Clinical Genetics M. Kent Froberg, MD 2009. Purpose This lecture is designed to illustrate two...
47
Clinical Genetics M. Kent Froberg, MD 2009
Transcript of Clinical Genetics M. Kent Froberg, MD 2009. Purpose This lecture is designed to illustrate two...

Clinical Genetics
M. Kent Froberg, MD
2009

Purpose
• This lecture is designed to illustrate two examples of the use of molecular genetics in the clinical laboratory
• Learn the difference between oncogenic and physiological gene rearrangements and how they are demonstrated by PCR & Southern blot
• Learn how Factor V Leiden leads to thrombosis and how to detect the mutation
• Learn the major genetic and environmental causes of thrombosis

CLONALITY
• Clonality of B-cell neoplasms can be demonstrated by molecular techniques
• Can replace demonstration of specific pathological alteration
• PCR and Southern Blot

TYPES OF REARRANGEMENTS
• Pathological oncogenes
• Physiological antigen receptor genes

ONCOGENE REARRANGEMENTS
• Translocations
• Not present in all lymphoid neoplasms
• Often detected by cytogenetics or FISH
• Need prior knowledge of type of tumor and genes
rearranged
• Presently molecular probes not available for 2/3
of lymphomas

IG REARRANGEMENTS
• Physiological
• Since Ig rearrangement is normal for B lymphocytes, neoplasia of B-cell tumors show clonal Ig rearrangement
• Clonality = Malignancy (rare exceptions)

ANTIGEN RECEPTOR REARRANGEMENTS
• Immunoglobulin (Ig) and T-cell Receptor
• Ig rearrangements present in >90% of B-cell
neoplasms
• Detected by Southern Blot or PCR
• Used for Dx, establish lineage, identify minimal
residual disease, Rx

IG REARRANGEMENTS HIERARCHICAL
• Germline Ig specificity determined by somatic rearrangement of heavy & light chain genes
• Involve V (variable), D (diversity), and J (joining) gene segments
• D/J of heavy chain alleles, then V/DJ, followed by kappa light chain, then lambda
• Ig heavy chain selected first, so most commonly rearranged

Heavy chain
rearrangement occurs
first

Kappa light chain
rearrangement
follows, then lambda

Clonality
• Tissue from Pt (biopsy of enlarged lymph node)
• Extract DNA
• Southern blot using probe for conserved region of IgM heavy chain
• If polyclonal smear (no discrete bands) besides germline
• If monoclonal see discrete bands (one germline & one clone)






Single bands indicate clonality


CONCLUSIONS
• Demonstration of Ig Clonal Rearrangement of B-cell lesions by PCR is becoming the standard for many molecular labs in Dx and lineage establishment for B-cell neoplasms
• This method is faster, more economical and more sensitive than other molecular techniques or cytogenetics

HEREDITARY THROMBOPHILIA
• Most Hypercoagulable States are Acquired
– Deficiency of anticoagulant system or defective fibrinolysis
– Post-operative, immobility, pregnancy, trauma, oral contraceptives, SLE, neoplasia
– Need to eliminate acquired causes first

HEREDITARY THROMBOPHILIA
• Anticoagulant Deficiences
– heterozygotes have 35-65% reduction in protein
– have 3-7x risk for venous thrombosis
– deficiencies may be quantitative or qualitative



HEREDITARY THROMBOPHILIA ANTICOAGULANT DEFICIENCIES
• Protein C, Protein S and Anti-thrombin III account
for ~8% of hereditary thrombophilia
• 1st thrombotic event prior to 50
• Anti-thrombin def highest risk
• Need functional & antigenic assays

HEREDITARY THROMBOPHILIA PROTHROMBIN MUTATION
• Described 1996
• G A mutation at nucleotide 20210
• Heterozygotes found in 2.3% of NL population
• 6.2% of pts with venous thrombosis
• Hence, 2.8-fold risk
• Mechanism unknown
• Does serum thrombin levels

HEREDITARY THROMBOPHILIA HYPERHOMOCYSTEINEMIA
• Described 1994
• Acquired (def B12, B6, or folate)
• Hereditary: mutation in one of many enzymes
• Hereditary form accounts for ~20% of venous
thrombosis that is genetic

HEREDITARY THROMBOPHILIA HYPERHOMOCYSTEINEMIA
• Also have risk of atherosclerosis
• Mechanism:
– endothelial dysfunction
– interference with:
• antithrombin
• NO
• thrombomodulin

HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• Described 1993 as activated protein C resistance (APCR)
• Activated protein C cleaves factors V and VIII at specific arginine sites to inhibit coagulation
• Factor V Leiden is a point mutation at 506 in 95% of cases

HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• FV:Q506 = arginine glutamine mutation
• Hence factor V resistant to proteolysis by activated
protein C
• Favors procoagulant state
• Carrier rate 5-7% of caucasians
• Accounts for >50% of hereditary venous thrombosis
(~20% of unselected pts)




HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• Suspect when obvious etiologies of acquired thrombosis have been ruled out
• Pts with thrombosis < 50
• Recurrent thrombosis
• < 50 and > one family member with thrombosis


HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
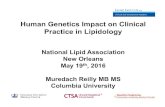
• Diagnosis: Assay for APCR (activated protein C
resistance)
• APCR: PTT performed + and - exogenous activated
protein C
• Plus APC = prolonged PTT
• Normal: ratio +APC/-APC=2.0
• APCR: ratio +APC/-APC<2.0

Normal Factor V
Factor V Leiden

PTT ratio: +APC/-APC is > 2.5 with
wild type Factor V
Ratio is < 2.0 for heterozygous Factor
V Leiden
Ratio is lowest for homozygous
Factor V Leiden
Assay for Activated Protein C Resistance


Case
• 51 year old physician with acute SOB on climbing stairs syncopal episode
• Taken to ED
• Perfusion Scan multiple pulmonary emboli


Followup
• Pt had APCR
• PCR for Factor V Leiden heterozygous
• 49 year old sister with Hx stroke 1 yr previously Factor V Leiden heterozygote
• Son of pt also Factor V Leiden +

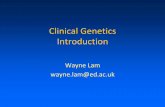
WT Heterozygote Homozygote
PCR for Factor V Leiden Mutation
Mutated band

HEREDITARY THROMBOPHILIA FACTOR V LEIDEN
• Confirmation: DNA analysis by PCR
• Factor V mutation eliminates a Mnl I restriction site
• Blood sample, isolate DNA, amplify mutation site
by PCR, subject to Mnl I cleavage (cleaves at
arginine site)
• Factor V Leiden is resistant to digestion at 506



Relative Risk of Thrombosis
Thrombophilic Status RRNormal 1OCP use 4Protein C, S or ATIII def 5-7Prothrombin 20210 3Hyperhomcysteimemia 2-4Factor V Leiden (heterozygous) 5-7Factor V Leiden + OCP 30-35Factor V Leiden (homozygous) 80

Rx of Hereditary Thrombophilia
• Anticoagulant therapy (heparin, warfarin) • 3% risk of major hemorrhage/yr from Rx• 1/5 fatal• Avoid other risk factors (smoking, OCP)• Genetic counseling