Chu Rg Strauss

of 2
-
Upload
chris-jara -
Category
Documents
-
view
220 -
download
0
Transcript of Chu Rg Strauss
-
8/11/2019 Chu Rg Strauss
1/2
498 MJA Volume 181 Number 9 1 November 2004
NOTABLE CASES
The Medical Journal of Australia ISSN: 0025-
729X 1 November 2004 181 9 498-499The Medical Journal of Australia 2004www.mja.com.auNotable Cases
hurgStrauss syndrome (CSS), or allergic granulomatosisand angiitis, is a granulomatous vasculitis affecting small-to medium-sized arteries and veins. Although CSS is a
systemic disease characterised by asthma and eosinophilia, variouslimited forms have been described.1Here, we report a patient withsuch a limited form of the disease.
Clinical record
A 35-year-old woman presented with a 15-day history of gangrene
of the fingertips of her left hand, and weakness of the right wristjoint and the left ankle joint. She had a 3-year history of recurrentparanasal sinusitis. There was no history of asthma or any otherallergic disorder, parasitic infestation, or smoking.
On presentation, the patient had a pulse rate of 78 beats/min,blood pressure of 150/90 mm/Hg, and a temperature of 38.8C.She had conjunctival pallor, gangrene involving all fingertips of theleft hand, palpable purpura on the anterior aspect of the left leg,and 3/5 grade motor weakness of the right wrist joint and left ankle
joint on dorsiflexion. The provisional diagnosis was systemicvasculitis syndrome. Blood tests on presentation showed (referenceranges in parentheses) a haemoglobin level of 93 g/L (110165g/L), a white blood cell count of 15 109 cells/L (411 109 cells/L),
an eosinophil count of 0.15
10
9
cells/L (00.4
10
9
cells/L), anderythrocyte sedimentation rate of 35 mm/h (< 15 mm/h). Levels ofurea, creatinine and electrolytes, fibrinogen level and prothrombintime, and the results of liver function tests, were within normalranges. Urinalysis showed 3+ proteinuria (3 g/L) and micro-scopic analysis showed 3040 red blood cells per high powerfield (reference range, < 4). The creatinine clearance rate was98 mL/min.
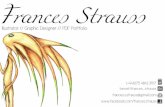
A chest x-ray demonstrated bilateral ground glass infiltrates,predominantly in the basal zones. High-resolution computed
tomography (CT) of the chest revealed bilateral patchy groundglass opacities (Box 1). Spirometry showed a forced vital capacity(FVC) of 65% predicted, a forced expiratory volume (FEV1) of68% predicted, and FEV1/FVC of 104%. An echocardiogram was
normal. A nerve conduction velocity study showed axonal involve-ment, with reduced nerve conduction velocity in the right radialand left superficial peroneal nerves. CT of the paranasal sinusesshowed chronic pansinusitis. Histopathological examination of the
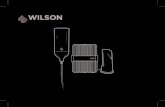
open-lung biopsy showed leukocytoclastic vasculitis, granulomaformation, and extravascular eosinophilic infiltration (Box 2).Renal biopsy showed pauci-immune, crescentic glomerulonephri-tis. Renal vessel Doppler ultrasonography and renal angiographygave normal results and ruled out any renal vessel involvement.The patient tested positive for perinuclear antineutrophilic cyto-plasmic antibodies (ANCAs) and negative for cytoplasmic ANCAsby the indirect immunofluorescence method. A more specific
enzyme-linked immunosorbent assay (ELISA) for anti-myeloper-oxidase was positive, and another, for anti-proteinase 3, wasnegative. These tests ruled out Wegners granulomatosis. Antinu-
A limited form of ChurgStrauss syndrome presentingwithout asthma and eosinophilia
Bhavneesh K Sharma, Mradul K Daga and Manisha Sharma
Respiratory Division, Department of Internal Medicine,Maulana Azad Medical College, University of Delhi, New Delhi, India.Bhavneesh K Sharma, MB BS, MD, Chief Resident;Mradul K Daga, MB BS, MD, Professor;Manisha Sharma, MB BS, DTCD, Research Associate.
Reprints will not be available from the authors. Correspondence:Dr Bhavneesh K Sharma, G-4/D, DDA Flats, Munirka,New Delhi-110067, India. [email protected]
C
We report a young woman presenting with digital gangrene, paranasal sinusitis, mononeuritis multiplex,
and rapidly progressive glomerulonephritis without asthma and eosinophilia an extremely rarevariant of this disease. (MJA 2004; 181: 498-499)
1 High-resolution computed tomography of the chest,
showing bilateral ground glass opacities
2 Open-lung biopsy specimen, showing leukocytoclasticvasculitis, granuloma formation, and extravasculareosinophilic infiltration
Magnification 100; haematoxylineosin stain.
-
8/11/2019 Chu Rg Strauss
2/2