CME Spinal Cord Injury

of 49
-
Upload
ellappa-ghanthan -
Category
Documents
-
view
218 -
download
0
Transcript of CME Spinal Cord Injury
-
8/11/2019 CME Spinal Cord Injury
1/49
Spinal Cord Injuries
-
8/11/2019 CME Spinal Cord Injury
2/49
-
8/11/2019 CME Spinal Cord Injury
3/49
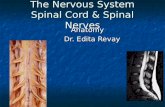
What is the anatomy of the spinal cord on
cross section?
-
8/11/2019 CME Spinal Cord Injury
4/49
What is the anatomy of the spinal cord on
cross section?
-
8/11/2019 CME Spinal Cord Injury
5/49
-
8/11/2019 CME Spinal Cord Injury
6/49
-
8/11/2019 CME Spinal Cord Injury
7/49
-
8/11/2019 CME Spinal Cord Injury
8/49
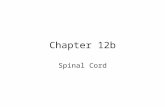
What are the clinically important descending
tracts and where do they cross over?
-
8/11/2019 CME Spinal Cord Injury
9/49
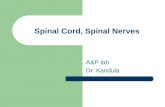
At what level does the spinal cord end and
why is it important?
-
8/11/2019 CME Spinal Cord Injury
10/49
What are the differences between UMN and
LMN? (e.g., cauda equina vs. myelopathy)
-
8/11/2019 CME Spinal Cord Injury
11/49
SPINAL TRAUMA
-
8/11/2019 CME Spinal Cord Injury
12/49
Acute vs. chronic injuries;
complete vs. incomplete injuries
Acute=sudden onset of symptoms
Complete ?
-
8/11/2019 CME Spinal Cord Injury
13/49
What is a completespinal cord injury?
Complete = absence of sensory and motor
function in the perianal area (S4-S5)
-
8/11/2019 CME Spinal Cord Injury
14/49
Terminology
Plegia = complete lesion
Paresis = some muscle strength is preserved
Tetraplegia (or quadriplegia)
Injury of the cervical spinal cord
Patient can usually still move his arms using the segmentsabove the injury (e.g., in a C7 injury, the patient can still flexhis forearms, using the C5 segment)
Paraplegia
Injury of the thoracic or lumbo-sacral cord, or cauda equina
Hemiplegia
Paralysis of one half of the body
Usually in brain injuries (e.g., stroke)
-
8/11/2019 CME Spinal Cord Injury
15/49
Motor: how do you test each segment?
-
8/11/2019 CME Spinal Cord Injury
16/49
Motor: how do you grade the strength?
-
8/11/2019 CME Spinal Cord Injury
17/49
Sensory: how do you determine the level?
-
8/11/2019 CME Spinal Cord Injury
18/49
What are the important vegetative
functions and when are they affected?
-
8/11/2019 CME Spinal Cord Injury
19/49
Reflexes
Deep Tendon Reflexes
Arm
Bicipital: C5
Styloradial: C6
Tricipital: C7
Leg
Patellar: L3, some L4
Achilles: S1
Pathological reflexes
Babinski (UMN lesion)
Hoffman (UMN lesion at or above cervical spinal cord)
Clonus (plantar or patellar) (long standing UMN lesion)
-
8/11/2019 CME Spinal Cord Injury
20/49
What is and how do you determine the level
of injury?
Motor level = the last level with at least 3/5
(against gravity) function NB: this is the most important for clinical purposes
Sensory level = the last level with preservedsensation
Radiographic level = the level of fracture on
plain XRays / CT scan / MRI
NB: spine level does not correspond to spinal cord
level below the cervical region
-
8/11/2019 CME Spinal Cord Injury
21/49
Case scenario
25 y/o male
Fell off the roof (20 feet)
Had to be intubated at the scene by EMS
Consciousness regained shortly thereafter
Could not move arms or legs
Could close and open eyes to command
Not able to breathe by himselftotallydependent on mechanical ventilation
-
8/11/2019 CME Spinal Cord Injury
22/49
High cervical injuries (C3 and above)
Motor and sensory deficits involve the entire
arms and legs
Dependent on mechanical ventilation for
breathing (diaphragm is innervated by C3-C5levels)
-
8/11/2019 CME Spinal Cord Injury
23/49
-
8/11/2019 CME Spinal Cord Injury
24/49
-
8/11/2019 CME Spinal Cord Injury
25/49
What is the difference between spinal shock
and neurogenic shock?
Spinal shock is mainly a loss of reflexes (flaccid
paralysis)
Neurogenic shock is mainly hypotension and
bradycardia due to loss of sympathetic tone
-
8/11/2019 CME Spinal Cord Injury
26/49
-
8/11/2019 CME Spinal Cord Injury
27/49
-
8/11/2019 CME Spinal Cord Injury
28/49
-
8/11/2019 CME Spinal Cord Injury
29/49
Case scenario
22 y/o female
Motor vehicle accident (hit a pole at 60mph)
+ for ethanol and Tetrahydrocannabinol
Short term loss of consciousness (10)
Not able to move or feel her legs
Deep Tendon Reflexes 2+ in both upper
extremities, 0 in both lower extremities No bladder / bowel control or sensation
Sensory level at the umbilicus
-
8/11/2019 CME Spinal Cord Injury
30/49
-
8/11/2019 CME Spinal Cord Injury
31/49
-
8/11/2019 CME Spinal Cord Injury
32/49
-
8/11/2019 CME Spinal Cord Injury
33/49
What is the difference between cauda equina and
conus medullaris syndrome?
-
8/11/2019 CME Spinal Cord Injury
34/49
What is an incompletelesion?
-
8/11/2019 CME Spinal Cord Injury
35/49
-
8/11/2019 CME Spinal Cord Injury
36/49
-
8/11/2019 CME Spinal Cord Injury
37/49
-
8/11/2019 CME Spinal Cord Injury
38/49
-
8/11/2019 CME Spinal Cord Injury
39/49
-
8/11/2019 CME Spinal Cord Injury
40/49
-
8/11/2019 CME Spinal Cord Injury
41/49
Lumbar Puncture
Sedate the patient and make your life easier
Measure opening pressure with legs straight
Always get head CT prior to LP to r/o
increased ICP or brain tumor
-
8/11/2019 CME Spinal Cord Injury
42/49
Cervical Spine Clearance
Occiput to T1 need to be cleared ER, Neurosurgery or Orthopedics physician
If the patient Is awake and oriented
Has no distracting injuries
Has no drugs on board
Has no neck pain
Is neurologically intact
then the c-spine can be cleared clinically, without any need forXRays
CT and/or MRI is necessary if the patient is comatoseor has neck pain
Subluxation >3.5mm is usually unstable
-
8/11/2019 CME Spinal Cord Injury
43/49
Cervical Traction
Gardner-Wells tongs
Provides temporary stability of the cervical spine
Contraindicated in unstable hyperextension injuries
Weight depends on the level
Cervical collar can be removed while patient is in
traction
Pin care: clean q shift with appropriate solution, then
apply povidone-iodine ointment
Take XRays at regular intervals and after every move
from bed
-
8/11/2019 CME Spinal Cord Injury
44/49
-
8/11/2019 CME Spinal Cord Injury
45/49
Surgical Decompression and/or Fusion
Indications
Decompression of the neural elements (spinal cord/nerves)
Stabilization of the bony elements (spine)
Timing Emergent
Incomplete lesions with progressive neurologic deficit
Elective
Complete lesions (3-7 days post injury)
Central cord syndrome (2-3 weeks post injury)
-
8/11/2019 CME Spinal Cord Injury
46/49
-
8/11/2019 CME Spinal Cord Injury
47/49
-
8/11/2019 CME Spinal Cord Injury
48/49
Long term care
Rehab for maximizing motor function
Bladder/bowel training
Psychological and social support
-
8/11/2019 CME Spinal Cord Injury
49/49
THANK YOU!