Clinical decision-making in the context of chronic illness
11
Viewpoint Clinical decision-making in the context of chronic illness Susan Watt DSW CSW School of Social Work, McMaster University, Hamilton, Ontario, Canada Introduction Mr and Mrs Arthur have come to see their physician. Mr Arthur is recovering from a surgery for prostate cancer. Mrs Arthur is being treated for high blood pressure and arthritis. He must decide whether or not he will begin a course of radiation therapy; she will be told that she should discontinue her arthritis medication because her blood pressure is elevated. Mr Arthur leaves the meeting with a clear course of action, convinced that he soon will be healthy, and planning for a winter vacation in Florida. Mrs Arthur leaves the same meeting feeling quite concerned about whether she could stay on her medication until next weekend. Her niece is getting married, and Mrs Arthur anticipates increased diculty getting around. She is Correspondence Dr Susan Watt School of Social Work McMaster University 1280 Main Street West Hamilton, Ontario, L8S 4M4 Canada E-mail: [email protected] Accepted for publication 28 September 1999 Keywords: clinical decision-making, chronic illness Abstract This paper develops a framework to compare clinical decision making in relation to chronic and acute medical conditions. Much of the literature on patient-physician decision making has focused on acute and often life-threatening medical situations in which the patient is highly dependent upon the expertise of the physician in providing the therapeutic options. Decision making is often constrained and driven by the overwhelming impact of the acute medical problem on all aspects of the individual’s life. With chronic conditions, patients are increasingly knowledgeable, not only about their medical conditions, but also about traditional, comple- mentary, and alternative therapeutic options. They must make multiple and repetitive decisions, with variable outcomes, about how they will live with their chronic condition. Consequently, they often know more than attending treatment personnel about their own situations, including symptoms, responses to previous treat- ment, and lifestyle preferences. This paper compares the nature of the illness, the characteristics of the decisions themselves, the role of the patient, the decision-making relationship, and the decision- making environment in acute and chronic illnesses. The author argues for a dierent understanding of the decision-making relationships and processes characteristic in chronic conditions that take into account the role of trade-os between medical regimens and lifestyle choices in shaping both the process and outcomes of clinical decision-making. The paper addresses the concerns of a range of professional providers and consumers. 6 Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6–16
-
Upload
susan-watt -
Category
Documents
-
view
213 -
download
1
Transcript of Clinical decision-making in the context of chronic illness

Viewpoint
Clinical decision-making in the contextof chronic illness
Susan Watt DSW CSW
School of Social Work, McMaster University, Hamilton, Ontario, Canada
Introduction
Mr and Mrs Arthur have come to see their
physician. Mr Arthur is recovering from a
surgery for prostate cancer. Mrs Arthur is being
treated for high blood pressure and arthritis. He
must decide whether or not he will begin a
course of radiation therapy; she will be told that
she should discontinue her arthritis medication
because her blood pressure is elevated. Mr
Arthur leaves the meeting with a clear course of
action, convinced that he soon will be healthy,
and planning for a winter vacation in Florida.
Mrs Arthur leaves the same meeting feeling
quite concerned about whether she could stay on
her medication until next weekend. Her niece is
getting married, and Mrs Arthur anticipates
increased di�culty getting around. She is
CorrespondenceDr Susan Watt
School of Social Work
McMaster University
1280 Main Street West
Hamilton, Ontario, L8S 4M4
Canada
E-mail: [email protected]
Accepted for publication28 September 1999
Keywords: clinical decision-making,
chronic illness
Abstract
This paper develops a framework to compare clinical decision
making in relation to chronic and acute medical conditions. Much
of the literature on patient-physician decision making has focused
on acute and often life-threatening medical situations in which the
patient is highly dependent upon the expertise of the physician in
providing the therapeutic options. Decision making is often
constrained and driven by the overwhelming impact of the acute
medical problem on all aspects of the individual's life. With chronic
conditions, patients are increasingly knowledgeable, not only about
their medical conditions, but also about traditional, comple-
mentary, and alternative therapeutic options. They must make
multiple and repetitive decisions, with variable outcomes, about
how they will live with their chronic condition. Consequently, they
often know more than attending treatment personnel about their
own situations, including symptoms, responses to previous treat-
ment, and lifestyle preferences. This paper compares the nature of
the illness, the characteristics of the decisions themselves, the role
of the patient, the decision-making relationship, and the decision-
making environment in acute and chronic illnesses. The author
argues for a di�erent understanding of the decision-making
relationships and processes characteristic in chronic conditions that
take into account the role of trade-o�s between medical regimens
and lifestyle choices in shaping both the process and outcomes of
clinical decision-making. The paper addresses the concerns of a
range of professional providers and consumers.
6 Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16

worried about her doctor's comments that she is
at increased risk for a stroke if her blood pres-
sure remains high. She is convinced that she will
never make it to Florida. The physician is sure
that when he sees Mr Arthur in 3 months he will
be well on the road to recovery but that Mrs
Arthur will return to his o�ce next month in
ongoing distress. Each has participated in a
clinical decision-making encounter ± one related
to an acute illness, the other to chronic condi-
tions. Could we have anticipated these outcomes
and the reactions of the participants based on
our current understanding of clinical decision-
making?
As the population has aged and advances
have occurred in acute medical care, chronic
conditions have become more prevalent. It is
likely that as we age, we will acquire more than
one chronic condition. So great is this increase in
prevalence that recent estimates indicate that in
excess of 60% of the health care expenditures in
North America are committed to the manage-
ment of chronic illnesses. Therefore, on the basis
of clinical frequency and costs, how both
consumers and providers approach decision-
making in relation to chronic conditions
warrants consideration if we are to understand a
major part of our work environment and
improve the quality of clinical decision-making.
Increasingly, responding to people with
chronic illnesses challenges the health care
system, designed to address acute illnesses. The
literature on clinical decision-making largely has
focused on serious, acute medical situations.1±6
Little attention has been placed on under-
standing the similarities and di�erences in clin-
ical decision-making as we currently understand
it, when those decisions relate to chronic
conditions.
Chronic conditions are those illnesses in which
no cure is possible and clinical decisions hold the
potential only for symptom reduction or
containment of deterioration. Even best e�orts
will not eliminate the ultimate life threatening
nature of some of these conditions (e.g. asthma,
chronic obstructive lung disease, and diabetes).
No one clinical decision will hold throughout
the course of the illness; decision-making in
relation to treatment, symptom management,
and lifestyle changes will recur with varying
frequencies. As a result of the increasing
prevalence of chronic conditions, the nature of
those conditions and the need to make multiple
decisions in relation to chronic illness, it is
important for clinicians and researchers to think
carefully about the ways in which decision-
making may vary when used in chronic and
acute illnesses.7
The purpose of this paper is to begin to
develop a framework for understanding the
similarities and di�erences in decision-making
when dealing with acute versus chronic illness.
Understanding clinical decision-making
Clinical decision-making has been studied in the
context of the doctor-patient* relationship.8±11
The models for this relationship, which range
from paternalism to collaborative problem
solving, place the doctor-patient encounter at
the centre of clinical decision-making with
peripheral and varying importance assigned to
the roles of signi®cant others, past experience,
personal preference, and lifestyle choices on the
decisions of the physician or the patient.12±14
Generally, research has focused either on how
to help patients make decisions or on how to
understand the degree of involvement in decis-
ion-making that is desired by the patient.
The ideal situation was cast as one in which the
patient and the physician would make the same
decision, or at least agree upon the most appro-
priate decision.15 It was supposed that decision-
making, which hitherto had been the sole
responsibility of the physician was a rational
process, based on scienti®c evidence and clinical
experience. Therefore, it was argued that patients
would make the same decision as would the
attending physician given an adequate exchange
of information between them.16 Rational, expert-
*The author is aware of the debate in the literature about the
use of the terms patient, consumer, and client. For the
purpose of this paper the term patient is used throughout
when referring to anyone receiving medical care unless a
clear distinction is made in the text.
Clinical decision-making in the context of chronic illness, S Watt
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
7

driven decision-making was viewed as the most
common, if not always preferred, model for these
types of clinical encounters.17,18
It was also argued in this literature that decis-
ion-making was a stable, predicable activity such
that, given the same set of options, the same
patient would make the same decision at di�erent
points in time.19 Indeed, decision-making was
depicted as a single activity or at most a discrete
series of activities which could be systematically
dissected, understood, and analysed. This view of
decision-making as a rational and linear process,
located information seeking on the part of
participants as a central activity, and led to the
position that the sharing of medical information
was central to decision-making whilst the role of
context in the decision-making of either the
consumer or the provider was secondary.20±23
Failure to achieve mutuality, to agree upon a
course of action, was perceived negatively and
labelled in terms of deviance or pathology on the
part of the patient. The physician traditionally
has been seen as the repository of both medical
knowledge and social power. Therefore, any
variation on paternalism in the decision-making
relationship represented an abrogation of power
and authority on the part of the physician.24,25
This interpretation of the physician-patient
relationship has been ®rmly rooted in models of
acute care in which short-term trade-o�s are
made between the physician, the patient, and the
larger society in return for the restoration of
health. The only real choice for the patient is the
decision whether or not to comply with the
physician's recommendation.26
Given that many acute care decision situ-
ations are immediate and high risk, the expert
role of the physician has been valued and
legitimated in decision-making. Generally, in
North America, we look to the physician as the
singular expert on our illnesses and how to treat
them. We want to believe that they know how to
cure our pain and su�ering.
More recently that relationship has been
changing in response to increasingly know-
ledgeable consumers, more ambiguous clinical
challenges and an increasing role of funders in
de®ning the availability of clinical options.
Further, the legitimate claim of other health
clinicians to knowledge about health has chal-
lenged traditional doctor-patient relationships.
These changes have led to both clinicians and
consumers questioning the appropriateness of
the physician as the sole or even dominant
arbitrator of clinical decisions.
When a consumer is facing a chronic illness,
the roles of the physician and the patient are
di�erent. By de®nition, the physician although
an expert, is not the healer and the patient,
despite good intentions and decisions, will not
be cured. How then are decisions and decision-
making under these conditions the same as and
di�erent from decision-making in acute
illnesses?
A framework for understanding
decision-making in chronic conditions
A variety of factors a�ect decision-making in the
context of chronic conditions. Whilst all the
factors exist in both the acute and chronic situa-
tions, their expression may be quite di�erent in
chronic illnesses. The factors that will be
considered in this framework are the nature of
the illness; the characteristics of the decisions to
be made; the role of the individual patient; the
nature of the decision-making relationship; and
the decision-making environment. Each factor is
discussed in the following sections with attention
to the similarities and di�erences in decision-
making in acute and chronic illnesses, and is
summarized in Table 1.
Nature of the illness
Illness in any form disrupts the life of a patient
but acute and chronic illnesses do so in di�erent
ways. When acutely ill, we expect that the
disruption will be time-limited and that we will
return to our previous good health. Having been
diagnosed with a chronic illness, we must
abandon the expectation of recovery in the
foreseeable future.
The division between acute and chronic illness
is an increasingly hazy one. What may begin as
an acute illness may end up being a chronic one
(e.g. a heart attack may herald the presence of
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
Clinical decision-making in the context of chronic illness, S Watt8
chronic arterial disease). Chronic illnesses may
have acute episodes (e.g. episodes of acute
hypoglycaemia in diabetics). Both types of
illness may be life threatening, time and energy
consuming, and ®nancially draining. They both
may have insidious or acute onset and symptoms
with varying degrees of incapacity. Acute
illnesses may also leave the patient with chronic
residual e�ects (e.g. paralysis after a stroke)
which may be devastating in and of themselves
regardless of the underlying pathological
processes.
However, unlike an acute illness, chronic
illness is, by de®nition, long lasting. It also may
produce di�ering, variable, and unpredictable
levels of incapacity and in many cases that
incapacity will increase over time. Even with
good choices, the results of following treatment
recommendations will not be a cure. At best, the
individual with a chronic illness can expect
remission or control of symptoms, a delay in
disease progression, or the prevention of
sequelae.
The illness remains and is likely to have an
increasing impact on the life of the individual.
One may be able to `buy time' or delay
symptoms, but the illness persists and one is
never again completely well. Normal life
routines will now include simple or complex
observation, intervention, and evaluation of
not only one's own health but also one's
illness.
One's de®nition of self as healthy and able,
which may be shaken by an acute illness, is
forever changed by a chronic illness.27±31 In its
simplest course, with an acute illness, the indi-
vidual gets sick, gets treatment, and gets well.
This is not the case with a chronic illness.
Even when making decisions in relation to
acute medical conditions, the pervasiveness of
the chronic condition is evident. For example,
decisions concerning the management of relat-
ively minor infections are modi®ed by the
presence of diabetes; chronic obstructive lung
disease changes treatment options for a
myocardial infarction. Patients may see them-
selves, or be seen by others including their
physicians, family, and coworkers, as their
disease (e.g. the diabetic, the arthritic) again
demonstrating the invasive and pervasive
quality of chronic illness.
Decisions ± nature, number and evidence used
For an acute illness, there is a direct relationship
between the illness and its treatment. There is an
assumption that the treatment will result in a
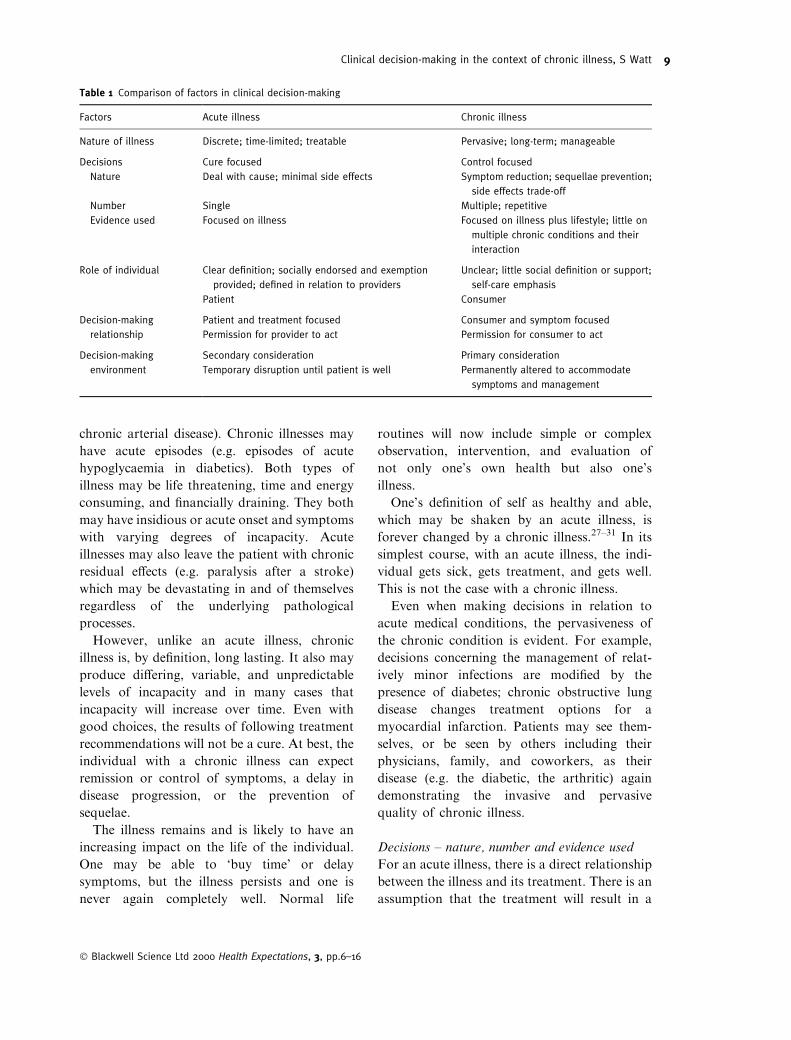
Table 1 Comparison of factors in clinical decision-making
Factors Acute illness Chronic illness
Nature of illness Discrete; time-limited; treatable Pervasive; long-term; manageable
Decisions Cure focused Control focused
Nature Deal with cause; minimal side effects Symptom reduction; sequellae prevention;
side effects trade-off
Number Single Multiple; repetitive
Evidence used Focused on illness Focused on illness plus lifestyle; little on
multiple chronic conditions and their
interaction
Role of individual Clear de®nition; socially endorsed and exemption
provided; de®ned in relation to providers
Unclear; little social de®nition or support;
self-care emphasis
Patient Consumer
Decision-making Patient and treatment focused Consumer and symptom focused
relationship Permission for provider to act Permission for consumer to act
Decision-making Secondary consideration Primary consideration
environment Temporary disruption until patient is well Permanently altered to accommodate
symptoms and management
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
9Clinical decision-making in the context of chronic illness, S Watt

cure. The range of options that will cure the
illness with the fewest and/or least serious side-
e�ects frames a care decision faced by both the
provider and the patient. Providers know, and
patients are cautioned, that in some instances a
cure will not result from treatment or that there
will be side-e�ects from the treatment. However,
any decision to act is predicated on a funda-
mental assumption that the disease can be cured
and that providers know what treatment will
work for a speci®c condition. Therefore, in
addition to a positive outcome in an acute
illness, there is a presumption that only one
major decision is necessary in relation to any
given episode.
For example, for the patient with an acute
appendix, decision-making is highly restricted ±
operate or risk dying from a ruptured appendix.
Once this decision has been made, it is assumed
that a reasonably predicable course of treatment
and recovery will follow. The trade-o� is clear
and, in this example at least, normally would
require little deliberation. With more high-risk
procedures the decision to treat, whilst more
complicated, is focused by an assumption of
cure.
In chronic illnesses, the nature of the decision
is often what Gafni has de®ned as `what if'
options.11 What if we were able to prevent future
damage? What if we could reduce, but not
eliminate, symptoms? What if we could reduce
your pain, but shorten your life?
The outcomes of each option are often
unpredictable, involve trade-o�s amongst neg-
ative options, and are not perceived by either the
provider or the patient as optimal. They are
essentially `phantom options' which inevitably
fall short of the desired outcome of cure. The
essential trade-o�s, which de®ne the decision
options, are far less clear or certain than in most
acute situations. The focus becomes manage-
ment not cure.
The number of decisions that must be made in
relation to a chronic illness also di�ers from the
number of decisions made about an acute illness.
There is no one decision. Instead, there is a series
of multiple decisions, often made each day, and
most often requiring trade-o�s with non-medical
variables.32±34 For example, diabetics must
decide many times each day whether or not to
inject insulin, how much insulin to take, and
consequently, how much of what type of food
they will eat, how much they will exercise, and
when all of these activities will occur. These
decisions become solely those of the patient who
then must develop a sophisticated understanding
of their illness and treatments, therapeutic
options, and the short and long-term conse-
quences of their decisions, some of which, as in
the case of the diabetic, may be immediately life
threatening.
Normally an individual has only one acute
illness at a time. However, individuals often
have more than one chronic illness. Each illness
has its own management regimen and, with this
accumulation, the regimens may become
competitive. For example, one medication is
taken twice a day whilst another, if compatible
with the ®rst, is taken every 4 hours. One illness
may require bed rest whilst another, regular
aerobic exercise. Choices must be made between
these competing regimens. Each choice requires
an evaluation of the relative merits of potential
outcomes created by sacri®cing one regimen to
another. These judgements are often made
without expert guidance but with con¯icting and
compelling advice from the respective specialists
consulted for each condition.
The accumulation of chronic illnesses will
impair the overall health status of the individual
and may drive certain clinical decisions.
The impact may not be just additive but also
exponential. For example, the person with
hypertension may take medications that predis-
pose them to Type II diabetes.
Time also takes on a di�erent meaning.
Treatments, like the illnesses themselves, never
end. Whilst they may change from time to time
to re¯ect changes in knowledge, treatment
options, or treatment preferences,35±38 they must
become part of the life of the individual and
their family for an inde®nite period and tend to
increase rather than decrease over time.
Normal life events further complicate many
chronic conditions (e.g. pregnancy and dia-
betes).26 Commitment to long-term treatment
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
10 Clinical decision-making in the context of chronic illness, S Watt

regimens is increasingly di�cult, as both the
temporal and causal link between treatment and
outcome is attenuated.39
Although the relationship between treatment
and outcome is clearer in acute illnesses,
compliance with treatment regimens has been
estimated at only 30±40%. When this rela-
tionship is even less evident, as it is in chronic
conditions, it is hard to imagine that someone
will be able to adhere to often complex,
demanding, and expensive treatment regimens.
When the patient cannot ®nd an immediate
link between treatment and its bene®ts, the
likelihood of compliance is decreased. Non-
compliance often leads to both the patient and
the provider believing that they have failed.
Even when available, research evidence
concerning treatment e�cacy is usually
restricted to speci®c illnesses.25 Little evidence
is available to either the physician or the
patient upon which to base decisions about
competing therapeutic choices for multiple
conditions ± a situation already identi®ed as
an increasingly common one.
In summary, the characteristics of the decis-
ions facing people with acute and chronic
conditions share some common features such
as weighing trade-o�s and anticipating
outcomes. However, in terms of the nature of
the decisions, the number of decisions, and the
evidence availability of useful evidence for both
providers and consumers, there is a major
di�erence in the characteristics of the decisions
themselves.
The role of the individual
The `sick role' de®nes the behaviours and
responsibilities expected of acutely ill individuals
as patients, exempting them from a variety of
social responsibilities, whilst getting well. On the
other hand, the person with a chronic condition
is often not perceived to be sick, despite the
presence of symptoms, a diagnosis, and medical
regimens. In fact, their patient role, present at
the time of initial diagnosis, is transformed often
into the role of a health care consumer.
In the process of decision-making, the indi-
vidual who is chronically ill lacks a clearly
established and socially validated role. Anger
and demands for accountability may replace
concern and exemption, the initial response of
others to an episode of acute illness.
There is signi®cant impact on family rela-
tions. Marriage can serve as either a bu�er or
`stressor' for the chronically ill person.40
Partners, relatives, friends, and colleagues are
often at a loss to know how to respond
beyond the acute phase or initial diagnosis.
They often interpret symptom remission, a
primary goal of intervention, as a sign of cure.
They, too, are faced with integrating decision-
making concerning their roles in relation to
the chronic illness into their lives and their
relationship with the patient.
The family may have to reorient their decis-
ion-making activities. Families, which are
traditionally oriented to the rearing of children,
are faced with both participating in decision-
making and being a�ected by the decisions made
by the chronically ill person (e.g. how much of a
care giving role will they take on; mother will no
longer drive the kids to hockey practice). They
will become active or passive participants in
decision-making.
There may be not only a decrease in the
resources available for the family but also a
redistribution of resources to meet the require-
ments of the chronically ill member. New
decisions will have to be made about how to deal
with these changing resources. Time, money,
emotional and social resources are changed by
the results of these decisions. Unlike child
rearing, the outcomes of these allocations are
not decreasing demands on resources, but the
probability of changing and likely increasing
demands over time. Much variation has been
found in the ways in which families adapt to
these changes; but they will change and be
changed.27,41,42
Chronic illnesses are the subjects of beliefs,
superstitions, cultural interpretation, and indi-
vidual meaning in much the same way as acute
illnesses.29,43 The meaning of chronic illness is
di�erent from acute illness for patients, provi-
ders and signi®cant others.14,28,30,31 Notions of
impairment, disability, and incapacity modify
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
11Clinical decision-making in the context of chronic illness, S Watt

the sick role. Individuals must adapt their de®-
nitions of themselves to the limitations, demands
and anticipated future imposed by the chronic
condition. In keeping with the ways in which
they change their self-image, the person with a
chronic illness will approach decision-making
with a di�erent perspective.
The patient largely operationalizes complex
and ongoing care decisions. The patient-as-pro-
vider becomes yet another role that distinguishes
the individual with an acute illness from one
with a chronic illness. Self-care is a hallmark of
chronic illness.28,29 Instead of the usual exemp-
tion from responsibility, self-care increases
responsibility on the patient often requiring that
the patient assimilate new knowledge and add
skills, which were neither sought nor desired by
the patient. Imposed by providers and the
community, the new role of `person with a
chronic illness' ± a health care consumer ± now
must be learned, practiced and adapted to the
con®guration of that particular individual in
their unique biopsychosocial environment.
Taking on this new role will in¯uence how the
patient approaches and deals with decision-
making.
Thus, whilst individuals with any illness take
one of their roles from that circumstance, an
acute illness casts the individual in the socially
de®ned and recognized role of patient with all
the rights and responsibilities characteristic of
that role. For the individual with a chronic
illness, the role is less well de®ned and tested. It
appears to be emerging as one more closely
aligned with our concept of a consumer rather
than a patient. Consumers are distinct from
patients in as much as they are expected to make
decisions based on the best available evidence,
product availability, and personal preference.
Consumer loyalty and trust is thought to be
earned through demonstration rather than
assumed as a function of provider status. Decis-
ion-making by the consumer is viewed as
rational and within their exclusive control.
Consumers are not provided with the exemp-
tions and protections associated with being a
patient.
The nature of the decision-making relationship
In chronic illnesses, the patient's relationships
with health care providers are complex. In the
Canadian health care system, family physicians
carry the major medical role with specialists
having episodic involvement. Therefore, clinical
decision-making involves at least two providers
as well as the patient. In contrast to the patient-
physician dyad, typically described in acute
illnesses, dyadic coalitions of provider-provider
or provider-patient can complicate decision-
making. Where medical information is not
de®nitive, physicians may disagree with one
another. For every additional provider the
probability of disagreement and of coalitions
increases.
The relationship with a family physician, and
probably a specialist, is necessarily long-term.
Systems of delivery may restrict the degree of
consumer choice of physician either by the
method of payment or the availability of provi-
ders. Episodic acute illness may add other
providers and further complicate decision-
making relationships.
With both acute and chronic illnesses, these
relationships exist for the sole purpose of caring
for the patient. The relationships are the vehicles
for the conveying of particular types of infor-
mation between the patient and the provider. As
they are professional relationships, they are
simultaneously patient and task focused, invol-
ving a series of negotiations about the care of the
patient. In relation to an acute illness, those
actions usually are performed or directed by the
provider. On the other hand, in relation to
chronic illness, the patient usually performs
those actions. Thus, the focus in one relationship
is on decisions that permit the provider to act
whilst, in the other, it is on permission for the
patient to act.
Patients are faced with the pre-eminence of
physical health criteria in evaluating their ability
to cope. The signs and symptoms of illness have
di�erent meanings for patients and providers
and hence di�erent impacts on the decision-
making relationship. For example, for the
rheumatologist, newly reported pain in ®nger
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
12 Clinical decision-making in the context of chronic illness, S Watt

joints is an indication of increased joint
involvement in arthritis. For the patient, the
same change in pain may prompt the giving up
of an activity such as sewing.
This di�erence in interpretation may not seem
to be a major problem. However, if sewing is the
individual's way to clothe a family or to give
gifts, or to be creative, the decision to give up
this one activity may have major ®nancial,
social, or psychological rami®cations of long
duration. Those who make the decision to
continue the activity in the face of painful
symptoms are likely to be criticized. Their ability
to make future decisions may be called into
question by providers and other signi®cant
people in their lives. These people may fail to
understand the di�erent meaning given to
symptoms by patients and providers, and the
trade-o� between physical symptoms and func-
tioning that are made by patients.
Whilst patients generally have become more
knowledgeable about health matters, those with
chronic conditions and access to the latest
information through the World Wide Web and
self-help sources, and a focus on their particular
problem, may have even more recent informa-
tion than many of their service providers. Their
decisions are in¯uenced by this information not
only in terms of treatment choices, but also in the
ways in which they evaluate treatment outcomes.
As providers of much of their own treatment,
whether willing or unwilling, patients with
chronic illnesses become both their own care
providers and evaluators. In the truest sense they
become consumers rather than patients. Thus,
whilst decision-making in acute situations
provides direction to providers, generally, decis-
ion-making in relation to chronic illnesses
directs the activities of patients.
The decision-making environment
Decisions concerning both acute and chronic
illnesses happen in a personal and social context.
Both acute and chronic illnesses are a�ected by
and disrupt this environment but in di�erent
ways.
Acute illness necessitates an abrupt but
temporary disruption. Decisions need to be
made in a timely manner and there is often a
sense that the illness is the dominant factor in
the life of the patient and their support system.
Tasks of daily living are displaced by the
immediate care seeking activities. Environment
is an obstacle to be overcome and is secondary
to the clinical decisions that are being made.
Tasks related to help seeking become the focus
of everyone's attention.
Chronic illness lacks the urgency accorded
acute illness. There is a sense, beyond the
initial diagnosis, that there is little urgency in
the situation. Securing and attending at
appointments is somehow less important than
with an acute illness. At least on the surface,
daily routines retain their pre-illness import-
ance and care seeking is `worked into' existing
schedules and commitments. There seems to be
time to think about clinical decisions, to delay
commitment, and to change your mind. The
home and work environment retains its pre-
eminence despite being permanently altered by
the symptoms and management of a chronic
illness.
As a result of the duration of the illness and
the complexity of treatment regimens, chronic
illnesses necessarily involve others who parti-
cipate in decision-making in multiple and
meaningful ways. As discussed early in this
paper, family members, friends and colleagues
are called upon to participate in decision-
making and to enact the decisions that are
made. The degree of involvement of others is
variable, determined not only by the care and
support needs of the patient but also by their
pre-illness relationships. They are called upon
to make a long-term commitment to support
the patient in making and acting upon their
decisions. Relationships must be renegotiated
to accommodate these new responsibilities and
obligations.
Conclusions
Decision-making is a complex process in which
both individual and environmental factors play
important roles. In both acute and chronic
conditions, the patient and provider are faced
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
13Clinical decision-making in the context of chronic illness, S Watt

with making decisions based on limited infor-
mation as to which option will produce the best
results in a speci®c situation.
In this paper it has been argued that clinical
decision-making in relation to acute and chronic
illnesses share some similarities but also striking
di�erences. These di�erences re¯ect the charac-
teristics of the illnesses, the diversity in the
nature and number of decisions to be made, the
di�erential availability of clinical evidence,
the distinctiveness of the patient role in each
situation, the subtleties of decision-making
relationships, and the di�erential impact of these
components in the decision-making environ-
ment.
Any individual who is chronically ill may be
involved in many types of clinical decision-
making. The presence of a chronic illness does
not determine how all clinical decisions will be
made. There may be di�erent decision-making
processes used at di�erent stages of the illness,
or for acute episodes of an illness that is
normally quiescent. Still another decision-
making process may be invoked for acute
illnesses.
Patients' decision-making ability is deter-
mined in large measure by their ability to exert
command over symptoms, treatments, personal
and social resources, and even over providers.
This ability is compromised during an acute
illness when providers control the information,
skills, and resources needed to restore health.
The patient's ability to exercise control in this
situation is seriously limited and their involve-
ment in decision-making re¯ects the willingness
of providers to relinquish clinical decision-
making control.
In chronic conditions, providers normally
hold little in the way of unique expertise and no
curative ability. Therefore clinical decision-
making is focused on disease management and
the patient is not only empowered, but also often
required, to take an active and central role in
this process.
Thus, the management strategies and expected
outcomes signi®cantly alter the role of both
patient and provider. Little is known about how
either patients or providers de®ne and adapt to
these changes. The added complexity of moving
from acute to chronic situations in the same
relationship, as is the case with the family
physician-patient relationship, is even less well
understood.
The framework presented in this paper begins
to address some of the distinguishing factors
that characterize these processes. In addition to
understanding the roles of the participants, we
need to understand the environments in which
the decision is being made and the processes
used in these decision-making circumstances.
Therefore, we need to research di�erent decis-
ion-making styles of both patients and of
providers and how these styles are enacted in a
variety of clinical decision-making encounters.
We need a better understanding of how decision-
making results in congruent or con¯icting
outcomes and how all participants evaluate such
outcomes if we are to understand this aspect of
clinical decision-making.
References11
1 Benbassat J, Pilpel D, Tidhar M. Patients' preferences
for participation in clinical decision making: a review
of published surveys. Behavioral Medicine, 1998;
24 (2): 81±88.
2 Guadagnoli E, Ward P. Patient participation in
decision making. Social Science and Medicine, 1998;
47 (3): 329±339.
3 Levine MN, Gafni A, Markham B et al. A bedside
decision instrument to elicit a patient's preference
concerning adjunctive chemotherapy for breast
cancer. Annals of Internal Medicine, 1992; 117: 53±58.
4 Petrisek AC, Laliberte LL, Allen SM, Mor V. The
treatment decision-making process: age differences in
a sample of women recently diagnosed with non-
recurrent, early-stage breast cancer. Gerontologist,
1997; 37 (5): 598±608.
5 Whittaker AA, Albee BJ. Factors in¯uencing patient
selection of dialysis treatment modality. American
Nephrology Nurses' Association Journal,2 1996; 23 (4):
369±375.
6 Chewning B, Sleath B. Medication decision making
and management: a client-centred model. Social
Science and Medicine, 1996; 42 (3): 389±398.
7 Pawlson LG. Chronic illness: implications of a new
paradigm for health care. Journal on Quality
Improvement, 1994; 20 (1): 33±39.
8 Beisecker A, Beisecker T. Using metaphors to char-
acterize doctor-patient relationships: paternalism
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
14 Clinical decision-making in the context of chronic illness, S Watt

versus consumerism. Health Communication, 1993;
5: 41±58.
9 Emanuel EJ, Emanuel LL. Four models of the
physician-patient relationship. Journal of the Amer-
ican Medical Association, 1992; 267 (16): 2221±2226.
10 Twemlow SW, Bradshaw SL Jr, Coyne L, Lerma BH.
Patterns of utilization of medical care and perceptions
of the relationship between doctor and patient with
chronic illness including chronic fatigue syndrome.
Psychology Report, 1997; 80 (2): 643±658.
11 Charles C, Gafni A, Whelan T. Decision making in
the physician-patient encounter: revisiting the shared
treatment decision-making model. Hamilton,
Ontario: CHEPA Working Paper, 1998.
12 Donovan JL. Patient decision making. The missing
ingredient in compliance research. International
Journal of Technology Assessment in Health Care,
1995; 11 (3): 443±455.
13 Playle JF, Keeley P. Non-compliance and profes-
sional power. Journal of Advanced Nursing, 1998;
27 (2): 304±311.
14 Wiebe JS, Christensen AJ. Patient adherence in
chronic illness: personality and coping in context.
Journal of Personality, 1996; 64 (4): 815±835.
15 Charles C, Gafni A, Whelan T. Shared decision
making in the medical encounter: what does it mean?
(or it takes at least two to tango). Social Science and
Medicine, 1997; 44 (5): 681±692.
16 Coulter A. Partnerships with patients: the pros and
cons of shared clinical decision making. Journal of
Health Services Research & Policy, 1997; 2:
112±121.
17 Quill TE, Brody H. Physician recommendations and
patient autonomy: ®nding a balance between physi-
cian power and patient choice. Annals of Internal
Medicine, 1996; 125 (9): 763±769.
18 Deber R. Physicians in health care management: 8.
The patient-physician partnership: decision making,
problem solving, and the desire to participate. Cana-
dian Medical Association Journal, 1994; 151 (4):
423±427.
19 Gafni A. Time in health: can we measure individuals'
`pure time preferences'? Medical Decision Making,
1995; 15 (1): 31±37.
20 Llewellyn-Thomas HA. Patients' health-care decision
making: a framework for descriptive and experi-
mental investigations. Medical Decision Making,
1995; 15 (2): 101±106.
21 Roter DL, Hall JA. Why physician gender matters in
shaping the physician-patient relationship. Journal of
Women's Health, 1998; 7 (9): 1093±1097.
22 Toombs SK. The Meaning of Illness. Boston. Kluwer
Academic Publishers, 1992: 1±25.
23 Ende J, Kazis L, Ash A, Moskowitz MA. Measuring
patients' desire for autonomy: decision making and
information-seeking preferences amongst medical
patients. Journal of General Internal Medicine, 1989;
4 (1): 23±30.
24 Gafni A, Charles C, Whelan T. The physician-patient
encounter: the physician as a perfect agent for the
patient versus the informed treatment decision-
making model. Social Science and Medicine, 1998;
47 (3): 347±354.
25 Loewe R, Schwartzman J, Freeman J, Quinn L,
Zucherman S. Doctor talk and diabetes: towards and
analysis of the clinical construction of a chronic
illness. Social Science and Medicine, 1998; 47 (9):
1267±1276.
26 Cameron K, Gregor F. Chronic illness and compli-
ance. Journal of Advanced Nursing, 1987; 12 (6):
671±676.
27 Andersen R, Bury M. Living with Chronic Illness: the
Experience of Patients and Their Families. London.
Unwin Hyman, 1988: 245±258.
28 Baker C, Stern PN. Finding meaning in chronic illness
as the key to self-care. Canadian Journal of Nursing
Research, 1993; 25 (2): 23±36.
29 Connelly CE. An empirical study of a model of self-
care in chronic illness. Clinical Nurse Specialist, 1993;
7 (5): 247±253.
30 Lindsey E. Experiences of the chronically ill. A covert
caring for the self. Journal of Holistic Nursing, 1997;
15 (3): 227±242.
31 Sherman JJ, Hughes ME, Tavakoli A. The relation-
ship amongst health status, functional status, and
chronic illness. Health Values, 1995; 19 (5): 3±9.
32 Pierce PF. When the patient chooses: describing
unaided decisions in health care. Human Factors,
1996; 38 (2): 278±287.
33 Ubel PA, Loewenstein G. The role of decision anal-
ysis in informed consent: choosing between intuition
and systematicity. Social Science and Medicine, 1997;
44 (5): 647±656.
34 Mehrez A, Gafni A. Quality-adjusted life years, utility
theory, and health-years equivalents. Medical Deci-
sion Making, 1989; 9 (2): 142±149.
35 Barry MJ, Fowler FJ Jr, Mulley AG, Henderson JV
Jr, Wennberg JE. Patient reactions to a program
designed to facilitate patient participation in treat-
ment decisions for benign prostatic hyperplasia.
Medical Care, 1995; 33 (8): 771±782.
36 Gafni A. Economic implications of IGT intervention:
the case of a `phantom alternative'? Diabetic Medi-
cine, 1996; 13 (3 (Suppl. 2): S25±S28.
37 Gafni A, Gibson ES, Johnston M et al. Is there a
trade-o� between income and health? The case of
hypertensive steelworkers in Canada. Inquiry, 1983;
20 (4): 343±349.
38 Wynne A, Monks J. Patients' decisions about conti-
nuing with therapy in chronic illness: a study of
hyperbaric oxygen therapy in multiple sclerosis.
Family Practice, 1989; 6 (4): 268±273.
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
15Clinical decision-making in the context of chronic illness, S Watt
39 Ubel PA, Spranca MD, Dekay ML, Hershey JC, Asch
DA. Public preferences for prevention versus cure:
what if anounce of prevention isworthonly anounceof
cure?Medical Decision Making, 1998; 18 (2): 141±148.
40 Revenson TA. Social support and marital coping with
chronic illness. Annals of Behavioral Medicine, 1994;
16 (2): 122±130.
41 Lieberman MA, Fisher L. The impact of chronic
illness on the health and well-being of family
members. Gerontologist, 1995; 35 (1): 94±102.
42 Patterson JM & Garwick AW. The impact of
chronic illness on families: a family systems
perspective. Annals of Behavioral Medicine, 1994;
16 (2): 131±142.
43 Bates MS, Rankin-Hill L, Sanchez-Ayendez, M.
The effects of the cultural context of health care on
treatment of and response to chronic pain and
illness. Social Science and Medicine, 1997; 45 (9):
1433±1447.
Ó Blackwell Science Ltd 2000 Health Expectations, 3, pp.6±16
16 Clinical decision-making in the context of chronic illness, S Watt