CMAJ MicieliArshinoff
2
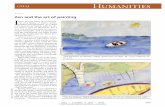
Reerences 1. Fost er A. Vision 2020: the cataract challenge. Community Eye Health 2000;13:17-9. 2. Rach miel R, T rope GE, C hipman ML, et al. C ata- ract surgery rates in Ontario, Canada, rom 1992 to 2004: more surgeries with ewer ophthalmologists. Can J Ophthalmol 2007;42:539-42. 3. Gree nbe rg PB, Tse ng VL, Wu WC, et al. P rev a- 2 Practice CMAJ 4 5 Five things to know about … Cataract surgery Jonathan A. Micieli BSc, Steve A. Arshinoff MD 1 Cataract surgery is one o the most common surgical procedures per- ormed in Canada and worldwide More than 9.5 million cataract surg- eries are perormed worldwide each year. 1 The number o procedures has more than doubled between 1992 and 2004 in the province o Ontario. 2 Through a sma ll i ncision (< 3.0 mm), a phacoemulsifcation probe that oscil- lates at ultrasonic speeds breaks up and removes the opaque cataract lens, and a permanent artifcial lens is in - serted into the original capsule that held the cataract. Serious postoperative complica- tions are uncommon Serious complications rom cata - ract surgery include retinal de - tachment (0.8%) and endoph- thalmitis (0.1%) (Figure 1). 3,4 Posterior capsular opacifcation, a more common postoperative condition (4.2% within 90 days), results rom the prolieration and migration o retained lens epi - thelial cells across the posterior capsule and can be easily treated with a laser to create a clear aperture in the visual axis. 3 3 Patients require glasses or near vision a ter standard cataract surgery Traditional artifcial intraocular lenses, now usually made o acrylic polymers, cannot change shape to allow or clear vision at dierent dis- tances like a young human lens can. One way to eliminate the need or glasses is to use multiocal intraocu- lar lenses Multiocal intraocular lenses simultane- ously ocus images o targets located at dierent distances rom the eye, allow- ing the brain to choose the best ocused image rom each eye. Although patients are generally satisfed with these lenses, some may be intolerant o the haloes, glare and reduced contrast sensitivity associated with them. 5 Another way to eliminate the need or glasses is monovision, whereby the power o the intraocular lens is chosen to enable midrange or near vision in one eye and distance vision in the other eye Ater a period o adaptation, which can take several weeks, the brain learns to select the clearest central image rom one eye at a particular distance and suppress the image rom the other eye. Because there may be some loss o three-dimensional stereo vision with this approach, it may not be suitable or all patients. 6 © 2011 Canadian Medical Association or its licensors CMAJ 1 Figure 1: Injection o prophylactic antibiotic to reduce the risk o postoperative inection and to infate the eye to a normal intraocu- lar pressure. The articial intraocular lens is seen beneath the surgical instrument. lence and predictors o ocular complications asso- ciated with cataract surgery in United States veter- ans. Ophthalmology 2011;118:507-14. 4. Taban M, Behrens A, Newcomb RL, et al. Acute endophthalmitis ollowing cataract surgery: a sys- tematic review o the literature. Arch Ophthalmol 2005;123:613-20. 5. Leyl and M, Pringle E. Multiocal v ersus mono- ocal intraocular lenses ater cataract extraction. Cochrane Database Syst Rev 2006;(4)CD003169. 6. Fink elman YM, Ng JQ, Ba rrett GD. P atien t sat is - action and visual unction ater pseudophakic mono- vision. J Cataract Refract Surg 2009;35:998-1002. Competing interests: Steve Arshino has re- ceived consultancy ees rom ArcticDx and Alcon Laboratories. No competing interests declared by Jonathan Micieli. This article has been peer reviewed. A fliations: From the Faculty o Medicine (Micieli), McGill University, Montréal, Que.; and York Finch Eye Associates (Arshino), Humber River Regional Hospital, Toronto, Ont., the De - partment o Ophthalmology and Vision Sciences (Arshino), University o Toronto, Toronto, Ont., and the Division o Ophthalmology (Arshino), McMaster University, Hamilton, Ont. Correspondence to: Dr. Steve A. Arshino, [email protected] CMAJ 2011. DOI:10.1503/cmaj.110549 Early release, published at www.cmaj.ca on August 8, 2011. Subject to revision.
Transcript of CMAJ MicieliArshinoff

8/3/2019 CMAJ MicieliArshinoff
http://slidepdf.com/reader/full/cmaj-micieliarshinoff 1/1