Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study

of 14
-
Upload
sarlitaindahpermatasari -
Category
Documents
-
view
215 -
download
0
Transcript of Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
1/14
OBSTETRICS
Chronic hypertension in pregnancy andthe risk of congenital malformations: acohort studyBrian T. Bateman, MD, MSc; Krista F. Huybrechts, MS, PhD; Michael A. Fischer, MD, MS;Ellen W. Seely, MD; Jeffrey L. Ecker, MD; Anna S. Oberg, MD, PhD; Jessica M. Franklin, PhD;Helen Mogun, MS; Sonia Hernandez-Diaz, MD, DrPH
OBJECTIVE: Chronic hypertension is a common medical condition inpregnancy. The purpose of the study was to examine the associationbetween maternal chronic hypertension and the risk of congenitalmalformations in the offspring.
STUDY DESIGN: We dened a cohort of 878,126 completed preg-nancies linked to infant medical records using the Medicaid AnalyticExtract. The risk of congenital malformations was compared betweennormotensive controls and those with treated and untreated chronichypertension. Confounding was addressed using propensity scorematching.
RESULTS: After matching, compared with normotensive controls,pregnancies complicated by treated chronic hypertension were atincreased risk of congenital malformations (odds ratio [OR], 1.3; 95%condence interval [CI], 1.2e 1.5), as were pregnancies with
untreated chronic hypertension (OR 1.2; 95% CI, 1.1e 1.3). In ouranalysis of organ-specic malformations, both treated and untreatedchronic hypertension was associated with a signicant increase inthe risk of cardiac malformations (OR, 1.6; 95% CI, 1.4e 1.9 and OR,1.5; 95% CI, 1.3e 1.7, respectively). These associations persistedacross a range of sensitivity analyses.
CONCLUSION: There is a similar increase in the risk of congenital mal-formations (particularly cardiac malformations) associated with treatedand untreated chronic hypertension that is independent of measuredconfounders. Studies evaluating the teratogenic potential of antihyper-tensive medications must control for confounding by indication. Fetusesand neonates of mothers with chronic hypertension should be carefullyevaluated for potential malformations, particularly cardiac defects.
Key words:birth defect, drug, epidemiology, hypertension, pregnancy
Cite this article as: Bateman BT, Huybrechts KF, Fischer MA, et al. Chronic hypertension in pregnancy and the risk of congenital malformations: a cohort study. Am JObstet Gynecol 2015;212:337.e1-14.
C hronic hypertension is a commonmedical condition in pregnancy,and its prevalence is rising because alarger number of parturients a re obeseand of advanced maternal age. 1,2 As aconsequence, exposure to antihyperten-sive medications during pregnancy,including in the rst trimester when
organogen esis occurs, is common andincreasing. 3-5
Certain classes of antihypertensive me-dications taken during the rst trimesterincluding beta blockers, diuretics, andangiotensin-converting enzyme inhibitorshave beenassociatedwithan increased risk of speci c congenital malformations. 6-11
However, several recent studies havesuggested that it may be the underlying chronic hypertension that confers risk and not exposure to these medicationsper se, because of the following:(1) an elevation in risk of malformationswas observed across antihypertensiveclasses and/or (2) the association with
From the Divisions of Pharmacoepidemiology and Pharmacoeconomics (Drs Bateman, Huybrechts, Fischer, and Franklin and Ms Mogun) and
Research ajog.org
http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
2/14
certain medications was no longer pre-sent when medication users were com-pared with a control group that includeduntreated hypertensive patients. 6,8,12
Little is known about the role of chronic hypertension alone in confer-ring a risk of congenital malformations,and there has been a call from expertsfor further study in this area. 13 Specif-ically, there are few data on whetherchronic hypertension confers a risk of
malformations independent of otherconfounding factors (eg, diabetes, ma-ternal age, antihypertensive agents) andwhich speci c malformations, if any, areassociated with hypertension. Such in-formation may be useful to cliniciansin counseling patients and in guiding screening for malformations.
It may also be important in informing the design of future studies of the te-ratogenic potential of antihypertensivemedications. We therefore sought toexamine the effect of chronic hyperten-sion on the risk of congenital malfor-mations in a large cohort of pregnanciesin Medicaid bene ciaries.
M ATERIALS AND METHODSCohortThe cohort was derived from the Me-dicaid Analytic eXtract (MAX), whichcontains information on Medicaid ben-e ciaries; Medicaid is the joint state andfederal health insurance program forlow-income individuals in the UnitedStates.
MAX is a health care utilizationdatabase that records Medicaid enroll-ment and utilization claims, including those for inpatient admissions and out-patient visits as well as outpatient phar-macy dispensing claims. Using the MAX
using a validated algorithm based ondiagnostic codes in the maternal andinfant records. 15
We restricted the cohort to womenwho were eligible for Medicaid continu-ously from 3 months prior to the esti-mated LMP month through 1 monthpostpartum. To ensure complete ascer-tainment of relevant claims, we re-stricted our analysis to women with 28days or more of enrollment each month
and without restricted bene ts, privateinsurance, or certain state-speci c man-aged care programs (that underreportclaims to MAX).
To allow for an accurate capture of congenital malformations, we also re-quired that the linked infants met thesame Medicaid eligibility criteria as themothers for at least 3 months following the birth (unless they died, in whichcase a shorter eligibility period wasallowed). The source cohort included891,699 completed pregnancies withlinked infants.
We excluded women who were ex-posed to known teratogenic medicationsincluding lithium, antineoplastic agents,
retinoids, or thalidomide from the esti-mated LMP through the date of delivery based on claims for dispensed medica-tions or who had an infant with aninpatient or outpatient diagnosis codeindicating the presence of a chromo-somal abnormality.
We also excluded women who wereexposed to antihypertensive medicationsduring the rst trimester but who lackeddiagnosis codes indicating chronic hy-pertension because of a signi cant risk of misclassifying the presence or absenceof hypertension in these patients (be-cause the women may have received the
chronic hypertension who were treatedwith an antihypertensive medicationduring the rst trimester, and (3)womenwith chronic hypertension who were nottreated with an antihypertensive medi-cation during the rst trimester.
Chronic hypertension was de ned by codes recorded on 2 or more distinctdates indicating chronic or preexisting hypertension recorded in the maternalinpatient or outpatient record at any
time from 3 months prior to the LMPthrough delivery. The codes werederived from the International Classi -cation of Disease-Clinical Modi cation,ninth edition, and included codes642.0x, 642.1x, 642.2x, 642.7x, and401.xx through 405.xx. These codes arespeci c to chronic hypertension and aredistinct from codes that indicate otherhypertensive disorders of pregnancy including gestational hypertension andpreeclampsia.
Antihypertensive exposure during therst trimester was de ned by a lled
prescription whose days ’ supply over-lapped the period from the LMP to90 days after the LMP. In de ning this
exposure, we used prescriptions lledfrom 3 months prior to the LMP until90 days after the LMP. Duration of exposure was estimated based on thenumber of days ’ supply. We accumulateddays’ supply for consecutive pre-scriptions of the same medication if themedication was re lled prior to the day that the prior prescription was expectedto run out. The list of antihypertensivemedications considered in the analysiscan be found in the Appendix (Supple-mentary Table 1 ).
Outcomes
Research Obstetrics ajog.org
http://-/?-http://-/?-http://-/?-http://www.ajog.org/http://www.ajog.org/http://-/?-http://-/?-http://-/?-
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
3/14
malformations; genitourinary malfor-mations; musculoskeletal malforma-tions; or other malformations.
We required 2 codes to de ne thepresence of malformations to excludecases in which a single mention may be recorded to justify a diagnostic testto rule out a condition. Our group haspreviously validated speci c cardiacmalformations using this approach withmedical records; the posit ive predictedvalue was greater than 75%. 16 Secondary outcomes included each of the organ-
(grouped as white [non-Hispanic], black [non-Hispanic], Hispanic, Asian/Paci cIslander, other, or missing); region of delivery (Northeast, South, West, orMidwest); and year of delivery.
Comorbid medical and obstetric con-ditions were identi ed by the presenceof 1 or more diagnosis codes in thematernal inpatient or outpatient recordfrom 3 months prior to the estimatedLMP through delivery. These includedpreexisting diabetes mellitus, chronicrenaldisease, obesity, tobacco use, alcohol
rst trimester (chronic hypertension,diabetes, obesity, etc) may not alwaysbe coded with delity during this rela-tively brief window. Additionally, con-ditions that develop later in pregnancy (eg, gestational diabetes) may be mark-ers for risk factors that are present inthe rst trimester (maternal obesity orhyperglycemia).
The validity of this approach rests onthe assumption that the development of
a congenital malformation in the infantdoes not lead to the development orpreferential recording of these maternalconditions. Although this is likely a safeassumption for the conditions assessed,we also conducted a sensitivity analysisto ensure that our ndings were robustwhen the window during which expo-sure and covariates were ascertained wascon ned to theprepregnancy period and
rst trimester (see the following text).Maternal medication exposures as-
sessed included exposure to either in-sulin or oral hypoglycemic medicationsfrom3 months prior to the LMP throughdelivery (which may be markers for thepresence or severity of maternal preex-
isting or gestational diabetes). We alsoidenti ed and considered as a covariatein our analyses exposure to any poten-tially teratogenic medications during the
rst trimester including uconazole,aminoglycosides, folic acid antagonists,methimazole, potassium iodide, tetra-cycline, danazol, misoprostol, statins,coumadin, and propylthiouracil, whichmay act as confounders if women withchronic hypertension are exposed tothese medications with a frequency thatis different from normotensive women.
Finally, we considered measures of health care utilization during the 3
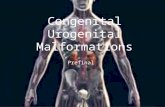
FIGURE 1Patient owchart
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
ajog.org Obstetrics Research
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
4/14
hypertension who did not receive anti-hypertensive medications in the rsttrimester (controls), women with chro-nic hypertension who were exposed toan antihypertensive medication during the rst trimester (treated chronic hy-pertensives), and women with chronichypertension who were not treated withan antihypertensive during the rsttrimester (untreated chronic hyperten-sives) and summarized them as counts
and proportions.We conducted 2 separate comparisonsin our analyses: (1) controls vs subjectstreated for chronic hypertension and (2)controls vs untreated chronic hyperten-sives. In each analysis, we rst deter-mined the frequency of and unadjustedodds ratio (OR) and 95% con denceintervals (CIs) for the primary and sec-ondary outcomes.
To account for the differences in thebaseline characteristics in the groupsthat are being compared, we performedpropensity score analyses. In the rstanalysis (comparing controls and sub- jects treated for hypertension), we used alogistic regression model to estimate the
probability of being a subject treated forhypertension (as opposed to a control)based on the maternal demographiccharacteristics, comorbid medical con-ditions, obstetric characteristics/condi-tions, maternal medication exposures,and measures of health care utilization,as de ned in previous text, withoutfurther selection (this probability is thepropensity score).
Controls and treated subjects treatedfor chronic hypertension were thenmatched on their propensity score in a
xed 3:1 ratio using a nearest neighboralgorithm with a maximum matching
for the presence of diabetes (ie, diabetesmay be more severe in the hypertensivepatients), we repeated our analysis ex-cluding patients with any codes ormedications indicating the presence of diabetes.
Speci cally, we excluded womenwho had any diagnosis codes indicating preexisting or gestational diabetes orwho had prescriptions for insulin or oraldiabetes medications from 3 months
prior to the LMP through delivery. Thetotal number of the excluded patientswas 88,937.
We then repeated the propensity scoree matched analysis, focusing on theoutcomes of overall congenital malfor-mations and cardiac malformations(which were signi cantly associated withboth treated and untreated hypertensionin the primary analysis).
We performed a second sensitivity analysis excluding patients with pretermdelivery. Preterm delivery has a com-plex relationship to congenital malfor-mations because of the following: (1)infants with congenital malformationsare more likely to deliver preterm, and
(2) infants born preterm will sometimeshave conditions that might be codedas malformations (eg, patent ductusarterious, patent foramen ovale, unde-scended testes) that would have sponta-neously resolved had the infant beencarried to term.
In the rst scenario, controlling forprematurity could induce an associationbetween hypertension or antihyperten-sives and malformations. In the secondscenario, controlling for prematurity would be justi ed if we were interestedin the direct effect of hypertension orantihypertensives not mediated through
In the primary analysis, we collectedinformation on covariates from priorto the LMP through delivery to im-prove our ascertainment of chronic hy-pertension and conditions that mightconfound the association of chronic hy-pertension and malformations. Howev-er, if a woman is diagnosed as carrying aninfant with a malformation on prenatalultrasound, it is possible that hermedicalconditions would be scrutinized more
carefully and/or recorded more accu-rately in the medical record (surveillancebias). To ensure that this potential biasdid not affect our results, we repeatedour analysis de ning chronic hyperten-sion and the covariates used in theanalysis based solely on codes recordedin the maternal record from 3 monthsprior to the LMP through the end of the rst trimester.
We required codes in the infant recordrecorded on separate days to de ne thepresence of an organ-speci c malfor-mation in the primary analysis. This wasdone to minimize the risk of identifying malformations based on codes used to justify rule-out diagnostic tests. Howev-
er, to test that our results were robust tothis approach, we repeated the primary analysis with the outcome de ned basedon 1 or more codes in infant inpatientor outpatient record from day of birthto day 90 of life.
To determine the potential effects of residual confounding in our analyses,we de ned the strength (confounder-outcome relative risk) of a hypotheticalresidual confounder that, if present,would explain the effect of treatedand untreated chronic hypertension onthe risk of developing a congenitalmalformation. Because the strength of
Research Obstetrics ajog.org
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
5/14
obstruction, single ventricle, secun-dum atrial septal defect, conotruncaldefect, and left ventricular out ow obstruction.
Analyses were performed in SASversion 9.3 (SAS Institute, Cary, NC).
R ESULTSOur primary cohort consistedof 878,126completed pregnancies. Overall, 19,789(2.3%) had chronic hypertension; of
these, 8307 (42.0%) were treated withantihypertensive medication. As shownin Table 1, there were important baselinedifferences in patients without hyper-tension, with treated hypertension, andwith untreated hypertension.
Patients with chronic hypertensiontended to be older, were more oftenAfrican-American, and had a higherprevalence of preexisting diabetes, ges-tational diabetes, and renal disease.They were also more often exposed toinsulin or other diabetic medications.These differences from normotensivecontrols were greater for patients withtreated chronic hypertension than un-treated hypertension. After propensity
score matching, these imbalances wereno longer present, with the absolutedifference in the frequency of all cova-riates less than 2% ( Table 2).
Congenital malformations in theoffspring were observed in 29,934 preg-nancies without chronic hypertension orantihypertensive exposure (3.49%), 491pregnancies with treated chronic hyper-tension (5.91%), and 581 pregnancieswith untreated hypertension (5.06%).The most commonly observed organ-speci c malformations in the offspring were cardiac, followed by musculoskel-etal, genitourinary, and gastrointestinal malformations, cardiac malformations, increased in the treated and untreated
TABLE 1Baseline characteristics of study patients
CharacteristicWithout chronichypertension
Treated chronichypertensives
Untreated chronichypertensives
Total 858,337 8307 11,482
Age group, y
19 256,973 (29.9) 402 (4.8) 2063 (18)
20-24 308,140 (35.9) 1539 (18.5) 3435 (29.9)
25-29 173,291 (20.2) 2396 (28.8) 2958 (25.8)
30-34 78,721 (9.2) 2201 (26.5) 1794 (15.6)35-39 33,987 (4) 1361 (16.4) 949 (8.3)
40 7225 (0.8) 408 (4.9) 283 (2.5)
Race/ethnicity
White, non-Hispanic 349,369 (40.7) 2684 (32.3) 4313 (37.6)
Black, non-Hispanic 289,867 (33.8) 4337 (52.2) 5179 (45.1)
Hispanic 131,057 (15.3) 689 (8.3) 1110 (9.7)
Asian 29,681 (3.5) 185 (2.2) 257 (2.2)
Other 41,039 (4.8) 248 (3) 402 (3.5)
Unknown 17,324 (2.0) 164 (2.0) 221 (1.9)
Patient characteristics
Preexisting DM 33,694 (3.9) 1989 (23.9) 1669 (14.5)
Gestational DM 67,081 (7.8) 2122 (25.5) 2216 (19.3)
Chronic renal disease 9362 (1.1) 404 (4.9) 517 (4.5)Tobacco use 71,216 (8.3) 661 (8.0) 1007 (8.8)
Medication exposure
Insulin 15,648 (1.8) 1343 (16.2) 1005 (8.8)
Oral diabetes medications 16,682 (1.9) 2042 (24.6) 1010 (8.8)
Values are numbers (percentages). Also included as covariates are the following: multiple births, muliparity, obesity, alcoholabuse, illicit drug use, potentially teratogenic medications during rst trimester, distinct none antihypertensive prescriptionsdrugs from 90 days before to 90 days after the LMP, number of physician visits for any reason from 90 days before to 90 days
after the LMP, year, and region.DM , diabetes mellitus; LMP , last menstrual period.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
ajog.org Obstetrics Research
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
6/14untreated chronic hypertension was Across each of the sensitivity analyses, We de ned the strength of a hypo-
TABLE 2Baseline characteristics of study patients after propensity score matching
Characteristic
Comparison 1 Comparison 2Without chronichypertension
Treated chronichypertensives
Without chronichypertension
Untreated chronichypertensives
Total 23,427 7809 34,434 11,478
Age group, y
19 1082 (4.6) 402 (5.2) 6069 (17.6) 2063 (18)
20-24 4590 (19.6) 1532 (19.6) 10,185 (29.6) 3434 (29.9)
25-29 6961 (29.7) 2322 (29.7) 9084 (26.4) 2957 (25.8)30-34 6178 (26.4) 2006 (25.7) 5369 (15.6) 1793 (15.6)
35-39 3563 (15.2) 1187 (15.2) 2899 (8.4) 948 (8.3)
40 1053 (4.5) 360 (4.6) 828 (2.4) 283 (2.5)
Race/ethnicity
White, non-Hispanic 7989 (34.1) 2585 (33.1) 13,362 (38.8) 4313 (37.6)
Black, non-Hispanic 11,793 (50.3) 3967 (50.8) 15,425 (44.8) 5175 (45.1)
Hispanic 2025 (8.6) 677 (8.7) 3205 (9.3) 1110 (9.7)
Asian 481 (2.1) 185 (2.4) 639 (1.9) 257 (2.2)
Other 692 (3) 241 (3.1) 1157 (3.4) 402 (3.5)
Unknown 447 (1.9) 154 (2) 646 (1.9) 221 (1.9)
Patient characteristics
Preexisting DM 4375 (18.7) 1553 (19.9) 4788 (13.9) 1665 (14.5)
Gestational DM 5458 (23.3) 1781 (22.8) 6639 (19.3) 2214 (19.3)Chronic renal disease 986 (4.2) 319 (4.1) 1402 (4.1) 514 (4.5)
Tobacco use 1827 (7.8) 632 (8.1) 2992 (8.7) 1007 (8.8)
Medication exposure
Insulin 2672 (11.4) 986 (12.6) 2843 (8.3) 1001 (8.7)
Oral diabetes medications 3698 (15.8) 1398 (17.9) 2636 (7.7) 1006 (8.8)
Values are numbers (percentages). Also included as covariates are the following: multiple births, muliparity, obesity, alcohol abuse, illicit drug use, potentially teratogenic medications during the rst
trimester, distinct none antihypertensive prescriptions drugs from 90 days before to 90 days after the LMP, number of physician visits for any reason from 90 days before to 90 days after the LMP,year, and region.DM , diabetes mellitus; LMP , last menstrual period.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
Research Obstetrics ajog.org
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
7/14
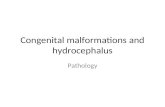
chronic hypertension if theprevalence of the confounder in the treated hyperten-sion group was 10%, a risk ratio of 3.2 if
the prevalence was 20% and a risk ratioof 2.3 if the prevalence was 30%.For the untreated chronic hypertension
effect to be explained by an unmeasuredconfounder, a confounder-outcome risk ratio of 6.6 would be required if the pre-valence of the confounder in the un-treated hypertension group was 10%, arisk ratio of 2.6 if the prevalence was20%, and a risk ratio of 1.9 if the preva-lence was 30% (Figure 2).
Having demonstrated an associationbetween cardiac malformations andboth treated and untreated hyperten-sion, we explored the association with
in the risk of congenital malformationsin the infant after adjusting for con-founding factors as compared with
normotensive controls. This increasein risk persisted across a number of sensitivity analyses. In our evaluationof organ-speci c malformations, bothtreated and untreated chronic hyperten-sion was associated with an increased risk of cardiac malformations.
Chronic hypertension has not beentraditionally identi ed as a risk factorfor congenital malformations in theoffspring. As such, most prior studies of the teratogenic potential of antihyper-tensive medications have not carefully accounted for potential confounding by indication. Our ndings therefore
offspring. A cohort studybyLiet al 12 of theteratogenic potential of angiotensin-converting enzyme inhibitors in the rst
trimester found that a comparison groupof patients withuntreatedhypertension, asde ned by diagnosis codes indicating hypertension from prior to pregnancy through delivery, had an increased risk of congenital heart defe cts and neural tubedefects. Caton et al,6 in a case-controlstudy, found that untreated hypertension(again, de ned by hypertension anytimeduring pregnancy) was associated with anincreased point estimate forcardiovascularmalformations but with wide CIs thatintersected the null.
Our ndings con rm and extendthese observations from previous
TABLE 3The association between chronic hypertension (treated and untreated) and congenital malformations compared
with normotensive controls
Characteristic
Treated chronic hypertensives Untreated chronic hypertensives
Unadjusted PS matched Unadjusted PS matched
Composite congenital malformations 1.7 (1.6e 1.9) 1.3 (1.2e 1.5) 1.5 (1.4e 1.6) 1.2 (1.1e 1.3)
Organ-specic malformation
Central nervous system malformations 2.0 (1.3e 3) 1.4 (0.8e 2.3) 1.4 (0.9e 2.1) 1.2 (0.7e 1.9)
Malformations of the eye, ear, neck, or face 0.9 (0.5e 1.7) 0.8 (0.4e 1.8) 1.1 (0.7e 1.9) 1.2 (0.7e 2.1)
Cardiac malformations 2.6 (2.3e 3) 1.6 (1.4e 1.9) 2.1 (1.9e 2.3) 1.5 (1.3e 1.7)Respiratory malformations 1.8 (1.2e 2.7) 1.5 (0.9e 2.4) 1.4 (0.9e 2) 1.3 (0.8e 2.1)
Cleft palate and lip 1.3 (0.7e 2.3) 1.3 (0.6e 2.6) 1.1 (0.7e 1.9) 1.1 (0.6e 2.1)
Gastrointestinal malformations 1.1 (0.8e 1.5) 1.0 (0.7e 1.5) 1.1 (0.9e 1.4) 1.0 (0.7e 1.3)
Genitourinary malformations 1.4 (1.1e 1.8) 1.1 (0.8e 1.5) 1.3 (1.1e 1.7) 1.1 (0.9e 1.5)
Musculoskeletal malformations 1.1 (0.9e 1.4) 0.9 (0.7e 1.2) 1.0 (0.8e 1.2) 0.8 (0.7e 1.1)
Other malformations 1.8 (1.3e 2.4) 1.6 (1.1e 2.3) 1.1 (0.8e 1.5) 1.0 (0.7e 1.4)
Odds ratios and 95% condence intervals are shown.
PS , propensity score.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
ajog.org Obstetrics Research
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
8/14
Second, our study examined a fullrange of organ-speci c congenital mal-formations in relation to hypertension,
nding that chronic hypertension isassociated most strongly with cardiac
malformations associated with treatedand untreated hypertension.
The association between chronic hy-pertension and malformations may be biologically plausible. Chronic hy-
mechanism may explain the link be-tween hyper tension and cardiacmalformations. 6
That being said, much remains to belearned about the biological mechanisms
TABLE 4Sensitivity and exploratory analyses
CharacteristicTreated chronic hypertensives,PS matched
Untreated chronic hypertensives,PS matched
Sensitivity analysis 1, excluding DM, GDM, insulin, anddiabetes medication
Composite congenital malformations 1.2 (1.0e 1.4) 1.2 (1.1e 1.3)
Cardiac malformations 1.5 (1.2e 1.8) 1.5 (1.2e 1.7)
Sensitivity analysis 2, excluding preterm deliveries
Composite congenital malformations 1.3 (1.1e 1.6) 1.1 (1.0e 1.3)Cardiac malformations 1.5 (1.2e 1.9) 1.1 (0.9e 1.4)
Sensitivity analysis 3 (all covariates dened based ontrimester 1)
Composite congenital malformations 1.3 (1.2e 1.6) 1.2 (0.9e 1.6)
Cardiac malformations 1.6 (1.3e 1.9) 1.3 (0.9e 1.9)
Sensitivity analysis 4 (outcome dened by a singlediagnostic code in the infant record)
Composite congenital malformations 1.2 (1.1e 1.3) 1.2 (1.1e 1.3)
Cardiac malformations 1.4 (1.3e 1.6) 1.5 (1.3e 1.6)
Exploratory analysis of specic cardiac malformations
Ventricular septal defect 1.4 (1.0e 2.0) 1.1 (0.8e 1.5)
Right ventricular outow obstruction 1.2 (0.2e 6.2) 1.3 (0.4e 3.5)
Single ventricle 3.0 (0.4e 21.3) 4.5 (0.8e 26.9)
Secundum atrial septal defect 1.5 (1.0e 2.4) 1.3 (0.9e 1.9)Conotruncal defect 1.7 (0.8e 3.5) 0.9 (0.4e 1.8)
Left ventricular outow obstruction 1.8 (0.8e 4.1) 1.1 (0.5e 2.2)
Odds ratios and 95% condence intervals shown.
DM , diabetes mellitus; GDM , gestational diabetes mellitus; PS , propensity score.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
Research Obstetrics ajog.org
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
9/14
that do not control for potential con-founding by indication must be inter-preted with caution. Future studiesexamining the role of speci c antihyper-tensive medications will need to carefully choose a comparator group of patientswith the same underlying condition to yield valid results.
The results of the study may informthe performance of antenatal screening tests. Guideline groups have advocatedfor the use of fetal echocardiography based on maternal comorbidities thatconfer increased ris k of congenital car-
Our results should be interpreted inthe context of limitations inherent in itsdesign. Although the MAX databasecontains detailed information on patientdemographics, outpatient medicationutilization, and inpatient and outpatientdiagnoses, it is health care utilizationdata that are not collected primarily forresearch purposes and thus lack somerelevant clinical details. For example, thepatients ’ blood pressures are not directly recorded in the MAX, and thus, we arereliant on physicians ’ diagnosis of chronic hypertension in de ning expo-
on 2 separate occasions. Such anapproach is expected to de ne bothexposure and outcome with high speci-
city. When the outcome is de ned withhigh speci city (even in the presence of limited sensitivity), results from anobservational study will yield unbiasedestimates of the relative risk of the as-sociation of the exposure with theoutcome. 28 Furthermore, any misclassi-
cation of the outcome in the study
would be expected to be nondifferentialin the groups compared. As a conse-quence, if the misclassi cation of outcome is present in our study, esti-mates of theassociation between chronichypertension and malformations would,if anything, be biased to the null.
In studying the association between achronic maternal condition and mal-formations, there is the possibility thatthe ndings may be subject to ascer-tainment bias if the infants of womenwith the condition are examined formalformations more carefully thanthose of unaffected women; however,this bias is unlikely to be playing a majorrole in the ndings of the present study
because chronic hypertension has nottraditionally been thought in the mal-formation to be a risk factor for mal-formations as well as the fact that many of the speci c cardiac malformationsassociated with hypertension ( Table 4)present a threat to the life of the infantand/or require surgical intervention.
The timing of the LMP is not recordeddirectly in the database but has to beestimated using an algorithm based ondiagnostic codes. Although the algo-rithm hasbeen demonstratedto performwell in claims data, misclassi cation of the LMP in some patients is possible.
FIGURE 2Confounder-outcome relative risk required to produce observed effects
AOR¼ 1.30 for treated chronic hypertension; AOR¼ 1.22 for untreated chronic hypertension. Theprevalence of the hypothetical confounder (C) in the unexposed population is 5%.AOR , adjusted odds ratio.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
ajog.org Obstetrics Research
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
10/14
study was conducted in a population of low-income Medicaid bene ciaries.Although the observed effect of chronichypertension on the risk of malforma-tions is very likely to be generalizable toother populations, even if this were notthe case, the results would be of interest,given the large proportion of births inthe United States covered by Medicaid.
Finally, we use propensity scorematching to control for confounders in
our analysis. The estimates of the effect of treated and untreated hypertensionon therisks of malformation should be inter-preted as generalizable to populationswith characteristics of the matched pop-ulations, as shown in Table 2.
Although we were careful to identify potential confounders of the associationbetween chronic hypertension and mal-formations using maternal inpatient andoutpatient diagnostic claims, medica-tions, and health care utilization vari-ables, it remains possible that residualbias is present because of unmeasured orunknown confounders. Our analysis of the potential effect of a hypotheticalconfounder suggests that for an unob-
servedconfounder to explain our results,it would need to have a strong associa-tion with the outcome and be highly prevalent in the exposed group.
Whereasthe presence of a singlehighly prevalent unmeasured confounder of strong effect is unlikely, given our longi-tudinal assessment of all women in thecohort from 3 months prior to theLMP through delivery, it cannot beexcluded that several unmeasured ornot perfectly measured confoundersmight together signi cantly attenuatethe observed associations. For example,although we accounted for confounding
residual confounding. Future work using other data sources will thus be needed tocon rm these results. That said, the im-plications of our results for the design of drug safety studies in pregnancy (need tocontrol for confounding by indicationbecause theconfounders measured in ourdata set are typical of those available indata setsusedtostudy drugsafety)andforclinical practice (need for close screening for malformation in women with hyper-
tension) remain, whether or not theobserved association is strictly causal.Our study also cannot directly address
whether treatment of chronic hyperten-sion in pregnancy will decrease the risk of malformations. However, if themechanism underlying the associationof chronic hypertension and malforma-tions is, in fact, uteroplacental insuf -ciency, it is unlikely that treatment willbe effective in doing so.
The risks of preeclampsia and smallfor gestational age associated withchronic hypertension, which may also besecondary to uteroplacental insuf -ciency, are not decreased thr ough the useof antihypertensive therapy. 29 Likewise,
although the estimate of risk of malfor-mations was similar for both treatedand untreated chronic hypertension,our study cannot exclude the possi-bility that certain antihypertensives areteratogenic. Future studies will need tofocus on evaluating the safety of partic-ular antihypertensives while carefully accounting for the confounders that areimportant to those agents.
Our ndings suggest that chronic hy-pertension,whether treatedor untreated,has an independent association with thedevelopment of major congenital mal-formations (particularly cardiac malfor-
confounding by indication. Clinically,the ndings suggest that hypertensivewomen may bene t from more intensivescreening for cardiac malformations inthe fetus/neonate. -
ACKNOWLEDGMENT
We thank Cora Allen-Coleman for her work as aresearch assistant on this project.
REFERENCES
1. Kuklina EV, Ayala C, Callaghan WM. Hyper-tensive disorders and severe obstetric morbidityin the United States. Obstet Gynecol 2009;113:1299-306 .2. Bateman BT, Bansil P, Hernandez-Diaz S,Mhyre JM, Callaghan WM, Kuklina EV. Preva-lence, trends, and outcomes of chronic hyper-tension: a nationwide sample of deliveryadmissions. Am J Obstet Gynecol 2012;206:134.e1-8 .3. Andrade SE, Raebel MA, Brown J, et al.Outpatient use of cardiovascular drugs duringpregnancy. Pharmacoepidemiol Drug Saf 2008;17:240-7 .4. Bateman BT, Hernandez-Diaz S,Huybrechts KF, Palmsten K, Mogun H,Ecker JL, Fischer MA. Patterns of outpatientantihypertensive medication use during preg-nancy in a medicaid population. Hypertension2012;60:913-20 .5. Xie RH, Guo Y, Krewski D, et al. Trends inusing beta-blockers and methyldopa for hyper-tensive disorders during pregnancy in a cana-dian population. Eur J Obstet Gynecol ReprodBiol 2013;171:281-5 .6. Caton AR, Bell EM, Druschel CM, et al. Anti-hypertensive medication use during pregnancyand the risk of cardiovascular malformations.Hypertension 2009;54:63-70 .7. YakoobMY,Bateman BT, HoE, etal. The risk
of congenital malformations associated withexposure to beta-blockers early in pregnancy: ameta-analysis. Hypertension 2013;62:375-81 .8. Lennestal R, Otterblad Olausson P, Kallen B.Maternal use of antihypertensive drugs in earlypregnancy and delivery outcome, notably thepresence of congenital heart defects in the in-fants Eur J Clin Pharmacol 2009;65:615 25
Research Obstetrics ajog.org
http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://www.ajog.org/http://www.ajog.org/http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref8http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref7http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref6http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref5http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref4http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref3http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref2http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1http://refhub.elsevier.com/S0002-9378(14)01016-3/sref1
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
11/14
and risk of malformations in offspring: a retro-spective cohort study. BMJ 2011;343:d5931 .13. Mitchell AA. Fetal risk from ace inhibitors inthe rst trimester. BMJ 2011;343:d6667 .14. Palmsten K, Huybrechts KF,Mogun H, et al.Harnessing the medicaid analytic extract (max)to evaluate medications in pregnancy: designconsiderations. PLoS One 2013;8:e67405 .15. Margulis AV, Setoguchi S, Mittleman MA,Glynn RJ, Dormuth CR, Hernandez-Diaz S. Al-gorithmsto estimate the beginningof pregnancyin administrative databases. Pharmacoepide-miol Drug Saf 2013;22:16-24 .16. Palmsten K, Huybrechts KF, Kowal MK,Mogun H, Hernández-Díaz S. Validity of maternal and infant outcomes within nationwidemedicaid data. Pharmacoepidemiol Drug Saf 2014;23:646-55 .17. Casson IF, Clarke CA, Howard CV, et al.Outcomes of pregnancy in insulin dependentdiabetic women: results of a ve year populationcohort study. BMJ 1997;315:275-8 .18. Allen VM, Armson BA, Wilson RD, et al. Teratogenicity associated with pre-existing and
gestational diabetes. J Obstet Gynaecol Can2007;29:927-44 .19. Hernandez-Diaz S, Schisterman EF,Hernan MA. The birth weight “ paradox ” uncov-ered? Am J Epidemiol 2006;164:1115-20 .20. Schneeweiss S. Sensitivity analysis andexternal adjustment for unmeasured confoundersin epidemiologic database studies of therapeutics.Pharmacoepidemiol Drug Saf 2006;15:291-303 .21. Rey E, Couturier A. The prognosis of preg-nancy in women with chronic hypertension. AmJ Obstet Gynecol 1994;171:410-6 .22. Sibai BM, Lindheimer M, Hauth J, et al. Risk factors for preeclampsia, abruptio placentae,and adverse neonatal outcomes among womenwith chronic hypertension. National institute of child healthandhumandevelopment network of maternal-fetal medicine units. N Engl J Med1998;339:667-71 .23. Allen VM, JosephK, MurphyKE, Magee LA,Ohlsson A. The effect of hypertensive disordersin pregnancy on small for gestational age andstillbirth: a population based study. BMC Preg-nancy Childbirth 2004;4:17 .
24. Sibai BM. Chronic hypertension in preg-nancy. Obstet Gynecol 2002;100:369-77 .25. Bateman BT, Simpson LL. Higher rate of stillbirth at the extremes of reproductive age: alarge nationwide sample of deliveries in theunited states. Am J Obstet Gynecol 2006;194:840-5 .26. Clark EB. Pathogenetic mechanisms of congenital cardiovascular malformations revis-ited. Semin Perinatol 1996;20:465-72 .27. Rychik J, Ayres N, Cuneo B, et al. AmericanSociety of Echocardiography guidelines andstandards for performance of the fetal echo-cardiogram. J Am Soc Echocardiogr 2004;17:803-10 .28. Schneeweiss S, Avorn J. A reviewof uses of health care utilization databases for epidemio-logic research on therapeutics. J Clin Epidemiol2005;58:323-37 .29. Abalos E, Duley L, Steyn DW, Henderson-Smart DJ. Antihypertensive drug therapy formild to moderate hypertension during preg-nancy. Cochrane Database Syst Rev 2007:CD002252 .
ajog.org Obstetrics Research
http://refhub.elsevier.com/S0002-9378(14)01016-3/sref12http://refhub.elsevier.com/S0002-9378(14)01016-3/sref12http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref24http://refhub.elsevier.com/S0002-9378(14)01016-3/sref24http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://www.ajog.org/http://www.ajog.org/http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref29http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref28http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref27http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref26http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref25http://refhub.elsevier.com/S0002-9378(14)01016-3/sref24http://refhub.elsevier.com/S0002-9378(14)01016-3/sref24http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref23http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref22http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref21http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref20http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref19http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref18http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref17http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref16http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref15http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref14http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref13http://refhub.elsevier.com/S0002-9378(14)01016-3/sref12http://refhub.elsevier.com/S0002-9378(14)01016-3/sref12
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
12/14
A PPENDIX
SUPPLEMENTARY TABLE 1Antihypertensive medicationsincluded in the analysis1. Diureticsa. Thiazides
BendroumethiazideBenzthiazideChlorothiazide
Chlorothiazide sodiumChlorthalidoneCyclothiazideHydrochlorothiazideHydroumethiazideIndapamideMethyclothiazideMetolazone
PolythiazideQuinethazoneTrichlormethiazide
b. Potassium-sparing agents Amiloride hydrochlorideSpironolactoneTriamterene
c. Acetazolamide Acetazolamide
2. Adrenergic inhibitorsa. Peripheral agents
Guanadrel sulfateGuanethidine sulfateReserpine
b. Central alpha-antagonistsClonidine hydrochlorideGuanabenz acetate
Guanfacine hydrochlorideMethyldopaMethyldopate hydrochloride
Phenoxybenzamine hydrochloride
Phentolamine hydrochlorideT l li h d hl id
SUPPLEMENTARY TABLE 1Antihypertensive medications
included in the analysis (continued) Carteolol hydrochlorideEsmolol hydrochlorideMetoprolol succinateMetoprolol tartrateNadololPenbutolol sulfatePindolol
Propranolol hydrochlorideSotalol hydrochlorideTimolol maleate
e. Combined alpha and beta blockersCarvedilolLabetalol hydrochloride
3. Direct vasodilatorsHydralazine hydrochloride
Minoxidil4. Calcium channel antagonistsa. Nondihydropyridines
Diltiazem hydrochlorideDiltiazem malateMibefradil dihydrochloride Verapamil hydrochloride
b. Dihydropyridines Amlodipine besylateBepridil hydrochlorideFelodipineIsradipineNicardipine hydrochlorideNifedipineNimodipineNisoldipine
5. ACE inhibitorsBenazepril hydrochlorideCaptoprilEnalapril maleateEnalaprilatEnalaprilat dihydrate
SUPPLEMENTARY TABLE 1Antihypertensive medications
included in the analysis (continued) Eprosartan mesylateIrbesartanLosartan potassiumOlmesartan medoxomilTelmisartan Valsartan
7. Combination drugs
a. Beta blockers and diureticsBendroumethiazide/nadololChlorthalidone/atenololHydrochlorothiazide/bisoprolol
fumarateHydrochlorothiazide/labetalol
hydrochlorideHydrochlorothiazide/metoprolol
tartrateHydrochlorothiazide/propranololHydrochlorothiazide/propranolol
hydrochlorideHydrochlorothiazide/timolol
b. ACE inhibitors and diureticsBenazepril hydrochloride/
hydrochlorothiazideCaptopril/hydrochlorothiazide
Enalapril maleate/ hydrochlorothiazideFosinopril sodium/
hydrochlorothiazideLisinopril/hydrochlorothiazideMoexipril hydrochloride/
hydrochlorothiazideQuinapril hydrochloride/
hydrochlorothiazide
c. Angiotensin II receptor antagonistsand diureticsCandesartan cilexetil/
hydrochlorothiazideIrbesartan/hydrochlorothiazideLosartan potassium/
hydrochlorothiazide
Research Obstetrics ajog.org
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
13/14
SUPPLEMENTARY TABLE 1Antihypertensive medications
included in the analysis (continued) e. Other combinations
Bendroumethiazide/potassiumchloride
Cryptenamine/methylclothiazideHydrochlorothiazide/spironolactoneSpironolactone/hydrochlorothiazideHydrochlorothiazide/triamterene
Hydrochlorothiazide/amiloridehydrochlorideClonidine hydrochloride/
chlorthalidoneDeserpidine/hydrochlorothiazideDeserpidine/methyclothiazideGuanethidine sulfate/
hydrochlorothiazideMethyldopa/chlorothiazide
Methyldopa/hydrochlorothiazideReserpine/benzthiazideReserpine/chlorothiazideReserpine/chlorthalidoneReserpine/hydrochlorothiazideReserpine/hydroumethiazideReserpine/methyclothiazideReserpine/polythiazideReserpine/quinethazoneReserpine/trichlormethiazideHydralazine hydrochloride/
hydrochlorothiazideHydralazine hydrochloride/reserpineHydralazine hydrochloride/reserpine/
hydrochlorothiazideHydralaz/reserpine/
hydrochlorothiazideHydralazine hydrochloride/
hydrochlorothiazidePrazosin hydrochloride/polythiazideMethylclothiazide/pargylineRauwola serpentina/
ajog.org Obstetrics Research
http://www.ajog.org/http://www.ajog.org/
-
8/18/2019 Chronic Hypertension in Pregnancy and the Risk of Congenital Malformations a Cohort Study
14/14
SUPPLEMENTARY TABLE 2Offspring with composite and organ-specic malformations in both the overall cohort and the propensity-score matched cohorts
Characteristic
Overall cohort PS matched PS matched
Without chronic
hypertension
Treated chronic
hypertensives
Untreated chronic
hypertensives
Without chronic
hypertension
Treated chronic
hypertensives
Without chronic
hypertension
Untreated chronic
hypertensivesTotal 858,337 8307 11,482 23,427 7809 34,434 11,478
Composite congenital malformations 29,934 (3.49) 491 (5.91) 581 (5.06) 1012 (4.32) 433 (5.54) 1442 (4.19) 581 (5.06)
Organ-specic malformation
Central nervous system malformations 1202 (0.14) 23 (0.28) 22 (0.19) 44 (0.19) 20 (0.26) 56 (0.16) 22 (0.19)
Malformations of the eye, ear,neck, or face
1044 (0.12) a 16 (0.14) 29 (0.12) a 41 (0.12) 16 (0.14)
Cardiac malformations 11,091 (1.29) 275 (3.31) 306 (2.67) 447 (1.91) 234 (3.0) 614 (1.78) 306 (2.67)Respiratory malformations 1403 (0.16) 24 (0.29) 26 (0.23) 49 (0.21) 24 (0.31) 58 (0.17) 26 (0.23)
Cleft palate and lip 943 (0.11) 12 (0.14) 14 (0.12) 24 (0.1) a 37 (0.11) 14 (0.12)
Gastrointestinal malformations 4065 (0.47) 43 (0.52) 60 (0.52) 113 (0.48) 39 (0.5) 188 (0.55) 60 (0.52)
Genitourinary malformations 4117 (0.48) 55 (0.66) 74 (0.64) 139 (0.59) 50 (0.64) 198 (0.58) 74 (0.64)
Musculoskeletal malformations 6542 (0.76) 69 (0.83) 85 (0.74) 207 (0.88) 62 (0.79) 304 (0.88) 85 (0.74)
Other malformations 2547 (0.3) 44 (0.53) 37 (0.32) 84 (0.36) 44 (0.56) 115 (0.33) 37 (0.32)
PS , propensity score.a Indicates cell size less than 11, which cannot be disclosed in accordance with the Data Use Agreement.
Bateman. Chronic hypertension and malformations. Am J Obstet Gynecol 2015.
R e s ea r ch O b s t e t r i c s
a j o g . or
g
3 3 7 . e 1 4
A m e r i c a n J o u r n a l o f O b s t e t r i c s & G y n e c o l o
g y M A R C H 2 0 1 5
http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/http://www.ajog.org/