Anu Peltola & Mikael Gummerus, FROSMO, Winning the future of UX, 26.10.2016

of 10
Upload
erlangga-perwira-negaraCategory
view
213download
07/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
1/10
Glycerol vs. Dexamethasone in Meningitis CID 2007:45 (15 November) 1277
M A J O R A R T I C L E
Adjuvant Glycerol and/or Dexamethasone to
Improve the Outcomes of Childhood BacterialMeningitis: A Prospective, Randomized, Double-Blind, Placebo-Controlled Trial
Heikki Peltola,1 Irmeli Roine,3 Josefina Fernandez,4 Ines Zavala,5 Silvia Gonzalez Ayala,7 Antonio Gonzalez Mata,10
Antonio Arbo,12 Rosa Bologna,8 Greta Mino,6 Jose Goyo,11 Eduardo Lopez,9 Solange Dourado de Andrade,13
and Seppo Sarna2
1Helsinki University Central Hospital, Hospital for Children and Adolescents, and 2University of Helsinki, Department of Public Health, Helsinki,
Finland; 3University Diego Portales, Faculty of Health Sciences, Santiago, Chile; 4Clinica Infantil Dr. Robert Reid Cabral, Santo Domingo,
Dominican Republic; 5Hospital de Ninos Dr. Roberto Gilbert, and 6Hospital del Nino Dr. Francisco de Icaza Bustamante, Guayaquil, Ecuador;7Hospital de Ninos Sor Mar a Ludovica, La Plata, and 8Hospital de Pediatra Dr. Juan P. Garrahan and 9Hospital de Ninos Dr. Ricardo Gutierrez,
Buenos Aires, Argentina; 10Hospital Pediatrico Dr. Agustin Zubillaga, Barquisimeto, and 11Hospital Universitario de los Andes, Merida, Venezuela;12Instituto de Medicina Tropical, Universidad Nacional de Asuncion, Asuncion, Paraguay; and 13Fundacao de Medicina Tropical do Amazonas,
Institute for Tropical Diseases, Manaus, Brazil
(See the editorial commentary by Saez-Llorens and McCracken on pages 12879)
Background. Despite favorable meta-analyses, no study involving third-generation cephalosporins for the treat-ment of childhood bacterial meningitis has documented a benefit of adjuvant dexamethasone therapy if theoutcomes are examined individually.
Methods. We conducted a prospective, randomized, double-blind trial comparing adjuvant dexamethasone orglycerol with placebo in children aged from 2 months through 16 years in Latin America. Ceftriaxone wasadministered to all children; children were randomized to also receive dexamethasone intravenously, glycerol orally,both agents, or neither agent. Primary end points were death, severe neurological sequelae, or deafness, with thefirst 2 end points forming a composite end point. A subgroup analysis for Haemophilus influenzaetype b meningitiswas undertaken. Intention-to-treat analysis was performed using binary logistic regression models.
Results. H. influenzaetype b, pneumococci, and meningococci were the main agents found among 654 patients;dexamethasone was given to 166, dexamethasone and glycerol were given to 159, glycerol was given to 166, andplacebo was given to 163. No adjuvant therapy significantly affected death or deafness. In contrast, glycerol anddexamethasone plus glycerol reduced severe neurological sequelae, compared with placebo; the odds ratios were0.31 (95% confidence interval [95% CI], 0.130.76; ) and 0.39 (95% CI, 0.170.93; ), respectively.Pp .010 Pp .033For neurological sequelae and death, the odds ratios were 0.44 (95% CI, 0.250.76; ) and 0.55 (95% CI,Pp .0030.320.93; ), respectively. Dexamethasone therapy prevented deafness in patients with H. influenzaetypePp .027b meningitis only if patients were divided grossly into dexamethasone recipients and nonrecipients and if timingbetween dexamethasone and ceftriaxone administration was not taken into account (odds ratio, 0.27; 95% CI,0.090.77; ).Pp .014
Conclusion. Oral glycerol therapy prevents severe neurological sequelae in patients with childhood meningitis.Safety, availability, low cost, and oral administration also add to its usefulness, especially in resource-limited settings.
Despite successful Haemophilus influenzaetype b (Hib)
and Streptococcus pneumoniae vaccinations in many
Received 2 March 2007; accepted 24 July 2007; electronically published 15
October 2007.
Reprints or correspondence: Prof. H. Peltola, HUCH, Hospital for Children and
Adolescents, P.O. Box 281 (11 Stenback St.), 00029 HUS Helsinki, Finland
Clinical Infectious Diseases 2007;45:127786
2007 by the Infectious Diseases Society of America. All rights reserved.
1058-4838/2007/4510-0004$15.00
DOI: 10.1086/522534
parts of the world [1], childhood bacterial meningitis
remains a challenge [24]. Even when seasonal menin-
gococcal epidemics in Africa are excluded, 11 million
people are affected annually; 350,000 die, and at least
30% of survivors experience sequelae. Death often fol-
lows neurological damage, especially in regions where
rehabilitation facilities are virtually nonexistent [4, 5].
Globally, Hib, S. pneumoniae, and Neisseria meningitidis
cause 90% of nonneonatal, nontuberculous cases of
bacterial meningitis.
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
2/10
1278 CID 2007:45 (15 November) Peltola et al.
Except in cases of drug-resistant infection, the use of anti-
microbials that are newer than third-generation cephalosporins
has not improved outcomes [6]. As has been documented by
biochemical parameters, dexamethasone dampens the inflam-
matory response [710], but no study of optimal antimicrobial
therapy for childhood meningitis has shown a significant re-
duction in deafness, neurological sequelae, or mortality when
these outcomes were examined separately. In Malawi, the firsttrial that was large enough to allow an examination of the
individual outcomes failed to find any benefit [11]. Unfortu-
nately, cephalosporins could not be used routinely in that piv-
otal study. Revised Cochrane analysis [12] supports the use of
corticosteroids in high-income countries; however, as in meta-
analysis in general, very dissimilar populations were directly
compared, and the presenting status of the children was not
taken into account.
Glycerol (glycerine, 1, 2, 3-propanetriol), which is a naturally
occurring trivalent alcohol, an essential compound of the hu-
man cell membrane, a hyperosmolar agent, and an osmotic
diuretic, was long used in neurosurgery, neurology, and oph-thalmology to reduce raised tissue pressure [1317]. Glycerol
was given experimentally to treat bacterial meningitis in a few
children in the United States in the 1970s [18], but the first
systematic trial was performed in Finland during the period
19871991 [19]. Glycerol appeared to reduce profound hearing
loss and persistent neurological abnormalities as efficaciously
as dexamethasone, but the series was too small for definitive
conclusions. To validate that finding, we launched a much larger
study in Latin America, in which the potentials of glycerol and
dexamethasone were examined in terms of different outcomes,
and the results were compared with those of a placebo group.
PATIENTS AND METHODS
Setting and patients. This prospective multicenter, random-
ized, double-blind clinical trial examined the potential of in-
travenous dexamethasone, oral glycerol, or their combination
as adjuvant medications to improve different outcomes of
childhood bacterial meningitis. The series comprised children
with bacterial meningitis who were aged 2 months through 16
years at 10 institutions in Argentina, Brazil, Dominican Re-
public, Ecuador, Paraguay, and Venezuela, during the period
19962003 (Santo Domingo and Manaus joined the trial in
2001).
Meningitis was defined by (1) CSF culture positive for a
bacterial agent known to cause meningitis, (2) characteristic
CSF findings and positive blood culture results, (3) character-
istic CSF findings and a CSF sample with a positive latex ag-
glutination test result, and (4) symptoms and signs that were
compatible with bacterial meningitis and at least 3 of the fol-
lowing criteria: CSF pleocytosis (WBC count, 1000 cells/
mm3), decreased CSF glucose level (!40 mg/dL), increased CSF
protein concentration (40 mg/dL), increased serum C-reac-
tive protein level (40 mg/L) [20, 21], or occasionally, when
data regarding C-reactive protein level was not available, blood
leukocyte count 115,000 cells/mm3. Bacteriological analysis was
performed at each institutes laboratory and was standardized
by training where necessary.
The exclusion criteria were a history of recent head injury,previous neurosurgical precedure (e.g., intracranial shunt place-
ment), previous neurological disease (e.g., cerebral palsy and
Down syndrome), immunosuppression, and known hearing
impairment. Pretreatment antimicrobial therapy was registered
in detail but did not prevent study enrollment if oral therapy
or 1 parenteral dose had been administered.
Study drugs. All children received intravenous ceftriaxone
at a dosage of 80100 mg per kg of body weight once daily for
710 days. Ceftriaxone was bought locally, although for the
centers in Guayaquil, Ecuador, and Asuncion, Paraguay, cef-
triaxone was purchased from Chile. Antipyretics were given as
needed, and convulsions were treated according to local prac-
tice. No fluid restriction was used [22, 23], but in patients with
hypovolemia, deficits were restored before changing to main-
tenance fluids with isotonic crystalloids.
The patients were randomized to 1 of the following adjuvant
medication groups: intravenous dexamethasone and oral pla-
cebo, intravenous dexamethasone and oral glycerol, oral glyc-
erol and intravenous placebo, or intravenous placebo and oral
placebo. The dosing of dexamethasone was 0.15 mg/kg ad-
ministered every 6 h for 48 h [24], the first dose being ad-
ministered 15 min prior to administration of ceftriaxone (if
possible).Oral 85% glycerol (1 mL of which contained 1 g of glycerol)
was given for 48 h at a dosage of 1.5 g (1.5 mL) per kg every
6 h; the maximum volume was 25 mL per dose. The first dose
was given 15 min prior to ceftriaxone administration. At most
study centers, a nasogastric tube was inserted routinely. If the
child vomited within 30 min, the dose was repeated
immediately.
Randomization and blinding. Stratified block randomi-
zation took place in blocks of 20, except at 2 hospitals in Buenos
Aires, Argentina, in which the placebo-placebo group was not
allowed; at these hospitals, the block size was 24. All treatment
kits were packaged according to the randomization lists in San-tiago, Chile. Saline and carboxymethylcellulose were the pla-
cebo preparations for dexamethasone and glycerol, respectively.
The agents were provided in identical ampoules or bottles and
were labeled only with a study code. Because all patients had
an intravenous line and received a test agent orally, the blinding
was complete. Each treatment kit, marked only with the study
number, contained the medication or placebo and a sealed
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
3/10
Glycerol vs. Dexamethasone in Meningitis CID 2007:45 (15 November) 1279
Table 1. Patient characteristics at presentation to the hospital.
Variables
DXM and
placebo group
(n p 166)
DXM and
glycerol group
(n p 159)
Glycerol and
placebo group
(n p 166)
Placebo and
placebo group
(n p 163)
Age, median months (range) 13.0 (2178) 12.0 (2184) 10.0 (2152) 10.0 (2168)
Male sex 93 (56) 94 (59) 92 (55) 98 (60)
First symptoms 2447 h before presentationa
42/146 (29) 34/145 (23) 41/144 (28) 47/144 (33)
First symptoms 48 h before presentation 19/146 (13) 20/145 (14) 18/144 (13) 19/144 (13)
Convulsions prior to or at hospital admission 55/154 (36) 52/150 (35) 50/153 (33) 54/153 (36)
Prior use of antimicrobialsb
49/154 (32) 52/144 (36) 52/147 (35) 61/144 (42)
Causative agent (no. of patients)
Haemophilus influenzae type b (221) 54 54 53 60
Streptococcus pneumoniae (132) 35 31 30 36
Meningococcus (110) 26 25 33 26
Other (21) 9 2 6 4
Unknown (170) 42 47 44 37
Glasgow Coma Scale
Mean score SD 12.2 2.8 12.4 2.8 12.5 2.5 12.1 3.0
Score !13 66/155 (43) 60/149 (40) 61/155 (39) 65/153 (42)
CSF test results
Leucocyte count, median cells/mm3 (IQR value) 2000 (6040) 1800 (7506) 1890 (3892) 1822 (6220)
Glucose level, median mg/dL (IQR value) 19 (33) 16 (43) 16 (32) 13 (28)
Protein level, median g/dL (IQR value) 151 (140) 144 (168) 155 (162) 171 (182)
Serological test results
Leucocyte count, median 103 cells/mm3 (IQR value) 15.0 (10.7) 15.6 (11.7) 14.9 (10.4) 15.1 (12.5)
Glucose level, median g/dL (IQR value) 106 (58) 105 (48) 100 (49) 106 (52)
Hemoglobin level, median g/dL (IQR value) 9.4 (3.2) 9.3 (3.0) 9.1 (3.0) 9.0 (2.6)
Sodium level, median mmoL/L (IQR value) 137 (7) 137 (6) 137 (7) 137 (8)
NOTE. Data are no. (%) of patients, unless otherwise indicated. Data is given for the intention-to-treat population. DXM, dexamethasone; IQR, interquartile
range.a
Irritability, vomiting, absent look, neck rigidity, or convulsions observed by mother.b
During present illness, before bacterial meningitis was diagnosed.
envelope. The envelope disclosed the medication and was to
be opened in an emergency (no envelopes were opened during
the course of the study). Persons treating the patients, the study
monitor (I.R.), and the scientific advisor (H.P.) were not aware
of the specific treatments until the code was broken. This was
done after the study was completed.
Sample size. The sample size was calculated assuming that
a given adjuvant medication would decrease the rate of sequelae
from 20% to 5%. Accepting a 5% error in a 2-tailed test and
a power of 80%, at least 88 patients in each arm were required.
To be able to adjust for possible confounding factors, the sample
size was doubled. However, enrollment was to be stopped on
31 December 2003, whatever the number of patients.
Follow-up. All findings at presentation were recorded on
specially designed forms by the physician in charge. Records
included exact information on the nature and route of all an-
timicrobials and of the test agents, the age-adjusted Glasgow
Coma Scale [25], and the Denver Developmental Score [26].
A child was assessed for neurological, developmental, and hear-
ing sequelae on hospital discharge. If any deficits were found,
he or she was scheduled for a follow-up visit 12 months later.
After 200 patients had been enrolled and again after 400
patients had been enrolled, an ethicist and a statistician who
were not involved in the study reviewed the data to ensure that
there was no statistical difference between groups with respect
to case-fatality rate. The study protocol was approved by all
local ethical committees. Because not all mothers were literate,
an oral consent was accepted, after full information had been
given. The study was designed, conducted, and analyzed in-
dependently of any funding source.
End points and statistical analysis. The 3 primary end
points were death, severe neurological sequelae, and profound
hearing loss (inability to detect sounds with the better ear at
80 dB, determined with brain stem evoked response audiometry
or traditional audiometry). Severe neurological sequelae were
defined as blindness, quadriparesis or quadriplegia, hydro-
cephalus requiring a shunt, or severe psychomotor retardation
(in which the patient does not sit or walk, does not speak or
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
4/10
1280 CID 2007:45 (15 November) Peltola et al.
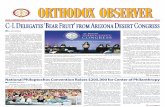
Figure 1. Study profile. DXM, dexamethasone; GLY, glycerol.
establish contact, or requires institutionalization). Because se-vere neurological sequelae and death may form a continuum
[4, 5], these 2 outcomes formed a composite end point. Because
it was unlikely that all patients would report for follow-up,
assessments were performed primarily at hospital discharge.
Dexamethasone has been reported to be especially beneficial
in treating Hib meningitis [810]. Therefore, we planned a
subgroup analysis for Hib versus non-Hib meningitis, taking
into account the receipt or nonreceipt of pretreatment anti-
microbial drugs. The 2 centers in Buenos Aires that did not
include the placebo-only arm were included in the analysis,
provided that their results did not change the results of the 4-
arm study.The x2 test was used to test the heterogeneity of proportions
between groups. To compare the main outcome measures, a
multivariable binary logistic model with and without covariates
was used. The treatment effects were taken into account by
applying a reference coding system using the (0.1)-indicator
variables, with the placebo recipients serving as the reference
group. All analyses were performed on an intention-to-treat
basis and were checked by per-protocol analysis.
Receipt of potential pretreatment antimicrobial drugs and
the timing of their administration with respect to the initiation
of adjuvant therapy were included as covariates in the post hoc
analysis for Hib meningitis versus other meningitides. We also
checked whether the findings remained the same when the
etiologically unconfirmed cases were excluded from analysis.
Finally, the entire series was divided into dexamethasone or
glycerol recipients and nonrecipients; this rough division was
intended to identify differences that were so small that they
would remain undetected in direct comparisons with the pla-
cebo-placebo group.
The results are expressed as ORs, 95% CIs, and Pvalues. An
OR!1.0 indicated a beneficial effect, and it was also consideredto be statistically significant if the upper value of the 95% CI
was !1.0. P values of !.05 were considered to be statistically
significant.
RESULTS
General. As shown by the patient characteristics at hospital
admission (table 1), there was no significant difference between
the 4 groups, and there was no major differences in enrollment
of patients or outcomes during the study period. Of the 763
patients who were assessed for eligibility, 109 did not fulfill the
criteria of bacterial meningitis. Thus, 654 children (figure 1)had data analyzed; of these, 166 received dexamethasone and
placebo, 159 received dexamethasone and glycerol, 166 received
glycerol and placebo, and 163 received placebo-placebo adju-
vant treatment. Per-protocol analysis, which did not change
the results, used data from 640 children; the reasons for ex-
cluding data from 14 children from this analysis are given in
figure 1. Eighty-six patients (13%) died. Of the remaining 568
children, 556 (98%) underwent a full neurological evaluation,
whereas 534 (94%) were tested for deafness (bilateral hearing
threshold, 80 dB).
In all, 37% of patients had received prior antimicrobial
treatment. Because inclusion of the 86 children from BuenosAires did not change the results, our data represent all 654
patients. Their characteristics during the hospital stay are
shown in table 2.
The causative agent was identified for 484 patients (74%).
Hib was the most common pathogen (found in 221 patients),
followed by S. pneumoniae (132 patients) and N. meningitidis
(110 patients); 21 patients had cases that were caused by other
bacteria (mostly Escherichia coli or Salmonella enteritidis). For
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
5/10
Glycerol vs. Dexamethasone in Meningitis CID 2007:45 (15 November) 1281
Table 2. Patient characteristics during hospital stay for the intention-to-treat population.
Variables
DXM and
placebo group
(n p 166)
DXM and
glycerol group
(n p 159)
Glycerol and
placebo group
(n p 166)
Placebo and
placebo group
(n p 163)
Duration of fever, mean days 1.9 2.4 2.6 2.4
Secondary fevera
65/143 (45) 65/140 (46) 69/143 (48) 66/144 (46)
Convulsions 48/155 (31) 43/148 (29) 42/148 (28) 50/150 (33)
Duration of Glasgow Coma Scale !15, mean days 3.2 3.3 3.3 3.5
Duration of neck stiffness, mean days 3.1 3.1 2.8 3.4
Duration of irritability, mean days 2.0 2.5 2.3 2.3
Duration of poor feeding, mean days 2.4 2.2 2.3 2.8
Vomiting 43/156 (28) 40/149 (27) 51/148 (34) 36/148 (24)
Diarrhea 25/156 (16) 16/144 (11) 29/141 (21) 17/145 (12)
Visible blood in stool 6/111 (5) 6/103 (6) 1/115 (1) 2/99 (2)
Mortality, by etiological agent (no. of patients who died)
Haemophilus influenzae type b (32) 7/54 (13) 8/54 (15) 7/53 (13) 10/60 (17)
Streptococcus pneumoniae (30) 8/35 (23) 6/31 (19) 6/30 (20) 10/36 (28)
Neisseria meningitidis (1) 0/26 (0) 0/25 (0) 0/33 (0) 1/26 (4)
Other (9) 5/9 (56) 1/2 (50) 2/6 (33) 1/4 (25)
Unknown (14) 3/42 (7) 5/47 (11) 2/44 (5) 4/37 (11)
Severe neurological sequelae, by etiological agent
(no. of patients with severe neurological sequelae)b
H. influenzae type b (13) 4/45 (9) 0/43 (0) 1/46 (2) 8/49 (16)
S. pneumoniae (13) 3/27 (11) 3/25 (12) 3/23 (13) 4/26 (15)
N. meningitidis (1) 0/25 (0) 0/24 (0) 0/33 (0) 1/25 (4)
Other (2) 0/4 (0) 1/1 (100) 1/4 (25) 0/3 (0)
Unknown (17) 3/38 (8) 4/41 (10) 2/41 (5) 8/34 (24)
Profound hearing loss, by etiological agent
(no. of patients with profound hearing loss)c
H. influenzae type b (21) 3/46 (7) 2/45 (4) 8/43 (19) 8/47 (17)
S. pneumoniae (9) 2/26 (7) 2/24 (8) 3/23 (13) 2/25 (8)
N. meningitidis (3) 2/24 (8) 1/23 (4) 0/30 (0) 0/24 (0)
Other (1) 0/3 (0) 1/1 (100) 0/3 (0) 0/3 (0)
Unknown (9) 3/36 (8) 3/39 (8) 1/37 (3) 2/32 (5)
NOTE. Data are no. (%) of patients, unless otherwise indicated. DXM, dexamethasone.a
Any fever after defeverscence of at least 24-h duration.bBlindness, quadriparesis or quadriplegia, hydrocephalus requiring a shunt, or severe psychmotor retardation.
cHearing threshold 80 dB in both ears. Audiological testing will be discussed in extenso in a separate article.
170 patients, 80 (47%) of whom had received pretreatment
antimicrobials, no causative agent was identified. In total, 174
patients were enrolled in Argentina, 143 in Ecuador, 122 in
Venezuela, 120 in the Dominican Republic, 80 in Paraguay, and
15 in Brazil.
Death, severe neurological sequelae, and hearing loss.
Table 3 shows the number of deaths (86 [13%] of 654), severe
neurological sequelae (44 [8%] of 556), deaths and severe neu-
rological sequelae combined (130 [20%] of 642), and profound
hearing loss (43 [8%] of 534) in the 4 groups. Poor outcomes
were most common in the placebo-placebo group, but statis-
tical significance was reached only with respect to severe neu-
rological sequelae and the category of severe neurological dam-
age or death. Profound hearing loss occurred with similar
frequency in all 4 groups (detailed audiological analysis will be
presented separately). For any end point, no significant inter-
action was observed between glycerol and dexamethasone.
The results with respect to outcome in the 3 adjuvant groups
tested against the placebo group are shown in table 4; this table
also gives data for children with information regarding the
timing of ceftriaxone therapy compared with that of adjuvant
therapy and data regarding etiologically confirmed cases. The
incidence of severe neurological sequelae was significantly re-
duced among patients who received glycerol alone (OR, 0.31
[95% CI, 0.130.76]; ) and patients who received thePp .01
dexamethasone-glycerol combination (OR, 0.39 [95% CI, 0.17
0.93]; ), whereas among those who received dexa-Pp .033
methasone alone, no more than a tendency towards a reduction
in severe neurological sequelae was observed. On the other
hand, a tendency towards lowered mortality rate was observed
in the group that received only glycerol. Receipt or nonreceipt
of pretreatment antimicrobials and the timing of their admin-
istration with respect to the initiation of an adjuvant medication
left the results essentially unchanged.
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
6/10
1282 CID 2007:45 (15 November) Peltola et al.
Table 3. Death, severe neurological sequelae, the composite end point of death or severe neurological sequelae, and profoundhearing loss, by treatment group.
Outcome
No. of
patients
evaluated
DXM and
placebo group
(n p 166)
DXM and
glycerol group
(n p 159)
Glycerol and
placebo group
(n p 166)
Placebo and
placebo group
(n p 163) Pa
Death
All patients 654 23/166 (14) 20/159 (13) 17/166 (10) 26/163 (16) .383
Patients with confirmed etiology 484 20/123 (16) 14/112 (13) 15/122 (12) 23/127 (18) .498
Severe neurological sequelaeb
All patients 556 10/139 (7) 8/134 (6) 7/147 (5) 19/136 (14) .022
Patients with confirmed etiology 403 7/100 (7) 4/94 (4) 5/106 (5) 13/103 (13) .081
Severe neurological sequelae or death
All patients 642 33/162 (20) 27/153 (18) 24/164 (15) 46/163 (28) .016
Patients with confirmed etiology 475 27/120 (23) 18/108 (17) 20/121 (17) 36/126 (29) .068
Profound hearing lossc
All patients 534 10/135 (7) 9/132 (7) 12/136 (9) 12/131 (9) .879
Patients with confirmed etiology 390 7/98 (7) 6/94 (6) 11/99 (11) 10/99 (10) .593
NOTE. Data are no. (%) of patients, unless otherwise indicated. DXM, dexamethasone.a
Determined by x2 test between 4 groups (for heterogeneity).b
Severe neurological sequelae included blindness (7 patients), quadriplegia (8), hydrocephalus requiring a shunt (4), or severe psychomotor retardation (26),
with each child counted only once.c
Hearing threshold of 80 dB for the better ear.
For the composite end point group (those who experienced
severe neurological sequelae or death), the results were similar.
The OR for the glycerol-only group was 0.44 (95% CI, 0.25
0.76; ), and for the dexamethasone-glycerol group, thePp .003
OR was 0.55 (95% CI, 0.320.93; ). Including thePp .027
timing of antimicrobial administration in the analysis or ex-
cluding the patients for whom an etiological agent was not
identified did not change the observation that the glycerol-only
group had the best outcomes, followed by the dexamethasone-
glycerol group; the group that received dexamethasone alone
had the worst outcomes.Hib versus non-Hib meningitis. Effects of the adjuvant
therapies on Hib versus non-Hib meningitis are presented in
table 5. All statistically significant differences were found in the
glycerol-only group. The incidence of severe neurological se-
quelae was reduced in patients with Hib meningitis, regardless
of whether all cases were examined (OR, 0.11 [95% CI, 0.01
0.95]; ) or only those cases with information on pre-Pp .045
treatment antimicrobials and the timing of adjuvant therapy
(OR 0.11 [95% CI, 0.010.96]; ).Pp .046
Examining severe neurological sequelae and death together,
the effect of treatment with glycerol remained statistically sig-
nificant among patients with Hib meningitis with information
on prior receipt of antimicrobials and the timing of adjuvant
therapy (OR, 0.33 [95% CI, 0.120.92]; ) and amongPp .035
children with non-Hib meningitis (OR, 0.46 [95% CI, 0.23
0.91]; ). Among children with non-Hib meningitis,Pp .025
even the mortality rate was somewhat reduced by receipt of
glycerol (OR, 0.49 [95% CI, 0.211.13]; ).Pp .094
When the data were analyzed taking into consideration only
whether glycerol or dexamethasone was or was not given, the
only new finding was with respect to Hib meningitis. Analyzing
all 181 cases together and neglecting the timing between dex-
amethasone and ceftriaxone administration, treatment with
dexamethasone prevented profound hearing loss (OR, 0.27
[95% CI, 0.090.77]; ). Statistical significance was lostPp .014
if data from patients with cases of Hib meningitis who had not
received pretreatment antimicrobials (123 patients) were ex-
amined separately.
Safety. Few adverse effects attributable to either adjuvant
medication were observed. Visible blood in the stool was noted
in 6 (5%) of 111 patients in the dexamethasone group and in5 (5%) of 101 patients in the dexamethasone-glycerol group
but in only 1 (1%) of 113 patients in the glycerol-only group
and 2 (2%) of 99 patients in the placebo group (table 2). The
difference between the dexamethasone recipients and thosewho
did not receive dexamethasone was statistically significant
( ). Vomiting or diarrhea were not more common inPp .032
the glycerol group, and massive gastrointestinal hemorrhage or
other severe adverse events were not found in any child.
DISCUSSION
This prospective, double-blind, randomized trial from 6 LatinAmerican countries that involved 654 patients is, to our knowl-
edge, the largest clinical study of childhood bacterial meningitis
to date. Oral glycerol improved outcomes especially by reducing
severe neurological sequelae. The study was performed in con-
ditions similar to those in which the great majority of children
with meningitis worldwide are treated [3, 4, 2729]. Many of
the children in our study presented late in the course of disease,
many were anemic, and many had previously been given oral
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
7/10
Glycerol vs. Dexamethasone in Meningitis CID 2007:45 (15 November) 1283
Table 4. Risk of death, severe neurological sequelae, the composite end point of death or severe neurological sequelae, and profoundhearing loss in the 3 adjuvant therapy groups, compared with the placebo only group.
Outcome
No. of
patients
evaluated
DXM and
placebo group
(n p 166)
DXM and
glycerol group
(n p 159)
Glycerol and
placebo group
(n p 166)
OR (95% CI) P OR (95% CI) P OR (95% CI) P
Death
Overall 654 0.82 (0.451.49) .509 0.69 (0.371.31) .257 0.58 (0.301.11) .099Including receipt of prior antimicrobial and timing of DXM
administrationa
All cases 578 0.92 (0.481.76) .796 0.79 (0.401.56) .502 0.60 (0.291.22) .155
Cases with confirmed etiology 430 0.94 (0.461.90) .853 0.75 (0.351.62) .466 0.63 (0.291.37) .239
Severe neurological sequelaeb
Overall 556 0.48 (0.211.07) .072 0.39 (0.170.93) .033 0.31 (0.130.76) .010
Including receipt of prior antimicrobial and timing of DXM
administrationa
All cases 497 0.50 (0.211.19) .119 0.46 (0.191.11) .084 0.37 (0.140.93) .034
Cases with confirmed etiology 363 0.52 (0.191.39) .192 0.32 (0.101.03) .057 0.36 (0.121.07) .065
Combined outcome of severe neurological sequelae or death
Overall 642 0.65 (0.391.09) .100 0.55 (0.320.93) .027 0.44 (0.250.76) .003
Including receipt of prior antimicrobial and timing of DXM
administrationa
All cases 572 0.72 (0.421.25) .241 0.63 (0.361.11) .108 0.47 (0.260.85) .013
Cases with confirmed etiology 425 0.75 (0.411.38) .357 0.56 (0.281.09) .088 0.49 (0.250.96) .037
Profound hearing loss
Overall 534 0.79 (0.331.91) .604 0.73 (0.301.79) .485 0.96 (0.422.22) .923
Including receipt of prior antimicrobial and timing of DXM
administrationa
All cases 476 0.70 (0.271.81) .455 0.78 (0.311.98) .603 1.04 (0.442.47) .932
Cases with confirmed etiology 351 0.56 (0.191.61) .279 0.62 (0.211.80) .378 1.11 (0.442.78) .825
NOTE. P values were determined by Walds test. DXM, dexamethasone.a
Receipt versus nonreceipt of prior antimicrobial treatment and timing of adjuvant medication administration versus initiation of ceftriaxone therapy (before
vs. at the same time or later) included as covariates.b
Severe neurological sequelae included blindness (7 patients), quadriplegia (8), hydrocephalus requiring a shunt (4), or severe psychomotor retardation (26),
with each child counted only once.
antimicrobials. A few of these children may have been infected
with HIV, although the prevalence of HIV infection in Latin
America was low during the study period [30].
Because most children could not be expected to return for
a control visit, we were forced to use the outcome data that
were available at hospital discharge. Some subtle sequelae may,
therefore, have remained undetected, but this shortcoming
probably did not distort the results, because most of the se-
quelae described in our study were very unlikely to resolve with
time. Children with these sequelae probably died or remained
permanently disabled. Other limitations of the study were the
inclusion of patients who had received pretreatment antimi-
crobial drugs (which are administered indiscriminately in Latin
America) and patients with etiologically unidentified cases;
however, the study design distributed such patients evenly to
each arm. Because the details of antimicrobial administration
were recorded meticulously, we could also examine children
who did not receive a single dose of any antimicrobial before
hospitalization.
The comprehensiveness of the series allowed us to analyze
the adjuvant effects separately for each outcome. Except for 2
earlier studies that were sufficiently poweredone from Africa,
involving children [11], and the other from Europe, involving
adults who received dexamethasone for 4 days [31]this has
not been possible before. By keeping the outcomes separated,
potential benefits between adjuvants could be examined spe-
cifically. Glycerol not only reduced severe neurological sequelae
but was also beneficial when severe neurological sequelae and
mortality were examined together [4, 5]. Nevertheless, preven-
tion of severe neurological sequelae alone was a major achieve-
ment; many clinicians classify survival with severe sequelae and
death as poor outcomes of equal importance [4]. Reducing the
impact of meningitis on the family and on society clearly re-
quires more than merely increasing the survival rate [32].
How does glycerol work? One-third of the children with
bacterial meningitis experience significantly impaired cerebral
blood flow [33, 34] and intracranial edema. Oral glycerol in-
creases plasma osmolality, which, among other effects, lowers
intraocular pressure within 30 min [17]. Oral glycerol also in-
creases plasma osmolality in children with bacterial meningitis
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
8/10
1284 CID 2007:45 (15 November) Peltola et al.
Table 5. Risk of death, severe neurological sequelae, the composite end point of death or severe neurological sequelae, and profoundhearing loss among the 3 adjuvant therapy groups, compared with the placebo group, in patients with Haemophilus influenzae typeb (Hib) meningitis and patients with non-Hib meningitis.
Outcome
No. of
patients
evaluated
DXM and
placebo group
(n p 166)
DXM and
glycerol group
(n p 159)
Glycerol and
placebo group
(n p 166)
OR (95% CI) P OR (95% CI) P OR (95% CI) P
DeathHib meningitis
Overall 221 0.75 (0.262.12) .508 0.87 (0.322.39) .787 0.76 (0.272.17) .608
Including prior antimicrobial and DXM
administration timinga
204 0.82 (0.282.42) .724 0.79 (0.272.30) .669 0.62 (0.192.00) .422
Optimal DXM therapyb
114 1.71 (0.397.60) .478 0.73 (0.114.77) .740 0.92 (0.175.02) .926
Non-Hib meningitis, overall 433 0.84 (0.401.77) .652 0.65 (0.301.45) .293 0.49 (0.211.13) .094
Severe neurological sequelaec
Hib meningitis
Overall 183 0.50 (0.141.79) .287 NE 0.11 (0.010.95) .045
Including prior antimicrobial and DXM
administration timinga
172 0.46 (0.131.68) .240 NE 0.11 (0.010.96) .046
Optimal DXM therapyb
100 0.29 (0.051.67) .167 NE 0.15 (0.021.41) .098
Non-Hib meningitis, overall 374 0.43 (0.161.21) .109 0.61 (0.241.57) .307 0.40 (0.141.12) .080
Severe neurological sequelaec
or death
Hib meningitis
Overall 215 0.61 (0.261.45) .265 0.42 (0.171.08) .072 0.41 (0.161.03) .058
Including prior antimicrobial and DXM
administration timinga
201 0.64 (0.261.58) .319 0.39 (0.151.06) .064 0.33 (0.120.92) .035
Optimal DXM therapyb
114 0.73 (0.232.30) .591 0.21 (0.041.09) .063 0.40 (0.101.52) .176
Non-Hib meningitis, overall 427 0.68 (0.361.28) .233 0.62 (0.321.20) .158 0.46 (0.230.91) .025
Profound hearing loss
Hib meningitis
Overall 181 0.34 (0.081.37) .130 0.23 (0.051.13) .071 1.11 (0.383.29) .845
Including prior antimicrobial and DXM
administration timinga
168 0.37 (0.091.52) .167 0.26 (0.051.33) .106 1.15 (0.383.47) .800
Optimal DXM therapyb
97 0.19 (0.021.86) .154 0.23 (0.022.21) .202 0.48 (0.082.89) .420
Non-Hib meningitis, overall 353 1.71 (0.486.06) .408 1.75 (0.496.21) .387 0.90 (0.223.71) .883
NOTE.Intention-to-treat subgroup analysis. For outcomes, see table 3. P values were determined by Walds test. DXM, dexamethasone; NE, not estimable.a
Receipt versus nonreceipt of prior antimicrobial treatment and timing of adjuvant medication administration versus initiation of ceftriaxone therapy (before
vs. at the same time or later) included as covariates.b
Patients with no prior antimicrobial treatment and ceftriaxone administered 15 min after dexamethasone.c
Severe neurological sequelae included blindness (7 patients), quadriplegia (8), hydrocephalus requiring a shunt (4), or severe psychomotor retardation (26),
with each child counted only once.
(S. Singhi, personal communication), as it does in adult healthy
volunteers [35]. This change in osmolality reduces edema and
enhances cerebral circulation by reducing the excretion of CSF
[36]. As water moves by osmosis back into the plasma, extra-
vascularization of water and subsequent occult hypovolemia
are reduced. Decrease of the intracranial pressure by glycerol-
induced osmotic diuresis seems to be less important [37], be-
cause a gradient between the body compartments requires an
intact or almost intact blood-brain barrier, and this is not the
case in patients with bacterial meningitis. Glycerol is also a
scavenger of free oxygen radicals, and this action may further
alleviate meningeal inflammation.
Our glycerol dosage (6 g per kg of body weight per day
divided into 4 doses) was not evidence-based but was derived
from dosages recommended earlier [38] in neurology and neu-
rosurgery. Our practice of keeping to a single maximum dose
of 25 mL was based on our previous experience [19], which
showed that some children vomited if they received a larger
total dose. In our study, vomiting was not more common
among glycerol recipients. No data suggest the substitution of
another osmotic diuretic, such as mannitol, for glycerol; in fact,
intravenous mannitol may be harmful in patients with bacterial
meningitis [39].
Further studies on adjuvant glycerol to treat bacterial men-
ingitis are clearly warranted. Interestingly, although the Malawi
trial [11] found no advantage associated with dexamethasone
treatment, some of our patients benefited. This was best shown
among patients with Hib meningitis when the dexamethasone
recipients were compared with the non-recipients and the tim-
ing of antimicrobial administration was not taken into account.
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
9/10
Glycerol vs. Dexamethasone in Meningitis CID 2007:45 (15 November) 1285
Unfortunately, we cannot easily identify patients who likely
would benefit from adjuvant dexamethasone. Evidently, they
are not simply those patients with nonpretreated Hib meningitis
for whom cephalosporin therapy was initiated after giving
dexamethasone.
In conclusion, oral glycerol reduced the incidence of severe
neurological sequelae associated with childhood bacterial men-
ingitis. Five properties of glycerol make its widespread use pos-sible and desirable: it can be taken orally, is inexpensive, is
easily available, has no special storage requirements, and is safe
[18, 19, 37, 40]. Glycerol is a common ingredient of ingested
(e.g., chewing gum) and topical (e.g., shampoo) substances.
Some patients have received intravenous glycerol for 1 week
[14]; we gave 8 oral doses over a 48-h period.
Glycerol is a novel tool for the treatment of bacterial men-
ingitis, which is a life-threatening disease that 5000 children
per day contract worldwide. Oral glycerol is also an agent that
is cheap enough and simple enough for treatment of the poorest
patients. Since the advent of chloramphenicol and ampicillin
40 years ago, no other medication has improved the prognosisof childhood meningitis, especially Hib meningitis, as much as
glycerol.
STUDY CONTRIBUTORS
Jesus Feris-Iglesias and Chabela Pena (Santo Domingo, Do-
minican Republic); Mariella Chang and Ruth Flor (Guayaquil,
Ecuador); Mara Rosa Agosti (La Plata, Argentina); Miriam
Maitin and Lesbia Colina (Barquisimeto, Venezuela); Dolores
Lovera (Asuncion, Paraguay); Mara Teresa Rosanova, Ilse Vil-
laroel, and Mari Carmen Cifro (Buenos Aires, Argentina); Mag-
dalena Correa (Merida, Venezuela); and Marcos Fernandes andVania Prazeres (Manaus, Brazil).
Bacteriological and other laboratory investigations were di-
rected by Jacqueline Sanchez (Santo Domingo, Dominican Re-
public); Rafael Roas (Barquisimeto, Venezuela); Cecilia Vescina,
Marta Altschuler, and Patricie Lazarte (La Plata, Argentina);
Wilma Basualdo (Asuncion, Paraguay); Maria del Carmen Cei-
nos (Buenos Aires, Argentina); and Rossicleia Monte (Manaus,
Brazil).
Audiological examinations were performed by Clemente Ter-
rero (Santo Domingo, Dominican Republic); Beila Pire (Bar-
quisimeto, Venezuela); Pedro Toledo (Guayaquil, Ecuador);
Luis Pedersoli, Alicia Calcaterra, and Silvia Jury (La Plata, Ar-gentina); Arturo Campos (Asuncion, Paraguay); and Mara E.
Prieto (Buenos Aires, Argentina).
The formula for the placebo of glycerol was developed by
Pedro Valora (Buenos Aires, Argentina).
Acknowledgments
We thank Dr. Ralf Clemens, who organized the initial grant for this
nonprofit study, and Dr. Elizabeth Molyneux, who revised the text. Ossi
Hiltunen (Orion Diagnostica) kindly provided the equipment for quan-
titative C-reactive protein measurements.
Financial support. GlaxoSmithKline, Alfred Kordelin, Paivikki and
Sakari Sohlberg, and Sigfrid Juselius Funds. Farmacia Ahumada do nated
glycerol and both placebo preparations. Laboratoriode Chilepartly donated
ceftriaxone.
Potential conflicts of interest. H.P. is currently a scientific consultant
of Serum Institute of India. All other authors: no conflicts.
References
1. Peltola H. Worldwide Haemophilus influenzae type b disease at the
beginning of the 21st century; global analysis of the disease burden 25
years after the use of polysaccharide vaccine and a decade after the
advent of conjugates. Clin Microbiol Rev 2000; 13:30217.
2. Daoud AS, Al-Sheyyab M, Batchoun RG, et al. Bacterial meningitis:
still a cause of high mortality and severe neurological morbidity in
childhood. J Trop Med Paed 1995; 41:30810.
3. Goetghebuer T, West TE, Wermenbol V, et al. Outcome of meningitis
caused by Streptococcus pneumoniae and Haemophilus influenzae type
b in children in The Gambia. Trop Med Int Health 2000; 5:20713.
4. Duke T, Mokela D, Frank D, et al. Management of meningitis in
children with oral fluid restriction or intravenous fluid at maintenance
volumes: a randomized trial. Ann Trop Paediatr 2002; 22:14557.
5. Principi N, Esposito S. Dexamethasone in acute bacterial meningitis.
Lancet 2002; 360:1610.
6. Peltola H, Anttila M, Renkonen O-V; The Finnish Study Group. Ran-
domised comparison of chloramphenicol, ampicillin, cefotaxime, and
ceftriaxone for childhood bacterial meningitis. Lancet 1989; 1:12817.
7. Mustafa MM, Ramilo O, Mertsola J, et al. Modulation of inflammation
and cachectin activity in relation to treatment of experimental Hae-
mophilus influenzae type b meningitis. J Infect Dis 1989; 160:81825.
8. Lebel MH, Freij BJ, Syrogiannopoulos GA, et al. Dexamethasone ther-
apy for bacterial meningitis: results of two double-blind, placebo-con-
trolled trials. N Engl J Med 1988; 319:96471.
9. Odio CM, Faingezicht I, Paris M, et al. The beneficial effects of early
dexamethasone administration in infants and children with bacterial
meningitis. N Engl J Med 1991;324:152531.
10. Schaad UB, Lips U, Gnehm HE, Blumberg A, Wedgwood J. Dexa-
methasone therapy for bacterial meningitis in children. The Swiss Men-
ingitis Study Group. Lancet 1993; 342:45761.11. Molyneux EM, Walsh AL, Forsyth H, et al. Dexamethasone treatment
in childhood bacterial meningitis in Malawi: a randomised controlled
trial. Lancet 2002; 360:2118.
12. van de Beek D, de Gans J, McIntyre P, Prasad K. Corticosteroids in
acute bacterial meningitis. Cochrane Database Syst Rev 2007:
CD004405.
13. Buckell M, Walsh L. Effect of glycerol by mouth on raised intracranial
pressure in man. Lancet 1964; 2:11512.
14. Gilsanz V, Rebollar JL, Buencuerpo J, Chantres MT. Controlled trial
of glycerol versus dexamethasone in the treatment of cerebral oedema
in acute cerebral infarction. Lancet 1975; 1:104951.
15. Rottenberg DA, Hurwitz BJ, Posner JB. The effect of oral glycerol on
intraventricular pressure in man. Neurology 1977; 27:6008.
16. Bayer AJ, Pathy MSJ, Newcombe R. Double-blind randomised trial of
intravenous glycerol in acute stroke. Lancet 1987; 1:4058.17. McCurdy DK, Schneider B, Scheie HG. Oral glycerol: the mechanism
on intraocular hypotension. Am J Ophthalmol 1966; 61:12449.
18. Herson VC, Todd JK. Prediction of morbidity in Haemophilus influen-
zae meningitis. Pediatrics 1977; 59:359.
19. Kilpi T, Peltola H, Kallio MK, et al. Oral glycerol versus intravenous
dexamethasone in preventing hearing impairment due to childhood
bacterial meningitis. Pediatr Infect Dis J 1995; 14:2708.
20. Peltola HO. C-reactive protein in rapid monitoring of infections of
the central nervous system. Lancet 1982; 1:9802.
21. Roine I, Banfi A, Bosch P, Ledermann W, Contreras C, Peltola H.
Serum C-reactive protein in childhood meningitis in countries with
7/28/2019 Clin Infect Dis.-2007-Peltola-1277-86.pdf
10/10
1286 CID 2007:45 (15 November) Peltola et al.
limited laboratory resources: a Chilean experience. Pediatr Infect Dis
J 1991; 10:9238.
22. Tureen JM, Tauber MG, Sande MA. Effect of hydration status on
cerebral blood flow and cerebrospinal fluid lactic acidosis in rabbits
with experimental meningitis. J Clin Invest 1992; 89:94753.
23. Singhi SC, Singhi PD, Srinivas B, et al. Fluid restriction does not
improve the outcome of acute meningitis. Pediatr Infect Dis J 1995;
14:495503.
24. Syrogiannopoulos GA, Lourida AN, Theodoridou MC, et al. Dexa-
methasone therapy for bacterial meningitis in children: 2- versus 4-
day regimen. J Infect Dis 1994; 169:8538.
25. Teasdale G, Jennett B. Assessment of coma and impaired consciousness:
a practical scale. Lancet 1974; 2:814.
26. Glascoe FP, Byrne KE, Ashford LK, Johnson KL, Chang B, Strickland
B. Accuracy of the Denver-II in developmental screening. Pediatrics
1992; 89:12215.
27. Peltola H. Haemophilus influenzae type b disease and vaccination in
Latin America and the Caribbean. Pediatr Infect Dis J 1997; 16:7807.
28. Basualdo W, Arbo A. Invasive Haemophilus influenzaetype b infections
in children in Paraguay. Arch Med Res 2004; 35:12633.
29. Peltola H. Burden of meningitis and other severe bacterial infections
of children in Africa: implications for prevention. Clin Infect Dis
2001; 32:6475.
30. Salooje H, Violari A. HIV infection in children. BMJ 2001; 323:6704.
31. de Gans J, van de Beek D; European Dexamethasone in Adulthood
Bacterial Meningitis Study Investigators. Dexamethasone in adults withbacterial meningitis. N Engl J Med 2002; 347:154956.
32. Dexamethasone therapy for bacterial meningitis. New Engl J Med
1989; 320:4635.
33. Ashwal S, Stringer W, Tornasi L, Schneider S, Thompson J, Perkin R.
Cerebral blood flow and carbon dioxide reactivity in children with
bacterial meningitis. J Pediatr 1990; 117:52330.
34. Mller K, Larsen FS, Qvist J, et al. Dependency of cerebral blood flow
on mean arterial pressure in patients with acute meningitis. Crit Care
Med 2000; 28:102732.
35. Sommer S, Nau R, Wieland E, Prange HW. Pharmacokinetics of glyc-
erol administered orally in healthy volunteers. Arzneimittelforschung1993;43:7447.
36. Zoghbi HV, Okumura S, Laurent JP, Fishman MA. Acute effect of
glycerol on net cerebrospinal fluid production in dogs. J Neurosurg
1985; 63:75962.
37. Nau R, Prins F-J, Kolenda H, Prange HW. Temporary reversal of serum
to cerebrospinal fluid glycerol concentration gradient after intravenous
infusion of glycerol. Eur J Clin Pharmacol 1992; 42:1815.
38. Frank MSB, Nahata MC, Hilty MD. Glycerol: a review of its phar-
macology, phamacokinetics, adverse reactions, and clinical use. Phar-
macotherapy 1981; 1:14760.
39. Syrogiannopoulos GA, Olsen KD, McCracken GH. Mannitol treatment
in experimental Haemophilus influenzaetype b meningitis. Pediatr Res
1987; 22:11822.
40. Tourtelotte WW, Reinglass JL, Newkirk TA. Cerebral dehydration ac-
tion of glycerol. I. Historical aspects with emphasis on the toxicity andintravenous administration. Clin Pharmacol Ther 1972; 13:15971.