CT scan pericolic inflammation, phlegmon, or abscess. inflammation, phlegmon, or abscess.

Uncomplicated DiverticulitisUncomplicated Diverticulitis
LLQ pain and tenderness. LLQ pain and tenderness. CT findings include pericolic soft tissue stranding, colonic wall CT findings include pericolic soft tissue stranding, colonic wall
thickening, and/or phlegmon. thickening, and/or phlegmon. Outpatient therapy with broad-spectrum oral antibiotics (7 to 10 Outpatient therapy with broad-spectrum oral antibiotics (7 to 10
days) and a low-residue diet..no improvewment in 48 to 72 hours days) and a low-residue diet..no improvewment in 48 to 72 hours think abscess think abscess
50 to 70% will have no further episodes. 50 to 70% will have no further episodes. elective sigmoid colectomy often is recommended after the elective sigmoid colectomy often is recommended after the
second episode of diverticulitis, second episode of diverticulitis, Resection often has been recommended after the first episode in Resection often has been recommended after the first episode in
very young patients or immunosupressed and often is very young patients or immunosupressed and often is recommended after the first episode of complicated diverticulitis. recommended after the first episode of complicated diverticulitis.
carcinoma must be excluded by colonoscopycarcinoma must be excluded by colonoscopy Sigmoidoscopy or colonoscopy is recommended 4 to 6 weeks after Sigmoidoscopy or colonoscopy is recommended 4 to 6 weeks after
recovery. recovery. sigmoid colectomy with a primary anastomosis is the procedure of sigmoid colectomy with a primary anastomosis is the procedure of
choice.choice.

Complicated DiverticulitisComplicated Diverticulitis
abscess, obstruction, diffuse peritonitis (free perforation), or fistulas between the colon and abscess, obstruction, diffuse peritonitis (free perforation), or fistulas between the colon and adjacent structures. adjacent structures.
Hinchey staging system Hinchey staging system Stage I includes colonic inflammation with an associated pericolic abscess; stage II includes colonic Stage I includes colonic inflammation with an associated pericolic abscess; stage II includes colonic
inflammation with a retroperitoneal or pelvic abscessinflammation with a retroperitoneal or pelvic abscess stage III is associated with purulent peritonitis; and stage IV is associated with fecal peritonitis. stage III is associated with purulent peritonitis; and stage IV is associated with fecal peritonitis. Urgent or emergent laparotomy may be required if an abscess is inaccessible to percutaneous Urgent or emergent laparotomy may be required if an abscess is inaccessible to percutaneous
drainage, if the patient's condition deteriorates or fails to improve, or if the patient presents with drainage, if the patient's condition deteriorates or fails to improve, or if the patient presents with free intra-abdominal air or peritonitis. free intra-abdominal air or peritonitis.
(Hinchey stages I and II) may be candidates for a sigmoid colectomy with a primary anastomosis (a (Hinchey stages I and II) may be candidates for a sigmoid colectomy with a primary anastomosis (a one-stage operation). In patients with larger abscesses, peritoneal soiling, or peritonitis, sigmoid one-stage operation). In patients with larger abscesses, peritoneal soiling, or peritonitis, sigmoid colectomy with end colostomy and Hartmann pouch is the most commonly used procedure. Sigmoid colectomy with end colostomy and Hartmann pouch is the most commonly used procedure. Sigmoid colectomy with end colostomy is the safest procedure to perform in this emergent setting.colectomy with end colostomy is the safest procedure to perform in this emergent setting.
FistulasFistulas 5% of patients with complicated diverticulitis develop fistulas 5% of patients with complicated diverticulitis develop fistulas Colovesical >colovaginal and coloenteric fistulas>colocutaneous Colovesical >colovaginal and coloenteric fistulas>colocutaneous Contrast enema and/or small bowel studies Contrast enema and/or small bowel studies malignancy, Crohn's disease, and radiation-induced fistulas. malignancy, Crohn's disease, and radiation-induced fistulas. colonoscopy or sigmoidoscopy usually is required to rule out malignancycolonoscopy or sigmoidoscopy usually is required to rule out malignancy resection of the affected segment resection of the affected segment HemorrhageHemorrhage erosion of the peridiverticular arteriole and may result in massive hemorrhage. erosion of the peridiverticular arteriole and may result in massive hemorrhage. 80% of patients, bleeding stops spontaneously80% of patients, bleeding stops spontaneously


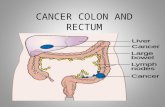
Adenocarcinoma and PolypsAdenocarcinoma and Polyps
IncidenceIncidence Colorectal carcinoma is the most common malignancy of the GI Colorectal carcinoma is the most common malignancy of the GI
tract. Over 150,000 new cases are diagnosed tract. Over 150,000 new cases are diagnosed Colon cancer is the second most lethal cancer in the USColon cancer is the second most lethal cancer in the US AgingAging Aging is the dominant risk factor Aging is the dominant risk factor rising steadily after age 50 years. 90% rising steadily after age 50 years. 90% Hereditary Risk FactorsHereditary Risk Factors 80% sporadic, 20% known family history 80% sporadic, 20% known family history Environmental and Dietary FactorsEnvironmental and Dietary Factors high in animal fat and low in fiber high in animal fat and low in fiber diet high in oleic acid (olive oil, coconut oil, fish oil) does not diet high in oleic acid (olive oil, coconut oil, fish oil) does not
increase risk. increase risk. diet high in vegetable fiber appears to be protective. alcohol diet high in vegetable fiber appears to be protective. alcohol
intake intake Obesity and sedentary Obesity and sedentary

Risk FactorsRisk Factors
Cigarette smoking Cigarette smoking Acromegaly, Acromegaly, Pelvic irradiation Pelvic irradiation Genetic DefectsGenetic DefectsInflammatory Bowel DiseaseInflammatory Bowel Disease Ulcerative pancolitis, the risk of carcinoma is approximately Ulcerative pancolitis, the risk of carcinoma is approximately
2% after 10 years, 8% after 20 years, and 18% after 30 2% after 10 years, 8% after 20 years, and 18% after 30 years. Patients with Crohn's pancolitis have similar risk. years. Patients with Crohn's pancolitis have similar risk.
Colonoscopy with multiple random mucosal biopsies has Colonoscopy with multiple random mucosal biopsies has been recommended annually after 8 years of disease for been recommended annually after 8 years of disease for patients with pancolitis and after 12 to 15 years of disease patients with pancolitis and after 12 to 15 years of disease for patients with left-sided colitisfor patients with left-sided colitis
..

GeneticsGenetics
APC gene APC gene present in 80% of sporadic cases present in 80% of sporadic cases tumor-suppressor genetumor-suppressor gene ADADK-ras K-ras proto-oncogene proto-oncogene only one allele only one allele G protein involved in intracellular GTP signal transduction. G protein involved in intracellular GTP signal transduction. MYH gene MYH gene base excision repair genebase excision repair gene biallelic deletion biallelic deletion ARARDCCDCC tumor-suppressor tumor-suppressor gene product is poorly understoodgene product is poorly understood differentiation and axonal migrationdifferentiation and axonal migration present in more than 70% of colorectal carcinomas present in more than 70% of colorectal carcinomas p53p53 tumor-suppressor gene tumor-suppressor gene crucial for initiating apoptosiscrucial for initiating apoptosis 75% of colorectal cancers75% of colorectal cancers

Neoplastic PolypsNeoplastic Polyps
Adenomatous polyps Adenomatous polyps 25% of the population older than 50 years of 25% of the population older than 50 years of Lesions are dysplastic. Size and type matterLesions are dysplastic. Size and type matter Tubular adenomas 5% malignancy Tubular adenomas 5% malignancy Villous adenomas in up to 40%. Villous adenomas in up to 40%. Tubulovillous intermediate risk (22%). Tubulovillous intermediate risk (22%). The risk of carcinoma in a polyp larger than 2 cm is 35 to 50%. The risk of carcinoma in a polyp larger than 2 cm is 35 to 50%. Pedunculated polyps are amenable to colonoscopic snare excisionPedunculated polyps are amenable to colonoscopic snare excision Sessile polyps are more challenging (saline lift and piecemeal Sessile polyps are more challenging (saline lift and piecemeal
snare)snare) Rectal sessile polyps, transanal operative excision Rectal sessile polyps, transanal operative excision Site of sessile polypectomies should be marked by injection of Site of sessile polypectomies should be marked by injection of
methylene blue or India ink to guide follow-up colonoscopy methylene blue or India ink to guide follow-up colonoscopy Risk perforation and bleeding.Risk perforation and bleeding. Colectomy if unable to removeColectomy if unable to remove

Neoplastic PolypsNeoplastic Polyps
Hamartomatous Polyps (Juvenile Polyps)Hamartomatous Polyps (Juvenile Polyps) Usually are not premalignant. Usually are not premalignant. Childhood but may occur at any age. Childhood but may occur at any age. Bleeding > intussusception and/or obstruction Bleeding > intussusception and/or obstruction Treated by polypectomy. Treated by polypectomy. Familial juvenile polyposis Familial juvenile polyposis Autosomal dominant Autosomal dominant Hundreds of polyps Hundreds of polyps May degenerate into adenomas and, eventually, carcinoma. Annual screening 10 and 12 years. May degenerate into adenomas and, eventually, carcinoma. Annual screening 10 and 12 years. Total proctocolectomy if rectal involvementTotal proctocolectomy if rectal involvementPeutz-Jeghers syndrome Peutz-Jeghers syndrome Small intestine >> colon and rectum. Small intestine >> colon and rectum. Melanin spots often are noted on the buccal mucosa and lips Melanin spots often are noted on the buccal mucosa and lips Hamartomas, low risk, carcinoma may occasionally develop. Hamartomas, low risk, carcinoma may occasionally develop. Surgery is reserved for obstruction or bleeding Surgery is reserved for obstruction or bleeding Above and below at age 20 years then annual flexible sigmoidoscopy thereafter.Above and below at age 20 years then annual flexible sigmoidoscopy thereafter.Inflammatory Polyps (Pseudopolyps)Inflammatory Polyps (Pseudopolyps) Inflammatory bowel disease>> amebic colitis, ischemic colitis, and schistosomal colitisInflammatory bowel disease>> amebic colitis, ischemic colitis, and schistosomal colitis Not premalignantNot premalignantHyperplastic PolypsHyperplastic Polyps Extremely common Extremely common Usually are small (<5 mm) Usually are small (<5 mm) Hyperplasia without any dysplasia, not premalignantHyperplasia without any dysplasia, not premalignant Large hyperplastic polyps (>2 cm) may have slight riskLarge hyperplastic polyps (>2 cm) may have slight risk

Familial Adenomatous Familial Adenomatous PolyposisPolyposis
Autosomal dominant Autosomal dominant Mutation in the APC gene, located on chromosome 5q. Mutation in the APC gene, located on chromosome 5q. Up to 25% without other affected family membersUp to 25% without other affected family members Thousands of adenomatous polyps shortly after pubertyThousands of adenomatous polyps shortly after puberty Lifetime risk approaches 100% by age 50 years.Lifetime risk approaches 100% by age 50 years. Flexible sigmoidoscopy of first-degree relatives of FAP patients Flexible sigmoidoscopy of first-degree relatives of FAP patients
beginning at age 10 to 15 years has been the traditional mainstay of beginning at age 10 to 15 years has been the traditional mainstay of screening. screening.
At risk for At risk for duodenalduodenal, periampullary carcinoma so need EGDs, periampullary carcinoma so need EGDs Total proctocolectomy with either an end (Brooke) ileostomy vs total Total proctocolectomy with either an end (Brooke) ileostomy vs total
abdominal colectomy with ileorectal anastomosis; and restorative abdominal colectomy with ileorectal anastomosis; and restorative proctocolectomy with ileal pouch–anal anastomosis with or without a proctocolectomy with ileal pouch–anal anastomosis with or without a temporary ileostomy. temporary ileostomy.
COX-2 inhibitors (celecoxib, sulindac) may slow polyp formationCOX-2 inhibitors (celecoxib, sulindac) may slow polyp formation FAP may be associated with congenital hypertrophy of the retinal FAP may be associated with congenital hypertrophy of the retinal
pigmented epithelium, desmoid tumors, epidermoid cysts, mandibular pigmented epithelium, desmoid tumors, epidermoid cysts, mandibular osteomas (Gardner's syndrome), and central nervous system tumors osteomas (Gardner's syndrome), and central nervous system tumors (Turcot's syndrome). (Turcot's syndrome).


Attenuated FAPAttenuated FAP
AFAP is a recently recognized variant AFAP is a recently recognized variant of FAP associated with mutations at of FAP associated with mutations at the 3' or 5' end of the APC gene. the 3' or 5' end of the APC gene.
Patients present later in life with Patients present later in life with fewer polyps (usually 10 to 100) fewer polyps (usually 10 to 100)
Carcinoma develops in more than Carcinoma develops in more than 50% of these patients50% of these patients

Hereditary Nonpolyposis Colon Hereditary Nonpolyposis Colon Cancer (Lynch Syndrome)Cancer (Lynch Syndrome)
Extremely rare (1 to 3%). Extremely rare (1 to 3%). Errors in mismatch repairErrors in mismatch repair Autosomal dominant Autosomal dominant Average age: 40 to 45 yearsAverage age: 40 to 45 years 70% of affected individuals will develop colorectal cancer. 70% of affected individuals will develop colorectal cancer. Risk of synchronous or metachronous colorectal carcinoma is 40%. Risk of synchronous or metachronous colorectal carcinoma is 40%. Associated with extracolonic malignancies, including endometrial, which is most Associated with extracolonic malignancies, including endometrial, which is most
common, ovarian, pancreas, stomach, small bowel, biliary, and urinary tract common, ovarian, pancreas, stomach, small bowel, biliary, and urinary tract carcinomas. carcinomas.
Diagnosis of HNPCC is made based upon family history. Diagnosis of HNPCC is made based upon family history. The Amsterdam criteriaThe Amsterdam criteria: three affected relatives with histologically verified : three affected relatives with histologically verified
adenocarcinoma of the large bowel (one must be a first-degree relative of one of the adenocarcinoma of the large bowel (one must be a first-degree relative of one of the others) in two successive generations of a family with one patient diagnosed before age others) in two successive generations of a family with one patient diagnosed before age 50 years. 50 years.
Screening colonoscopy is recommended annually for at-risk patients beginning at either Screening colonoscopy is recommended annually for at-risk patients beginning at either age 20 to 25 years or 10 years younger than the youngest age at diagnosis in the age 20 to 25 years or 10 years younger than the youngest age at diagnosis in the family, whichever comes first.family, whichever comes first.
Transvaginal ultrasound or endometrial aspiration biopsy also is recommended annually Transvaginal ultrasound or endometrial aspiration biopsy also is recommended annually after age 25 to 35 years. after age 25 to 35 years.
Total colectomy with ileorectal anastomosis is recommended once adenomas or a colon Total colectomy with ileorectal anastomosis is recommended once adenomas or a colon carcinoma is diagnosedcarcinoma is diagnosed
Annual proctoscopy Annual proctoscopy

Familial Colorectal Cancer Familial Colorectal Cancer (Nonsyndromic)(Nonsyndromic)
10 to 15% of patients with colorectal 10 to 15% of patients with colorectal cancercancer
Approximately 6%, but rises to 12% if Approximately 6%, but rises to 12% if one first-degree relative is affected and one first-degree relative is affected and to 35% if two first-degree relatives to 35% if two first-degree relatives
Colonoscopy is recommended every 5 Colonoscopy is recommended every 5 years beginning at age 40 years or years beginning at age 40 years or beginning 10 years before the age of the beginning 10 years before the age of the earliest diagnosed patient in the earliest diagnosed patient in the pedigree. pedigree.

ScreeningScreening
Fecal Occult Blood TestingFecal Occult Blood Testing Reduces colorectal cancer mortality by 33% and metastatic cases by 50%. relatively Reduces colorectal cancer mortality by 33% and metastatic cases by 50%. relatively
insensitive, missing up to 50% of cancers and the majority of adenomasinsensitive, missing up to 50% of cancers and the majority of adenomas Specificity VERY low Specificity VERY low Flexible SigmoidoscopyFlexible Sigmoidoscopy Screening by flexible sigmoidoscopy every 5 years may lead to a 60 to 70%Screening by flexible sigmoidoscopy every 5 years may lead to a 60 to 70% Combination of FOBT annually and flexible sigmoidoscopy every 5 yearsCombination of FOBT annually and flexible sigmoidoscopy every 5 yearsColonoscopyColonoscopy Highly sensitive for detecting even small polyps (<1 cm) and allows biopsy, polypectomy, Highly sensitive for detecting even small polyps (<1 cm) and allows biopsy, polypectomy,
control of hemorrhage, and dilation of stricturescontrol of hemorrhage, and dilation of strictures Require mechanical bowel preparation and the discomfort Require mechanical bowel preparation and the discomfort More expensive More expensive Perforation and hemorrhage rare Perforation and hemorrhage rare Air-Contrast Barium EnemaAir-Contrast Barium Enema Highly sensitive for detecting polyps greater than 1 cm Highly sensitive for detecting polyps greater than 1 cm Often is combined with flexible sigmoidoscopy for screening purposes. Often is combined with flexible sigmoidoscopy for screening purposes. Computed Tomographic Colonography (Virtual Colonoscopy)Computed Tomographic Colonography (Virtual Colonoscopy) Helical CT technology and three-dimensional reconstruction Helical CT technology and three-dimensional reconstruction Require a mechanical bowel preparation filled with air Require a mechanical bowel preparation filled with air Sensitivity appears to be as good as colonoscopy Sensitivity appears to be as good as colonoscopy Colonoscopy is required if a lesion is identifiedColonoscopy is required if a lesion is identified False-positive results from retained stool, diverticular disease, haustral folds False-positive results from retained stool, diverticular disease, haustral folds

Current American Cancer Society Current American Cancer Society guidelines advocate screening guidelines advocate screening
Beginning at age 50 yearsBeginning at age 50 years Recommended procedures include: Recommended procedures include:
Yearly FOBTYearly FOBT Flexible sigmoidoscopy every 5 years Flexible sigmoidoscopy every 5 years FOBT and flexible sigmoidoscopy in FOBT and flexible sigmoidoscopy in
combination, combination, Air-contrast barium enema every 5 yearsAir-contrast barium enema every 5 years Colonoscopy every 10 years. Colonoscopy every 10 years.

T stage (depth of invasion) is the single most significant T stage (depth of invasion) is the single most significant predictor of lymph node spread. predictor of lymph node spread.
Even if confined to the bowel wall (T1 and T2) LN metastasis in Even if confined to the bowel wall (T1 and T2) LN metastasis in 5 to 20% of cases5 to 20% of cases
Through the bowel wall or into adjacent organs (T3 and T4) are Through the bowel wall or into adjacent organs (T3 and T4) are likely to have lymph node metastasis in more than 50% likely to have lymph node metastasis in more than 50%
Four or more involved lymph nodes predict a poor prognosis. Four or more involved lymph nodes predict a poor prognosis. Upper rectum, drainage ascends along the superior rectal Upper rectum, drainage ascends along the superior rectal
vessels to the inferior mesenteric nodes. In the lower rectum, vessels to the inferior mesenteric nodes. In the lower rectum, lymphatic drainage may course along the middle rectal lymphatic drainage may course along the middle rectal vessels. vessels.
Most common site of distant metastasis from colorectal cancer Most common site of distant metastasis from colorectal cancer is the liver. is the liver.
Hematogenous spread via the portal venous systemHematogenous spread via the portal venous system Lung #2 siteLung #2 site Carcinomatosis (diffuse peritoneal metastases) Carcinomatosis (diffuse peritoneal metastases)

Preoperative EvaluationPreoperative Evaluation
Evaluated for synchronous tumors, usually by colonoscopy. Evaluated for synchronous tumors, usually by colonoscopy. Synchronous disease (5%) Synchronous disease (5%)
Rectal cancers, digital rectal examination and rigid proctoscopy Rectal cancers, digital rectal examination and rigid proctoscopy Chest/abdominal/pelvic CT scan Chest/abdominal/pelvic CT scan PET scan may be useful in evaluating lesions seen on CT scan, PET scan may be useful in evaluating lesions seen on CT scan, Subtotal or total colectomy should be considered with presence Subtotal or total colectomy should be considered with presence
of synchronous cancers or adenomas or a strong family history of synchronous cancers or adenomas or a strong family history Minimum of 12 lymph nodes in the resected specimen are Minimum of 12 lymph nodes in the resected specimen are
necessary for adequate staging, more nodes are harvested have necessary for adequate staging, more nodes are harvested have better long-term outcomebetter long-term outcome
If unexpected metastatic disease is encountered at the time of a If unexpected metastatic disease is encountered at the time of a laparotomy, the primary tumor should be resected, if technically laparotomy, the primary tumor should be resected, if technically feasible and safe. If primary tumor is not resectable, a palliative feasible and safe. If primary tumor is not resectable, a palliative procedure can be performed and usually involves a proximal procedure can be performed and usually involves a proximal stoma or bypass. stoma or bypass.

Stage-Specific TherapyStage-Specific Therapy
Stage 0 (Tis, N0, M0)Stage 0 (Tis, N0, M0) polyps should be excised completely and pathologic margins should be free of polyps should be excised completely and pathologic margins should be free of
dysplasia. dysplasia. Stage I: The Malignant Polyp (T1, N0, M0)Stage I: The Malignant Polyp (T1, N0, M0)
no stalk involvement resected endoscopically. lymphovascular invasion, poorly no stalk involvement resected endoscopically. lymphovascular invasion, poorly differentiated histology, or tumor within 1 mm of the resection margin differentiated histology, or tumor within 1 mm of the resection margin needsegmental colectomy is then indicated. needsegmental colectomy is then indicated.
Stages I and II: Localized Colon Carcinoma (T1–3, N0, M0)Stages I and II: Localized Colon Carcinoma (T1–3, N0, M0) Adjuvant chemotherapy has been suggested for selected patients with stage II Adjuvant chemotherapy has been suggested for selected patients with stage II
disease (young patients, tumors with "high-risk" histologic findings) (controversial) disease (young patients, tumors with "high-risk" histologic findings) (controversial) Stage III: Lymph Node Metastasis (Tany, N1, M0)Stage III: Lymph Node Metastasis (Tany, N1, M0)
significant risk for both local and distant recurrence, and adjuvant chemotherapy significant risk for both local and distant recurrence, and adjuvant chemotherapy 5-fluorouracil (5-FU)–based regimens (with levamisole or leucovorin) reduce 5-fluorouracil (5-FU)–based regimens (with levamisole or leucovorin) reduce
recurrences and improve survival in this patient populationrecurrences and improve survival in this patient population Stage IV: Distant Metastasis (Tany, Nany, M1)Stage IV: Distant Metastasis (Tany, Nany, M1)
Resectable metastases may benefit from resection Resectable metastases may benefit from resection liver- 20% are potentially resectable for cure. Survival is improved All patients liver- 20% are potentially resectable for cure. Survival is improved All patients
require adjuvant chemotherapy. Lung- long-term survival benefit can be expected require adjuvant chemotherapy. Lung- long-term survival benefit can be expected in 30 to 40%.in 30 to 40%.
Others should be palliation. Others should be palliation. colonic stenting for obstructing lesions of the left colon, diverting stoma.colonic stenting for obstructing lesions of the left colon, diverting stoma.

Therapy for Rectal Therapy for Rectal CarcinomaCarcinoma
More difficult to achieve negative radial margins More difficult to achieve negative radial margins Local recurrence is higher than with similar stage colon cancers. Local recurrence is higher than with similar stage colon cancers. easier to treat rectal tumors with radiation. easier to treat rectal tumors with radiation. Local TherapyLocal Therapy The distal 10 cm of the rectum are accessible transanally. The distal 10 cm of the rectum are accessible transanally. Transanal excision (full thickness or mucosal) is an excellent approach for Transanal excision (full thickness or mucosal) is an excellent approach for
noncircumferential, benign, villous adenomas of the rectum. No LN and high noncircumferential, benign, villous adenomas of the rectum. No LN and high recurrence.recurrence.
Radical ResectionRadical Resection Radical resection is preferred , attempt to obtain a 2-cm distal mural margin for Radical resection is preferred , attempt to obtain a 2-cm distal mural margin for
curative resections.curative resections. Total mesorectal excision (TME) is dissection along anatomic planes to ensure Total mesorectal excision (TME) is dissection along anatomic planes to ensure
complete resection of the rectal mesentery during low and extended low complete resection of the rectal mesentery during low and extended low anterior resections. anterior resections.
Less blood loss and less risk to the pelvic nerves and presacral plexus than is blunt Less blood loss and less risk to the pelvic nerves and presacral plexus than is blunt dissection. dissection.
When the radial margin is threatened or involved, neoadjuvant When the radial margin is threatened or involved, neoadjuvant chemoradiation is recommended.chemoradiation is recommended.
Villous adenomas harboring carcinoma in situ (high-grade dysplasia) are Villous adenomas harboring carcinoma in situ (high-grade dysplasia) are ideally treated with local excision. A 1-cm margin should be obtained. ideally treated with local excision. A 1-cm margin should be obtained.

Stage Specific TherapyStage Specific Therapy
Stage I: Localized Rectal Carcinoma (T1–2, N0, M0)Stage I: Localized Rectal Carcinoma (T1–2, N0, M0) Radical resection is strongly recommended in all good-risk patients. Radical resection is strongly recommended in all good-risk patients. Lesions with unfavorable histologic characteristics and those located in the Lesions with unfavorable histologic characteristics and those located in the
distal third of the rectum, in particular, are prone to recurrence. distal third of the rectum, in particular, are prone to recurrence. Locally Advanced Rectal Cancer (Stages II and III)Locally Advanced Rectal Cancer (Stages II and III)Stage II: Localized Rectal Carcinoma (T3–4, N0, M0)Stage II: Localized Rectal Carcinoma (T3–4, N0, M0) Total mesorectal resection vs stages II and III rectal cancers will benefit from Total mesorectal resection vs stages II and III rectal cancers will benefit from
chemoradiation. chemoradiation. Stage III: Lymph Node Metastasis (Tany, N1, M0)Stage III: Lymph Node Metastasis (Tany, N1, M0) Chemotherapy and radiation either pre- or postoperatively for node-positive Chemotherapy and radiation either pre- or postoperatively for node-positive
rectal cancers. rectal cancers. Both improved local control and prolonged survival, Both improved local control and prolonged survival, Most colorectal surgeons in the United States continue to recommend adjuvant Most colorectal surgeons in the United States continue to recommend adjuvant
or neoadjuvant therapy for patients with locally advanced disease. or neoadjuvant therapy for patients with locally advanced disease. Most surgeons consider preoperative chemoradiation to be the most Most surgeons consider preoperative chemoradiation to be the most
appropriate therapy for locally advanced rectal cancer.75appropriate therapy for locally advanced rectal cancer.75Stage IV: Distant Metastasis (Tany, Nany, M1)Stage IV: Distant Metastasis (Tany, Nany, M1) Resect isolated mets but otherwise palliative procedures (intraluminal stents, Resect isolated mets but otherwise palliative procedures (intraluminal stents,
diverting colostomy) diverting colostomy)

Follow-Up and SurveillanceFollow-Up and Surveillance Colonoscopy should be performed within 12 months after the diagnosis Colonoscopy should be performed within 12 months after the diagnosis
of the original cancer, if normal, colonoscopy should be repeated every of the original cancer, if normal, colonoscopy should be repeated every 3 to 5 years thereafter3 to 5 years thereafter
Re-resection often is technically challenging and highly morbid, with Re-resection often is technically challenging and highly morbid, with only a limited chance of achieving long-term survival. Highest in 2 years only a limited chance of achieving long-term survival. Highest in 2 years
CEA often is followed every 2 to 3 months for 2 years. CEA often is followed every 2 to 3 months for 2 years. Between 20 and 40% for colorectal carcinoma will develop recurrent Between 20 and 40% for colorectal carcinoma will develop recurrent
disease. disease. Sentinel Lymph Node Biopsy for Colorectal Carcinoma can improve Sentinel Lymph Node Biopsy for Colorectal Carcinoma can improve
staging.staging.Minimally Invasive Techniques for ResectionMinimally Invasive Techniques for Resection The Clinical Outcomes of Surgical Therapy Study Group (COST), the The Clinical Outcomes of Surgical Therapy Study Group (COST), the
Colon Carcinoma Laparoscopic or Open Resection (COLOR) trial, and the Colon Carcinoma Laparoscopic or Open Resection (COLOR) trial, and the United Kingdom Medical Research Council Conventional vs. United Kingdom Medical Research Council Conventional vs. Laparoscopic-Assisted Surgery in Colorectal Cancer (CLASSICC) trial Laparoscopic-Assisted Surgery in Colorectal Cancer (CLASSICC) trial have all shown oncologic equivalence between open and laparoscopic have all shown oncologic equivalence between open and laparoscopic techniques. techniques.


Other NeoplasmsOther Neoplasms
Carcinoid TumorsCarcinoid Tumors up to 25% found in the rectum. up to 25% found in the rectum. Most benign, survival is greater than 80%. Most benign, survival is greater than 80%. 60% of tumors greater than 2 cm in diameter distant metastases. 60% of tumors greater than 2 cm in diameter distant metastases. Proximal colon carcinoid usually more aggressive and larger by diagnosis Symptoms of carcinoid Proximal colon carcinoid usually more aggressive and larger by diagnosis Symptoms of carcinoid
syndrome often can be alleviated with somatostatin analogues (octreotide) and/or interferon-syndrome often can be alleviated with somatostatin analogues (octreotide) and/or interferon-LipomasLipomas submucosa of the colon and rectum. submucosa of the colon and rectum. benign lesions, but rarely may cause bleeding, obstruction, or intussusceptionbenign lesions, but rarely may cause bleeding, obstruction, or intussusceptionLymphomaLymphoma rare, but accounts for about 10% of all GI lymphomas. rare, but accounts for about 10% of all GI lymphomas. bleeding and obstructionbleeding and obstruction Bowel resection Bowel resection Leiomyoma Leiomyoma benign tumors benign tumors upper GI tractupper GI tract asymptomatic>> cause bleeding or obstruction. asymptomatic>> cause bleeding or obstruction. should be resected should be resected Recurrence is common Recurrence is common Lesions >5 cm need radical resectionLesions >5 cm need radical resectionLeiomyosarcoma Leiomyosarcoma Rare, rectum is the most common site. Rare, rectum is the most common site. bleeding and obstructionbleeding and obstruction radical resection radical resection

Retrorectal/Presacral TumorsRetrorectal/Presacral Tumors RareRare Often heterogeneousOften heterogeneous Congenital lesions are most commonCongenital lesions are most common Malignancy is more common in the pediatric population Malignancy is more common in the pediatric population Cysts: dermoid and epidermoid, enterogenous, Cysts: dermoid and epidermoid, enterogenous,
meningocele and myelomeningocele meningocele and myelomeningocele Solid lesions include teratomas, chordomas, neurologic Solid lesions include teratomas, chordomas, neurologic
tumors, or osseus lesions. tumors, or osseus lesions. Present with pain (lower back, pelvic, or lower extremity), Present with pain (lower back, pelvic, or lower extremity),
GI symptoms, or urinary tract symptoms. GI symptoms, or urinary tract symptoms. digital rectal examination. pelvic MRI >>CT digital rectal examination. pelvic MRI >>CT Biopsy is not indicatedBiopsy is not indicated surgical resectionsurgical resection

Anal Canal and Perianal Anal Canal and Perianal TumorsTumors
Cancers of the anal canal are uncommon and account for approximately 2% of all colorectal malignancies. Cancers of the anal canal are uncommon and account for approximately 2% of all colorectal malignancies. Major division is the dentate line: anal margin (distal) vs anal canal (proximal), lymphatics Major division is the dentate line: anal margin (distal) vs anal canal (proximal), lymphatics Anal Intraepithelial Neoplasia (Bowen's Disease)Anal Intraepithelial Neoplasia (Bowen's Disease) Bowen's disease refers to squamous cell carcinoma in situ of the anus. Bowen's disease refers to squamous cell carcinoma in situ of the anus. Precursor to an invasive squamous cell carcinoma Precursor to an invasive squamous cell carcinoma Associated with infection with the human papillomavirus (HPV), especially HPV types 16 and 18. Associated with infection with the human papillomavirus (HPV), especially HPV types 16 and 18. high recurrence and/or reinfection ratehigh recurrence and/or reinfection rateEpidermoid CarcinomaEpidermoid Carcinoma cell carcinoma, cloacogenic carcinoma, transitional carcinoma, and basaloid carcinoma. Behave the same cell carcinoma, cloacogenic carcinoma, transitional carcinoma, and basaloid carcinoma. Behave the same slow-growing tumor, and slow-growing tumor, and Mass effect >> pain and bleeding Mass effect >> pain and bleeding Wide local excision Wide local excision Chemotherapy and radiation if simple excision not possible (the Nigro protocol: 5-FU, mitomycin C, and 3000 cGy external Chemotherapy and radiation if simple excision not possible (the Nigro protocol: 5-FU, mitomycin C, and 3000 cGy external
beam radiation)beam radiation) 80% cure80% cure Recurrence usually requires radical resection (APR). Recurrence usually requires radical resection (APR). Verrucous Carcinoma (Buschke-Lowenstein Tumor, Giant Condyloma Acuminata)Verrucous Carcinoma (Buschke-Lowenstein Tumor, Giant Condyloma Acuminata) Verrucous carcinoma is a locally aggressive form of condyloma acuminata. Verrucous carcinoma is a locally aggressive form of condyloma acuminata. Wide local excision Wide local excision Basal Cell CarcinomaBasal Cell Carcinoma Basal cell carcinoma of the anus is rare and resembles basal cell carcinoma elsewhere Basal cell carcinoma of the anus is rare and resembles basal cell carcinoma elsewhere Wide local excision is the treatment of choiceWide local excision is the treatment of choice recurrence occurs in up to 30%recurrence occurs in up to 30%MelanomaMelanoma Anorectal melanoma is rare, comprising less than 1% of all anorectal malignancies and 1 to 2% of melanomas. Anorectal melanoma is rare, comprising less than 1% of all anorectal malignancies and 1 to 2% of melanomas. 5-year survival is less than 10%, 5-year survival is less than 10%, radical resection (APR, no survival advantage) and wide local excision have been advocated. radical resection (APR, no survival advantage) and wide local excision have been advocated. adjuvant chemotherapy, biochemotherapy, vaccines, or radiotherapy may be of benefit in some patients, but efficacy adjuvant chemotherapy, biochemotherapy, vaccines, or radiotherapy may be of benefit in some patients, but efficacy
remains unproven.remains unproven.

Rectal Prolapse and Solitary Rectal Prolapse and Solitary Rectal Ulcer SyndromeRectal Ulcer Syndrome
Women, with a female:male ratio of 6:1. Women, with a female:male ratio of 6:1. Age, peaks in the seventh decade of life. Age, peaks in the seventh decade of life. Incontinence and diarrhea to constipation and outlet Incontinence and diarrhea to constipation and outlet
obstruction.obstruction. Colonoscopy or air-contrast barium enema to exclude Colonoscopy or air-contrast barium enema to exclude
neoplasms or diverticular disease. neoplasms or diverticular disease. Abdominal rectopexy (with or without sigmoid Abdominal rectopexy (with or without sigmoid
resection) offers the most durable repair, with resection) offers the most durable repair, with recurrence occurring in fewer than 10% of patients. recurrence occurring in fewer than 10% of patients.
Perineal rectosigmoidectomy avoids an abdominal Perineal rectosigmoidectomy avoids an abdominal operation preferable in high-risk patientsoperation preferable in high-risk patients


VolvulusVolvulus
Air-filled segment of the colon twists about its Air-filled segment of the colon twists about its mesentery. The sigmoid colon is involved in mesentery. The sigmoid colon is involved in up to 90% >> cecum (<20%) or transverse up to 90% >> cecum (<20%) or transverse colon. colon.
Reduce spontaneously, bowel obstruction, Reduce spontaneously, bowel obstruction, strangulation, gangrene, and perforation. strangulation, gangrene, and perforation.
Abdominal distention, nausea, and vomiting. Abdominal distention, nausea, and vomiting. Fever and leukocytosis are heralds of Fever and leukocytosis are heralds of
gangrene and/or perforation. gangrene and/or perforation. History of intermittent obstructive symptoms History of intermittent obstructive symptoms
and distention, suggesting intermittent and distention, suggesting intermittent chronic volvulus.chronic volvulus.

Sigmoid VolvulusSigmoid Volvulus
Characteristic bent inner tube, convexity of the loop lying in Characteristic bent inner tube, convexity of the loop lying in the right upper quadrant the right upper quadrant
Gastrografin enema shows a narrowing at the site of the Gastrografin enema shows a narrowing at the site of the volvulus and a pathognomonic bird's beak volvulus and a pathognomonic bird's beak
Unless gangrene or peritonitis, resuscitation followed by Unless gangrene or peritonitis, resuscitation followed by endoscopic detorsion with rigid proctoscope > flexible endoscopic detorsion with rigid proctoscope > flexible sigmoidoscope/colonoscope sigmoidoscope/colonoscope
Rectal tube may be inserted to maintain decompression. Rectal tube may be inserted to maintain decompression. Recurrence is high (40%) Recurrence is high (40%) Elective sigmoid colectomy after stabilized & bowel Elective sigmoid colectomy after stabilized & bowel
preparation.preparation. Clinical evidence of gangrene or perforation mandates Clinical evidence of gangrene or perforation mandates
immediate surgical exploration without an attempt at immediate surgical exploration without an attempt at endoscopic decompression. endoscopic decompression.
Sigmoid colectomy with end colostomy Sigmoid colectomy with end colostomy

Cecal VolvulusCecal Volvulus
Rotation occurs around the ileocolic blood Rotation occurs around the ileocolic blood vessels and vascular impairment occurs early. vessels and vascular impairment occurs early.
Kidney-shaped, air-filled structure in the left Kidney-shaped, air-filled structure in the left upper quadrant upper quadrant
Can almost never be detorsed endoscopically. Can almost never be detorsed endoscopically. Surgical exploration is necessary at diagnosis Surgical exploration is necessary at diagnosis Right hemicolectomy with a primary ileocolic Right hemicolectomy with a primary ileocolic
anastomosis anastomosis

MegacolonMegacolon
chronically dilated, elongated, hypertrophied large chronically dilated, elongated, hypertrophied large bowel. bowel.
congenital or acquired and usually is related to congenital or acquired and usually is related to chronic mechanical or functional obstruction. chronic mechanical or functional obstruction.
must exclude a surgically correctable mechanical must exclude a surgically correctable mechanical obstruction.obstruction.
Hirschsprung's disease (neural crest cells) Hirschsprung's disease (neural crest cells) infection or chronic constipation. (Chagas' disease) infection or chronic constipation. (Chagas' disease) neurologic disorders neurologic disorders Diverting ileostomy or subtotal colectomy with an Diverting ileostomy or subtotal colectomy with an
ileorectal anastomosis is occasionally necessaryileorectal anastomosis is occasionally necessary

Colonic Pseudo-Obstruction Colonic Pseudo-Obstruction (Ogilvie's Syndrome)(Ogilvie's Syndrome)
Disorder in which the colon becomes massively dilated in the Disorder in which the colon becomes massively dilated in the absence of mechanical obstruction. absence of mechanical obstruction.
Most commonly occurs in hospitalized patients Most commonly occurs in hospitalized patients Associated with the use of narcotics, bedrest, and comorbid Associated with the use of narcotics, bedrest, and comorbid
disease. disease. Cassive dilatation of the colon (usually predominantly the Cassive dilatation of the colon (usually predominantly the
right and transverse colon) in the absence of a mechanical right and transverse colon) in the absence of a mechanical obstruction. obstruction.
Cessation of narcotics, anticholinergics, or other medications Cessation of narcotics, anticholinergics, or other medications Strict bowel rest and IV hydration are crucial. Strict bowel rest and IV hydration are crucial. IV neostigmine > colonoscopic decompression often is IV neostigmine > colonoscopic decompression often is
effective. effective. Crucial to exclude mechanical obstruction (usually with a Crucial to exclude mechanical obstruction (usually with a
Gastrografin or barium enema) before medical or endoscopic Gastrografin or barium enema) before medical or endoscopic treatment treatment

Ischemic ColitisIschemic Colitis
Most commonly in the colonMost commonly in the colon Predominately low flow and/or small vessel occlusion. Predominately low flow and/or small vessel occlusion. Vascular disease, diabetes mellitus, vasculitis, and hypotension. Vascular disease, diabetes mellitus, vasculitis, and hypotension. Ligation of the inferior mesenteric artery during aortic surgery Ligation of the inferior mesenteric artery during aortic surgery Splenic flexure is the most common (water shed area)Splenic flexure is the most common (water shed area) Mild cases, patients may have diarrhea (usually bloody) without pain. Mild cases, patients may have diarrhea (usually bloody) without pain. Severe ischemia with intense abdominal pain (often out of proportion to the Severe ischemia with intense abdominal pain (often out of proportion to the
clinical examination), tenderness, fever, and leukocytosis clinical examination), tenderness, fever, and leukocytosis Diagnosis - clinical history and physical examination. Diagnosis - clinical history and physical examination. CT often shows nonspecific colonic wall thickening and pericolic fat CT often shows nonspecific colonic wall thickening and pericolic fat
stranding. stranding. Sigmoidoscopy is relatively contraindicated Sigmoidoscopy is relatively contraindicated Majority can be treated medically 80% Majority can be treated medically 80% Bowel rest and broad-spectrum antibiotics are the mainstay of therapy, Bowel rest and broad-spectrum antibiotics are the mainstay of therapy, Colonoscopy should be performed after recovery Colonoscopy should be performed after recovery Failure to improve after 2 to 3 days of medical management, progression of Failure to improve after 2 to 3 days of medical management, progression of
symptoms, or deterioration -> surgical explorationsymptoms, or deterioration -> surgical exploration Primary anastomosis should be avoided Primary anastomosis should be avoided

Pseudomembranous Colitis Pseudomembranous Colitis (Clostridium difficile Colitis)(Clostridium difficile Colitis)
Extremely common, leading cause of nosocomially acquired Extremely common, leading cause of nosocomially acquired diarrheadiarrhea
Result from overgrowth Result from overgrowth Almost any antibiotic, even a single dose Almost any antibiotic, even a single dose Immunosuppression, medical comorbidities, prolonged Immunosuppression, medical comorbidities, prolonged
hospitalization or nursing home residence, and bowel hospitalization or nursing home residence, and bowel surgery increase the risk.surgery increase the risk.
Two toxins: toxin A (an enterotoxin) and toxin B (a cytotoxin)Two toxins: toxin A (an enterotoxin) and toxin B (a cytotoxin) Management : immediate cessation of the offending Management : immediate cessation of the offending
antimicrobial agent. Patients with mild disease10-day course antimicrobial agent. Patients with mild disease10-day course of oral metronidazole. of oral metronidazole.
Severe diarrhea associated fever and abdominal pain - bowel Severe diarrhea associated fever and abdominal pain - bowel rest, IV hydration, and oral metronidazole or vancomycinrest, IV hydration, and oral metronidazole or vancomycin
Fulminant colitis -> emergent laparotomy, total abdominal Fulminant colitis -> emergent laparotomy, total abdominal colectomy with end ileostomy colectomy with end ileostomy

Anorectal Diseases Anorectal Diseases

HemorrhoidsHemorrhoids
Cushions of submucosal tissue containing venules, arterioles, and Cushions of submucosal tissue containing venules, arterioles, and smooth-muscle fibers smooth-muscle fibers
Left lateral, right anterior, and right posterior positionsLeft lateral, right anterior, and right posterior positions Treatment is only indicated if they become symptomaticTreatment is only indicated if they become symptomatic Straining, increased abdominal pressure, and hard stools increase Straining, increased abdominal pressure, and hard stools increase
venous engorgement venous engorgement External hemorrhoids distal to the dentate line, thrombosis leads to External hemorrhoids distal to the dentate line, thrombosis leads to
significant pain (anoderm sensate)significant pain (anoderm sensate) Internal hemorrhoids proximal to the dentate line, insensate Internal hemorrhoids proximal to the dentate line, insensate Prolapse or bleed, but rarely become painful Prolapse or bleed, but rarely become painful Combined internal and external hemorrhoids straddle the dentate Combined internal and external hemorrhoids straddle the dentate
line and have characteristics of both internal and external line and have characteristics of both internal and external hemorrhoidshemorrhoids
Surgery required for large, symptomatic, combined hemorrhoids Surgery required for large, symptomatic, combined hemorrhoids Hemorrhoidectomy is often the treatment of choiceHemorrhoidectomy is often the treatment of choice Rectal varices are best treated by lowering portal venous pressure Rectal varices are best treated by lowering portal venous pressure Surgical hemorrhoidectomy should be avoided Surgical hemorrhoidectomy should be avoided

TreatmentTreatment
Medical TherapyMedical Therapy First- and second-degree hemorrhoids - dietary fiber, stool softeners, increased fluid intake, and First- and second-degree hemorrhoids - dietary fiber, stool softeners, increased fluid intake, and
avoidance of straining. avoidance of straining. Rubber band ligation, infrared photocoagulation, Rubber band ligation, infrared photocoagulation, Sclerotherapy for first-, second-, and some third-degree hemorrhoids. Sclerotherapy for first-, second-, and some third-degree hemorrhoids. Excision Excision Thrombosed External HemorrhoidsThrombosed External Hemorrhoids Elliptical excision Elliptical excision Operative HemorrhoidectomyOperative Hemorrhoidectomy Closed Submucosal HemorrhoidectomyClosed Submucosal Hemorrhoidectomy Redundant mucosa are identified and excised using an elliptical incision starting just distal to the anal Redundant mucosa are identified and excised using an elliptical incision starting just distal to the anal
verge and extending proximally to the anorectal ring and the apex of the hemorrhoidal plexus is then verge and extending proximally to the anorectal ring and the apex of the hemorrhoidal plexus is then ligatedligated
Identify the fibers of the internal sphincter and avoid themIdentify the fibers of the internal sphincter and avoid them Close with a running absorbable suture or can be left open Close with a running absorbable suture or can be left open Stapled HemorrhoidectomyStapled Hemorrhoidectomy removes a short circumferential segment of rectal mucosa proximal to the dentate line using a circular removes a short circumferential segment of rectal mucosa proximal to the dentate line using a circular
stapler. stapler. Complications of HemorrhoidectomyComplications of Hemorrhoidectomy Urinary retention 10 to 50% of patientsUrinary retention 10 to 50% of patients Fecal impaction Fecal impaction Hemorrhage Hemorrhage Incontinence Incontinence Anal stenosis Anal stenosis

Anal FissureAnal Fissure
Tear in the anoderm distal to the dentate line. Tear in the anoderm distal to the dentate line. Trauma from either the passage of hard stool or prolonged diarrhea. Trauma from either the passage of hard stool or prolonged diarrhea. Causes spasm of the internal anal sphincter -> pain, increased Causes spasm of the internal anal sphincter -> pain, increased
tearing, and decreased blood supply tearing, and decreased blood supply Majority of anal fissures occur in the posterior midline. Ten to 15% Majority of anal fissures occur in the posterior midline. Ten to 15%
occur in the anterior midline. occur in the anterior midline. Extremely commonExtremely common Pain with defecation and hematochezia Pain with defecation and hematochezia Intense and painful anal spasm lasting for several hours after a BMIntense and painful anal spasm lasting for several hours after a BM Acute fissure is a superficial tear of the distal anoderm and almost Acute fissure is a superficial tear of the distal anoderm and almost
always heals with medical management. always heals with medical management. Chronic fissures develop ulceration and heaped-up edges with the Chronic fissures develop ulceration and heaped-up edges with the
white fibers of the internal anal sphincter visible at the base of the white fibers of the internal anal sphincter visible at the base of the ulcer, often is an associated external skin tag and/or a ulcer, often is an associated external skin tag and/or a hypertrophied anal papilla internally. hypertrophied anal papilla internally.
Lateral location, not normal, think Crohn's disease, HIV, syphilis, etc. Lateral location, not normal, think Crohn's disease, HIV, syphilis, etc.

TreatmentTreatment
Bulk agents, stool softeners, and warm sitz baths, Bulk agents, stool softeners, and warm sitz baths, 2% lidocaine jelly 2% lidocaine jelly
Nitroglycerin ointmentNitroglycerin ointment Calcium channel blockers (diltiazem and nifedipine)Calcium channel blockers (diltiazem and nifedipine) Effective in most acute fissures, but will heal only Effective in most acute fissures, but will heal only
approximately 50 to 60% of chronic fissuresapproximately 50 to 60% of chronic fissures Botulinum toxin Botulinum toxin Alternative to surgical sphincterotomy for chronic fissure. Alternative to surgical sphincterotomy for chronic fissure. Surgical therapy traditionally has been recommended for Surgical therapy traditionally has been recommended for
chronic fissures that have failed medical therapy, and chronic fissures that have failed medical therapy, and lateral internal sphincterotomy is the procedure of choice lateral internal sphincterotomy is the procedure of choice
30% of the internal sphincter fibers are divided 30% of the internal sphincter fibers are divided Healing is achieved in more than 95% Healing is achieved in more than 95%

Anorectal Sepsis and Anorectal Sepsis and Cryptoglandular AbscessCryptoglandular Abscess
Infections of the anal glands (cryptoglandular infection) Infections of the anal glands (cryptoglandular infection) found in the intersphincteric plane. found in the intersphincteric plane. These glands traverse the internal sphincter and empty into These glands traverse the internal sphincter and empty into
the anal crypts at the level of the dentate line. the anal crypts at the level of the dentate line. DiagnosisDiagnosis Severe anal pain Severe anal pain Palpable mass Palpable mass CT or MRI to fully delineate the anatomy of the abscess.CT or MRI to fully delineate the anatomy of the abscess.TreatmentTreatment Drainage as soon as the diagnosis is established. Drainage as soon as the diagnosis is established. Examination under anesthesia Examination under anesthesia Antibiotics only if overlying cellulitis or if the patient is Antibiotics only if overlying cellulitis or if the patient is
immunocompromised, has diabetes mellitus, or has immunocompromised, has diabetes mellitus, or has valvular heart disease. valvular heart disease.

Ischiorectal AbscessesIschiorectal Abscesses Horseshoe abscesses require drainage of the deep postanal space and often Horseshoe abscesses require drainage of the deep postanal space and often
require counterincisions over one or both ischiorectal spaces require counterincisions over one or both ischiorectal spaces Intersphincteric AbscessIntersphincteric Abscess Intersphincteric abscesses - difficult to diagnose, few external signsIntersphincteric abscesses - difficult to diagnose, few external signs deep pain that is more internal feelingdeep pain that is more internal feeling worse with coughing or sneezing worse with coughing or sneezing pain limits DRE usually requires an examination under anesthesia pain limits DRE usually requires an examination under anesthesia drain through a limited, usually posterior, internal sphincterotomydrain through a limited, usually posterior, internal sphincterotomySupralevator AbscessSupralevator Abscess uncommonuncommon can mimic intra-abdominal conditions (high location)can mimic intra-abdominal conditions (high location) DRE may reveal an indurated, bulging mass above the anorectal ringDRE may reveal an indurated, bulging mass above the anorectal ring It is essential to identify the origin - secondary to an upward extension of an It is essential to identify the origin - secondary to an upward extension of an
intersphincteric abscess, drain via rectum.intersphincteric abscess, drain via rectum. upward extension of an ischiorectal abscess drain through the ischiorectal upward extension of an ischiorectal abscess drain through the ischiorectal
fossa. fossa. If from intra-abdominal disease primary process treatment and drainage via the If from intra-abdominal disease primary process treatment and drainage via the
most direct route (transabdominally, rectally, or through the ischiorectal fossa). most direct route (transabdominally, rectally, or through the ischiorectal fossa).

Necrotizing Soft Tissue Necrotizing Soft Tissue Infection of the PerineumInfection of the Perineum
Rare, but lethal, conditionRare, but lethal, condition Polymicrobial and synergisticPolymicrobial and synergistic Undrained or inadequately drained cryptoglandular abscess Undrained or inadequately drained cryptoglandular abscess
or a urogenital infection, or post opor a urogenital infection, or post op Immunocomprimised patients and diabetic patients are at Immunocomprimised patients and diabetic patients are at
increased riskincreased risk Necrotic skin, bullae, or crepitus and systemic toxicity and Necrotic skin, bullae, or crepitus and systemic toxicity and
may be hemodynamically unstablemay be hemodynamically unstable Prompt surgical débridement of all nonviable tissue is Prompt surgical débridement of all nonviable tissue is
required, including multiple operations required, including multiple operations Broad-spectrum antibiotics Broad-spectrum antibiotics Colostomy with extensive resection of the sphincter or stool Colostomy with extensive resection of the sphincter or stool
contamination of woundcontamination of wound Mortality approximately 50%.Mortality approximately 50%.

Fistula in AnoFistula in Ano
50% abscesses develop a persistent fistula in ano. 50% abscesses develop a persistent fistula in ano. Originates in the infected crypt (internal opening) and tracks to Originates in the infected crypt (internal opening) and tracks to
the external opening, usually the site of prior drainage. the external opening, usually the site of prior drainage. Fistulas are cryptoglandular in origin, trauma, Crohn's disease, Fistulas are cryptoglandular in origin, trauma, Crohn's disease,
malignancy, radiation, or unusual infections (tuberculosis, malignancy, radiation, or unusual infections (tuberculosis, actinomycosis, and chlamydia) = complex, recurrent, or actinomycosis, and chlamydia) = complex, recurrent, or nonhealing fistula.nonhealing fistula.
Persistent drainage from openings. Indurated tract often palpable. Persistent drainage from openings. Indurated tract often palpable. Goodsall's rule - guide in determining the location of the internal Goodsall's rule - guide in determining the location of the internal
opening opening External opening anteriorly connect to the internal opening by a External opening anteriorly connect to the internal opening by a
short, radial tract. short, radial tract. External opening posteriorly track in a curvilinear fashion to the External opening posteriorly track in a curvilinear fashion to the
posterior midline posterior midline Exceptions -anterior external opening is greater than 3 cm from Exceptions -anterior external opening is greater than 3 cm from
the anal margin, usually track to the posterior midline. the anal margin, usually track to the posterior midline.


TreatmentTreatment
The goal of treatment of fistula in ano is eradication of sepsis The goal of treatment of fistula in ano is eradication of sepsis without sacrificing continence. without sacrificing continence.
Encircle variable amounts of the sphincter complex Encircle variable amounts of the sphincter complex Internal opening can be ID'd with hydrogen peroxide or dilute Internal opening can be ID'd with hydrogen peroxide or dilute
methylene bluemethylene blue Simple intersphincteric fistulas often can be treated by Simple intersphincteric fistulas often can be treated by
fistulotomy, curettage, and healing by secondary intention fistulotomy, curettage, and healing by secondary intention Fistulas that include less than 30% of the sphincter muscles often Fistulas that include less than 30% of the sphincter muscles often
can be treated by sphincterotomy can be treated by sphincterotomy High transsphincteric and suprasphincteric fistulas, which encircle High transsphincteric and suprasphincteric fistulas, which encircle
a greater amount of muscle, are more safely treated by initial a greater amount of muscle, are more safely treated by initial placement of a seton placement of a seton
Higher fistulas may be treated by an endorectal advancement flapHigher fistulas may be treated by an endorectal advancement flap Fibrin glue and a variety of collagen-based plugs Fibrin glue and a variety of collagen-based plugs All fistulas resulting from radiation should be biopsied to rule out All fistulas resulting from radiation should be biopsied to rule out
cancer cancer

Human PapillomavirusHuman Papillomavirus
HPV causes condyloma acuminata (anogenital warts) HPV causes condyloma acuminata (anogenital warts) and is associated with AIN and squamous cell and is associated with AIN and squamous cell carcinoma (see Anal Canal and Perianal Tumors carcinoma (see Anal Canal and Perianal Tumors above). above).
HPV types 16 and 18, predispose to malignancy and HPV types 16 and 18, predispose to malignancy and often cause flat dysplasia in skin unaffected by wartsoften cause flat dysplasia in skin unaffected by warts
Small warts on the perianal skin and distal anal canal Small warts on the perianal skin and distal anal canal may be treated in the office with topical application of may be treated in the office with topical application of bichloracetic acid or podophyllin. Although 60 to 80% bichloracetic acid or podophyllin. Although 60 to 80% of patients will respond to these agents, recurrence of patients will respond to these agents, recurrence and reinfection are commonand reinfection are common
Larger and/or more numerous warts require excision Larger and/or more numerous warts require excision and/or fulguration in the operating room. Excised warts and/or fulguration in the operating room. Excised warts should be sent for pathologic examination to rule out should be sent for pathologic examination to rule out dysplasia or malignancy dysplasia or malignancy

TraumaTrauma
Penetrating Colorectal InjuryPenetrating Colorectal Injury Trauma surgeons are increasingly performing primary repairs in Trauma surgeons are increasingly performing primary repairs in
selected patientsselected patients Contraindications to primary repair include shock, injury to more Contraindications to primary repair include shock, injury to more
than two other organs, mesenteric vascular damage, and than two other organs, mesenteric vascular damage, and extensive fecal contaminationextensive fecal contamination
Majority of penetrating rectal injuries should be treated with Majority of penetrating rectal injuries should be treated with proximal fecal diversion and copious irrigation of the rectum proximal fecal diversion and copious irrigation of the rectum
Intractable rectal bleeding may require angiographic embolizationIntractable rectal bleeding may require angiographic embolizationBlunt Colorectal InjuryBlunt Colorectal Injury Less common than penetrating injury. Management of these Less common than penetrating injury. Management of these
injuries should follow the same principles injuries should follow the same principles A A serosal hematomaserosal hematoma alone does alone does not mandate resectionnot mandate resection Crush injuries, require débridement of all nonviable tissue, Crush injuries, require débridement of all nonviable tissue,
proximal fecal diversion, and a distal rectal washout, with or proximal fecal diversion, and a distal rectal washout, with or without drain placement. without drain placement.

Anal Sphincter InjuryAnal Sphincter Injury
Obstetric trauma>> hemorrhoidectomy, Obstetric trauma>> hemorrhoidectomy, sphincterotomy, abscess drainage, or fistulotomy. sphincterotomy, abscess drainage, or fistulotomy. Patients with incontinence and a suspected sphincter Patients with incontinence and a suspected sphincter injury can be evaluated with anal manometry, EMG, injury can be evaluated with anal manometry, EMG, and endoanal ultrasound.and endoanal ultrasound.
Mild- may respond to dietary changes and/or Mild- may respond to dietary changes and/or biofeedback. biofeedback.
Isolated sphincter injury -> repair primarily. Isolated sphincter injury -> repair primarily. Rectal injury accompanied by sphincter injury -> fecal Rectal injury accompanied by sphincter injury -> fecal
diversion, distal rectal washout, and drain placement.diversion, distal rectal washout, and drain placement. Most common method of repair of the anal sphincter Most common method of repair of the anal sphincter
is a wrap-around sphincteroplasty is a wrap-around sphincteroplasty

Human Immunodeficiency Human Immunodeficiency VirusVirus
Diarrhea, in particular, is extremely common. Diarrhea, in particular, is extremely common. Opportunistic infections with bacteria (Salmonella, Shigella, Opportunistic infections with bacteria (Salmonella, Shigella,
Campylobacter, Chlamydia, and Mycobacterium species), fungi Campylobacter, Chlamydia, and Mycobacterium species), fungi (Histoplasmosis, Coccidiosis, Cryptococcus), protozoa (Toxoplasmosis, (Histoplasmosis, Coccidiosis, Cryptococcus), protozoa (Toxoplasmosis, Cryptosporidiosis, Isosporiasis), and viruses (CMV, herpes simplex Cryptosporidiosis, Isosporiasis), and viruses (CMV, herpes simplex virus) can cause diarrhea, abdominal pain, and weight loss. virus) can cause diarrhea, abdominal pain, and weight loss.
CMVCMV in particular may cause in particular may cause severe enterocolitissevere enterocolitis and is the most and is the most common infectious cause of emergency laparotomy in AIDS patients. common infectious cause of emergency laparotomy in AIDS patients.
C. difficile colitis is a major concern in these patients, especially C. difficile colitis is a major concern in these patients, especially because many patients are maintained on suppressive antibiotic because many patients are maintained on suppressive antibiotic therapy. therapy.
The incidence of GI malignancy also is increased in patients with HIV The incidence of GI malignancy also is increased in patients with HIV infection. infection. Kaposi's sarcomaKaposi's sarcoma is the most common malignancy in AIDS is the most common malignancy in AIDS patients and can affect any part of the GI tract. patients and can affect any part of the GI tract.
asymptomatic or may develop bleeding or obstruction.asymptomatic or may develop bleeding or obstruction. GI lymphoma (usually non-Hodgkin's lymphoma) also is commonGI lymphoma (usually non-Hodgkin's lymphoma) also is common