CNS & Neurological Disorders - Drug Targets , 2007,...
14
CNS & Neurological Disorders - Drug Targets, 2007, 6, 205-218 205 1871-5273/07 $50. 00+. 00 © 2007 Bentham Science Publishers Ltd. Adult Hippocampal Neurogenesis as Target for the Treatment of Depression Michael R. Drew *,1,2 and Rene Hen 1,2,3 1 Center for Neurobiology and Behavior, Columbia University, USA 2 Division of Integrative Neuroscience, New York State Psychiatric Institute, USA 3 Department of Pharmacology, Columbia University, USA Abstract: The dentate gyrus (DG) is one of only two brain structures known to retain the ability to produce new neurons in adulthood. The functional significance of adult neurogenesis in the DG is not yet well understood, but recent evidence has implicated adult neurogenesis in the etiology and treatment of depression. Elevated stress hormone levels, which are present in some depressed patients and can precipitate the onset of depression, reduce neurogenesis in animal models. Conversely, virtually all antidepressant treatments studied to date, including drugs of various classes, electroconvulsive therapy, and behavioral treatments, increase neurogenesis in the DG. We critically review this literature linking DG neu- rogenesis with depression, looking to both animal and human studies. We conclude that a reduction in neurogenesis by it- self is not likely to produce depression. However, at least some therapeutic effects of antidepressant treatments appear to be neurogenesis-dependent. We review the cellular pathways through which antidepressant drugs boost neurogenesis and present several hypotheses about how DG neurogenesis may be instrumental in the therapeutic effects of these drugs. 1. INTRODUCTION For most of the history of neuroscience, the consensus view was that no new neurons are created in the adult central nervous system (see [1] for review). This view began to be seriously challenged beginning in the 1960’s by the work of Altman [2] and later by Kaplan [3] and others, but it was not until the 1990’s that adult neurogenesis became accepted as a bona fide phenomenon. This sea change was due in large part to advances in technology, such as the development of immunohistochemical techniques for labeling dividing cells and identifying cells as neurons [1]. Using these technolo- gies, researchers produced convincing evidence that neuro- genesis occurs in adults of numerous mammalian species, including rodents [4], new-[5] and old-world [6, 7] primates, and humans [8]. In adult mammals neurogenesis occurs primarily in two germinal zones: the subgranular zone (SGZ) of the dentate gyrus (DG) (Fig. 1) and the subventricular zone (SVZ). In humans, only SGZ neurogenesis has been conclusively dem- onstrated [8]. In non-human animals constitutive neurogene- sis has also been reported in neocortex [9, 10], striatum [10], substantia nigra [11], olfactory bulb [12], and hypothalamus [13], but neurogenesis in these regions remains controversial [14-16]. The majority of neurons born in SVZ migrate along the rostral migratory stream to the olfactory bulb where they differentiate into granule and periglomerular inhibitory neu- rons [17]. Neurons born in the SGZ migrate into the granule cell layer of DG where they mature into granule cells that extend axons to the CA3 hippocampal subfield and receive functional synaptic inputs from the perforant path [18-21]. *Address correspondence to this author at the 1051 Riverside Drive, Unit 87, Kolb Annex Rm. 767, New York, NY 10025, USA; Tel: 212-543-5477; E-mail: [email protected] The realization that the adult brain generates new neu- rons has created great excitement. There is the possibility that adult neurogenesis represents a previously unknown form of brain plasticity. As such, adult neurogenesis may mediate forms of learning and memory or other kinds of ex- perience-dependent adaptations [17, 22]. There is also hope that adult neurogenesis can be harnessed to promote recov- ery after brain injury. The fact that adult-born neurons inte- grate into the existing DG circuitry provides proof of princi- ple that functional neurons can be created in the adult brain, and the comparative study of neurogenic versus non- neurogenic regions of the brain will help to identify the par- ticular features and signals that promote new nerve growth in the adult brain. Finally, there has recently been great interest in a possible connection between neurogenesis and depres- sion. It has been proposed that reductions in adult SGZ neu- rogenesis play a causal role in the etiology of depression [23]. There is also evidence that antidepressant (AD) drugs act by increasing SGZ neurogenesis [24]. This review will critically examine the evidence of a link between depression and neurogenesis. Particular attention will be paid to the hypothesis that increased SGZ neurogene- sis is a mechanism of action of AD treatments. After briefly discussing experimental methods for assaying neurogenesis, we examine evidence linking hippocampus (Hp) to emotion and depression. There is evidence that Hp volume is reduced in depressed patients, and some have speculated that a reduc- tion in SGZ neurogenesis may be the cause. We assess the evidence that Hp neurogenesis is reduced in depressed pa- tients, looking to postmortem histological studies and in vivo studies examining links among depression, stress, and neu- rogenesis. Then we turn primarily to animal data to address whether reductions in SGZ neurogenesis are sufficient to bring about depressive symptoms and whether increases in SGZ neurogenesis underlie the therapeutic effects of AD treatments. Finally, we provide a brief overview of the cellu-
Transcript of CNS & Neurological Disorders - Drug Targets , 2007,...

CNS & Neurological Disorders - Drug Targets, 2007, 6, 205-218 205
1871-5273/07 $50. 00+. 00 © 2007 Bentham Science Publishers Ltd.
Adult Hippocampal Neurogenesis as Target for the Treatment of Depression
Michael R. Drew*,1,2
and Rene Hen1,2,3
1Center for Neurobiology and Behavior, Columbia University, USA
2Division of Integrative Neuroscience, New York State Psychiatric Institute, USA
3Department of Pharmacology, Columbia University, USA
Abstract: The dentate gyrus (DG) is one of only two brain structures known to retain the ability to produce new neurons
in adulthood. The functional significance of adult neurogenesis in the DG is not yet well understood, but recent evidence
has implicated adult neurogenesis in the etiology and treatment of depression. Elevated stress hormone levels, which are
present in some depressed patients and can precipitate the onset of depression, reduce neurogenesis in animal models.
Conversely, virtually all antidepressant treatments studied to date, including drugs of various classes, electroconvulsive
therapy, and behavioral treatments, increase neurogenesis in the DG. We critically review this literature linking DG neu-
rogenesis with depression, looking to both animal and human studies. We conclude that a reduction in neurogenesis by it-
self is not likely to produce depression. However, at least some therapeutic effects of antidepressant treatments appear to
be neurogenesis-dependent. We review the cellular pathways through which antidepressant drugs boost neurogenesis and
present several hypotheses about how DG neurogenesis may be instrumental in the therapeutic effects of these drugs.
1. INTRODUCTION
For most of the history of neuroscience, the consensus view was that no new neurons are created in the adult central nervous system (see [1] for review). This view began to be seriously challenged beginning in the 1960’s by the work of Altman [2] and later by Kaplan [3] and others, but it was not until the 1990’s that adult neurogenesis became accepted as a bona fide phenomenon. This sea change was due in large part to advances in technology, such as the development of immunohistochemical techniques for labeling dividing cells and identifying cells as neurons [1]. Using these technolo-gies, researchers produced convincing evidence that neuro-genesis occurs in adults of numerous mammalian species, including rodents [4], new-[5] and old-world [6, 7] primates, and humans [8].
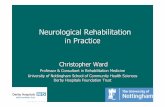
In adult mammals neurogenesis occurs primarily in two germinal zones: the subgranular zone (SGZ) of the dentate gyrus (DG) (Fig. 1) and the subventricular zone (SVZ). In humans, only SGZ neurogenesis has been conclusively dem-onstrated [8]. In non-human animals constitutive neurogene-sis has also been reported in neocortex [9, 10], striatum [10], substantia nigra [11], olfactory bulb [12], and hypothalamus [13], but neurogenesis in these regions remains controversial [14-16]. The majority of neurons born in SVZ migrate along the rostral migratory stream to the olfactory bulb where they differentiate into granule and periglomerular inhibitory neu-rons [17]. Neurons born in the SGZ migrate into the granule cell layer of DG where they mature into granule cells that extend axons to the CA3 hippocampal subfield and receive functional synaptic inputs from the perforant path [18-21].
*Address correspondence to this author at the 1051 Riverside Drive, Unit
87, Kolb Annex Rm. 767, New York, NY 10025, USA; Tel: 212-543-5477;
E-mail: [email protected]
The realization that the adult brain generates new neu-rons has created great excitement. There is the possibility that adult neurogenesis represents a previously unknown form of brain plasticity. As such, adult neurogenesis may mediate forms of learning and memory or other kinds of ex-perience-dependent adaptations [17, 22]. There is also hope that adult neurogenesis can be harnessed to promote recov-ery after brain injury. The fact that adult-born neurons inte-grate into the existing DG circuitry provides proof of princi-ple that functional neurons can be created in the adult brain, and the comparative study of neurogenic versus non-neurogenic regions of the brain will help to identify the par-ticular features and signals that promote new nerve growth in the adult brain. Finally, there has recently been great interest in a possible connection between neurogenesis and depres-sion. It has been proposed that reductions in adult SGZ neu-rogenesis play a causal role in the etiology of depression [23]. There is also evidence that antidepressant (AD) drugs act by increasing SGZ neurogenesis [24].
This review will critically examine the evidence of a link between depression and neurogenesis. Particular attention will be paid to the hypothesis that increased SGZ neurogene-sis is a mechanism of action of AD treatments. After briefly discussing experimental methods for assaying neurogenesis, we examine evidence linking hippocampus (Hp) to emotion and depression. There is evidence that Hp volume is reduced in depressed patients, and some have speculated that a reduc-tion in SGZ neurogenesis may be the cause. We assess the evidence that Hp neurogenesis is reduced in depressed pa-tients, looking to postmortem histological studies and in vivo studies examining links among depression, stress, and neu-rogenesis. Then we turn primarily to animal data to address whether reductions in SGZ neurogenesis are sufficient to bring about depressive symptoms and whether increases in SGZ neurogenesis underlie the therapeutic effects of AD treatments. Finally, we provide a brief overview of the cellu-

206 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
lar pathways that regulate SGZ neurogenesis and the mecha-nisms through which AD drugs boost neurogenesis.
2. ASSAYING NEUROGENESIS
2.1. Biological Significance of Neurogenesis
Before going into the evidence for a link between SGZ neurogenesis and depression, it is worth considering whether neurogenesis in the adult is sufficiently robust to render a functional role such as this plausible. In the rat, the species for which the best data are available, it is estimated that 9000 new cells are born each day in the DG, and, of these, ap-proximately 50% survive for at least one month [4, 25]. About 80% of the surviving cells in the granule cell layer are neurons [25]. At this rate, the number of new granule neu-rons born each month is equal to 6% of the mature granule cell population [4]. Others have estimated that immature, adult-born neurons comprise 5-10% of the total dentate granule cell population [26]. These estimates are from rats housed in standard laboratory conditions; in animals housed in more complex environments, the amount of neurogenesis is significantly higher [27, 28]. There is also great variability between species and even between strains of the same spe-cies. For instance, proliferation rates are about 50% higher in the C57BL6 mouse strain than in the 129/SvJ strain [29]. In non-human primates, the amount of neurogenesis may be lower than that seen in rodents [7, 8]. Although SGZ neuro-genesis has been detected in humans, there is little informa-tion about its rate. In the one study assaying neurogenesis in the human SGZ, tissue samples were taken from cancer pa-tients injected with BrdU before death [8]. The number of BrdU labeled neurons was somewhat lower than that seen in marmosets and rodents. However, the mean age of the pa-tients at death was 66.4. Neurogenesis is known to decline precipitously with age in rodents [30]; therefore it is unclear to what extent the relatively low level of neurogenesis ob-served in the human patients is representative of neurogene-sis across the human lifespan.
There is also reason to expect that these numerical esti-mates may underestimate the true functional significance of adult neurogenesis. This is because young adult-born neu-rons have some unique features that may exaggerate their
impact on plasticity within DG. In the first weeks after their birth, neurons in the DG are excited by GABA rather than inhibited, owing to their elevated resting membrane potential [31]. Perhaps, as a result, these cells appear able to undergo long-term potentiation (LTP) under conditions of strong GABA-ergic inhibition that block LTP in mature neurons [26, 32]. Relative to mature neurons, young neurons can be depolarized using very small amplitude currents, probably due to the activity of low threshold calcium channels [33]. Possibly as a result of this increased excitability, young neu-rons exhibit a reduced threshold for LTP induction as com-pared to mature neurons [32, 33]. Field recordings have identified a form of LTP that can be elicited in the DG by weak stimulation of the medial perforant path. Arresting neurogenesis via various methods eliminates this form of LTP [26, 34]. These unique features of young neurons mean that neurogenesis does not simply add new cells to the exist-ing population of mature granule cells; rather, it creates a transient and distinct population of excitable, highly plastic young cells. It is conceivable that this population has a unique biological function, distinct from that of mature granule neurons.
More direct evidence for a behavioral or psychological function for adult neurogenesis comes from rodent behav-ioral studies. Participation in challenging Hp-dependent learning tasks, such as maze learning, causes immediate-early genes such as cFos to be expressed in adult-born neu-rons [35] and increases the probability that these neurons will survive for the long-term [27, 36], suggesting that these cells somehow participate in the underlying learning. Con-versely, blocking neurogenesis in the SGZ impairs perform-ance in some of the same tasks [34, 37-39].
In sum, research so far suggests that neurogenesis is likely to be behaviorally significant. In rodents, behavioral significance has been demonstrated explicitly in experiments showing that the arrest of neurogenesis produces behavioral impairments. Even if the amount of neurogenesis in humans is lower than that in rodents –and this has yet to be solidly demonstrated- there is reason to expect that a small popula-tion of young, adult-born neurons can make a significant functional contribution because of the unique properties of these neurons.
Fig. (1). Immunohistochemical labeling of adult-born neurons in the mouse. (A) Doublecortin (DCX) immunohistochemistry labels the im-
mature neurons and neuroblasts that line the inner granule cell layer and subgranular zone of the dentate gyrus. DCX is expressed in neurons
until about 28 days of age. (Color is saturated to expose the dendrites traversing the GCL.) (B) BrdU-positive and BrdU/NeuN double-
positive cells in the dentate. BrdU is a birthdating marker (see section 2.2), and NeuN is a neuron-specific marker. The mouse was injected
with BrdU (150 mg/kg) once per day for 3 days and then sacrificed on the fourth day. (Scale bars = 50 m).

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 207
2.2. Methodology
Generally, there are three ways in which a given treat-ment can influence the number of adult-born neurons present in a system at a given time. The treatment can affect prolif-eration by influencing the frequency at which progenitor cells in the SGZ divide. The new cells born can be neurons, glia, or, through symmetric division, additional progenitors. Treatments can affect the relative numbers of postmitotic cells adopting these different phenotypes. Finally, after a neuron is born, it can either survive or die. Some manipula-tions, such as environmental enrichment (see below), can affect the probability of survival without altering prolifera-tion.
These different modes of affecting neurogenesis can be differentiated using a birthdating marker, most commonly bromodeoyxuridine (BrdU). BrdU is a base analogue of thymidine that is incorporated into DNA during replication. BrdU can be injected into an animal systemically, and, as a result, all cells undergoing S-phase while the BrdU is present will contain BrdU, which can then be detected using immu-nohistochemistry [40]. If tissue is collected within several hours after injection of BrdU, the resulting BrdU-positive cell counts will reflect cell proliferation primarily. If tissue is collected days to weeks after the injection, one can assess the relative likelihood that the dividing cells adopted a neuronal or glial fate by assessing co-localization of BrdU with neu-ronal- or glial-specific antigenic markers [4]. Finally, by injecting BrdU just prior to commencing a given experimen-tal treatment, and then collecting the brain tissue after sev-eral weeks of the treatment, one can determine whether the treatment regulates survival of new cells independent of ef-fects on proliferation (e.g. [41]).
BrdU labeling has some limitations. Because BrdU can only be detected by immunohistochemistry, it is not possible to identify its presence in live cells. Furthermore, BrdU la-bels not only newly-born neurons and glia, but also progeni-tor cells, which continue to divide after all free BrdU has been eliminated. These progenitors transmit BrdU to their progeny, and as a result, new BrdU-labeled cells continue to be born for several days after a BrdU injection [25]. As a result, it can be difficult to precisely quantify cell birth rates using BrdU.
Because BrdU cannot be visualized in vivo, researchers have begun using genetic strategies to tag adult-born cells. One approach for labeling adult-born cells has been to inject into DG retroviruses coding for a fluorescent protein [18, 31, 42]. The retroviral DNA will be incorporated only into divid-ing cells, and as a result, progenitor cells and their progeny will express the fluorophor, but cells born before the injec-tion will not. Another approach is to express a fluorophor transgenically under a promoter that is active only in a spe-cific cell type, such as neuronal progenitors [43]. This ap-proach has the advantage that the fluorescent label can be targeted to specific cell types, but it requires careful verifica-tion that the expression pattern is faithful to that of the en-dogenous promoter. Because fluorophors can be visualized in live hippocampal slices, they allow specific cell popula-tions to be identified for intracellular electrophysiological recordings or cell sorting. These genetic approaches for fluo-rescent labeling of cells have led to great progress in under-
standing the unique electrophysiology and morphology of young neurons and neural progenitors [31, 42, 44]
3. HIPPOCAMPUS, NEUROGENESIS, AND THE ETIOLOGY OF DEPRESSION
3.1. Hippocampus and Emotion
Hp is traditionally thought of as a learning and memory center. Its role in this domain was first proposed over a hun-dred years ago but became cemented with Milner’s famous studies of the patient H.M., whose temporal lobe was re-sected in treatment of epilepsy [45] (for review see [46]). Studies of learning and memory continue to dominate the Hp literature, but over the past 30 years a considerable body of work has emerged in parallel documenting a role for Hp in the control of aspects of emotionality. Gray and McNaugh-ton, for instance, have argued at length that the septo-hippocampal system is instrumental in regulating anxiety [47]. The foundation of their theory includes the observation that all anxiolytic drugs impair the septo-hippocampal theta rhythm, which is the phasic firing pattern of cells in the hip-pocampus and related structures thought to ready the system for information processing [48]. Furthermore, lesions to the medial septum, which generates the hippocampal theta rhythm, or to Hp directly, produce behavioral effects similar to those of anxiolytic drugs [47, 49].
More recent work suggests that the mnemonic and emo-tional functions of Hp may be segregated along its long, septo-temporal axis. Lesions to the septal half of the Hp (also known as dorsal Hp in rodents and posterior Hp in hu-mans) impair spatial maze performance to the same extent as whole Hp lesions [50], but similarly-sized lesions to the temporal (ventral in rodents, anterior in humans) portion of Hp are of no effect in these tasks [51, 52]. Conversely, tem-poral Hp lesions produce anxiolytic-like effects in a number of tasks, including novelty-suppressed feeding (NSF; de-scribed below) and the light-dark choice test, but septal Hp lesions have little or no effect in the same tasks [51-53]. The lesion data suggest that septal Hp is specialized for process-ing spatial (or affectively neutral) information, while the temporal Hp controls responses to anxiogenic stimuli (cf. [47]). These specializations are consistent with differences in physiology and connectivity along the septo-temporal axis. Septal Hp is more densely populated with place cells than is temporal Hp, and it receives the majority of visual sensory inputs [54]. The ventral Hp is more closely connected to limbic structures, having reciprocal connections with amygdala [55] and extending projections to nucleus accum-bens, prefrontal cortex, and hypothalamus [56].
Less is known about the specific role of DG in emotional regulation. Most of the work on DG has focused on informa-tion processing (for a through summary, several excellent reviews are available [57-59]). Three features are thought to be central to the DG’s information processing functions [57, 58]: its highly divergent input from the entorhinal cortex, with 200,000 entorhinal cortical cells projecting to over 2,000,000 DG granule cells (in the rat); its competitive feed-back inhibition, which ensures that only the most active neu-rons maintain activity in response to a stimulus; and the rela-tively sparse mossy fiber inputs to CA3. These characteris-tics are thought to enable DG granule cells to produce a sparse and non-redundant representation of entorhinal inputs,

208 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
a function that may help give similar experiences unique mnemonic representations. Consistent with this interpreta-tion, lesions to DG impair fine spatial discriminations but do not affect more gross spatial discriminations [60]. It is also thought that the DG may be more important for encoding of memories than for retrieval [58], and there is some behav-ioral evidence to this effect [61].
What is the role of neurogenesis in these processes? One possibility is that the addition of new granule neurons allows the sparseness of the DG code to be maintained even as new memories are continually added [59]. Alternatively, the addi-tion of highly plastic young neurons to the network may es-sentially reduce the sparseness of the DG code, allowing experiences that occur in close temporal proximity to be bound into cohesive and distinct episodic memories [62]. As the new neurons encoding a particular episode mature out of their highly plastic stage, their reduced capacity for plasticity ensures that new experiences do not interfere. Both of these accounts predict that reductions in neurogenesis will reduce the degree to which episodic memories are discriminable from each other. How could this relate to depression? Per-haps reductions in neurogenesis cause negative experiences to be overgeneralized across space and time. Of course, posi-tive experiences should be similarly overgeneralized, so ad-ditional mechanisms would be needed to explain how re-duced neurogenesis could produce a net negative change in affect.
3.2. Depression is Associated with Hippocampal Atrophy
MRI has been used extensively to determine whether depression is associated with changes in brain morphology. Some studies report a reduced Hp volume in depressed pa-tients [63-67] and others not [68-70], but a recent meta-analysis of 17 published MRI studies concludes that the ag-gregate data favor a reduction in Hp volume in depressed patients [67]. Discrepancies between individual studies may be due to procedural factors [67]. Specifically, inclusion of the amygdala in volumetric measurements of Hp tended to reduce the effect size of volumetric differences, perhaps be-cause the amygdala may be enlarged in depressed patients [71]. In addition, there is evidence that the Hp volume loss in depression is correlated with the duration for which depres-sion is untreated [72]. Therefore, inclusion of first-episode patients or patients that have been treated for an extended period may reduce the observed Hp volume loss. Consistent with the anatomical data, depressed patients show impair-ments in Hp-related cognitive tasks [67, 73].
At the cellular level, there are presumably three possible (non-exclusive) mechanisms by which this decrease in Hp volume could occur: cell loss through cell death, cell loss through non-replacement (i.e., a reduction in neurogenesis or gliogenesis), and cell atrophy (of somata and/or neurites). At present, there is relatively little patient histological data to help distinguish among these hypotheses. Two studies using the same brain specimens reported no cell loss and only mi-nor increases in apoptosis in Hp of depressed patients [74, 75]. Another study also found no cell loss in Hp but reported that the soma size of pyramidal and granule neurons is re-duced in the Hp and DG of depressed patients [76]. These data suggest that cell loss is not the primary mediator of de-pression-related decreases in Hp volume (for other possible
mediators, see [77]). Finally, one study examined expression of a marker of cell proliferation (Ki-67) in postmortem tissue from depressed and control individuals [78]. There was no decrease in Ki-67 expression in the DG of depressed pa-tients. However, most of the patients were being treated with AD medications at the time of death; because AD drugs in-crease neurogenesis (discussed in detail below), depression-related decreases in proliferation may have been masked. In summary, post-mortem studies have not uncovered evidence of reduced neurogenesis in depression, but this absence of evidence should be interpreted with caution because of the paucity of data available.
3.3. Stress, Depression, and Neurogenesis are Interre-lated
Dysregulation of the HPA axis is a common feature of depression, although it may not be present in all subtypes of the disease [79]. About half of all depressed patients show an abnormal response to the dexamethasone suppression test [80, 81], which measures the ability of an exogenous gluco-corticoid receptor agonist to suppress endogenous stress hormone release. In some depressed patients this suppression is blunted, suggesting a downregulation of glucocorticoid receptors and impaired negative feedback regulation of the stress response [82]. Baseline cortisol levels are also ele-vated in some depressed patients [83, 84].
It is difficult to know for sure whether dysregulation of the HPA axis is a cause or an effect of depression. However, several lines of evidence suggest that stress can play a causal role. Generalized anxiety disorder is a major risk factor for depression, and depressive episodes are commonly precipi-tated by stressful life events [85]. Of course, the effects of stressful life experiences can be moderated by underlying genetic predispositions, a point that is illustrated by a re-markable recent study by Caspi and colleagues [86]. The study showed that the effect of stressful life experiences on lifetime depression risk varies depending on a polymorphism in the serotonin transporter gene. In all subjects the probabil-ity of a depressive episode increased with the number of stressful events experienced. However, the effect of the stressful life events on depression risk was much larger in individuals possessing the “short” allele than in those pos-sessing the “long” allele of the gene.
The effects of chronic stress have also been studied ex-perimentally in animals. One strongly validated animal model is the chronic mild stress paradigm [87]. In it, rodents are exposed continuously to various mild stressors, such as food and water deprivation, temperature changes, and changes in cage mates. Rats exposed to this procedure for several weeks show a number of symptoms that parallel those seen in depressed patients, including anhedonia, altera-tions in sleep-wake cycle, and reduced sexual and self-care behavior. Mice subjected to the treatment show increased anxiety-like behavior in some tests, decreased grooming, and increased aggression, but it is noteworthy that the effects vary greatly between strains and the reliability of these find-ings has been questioned [88-90]. Chronic stress also causes a decrease in SGZ neurogenesis [91]. The effect of chronic stress on neurogenesis has been replicated numerous times using different stress paradigms and species. This work has been carefully reviewed elsewhere [92-94], so we will not

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 209
detail it here. Importantly, both the behavioral symptoms and the reduction in neurogenesis caused by chronic stress can be prevented or reversed by AD treatments [87] (for review see [92]).
In summary, some subtypes of depression are associated with elevated stress hormone levels, and stress appears to play a causal role in the generation of depression. Research using animal models indicates that chronic stress decreases neurogenesis and produces behavioral outcomes similar to those seen in depression. These data suggest that neurogene-sis may be reduced in at least some depressed patients and have fostered speculation that reductions in neurogenesis play a causal role in the disease [23].
3.4. Reducing SGZ Neurogenesis Does Not Induce De-pressive Symptoms
Recent work using animal models has begun to address whether reductions in neurogenesis produce depressive symptoms. Two recent studies examined whether levels of neurogenesis correlate with behavioral responses in a learned helplessness (LH) procedure [95, 96]. In LH, animals are first exposed (or not exposed) to inescapable shock and then transferred to an escape/avoidance task in which shock is controllable [97, 98]. Exposure to inescapable shock impairs subsequent acquisition of the escape/avoidance task, argua-bly because the inescapable shock teaches animals that they are ineffectual, or helpless. However, there can be marked interindividual variability in the effects of the inescapable shock, with some animals showing large impairments in sub-sequent escape/avoidance acquisition and others showing none. One study demonstrated that exposure to inescapable but not escapable shock reduces cell proliferation for at least 9 days [96], but this study did not differentiate between help-less and non-helpless animals. A second study, by Vollmayr and Henn, found that helpless and nonhelpless animals had equal reductions in proliferation [95], suggesting that changes in proliferation could not have produced the helpless phenotype. Consistent with this interpretation is the finding that the behavioral and anti-proliferative effects of inescap-able shock followed different time-courses: the behavioral impairments in avoidance manifested within 1 day after in-escapable shock, but the reductions in proliferation were not observed until 7 days after. There are, however, several fac-tors that complicate interpretation of the Vollmayr and Henn results. First, the neuronal or glial identity of BrdU-labeled cells was not determined; thus, it is not known whether the experimental groups differed in their numbers of newborn neurons. Second, it is not known whether the impaired and unimpaired subjects differed in their pre-treatment levels of neurogenesis. Finally, questions have been raised about the construct validity of LH as a model of depression, because the behavioral effects of inescapable shock exposure are short-term [99], can be prevented by subchronic (not only chronic) AD treatment [96], and can be explained by psycho-logical mechanisms other than “learned helplessness”[100].
A more definitive way to evaluate the putative causal role of neurogenesis in depression may be to experimentally block neurogenesis in animals and then evaluate whether depression-like symptoms are produced. Our research group has begun using this approach. One method of arresting neu-rogenesis is to subject the brain to low doses of irradiation.
Irradiation kills dividing progenitor cells and alters the SGZ microenvironment such that neurogenesis levels are reduced significantly or eliminated altogether [101-103]. We have shown that completely blocking SGZ neurogenesis using a targeted irradiation procedure has no effect on performance in a number of relevant behavioral tasks. For instance, irra-diation does not alter latency-to-feed in either the NSF test [24] or the novelty-induced hypophagia test (our unpub-lished data). Both of these tests are AD screens that measure the latency of a mouse to venture into the center of an open field to obtain food. Latency-to-feed is decreased by chronic AD drug treatment and acute anxiolytic treatment, but not by acute AD drug treatment [104, 105]. Irradiation also fails to affect behavior in two traditional anxiety tests, the elevated-plus maze and light-dark choice test (our unpublished data).
We have replicated some of these negative results using an alternative method for arresting neurogenesis. The alter-native method is a transgenic mouse in which herpes-simplex virus thymidine kinase (HSV-TK) is expressed un-der the GFAP promoter. GFAP is expressed in the neural stem cells located in the SGZ and SVZ [106]. The presence of HSV-TK in dividing cells confers sensitivity to the cyto-toxic effects of the antiviral drug ganciclovir. Thus, in the transgenic mouse, administration of ganciclovir kills divid-ing neural stem cells and reduces neurogenesis to low levels [106]. Non-neurogenic glial cells also express GFAP but because these cells are not dividing they are not killed by ganciclovir [34]. Similar to our results with irradiation, blocking neurogenesis in the transgenic mice had no affect on behavior in the open field, NSF test, or light-dark choice test [34].
The only domain in which direct effects of blocking neu-rogenesis have been reported is learning and memory. Re-ducing or blocking SGZ neurogenesis in rats or mice has been reported to cause impairments in a Hp-dependent form of classical conditioning (trace conditioning) [37, 38], long-term spatial memory [39], contextual fear conditioning [34, 107], and a test of working memory [107]. There is contro-versy surrounding some of these reports because the methods used to arrest neurogenesis are known to have side-effects [102, 108]. Currently the most solid finding is the deficit in contextual fear conditioning, which has been replicated three times using three different methods for blocking neurogene-sis and two different species (rats [107] and mice [34]). Con-textual fear conditioning is a form of classical conditioning produced by pairing an aversive footshock with a particular spatial context [109]. As a result of the pairing, the subject exhibits fear when returned to the shock-paired context. Animals in which neurogenesis has been arrested exhibit reduced fear of the shock-paired context compared to control animals. It is as yet unclear whether this reduction stems from impairments in the acquisition or expression of the as-sociation. It is also unclear whether or how this impairment relates to depression. To our knowledge, contextual fear conditioning has not been examined in depressed patients. Further research will be needed to determine if impaired fear conditioning is an endophenotype of depression and whether an impairment of this sort can give rise to the affective fea-tures of the disease.
In summary, the elevated HPA activity associated with depression makes it likely that SGZ neurogenesis levels are

210 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
reduced in at least some depressed patients. However, there is currently no evidence that reduced neurogenesis produces depressive symptoms. Using two independent methods for blocking neurogenesis in mice and multiple behavioral out-come measures, we found no evidence that arresting neuro-genesis produces a depression-like or anxious state. The only known effects of arresting neurogenesis are impairments in specific forms of learning and memory. More research is needed to determine whether these deficits are relevant to depression.
4. NEUROGENESIS AND THE TREATMENT OF DE-PRESSION
4.1. AD Treatments Enhance SGZ Neurogenesis
The most compelling evidence linking neurogenesis to depression is that virtually all AD treatments studied to date increase SGZ neurogenesis. SRIs, tricyclic ADs, and lithium all increase neurogenesis after chronic (> 2 weeks) treatment (for review see [93, 110, 111]). The neurogenic effects of these drugs are limited to the SGZ; no increase in neuro-genesis is observed in the SVZ. With some of these drugs, namely fluoxetine and agomelatine, it has been shown that acute or subchronic treatment (<7 days) is not sufficient to increase neurogenesis [112, 113]. Therefore, neurogenic effects of these drugs roughly parallel the “therapeutic lag” seen in human patients.
Neurogenesis is also enhanced by other compounds not traditionally classified as ADs but that possess AD proper-ties. These include estrogen [114], which has AD properties in some circumstances [115], and some atypical antipsychot-ics [116]. Conversely, a number of drugs without AD prop-erties (typical antipsychotics, opiates, ethanol) have been demonstrated to either have no effect on or reduce SGZ neu-rogenesis [117-121].
The birthdating marker BrdU has been used to assess whether AD drugs influence neurogenesis by increasing neu-ronal proliferation or by promoting survival of newborn neu-rons. When BrdU was administered 2h before sacrifice to mice treated for 14 days with fluoxetine, there was increased BrdU incorporation in the SGZ, consistent with an increase in cell proliferation [113]. When BrdU was administered just before commencement of a 14-day course of fluoxetine, no increase in BrdU-labeled neurons was reported [113]. How-ever, when BrdU was administered prior to a 28-day course of fluoxetine, an increase in the number of BrdU-labeled neurons was reported [41]. Apparently the effects of fluoxet-ine on the survival of existing newborn cells do not manifest until after the proliferative effects, suggesting these effects have different underlying mechanisms. The relative numbers of BrdU-labeled cells co-expressing neuronal- or glial-specific markers are not affected by fluoxetine [113], indicat-ing that the drug does not affect cell fate determination. The increase in SGZ neurogenesis caused by these AD drugs is thus mediated by increases in both cell proliferation and sur-vival, and not by changes in the relative numbers of cells adopting neuronal versus glial fates.
SGZ neurogenesis is also upregulated by electroconvul-sive seizure (ECS) treatment [113, 122]. ECS is a rodent model of electroconvulsive therapy (ECT), a highly effective AD treatment often used with patients resistant to pharma-
cotherapy [123]. The effects of ECS on neurogenesis are stronger than those of AD drugs [113]. As with the pharma-cological treatments, ECS does not markedly change the ratio of neurons to glia born, and the extra neurons born sur-vive long past the end of the treatment [113, 124]. The pro-liferative effect of a single ECS treatment reaches a maxi-mum within 72 h [122]. This suggests that the proliferative effect of ECT is considerably faster than that of AD drugs. The therapeutic effects of ECT are similarly rapid, appearing within the first few treatments and reaching a maximum within 2-4 weeks of treatment [125]. However, it should be noted that the very rapid-onset effects of ECT are unlikely to be mediated by increases in neurogenesis, because new neu-rons do not become functionally integrated until at least a week after their birth [126].
Two other treatments that potently upregulate neurogene-sis are exercise and environmental enrichment. In humans, exercise tends to have a mood elevating effect [127], but it is unclear whether the same is true in rodents. In rodent mod-els, exercise is usually operationalized as the housing of animals in a cage containing a running wheel. Some strains will run up to 18km a day [128]. Running increases cell pro-liferation two- to four-fold, modestly increases the propor-tion of newborn cells that adopt a neuronal fate, but does not markedly alter cell survival [128, 129]. Enrichment usually comprises housing animals in larger, more complex envi-ronments containing toys, enclosures, and sometimes run-ning wheels. Rodents housed in an enriched environment tend to be less anxious than those housed in standard labora-tory cages [130-133] and show improved learning and mem-ory ability [133]. Enrichment’s effects on neurogenesis are strain-dependent in mice. In one mouse strain that has a rela-tively low baseline level of neurogenesis (129/SvJ), enrich-ment increases both proliferation and survival [134]. In an-other strain with higher baseline levels (C57BL/6), enrich-ment enhances neuronal survival but does not affect prolif-eration [28, 135]. The neurogenic effects of both enrichment and exercise are limited to the SGZ [136].
The one putative AD treatment that has not been demon-strated to upregulate SGZ neurogenesis is transcranial mag-netic stimulation (TMS). TMS uses strong magnets to induce electrical currents in frontal cortical areas. Data on clinical efficacy are preliminary but suggest that TMS is superior to a sham treatment in humans [137]. In the rat TMS has been shown to prevent the effects of repeated social defeat stress on stress hormone levels [138]. In this study TMS only par-tially reduced the effects of stress on neuronal proliferation and may have exacerbated the effects on neuronal survival. No data were collected on the behavioral effects of TMS in this experiment, but in other rodent studies TMS has had only mixed success in producing antidepressant-like behav-ioral effects [139-141]. This mixed success may have to do with the difficulty of recapitulating the correct stimulation parameters in the rat. Until reliable behavioral effects of TMS in rodent models are established, data on the presence or absence of neurogenic effects will be uninformative.
In sum, there is considerable evidence that AD treat-ments, both pharmacological and non-pharmacological, upregulate SGZ neurogenesis. The diversity of treatments that have this effect is striking. Among pharmacotherapies, at least four different classes of drug are included (SRIs,

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 211
tricyclic ADs, atypical ADs, atypical antipsychotics); behav-ioral treatments (exercise, enrichment) are included, as is ECT. The data suggest that upregulation of neurogenesis may be a common pathway through which different AD treatments act. On the other hand, it is also possible that the upregulation of neurogenesis is a marker of AD treatment with no intrinsic therapeutic efficacy. As described below, recent animal studies have attempted to distinguish between these two hypotheses.
4.2. Neurogenesis is Required for Some Behavioral Effects of AD Treatments
If the upregulation of neurogenesis mediates the thera-peutic effects of AD treatments, then blocking neurogenesis should interfere with the effects of these treatments. Three recent studies have tested this hypothesis using mouse mod-els. All three studies used a targeted irradiation procedure to eliminate cell proliferation in the SGZ without affecting SVZ neurogenesis. One study conducted in our lab demonstrated that irradiation blocked the effects of both imipramine and fluoxetine in two mouse behavioral screens for AD activity [24]. One screen was the NSF test described above. A virtue of this test as a screen for AD activity is that latency-to-feed is reduced by chronic AD treatment and not by acute or sub-chronic treatment, paralleling the therapeutic lag seen in hu-man patients. Chronic treatment with these drugs reduced latency to feed in control mice but not irradiated mice. The other behavioral screen was the chronic unpredictable stress paradigm, a variation on the chronic mild stress procedure described above. Chronic stress diminished grooming behav-ior, and this diminishment was prevented by fluoxetine treatment in control mice but not irradiated mice. In a sepa-rate series of experiments conducted by another lab, irradia-tion was shown to block the anxiolytic effects of chronic treatment with the synthetic cannabinoid HU210 [142]. Thus, neurogenesis was required for the behavioral effects of three different drugs in two different AD screens.
In interesting contrast to the previous studies, we recently discovered that the effects of environmental enrichment on NSF performance do not require neurogenesis [133]. In this study, adult mice were subjected to the targeted irradiation procedure, and then after a recovery period were housed in an enriched environment that included running wheels. After 6 weeks of enrichment, latency-to-feed was reduced in the enriched mice, suggesting that enrichment had an anxiolytic effect, like AD drugs. However, the effect was not blocked by irradiation, indicating that this behavioral effect was neu-rogenesis-independent.
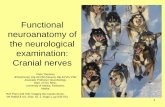
In sum, these three studies suggest that AD-like effects can be achieved through at least two different pathways (Fig. 2), one that is neurogenesis-dependent and one that is neuro-genesis-independent. AD drugs and cannabinoids appear to use a neurogenesis-dependent pathway, while enrichment uses a neurogenesis-independent pathway either alone or in combination with the neurogenesis–dependent pathway. An important outstanding question not addressed by these ex-periments is whether the upregulation of neurogenesis is sufficient to produce AD effects. A related concern is that there may be other relevant effects of AD drugs that are not neurogenesis-dependent and that were not assayed by the two behavioral tests employed in the studies cited above.
Indeed, it is unlikely that any two behavioral tests will have perfect predictive validity or will detect all therapeutically-relevant effects of a drug. Future research should assess the effects of AD drugs and neurogenesis disruption in a broader array of animal depression screens and models.
Fig. (2). Animal models suggest that antidepressant drugs reduce
anxiety through a neurogenesis-dependent mechanism. It is possible
that other effects of these drugs occur through a neurogenesis-
independent mechanism. Environmental enrichment boosts neuro-
genesis and decreases anxiety, but in this case the anxiolytic effect
is neurogenesis-independent. Presumably anxiolytic effects can be
achieved through both neurogenesis-dependent and –independent
mechanisms.
5. REGULATION OF NEUROGENESIS: CELLULAR AND NETWORK MECHANISMS
Much recent work has been devoted to identifying the cellular pathways controlling the proliferation, differentia-tion, and circuit integration of adult-born cells. A thorough understanding of these pathways will be an important tool for the rational development of new ADs that target neuro-genesis.
5.1. The SGZ and SVZ are Uniquely Permissive of Neu-rogenesis
The SGZ and SVZ provide microenvironments that are uniquely permissive of neurogenesis relative to other areas of the CNS. Although proliferating cells reside throughout the CNS, it is only in the SGZ and SVZ that these cells retain the ability to produce both neurons and glia. In other regions, proliferating cells give rise to glia exclusively. This exclusiv-ity is dictated by cues from surrounding tissue, not by intrin-sic properties of the proliferating cells [143]. Proliferating cells isolated from the spinal cord, a non-neurogenic tissue, give rise to neurons when transplanted into the SGZ. When transplanted into other subfields of the HP, the cells give rise to glia only. The neurogenic property of the SGZ appears to be conferred by astrocyte-derived signals [144]. Progenitor cells do not produce new neurons or glia when plated onto a medium free of other cells. When plated onto a culture con-sisting primarily of Hp-derived neurons, the progenitors pro-

212 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
duce many oligodendrocytes and few neurons. Conversely, when plated onto a culture of Hp-derived astrocytes, the pro-genitors produce many neurons and few glia. Astrocytes appear to instruct progenitors to produce neurons via the diffusible signal Wnt3 [145]. Wnt3 is expressed by adult HP astrocytes, and progenitor cells express its receptors. Block-ing the Wnt pathway by interfering with its intracellular sig-naling mechanisms within progenitor cells significantly re-duces neurogenesis in progenitor cell/astrocyte co-cultures. Furthermore, virally-mediated overexpression of Wnt3 in the DG in vivo markedly increases neurogenesis.
5.2. Progenitor Cells in the SGZ
The pool of neuronal progenitor cells in the SGZ consists of two major classes. The first class, usually called Type I [146] or B [147] cells, consists of stem-like cells [148] with radial-glia-like morphology and electrophysiological charac-teristics of adult hippocampal astrocytes [149]. It is thought that these cells divide relatively infrequently and give rise through asymmetric division to the second major class of proliferative cell, the Type II or D cell. Type II cells have more neuronal characteristics, such as fast voltage-gated inward currents and expression of PSA-NCAM and double-cortin, markers of immature neurons. The Type II cells are transiently-amplifying cells that divide rapidly and give rise to postmitotic neuroblasts, which migrate into the granule cell layer and develop into granule cells with functional syn-apses (see [146, 148] for review). The Type II cells have been sub-classified into several different types according to their proliferative potential, morphology, and level of neu-ronal differentiation [146, 147].
5.3. Neuronal Proliferation is Regulated by Network Ac-tivity
The frequency with which type II progenitors cell give rise to neurons appears to be regulated by network activity in the DG. As noted above, various systemic manipulations that putatively increase hippocampal activity also increase neu-rogenesis. These include running, Hp-dependent learning, LTP induction [150, 151], and status epilepticus [152]. The progenitors themselves appear able to sense this activity di-rectly via neurotransmitter receptors, but there is some con-troversy as to the identity of the neurotransmitters involved. One study by Deisseroth, Singla and colleagues examined neuronal progenitor cells cultured in a medium containing no other live cells [153]. In this preparation, the application of NMDA increased the number of neurons produced, and this effect could be blocked with L-type calcium channel block-ers. These data suggest that glutamatergic inputs to progeni-tor cells activate L-type calcium channels, which direct the cells to exit the cell cycle and terminally differentiate into neurons. Consistent with this interpretation, in vivo admini-stration of L-type calcium channel agonist and antagonist drugs increased and decreased, respectively, the amount of neurogenesis. Another study by Tozuka et al. made intracel-lular recordings from GFP-labeled type II progenitors in a hippocampal slice preparation [44]. These researchers found that focal application of GABA evoked inward (depolariz-ing) currents in the progenitors but NMDA had no effect. The GABA-mediated depolarization increased expression of NeuroD, a transcription factor that promotes neuronal differ-entiation, and increased the proportion of progenitor cells
that differentiated into neurons. It is unclear why NMDA-mediated currents were not detected in this study. One possi-bility is that the progenitors were in a slightly different matu-rational state than those examined by Deisseroth [154]. What both studies make clear, however, is that progenitors have the ability to directly sense network activity and that depo-larization of these cells promotes neuronal differentiation.
5.4. GABA Regulates Neuronal Differentiation
In addition to acting on type II progenitors to promote neuronal differentiation, GABA acts directly on immature neurons to promote differentiation and circuit integration. Although GABA is primarily inhibitory to mature neurons, immature neurons are excited by GABA, owing to their ele-vated intracellular chloride levels [155]. Stimulation of GABAA receptors opens Cl- channels, leading in immature neurons to a depolarizing outward flow of Cl- ions. The high intracellular Cl- concentration in immature neurons is due to a high concentration of the Cl- importing transporter NKCC1 and a low concentration of the Cl- exporting transporter KCC2. In a remarkable recent study NKCC1 expression was knocked down in postmitotic neurons using a short-hairpin RNA (shRNA) [31]. Transducing postmitotic neurons with the shRNA converted GABA responses from depolarizing to hyperpolarizing. Importantly, when examined 2 weeks after transduction, the neurons exhibited less dendritic arboriza-tion and weaker synaptic inputs than control cells. The result suggests that GABA-mediated excitation of postmitotic neu-rons promotes their development and integration into local circuits.
In summary, activity within the DG is a primary regula-tor of neuronal proliferation and survival. Activity is sensed both by progenitors and by postmitotic neurons themselves. At the level of progenitor cells, activity in the DG activates NMDA, L-type Ca
++ channels, and/or GABA receptors,
which depolarize the progenitor cells and promote neuron production. Postmitotic neurons sense DG activity through GABA receptors, which, when activated, depolarize the cell and promote differentiation and circuit integration. It seems likely that some AD treatments, particularly those that in-crease network activity in Hp, such as ECT, exercise, and possibly enrichment, take advantage of these excitation-neurogenesis coupling mechanisms. However, little is known about the specifics of these interactions. The majority of studies on the link between AD treatments and neurogenesis have focused on the role of neurotrophic factors. This work is described in the next section.
6. REGULATION OF NEUROGENESIS BY AD TREATMENTS
The pathways through which AD treatments upregulate neurogenesis are currently a subject of great interest. Most AD drugs acutely increase serotonin or norepinephrine levels but also produce numerous downstream changes in gene expression [156]. The effects of ECT are similarly complex [157]. Considerable effort has been put forth in trying to identify which of these downstream changes are instrumental in the therapeutic effects of the treatments. Among the many downstream changes observed are increases in neurotrophin levels (for review see [110]). Because neurotrophins are known to regulate neurogenesis both at the level of cell pro-liferation and differentiation, it seems very likely that these

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 213
factors are involved in the neurogenic effects of AD treat-ments. Indeed, there is now a growing body of literature in-dicating that neurotrophins are required for the neurogenic effects of AD treatments.
6.1. AD Treatments Boost Neurotrophin Levels in Hp
A number of studies have shown that AD treatments, both pharmacologic and non-pharmacologic, increase neu-rotrophin levels within the HP. Gene expression profiling in the rat has shown that chronic ECS treatment upregulates expression of the mRNAs for brain-derived neurotrophic factor (BDNF) [157-161]; its receptor, TrkB [160]; and vas-cular-endothelial growth factor (VEGF)[157, 158]. Acute ECS additionally upregulates fibroblast growth factor-2 (FGF2) mRNA [157]. Numerous AD drugs, including tri-cyclics, monoamine-oxidase inhibitors, and selective-serotonin reuptake inhibitors, have been reported to increase BDNF mRNA in HP [160] (for review see [162]). Some AD drugs have been additionally reported to increase expression in Hp of TrkB [160], insulin-like growth factor [163], and VEGF [92]. It is notable that some studies failed to detect an increase in BDNF protein in HP after chronic treatment with AD drugs [159, 161]. However, these negative results should be interpreted cautiously in light of data that autophosphory-lation of the TrkB receptor is increased under similar condi-tions [164]. Autophosphorylation of TrkB is the first step in the neurotrophin signaling cascade and has been validated as a measure of neurotrophin release [165].
Some of these neurotrophins have additionally been im-plicated in the etiology of depression. FGF-family mRNAs were reported to be differentially expressed in the brains of untreated depressed patients, as compared to normals and treated depressed patients [166]. In a mouse model, chronic social defeat stress downregulated expression of two BDNF mRNA splice variants (transcripts III and IV) and increased methylation at their corresponding promoter regions [167]. Chronic treatment with imipramine reversed both the behav-ioral effects of stress and the downregulation of BDNF mRNA.
6.2. BDNF and VEGF are Necessary for the Neurogenic Effects of Some AD Treatments
BDNF and VEGF have received the most attention as potential mediators of the neurogenic effects of AD treat-ments. VEGF has been shown to stimulate neuronal prolif-eration both in vitro [168] and in vivo [168, 169]. Inhibition of VEGF signaling has been reported to block the upregula-tion of neurogenesis by environmental enrichment [169], exercise [170], ECT [92], and AD drugs [92]. BDNF promo-tes neuronal survival, plasticity, and differentiation [171]. Genetic interference with BDNF signaling, either through the use BDNF
+/- mice or through transgenic overexpression
of a dominant-negative TrkB, blocks both the neurogenic effects of fluoxetine and imipramine [172] and the behav-ioral effects of these drugs in the forced-swim test [164]. In addition, infusion of BDNF into the DG produces AD behav-ioral effects in the rat [173]. Thus it appears that both VEGF and BDNF are critical mediators of the neurogenic and pos-sibly behavioral effects of AD treatments.
The effects of AD drugs in BDNF+/-
and dominant-negative TrkB mutant mice also provide key information
about which component of the neurogenic process is re-quired for the therapeutic effects of these drugs. Both prolif-eration and survival are enhanced by AD drugs [174]. Theo-retically, the therapeutic effects of these drugs could be me-diated by neuronal proliferation itself, with survival of post-mitotic neurons being unnecessary. Or the effects may de-pend on the addition of new, functional neurons to the DG, which requires both proliferation and survival. In BDNF
+/-
and dominant-negative trkB mice these processes are disso-ciated: AD drugs significantly increase neuronal prolifera-tion in these mice, but survival of postmitotic neurons is se-verely impaired, such that AD treatment fails to increase the number of neurons surviving to 3 weeks of age [164]. The fact that the behavioral effects of AD drugs are absent in these mice suggests that increasing proliferation alone is not sufficient to produce an AD effect. The behavioral effects require an increased number of surviving neurons.
6.3. CREB may Mediate Neurotrophin Effects on Neuro-genesis
Another factor linking AD treatments and neurogenesis is cAMP-response-element binding protein (CREB). CREB is a transcription factor that is activated by several signaling pathways, including Ras/ERK, cAMP/protein-kinase A, and Ca
++-calmodulin-dependent kinase IV [175]. These pathways
convert CREB to its transcriptionally active form (pCREB) by phosphorylating a Ser133 residue. In addition to playing a role in long-term synaptic plasticity, CREB appears to medi-ate neurotrophin effects on cell survival [176]. Cerebellar granule cells cultured in a minimal medium can be saved from programmed cell death by application of BDNF [177]. Expression of a dominant-negative CREB in these cells blocks the survival-promoting effects of BDNF. Conversely, expression of a constitutively active form of CREB promotes cell survival in the absence of BDNF. CREB appears to promote survival by inducing expression of the anti-apoptotic gene bcl-2 [176].
In vivo, pCREB, the transcriptionally-active form of CREB, is enriched in SGZ, the region of DG that harbors proliferative cells and early postmitotic neurons [41, 178]. Chronic administration of fluoxetine and desiprimine in-crease pCREB levels in DG [179]. Inhibition of pCREB ac-tivity by transgenic expression of a dominant-negative CREB decreases neuronal proliferation in DG [41, 178]. Consistent with a role for CREB in AD effects, stimulation of the cAMP-CREB pathway with the phosphodiesterase-IV inhibitor rolipram increases neuronal proliferation and sur-vival in DG [178] and produces AD-like effects in the learned-helplessness paradigm [180].
CREB may thus link AD effects on neurotrophins to in-creases in neurogenesis. One possible pathway, suggested by the cell culture experiments cited above, is that CREB medi-ates the survival-promoting effects of neurotrophins like BDNF by inducing transcription of genes like bcl-2. On the other hand, the BDNF gene itself contains a cAMP response element, which suggests that CREB may regulate the expres-sion of BDNF [156]. Many AD drugs stimulate 5-HT and NE receptors that are coupled to the second messenger sys-tems that activate CREB [156]. Thus CREB may control the production of BDNF while also mediating some of its ef-fects.

214 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
7. CONCLUSIONS
7.1. A Paradox: Neurogenesis is Related to the Treatment
But Not Etiology of Depression
The hypothesis that reductions in neurogenesis cause depression has received virtually no experimental support. Neurogenesis levels are not predictive of a rodent’s response to learned helplessness training. Experimentally blocking neurogenesis, either through irradiation or through a genetic manipulation, fails to affect performance in a variety of be-havioral tests that should be sensitive to depression-like be-havior. Conversely, data are generally supportive of the hy-pothesis that AD treatments act, at least in part, through a neurogenesis-dependent mechanism. Virtually all AD treat-ments studied to date increase neurogenesis in the SGZ, and arresting neurogenesis blocks the effects of AD drugs in two mouse models.
This presents a paradox: Why would increasing neuro-genesis be anti-depressive while decreasing neurogenesis is not pro-depressive? One simple explanation is that AD drugs work through mechanisms orthogonal to the root causes of the disease. This supposes that there are multiple pathways for regulating mood, some of which are dysfunctional in depression and others of which respond to the boost in neu-rogenesis caused by AD treatments. A related possibility is that depression requires the simultaneous presence of multi-ple insults or “hits.” Impaired neurotrophin signaling, Hp atrophy, reduced neurogenesis, as well as extra-hippocampal abnormalities [181] may all be required, and it is possible that the alleviation of any one of these is sufficient to induce remission.
Two other alternatives are worthy of consideration. One is that reduced neurogenesis is actually pro-depressive, but our behavioral measures were not adequate to detect this effect. For instance, reducing neurogenesis may create a dia-thesis for depression but not depression itself. Detecting this type of effect would require exposing animals to various stressors and assaying their resilience. Most of our behav-ioral assays were designed to detect direct effects of reduced neurogenesis on behavior and would probably have been insensitive to this type of diathesis-stress interaction. How-ever, one assay, the chronic unpredictable stress paradigm, did assess mouse responses to stress and did not detect in-creased sensitivity to stress in irradiated mice [24]. Another reason why our behavioral tests might not have detected a pro-depressive effect of reduced neurogenesis is because laboratory animals are already “depressed” due to the im-poverishment of laboratory housing relative to their natural habitat. This interpretation is undermined by the finding that environmental enrichment, which reduces anxiety-like be-havior and enhances Hp-dependent learning, fails to increase sensitivity to neurogenesis disruption in the mouse. Moreo-ver, the fact that chronic mild stress produces behavioral effects in laboratory mice indicates that at baseline condi-tions these mice are not at an absolute ceiling with respect to anxiety-like behavior.
A second possibility is that the behavioral effects of AD drugs were blocked not by the arrest of neurogenesis but by some other effect of the irradiation. Irradiation is known produce lasting inflammation [102], alter levels of some in-tracellular signaling molecules [182], and can change the
microvasculature of DG [101]. On the other hand, the rela-tively low dose of irradiation used in these studies was below the threshold for producing epithelial apoptosis, demyelina-tion, or radionecrosis. Many Hp-dependent behaviors are unaffected by irradiation, indicating that no gross damage has occurred [34]. A form of LTP that is sensitive to very modest perturbations of the DG is not impaired by irradia-tion [103]. Furthermore, we have observed that the apoptotic effects of irradiation are precisely confined to the SGZ, indi-cating that mature granule cells are not killed [24].
Thus, at this point, the data are consistent with the hy-potheses that neurogenesis is involved in the treatment but not etiology of depression. At the same time, reasonable concerns exist about the sensitivity and external validity of the behavioral methods and the specificity of the neurogene-sis ablation methods used in animal experiments investigat-ing a causal link between neurogenesis and depression. More definitive testing of the role of neurogenesis in depression and the antidepressant response will require a convergent approach. Specifically, neurogenesis can be blocked using multiple, independent methods. If similar results are ob-tained using different methods with different side-effects, this will constitute strong evidence that the behavioral effects were caused by the disruption of neurogenesis and not by secondary effects of the manipulation. Similarly, in model-ing depression or AD effects in animals, multiple behavioral outcome measures must be used, because no single measure is likely to capture all clinically-relevant features of the dis-ease or drug response. Finally, a broader range of AD treat-ments should be tested for their neurogenesis dependence. If the upregulation of neurogenesis is a common mechanism of AD action, then the effects of multiple treatments should be blocked by the arrest of neurogenesis.
7.2. Do Antidepressants Work by Increasing Neurogene-sis?
Although we have argued that neurogenesis is required for at least some therapeutic effects of AD drugs, it does not follow that AD drugs work by increasing the number of new neurons added to the DG. The term “neurogenesis” refers literally to the birth of new neurons, but this definition does not capture the full biological significance of the process. Neurogenesis, in effect, maintains a rotating stock of young neurons with unique properties and initiates a cellular matu-rational process that culminates in either the addition of a new granule cell to the DG or apoptotic cell death. Neuro-genesis thus produces a cascade of effects within DG, and it remains to be determined which of these effects is instru-mental in the actions of AD treatments.
It is certainly not true that AD treatments act solely by increasing the amount of cell proliferation in DG. Newborn neurons do not receive any afferent inputs until about 7 days of age, and excitatory glutamatergic inputs do not arise until about 18 days of age [126]. Thus, some amount of matura-tion is required before these cells could make a functional impact, a point that is confirmed by studies of BDNF
+/- mice
[164, 172]. AD drugs increase the amount of cell prolifera-tion in these mice, but the new neurons die within 4 weeks. Behavioral effects of AD drugs are absent in these mice, suggesting that proliferation alone is not sufficient. Which aspect of the neurogenesis cascade, then, is instrumental in

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 215
mediating AD effects? Several hypotheses follow (see also Fig. 3).
1. AD drugs may act by increasing the number of ma-ture granule cells added to the DG. This could trans-late into an expansion of the granule cell population, which may affect cognitive capacity.
2. Alternatively, if new cells replace (and/or compete with) old cells, increasing the number of granules added to the DG might lead to increased death of old cells and thus increased cell turnover, as has been suggested [172]. Network modeling suggests that in-creasing the turnover rate can enhance the encoding of new memories while simultaneously degrading re-call of old memories [183] (see also [184]). It is easy to imagine how this kind of “cleaning of the slate” could be valuable in the recovery from depression.
3. Neurogenesis creates a pool of excitable, highly-plastic young neurons. ADs may act by enlarging this pool. Enlarging the pool may increase the capacity for certain types of plasticity within the DG, as suggested by electrophysiological studies evidencing a neuro-genesis-dependent form of LTP [26, 34].
4. The presence of a pool of young neurons might ren-der the DG receptive to AD drugs, with enlargement of the pool being extraneous. For instance, AD drugs may exert effects directly on young neurons. In this case, irradiation would block AD effects not because
it blocks the upregulation of neurogenesis, but be-cause it eliminates a pool of cells that is uniquely re-ceptive to the drug.
Testing these hypotheses will require new methods for manipulating specific features of neurogenesis while leaving others intact. Our lab is currently pursuing genetic strategies that may afford this kind of specificity. A valuable tool will be cell-type-specific genetic manipulations. For example, doublecortin, which is expressed primarily in young neurons and neural progenitors [185], can be used to drive expression of a recombinase such as Cre, which would make it possible to target genetic manipulations specifically to immature neu-rons. Plasticity in young neurons could be reduced or elimi-nated by abolishing glutamatergic neurotransmission. Long-term survival of young neurons could be blocked by interfer-ing with CREB activity or BDNF signaling. New insight into AD mechanisms will be generated by examining whether very specific manipulations like these block the effects of AD treatments. In addition, similarly targeted methods of boosting neurogenesis can be developed and used to test whether increases in neurogenesis, or a specific component of neurogenesis, are sufficient to achieve an AD effect.
Future studies should also consider the possible hetero-geneity of neurogenesis’ functional significance across the septo-temporal axis. Of the many studies that have examined the effects of stress or antidepressant treatment on neuro-genesis, few have looked for septal versus temporal differ-ences. Some studies have only analyzed septal Hp [122],
Fig. (3). Four hypotheses about how neurogenesis is involved in the effects of AD drugs. The left image represents the granule cell layer of
the DG prior to treatment with AD drugs. The four images on the right represent four different effects of AD drugs that might be instrumen-
tal in the AD response.

216 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
while others have analyzed the whole Hp but not differenti-ated between its septal and temporal extents [24]. In contrast, it was recently shown that the novel antidepressant agomelatine, a melatonin agonist and 5-HT2C antagonist, specifically upregulates neurogenesis in the temporal Hp [112]. This finding suggests that increasing neurogenesis in the temporal Hp alone may be sufficient to produce antide-pressant effects.
7.3. Discovery of New Neurogenesis-Based Therapies
If it is true that AD treatments work through a neuro-genesis-dependent mechanism, it may be possible to produce better medications by specifically targeting neurogenesis. One obvious approach is to seek new compounds that boost neurogenesis. The rapidly developing literature on the mo-lecular mechanisms of proliferation and differentiation of new neurons suggests several strategies. Proliferation can potentially be enhanced by stimulating the Wnt pathway or neurotrophins such as VEGF, or by increasing GABAergic or glutamatergic neurotransmission in the DG. Because a large percentage of newborn neurons die before reaching maturity [25], manipulations that affect neuronal survival can also have a big effect on the net number of cells added to DG. Potential targets include neurotrophin pathways and related anti-apoptotic signaling molecules bcl-2 and pCREB. Conversely, it may be possible to use the upregulation of neurogenesis as a screen for compounds with AD efficacy. Assaying neurogenesis may prove to be a more cost-effective and accurate method for identifying new com-pounds than is animal behavioral testing.
Finally, it is worth emphasizing the potential importance of young neurons –as opposed to neural proliferation per se– in AD effects. Because the behavioral effects of AD drugs arise within a month after commencing treatment, and be-cause newborn neurons do not become fully mature until at least one month of age [186], it is very likely that young neu-rons play a critical role in the AD response. As described in the previous section (hypotheses 3 and 4) AD drugs may act by increasing the size of the pool of young neurons or by altering the behavior of the young cells themselves. Drug developers should therefore be mindful of the unique proper-ties of these cells. In addition to seeking new drugs that boost neurogenesis, it may be worth pursuing ways to phar-macologically mimic the effects of young cells or to other-wise increase the influence of young cells on the system. For example, treatments can be designed to increase the duration for which new cells retain immature properties or to confer immature properties on old cells. For these strategies to be viable, more basic research is needed into the unique physi-ology, gene expression patterns, and proteomics of young neurons.
ACKNOWLEDGEMENTS
The authors thank E. David Leonardo, Amar Sahay, Holly Moore, and Victoria Cressman for their thoughtful comments on the manuscript and Bill Brennan and Lindsay Miller for their assistance with Figs. 1 and 3. Address corre-spondence to R.H. ([email protected]). The preparation of this paper was supported by NARSAD (R.H. and M.R.D.) and a Charles H. Revson Foundation Senior Fellowship in Biomedical Science (M.R.D.).
REFERENCES
[1] Gross, C. G. Nat. Rev. Neurosci., 2000, 1, 67-73.
[2] Altman, J.; Das, G. D. J. Comp. Neurol., 1965, 124, 319-35. [3] Kaplan, M. S. J Comp Neurol, 1981, 195, 323-38.
[4] Cameron, H. A.; McKay, R. D. J. Comp. Neurol., 2001, 435, 406-17.
[5] Gould, E.; Tanapat, P.; McEwen, B. S.; Flugge, G.; Fuchs, E. Proc. Natl. Acad. Sci. USA, 1998, 95, 3168-71.
[6] Gould, E.; Reeves, A. J.; Fallah, M.; Tanapat, P.; Gross, C. G.; Fuchs, E. Proc. Natl. Acad. Sci. USA, 1999, 96, 5263-7.
[7] Kornack, D. R.; Rakic, P. Proc. Natl. Acad. Sci. USA, 1999, 96, 5768-73.
[8] Eriksson, P. S.; Perfilieva, E.; Bjork-Eriksson, T.; Alborn, A. M.; Nordborg, C.; Peterson, D. A.; Gage, F. H. Nat. Med., 1998, 4,
1313-7. [9] Gould, E.; Reeves, A. J.; Graziano, M. S.; Gross, C. G. Science,
1999, 286, 548-52. [10] Dayer, A. G.; Cleaver, K. M.; Abouantoun, T.; Cameron, H. A. J.
Cell Biol., 2005, 168, 415-27. [11] Zhao, M.; Momma, S.; Delfani, K.; Carlen, M.; Cassidy, R. M.;
Johansson, C. B.; Brismar, H.; Shupliakov, O.; Frisen, J.; Janson, A. M. Proc. Natl. Acad. Sci. USA, 2003, 100, 7925-30.
[12] Gritti, A.; Bonfanti, L.; Doetsch, F.; Caille, I.; Alvarez-Buylla, A.; Lim, D. A.; Galli, R.; Verdugo, J. M.; Herrera, D. G.; Vescovi, A.
L. J. Neurosci., 2002, 22, 437-45. [13] Kokoeva, M. V.; Yin, H.; Flier, J. S. Science, 2005, 310, 679-83.
[14] Kornack, D. R.; Rakic, P. Science, 2001, 294, 2127-30. [15] Lie, D. C.; Dziewczapolski, G.; Willhoite, A. R.; Kaspar, B. K.;
Shults, C. W.; Gage, F. H. J. Neurosci., 2002, 22, 6639-49. [16] Frielingsdorf, H.; Schwarz, K.; Brundin, P.; Mohapel, P. Proc.
Natl. Acad. Sci. USA, 2004, 101, 10177-82. [17] Doetsch, F.; Hen, R. Curr. Opin. Neurobiol., 2005, 15, 121-8.
[18] van Praag, H.; Schinder, A. F.; Christie, B. R.; Toni, N.; Palmer, T. D.; Gage, F. H. Nature, 2002, 415, 1030-4.
[19] Markakis, E. A.; Gage, F. H. J. Comp. Neurol., 1999, 406, 449-60. [20] Hastings, N. B.; Gould, E. J. Comp. Neurol., 1999, 413, 146-54.
[21] Stanfield, B. B.; Trice, J. E. Exp. Brain Res., 1988, 72, 399-406. [22] Leuner, B.; Gould, E.; Shors, T. J. Hippocampus, 2006, 16, 216-24.
[23] Jacobs, B. L.; Praag, H.; Gage, F. H. Mol. Psychiatry, 2000, 5, 262-9.
[24] Santarelli, L.; Saxe, M.; Gross, C.; Surget, A.; Battaglia, F.; Dula-wa, S.; Weisstaub, N.; Lee, J.; Duman, R.; Arancio, O.; Belzung,
C.; Hen, R. Science, 2003, 301, 805-9. [25] Dayer, A. G.; Ford, A. A.; Cleaver, K. M.; Yassaee, M.; Cameron,
H. A. J. Comp. Neurol., 2003, 460, 563-72. [26] Snyder, J. S.; Kee, N.; Wojtowicz, J. M. J. Neurophysiol., 2001, 85,
2423-31. [27] Gould, E.; Beylin, A.; Tanapat, P.; Reeves, A.; Shors, T. J. Nat.
Neurosci., 1999, 2, 260-5. [28] Kempermann, G.; Kuhn, H. G.; Gage, F. H. Nature, 1997, 386,
493-5. [29] Kempermann, G.; Kuhn, H. G.; Gage, F. H. Proc. Natl. Acad. Sci.
USA, 1997, 94, 10409-14. [30] Bizon, J. L.; Gallagher, M. Eur. J. Neurosci., 2003, 18, 215-9.
[31] Ge, S.; Goh, E. L.; Sailor, K. A.; Kitabatake, Y.; Ming, G. L.; Song, H. Nature, 2006, 439, 589-93.
[32] Wang, S.; Scott, B. W.; Wojtowicz, J. M. J. Neurobiol., 2000, 42, 248-57.
[33] Schmidt-Hieber, C.; Jonas, P.; Bischofberger, J. Nature, 2004, 429, 184-7.
[34] Saxe, M. D.; Battaglia, F.; Wang, J.; Malleret, G.; David, D. J.; Monckton, J. E.; Garcia, A. D. R.; Sofroniew, M. V.; Kandel, E.
R.; Santarelli, L.; Hen, R.; Drew, M. R. Proc. Natl. Acad. Sci. USA, in press.
[35] Jessberger, S.; Kempermann, G. Eur. J. Neurosci., 2003, 18, 2707-12.
[36] Dobrossy, M. D.; Drapeau, E.; Aurousseau, C.; Le Moal, M.; Piaz-za, P. V.; Abrous, D. N. Mol. Psychiatry, 2003, 8, 974-82.
[37] Shors, T. J.; Miesegaes, G.; Beylin, A.; Zhao, M.; Rydel, T.; Gould, E. Nature, 2001, 410, 372-6.
[38] Shors, T. J.; Townsend, D. A.; Zhao, M.; Kozorovitskiy, Y.; Gould, E. Hippocampus, 2002, 12, 578-84.
[39] Snyder, J. S.; Hong, N. S.; McDonald, R. J.; Wojtowicz, J. M. Neuroscience, 2005, 130, 843-52.
[40] Miller, M. W.; Nowakowski, R. S. Brain Res., 1988, 457, 44-52.

Adult Hippocampal Neurogenesis CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 217
[41] Nakagawa, S.; Kim, J. E.; Lee, R.; Chen, J.; Fujioka, T.; Malberg,
J.; Tsuji, S.; Duman, R. S. J. Neurosci., 2002, 22, 9868-76. [42] Zhao, C.; Teng, E. M.; Summers, R. G., Jr.; Ming, G. L.; Gage, F.
H. J. Neurosci., 2006, 26, 3-11. [43] Encinas, J. M.; Vaahtokari, A.; Enikolopov, G. Proc. Natl. Acad.
Sci. USA, 2006, 103, 8233-8. [44] Tozuka, Y.; Fukuda, S.; Namba, T.; Seki, T.; Hisatsune, T. Neuron,
2005, 47, 803-15. [45] Scoville, W. B.; Milner, B. J. Neurol. Neurosurg. Psychiatry, 1957,
20, 11-21. [46] Squire, L. R.; Stark, C. E.; Clark, R. E. Annu. Rev. Neurosci., 2004,
27, 279-306. [47] Gray, J. A.; McNaughton, N. The neuropsychology of anxiety : an
enquiry into the functions of the septo-hippocampal system, Oxford University Press: Oxford ; New York 2000.
[48] Buzsaki, G. Neuron, 2002, 33, 325-40. [49] Gordon, J. A.; Lacefield, C. O.; Kentros, C. G.; Hen, R. J. Neuros-
ci., 2005, 25, 6509-19. [50] Moser, E.; Moser, M. B.; Andersen, P. J. Neurosci., 1993, 13,
3916-25. [51] Bannerman, D. M.; Deacon, R. M.; Offen, S.; Friswell, J.; Grubb,
M.; Rawlins, J. N. Behav. Neurosci., 2002, 116, 884-901. [52] Bannerman, D. M.; Yee, B. K.; Good, M. A.; Heupel, M. J.;
Iversen, S. D.; Rawlins, J. N. Behav. Neurosci., 1999, 113, 1170-88.
[53] McHugh, S. B.; Deacon, R. M.; Rawlins, J. N.; Bannerman, D. M. Behav. Neurosci., 2004, 118, 63-78.
[54] Moser, M. B.; Moser, E. I. Hippocampus, 1998, 8, 608-19. [55] Pitkanen, A.; Pikkarainen, M.; Nurminen, N.; Ylinen, A. Ann. N. Y.
Acad. Sci., 2000, 911, 369-91. [56] van Groen, T.; Wyss, J. M. J. Comp. Neurol., 1990, 302, 515-28.
[57] Rolls, E. T.; Kesner, R. P. Prog. Neurobiol., 2006, 79, 1-48. [58] Rolls, E. T.; Treves, A. Neural Networks and Brain Function,
Oxford UP: New York 1998. [59] Wiskott, L.; Rasch, M. J.; Kempermann, G. Hippocampus, 2006,
16, 329-43. [60] Gilbert, P. E.; Kesner, R. P.; Lee, I. Hippocampus, 2001, 11, 626-
36. [61] Lee, I.; Kesner, R. P. Hippocampus, 2004, 14, 66-76.
[62] Aimone, J. B.; Wiles, J.; Gage, F. H. Nat. Neurosci., 2006, 9, 723-7.
[63] Sheline, Y. I.; Sanghavi, M.; Mintun, M. A.; Gado, M. H. J. Neuro-sci., 1999, 19, 5034-43.
[64] Sheline, Y. I.; Wang, P. W.; Gado, M. H.; Csernansky, J. G.; Van-nier, M. W. Proc. Natl. Acad. Sci. USA, 1996, 93, 3908-13.
[65] Steffens, D. C.; Byrum, C. E.; McQuoid, D. R.; Greenberg, D. L.; Payne, M. E.; Blitchington, T. F.; MacFall, J. R.; Krishnan, K. R.
Biol. Psychiatry, 2000, 48, 301-9. [66] Mervaala, E.; Fohr, J.; Kononen, M.; Valkonen-Korhonen, M.;
Vainio, P.; Partanen, K.; Partanen, J.; Tiihonen, J.; Viinamaki, H.; Karjalainen, A. K.; Lehtonen, J. Psychol. Med., 2000, 30, 117-25.
[67] Campbell, S.; Macqueen, G. J. Psychiatry Neurosci., 2004, 29, 417-26.
[68] Vakili, K.; Pillay, S. S.; Lafer, B.; Fava, M.; Renshaw, P. F.; Bonello-Cintron, C. M.; Yurgelun-Todd, D. A. Biol. Psychiatry,
2000, 47, 1087-90. [69] von Gunten, A.; Fox, N. C.; Cipolotti, L.; Ron, M. A. J. Neuropsy-
chiatry Clin. Neurosci., 2000, 12, 493-8. [70] Posener, J. A.; Wang, L.; Price, J. L.; Gado, M. H.; Province, M.
A.; Miller, M. I.; Babb, C. M.; Csernansky, J. G. Am. J. Psychiatry, 2003, 160, 83-9.
[71] Frodl, T.; Meisenzahl, E.; Zetzsche, T.; Bottlender, R.; Born, C.; Groll, C.; Jager, M.; Leinsinger, G.; Hahn, K.; Moller, H. J. Biol.
Psychiatry, 2002, 51, 708-14. [72] Sheline, Y. I.; Gado, M. H.; Kraemer, H. C. Am. J. Psychiatry,
2003, 160, 1516-8. [73] O'Brien, J. T.; Lloyd, A.; McKeith, I.; Gholkar, A.; Ferrier, N. Am.
J. Psychiatry, 2004, 161, 2081-90. [74] Lucassen, P. J.; Muller, M. B.; Holsboer, F.; Bauer, J.; Holtrop, A.;
Wouda, J.; Hoogendijk, W. J.; De Kloet, E. R.; Swaab, D. F. Am. J. Pathol., 2001, 158, 453-68.
[75] Muller, M. B.; Lucassen, P. J.; Yassouridis, A.; Hoogendijk, W. J.; Holsboer, F.; Swaab, D. F. Eur. J. Neurosci., 2001, 14, 1603-12.
[76] Stockmeier, C. A.; Mahajan, G. J.; Konick, L. C.; Overholser, J. C.; Jurjus, G. J.; Meltzer, H. Y.; Uylings, H. B.; Friedman, L.; Raj-
kowska, G. Biol. Psychiatry, 2004, 56, 640-50.
[77] McEwen, B. S. Annu. Rev. Neurosci., 1999, 22, 105-22.
[78] Reif, A.; Fritzen, S.; Finger, M.; Strobel, A.; Lauer, M.; Schmitt, A.; Lesch, K. P. Mol. Psychiatry, 2006, 11, 514-22.
[79] Gold, P. W.; Gabry, K. E.; Yasuda, M. R.; Chrousos, G. P. Endo-crinol. Metab. Clin. North Am., 2002, 31, 37-62, vi.
[80] Holsboer, F.; Liebl, R.; Hofschuster, E. J. Affect Disord., 1982, 4, 93-101.
[81] Carroll, B. J.; Martin, F. I.; Davies, B. Br. Med. J., 1968, 3, 285-7. [82] Modell, S.; Yassouridis, A.; Huber, J.; Holsboer, F. Neuroendocri-
nology, 1997, 65, 216-22. [83] Board, F.; Persky, H.; Hamburg, D. A. Psychosom. Med., 1956, 18,
324-33. [84] Arborelius, L.; Owens, M. J.; Plotsky, P. M.; Nemeroff, C. B. J.
Endocrinol., 1999, 160, 1-12. [85] Hettema, J. M.; Kuhn, J. W.; Prescott, C. A.; Kendler, K. S. Psy-
chol. Med., 2006, 1-7. [86] Caspi, A.; Sugden, K.; Moffitt, T. E.; Taylor, A.; Craig, I. W.;
Harrington, H.; McClay, J.; Mill, J.; Martin, J.; Braithwaite, A.; Poulton, R. Science, 2003, 301, 386-9.
[87] Willner, P. Neuropsychobiology, 2005, 52, 90-110. [88] Cryan, J. F.; Mombereau, C. Mol. Psychiatry, 2004, 9, 326-57.
[89] Mineur, Y. S.; Belzung, C.; Crusio, W. E. Behav. Brain Res., 2006. [90] Mineur, Y. S.; Prasol, D. J.; Belzung, C.; Crusio, W. E. Behav.
Genet., 2003, 33, 513-9. [91] McEwen, B. S. Metabolism, 2005, 54, 20-3.
[92] Warner-Schmidt, J. L.; Duman, R. S. Hippocampus, 2006, 16, 239-49.
[93] Duman, R. S. Biol. Psychiatry, 2004, 56, 140-5. [94] Dranovsky, A.; Hen, R. Biol. Psychiatry, 2006, 59, 1136-43.
[95] Vollmayr, B.; Simonis, C.; Weber, S.; Gass, P.; Henn, F. Biol. Psychiatry, 2003, 54, 1035-40.
[96] Malberg, J. E.; Duman, R. S. Neuropsychopharmacology, 2003, 28, 1562-71.
[97] Overmier, J. B.; Seligman, M. E. J. Comp. Physiol. Psychol., 1967, 63, 28-33.
[98] Seligman, M. E.; Maier, S. F. J. Exp. Psychol., 1967, 74, 1-9. [99] Cryan, J. F.; Holmes, A. Nat. Rev. Drug Discov., 2005, 4, 775-90.
[100] Willner, P.; Mitchell, P. J. Behav. Pharmacol., 2002, 13, 169-88. [101] Monje, M. L.; Mizumatsu, S.; Fike, J. R.; Palmer, T. D. Nat. Med.,
2002, 8, 955-62. [102] Monje, M. L.; Toda, H.; Palmer, T. D. Science, 2003, 302, 1760-5.
[103] Wojtowicz, J. M. Hippocampus, 2006, 16, 261-6. [104] Bodnoff, S. R.; Suranyi-Cadotte, B.; Quirion, R.; Meaney, M. J.
Psychopharmacology (Berl), 1989, 97, 277-9. [105] Dulawa, S. C.; Holick, K. A.; Gundersen, B.; Hen, R. Neuropsy-
chopharmacology, 2004, 29, 1321-30. [106] Garcia, A. D.; Doan, N. B.; Imura, T.; Bush, T. G.; Sofroniew, M.
V. Nat. Neurosci., 2004, 7, 1233-41. [107] Winocur, G.; Wojtowicz, J. M.; Sekeres, M.; Snyder, J. S.; Wang,
S. Hippocampus, 2006, 16, 296-304. [108] Dupret, D.; Montaron, M. F.; Drapeau, E.; Aurousseau, C.; Le
Moal, M.; Piazza, P. V.; Abrous, D. N. Eur. J. Neurosci., 2005, 22, 778-83.
[109] Phillips, R. G.; LeDoux, J. E. Behav. Neurosci., 1992, 106, 274-85. [110] Castren, E. Curr. Opin. Pharmacol., 2004, 4, 58-64.
[111] Duman, R. S.; Nakagawa, S.; Malberg, J. Neuropsychopharmaco-logy, 2001, 25, 836-44.
[112] Banasr, M.; Soumier, A.; Hery, M.; Mocaer, E.; Daszuta, A. Biol. Psychiatry, 2006.
[113] Malberg, J. E.; Eisch, A. J.; Nestler, E. J.; Duman, R. S. J. Neuros-ci., 2000, 20, 9104-10.
[114] Tanapat, P.; Hastings, N. B.; Reeves, A. J.; Gould, E. J. Neurosci., 1999, 19, 5792-801.
[115] Osterlund, M. K.; Witt, M. R.; Gustafsson, J. A. Endocrine, 2005, 28, 235-42.
[116] Kodama, M.; Fujioka, T.; Duman, R. S. Biol. Psychiatry, 2004, 56, 570-80.
[117] Malberg, J. E.; Schechter, L. E. Curr. Pharm. Des., 2005, 11, 145-55.
[118] Eisch, A. J.; Barrot, M.; Schad, C. A.; Self, D. W.; Nestler, E. J. Proc. Natl. Acad. Sci. USA, 2000, 97, 7579-84.
[119] Yamaguchi, M.; Suzuki, T.; Seki, T.; Namba, T.; Juan, R.; Arai, H.; Hori, T.; Asada, T. Ann. N. Y. Acad. Sci., 2004, 1025, 351-62.
[120] Crews, F. T.; Mdzinarishvili, A.; Kim, D.; He, J.; Nixon, K. Neuro-science, 2006, 137, 437-45.

218 CNS & Neurological Disorders - Drug Targets, 2007, Vol. 6, No. 3 Drew and Hen
[121] He, J.; Nixon, K.; Shetty, A. K.; Crews, F. T. Eur. J. Neurosci.,
2005, 21, 2711-20. [122] Madsen, T. M.; Treschow, A.; Bengzon, J.; Bolwig, T. G.; Lind-
vall, O.; Tingstrom, A. Biol. Psychiatry, 2000, 47, 1043-9. [123] Information, N. C. f. B.; National Library of Medicine, 2003; Vol.
2006. [124] Scott, B. W.; Wojtowicz, J. M.; Burnham, W. M. Exp. Neurol.,
2000, 165, 231-6. [125] Daly, J. J.; Prudic, J.; Devanand, D. P.; Nobler, M. S.; Lisanby, S.
H.; Peyser, S.; Roose, S. P.; Sackeim, H. A. Bipolar Disord., 2001, 3, 95-104.
[126] Esposito, M. S.; Piatti, V. C.; Laplagne, D. A.; Morgenstern, N. A.; Ferrari, C. C.; Pitossi, F. J.; Schinder, A. F. J. Neurosci., 2005, 25,
10074-86. [127] Callaghan, P. J. Psychiatr. Ment. Health Nurs., 2004, 11, 476-83.
[128] Rhodes, J. S.; van Praag, H.; Jeffrey, S.; Girard, I.; Mitchell, G. S.; Garland, T., Jr.; Gage, F. H. Behav. Neurosci., 2003, 117, 1006-16.
[129] van Praag, H.; Shubert, T.; Zhao, C.; Gage, F. H. J. Neurosci., 2005, 25, 8680-5.
[130] Friske, J. E.; Gammie, S. C. Physiol. Behav., 2005, 85, 187-94. [131] Fernandez-Teruel, A.; Escorihuela, R. M.; Castellano, B.; Gon-
zalez, B.; Tobena, A. Behav. Genet., 1997, 27, 513-26. [132] Benaroya-Milshtein, N.; Hollander, N.; Apter, A.; Kukulansky, T.;
Raz, N.; Wilf, A.; Yaniv, I.; Pick, C. G. Eur. J. Neurosci., 2004, 20, 1341-7.
[133] Meshi, D.; Drew, M. R.; Saxe, M.; Ansorge, M. S.; David, D.; Santarelli, L.; Malapani, C.; Moore, H.; Hen, R. Nat. Neurosci.,
2006, 9, 729-31. [134] Kempermann, G.; Brandon, E. P.; Gage, F. H. Curr. Biol., 1998, 8,
939-42. [135] Kempermann, G.; Kuhn, H. G.; Gage, F. H. J. Neurosci., 1998, 18,
3206-12. [136] Brown, J.; Cooper-Kuhn, C. M.; Kempermann, G.; Van Praag, H.;
Winkler, J.; Gage, F. H.; Kuhn, H. G. Eur. J. Neurosci., 2003, 17, 2042-6.
[137] Loo, C. K.; Mitchell, P. B. J. Affect. Disord., 2005, 88, 255-67. [138] Czeh, B.; Welt, T.; Fischer, A. K.; Erhardt, A.; Schmitt, W.; Mul-
ler, M. B.; Toschi, N.; Fuchs, E.; Keck, M. E. Biol. Psychiatry, 2002, 52, 1057-65.
[139] Hedges, D. W.; Higginbotham, B. J.; Salyer, D. L.; Lund, T. D. J. Ect., 2005, 21, 25-30.
[140] Keck, M. E.; Welt, T.; Post, A.; Muller, M. B.; Toschi, N.; Wigger, A.; Landgraf, R.; Holsboer, F.; Engelmann, M. Neuropsychophar-
macology, 2001, 24, 337-49. [141] Sachdev, P. S.; McBride, R.; Loo, C.; Mitchell, P. M.; Malhi, G. S.;
Croker, V. Biol. Psychiatry, 2002, 51, 474-9. [142] Jiang, W.; Zhang, Y.; Xiao, L.; Van Cleemput, J.; Ji, S. P.; Bai, G.;
Zhang, X. J. Clin. Invest., 2005, 115, 3104-16. [143] Shihabuddin, L. S.; Horner, P. J.; Ray, J.; Gage, F. H. J. Neurosci.,
2000, 20, 8727-35. [144] Song, H.; Stevens, C. F.; Gage, F. H. Nature, 2002, 417, 39-44.
[145] Lie, D. C.; Colamarino, S. A.; Song, H. J.; Desire, L.; Mira, H.; Consiglio, A.; Lein, E. S.; Jessberger, S.; Lansford, H.; Dearie, A.
R.; Gage, F. H. Nature, 2005, 437, 1370-5. [146] Kempermann, G.; Jessberger, S.; Steiner, B.; Kronenberg, G.
Trends Neurosci., 2004, 27, 447-52. [147] Seri, B.; Garcia-Verdugo, J. M.; Collado-Morente, L.; McEwen, B.
S.; Alvarez-Buylla, A. J. Comp. Neurol., 2004, 478, 359-78. [148] Abrous, D. N.; Koehl, M.; Le Moal, M. Physiol. Rev., 2005, 85,
523-69. [149] Fukuda, S.; Kato, F.; Tozuka, Y.; Yamaguchi, M.; Miyamoto, Y.;
Hisatsune, T. J. Neurosci., 2003, 23, 9357-66. [150] Bruel-Jungerman, E.; Davis, S.; Rampon, C.; Laroche, S. J. Neuro-
sci., 2006, 26, 5888-93. [151] Derrick, B. E.; York, A. D.; Martinez, J. L., Jr. Brain Res., 2000,
857, 300-7. [152] Parent, J. M.; Yu, T. W.; Leibowitz, R. T.; Geschwind, D. H.;
Sloviter, R. S.; Lowenstein, D. H. J. Neurosci., 1997, 17, 3727-38. [153] Deisseroth, K.; Singla, S.; Toda, H.; Monje, M.; Palmer, T. D.;
Malenka, R. C. Neuron, 2004, 42, 535-52. [154] Deisseroth, K.; Malenka, R. C. Neuron, 2005, 47, 775-7.
[155] Ben-Ari, Y. Nat. Rev. Neurosci., 2002, 3, 728-39.
[156] Malberg, J. E.; Blendy, J. A. Trends Pharmacol. Sci., 2005, 26, 631-8.
[157] Newton, S. S.; Collier, E. F.; Hunsberger, J.; Adams, D.; Terwil-liger, R.; Selvanayagam, E.; Duman, R. S. J. Neurosci., 2003, 23,
10841-51. [158] Altar, C. A.; Laeng, P.; Jurata, L. W.; Brockman, J. A.; Lemire, A.;
Bullard, J.; Bukhman, Y. V.; Young, T. A.; Charles, V.; Palfrey-man, M. G. J. Neurosci., 2004, 24, 2667-77.
[159] Altar, C. A.; Whitehead, R. E.; Chen, R.; Wortwein, G.; Madsen, T. M. Biol. Psychiatry, 2003, 54, 703-9.
[160] Nibuya, M.; Morinobu, S.; Duman, R. S. J. Neurosci., 1995, 15, 7539-47.
[161] Jacobsen, J. P.; Mork, A. Brain Res., 2004, 1024, 183-92. [162] Tardito, D.; Perez, J.; Tiraboschi, E.; Musazzi, L.; Racagni, G.;
Popoli, M. Pharmacol. Rev., 2006, 58, 115-34. [163] Khawaja, X.; Xu, J.; Liang, J. J.; Barrett, J. E. J. Neurosci. Res.,
2004, 75, 451-60. [164] Saarelainen, T.; Hendolin, P.; Lucas, G.; Koponen, E.; Sairanen,
M.; MacDonald, E.; Agerman, K.; Haapasalo, A.; Nawa, H.; Aloyz, R.; Ernfors, P.; Castren, E. J. Neurosci., 2003, 23, 349-57.
[165] Aloyz, R.; Fawcett, J. P.; Kaplan, D. R.; Murphy, R. A.; Miller, F. D. Learning & Memory, 1999, 6, 216-31.
[166] Evans, S. J.; Choudary, P. V.; Neal, C. R.; Li, J. Z.; Vawter, M. P.; Tomita, H.; Lopez, J. F.; Thompson, R. C.; Meng, F.; Stead, J. D.;
Walsh, D. M.; Myers, R. M.; Bunney, W. E.; Watson, S. J.; Jones, E. G.; Akil, H. Proc. Natl. Acad. Sci. USA, 2004, 101, 15506-11.
[167] Tsankova, N. M.; Berton, O.; Renthal, W.; Kumar, A.; Neve, R. L.; Nestler, E. J. Nat. Neurosci., 2006, 9, 519-25.
[168] Jin, K.; Zhu, Y.; Sun, Y.; Mao, X. O.; Xie, L.; Greenberg, D. A. Proc. Natl. Acad. Sci. USA, 2002, 99, 11946-50.
[169] Cao, L.; Jiao, X.; Zuzga, D. S.; Liu, Y.; Fong, D. M.; Young, D.; During, M. J. Nat. Genet., 2004, 36, 827-35.
[170] Fabel, K.; Fabel, K.; Tam, B.; Kaufer, D.; Baiker, A.; Simmons, N.; Kuo, C. J.; Palmer, T. D. Eur. J. Neurosci., 2003, 18, 2803-12.
[171] Huang, E. J.; Reichardt, L. F. Annu. Rev. Neurosci., 2001, 24, 677-736.
[172] Sairanen, M.; Lucas, G.; Ernfors, P.; Castren, M.; Castren, E. Jour-nal of Neuroscience, 2005, 25, 1089-94.
[173] Shirayama, Y.; Chen, A. C.; Nakagawa, S.; Russell, D. S.; Duman, R. S. J. Neurosci., 2002, 22, 3251-61.
[174] Malberg, J. E. Journal of Psychiatry & Neuroscience, 2004, 29, 196-205.
[175] West, A. E.; Griffith, E. C.; Greenberg, M. E. Nat. Rev. Neurosci., 2002, 3, 921-31.
[176] Finkbeiner, S. Neuron, 2000, 25, 11-4. [177] Bonni, A.; Brunet, A.; West, A. E.; Datta, S. R.; Takasu, M. A.;
Greenberg, M. E. Science, 1999, 286, 1358-62. [178] Nakagawa, S.; Kim, J. E.; Lee, R.; Malberg, J. E.; Chen, J.; Steffen,
C.; Zhang, Y. J.; Nestler, E. J.; Duman, R. S. J. Neurosci., 2002, 22, 3673-82.
[179] Thome, J.; Sakai, N.; Shin, K.; Steffen, C.; Zhang, Y. J.; Impey, S.; Storm, D.; Duman, R. S. J. Neurosci., 2000, 20, 4030-6.
[180] Itoh, T.; Tokumura, M.; Abe, K. Eur. J. Pharmacol., 2004, 498, 135-42.
[181] Mayberg, H. S.; Lozano, A. M.; Voon, V.; McNeely, H. E.; Semi-nowicz, D.; Hamani, C.; Schwalb, J. M.; Kennedy, S. H. Neuron,
2005, 45, 651-60. [182] Silasi, G.; Diaz-Heijtz, R.; Besplug, J.; Rodriguez-Juarez, R.; Ti-
tov, V.; Kolb, B.; Kovalchuk, O. Biochem. Biophys. Res. Commun., 2004, 325, 1223-35.
[183] Meltzer, L. A.; Yabaluri, R.; Deisseroth, K. Trends Neurosci., 2005, 28, 653-60.
[184] Feng, R.; Rampon, C.; Tang, Y. P.; Shrom, D.; Jin, J.; Kyin, M.; Sopher, B.; Miller, M. W.; Ware, C. B.; Martin, G. M.; Kim, S. H.;
Langdon, R. B.; Sisodia, S. S.; Tsien, J. Z. Neuron, 2001, 32, 911-26.
[185] Nacher, J.; Crespo, C.; McEwen, B. S. Eur. J. Neurosci., 2001, 14, 629-44.
[186] Overstreet-Wadiche, L. S.; Westbrook, G. L. Hippocampus, 2006, 16, 208-15.
Received: February 5, 2007 Accepted: February 19, 2007