Chronic Pain Management Guidelines Purpose
17
1 2 DRAFT: DO NOT CITE OR DISTRIBUTE 3 Send comments to [email protected] 4 5 Chronic Pain Management Guidelines 6 Purpose 7 The purpose of these guidelines is to support Certified Registered Nurse Anesthetists (CRNAs) 8 in the delivery of safe and effective chronic pain management and treatment. An 9 interdisciplinary team approach that uses a multidimensional pain strategy and integrates the 10 patient’s unique experiences and perspective may help achieve effective pain management and 11 treatment with the goal to improve the patient’s well-being, functionality, and quality of life. The 12 guidelines emphasize the importance of reduction in the risk of opioid overdose and need for 13 prescription opioids, which may lead to opioid use disorder. 14 The Chronic Pain Management Guidelines are intended to promote high-quality care and do not 15 assure specific outcomes. The Standards for Nurse Anesthesia Practice 1 are the foundation for 16 chronic pain management practice. The Scope of Nurse Anesthesia Practice 2 affirms that 17 chronic and interventional pain management services are within the CRNA scope of practice. 18 Background 19 Definition of Pain 20 The International Association for the Study of Pain (IASP) recently revised its definition of pain 21 to “an unpleasant sensory and emotional experience associated with, or resembling that 22 associated with, actual or potential tissue damage.” 3 The new definition includes six key notes 23 that provide further context for understanding pain as a multidimensional, complex experience: 3 24 • “Pain is always a personal experience that is influenced to varying degrees by biological, 25 psychological, and social factors.” 26 • “Pain and nociception are different phenomena. Pain cannot be inferred solely from 27 activity in sensory neurons.” 28 • “Through their life experiences, individuals learn the concept of pain.” 29 • “A person’s report of an experience as pain should be respected.” 30 • “Although pain usually serves an adaptive role, it may have adverse effects on function 31 and social and psychological well-being.” 32 • “Verbal description is only one of several behaviors to express pain; inability to 33 communicate does not negate the possibility that a human or a nonhuman animal 34 experiences pain.” 35 36 Types of Pain 37 Pain exists along a continuum. Acute pain typically occurs suddenly and has a specific cause, 38 such as tissue injury that lasts less than three months. 4,5 If left untreated, acute pain may lead 39 to chronic pain making the patient more sensitive to pain (hyperalgesia) and experience severe 40 pain even from nonpainful stimuli (allodynia). 6,7 41
Transcript of Chronic Pain Management Guidelines Purpose
1 2
DRAFT: DO NOT CITE OR DISTRIBUTE 3 Send comments to [email protected] 4
5 Chronic Pain Management Guidelines 6
Purpose 7
The purpose of these guidelines is to support Certified Registered Nurse Anesthetists (CRNAs) 8 in the delivery of safe and effective chronic pain management and treatment. An 9 interdisciplinary team approach that uses a multidimensional pain strategy and integrates the 10 patient’s unique experiences and perspective may help achieve effective pain management and 11 treatment with the goal to improve the patient’s well-being, functionality, and quality of life. The 12 guidelines emphasize the importance of reduction in the risk of opioid overdose and need for 13 prescription opioids, which may lead to opioid use disorder. 14
The Chronic Pain Management Guidelines are intended to promote high-quality care and do not 15 assure specific outcomes. The Standards for Nurse Anesthesia Practice1 are the foundation for 16 chronic pain management practice. The Scope of Nurse Anesthesia Practice2 affirms that 17 chronic and interventional pain management services are within the CRNA scope of practice. 18
Background 19
Definition of Pain 20
The International Association for the Study of Pain (IASP) recently revised its definition of pain 21 to “an unpleasant sensory and emotional experience associated with, or resembling that 22 associated with, actual or potential tissue damage.”3 The new definition includes six key notes 23 that provide further context for understanding pain as a multidimensional, complex experience:3 24
• “Pain is always a personal experience that is influenced to varying degrees by biological, 25 psychological, and social factors.” 26
• “Pain and nociception are different phenomena. Pain cannot be inferred solely from 27 activity in sensory neurons.” 28
• “Through their life experiences, individuals learn the concept of pain.” 29 • “A person’s report of an experience as pain should be respected.” 30 • “Although pain usually serves an adaptive role, it may have adverse effects on function 31
and social and psychological well-being.” 32 • “Verbal description is only one of several behaviors to express pain; inability to 33
communicate does not negate the possibility that a human or a nonhuman animal 34 experiences pain.” 35 36
Types of Pain 37
Pain exists along a continuum. Acute pain typically occurs suddenly and has a specific cause, 38 such as tissue injury that lasts less than three months. 4,5 If left untreated, acute pain may lead 39 to chronic pain making the patient more sensitive to pain (hyperalgesia) and experience severe 40 pain even from nonpainful stimuli (allodynia).6,7 41
DRAFT: DO NOT CITE OR DISTRIBUTE
2 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
Chronic non-cancer pain is defined as ongoing or recurrent pain that is moderate or severe, 42 lasting more than three months. It includes conditions such as low back pain, osteoarthritis, 43 rheumatoid arthritis, neuropathic pain, and fibromyalgia.4,5 44
Epidemiology 45
In 2016, chronic pain affected an estimated 20.4 percent of U.S. adults, approximately eight 46 percent of which had high-impact chronic pain that interfered with their ability to work outside 47 the home.8 48
Chronic pain represents a significant economic burden, costing between $560 billion to $635 49 billion annually in healthcare expenses and lost productivity.9 It remains the top reason people 50 seek healthcare.10 51
People with chronic pain are at high risk for opioid misuse and addiction. For example, a 52 systematic review of 38 studies reports opioid misuse rates of 21 to 29 percent and addiction 53 rates of eight to twelve percent in patients with chronic pain.11 54
Untreated chronic pain can negatively affect individuals, and contribute to limited function, 55 depression, anxiety, and reduced quality of life.8 For example, patients who are diagnosed with 56 both depression and chronic pain tend to experience worse outcomes compared to patients 57 diagnosed with chronic pain only. Patients with dual diagnosis should be closely monitored to 58 avoid progression to severe pain.12 59
Chronic pain can also contribute to suicide risk. In a recent study, Petrosky et al.13 examined 60 123,181 suicide deaths across 18 states between 2003 and 2014. They found that almost nine 61 percent of cases had evidence of chronic pain, with back pain, cancer, and arthritis being the 62 leading causes of suicide in this chronic pain subpopulation. Certain groups such as veterans 63 and individuals with fibromyalgia are at increased risk of suicide, especially if they have both 64 chronic pain and mental health diagnoses.14,15 65
Risk Factors 66
The experience of chronic pain is unique to each patient and involves complex biological (e.g., 67 age, gender), psychological (e.g., childhood trauma), and social (e.g., social and economic 68 disadvantages) factors.16 As people age, they are at high risk for developing chronic pain 69 conditions, such as osteoarthritis, diabetic neuropathy, and post-stroke pain.17,18 Women are 70 more likely than men to report chronic pain;18 they are also more likely to experience a higher 71 level of pain intensity and higher pain-related disability than men.19 72
Social and economic disadvantages correlate with chronic pain. Low socioeconomic status, 73 being a racial/ethnic minority, poverty, unemployment, geographic isolation, and inadequate 74 insurance coverage are associated with higher prevalence and intensity of chronic pain 75 compared to people without these characteristics.17,19 76
Other important predictors of chronic pain include the presence of another site of acute or 77 chronic pain within the body, obesity, sleep disorders, and past surgeries and medical 78 interventions.19,20 Lifestyle factors may also play a role in contributing to chronic pain and 79 include smoking and alcohol use, low levels of physical activity, living in colder climates, and low 80
DRAFT: DO NOT CITE OR DISTRIBUTE
3 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
levels of vitamin D.19 Those who experienced stressful events in childhood, such as neglect or 81 abuse, are at an increased risk of chronic stress in adulthood.21 82
Mental health conditions, such as anxiety and depression, and negative emotions, such as 83 anger and pain catastrophizing, can exacerbate chronic pain and reduce quality of life.22,23 Self-84 efficacy (i.e., one’s belief that they can exercise control over pain), pain acceptance, and access 85 to a social support network may act as protective factors.22,24 86
CRNA Scope of Practice 87
CRNAs practice in accordance with their professional scope of practice, federal, state, and local 88 law, facility accreditation standards, and healthcare organization policy to provide chronic pain 89 management services.2 90 91 As advanced practice registered nurses, CRNAs are uniquely skilled to deliver pain 92 management in a compassionate and holistic manner. CRNAs provide chronic pain 93 management services in various settings, such as hospitals, ambulatory surgical centers 94 (ASCs), offices, and pain management clinics. By virtue of education and individual clinical 95 experience and competency, a CRNA may practice chronic pain management utilizing a variety 96 of therapeutic, physiological, pharmacological, interventional, and psychological modalities in 97 the management and treatment of pain. 98 99 As part of their nurse anesthesiologist educational preparation, CRNAs learn and demonstrate 100 competence in the management and treatment of pain, a critical component of anesthesia care. 101 The Council on Accreditation of Nurse Anesthesia Educational Programs (COA) standards25 102 require that nurse anesthesia programs provide content in anatomy, physiology, 103 pathophysiology, pharmacology, and pain management, and require that nurse anesthesia 104 students obtain clinical experiences in regional anesthetic techniques (i.e., spinal, epidural, and 105 peripheral nerve blocks). 106 107 As knowledge of the pain experience, corresponding transmission processes, pain management 108 and treatment modalities, and related technologies evolve, the role of healthcare professionals 109 in managing and treating pain will also evolve. These advancements will translate into clinical 110 practice with the goal of improving patient outcomes. For additional guidance, review the 111 AANA’s CRNA Specialty Clinical Practice.26 112 113 An Interdisciplinary Team Approach 114
CRNAs provide chronic pain management services in a variety of practice models based on 115 patient, provider, and facility needs. CRNAs may work with a primary care provider, 116 orthopedist, neurologist, psychiatrist, social worker, radiologist, physical therapist, another pain 117 specialist, or other providers. The CRNA may receive referrals from other clinicians or serve as 118 the sole provider of chronic pain management services. CRNAs provide patient-centered 119 chronic pain management and treatment, working toward the common goal of decreasing the 120 patient’s pain and improving the patient’s quality of life and functionality. 121 122 When working in collaboration with a patient’s primary care provider or other referring clinician, 123 CRNAs may share certain responsibilities of chronic pain management. The CRNA reviews 124 and may add relevant findings (e.g., history and physical, diagnostic results) to information 125
DRAFT: DO NOT CITE OR DISTRIBUTE
4 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
provided by a referring clinician in order to administer chronic pain management services safely. 126 CRNAs are responsible and accountable for judgments made and actions taken in their 127 professional practice. 128
Chronic Pain Management Guidelines 129
1. Patient Assessment and Evaluation 130 The goal of patient assessment and evaluation is to understand the nature, causes, and 131 severity of pain, and their impact on the patient’s functionality, mood, and overall quality 132 of life.4 This information will help establish a diagnosis and formulate an appropriate plan 133 of care with specific objectives of treatment.27 134
Pain is a subjective experience.28 The patient’s ability to communicate their pain may 135 depend on personal attributes (e.g., age, developmental stage, culture), as well as 136 physiological, emotional, and cognitive states.28 The patient may feel reluctant to discuss 137 their pain openly with a healthcare professional for fear of being judged (e.g., being 138 perceived as responsible for their own pain or come across as complaining too much).29 139
Establishing a patient-CRNA relationship based on communication, empathy, openness, 140 trust, and a non-judgmental attitude is the first step to understanding the patient’s 141 perception of and experience with pain.29-31 The following questions may serve as a 142 guide in the initial patient-CRNA discussion:31-33 143
• Onset: Tell me about your pain: When did it start? How long does it last? How 144 often does it occur? 145
• Location: Where do you feel pain? Do you feel pain in more than one area? 146 • Severity: On a 0-10 scale, where 0 is no pain and 10 is the worst pain 147
imaginable, what is your pain now? … in the last 24 hours? [ Note: There are 148 other available tools to help assess pain, such as Brief Pain Inventory or Wong-149 Baker FACES® Pain Rating Scale.]. 150
• Quality: What does your pain feel like (e.g., aching; dull; sharp; burning; 151 unbearable)? 152
• Alleviating/aggravating factors: What makes your pain better/worse? How 153 does it affect you (e.g., sleep, mood, relationships)? Are there any other 154 symptoms? 155
• Expectations: Do you expect your pain to improve? 156 In addition to the initial discussion, the CRNA should perform a comprehensive 157 patient assessment and evaluation. The patient health history should involve a 158 review of the following: (a) the patient’s medications, including use or misuse; (b) 159 allergies; (c) health and surgical history; (d) psychosocial health, including substance 160 use or misuse; and (e) issues related to respiratory, cardiovascular, renal, hepatic, 161 gastrointestinal, neurologic, endocrine, musculoskeletal, and hematologic 162 systems.1,34 163
The CRNA should conduct a focused pain assessment and evaluation addressing 164 pain symptoms, identification of pain risk factors, and current and previous pain 165 management, including physical and cognitive therapies, alternative modalities, and 166
DRAFT: DO NOT CITE OR DISTRIBUTE
5 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
responses to these therapies.35 Validated instruments should be used when 167 appropriate to evaluate the patient’s quality of life, physical, social, emotional 168 functions, and sleep quality.35-38 For examples of validated instruments, see the 169 American Academy of Family Physician’s Chronic Pain Toolkit.39 The CRNA should 170 also review the patient’s diagnosis and results of relevant diagnostic testing and 171 psychological evaluation. 172
The CRNA may perform further non-interventional and interventional diagnostic 173 procedures in the assessment and evaluation of the patient’s pain that can be used 174 to establish the diagnosis. These procedures may include, but are not limited to, 175 laboratory testing, diagnostic imaging, electrodiagnostic studies, and focused 176 regional injections as indicated.35,40,41 177
2. Management 178 a. Plan of Care 179
The CRNA should formulate a patient-specific management and treatment plan 180 based on findings from the comprehensive assessment and evaluation. The plan 181 should also consider the patient’s values, beliefs, and knowledge and level of 182 understanding about pain, pain management and treatment options.42,43 183
The plan should integrate baseline functional capacity and set realistic functional 184 goals, including measurable targets for pain management.44 A plan to implement 185 alternative modalities should be considered and developed, as appropriate, if the 186 original goals and targets are not met. 187
b. Communication 188 The CRNA and the patient’s treatment team and primary care provider or referring 189 clinician should have ongoing communication regarding the patient’s status, 190 treatment plan, treatment compliance, and prognosis to coordinate the plan for 191 ongoing chronic pain management.42,45,46 192 193
c. Patient Education 194 195
Patient and family/caregiver education should be made available in their preferred 196 method and language regarding etiology of pain, management/treatment plan and 197 goals, potential alternative therapy, and consequences for non-adherence to the 198 plan.45,47-49 Evidence suggests patients who understand their chronic condition are 199 more effective at managing it and report better outcomes compared to those without 200 such knowledge.50 201 202 The CRNA should discuss possible side effects and complications of the regimen 203 with the patient and family/caregiver. In addition, the CRNA should provide 204 instructions to address side effects and respond to complications, should they 205 occur.51 206
Managing the patient’s expectations is critical for successful pain management and 207 treatment. The CRNA and the patient should agree on realistic goals of pain 208 management and how to achieve them (see the “Plan of Care” section above). 209
DRAFT: DO NOT CITE OR DISTRIBUTE
6 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
While patients may experience significant improvement in chronic pain with 210 treatment, complete elimination of pain may not be possible. According to recent 211 estimates, on average, patients achieve only 30 percent reduction in pain with 212 treatment. The CRNA should communicate to the patient that even an incremental 213 reduction in pain can have a positive impact on function and overall quality of life.50 214 Failure to manage patients’ expectations early in the process may lead to non-215 adherence to the plan, poor satisfaction with services received, and poor health 216 outcomes.52 217
When working with racial/ethnic minorities and socioeconomically disadvantaged 218 patients, the CRNA should be aware that these populations are at increased risk for 219 all-cause morbidity and mortality; they may also face psychosocial issues that make 220 them especially vulnerable to undertreatment for pain. By understanding the 221 patient’s perspective, the CRNA can provide effective education that is 222 compassionate and empathetic, thereby reducing stigma, biases, and 223 discrimination.31,53 For additional guidance, review the AANA’s CRNA’s Role in 224 Addressing Racial and Ethnic Disparities in Anesthesia Care.54 225
d. Informed Consent and Treatment Agreement 226 The CRNA should obtain and document informed consent. The informed consent 227 process should include a discussion of the individualized treatment plan, planned 228 procedures, alternative methods of treatment, and risk and benefits of the plan. The 229 patient should be able to demonstrate the “decision-making capacity” or ability to 230 make a meaningful decision about whether or not to undergo treatment, including 231 appreciating the significance of the plan of care and its potential consequences.51 232 The patient should also have an opportunity to ask questions and clarify any 233 information. If desired by the patient, the family or caregiver may participate in this 234 process. For additional guidance regarding informed consent, review the AANA’s 235 Informed Consent for Anesthesia Care.51 This document also includes 236 recommendations on how to effectively facilitate communication with patients from 237 diverse backgrounds and patients requiring special assistance (e.g., patients with 238 limited English proficiency (LEP), visual or hearing impairments, learning disabilities, 239 or cognitive impairments). 240 241 CRNAs should be aware of potential drug-seeking behavior and enter into a pain 242 management treatment agreement with the patient, when appropriate. The pain 243 management treatment agreement establishes an understanding of the elements of 244 the treatment plan and outlines patient and provider responsibilities, expectations for 245 compliance, and response to emergency issues.55 The pain management agreement 246 keeps the patient more accountable and engaged in their care and increases their 247 likelihood of adhering to the plan of care.55 The following questions should be 248 addressed before the patient signs the pain management treatment agreement:56 249
• What medications does the agreement include? 250 • What are the risks with the patient taking these medications? 251 • How does the agreement affect emergency care? 252 • What happens if the patient fails to follow the agreement? 253
DRAFT: DO NOT CITE OR DISTRIBUTE
7 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
254 If applicable, the CRNA should consult their state’s Prescription Drug Monitoring 255 Program (PDMP), a database consisting of every patient’s controlled drug 256 prescriptions by every provider, before prescribing a controlled substance.55 257 258
e. Non-Pharmacologic Management 259 260 Results of studies of non-pharmacologic modalities have been inconclusive due to a 261 lack of large scale, high-level research, and mixed findings regarding the 262 effectiveness of these modalities. Overall, research suggests non-pharmacologic 263 modalities are safe and well-tolerated, and when appropriate, should be considered 264 as part of the plan of care.4 There is also evidence that limited access to non-265 pharmacologic services, such as physical therapy, is associated with an increase in 266 opioid prescriptions; however, more research is needed to investigate this 267 relationship further.57 268 269 The CRNA may work with another provider to implement non-pharmacologic 270 management modalities as part of the plan of care. These modalities may include, 271 but are not limited to:58-62 272
• Physical rehabilitation modalities: therapeutic exercise, transcutaneous 273 elective nerve stimulation, massage therapy, traction, cold and heat 274 therapies, therapeutic ultrasound, bracing, touch therapy. 275
• Psychological and behavioral health approaches: cognitive behavioral 276 therapies, psychological skills training (PST), mindfulness-based stress 277 reduction programs. 278
• Complimentary approaches: yoga, tai chi, acupuncture. 279 • Other modalities: cryoneurolysis (pain management technique that uses 280
cold temperatures to ablate the sensory nerves that cause pain).63 281 282
f. Pharmacologic Management 283 284 Examples of pharmacologic management modalities include, but are not limited 285 to:36,61,64,65 286
• Traditional analgesics: local anesthetics, acetaminophen, nonsteroidal anti-287 inflammatory drugs (NSAIDs), and opioids. 288
• Non-traditional analgesics: anticonvulsants (e.g., gabapentin, pregabalin), 289 N-methyl-D-Aspartate [NMDA]-receptor antagonists (e.g., ketamine), alpha-2 290 adrenergic agonists (e.g., dexmedetomidine), and antidepressants (e.g., 291 duloxetine). 292
Pharmacologic treatment should be tailored to the patient’s health status (e.g., 293 cardiovascular, hepatic, renal, and cognitive issues) due to potential for drug side 294 effects, drug clearance, and drug-drug interactions.66 Pharmacologic treatment 295 should also take into consideration the patient’s type (e.g., neuropathic vs. 296 nociceptive) and level of pain, functionality, and response.66 Additionally, the 297
DRAFT: DO NOT CITE OR DISTRIBUTE
8 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
patient should be assessed and treated for disturbed sleep or depressed or 298 anxious mood that may help increase response to treatment.66 299
Medications should be titrated incrementally to achieve an adequate level of 300 analgesia.43,67,68 Tapering or discontinuing medications should be considered if 301 the patient’s pain is not adequately controlled when taking appropriate doses or if 302 there is no functional improvement on medication therapy. 303
Opioid Therapy 304
Non-opioid modalities should be used as the first line of treatment for 305 chronic pain. Consider opioid therapy only if the benefits outweigh the 306 risks and the patient is not responsive to other pharmacologic and non-307 pharmacologic treatment modalities. Opioids should be used at the lowest 308 effective dose and for shortest duration of time to achieve adequate pain 309 control, with the intention of mitigating negative side effects and opioid 310 addiction risk. 66,69-72 311
Prior to considering/initiating opioid therapy, the CRNA should:66,69-72 312 • Discuss the risks (e.g., addiction, overdose) and benefits of opioids, as well 313
as alternative treatment modalities with the patient. 314 • After completing a comprehensive patient assessment and evaluation, 315
assess the patient’s risk potential for overdose and substance use disorder. 316 Risk factors include sociodemographic factors, pain and drug-related factors, 317 genetics and environment, psychosocial and family history, psychopathology, 318 and alcohol and substance use disorders. The patient who has risk factors in 319 each of the following three categories - psychosocial, drug-related, and 320 genetic - is at the highest risk for prescription drug abuse.73For additional 321 guidance, review the AANA’s Analgesia and Anesthesia for Substance Use 322 Disorder Patient.74 323
• Establish a diagnosis, medical necessity, and treatment goals with 324 measurable outcomes, including function, quality of life and activities of daily 325 living. 326
• Complete informed consent and treatment agreement (see the “Informed 327 Consent and Treatment Agreement” section above). The agreement should 328 also include the patient’s consent to random drug screens. 329
• Provide patient education regarding prescription management, security of 330 medications, and the risk of overdose and potential for substance use 331 disorder. 332
• Work with the patient and their family to set realistic expectations and goals 333 for opioid therapy as well as reasonable expectations about opioid risks. 334
• Use opioids at lowest effective dosage and shortest duration of time to 335 achieve adequate pain management. 336
• Regularly assess risks and benefits after starting treatment or increasing a 337 dose. If risks outweigh benefits or if the patient violates the pain management 338
DRAFT: DO NOT CITE OR DISTRIBUTE
9 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
treatment agreement, make appropriate changes to therapy (e.g., taper or 339 discontinue the opioid while avoiding withdrawal symptoms). 340
• Conduct adherence monitoring for therapeutic outcomes and misuse, abuse, 341 or development of opioid use disorder. Techniques may include qualitative 342 and confirmatory urine drug testing (UDT); consulting PDMP before each 343 prescription; medication reconciliation or “pill counts” and behavioral 344 assessments. Periodic administration of questionnaires, such as Current 345 Opioid Misuse Measure,75,76 Pain Assessment and Documentation Tool,77 or 346 Pain Medication Questionnaire78, can also be helpful in adherence 347 monitoring. 348
• In conjunction with an opioid prescription, consider prescribing naloxone 349 hydrochloride and providing patient instructions for use to mitigate the risk of 350 overdose death.79-81 351
For additional guidance regarding opioid therapy, review the following guidelines and 352 resources: 353
• About CDC’s Opioid Prescribing Guideline (Web resource)82 354 • CDC Guideline for Prescribing Opioids for Chronic Pain – United States, 355
2016 71 356 • Model Policy for the Use of Controlled Substances for the Treatment of Pain 357
Federation of State Medical Boards of the United States, Inc.83 358 • HHS Pain Management Best Practice 72 359 • American Pain Society/American Academy of Pain Medicine Clinical 360
Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer 361 Pain84 362
• VA/DoD Clinical Practice Guideline for Management of Opioid Therapy for 363 Chronic Pain85 364
• WHO Opioid Overdose Guidelines86 365 • WHO Guidelines for Managing Chronic Pain in Pediatric Patients87 366 • The American Academy of Family Physician’s Chronic Pain Toolkit.39 367
368 g. Interventional Therapeutic Techniques 369
Interventional procedures may be indicated in the management of chronic pain in 370 conjunction with or following non-pharmacologic and/or pharmacologic treatment 371 modalities. These techniques may include, but are not limited to: trigger point 372 injection, peripheral nerve block, sympathetic nerve block, intravenous regional 373 anesthesia, medial or lateral branch block, joint injection (e.g., facet, sacroiliac), 374 intrathecal injection, epidural injection with or without steroids, nerve ablation 375 techniques, and evaluation and management of implantable systems.50,88,89 376 377
h. Ongoing Assessment and Evaluation 378 Monitor, measure, and evaluate the patient’s pain, functionality, and response to the 379 treatment plan and adjust the treatment plan accordingly.69 380
e. Safety 381
Valentina Lukyanova
What is your experience with implantable devices? Is this language appropriate?
DRAFT: DO NOT CITE OR DISTRIBUTE
10 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
Patient and healthcare provider safety are paramount. CRNAs integrate safety into 382 the delivery of care and adhere to standards, guidelines, applicable law, and facility 383 policies. Chronic pain management practice incorporates confirmation of patient’s 384 identity; site, procedure, and consent verification, and site marking;90 appropriate 385 patient monitoring;1 procedure time-out;90 universal infection prevention and control 386 precautions;91 safe injection practices;92 and radiation safety.93 For additional 387 guidance, review the AANA’s Standards for Nurse Anesthesia Practice,1 Patient-388 Centered Perianesthesia Communication,90 Infection Control and Prevention 389 Guidelines for Anesthesia Care,91 and Safe Injection Guidelines for Needle and 390 Syringe Use.92 391 392
3. Imaging Technology 393 Ultrasound, fluoroscopy, CT guidance, magnetic resonance imaging (MRI), and emerging 394 imaging technology, such as neuroimaging and virtual reality (VR), may be used, as 395 appropriate, to enhance patient safety and accuracy of invasive diagnostic and therapeutic 396 procedures.94-102 397 398
4. Documentation 399 Document pertinent information and related activities on the patient’s healthcare record in a 400 legible, timely, accurate, and complete manner.1 The patient’s record should include: the 401 results of the patient assessment and evaluation; diagnosis with supporting documentation 402 (e.g., diagnostic testing, laboratory results); the patient-specific treatment plan, goals, and 403 objectives; documentation of informed consent; documentation of the procedure and 404 interventions; and images of needle placement, if imaging technology was used.103 For 405 additional guidance, review the AANA’s Documenting Anesthesia Care.103 For examples of 406 resources regarding documentation for opioid therapy, see Opioid Prescribing Part 1: A 407 Practical Guide to Appropriate Documentation104,105 and Opioid Prescribing Part 2: 408 Appropriate Documentation of Follow-up Visits.105 409
410
5. Telehealth 411 Telehealth has become one of the key strategies to improve access to pain management 412 services and promote self-management, especially in rural/remote and resource-poor 413 settings.106,107 Research shows that patients derive many benefits from the pain 414 management services via telehealth, such as improvements in pain acceptance, pain 415 interference, overall function, mood, and physical activity. Patients with access to telehealth 416 also report high satisfaction with care and lower healthcare costs.106-108 According to Currie 417 et al.’s107 study, telehealth would be more beneficial to the patient if it supplemented 418 traditional in-person care rather than completely replacing it. 419
420
6. Continuous Quality Improvement 421 CRNAs demonstrate continued competency in chronic pain management and treatment, 422 including procedures performed and technology employed. CRNAs engage in continuous 423 quality improvement by using performance metrics, collecting relevant data, and monitoring 424
DRAFT: DO NOT CITE OR DISTRIBUTE
11 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
performance outcomes. For additional guidance, review the AANA’s Standards for Nurse 425 Anesthesia Practice,1 Scope of Nurse Anesthesia Practice,2 Clinical Privileges and Other 426 Responsibilities of Certified Registered Nurse Anesthetists,93 and Continued Competency.109 427
428 Barriers to Chronic Pain Management Services 429
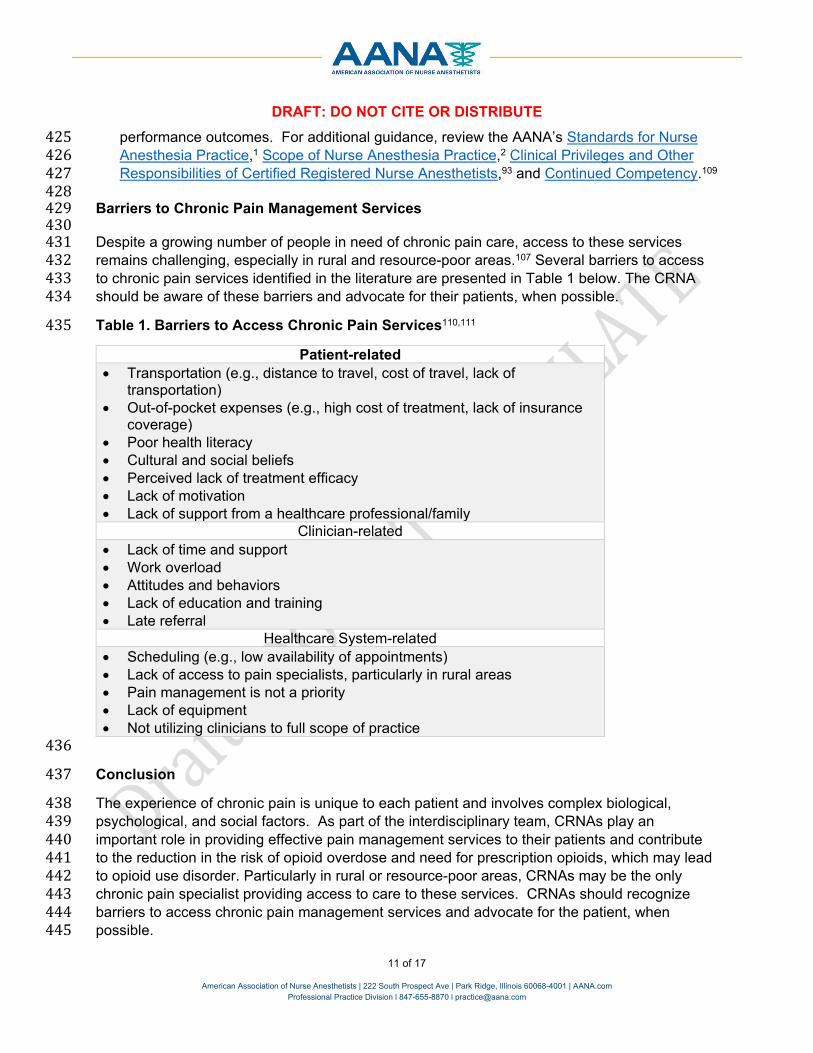
430 Despite a growing number of people in need of chronic pain care, access to these services 431 remains challenging, especially in rural and resource-poor areas.107 Several barriers to access 432 to chronic pain services identified in the literature are presented in Table 1 below. The CRNA 433 should be aware of these barriers and advocate for their patients, when possible. 434
Table 1. Barriers to Access Chronic Pain Services110,111 435
Patient-related • Transportation (e.g., distance to travel, cost of travel, lack of
transportation) • Out-of-pocket expenses (e.g., high cost of treatment, lack of insurance
coverage) • Poor health literacy • Cultural and social beliefs • Perceived lack of treatment efficacy • Lack of motivation • Lack of support from a healthcare professional/family
Clinician-related • Lack of time and support • Work overload • Attitudes and behaviors • Lack of education and training • Late referral
Healthcare System-related • Scheduling (e.g., low availability of appointments) • Lack of access to pain specialists, particularly in rural areas • Pain management is not a priority • Lack of equipment • Not utilizing clinicians to full scope of practice
436
Conclusion 437
The experience of chronic pain is unique to each patient and involves complex biological, 438 psychological, and social factors. As part of the interdisciplinary team, CRNAs play an 439 important role in providing effective pain management services to their patients and contribute 440 to the reduction in the risk of opioid overdose and need for prescription opioids, which may lead 441 to opioid use disorder. Particularly in rural or resource-poor areas, CRNAs may be the only 442 chronic pain specialist providing access to care to these services. CRNAs should recognize 443 barriers to access chronic pain management services and advocate for the patient, when 444 possible. 445
DRAFT: DO NOT CITE OR DISTRIBUTE
12 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
References 446
1. Standards for Nurse Anesthesia Practice. Park Ridge, IL: American Association of Nurse 447 Anesthetists; 2019. 448
2. Scope of Nurse Anesthesia Practice. Park Ridge, IL: American Association of Nurse 449 Anesthetists; 2020. 450
3. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of 451 Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976-452 1982. 453
4. Edinoff A, Sathivadivel N, McBride T, et al. Chronic Pain Treatment Strategies in 454 Parkinson's Disease. Neurol Int. 2020;12(3):61-76. 455
5. Genova A, Dix O, Thakur M, Sangha PS. Chronic Non-cancer Pain Management and 456 Addiction: A Review. Cureus. 2020;12(2):e6963. 457
6. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by 458 central neural plasticity. J Pain. 2009;10(9):895-926. 459
7. McGreevy K, Bottros MM, Raja SN. Preventing Chronic Pain following Acute Pain: Risk 460 Factors, Preventive Strategies, and their Efficacy. Eur J Pain Suppl. 2011;5(2):365-372. 461
8. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of Chronic Pain and High-Impact 462 Chronic Pain Among Adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 463 2018;67(36):1001-1006. 464
9. Smith TJ, Hillner BE. The Cost of Pain. JAMA Netw Open. 2019;2(4):e191532. 465 10. Khan TW, Imani F. The Management of Chronic Pain; Caught Between a Rock and a 466
Hard Place: The Case for a Renewed Focus on Provider, Patient, and Payer Education. 467 Anesth Pain Med. 2017;7(1):e40951. 468
11. Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of 469 opioid misuse, abuse, and addiction in chronic pain: a systematic review and data 470 synthesis. Pain. 2015;156(4):569-576. 471
12. Sheng J, Liu S, Wang Y, Cui R, Zhang X. The Link between Depression and Chronic 472 Pain: Neural Mechanisms in the Brain. Neural Plast. 2017;2017:9724371. 473
13. Petrosky E, Harpaz R, Fowler KA, et al. Chronic Pain Among Suicide Decedents, 2003 474 to 2014: Findings From the National Violent Death Reporting System. Ann Intern Med. 475 2018;169(7):448-455. 476
14. Baldwin M, Boilini H, Lamvu G. Chronic Pain and Suicide: Is There a Role for Ketamine? 477 Mil Med. 2017;182(11):1746-1748. 478
15. Jimenez-Rodriguez I, Garcia-Leiva JM, Jimenez-Rodriguez BM, Condes-Moreno E, 479 Rico-Villademoros F, Calandre EP. Suicidal ideation and the risk of suicide in patients 480 with fibromyalgia: a comparison with non-pain controls and patients suffering from low-481 back pain. Neuropsychiatr Dis Treat. 2014;10:625-630. 482
16. Berube M, Gelinas C, Choiniere M, et al. The effect of psychological interventions on the 483 prevention of chronic pain in adults: a systematic review protocol. Syst Rev. 484 2017;6(1):190. 485
17. Janevic MR, McLaughlin SJ, Heapy AA, Thacker C, Piette JD. Racial and 486 Socioeconomic Disparities in Disabling Chronic Pain: Findings From the Health and 487 Retirement Study. J Pain. 2017;18(12):1459-1467. 488
18. Majedi H, Dehghani SS, Soleyman-Jahi S, et al. Assessment of Factors Predicting 489 Inadequate Pain Management in Chronic Pain Patients. Anesth Pain Med. 490 2019;9(6):e97229. 491
19. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and 492 associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273-e283. 493
DRAFT: DO NOT CITE OR DISTRIBUTE
13 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
20. Burgess HJ, Burns JW, Buvanendran A, et al. Associations Between Sleep Disturbance 494 and Chronic Pain Intensity and Function: A Test of Direct and Indirect Pathways. Clin J 495 Pain. 2019;35(7):569-576. 496
21. Gooding H, Stedmon J, Crix D. 'All these things don't take the pain away but they do 497 help you to accept it': making the case for compassion-focused therapy in the 498 management of persistent pain. Br J Pain. 2020;14(1):31-41. 499
22. Crawford A, Tripp DA, Nickel JC, et al. Depression and helplessness impact interstitial 500 cystitis/bladder pain syndrome pain over time. Can Urol Assoc J. 2019;13(10):328-333. 501
23. Gerhart JI, Burns JW, Bruehl S, et al. Variability in negative emotions among individuals 502 with chronic low back pain: relationships with pain and function. Pain. 2018;159(2):342-503 350. 504
24. Penn TM, Trost Z, Parker R, et al. Social support buffers the negative influence of 505 perceived injustice on pain interference in people living with HIV and chronic pain. Pain 506 Rep. 2019;4(2):e710. 507
25. Standards for Accreditation of Nurse Anesthesia Programs: Practice Doctorate. Park 508 Ridge, IL: Council on Accreditation of Nurse Anesthesia Educational Programs; 2021. 509
26. CRNA Specialty Practice Park Ridge, IL: American Association of Nurse Anesthetists; 510 2018. 511
27. Dansie EJ, Turk DC. Assessment of patients with chronic pain. Br J Anaesth. 512 2013;111(1):19-25. 513
28. Wilcox CE, Mayer AR, Teshiba TM, et al. The Subjective Experience of Pain: An FMRI 514 Study of Percept-Related Models and Functional Connectivity. Pain Med. 515 2015;16(11):2121-2133. 516
29. Hambraeus J, Hambraeus KS, Sahlen KG. Patient perspectives on interventional pain 517 management: thematic analysis of a qualitative interview study. BMC Health Serv Res. 518 2020;20(1):604. 519
30. Haverfield MC, Giannitrapani K, Timko C, Lorenz K. Patient-Centered Pain Management 520 Communication from the Patient Perspective. J Gen Intern Med. 2018;33(8):1374-1380. 521
31. Hirsh AT, Miller MM, Hollingshead NA, et al. A randomized controlled trial testing a 522 virtual perspective-taking intervention to reduce race and socioeconomic status 523 disparities in pain care. Pain. 2019;160(10):2229-2240. 524
32. Fink R. Pain assessment: the cornerstone to optimal pain management. Proc (Bayl Univ 525 Med Cent). 2000;13(3):236-239. 526
33. Yasaei R, Peterson E, Saadabadi A. Chronic Pain Syndrome. StatPearls. Treasure 527 Island (FL)2021. 528
34. Pestka E, Nash V, Evans M, et al. Assessment of family history of substance abuse for 529 preventive interventions with patients experiencing chronic pain: A quality improvement 530 project. Int J Nurs Pract. 2016;22(2):121-128. 531
35. Anderson MA, Akshintala V, Albers KM, et al. Mechanism, assessment and 532 management of pain in chronic pancreatitis: Recommendations of a multidisciplinary 533 study group. Pancreatology. 2016;16(1):83-94. 534
36. Vega E, Beaulieu Y, Gauvin R, et al. Chronic non-cancer pain in children: we have a 535 problem, but also solutions. Minerva Anestesiol. 2018;84(9):1081-1092. 536
37. Morgan KJ, Anghelescu DL. A Review of Adult and Pediatric Neuropathic Pain 537 Assessment Tools. Clin J Pain. 2017;33(9):844-852. 538
38. Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. Br J Anaesth. 539 2008;101(1):17-24. 540
DRAFT: DO NOT CITE OR DISTRIBUTE
14 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
39. The American Academy of Family Physicians. Chronic Pain Toolkit. 541 https://www.aafp.org/dam/AAFP/documents/patient_care/pain_management/cpm-542 toolkit.pdf. Accessed May 1, 2021. 543
40. Allen GM. The diagnosis and management of shoulder pain. J Ultrason. 544 2018;18(74):234-239. 545
41. Chuang CW, Hung SK, Pan PT, Kao MC. Diagnosis and interventional pain 546 management options for sacroiliac joint pain. Ci Ji Yi Xue Za Zhi. 2019;31(4):207-210. 547
42. Jackman RP, Purvis JM, Mallett BS. Chronic nonmalignant pain in primary care. Am 548 Fam Physician. 2008;78(10):1155-1162. 549
43. Burton AW, Fine PG, Passik SD. Transformation of acute cancer pain to chronic cancer 550 pain syndromes. J Support Oncol. 2012;10(3):89-95. 551
44. Teichman PG. A tool for safely treating chronic pain. Fam Pract Manag. 2001;8(10):47-552 49. 553
45. Turk DC, Stanos PS, Palermo TM, et al. Interdisciplinary Pain Management. Glenview, 554 IL: American Pain Society. 2010. 555
46. Blau WS. The needle in a haystack: appropriate use of interventional techniques in the 556 management of chronic pain. N C Med J. 2013;74(3):215-217. 557
47. Morlion B, Kempke S, Luyten P, Coppens E, Van Wambeke P. Multidisciplinary pain 558 education program (MPEP) for chronic pain patients: preliminary evidence for 559 effectiveness and mechanisms of change. Curr Med Res Opin. 2011;27(8):1595-1601. 560
48. Dorflinger L, Kerns RD, Auerbach SM. Providers' roles in enhancing patients' adherence 561 to pain self management. Translational behavioral medicine. 2013;3(1):39-46. 562
49. Butow P, Sharpe L. The impact of communication on adherence in pain management. 563 Pain. 2013;154 Suppl 1:S101-107. 564
50. Tauben DJ, Stacey BR. Approach to the management of chronic non-cancer pain in 565 adults. 2020; https://www.uptodate.com/contents/approach-to-the-management-of-566 chronic-non-cancer-pain-in-adults. Accessed May 5, 2021. 567
51. Informed Consent for Anesthesia Care. Park Ridge, IL: American Association of Nurse 568 Anesthetists; 2016. 569
52. Henry SG, Matthias MS. Patient-Clinician Communication About Pain: A Conceptual 570 Model and Narrative Review. Pain Med. 2018;19(11):2154-2165. 571
53. Johnson-Jennings M, Duran B, Hakes J, Paffrath A, Little MM. The influence of 572 undertreated chronic pain in a national survey: Prescription medication misuse among 573 American indians, Asian Pacific Islanders, Blacks, Hispanics and whites. SSM Popul 574 Health. 2020;11:100563. 575
54. The CRNA’s Role in Addressing Racial and Ethnic Disparities in Anesthesia Care. Park 576 Ridge, IL: American Association of Nurse Anesthetists; 2021. 577
55. Kaye AD, Kandregula S, Kosty J, et al. Chronic pain and substance abuse disorders: 578 Preoperative assessment and optimization strategies. Best Pract Res Clin Anaesthesiol. 579 2020;34(2):255-267. 580
56. WebMD. Your pain treatment agreement. https://www.webmd.com/pain-581 management/pain-management-pain-treatment-agreement. Accessed May 11, 2021. 582
57. Karmali RN, Skinner AC, Trogdon JG, Weinberger M, George SZ, Hassmiller Lich K. 583 The association between the supply of select nonpharmacologic providers for pain and 584 use of nonpharmacologic pain management services and initial opioid prescribing 585 patterns for Medicare beneficiaries with persistent musculoskeletal pain. Health Serv 586 Res. 2020. 587
DRAFT: DO NOT CITE OR DISTRIBUTE
15 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
58. Patil NJ, Nagaratna R, Tekur P, Manohar PV, Bhargav H, Patil D. A Randomized Trial 588 Comparing Effect of Yoga and Exercises on Quality of Life in among nursing population 589 with Chronic Low Back Pain. Int J Yoga. 2018;11(3):208-214. 590
59. Khoo EL, Small R, Cheng W, et al. Comparative evaluation of group-based mindfulness-591 based stress reduction and cognitive behavioural therapy for the treatment and 592 management of chronic pain: A systematic review and network meta-analysis. Evid 593 Based Ment Health. 2019;22(1):26-35. 594
60. Moseley GL, Baranoff J, Rio E, Stewart M, Derman W, Hainline B. Nonpharmacological 595 Management of Persistent Pain in Elite Athletes: Rationale and Recommendations. Clin 596 J Sport Med. 2018;28(5):472-479. 597
61. Manworren RC. Multimodal pain management and the future of a personalized medicine 598 approach to pain. AORN J. 2015;101(3):308-314; quiz 315-308. 599
62. Marley J, Tully MA, Porter-Armstrong A, et al. The effectiveness of interventions aimed 600 at increasing physical activity in adults with persistent musculoskeletal pain: a systematic 601 review and meta-analysis. BMC Musculoskelet Disord. 2017;18(1):482. 602
63. Smiley A, McGuire J. Cryoneurolysis for the Treatment of Sensory Nerve Pain. AANA J. 603 2018;86(6):495-503. 604
64. Enamandram M, Rathmell JP, Kimball AB. Chronic pain management in dermatology: a 605 guide to assessment and nonopioid pharmacotherapy. J Am Acad Dermatol. 606 2015;73(4):563-573; quiz 573-564. 607
65. Wren K, Lancaster RJ, Walesh M, et al. Intravenous Lidocaine for Relief of Chronic 608 Neuropathic Pain. AANA J. 2019;87(5):351-355. 609
66. Tauben DJ, Stacey BR. Pharmacologic management of chronic non-cancer pain. 2020. 610 67. Debono DJ, Hoeksema LJ, Hobbs RD. Caring for patients with chronic pain: pearls and 611
pitfalls. J Am Osteopath Assoc. 2013;113(8):620-627. 612 68. Leung L. From ladder to platform: a new concept for pain management. J Prim Health 613
Care. 2012;4(3):254-258. 614 69. Nafziger AN, Barkin RL. Opioid Therapy in Acute and Chronic Pain. J Clin Pharmacol. 615
2018;58(9):1111-1122. 616 70. Centers for Disease Control and Prevention. Checklist for prescribing opioids for chronic 617
pain. https://www.cdc.gov/drugoverdose/pdf/pdo_checklist-a.pdf. Accessed May 6, 618 2021. 619
71. Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic 620 Pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1-49. 621
72. Cheng J, Rutherford M, Singh VM. The HHS Pain Management Best Practice Inter-622 Agency Task Force Report Calls for Patient-Centered and Individualized Care. Pain 623 Med. 2020;21(1):1-3. 624
73. Kaye AD, Jones MR, Kaye AM, et al. Prescription Opioid Abuse in Chronic Pain: An 625 Updated Review of Opioid Abuse Predictors and Strategies to Curb Opioid Abuse: Part 626 1. Pain Physician. 2017;20(2S):S93-S109. 627
74. Analgesia and Anesthesia for the Substance Use Disorder Patient. Park Ridge, IL: 628 American Association of Nurse Anesthetists; 2019. 629
75. Butler SF, Budman SH, Fernandez KC, et al. Development and validation of the Current 630 Opioid Misuse Measure. Pain. 2007;130(1-2):144-156. 631
76. Butler SF, Budman SH, Fanciullo GJ, Jamison RN. Cross validation of the current opioid 632 misuse measure to monitor chronic pain patients on opioid therapy. Clin J Pain. 633 2010;26(9):770-776. 634
DRAFT: DO NOT CITE OR DISTRIBUTE
16 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
77. Passik SD, Kirsh KL, Whitcomb L, et al. A new tool to assess and document pain 635 outcomes in chronic pain patients receiving opioid therapy. Clin Ther. 2004;26(4):552-636 561. 637
78. Adams LL, Gatchel RJ, Robinson RC, et al. Development of a self-report screening 638 instrument for assessing potential opioid medication misuse in chronic pain patients. J 639 Pain Symptom Manage. 2004;27(5):440-459. 640
79. National Institute on Drug Abuse. Naloxone DrugFacts. 641 https://www.drugabuse.gov/publications/drugfacts/naloxone. Accessed June 14, 2021. 642
80. U.S. Food and Drug Administration. Drug Safety Communication. 2020; 643 https://www.fda.gov/media/140360/download. Accessed June 14, 2021. 644
81. Susbance Abuse and Mental Health Services Administration. Naloxone. . 645 https://www.samhsa.gov/medication-assisted-treatment/medications-counseling-related-646 conditions/naloxone. Accessed June 14, 2021. 647
82. Centers for Disease Control and Prevention. About CDC's Opioid Prescribing Guideline. 648 https://www.cdc.gov/drugoverdose/prescribing/guideline.html. Accessed May 5, 2021. 649
83. The Federation of State Medical Boards of the United States, Inc. Guidelines for the 650 chronic use of opioid analgesics. 2017; 651 https://www.fsmb.org/siteassets/advocacy/policies/opioid_guidelines_as_adopted_april-652 2017_final.pdf. Accessed May 5, 2021. 653
84. Chou R. 2009 Clinical Guidelines from the American Pain Society and the American 654 Academy of Pain Medicine on the use of chronic opioid therapy in chronic noncancer 655 pain: what are the key messages for clinical practice? Pol Arch Med Wewn. 2009;119(7-656 8):469-477. 657
85. VA/DoD Clinical Practice Guideline for Management of Opioid Therapy for Chronic Pain. 658 2017; https://www.healthquality.va.gov/guidelines/Pain/cot/VADoDOTCPG022717.pdf. 659 Accessed May 5, 2021. 660
86. World Health Organization. Community Management of Opioid Overdose. 2014; 661 https://www.who.int/publications/i/item/9789241548816. Accessed May 11, 2021. 662
87. World Health Organization. Guidelines on the management of chronic pain in children. 663 2020; https://www.who.int/publications/i/item/9789240017870. Accessed May 24, 2021. 664
88. Mesregah MK, Feng W, Huang WH, et al. Clinical Effectiveness of Interlaminar Epidural 665 Injections of Local Anesthetic with or without Steroids for Managing Chronic Neck Pain: 666 A Systematic Review and Meta-Analysis. Pain Physician. 2020;23(4):335-348. 667
89. Vega E, Rivera G, Echevarria GC, Prylutskyy Z, Perez J, Ingelmo P. Interventional 668 procedures in children and adolescents with chronic non-cancer pain as part of a 669 multidisciplinary pain treatment program. Paediatr Anaesth. 2018;28(11):999-1006. 670
90. Patient-Centered Perianesthesia Communication. Park Ridge, IL: American Association 671 of Nurse Anesthesia; 2014. 672
91. Infection Prevention and Control Guidelines for Anesthesia Care. Park Ridge, IL: 673 American Association of Nurse Anesthetists; 2015. 674
92. Safe Injection Guidelines for Needle and Syringe Use. . Park Ridge, IL: American 675 Association of Nurse Anesthetists; 2014. 676
93. Clinical Privileges and Other Responsibilities of Certified Registered Nurse Anesthetists. 677 Park Ridge, IL: American Association of Nurse Anesthetists; 2019. 678
94. Kline JP. Ultrasound guidance in anesthesia. AANA J. 2011;79(3):209-217. 679 95. Jee H, Lee JH, Kim J, Park KD, Lee WY, Park Y. Ultrasound-guided selective nerve root 680
block versus fluoroscopy-guided transforaminal block for the treatment of radicular pain 681 in the lower cervical spine: a randomized, blinded, controlled study. Skeletal Radiol. 682 2013;42(1):69-78. 683
DRAFT: DO NOT CITE OR DISTRIBUTE
17 of 17
American Association of Nurse Anesthetists | 222 South Prospect Ave | Park Ridge, Illinois 60068-4001 | AANA.com Professional Practice Division l 847-655-8870 l [email protected]
96. Wald JT, Maus TP, Diehn FE, et al. CT-guided cervical transforaminal epidural steroid 684 injections: Technical insights. J Neuroradiol. 2014;41(3):211-215. 685
97. Wald JT, Maus TP, Geske JR, et al. Safety and efficacy of CT-guided transforaminal 686 cervical epidural steroid injections using a posterior approach. AJNR Am J Neuroradiol. 687 2012;33(3):415-419. 688
98. Evansa I, Logina I, Vanags I, Borgeat A. Ultrasound versus fluoroscopic-guided epidural 689 steroid injections in patients with degenerative spinal diseases: A prospective, 690 randomised study. Eur J Anaesthesiol. 2014. 691
99. Martucci KT, Mackey SC. Imaging Pain. Anesthesiol Clin. 2016;34(2):255-269. 692 100. Martucci KT, Ng P, Mackey S. Neuroimaging chronic pain: what have we learned and 693
where are we going? Future Neurol. 2014;9(6):615-626. 694 101. Martucci KT, Mackey SC. Neuroimaging of Pain: Human Evidence and Clinical 695
Relevance of Central Nervous System Processes and Modulation. Anesthesiology. 696 2018;128(6):1241-1254. 697
102. Jones T, Moore T, Choo J. The Impact of Virtual Reality on Chronic Pain. PLoS One. 698 2016;11(12):e0167523. 699
103. Documenting anesthesia care. Park Ridge, IL: The American Association of Nurse 700 Anesthetists; 2016. 701
104. Schneider J. Opioid prescribing part 1: A practical guide to appropriate documentation. 702 Practical Pain Management. 2014;14(1). 703
105. Schneider J. Opioid prescribing part 2: Appropriate documentation of follow-up visits. 704 Practical Pain Management. 2014;14(2). 705
106. Scriven H, Doherty DP, Ward EC. Evaluation of a multisite telehealth group model for 706 persistent pain management for rural/remote participants. Rural Remote Health. 707 2019;19(1):4710. 708
107. Currie M, Philip LJ, Roberts A. Attitudes towards the use and acceptance of eHealth 709 technologies: a case study of older adults living with chronic pain and implications for 710 rural healthcare. BMC Health Serv Res. 2015;15:162. 711
108. Pronovost A, Peng P, Kern R. Telemedicine in the management of chronic pain: a cost 712 analysis study. Can J Anaesth. 2009;56(8):590-596. 713
109. Continued Competency. Park Ridge, IL: American Association of Nurse Anesthetists; 714 2013. 715
110. Becker WC, Dorflinger L, Edmond SN, Islam L, Heapy AA, Fraenkel L. Barriers and 716 facilitators to use of non-pharmacological treatments in chronic pain. BMC Fam Pract. 717 2017;18(1):41. 718
111. Goucke CR, Chaudakshetrin P. Pain: A Neglected Problem in the Low-Resource 719 Setting. Anesth Analg. 2018;126(4):1283-1286. 720
721