Chronic Disease Registries: A Product Review€¦ · Chronic Disease Registries: A Product Review...
44
Chronic Disease Registries: A Product Review Prepared by NAS Consulting Services May 2004
Transcript of Chronic Disease Registries: A Product Review€¦ · Chronic Disease Registries: A Product Review...
C h ronic Disease Registries:A Product Review
Prepared by NAS Consulting ServicesMay 2004

The iHealth Re p o rts series focuses on the effective adoption of IT in healthc a re by analyzing the marketplace, inspiring innovation, and providing practical information on emerging technology tre n d s .
Related CHCF re p o rt s :
• Using Computerized Registries in Chronic Disease Ca re
• E-Disease Ma n a g e m e n t
• Examining Chronic Ca re in Ca l i f o rn i a’s Safety Ne t
• Availability and Quality of Medical Group Da t a
• Use and Adoption of Computer-based Patient Re c o rd s

Chronic DiseaseRegistries: A Product Review
Pre p a red for:
CALIFORNIA HEALTHCARE FOUNDATION
Pre p a red by :
NAS Consulting Se rv i c e s
Au t h o r s :
Jodi Simon, M.S. and Margie Powers, M.S.W., M.P. H .
May 2004

A c k n o w l e d g m e n t s
About the AuthorJodi Simon, M.S., formerly with NAS consulting, is an inde-pendent health care consultant specializing in informationtechnology and chronic disease management. Margie Powe r s ,M . S . W., M.P.H, formerly with NAS consulting, is an inde-pendent consultant specializing in the assessment, design andi m p rovement of chronic care delive ry systems. CHCF and theauthors would like to thank Michael Hindmarsh at theMacColl Institute for He a l t h c a re In n ovation, Group He a l t hC o o p e r a t i ve of Puget Sound and Jane Metzger at Fi r s tConsulting Group for their input and assistance.
About the FoundationThe Ca l i f o rnia He a l t h Ca re Fo u n d a t i o n, based in Oakland, is an independent philanthropy committed to improv i n gC a l i f o r n i a’s health care delive ry and financing systems. Fo r m e din 19 9 6, its goal is to ensure that all Californians have access toa f f o rdable, quality health care. For more information, visit usat w w w. c h c f . o r g
This re p o rt was produced under the direction of CHCF’sC h ronic Disease Care Program with support from the He a l t hInformation Technology gro u p. The Chronic Disease CareProgram seeks to improve the health of Californians by work-ing to assure those with chronic diseases re c e i ve care based onthe best scientific knowledge. Visit w w w. c h c f . o r g / p ro g r a m sfor more information.
ISBN 1-9 3 2 0 6 4- 5 8- 3
Copyright © 2004 California He a l t h C a re Fo u n d a t i o n

C o n t e n t s4 Executive Summary
6 I. Introduction to Chronic CarePurpose and Scope of Report
8 II. O v e rview of Computerized Disease R e g i s t r i e s
9 III. Considerations in Disease Registry S e l e c t i o nRegistry Ty p e s
Building a Custom Registry
Public Domain Software
Commercial Registry Software
13 I V. Detailed Product ProfilesPublic Domain Products
Commercial Software Products
Product Comparisons
3 7 Appendix A. Registry Product Contact Information
3 9 Appendix B. Report Methodology
4 0 Appendix C. Glossary
4 2 E n d n o t e s

CH RO N I C D I S E A S E S A R E P LAC I N G A G ROW I N Gb u rden on the health care system in the United States. As aresult, provider organizations are seeking new strategies fore f f e c t i vely managing these large and expensive populations.C o m p u t e r i zed disease registries are one tool being used to s u p p o rt care management efforts for groups of patients withc h ronic diseases. These tools capture and track key patientinformation to assist care team members in pro a c t i vely manag-ing patients. Sp e c i f i c a l l y, they prov i d e :
■ Printed patient re p o rts used at the point of care to commu-nicate condition-specific information and prompt physi-cians and their teams to deliver recommended care ;
■ Exception re p o rts to identify patients ove rdue for care ornot meeting management goals; and
■ Pro g ress re p o rts to provide information about how well individual providers and overall organizations aredoing in delivering recommended care to specific patientpopulations.
This re p o rt evaluates 16 computer re g i s t ry applications and isintended to assist physician and provider organizations intere s t-ed in purchasing a re g i s t ry product. The products are dividedinto two categories: public domain software and commerc i a ls o f t w a re. Public domain software is the most pre valent type ofre g i s t ry software in use today. The majority of these pro d u c t sa re developed by Quality Im p rovement Organizations (QIOs )in various states, with one of the most widely used pro d u c t sbeing the Diabetes El e c t ronic Management System (DEMS),and deriva t i ve products in the DEMS family. DEMS was ini-tially developed by the Washington State Diabetes Pre ve n t i o nand Control Program (funded by the Centers for Di s e a s eC o n t rol) and then adapted by the Bu reau of Pr i m a ry He a l t hC a re (BPHC) to be used by federally qualified communityhealth centers participating in the national Health Di s p a r i t i e sC o l l a b o r a t i ves across the country. The most beneficial attributeof the public domain products is the fact that they are free andh a ve been used in a variety of settings.
Fi ve commercial products are also profiled in this re p o rt. T h emajor advantages of the commercial software over the publicdomain tools are a more sophisticated and scalable arc h i t e c t u re ,tech support (e.g., upgrades and help desk), and more ro b u s t
Executive Summary
4 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

C h ronic Disease Registries: A Product Re v i e w | 5
functionality including patient education toolsand point-of-care tools such as messaging andreminders. A glossary that defines some of thetechnical terms used in the re p o rt can be foundon page 40.
The sixteen products we re evaluated along eightkey decision-making criteria: Patient vs. diseasefocus, ease of use, market penetration, customiz-a b i l i t y, ease of set up, import or interface capabil-i t y, scalability, and cost. Re g i s t ry selectiondepends upon which of these criteria are mostcritical to the organization. If upfro n t / p u rc h a s i n gcosts is the key consideration, two public pro d-ucts stand out—CDEMS, a more customizablevariation of the DEMS product and the Chro n i cDisease Management System (CDMS), a We b -based re g i s t ry tool that was developed by theMo u n t a i n - Pacific Quality Health Fo u n d a t i o n .For organizations able to make a more substantialm o n e t a ry investment, Pa t i e n t Planner byDo c Si t eS M rated highly on all criteria. In addition,the Delphi Diabetes Re g i s t ry rated high and isa p p ropriate for organizations seeking a pro d u c tspecifically tailored for diabetes.

I. Introduction to Chronic Care1
6 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
CH RO N I C C O N D I T I O N S S U C H A S D I A B E T E S,asthma, and coro n a ry art e ry disease are the major cause of ill-ness, disability, and death in the United States. In 2000, themedical cost of chronic disease amounted to 75 percent ofhealth care spending.2 In t e rest in a more systematic appro a c hto managing patients with chronic disease is being spurred by ag rowing awareness of the inefficiencies in delivering care topatients with a chronic disease. Ap p ropriate and timely carecan pre vent chronic disease altogether and delay or avoid manyof the complications associated with the diseases.
In Crossing the Quality Chasm, the Institute of Me d i c i n e(IOM) concluded, “The current delive ry system responds pri-marily to acute and urgent health care problems… Those withc h ronic conditions are better served by a systematic appro a c hthat emphasizes self-management, care planning with a multi-d i s c i p l i n a ry team, and ongoing assessment and follow - u p. ”3
The IOM also emphasized the importance of “good informa-tion about patients, their care, and outcomes in order toi m p rove outcomes.”
By tracking key patient information, a disease re g i s t ry helpsphysicians and other members of their team identify and re a c hout to patients who may have gaps in their care. It alsoreminds them to do the right things during patient visits.Paper registries have been used in the past to track import a n tinformation about conditions such as cancer. Computerize dsystems for managing the necessary patient information havethe advantage of quickly providing the information necessaryto support chronic care, including reminders during encoun-ters, lists of patients needing follow - u p, and re p o rts prov i d i n gfeedback to physicians about how well they are doing withtheir patients. Systems also provide feedback to patients abouth ow well they are self-managing their care .

Purpose and Scope of ReportThis re p o rt is intended to help physicians, med-ical groups, and other organizations consideringthe purchase of an electronic re g i s t ry application.The re p o rt provides an ove rv i ew of the types ofe l e c t ronic re g i s t ry products that are publicly andc o m m e rcially available and describes fifteen ofthose products in detail. The re p o rt outlines anumber of decision criteria that are important forp u rchasers to consider in choosing a product andp rovides details about which products are best forc e rtain types of organizations.
The focus of this re p o rt is stand-alone re g i s t rys o f t w a re products. While some electronic medicalre c o rds and practice management systems arecapable of supporting re g i s t ry functions, thosep roducts we re not re v i ewed for this re p o rt. Inaddition, while many organizations choose tobuild re g i s t ry software themselves, this type ofstrategy was not evaluated in depth.
Fi n a l l y, re g i s t ry software products typically donot have fully automated data integration capa-bilities, including the ability to normalize, inte-grate, and match data from disparate sourc e s .This product re v i ew does not evaluate supple-m e n t a ry softwaredatabases, patient matchings o f t w a re, and other interface technologies that a re necessary to support a fully automated disease re g i s t ry.
C h ronic Disease Registries: A Product Re v i e w | 7

8 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
A COMPUTERIZED DISEASE REGISTRY IS ONE TYPEof clinical information system that is effective in support i n go r g a n i zed care management. A re g i s t ry can assist physicians int h ree key processes for managing chronic disease:
■ Printed patient re p o rt s used at the point of care commu-nicate condition-specific information and prompt physi-cians and their teams to conduct appropriate assessmentsand deliver recommended care .
■ Re g i s t ry-generated exception re p o rt s identify patientswho have missed appointments, are ove rdue for care or arenot meeting management goals. Re p o rts provide informa-tion to aid in reaching patients (outreach) and helpingthem meet goals (compliance).
■ Pro g ress re p o rt s p rovide information about how we l lindividual care teams and overall provider organizationsa re doing in delivering recommended care to specificpatient populations.
■ Stratified population re p o rt s separate patients into va r i-ous categories of risk in order to target interventions at thepatients with the highest needs.
C o m p u t e r i zed registries generally re q u i re a database to storeintegrated patient information and a software application thatcan sort the information into different views and re p o rts, asdescribed above. One major drawback of current re g i s t ry soft-w a re is that most products do not have the capability to nor-m a l i ze, integrate, and match data from disparate electro n i cs o u rces. Instead, most re g i s t ry software manages electronic datathat has already been integrated, or re q u i res manual data entry.
Registries are different from electronic medical re c o rds (EMRs)in that they manage only selected information re l e vant to oneor more chronic diseases, rather than containing more compre-h e n s i ve information about patient problems, health historyand care. Fu rt h e r, the re g i s t ry is generally not the legal docu-mentation of care provided to the patient.
For more information on disease registries, see Us i n gC o m p u t e r i zed Registries in Chronic Disease Ca re. The re p o rtp rovides an ove rv i ew of the function and use of computerize ddisease registries and outlines issues for consideration inobtaining re g i s t ry software and integrating re g i s t ry pro d u c t sinto the routine work of the physician practice. It can be found at w w w. c h c f . o r g / t o p i c s / v i e w. c f m ? i t e m i d = 2 1 7 1 8 .
I I . O v e rview of Computerized Disease Registries

WH I C H TY PE O F R E G I S T RY S O F TWA R E TOimplement is a decision that must be informed by several factors. It is not uncommon for a provider organization toselect a re g i s t ry product and subsequently find that it is nota p p ropriate for their patient population or does not synchro-n i ze with their organization’s strategy or capabilities. This canresult in expensive and time-consuming re g i s t ry modificationsor may re q u i re discarding the re g i s t ry and implementinganother pro d u c t .
To pre vent poor decisions, organizations should care f u l l yweigh the following factors as they choose their re g i s t ry :
1 .O verall disease management strategy. A re g i s t ry is justone component of a compre h e n s i ve disease managements t r a t e g y. A systematic and compre h e n s i ve approach to dis-ease management includes a range of interventions, suchas case management, physician feedback, clinical informa-tion systems to track patient care, adoption of clinicalpractice guidelines, outreach to patients who need tocome in for care, and a focus on patient self-managementskills. Relying on a re g i s t ry to improve care withoutchanging care-management functions is unrealistic andmay lead to disappointment and frustration after re g i s t ryimplementation. The organization should also considerany long-range plans for technical expansion, such asplans to implement an EMR, and how the re g i s t ry wills y n c h ro n i ze with these efforts. For some organizations,registries may be considered a transitional technologyuntil they implement an EMR with full-re g i s t ry function-a l i t y. These organizations should choose the least-costlyoptions in registries with an eye tow a rd the future.
2 .Di rect vs. indirect costs. The direct, monetary costs ofthe re g i s t ry product are not necessarily the most signifi-cant costs associated with the product. Setting up andmanaging a re g i s t ry re q u i res a substantial labor effort thatcannot be minimized. Implementing the system itself willre q u i re technical and programming support, possibleh a rd w a re costs and training personnel how to utilize there g i s t ry. In addition, “s e l l i n g” the re g i s t ry to fre q u e n t l yindependent-minded physician users can be the mostl a b o r - i n t e n s i ve portion of implementation. Fi n a l l y,inputting data into the re g i s t ry will have va rying costs
I I I . Considerations in Disease Registry Selection
C h ronic Disease Registries: A Product Re v i e w | 9

Registry Ty p e sProvider organizations must weigh each of thesea p p roaches carefully when deciding which typeof software product to implement. Or g a n i z a t i o n smay choose to build their own registry, down-load public domain software, or purchase com-mercial registry software. A brief overview ofeach registry type follows; however, this productreview will focus on facilitating the choicebetween public domain and commercial registrysoftware products.
Building a Custom Registry Many provider organizations choose to buildtheir own re g i s t ry rather than use existing soft-w a re tools. These “home grow n” registries take avariety of forms. Some groups create re g i s t r i e susing Mi c rosoft Access or Mi c rosoft Excel, whileothers utilize their internal data warehouses toc reate a re g i s t ry.
Major Benefits:■ Organizational control—The builder re t a i n s
complete control over the re g i s t ry’s function-ality and data. T h e re is also no risk associat-ed with a potentially unreliable or unre s p o n-s i ve external ve n d o r.
■ Product flexibility—When the organizationis ready to change re g i s t ry products, dataf rom these solutions can be easily import e dinto many existing re g i s t ry software pro d u c t sor into an EMR.
■ C o s t — For those organizations with limitedre s o u rces, building a custom re g i s t ry cana l l ow for tighter control of up-front costs.Organizations can be selective about func-tionality based on internal deve l o p m e n tre s o u rces available.
10 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
depending on whether it is manually entere dby staff or automatically dow n l o a d e dt h rough data stre a m s .
3 .Data management. One of the most signifi-cant efforts needed to maintain a re g i s t ry iscollecting, integrating and managing data.Provider organizations must decide whichdata sets will be incorporated into the re g-i s t ry (i.e., laboratory, pharmacy, encounters),and how the data will actually enter the re g-i s t ry. If data is automatically dow n l o a d e d ,relationships must be formed and cultiva t e dwith outside data sources such as laborato-ries. If data is manually entered, staff mustbe identified who will consistently enter datainto the re g i s t ry. For registries to be used in am e a n i n gful way, data quality is of utmosti m p o rtance. Providers expect data to be cur-rent, accurate, and useful, and will oftenreject re p o rts that are perc e i ved to be basedon inaccurate data.
4 .Re t u rn on investment (RO I ) . A care f u laccounting of project costs is import a n tb e f o re acquiring any software, be it publicdomain or commercial. Costs often ove r-looked are those related to establishing inter-faces with external systems, as well as main-tenance, data entry, and the necessary inve s t-ment in implementation, primarily trainingand process change. For clinical systems suchas chronic disease registries, there are rare l yenough financial benefits to offset all thecosts. California’s “Pay for Pe rf o r m a n c e” ini-t i a t i ve may provide an opportunity to re c o u psome of the investment; howe ve r, factoringthis into the value proposition re q u i res infor-mation about numbers of patients and anestimate of potential incentive payments.

C h ronic Disease Registries: A Product Re v i e w | 11
Major Obstacles:■ Internal technical capacity—The builder is
constrained in upgrading the product by thea vailability and skill of internal technicalre s o u rces. For example, organizations thatchoose to increase the number of chro n i cconditions managed with registries may findthe project re q u i res substantial internal infor-mation technology (IT) re s o u rc e s .
■ So f t w a re limitations—The typical solutionrelies on a Mi c rosoft Access database andeither addresses one chronic condition ormultiple conditions in separate registries. Ittypically includes only a small number ofs t o red queries available to generate re p o rt s .
■ Duplication of effort — Organizations maybe trying to solve data management chal-lenges that have already been addressed ands o l ved by others.
■ Data security—Re q u i res local managementof data access and mechanism for re g u l a rback up.
■ Ti m e — De velopment time will prolong thetime to implementation.
Public Domain SoftwarePublic domain software—which is available foruse by the general public without licensing orfees—is the most pre valent type of re g i s t ry soft-w a re in use today. The majority of the pro d u c t swe re developed by Quality Im p rove m e n tOrganizations (QIOs) in various states. One ofthe earliest products, the Diabetes El e c t ro n i cManagement System (DEMS), was developed bythe CDC-funded Washington State Di a b e t e sPre vention and Control Program. This pro d u c t’ssuccess quickly spread to other organizations andQ I Os, who created numerous variations of theoriginal product.
The public domain tools are primarily simples o f t w a re programs based on Mi c rosoft Ac c e s s .The tools usually do not have sophisticated arc h i-t e c t u re or in-depth functionality.
Major Benefits:■ Cost—The greatest advantage of the public
domain tools is that they are free. Many canbe downloaded from public Web sites.
■ St r a i g h t f o rw a rd technology—The tools arere l a t i vely simple to use and do not re q u i re asignificant information technology infra-s t ru c t u re. Limited support is needed,although many QIOs offer training and sup-p o rt for their software in their own state.
■ Community support — Nu m e rous chro n i cdisease collaboratives utilize various publicdomain tools. Pa rticipation in the collabora-t i ve provides users with training and otherre g i s t ry support. The DEMS Web site alsohas an online community for support.
■ Product testing—Many of these tools havebeen thoroughly tested in a provider organi-zation setting. The feedback from theseimplementations has resulted in pro d u c t swith few bugs and the re g i s t ry containsmany of the features found to be most criti-cal to provider organizations.
Major Obstacles:■ Manual data entry — Few public domain
p roducts have real-time interfaces to lab orencounter systems and there f o re have as t rong reliance on manual data entry. T h eability to import data electronically on aperiodic basis is also limited.
■ S c a l a b i l i t y — Many of the public domaintools are Mi c rosoft Access-based, and, there-f o re, are limited to 10 concurrent users. T h i sdoes not apply to the Web-based publicdomain tools.

■ Fl e x i b i l i t y — Some public domain pro d u c t sa l l ow for ve ry limited customization of dis-ease management guideline parameters andp re - p rogrammed re p o rts
■ Limited support — Many products have beend e veloped for specific users and, while ava i l-able in public domain, support is usuallylimited to these target organizations of thed e velopers.
Commercial Registry SoftwareA small number of vendors sell private, stand-alone re g i s t ry software. Fo r - p rofit entities selltheir applications to provider organizations on aper-user or per-patient basis.
Major Benefits:■ S c a l a b i l i t y — C o m m e rcial software often has
a more sophisticated and scalable arc h i t e c-t u re than the public domain programs. Alarge number of users can enter or view datasimultaneously and the databases are opti-m i zed for vast amounts of data.
■ Enhanced functionality—These pro d u c t stypically have robust functionality, includingpatient education tools and point of caretools such as messaging or reminders, as we l las flexibility to customize guideline parame-ters, data sets to be tracked, and re p o rts.
■ Technical sophistication—Some vendors areequipped to perform services such as build-ing data interfaces and may be more likely tod e velop Web-based products in the future .
Major Obstacles:■ Cost—While the cost of the products va r i e s
considerably and the companies use a va r i e t yof pricing models, costs range from $36 perpatient per year to $600 per individual userper ye a r, which may be pro h i b i t i ve for someo r g a n i z a t i o n s .
■ Data ow n e r s h i p — Some commercial compa-nies may house the data in their own data-base or serve r, with the provider group possi-bly having limited access to ove rv i ews of thedata.
■ Se c u r i t y — For some providers, it is impor-tant to retain all patient data in a databaseunder local management. This may also raiseconcerns about security, priva c y, and otherH I PAA issues.
■ Vendor stability—There is also real concernabout the possible long-term financial stabili-ty of some vendors and their products, making it difficult to predict their futurea vailability for support, upgrades, and m o d i f i c a t i o n s .
■ Lack of testing—Commercial solutions haveusually only been implemented in a handfulof organizations, so have not yet been exten-s i vely market tested.
12 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
THIS GUIDE EVALUATES 16 REGISTRY PRODUCTS,which can be divided into two categories: public domain soft-w a re and commercial software. Each software product re v i ewe db e l ow includes an ove rv i ew of functionality, strengths andweaknesses, and cost. An ove rv i ew of the public domain soft-w a re functionality can be found at Table 2, with commerc i a ls o f t w a re functionality summarized in Table 3.
Public Domain Products
1. DEMS Product FamilyO ve rv i e w : The original Diabetes El e c t ronic Ma n a g e m e n tSystem (DEMS) product was developed in 1999 by theWashington State Diabetes Pre vention and Contro lProgram. A straightforw a rd, Mi c rosoft Access-based tool fortracking and re p o rting on patients with diabetes, the tool atone time was being used by 65- 75 clinics in Wa s h i n g t o nState and had over 13,000 users.
The success of DEMS resulted in additional QIOs deve l o p i n gtheir own re g i s t ry software for other states and gove r n m e n torganizations. DEMS is now being phased out because a n ew version with greater flexibility and functionality has beend e veloped: the Chronic Disease El e c t ronic Ma n a g e m e n tSystems (CDEMS) product. Many created variations of theoriginal DEMS software and are actively promoting and sup-p o rting them. An ove r a rching summary of the DEMS pro d u c tfamily is provided below, followed by brief descriptions of thep roduct variations. See Table 1 for a comparison of all theDEMS products.
Fu n c t i o n a l i t y :■ Patient visit note form (See sample form at Fi g u re 1)—
Used to view and enter data for a given patient. This formcan be printed and filed in the chart and accessed duringpatient encounters. Di f f e rent layouts are available. Types ofinformation contained on the form are :
• De m o g r a p h i c s• Encounter information• C o n d i t i o n s• Se rv i c e s• L a b s• Me d i c a t i o n s• Patient handout information• Custom (free text)
I V. Detailed Product Profiles
C h ronic Disease Registries: A Product Re v i e w | 13

14 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Figure 1. DEMS Patient Visit Note

■ Re p o rt i n g — St a n d a rd re p o rts are available atboth a provider and clinic level. Us e r sk n owledgeable in Mi c rosoft Access can writetheir own queries to create additionalre p o rt s .
■ Manual data entry — Re q u i red in mostDEMS product family implementations.Data entry can be performed by anyone withaccess to the database—the physician, anoth-er care prov i d e r, or front office staff. Ro u g hestimates of data entry times are thre e - a n d - a -half minutes to enter a new patient and oneminute to enter data from a follow-up visitfor an existing patient.4
■ Im p o rt capability—Processes for import i n glab data have been set up with some of themajor labs in Washington State (LabCorp,D y n a c a re, Pathology Associates Me d i c a lLaboratories, and Qu e s t ) .5 Users outside of Washington State may benefit from thelessons learned in these implementations.
St re n g t h s : The DEMS product family can bean appropriate option for an organization withlimited technical re s o u rces to get started. Itoffers a simple, clean interface, re q u i res littleor no training and can be installed in a singled a y. The product has been extensively testedin a provider organization setting and re g u l a r-ly refined over a thre e - year period. The patientvisit note is a key asset of the product as itp rovides critical summary information for useat the point of care, as well as longitudinalgraphs of labs and vitals.
We a k n e s s e s : Despite its success, the DEMSp roduct family has several limitations. So m eregistries can only be used for a single condi-tion and only a predefined set of informationcan be captured. Re p o rting capability is limit-ed, particularly for re p o rts of historical data.Without technical skill or advanced know l-edge of Mi c rosoft Access, the user cannot addn ew fields or modify re p o rts. In addition, aswith all Mi c rosoft Access-based solutions, thetool will not scale to serve a large number of
users. Ten concurrent users entering data is thelimit in Mi c rosoft Access. As mentioneda b ove, the need to manually enter data intothe re g i s t ry, there by increasing staff time andthe chance of erro r, is another limitation ofDEMS pro d u c t s .
C o s t : DEMS and CDEMS are free publicdomain software. The Washington St a t eDiabetes Pre vention and Control Pro g r a moffers limited support to organizations outsidethe state.
Noted below are the primary differences betwe e nDEMS and CDEMS, as well as subsequent ve r-sions developed by other entities.
CDEMS (Chronic Disease El e c t ro n i cManagement Sy s t e m s )■ Condition tracking—Users can choose
which conditions to track and what va r i a b l e sa re of interest for each condition. The usercan also create and edit dro p - d own lists forfaster data entry. These customizations canbe accomplished through user-friendly wiz-a rd s .
■ Re p o rt i n g — Two types of standards re p o rt sa re available: In t e rvention re p o rts that con-tain lists of patients with certain characteris-tics or in need of services and summaryre p o rts of clinic statistics. Su m m a ry re p o rt sa re generated using a template in which theuser can choose the population and parame-ters of interest. CDEMS also has a re p o rtw i z a rd that allows the design of customq u e r i e s .
■ Web forum—This discussion board prov i d e sthe opportunity for users to pose questions,s h a re solutions, and discuss issues relating tothe DEMS and CDEMS programs.
CVDEMS (Ca rd i ovascular/Diabetes El e c t ro n i cManagement Sy s t e m )■ Condition tracking—Ability to track card i o-
vascular disease as well as diabetes.
C h ronic Disease Registries: A Product Re v i e w | 15

■ Im p o rt capability—Data can be import e df rom DEMS, but the product does not havethe capability to import lab or other data.
■ Community support — Promoted by theBu reau of Pr i m a ry Health Care for use byorganizations participating in their chro n i cdisease collaboratives. Howe ve r, BPHC tech-nical support of updating/debugging thisp roduct has ended, in favor of the new,i m p roved BPHC re g i s t ry pro g r a m — t h ePatient El e c t ronic Care System, or PE C S .
DEMS Lite (developed by the New Me x i c oMedical Review As s o c i a t i o n )■ In t e rface—A more streamlined version of
DEMS containing only two-thirds of thefields in the original product. The elimina-tion of these fields has resulted in a simpli-fied interface.
■ Re p o rt i n g — Addition of over 20 standardre p o rts.
OR-DEMS (developed by Ore g o n’s QIO,O M P RO )■ Patient visit note—Enhanced ve r s i o n
includes availability in English and Sp a n i s h ,an upgraded provider version with color-coded “g r a d e s” for lab results and due datesand diabetes guidelines.
■ Su p p o rt — O M P RO provides support onlyto organizations participating in the Ore g o nDiabetes Collaborative.
PHEMS (Pre ve n t i ve Health El e c t ro n i cManagement System by the Missouri PRO )■ Pre ve n t i ve serv i c e s — Expanded ability to
track pre ve n t i ve serv i c e s .
■ Automated back-up/re s t o re utility.
■ Medication dosages and frequency tracking.
■ Re p o rt i n g — Includes twenty standardre p o rts, all at a clinic or population leve l .Se veral new re p o rts added and existingre p o rts updated with new data fields.
16 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Table 1. Summary of the DEMS Family of Products
Product Conditions Base Product Key Differences
DEMS Diabetes Original product N/A
CDEMS Can be customized for DEMS Ability to customize for any condition;any condition enhanced reporting capability.
CVDEMS Diabetes; cardiovascular disease DEMS Ability to track cardiovascular disease.
DEMS Lite Diabetes; immunizations DEMS Simplified version of DEMS. One-thirdfewer data capture fields. Simpler interface. Additional standardized reports. New graph on patient visit summary.
OR-DEMS Diabetes DEMS Added a visit summary for the patient (available in English and Spanish).
PHEMS Diabetes; cardiovascular disease CVDEMS Added a prevention tracking component; added an automated Backup/Restore utility; minor data field additions (dosage and f requencies of medications, Mi c roalbuminaria test); several new reports added and existing reports updated with new data fields.

2. Adult Preventive Health ServicesSoftware (APHS)
O ve rview: A PHS is a Mi c rosoft Ac c e s s - b a s e dre g i s t ry tool for tracking pre ve n t i ve serv i c e sfor adults, with additional modules specific tow o m e n’s health and diabetes. It was deve l o p e dby Qualis, Id a h o’s QIO.
Fu n c t i o n a l i t y :■ Patient data—Patient demographic informa-
tion, patient history, pre ve n t i ve services, gen-eral screening tests and immunizations, andall the major diabetes services can be trackedfor a given patient.
■ Clinical breast/mammogram case manage-m e n t — Tracks the date and results of the lastexam and mammogram, follow up steps,p re f e r red frequency of service, and the dateof the next service. The pap case manage-ment component captures similar informa-tion for pelvic exams and pap smears.
■ Decision support — Embedded guidelinessuggest service frequency based on thep a t i e n t’s age and gender. Alerts are also pro-vided if the user adds a service that may notbe necessary.
■ Patient information pro f i l e — Su m m a r i zes thep a t i e n t’s history, demographics, and serv i c e sneeded. A graphing capability allows the userto generate graphs for viewing lab or vitalm e a s u rements over time.
■ Re p o rting—A number of standard re p o rt scan be run at a provider or facility leve l .Patient information and history can bei m p o rted from a comma delimited text file,if rigid data format re q u i rements are met.
St re n g t h s : A PHS’ strength lies in its ability toc a p t u re in-depth information about pre ve n t i ves e rvices. Pa rticularly detailed information canbe captured for mammograms and pap smearsif necessary. The basic embedded guidelinesa re also valuable.
We a k n e s s e s : This product does not offer theuser great flexibility in customizing the systemto meet local needs. Guidelines can be ove r-ridden but not changed at the organizationall e vel. Modifications or customizations cannotbe augmented without advanced knowledge ofMi c rosoft Access. As with many of theDEMS-like products, import capability is lim-ited and may result in most implementationsrelying primarily on manual data entry. Inaddition, as with all Mi c rosoft Ac c e s s - b a s e dsolutions, the tool will not scale to large num-ber of users.
C o s t : A PHS is free public domain softwarea vailable through Qualis Health. While there g i s t ry is still in use at locations inWashington and Idaho, Qualis Health is nolonger actively re c ruiting new users for thes o f t w a re .
3. Chronic Disease Management System(CDMS)
O ve rv i e w : CDMS is a Web-based re g i s t ry toolthat was developed by the Mo u n t a i n - Pa c i f i cQuality Health Foundation (Helena, MT) .CDMS can be customized for managing pop-ulations with any condition or for trackingp re ve n t i ve services. The Mo u n t a i n - Pa c i f i cQIO hosts the data.
Fu n c t i o n a l i t y :■ Patient profile/patient history — In f o r m a t i o n
on chronic diseases, current medications,d rug sensitivities, drug allergies, clinicalexams, and lab data. The patient history con-tains graphs of clinical exam results ove rt i m e .
■ Decision support — Embedded guidelines fora variety of chronic diseases (diabetes, atrialfibrillation, heart failure, coro n a ry art e ry dis-ease, hyperlipidimia, depression, asthma,o s t e o p o rosis, and pre ve n t i ve services). Pa t i e n tdue dates for tests and services are calculatedbased on these guidelines. Providers can
C h ronic Disease Registries: A Product Re v i e w | 17

print a list of patients ove rdue for interve n-tions or access a calendar view of due datesfor all patients. Providers also have the abilityto modify any of the guidelines for a give npatient or their entire panels.
■ Re p o rt i n g — Includes re p o rts comparingp roviders to each other and to national de-identified data (e.g., health information thathas been stripped of elements that couldidentify the individual and a re p o rt thattracks the behavioral goals and other indica-tors re q u i red by the American Di a b e t e sA s s o c i a t i o n’s Education Recognition pro-gram (the ADA Education Re c o g n i t i o nProgram assesses whether applicants meet theNational St a n d a rds for Diabetes Se l f -Management Education Programs and thenendorses those programs). CDMS also has ageneric re p o rting engine in which users with-out technical skill may define new customre p o rts by selecting population and indica-tors of intere s t .
■ Im p o rt capability—Able to import dataf rom a variety of billing systems (Me d i t e c h ,IDX, Sm a rt Practice, Medical Ma n a g e r,Medical ABC). The process entails ru n n i n g“ i m p o rt agents” that extract the data fro mthe billing systems in the appropriate formatand import them into CDMS. Auto data-population function can also be perf o r m e dfor select formats.
■ Medicaid call center—Telephonic outre a c hcapability for Medicaid patients with dia-betes, congestive heart failure, and asthma.Call center coordinators create clinical assessments during telephone outreach withp a t i e n t s .
St rengths: The scalable, Web-based platformp rovides considerable advantages over otherp roducts. Web-based access gives users theability to access information from any facility
and eliminates problems associated with con-necting multiple clinics. The ability to trackmultiple conditions in a single product is anadditional strength. Embedded guidelines arealso valuable. Fi n a l l y, the product has stro n gre p o rting capabilities including a compre h e n-s i ve set of standard re p o rts and a genericre p o rting engine.
We a k n e s s e s : The robust functionality ofCDMS results in greater complexity in settingup and using the system, as well as gre a t e rtraining needs.
C o s t : CDMS is free public domain softwarebut currently only available in the follow i n gstates: Montana, Wyoming, Hawaii, In d i a n a ,Ke n t u c k y, and Rhode Island.
4. Patient Care Management System O ve rv i e w : The Patient Care Ma n a g e m e n tSystem is a Mi c rosoft Access-based diabetesre g i s t ry tool developed by Me t a s t a r, In c . ,Wi s c o n s i n’s QIO.
Fu n c t i o n a l i t y :■ Diabetes re g i s t ry — Provides the ability to
track diabetes provider visits, diabetes labw o rk, and eye and foot exams.
■ American Diabetes Association re c o g n i-t i o n — Adds to the diabetes re g i s t ry the abili-ty to track educational visits and self-man-agement goals.
■ Pre ve n t i ve serv i c e s — Tracks vital signs, pre-ve n t i ve labs, immunizations, and other pre-ve n t i ve serv i c e s .
■ Patient visit note—A one-page summary ofclinical and demographic information, forthe prov i d e r.
■ Re p o rting—A variety of population-leve ls t a n d a rd re p o rts are available along with alimited number of provider and patient spe-
18 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

ing and follow - u p, and depression. T h e re arealso some elements to support HIV care andp re vention. It was developed by The AristosGro u p, and until recently was being usede xc l u s i vely by the Bu reau of Pr i m a ry He a l t hCare collaboratives. It will be available com-mercially under the PECSYS name on March31, 2004 (see the PECSYS product descrip-tion in the Commercial Products section onpage 27).
6. STEPS Electronic Collection andAnalysis Tool (SECAT)
O ve rview: S E C AT is a Mi c rosoft Ac c e s s - b a s e dre g i s t ry tool for tracking pre ve n t i ve serv i c e sand diabetes indicators. It was developed bythe Iowa Foundation for Medical Care andthe Illinois Foundation for Quality He a l t hC a re.
Fu n c t i o n a l i t y :■ Diabetes data collection tool and pre ve n t i ve
c a re data collection tool—Used for datae n t ry and maintenance.
■ S E C AT analysis tool—Case summaries of allre l e vant patient data, flow sheets show i n grecent information, and indicator re p o rts dis-playing trends. Be n c h m a rk re p o rts for dia-betes indicators show clinic performance re l-a t i ve to national benchmarks in a bar graphformat. Pe rformance re p o rts show clinic-leve la g g regate statistics re l a t i ve to benchmarks ina table format.
■ Data query tool—Enables the generation ofc u s t o m i zed lists of patients based on user-defined criteria.
■ Patient tracking tool—Used to pro d u c epatient-specific or generic notification lettersand mailing labels.
■ Assignment of user rights—Levels of userrights include system administration, datae n t ry, and viewing data only.
C h ronic Disease Registries: A Product Re v i e w | 19
cific re p o rts. The re g i s t ry also contains theability to generate reminder letters forpatients who have not had a recent visit.
■ Im p o rt capability—Demographic and labdata can be imported from a comma-delim-ited text file if rigid data format re q u i re m e n t sa re met.
St rengths: Like the DEMS products, thes t rength of this tool lies in its simplicity. It canbe rapidly implemented and offers a straight-f o rw a rd user interface. The ability to track thedata re q u i red for the ADA Ed u c a t i o nRecognition program is an additionals t re n g t h .
We a k n e s s e s : One weakness of the product isthat it can only be used for a single condi-tion—diabetes—and only a predefined set ofinformation can be captured. Without techni-cal skill or advanced knowledge of Mi c ro s o f tAccess, the user cannot add new fields ormodify re p o rts. The import capability is ve rylimited and may result in most implementa-tions relying on manual data entry. In addi-tion, as with all Mi c rosoft Access-based solu-tions, the tool will not scale to large numberof users. As mentioned above, the need tomanually enter data into the re g i s t ry, there byi n c reasing staff time and the chance of erro r, isanother limitation of PCMS.
C o s t : The Patient Care Management System isf ree public domain software and can be dow n-loaded from www. m e t a s t a r. c o m / p ro f e s s i o n a l /p c m _ f o r m _ x p. a s p. Me t a Star cannot offer s u p p o rt to organizations outside the state ofWisconsin.
5. Patient Electronic Care System (PECS2) O ve rv i e w : PECS2 is an n-tiered SQL serve r -based re g i s t ry product that can be used totrack clinical data for patients with any chro n-ic disease and is currently tailored for diabetes,asthma, card i ovascular disease, cancer scre e n-

■ Cu s t o m i z a t i o n — Administrator can add upto six new fields to the diabetes tool and asmany as 10 to the pre ve n t i ve care tool.
■ Im p o rt capability—Data can be uploadedonly if rigid data format re q u i rements aremet and a consistent set of patient identifiersis used.
St rengths: S E C AT is a simple tool that hasbeen well tested within the states of Il l i n o i sand Iowa. It has been refined numerous timessince its initial release in 2001 based on feed-back from over 75 implementations. It ss t rengths include some ability to customizedata fields, fairly robust re p o rting and query-ing capability, and the ability to track data forthe ADA Education Recognition.
We a k n e s s e s : One drawback of the system is thefact that it is limited to diabetes and pre ve n-t i ve services. While indicators within thesetopic areas can be added, the system cannot bec u s t o m i zed to track patients with other condi-tions or, for that matter, multiple conditionsof a patient with diabetes. A second we a k n e s sof the program is its limited data import capa-bilities. In addition, as with all Mi c ro s o f tAccess-based solutions, the tool will not scaleto large number of users.
C o s t: SECAT is free public domain software .Limited support is available for organizationsoutside the states of Illinois or Iowa.
20 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

Table 2. Public Domain Registry Software—Functionality Overview
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
Adult Pre ve n t i ve Health Se rvices So f t w a re (APH S )
C h ronic Disease El e c t ronic Management System (CDEMS)
C h ronic Disease Management System (CDMS)
Ca rd i ovascular and Diabetes El e c t ro n i cManagement System ( C V D E M S )
C h ronic Disease Registries: A Product Re v i e w | 21
Pre ve n t i ve s e rv i c e s *
Can be cus-t o m i zed for any condition
Can be cus-t o m i zed forany condition
Diabetes; c a rd i ova s c u l a rd i s e a s e
Client serve rs o f t w a re (MSAccess based**);database can bes t o red on a s e rve r
Client serve rs o f t w a re (MSAccess based);database can bes t o red on a PCor local networks e rve r
Web-based; datais hosted by theMountain QIO
Client serve rs o f t w a re (MSAccess based);database can bes t o red on a s e rve r
N / A
• No secure Web access
• Visit notes,e xc e p t i o nre p o rts containvisible patienti d e n t i f i e r s
• Access hasn a t i ve tiere dsecurity system,plus networks e c u r i t ys c h e m e .
N / A
N / A
N / A
• Users cane x p o rt any datato Wo rd, Exc e lor statisticalpackages suchas SAS or St a t a
• Data ow n e r-ship re s i d e swith clinic
• Less than 60seconds inputtime perp a t i e n t
N / A
N / A
• Patient s u m m a ry forc l i n i c i a n * * *
• Graphs forpatient of labvalues over t i m e
• Patient s u m m a ry forclinician withclinical g u i d e l i n e s
• Patient s u m m a ry forc l i n i c i a n
• C a re plannertool that con-tains calendarv i ew of whenpatients are duefor serv i c e s
• Pro g ress No t e swith automatedt e m p l a t e s
• e Prescribe function with digitala u t h e n t i c a t i o n
• Patient summa-ry for clinic;clinician; allp a t i e n t s
• Pa t i e n tEn c o u n t e rNote includesgraphs forpatient ove rt i m e
• Lists of patients in need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Patient datagraph for takehome use ore d u c a t i o n a ltalking point
• Lists of patientsin need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patientsin need of s e rv i c e s
• Reminder l e t t e r s
• Patient carep l a n
• Se l f - m a n a g e-ment and RN-case manage-ment tools fordiabetes, con-g e s t i ve heartf a i l u re and a s t h m a
• Lists of patientsin need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
O ver 25 standardre p o rts includings t a n d a rd s - b a s e d(HEDIS, DQIP,BCCP) popula-tion level re p o rt s .Additional queriescan be written ifusers have k n owledge of MS Ac c e s s .
Set of standardre p o rts; ability togenerate customstatistical summa-ry re p o rts. Nop ro g r a m m i n gk n ow l e d g ere q u i re d .
Set of standardre p o rts; re p o rt i n gtool that allow sfor user-definedqueries. No pro-gramming know l-edge re q u i re d .Can also generatere p o rts comparingphysicians to eachother and tonational de-iden-tified data.In t e rvention and Chro n i cC o n d i t i o nRe p o rt s .
Set of standardre p o rts plus addi-tional queries canbe written if usersh a ve know l e d g eof MS Ac c e s s .

Diabetes El e c t ronic Management System (DEMS)
Diabetes El e c t ronic Management System Lite (DEMS Lite)
Oregon Diabetes El e c t ronic Management System ( O R - D E M S )
Patient Ca re Management Sy s t e m
22 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Di a b e t e s
Di a b e t e s ;i m m u n i z a t i o n s ;c a rd i ova s c u l a r
Di a b e t e s
Diabetes; p re ve n t i ve s e rv i c e s
Client serve rs o f t w a re (MSAccess based);database can bes t o red on a PCor local networks e rver; maximum10 concurre n tu s e r s .
Client serve rs o f t w a re (MSAccess based);database can bes t o red on a PCor network / s e rv-er; no limitationon number ofu s e r s .
Client serversoftware (MSAccess based);database can bestored on a PCor local server.
Client serversoftware (MSAccess based);database can bestored on a PCor network;maximum 10concurrent users
• No secure Web access
• Visit notes,e xc e p t i o nre p o rts containvisible patienti d e n t i f i e r s
• Access hasn a t i ve tiere dsecurity system,plus networks e c u r i t ys c h e m e .
• Web access p o s s i b l e
• Visit notes contain visiblepatient i d e n t i f i e r s
• Pa s s w o rd pro-tected or net-w o rk securityre s t r i c t i o n s .
• No secure Web access
• Patient identi-fiers visible
• Access to datac o n t rolled byp rov i d e r.
• Users cane x p o rt any datato Wo rd, Exc e lor statisticalpackages suchas SAS or St a t a
• Data ow n e r-ship re s i d e swith clinic
• Less than 60seconds inputtime perp a t i e n t
• Users cane x p o rt any datato Wo rd, Exc e lor statisticalpackages suchas SAS or St a t a
• Data ow n e r-ship re s i d e swith re g i s t ryu s e r s / m a n a g e r
• Data inputtime is 7-10minutes forn ew patient; 3-5 minutes for existingp a t i e n t .
• Noe x p o rt / i m p o rtc a p a b i l i t y
• Data ow n e r-ship re s i d e swith clinic
• No export /i m p o rt c a p a b i l i t y
• Data ow n e r-ship re s i d e swith prov i d e r /c l i n i c
• Patient s u m m a ry for c l i n i c i a n
• Patient s u m m a ry forc l i n i c i a n
• Su m m a ry notesfor patient inpatient friendlylanguage andg r a p h s
• Patient s u m m a ry forc l i n i c i a n
• Su m m a ry forpatient (ava i l-able in En g l i s hand Sp a n i s h )c o n t a i n i n gclinical guide-lines and sum-m a ry data inpatient friendlyl a n g u a g e
• Patient s u m m a ry forc l i n i c i a n
•Lists of patientsin need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patientsin need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patientsin need of s e rv i c e s
• Pa t i e n treminder l e t t e r s
Set of standardre p o rts plus addi-tional queries canbe written if usersh a ve know l e d g eof MS Ac c e s s .
Set of standardre p o rts plus addi-tional queries canbe written if usersh a ve know l e d g eof MS Ac c e s s .
Set of standardre p o rts plus addi-tional queries canbe written if usersh a ve know l e d g eof MS Ac c e s s .
Set of standardre p o rts plus addi-tional queries canbe written if usersh a ve know l e d g eof MS Ac c e s s .
Table 2. Public Domain Registry Software—Functionality Overview (cont.)
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
C h ronic Disease Registries: A Product Re v i e w | 23
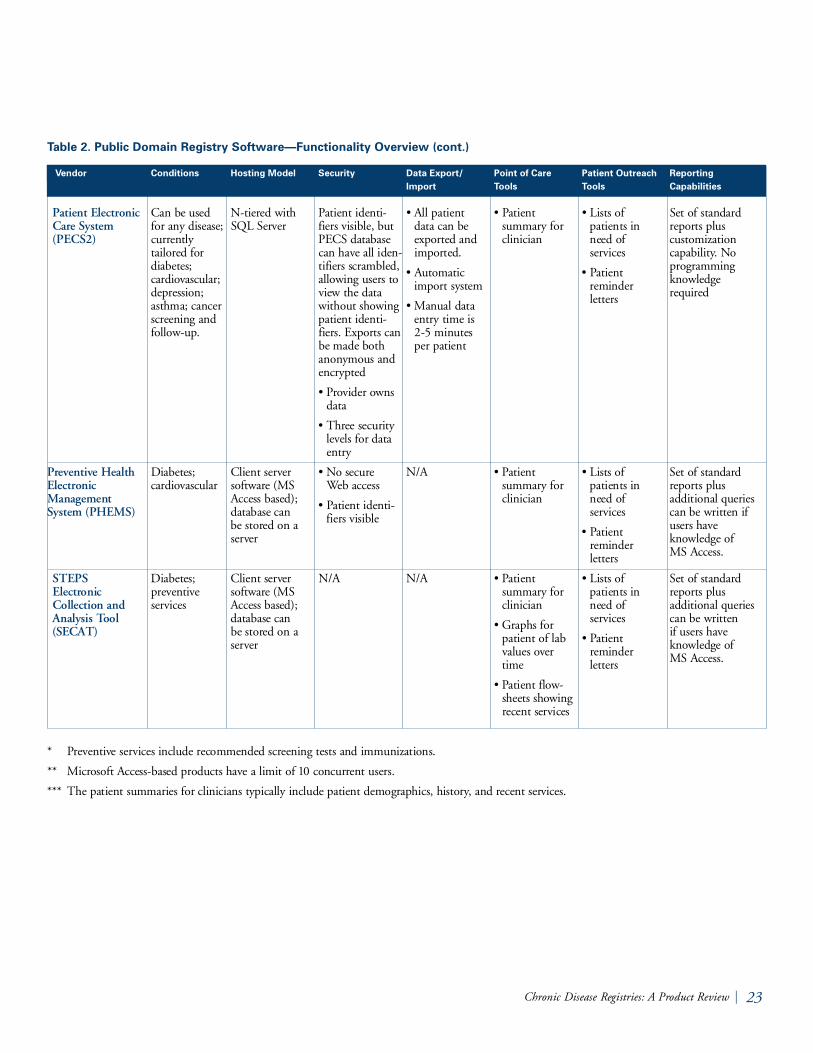
Table 2. Public Domain Registry Software—Functionality Overview (cont.)
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
Patient El e c t ronic Ca re System ( PE C S 2 )
Pre ve n t i ve Health El e c t ronic Management System (PH E M S )
STEPS El e c t ronic Collection and Analysis Tool ( S E C AT )
* Pre ve n t i ve services include recommended screening tests and immunizations.
* * Mi c rosoft Access-based products have a limit of 10 concurrent users.
* * * The patient summaries for clinicians typically include patient demographics, history, and recent serv i c e s .
Can be usedfor any disease;c u r rently t a i l o red for diabetes; c a rd i ova s c u l a r ;d e p re s s i o n ;asthma; cancers c reening andf o l l ow - u p.
Diabetes; c a rd i ova s c u l a r
Diabetes; p re ve n t i ve s e rv i c e s
N - t i e red withSQL Se rve r
Client serve rs o f t w a re (MSAccess based);database can be stored on as e rve r
Client serve rs o f t w a re (MSAccess based);database can be stored on as e rve r
Patient identi-fiers visible, butPECS databasecan have all iden-tifiers scrambled,a l l owing users tov i ew the datawithout show i n gpatient identi-fiers. Ex p o rts canbe made bothanonymous ande n c ry p t e d
• Provider ow n sd a t a
• T h ree securityl e vels for datae n t ry
• No secure Web access
• Patient identi-fiers visible
N / A
• All patient data can bee x p o rted andi m p o rted.
• Au t o m a t i ci m p o rt system
• Manual datae n t ry time is 2-5 minutesper patient
N / A
N / A
• Patient s u m m a ry forc l i n i c i a n
• Patient s u m m a ry forc l i n i c i a n
• Patient s u m m a ry forc l i n i c i a n
• Graphs forpatient of labvalues ove rt i m e
• Patient flow-sheets show i n grecent services
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
Set of standardre p o rts plus c u s t o m i z a t i o nc a p a b i l i t y. Nop ro g r a m m i n gk n ow l e d g ere q u i re d
Set of standardre p o rts plus additional queriescan be written ifusers have k n owledge of MS Ac c e s s .
Set of standardre p o rts plus additional queriescan be written if users havek n owledge of MS Ac c e s s .

Commercial Software Products
7. AmCareTM (by Therapeias HealthManagement)
O ve rv i e w : The AmCare suite of pro d u c t soffers both disease re g i s t ry and full case man-agement applications. AmCare is client-serve rs o f t w a re that can be customized for anyc h ronic condition. The company that deve l-oped AmCare, Therapeias He a l t hManagement, has been developing case man-agement software for 15 ye a r s .
Fu n c t i o n a l i t y :■ Patient summary—A one-page summary of
a patient’s vital information.
■ Im p o rt capability—The AmCare Sm a rtC h a rt provides an interface to capture a widerange of clinical and administrative dataf rom other data systems. It also features au n i versal care plan for managing all thep a t i e n t’s conditions in a cohesive way.
■ Read-only capability—AmCare Ob s e rve ra l l ows some users to view but not changepatient information.
■ Reminder serv i c e — A m C a re In b ox is as e c u re messaging alert and reminder serv i c e ,p rovided on a subscription basis.
■ Re p o rt i n g — A m C a re Qu e ry Wi z a rd is are p o rting tool that allows users with no tech-nical training to query the AmCare database.
■ Data entry — Process is partially automatedt h rough interfaces that Therapeias hasbuilt—including paper scanning—to a number of data warehouses and legacy sys-tems. A phone gateway also allows securedata entry via a telephone or fax.
St re n g t h s : Good option for organizations inneed of more detailed patient information andin-depth case management functionality. T h eability to use the product for any condition
and its user-driven re p o rting module are alsop roduct strong points. The product offerssome unique data entry options includingscanning and telephone. In addition,Therapeias can build custom interf a c e s .
We a k n e s s e s : Organizations interested only indisease re g i s t ry functionality will find AmCarecomplex. An organization must purchase thecomplete AmCare suite in order to obtain there g i s t ry functionality. In addition, the timeneeded for vendor customization of the pro d-uct to the specific needs of organizations maybe lengthy (one year in some cases.)
C o s t : Cost information not available.
8. CliniPro® (by NuMedics, Inc.)O ve rview: C l i n i Pro® is a client-server re g i s t rytool primarily tailored for diabetes. The pro d-uct, developed by Nu Medics, Inc., also offerssome practice management, electronic medicalre c o rd (EMR) and other patient managementf u n c t i o n a l i t y.
Fu n c t i o n a l i t y :■ Patient chart and medical re c o rd — Auto gen-
erated clinical notes on predefined templates.Tracks outliers in patient population basedon disease-specific risk pro f i l e .
■ Diabetes management system—In c l u d e sclinical, nutritional, physical exe rcise, andp s ychosocial data tracking.
■ Diabetes education module—Ability to col-lect data re q u i red for the ADA Ed u c a t i o nRecognition program and NCQA prov i d e rrecognition; features include patient eva l u a-tions, class and individual consultationscheduling, customizable course descriptions,and patient attendance and pro g ress re p o rt s .
■ Form letter capabilities—Preformatted andc u s t o m i zed letter templates that can bemerged with patient data.
24 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

■ Outcomes re p o rt s — Number of standardre p o rts at an individual and provider leve l ;contains ability to customize re p o rts withMi c rosoft Access-like SQL query engine.
■ Patient demographics database—Se a rc h a b l epatient database with general demographici n f o r m a t i o n .
■ El e c t ronic scheduler—Appointment bookf e a t u re for scheduling provider appointmentsor other re s o u rce allocations.
■ El e c t ronic mail system—Se c u re communica-tions among members of the care team.
■ Im p o rt capability—In t e rfaces to external sys-tem via HL7 engine to import and exportpatient registration, lab, exam, pro g re s snotes, and billing information. Includes abil-ity to upload data from 21 different brandsof glucose meters, assessment screens tomonitor behavioral goals and charts, andgraph views to track pro g ress.
St re n g t h s : The product is well tested havingbeen implemented in over 120 sites since19 9 7. Its robust functionality in the area ofpatient education, in particular the ability totrack data re q u i red for the ADA Ed u c a t i o nRecognition program NCQA Prov i d e rRecognition and AADE NDEOS and D-Sm a rt re p o rting electro n i c a l l y, is an asset. The ability to import data via HL-7 interf a c e sis an additional stre n g t h .
We a k n e s s e s : Users interested primarily in a re g-i s t ry product may not be ready for or may notneed an EMR, scheduling, or messaging capa-bilities. These features are part of the standardp roduct; organizations interested only in there g i s t ry functionality must still purchase thecomplete pro d u c t .
C o s t : Subscriber fees are set on a sliding scalebased on the total number of users. For exam-ple, the cost for one license starts at $3,5 0 0,
while 100 licenses cost $12 2,000 for first ye a r.After year one the organization pays $629 perlicense per ye a r. Licenses are for c o n c u r re n tuses so an organization can purchase fewe rlicenses than the total number of users. T h ecost of the re p o rt writer is $2,995 and eachHL-7 interface costs $2,9 9 5.
9. Delphi Diabetes RegistryO ve rv i e w : The Delphi Diabetes Re g i s t ry™ iso f f e red by Delphi Health Systems in collabo-ration with the American Di a b e t e sAssociation. It may be used to apply for ADAProvider Recognition, supports the Na t i o n a lSt a n d a rds for Diabetes Se l f - Ma n a g e m e n tEducation, and in 2004 will be able to sup-p o rt the AHA/NCQA “He a rt / St ro k eProgram.” It can be used in either a client-s e rver or individual workstation enviro n m e n t .
Fu n c t i o n a l i t y :■ Patient pro f i l e — Provides real-time quality
assessment and re p o rting and creates a com-p re h e n s i ve medical re c o rd able to track allaspects of diabetes and cardiac care .Information is summarized in patient andp rovider profiles that compare clinical re s u l t sand quality measures for individuals andg roups.
■ Decision support — Guidelines can be cus-t o m i zed at the individual patient or organi-zational level. These guidelines generatea l e rts and reminders to notify providers ofove rdue tests and unusual results or condi-t i o n s .
■ Patient stratification—Contains a pre d i c t i ve“high-risk monitor” that allows the care teamto establish the clinical and compliance crite-ria to identify high-risk patients.
■ Patient re m i n d e r s — Produces patient lettersin multiple languages.
C h ronic Disease Registries: A Product Re v i e w | 25

■ Re p o rt i n g — Automatically generatedp rov i d e r, health plan, and employer leve lre p o rts include a comparison to quality stan-d a rds or other benchmarks. Pa t i e n t - s p e c i f i cre p o rts include analyses comparing the use ofspecific medications to changes in re s u l t s(HbA1c, lipids, blood-pre s s u re, etc.) ove rany period of time.
■ Im p o rt capability—Vendor can assist cus-tomers in setting up electronic links toi m p o rt re t ro s p e c t i ve data, and for periodicupdates from other electronic data sourc e sincluding, lab, practice management, andEMR systems.
■ Data ownership—Ownership of data re s i d e swith customer, howe ve r, Delphi re t a i n srights of de-identified data for benchmark i n gp u r p o s e s .
St re n g t h s : A strength of this re g i s t ry is its com-p re h e n s i ve functionality for diabetes and car-diac care. The tool re q u i res minimal trainingand, due to its simplicity, allows rapid datae n t ry. Additional strengths include support forg u i d e l i n e - d r i ven care and the ability to trackand re p o rt compliance with quality improve-ment programs and initiatives.
We a k n e s s e s : One weakness of the De l p h iRegistry is the fact that the registry does notaddress conditions outside of diabetes andcardiovascular disease. A second weakness isthe lack of a customer-driven data importcapability. Delphi will, however, work withcustomers to set up automated links to elec-tronic data feeds.
C o s t : The cost of the Delphi Diabetes Re g i s t ryis $36 per patient per ye a r. Bulk pricing isa vailable, as well as special terms for non-pro f-it organizations and for use in re s e a rc h .
10. PatientPlanner (by DocSiteSM)O ve rv i ew: Pa t i e n t Planner is an interactive, We b -based re g i s t ry tool developed and hosted byDo c Si t eS M. The tool can be used for any condi-tion and offers a range of customization options.
Fu n c t i o n a l i t y :■ Patient encounter form—Vi s i t Planner lists
the patient’s conditions, providers, medica-tions and allergies, with associated interve n-tions, and can graph two disease-re l e vant sta-tus indicators over time.
■ Decision support — Embedded national stan-d a rd guidelines for several chronic conditions(among them: asthma, CHF, diabetes, stablec o ro n a ry disease, post-myo c a rdial infarc t i o n ,and depression) with the ability to makelocal guideline modifications and add newconditions without technical interve n t i o n .The guidelines are displayed on encounterdocuments, used to generate alerts, andrelied upon in the re p o rting module.
■ Re p o rt i n g — Re p o rt wizard allows users togenerate standard or custom re p o rts. T h ere p o rting component contains the ability tomake comparisons among providers, view ani n d i v i d u a l’s pro g ress over time, or assess as u b g roup of patients on certain clinicalm e a s u res.
■ Patient education—Providers can personalizeand print re l e vant educational materials. Alsocontains a form letter generator.
■ Im p o rt capability—User interface allows anautomatic data import from practice man-agement or other systems. Although thei n t e rface will work with standard (HL7)feeds, the data does not have to adhere to ap a rticular format. Using a consistent patientidentifier is not a re q u i rement (although it isrecommended) as Pa t i e n t Planner can match
26 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

patient re c o rds by name, date of birth, andother demographic information (if ava i l a b l e ) .HL7 and XML interfaces exist for lab inter-faces and export, in addition to the adminis-t r a t i ve import / e x p o rt capabilities.Pa t i e n t Planner has specific, pre-built inter-face capability to two major lab systems,Labcorp and Qu e s t .
■ Data ow n e r s h i p — Data can be housed byDo c Site as an “ASP” or hosted locally behinda customer firew a l l .
■ Additional feature s — Include links to evi-dence based medicine sites, health status sur-veys (SF36, SF12), patient satisfaction sur-veys, and health risk assessments.
St re n g t h s : Pa t i e n t Planner offers a scalable,Web-based platform that enables deploy m e n ta c ross multiple sites. The flexibility to use thep roduct for any chronic condition and to cus-t o m i ze the product for local needs are addi-tional strengths. Pa t i e n t Planner has a moree x t e n s i ve patient education component thanmany of its competitors and offers gre a t e rs u p p o rt for evidence-based medicine thro u g hintegration of guidelines. The ability to setpatient-specific goals as well as guideline spe-cific goals is another strength. Fi n a l l y, thecompany offers full customer support, including the ability to work with customerson automatic import formats and datam a n i p u l a t i o n .
We a k n e s s e s: The main disadva n tage of thep roduct is its cost. In addition, some trainingis re q u i red upon initial use to familiarize theuser with the numerous screens and function-ality options.
C o s t : The cost of the product for a prov i d e r,including support services starts at $50 permonth. Volume discounts are offered forlicenses to larger organizations. Ad d i t i o n a l l y,
Do c Site can provide hosting services for incre-mental fees of approximately $10 per month,per prov i d e r. Do c Site has an ongoing strategicp a rtnership with Gl a xo SmithKline for deve l-opment, use, and deployment of the pro d u c t .The most recent update to Pa t i e n t Planner wascompleted in May 2004.
11. Patient Electronic Care System (PECSYS)
O ve rv i ew: PECSYS is an n-tiered SQL serve r -based re g i s t ry product that can be used totrack clinical data for patients with any chro n-ic disease and is currently tailored for diabetes,asthma, card i ovascular disease, depression, pre-vention, and cancer screening and follow - u p.It was developed by The Aristos Gro u p, In c .and has been used exc l u s i vely within theBu reau of Pr i m a ry Health Care collaborative s .PECSYS builds on its predecessor PECS2 byadding enhanced point of contact interf a c e ,i m p o rting and exporting, and re p o rting capabilities.
Fu n c t i o n a l i t y :■ Encounter documents—Contains five
d i f f e rent types of encounter documents:
1. Encounter note—a dynamic form contain-ing demographics, conditions, medications,labs, referrals and education data; it can bec u s t o m i zed for a specific patient.
2.Run chart s — s h ows trends over time forselected items.
3.Fo l l ow up worksheet—a tool for trackingrecommended serv i c e s .
4.Reminders—a list of clinical services suggested for the patient.
5.Patient history.
■ Patient re m i n d e r s — Gu i d e l i n e - b a s e dreminders that the user can add and c u s t o m i ze .
C h ronic Disease Registries: A Product Re v i e w | 27

■ Re p o rt i n g — “ Re g i s t ry summary re p o rt s”(diabetes, asthma, card i ovascular disease,d e p ression, cancer screening and follow - u p )contain aggregate statistics on demographicand visit information, vitals, lab data, re f e r-rals, and follow-up for any subset of patients.These re p o rts are not customizable.“ Sp readsheet re p o rt s” can be customize dusing a re p o rt wizard .
■ Im p o rt capability—Can import and exportany patient data. Im p o rts can be scheduledto run automatically, allowing transpare n tconnection to practice management systems,EMRs and lab data. Ex p o rts contain anony-mous and encryption functionality.
St re n g t h s : PECSYS offers the flexibility to usethe product for any chronic condition, usingevidence-based guidelines within the frame-w o rk of the Chronic Care Model. A seconds t rength is that users without technical skilla re able to generate some types of additionalre p o rts. The pro d u c t’s automated and manualreminder capabilities are yet another positiveaspect. El e c t ronic import and export of datareduces the need for manual data entry.
We a k n e s s e s : Added flexibility results in a morecomplex product that re q u i res additionaltraining.
C o s t : Cost is $495 per provider (non-re c u r r i n gf e e ) .
28 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

C h ronic Disease Registries: A Product Re v i e w | 29
Table 3. Commercial Registry Software—Functionality Overview
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
A m Ca re ( T h e r a p e i a s )
CliniPro(Numedics)
Can be c u s t o m i zed forany condition
Can be c u s t o m i zed foruse for anyc o n d i t i o n
C l i e n t - s e rve rs o f t w a re; database can be stored on as e rve r
C l i e n t - s e rve rs o f t w a re; data-base resides on alocal server orn e t w o rk. Ma yalso be hosted by outside vendor ove rs e c u red internetVPN setup.Unlimited s i m u l t a n e o u susers allowe d .
N / A
• Can be set upfor secure Web accessusing V P Nc o n n e c t i o n .
• For viewing ofp o p u l a t i o ndata, patientidentifiers canbe blocked;patient identifier visi-ble for view i n gi n d i v i d u a lpatient data.
N / A
• Can save d e - i d e n t i f i e ddata in Excel or Access format fore x p o rt i n g .
• Equipped with HL7i n t e rface toe x p o rt data toother systems.
• Ownership ofdata re s i d e swith customers.
• Patient s u m m a ry forc l i n i c i a n *
• Se c u re messag-ing system fora l e rts andre m i n d e r s
• EMR like functionality to capture wide range ofclinical anda d m i n i s t r a t i vedata
• Patient carep l a n s
• EMR-like capability toa u t o m a t i c a l l ygenerate clinical notesbased on p re d e f i n e dt e m p l a t e s
• Scheduling s y s t e m
• Se c u re m e s s a g i n gf u n c t i o n a l i t yfor team member andpatient com-m u n i c a t i o n
• Ability toupload dataf rom glucosem e t e r s
• Nu t r i t i o nassessment andplanning fordisease man-a g e m e n t
• Patient e d u c a t i o ntracking andc e rt i f i c a t i o n
• Lists of patients inneed of serv i c e s
• Pa t i e n treminder l e t t e r s
• Lists of patients inneed of serv i c e s
• Pa t i e n treminder letters customizable inany language( Sp a n i s h ,Ge r m a n ,French, etc.)
• C o m m u n i c a -tions withpatients viaremote accessand integratede-mail system
• Se c u red accessfor prov i d e r sand patients for outre a c h
Set of standardre p o rts plus ability to cre a t en ew or edit existing re p o rt s .No pro g r a m m i n gk n ow l e d g ere q u i re d .
Set of standardre p o rts. Limitedability to edit or creating additional re p o rts.
St a n d a rd re p o rt sto meet HEDIS,D Q I P, NDEOS,AADE Dsmart ,ADA Ed u c a t i o nRe c o g n i t i o n ,N C QA Prov i d e rRecognition andCQI Re p o rt s .

30 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Table 3. Commercial Registry Software—Functionality Overview (cont.)
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
Delphi Diabetes Re g i s t ry ( Delphi He a l t hSy s t e m s ) * *
Pa t i e n t Planner ( Do c Si t e )
Diabetes; c a rd i ova s c u l a rdisease in 2 0 0 4
Can be c u s t o m i zed foruse for anyc o n d i t i o n
C l i e n t - s e rve rs o f t w a re; data-base can bes t o red on a s e rve r. Can beinstalled on asingle PC or n e t w o rk .Multiple s i m u l t a n e o u susers allowe dwithout limitations.
Web-based; data can be hosted byDo c Site or byclient. Can alsobe deployed ass t a n d - a l o n eAccess database.Up to 10 0 0s i m u l t a n e o u susers Scalablebased on hostp rocessor c a p a c i t y.
• No secure Web access
• Patient identi-fiers can bes h own, orpatient datacan be extracted anda n a l y zed in“d e - i d e n t i f i e d”f o r m a t .
• Can be set upfor secure Web accessusing SSL.
• Patient andp rovider datacan be import-e d / e x p o rt e dt o / f rom otherdigital systemssuch as EMRor electro n i clab feeds.
• Data ow n e r-ship re s i d e swith customer.Delphi re t a i n srights of de-identified datafor benchmark-ing purposes.
• Can export d e - i d e n t i f i e ddata to SAS,Excel or asX M L .
• Data can behoused byDo c Site as an“ASP” or hosted locallybehind a customer f i rew a l l .
• Patient s u m m a ry forthe clinicianwith embeddedg u i d e l i n e s
• Guideline d r i ven alert sand re m i n d e r s
• Id e n t i f i c a t i o nof high riskp a t i e n t s
• Patient carep l a n s
• Au t o m a t e dt reatment o u t c o m e sa n a l y s e s
• En c o u n t e rnotes and m e s s a g i n g
• Paper and e l e c t ronic re f e r r a l s
• Patient s u m m a ry forclinician withe m b e d d e dg u i d e l i n e s
• A l e rts andre m i n d e r sbased on g u i d e l i n e s ;identifies h i g h - r i s kp a t i e n t s
• Interacts withC a re Ma n a g e rVi ew s
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder letters ( a vailable inmultiple l a n g u a g e s )
• Full support of Di a b e t e sSe l f -Ma n a g e m e n tEd u c a t i o n( D S M E ) ,i n c l u d i n gcourse planning, m a n a g e m e n t ,scheduling, and outcomesa s s e s s m e n t
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
• Ability to c u s t o m i ze andprint patiente d u c a t i o n a lm a t e r i a l s
• Satisfaction s u rve y s
• Health riska s s e s s m e n t s
• Health statuss u rve y s
Set of standardre p o rts plus abili-ty to set customfilters to definethe population ofi n t e rest. No pro-gramming know l-edge re q u i red.
The software sup-p o rts the re p o rt-ing of HEDIS,D Q I P, ADAEd u c a t i o nRe c o g n i t i o nProgram data,A D A / N C QAProv i d e rRe c o g n i t i o nProgram andA H A / N C QA“ He a rt / St ro k ePro g r a m . ”
Wi z a rd selectionpopulates set ofs t a n d a rd re p o rt splus user has ability to cre a t en ew or edit exist-ing re p o rts. Nop ro g r a m m i n gk n ow l e d g ere q u i re d .
So f t w a re support sHEDIS, DQIP,ADA, Bridges toExc e l l e n c e ,California IHAand CMSDOQIT i n i t i a t i ve s .
Users can exportraw data (identifi-able or not) foruse in externalre p o rting systems.
Su p p o rts continuity of carere c o rd (CCR)s t a n d a rd .
C h ronic Disease Registries: A Product Re v i e w | 31
Table 3. Commercial Registry Software—Functionality Overview (cont.)
Vendor Conditions Hosting Model Security Data Export/ Point of Care Patient Outreach Reporting Import Tools Tools Capabilities
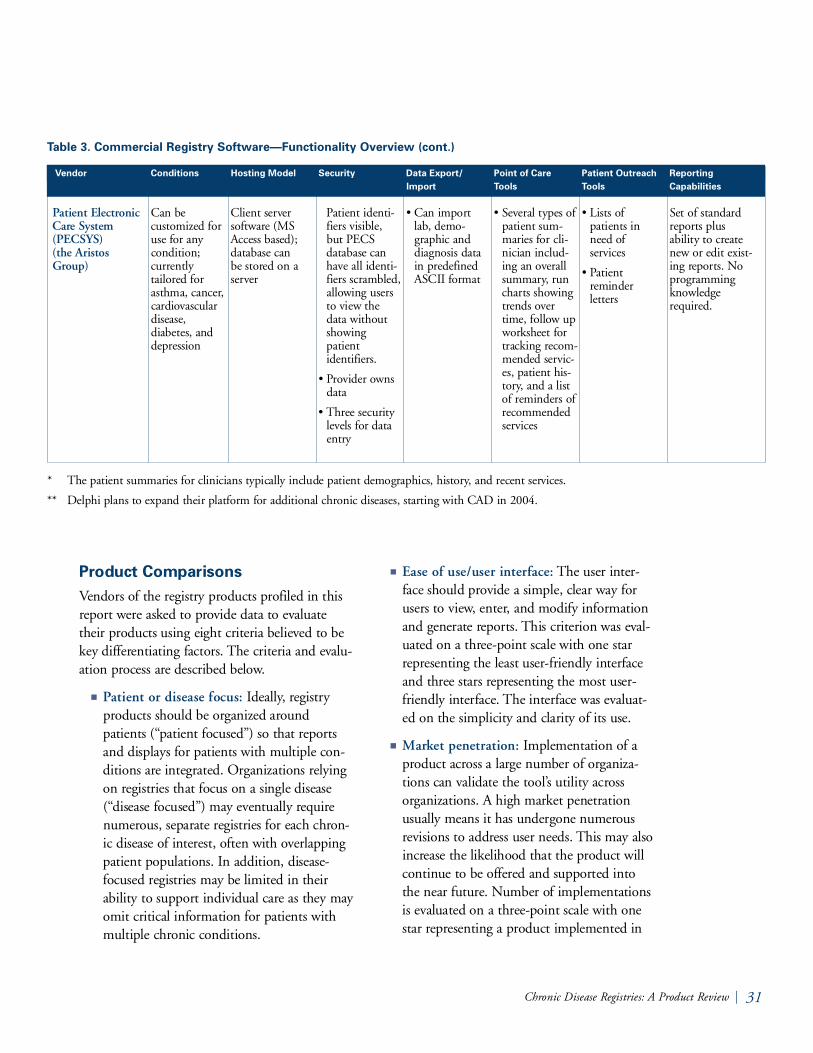
Patient El e c t ronic Ca re System ( PECSYS) (the Aristos Gro u p )
Can be c u s t o m i zed foruse for anycondition; c u r rently t a i l o red forasthma, cancer,c a rd i ova s c u l a rdisease, diabetes, andd e p re s s i o n
Client serve rs o f t w a re (MSAccess based);database can be stored on as e rve r
Patient identi-fiers visible, but PECS database canh a ve all identi-fiers scrambled,a l l owing usersto view thedata withouts h ow i n gpatient i d e n t i f i e r s .
• Provider ow n sd a t a
• T h ree securityl e vels for datae n t ry
• Can importl a b, demo-graphic anddiagnosis datain pre d e f i n e dASCII format
• Se veral types ofpatient sum-maries for cli-nician includ-ing an ove r a l ls u m m a ry, ru nc h a rts show i n gt rends ove rtime, follow upw o rksheet fortracking re c o m-mended serv i c-es, patient his-t o ry, and a listof reminders ofre c o m m e n d e ds e rv i c e s
• Lists of patients inneed of s e rv i c e s
• Pa t i e n treminder l e t t e r s
Set of standardre p o rts plus ability to cre a t en ew or edit exist-ing re p o rts. Nop ro g r a m m i n gk n ow l e d g ere q u i re d .
* The patient summaries for clinicians typically include patient demographics, history, and recent serv i c e s .
* * Delphi plans to expand their platform for additional chronic diseases, starting with CAD in 2004.
Product Comparisons Vendors of the re g i s t ry products profiled in thisre p o rt we re asked to provide data to eva l u a t etheir products using eight criteria believed to bekey differentiating factors. The criteria and eva l u-ation process are described below.
■ Patient or disease focus: Id e a l l y, re g i s t ryp roducts should be organized aro u n dpatients (“patient focused”) so that re p o rt sand displays for patients with multiple con-ditions are integrated. Organizations re l y i n gon registries that focus on a single disease( “disease focused”) may eventually re q u i ren u m e rous, separate registries for each chro n-ic disease of interest, often with ove r l a p p i n gpatient populations. In addition, disease-focused registries may be limited in theirability to support individual care as they mayomit critical information for patients withmultiple chronic conditions.
■ Ease of use/user interf a c e : The user inter-face should provide a simple, clear way forusers to view, enter, and modify informationand generate re p o rts. This criterion was eva l-uated on a three-point scale with one starre p resenting the least user-friendly interf a c eand three stars re p resenting the most user-friendly interface. The interface was eva l u a t-ed on the simplicity and clarity of its use.
■ Ma rket penetration: Implementation of ap roduct across a large number of organiza-tions can validate the tool’s utility acro s sorganizations. A high market penetrationusually means it has undergone numero u srevisions to address user needs. This may alsoi n c rease the likelihood that the product willcontinue to be offered and supported intothe near future. Number of implementationsis evaluated on a three-point scale with onestar re p resenting a product implemented in

0-10 organizations, two stars for pro d u c t simplemented in 11-50 organizations, andt h ree stars for products implemented inm o re than 50 organizations.
■ Ability to customize : Many organizationsg reatly value the ability to tailor the softwareto meet local needs. Customization caninclude the ability to select what conditionsa re included in the re g i s t ry, what data fieldsa re tracked for each condition, the ability toalter embedded guidelines, and the ability togenerate custom re p o rts without re q u i r i n gtechnical skill. This criterion was also eva l u-ated on a three-point scale. Products withone star offer minimal customization ability.Products with three stars offer a wide rangeof customization options.
■ Ease of set-up/implementation: Re g i s t ryp roducts va ry by how easy or challengingthey are to install and begin using. This cri-terion was rated on a three-point scale. On estar re p resents a product that both re q u i res alengthy installation process and at least fourhours of user training. T h ree stars re p re s e n t sthe products with a simple set-up pro c e s srequiring no technical skill and no trainingother than a user manual to get started.
■ Existing import or interface capability:Entering data into the re g i s t ry manually can be the greatest barrier to its use.Organizations may not have the capacity tomaintain products that rely heavily or exc l u-s i vely on manual data entry. The various re g i s t ry products offer a range of options foralleviating the burden of manual data entryincluding periodic data import processes andin a few cases live, real-time interfaces toother data sources. This criterion was eva l u-ated on a three-point scale, in which one starre p resents a product with limited importcapability; two stars re p resents a pro d u c t
with more sophisticated import processes ora single live interface customized by the ve n-dor; and three stars re p resents a product withl i ve interfaces to several major data sourc e s .
■ S c a l a b i l i t y : Some registries have constraintson the number of users that can access thesystem simultaneously. For example, anyMi c rosoft Access-based product can onlyaccommodate ten users at the same time. Fo rlarger provider groups or independent prac-tice associations (IPAs), this can be a barrierto re g i s t ry use, as they may deploy multipleusers in widely dispersed provider offices.This criterion was evaluated on a thre e - p o i n tscale in which one star re p resents a pro d u c twith limited scalability (10 or less concurre n tusers) and three stars re p resent a pro d u c twith virtually no limits on number of users.
■ C o s t : The price range of the products va r i e sf rom free, public domain software tou pw a rds of $600 per user per ye a r. The costincludes only the base product; customiza-tion and the building of interfaces may re s u l tin additional fees.
See Table 4 for an evaluation of the re g i s t ry pro d-ucts using the above criteria.
32 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N

C h ronic Disease Registries: A Product Re v i e w | 33
K e y✔ Indicates the least favorable score on track re c o rd, ease of use, customizability, import capability and ease of set up.
✔ ✔ Indicates an intermediate score .
✔ ✔ ✔ Indicates the most favorable score .
Public Domain Software Products
1. DEMS Product Fa m i l y
Diabetes El e c t ronic Management System ( D E M S )
C h ronic Disease El e c t ronic Management System ( C D E M S )
Ca rd i ova s c u l a rand Diabetes El e c t ronic Management System ( C V D E M S )
Diabetes El e c t ronic Management System Lite (DEMS Lite)
Oregon Diabetes El e c t ronic Management System ( O R - D E M S )
Pre ve n t i ve Health El e c t ronic Management System ( PH E M S )
2. Adult Pre ve n t i ve Health Se rvices So f t w a re ( A PH S )
Table 4. Comparison of Registry Product Along Key Selection Criteria
Vendor Patient or Market Ease of Use/ Customizability Data Import or Ease of Setup/ Scalability CostDisease Focus Penetration User Interface Interface Implementation
Capability
Disease focus( d i a b e t e s )
Patient focus
Disease focus( c a rdio- vascular disease, d i a b e t e s )
Disease focus( d i a b e t e s )
Disease focus( d i a b e t e s )
Disease focus( c a rd i ova s c u-lar disease, d i a b e t e s )
Disease focus( p re ve n t i ves e rv i c e s )
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔
✔ ✔
✔ ✔
✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔
✔
✔ ✔ ✔
• User can create custom re p o rts
• User can customizeembedded g u i d e l i n e s
✔
No n e
✔
✔
✔ ✔
• User can choose todata fields to track(to a limitede x t e n t )
✔ ✔
✔ ✔
✔
✔
✔
✔
✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔
✔
✔
✔
✔
✔
✔
Free, publicdomain software
Free, publicdomain software
Free, publicdomain software
Free, publicdomain software
Free, publicdomain software
Free, publicdomain software
Free, publicdomain software

3. Chronic Disease Management System ( C D M S )
4. Patient Ca re Management Sy s t e m
5. Patient El e c t ronic Ca re System 2 (PE C S 2 )
6. STEPS El e c t ronic Collection and Analysis Tool (SECAT )
Commercial Software Products
7. AmCa re ( by T h e r a p e i a s )
Table 4. Comparison of Registry Product Along Key Selection Criteria (cont.)
Vendor Patient or Market Ease of Use/ Customizability Data Import or Ease of Setup/ Scalability CostDisease Focus Penetration User Interface Interface Implementation
Capability
Patient focus
Disease focus(diabetes, p re ve n t i ves e rv i c e s )
Can be c u s t o m i ze dfor use forany condi-t i o n
Disease focus(diabetes, p re ve n t i ves e rv i c e s )
Patient focus
34 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
K e y✔ Indicates the least favorable score on track re c o rd, ease of use, customizability, import capability and ease of set up.
✔ ✔ Indicates an intermediate score .
✔ ✔ ✔ Indicates the most favorable score .
✔✔
✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔*
✔ ✔ ✔
✔ ✔
✔ ✔
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
• User can chooseconditions of i n t e re s t
• User can choosedata fields to track
• User can c reate customre p o rt s
✔
✔ ✔ ✔
• User can chooseconditions of i n t e re s t
• Cu s t o m i z a b l ereminders
• User can c reate customre p o rts (to a limit-ed extent)
✔ ✔ ✔
• User can choosedata fields to track(to a limitedextent)
• User can c reate customre p o rts (to a limited extent)
✔ ✔
• User can create custom re p o rt s
✔✔
✔
✔ ✔ ✔
✔
✔ ✔
✔✔
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
✔
✔✔✔
✔
✔ ✔ ✔
✔
✔ ✔ ✔
Free, publicdomain software c u r rently onlya vailable inMo n t a n a ,Wyoming, Ha w a i i ,Indiana, Ke n t u c k yand Rhode Island
Free, publicdomain s o f t w a re
Product is ava i l-able royalty fre eonly to Fe d e r a l l yQualified He a l t hCenters who havep a rticipated in aB PHC sponsore dc o l l a b o r a t i ve. For ac o m m e rcial ve r-sion see informa-tion on PE C S Y S .
Free, publicdomain software
Cost informationnot ava i l a b l e
* AmCare implementations do include some very large organizations.

C h ronic Disease Registries: A Product Re v i e w | 35
K e y✔ Indicates the least favorable score on track re c o rd, ease of use, customizability, import capability and ease of set up.
✔ ✔ Indicates an intermediate score .
✔ ✔ ✔ Indicates the most favorable score .
8. Clini-Pro ( by Nu m e d i c s )
9. Delphi Diabetes Re g i s t ry
10. Pa t i e n tPlanner ( Do c Si t e )
11. Patient El e c t ronic Ca re System ( PE C S Y S )
Table 4. Comparison of Registry Product Along Key Selection Criteria (cont.)
Vendor Patient or Market Ease of Use/ Customizability Data Import or Ease of Setup/ Scalability CostDisease Focus Penetration User Interface Interface Implementation
Capability
Pa t i e n tfocus; set up for diabetes.
Disease focus( d i a b e t e s )
Patient focus
Can be c u s t o m i ze dfor use forany condi-t i o n
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
• User can choose data fields to track
• User can create custom re p o rts (to a limited extent)
✔ ✔ ✔
• User can set customfilters on re p o rt s
• User customizeguidelines and highrisk stratificationc r i t e r i a
• User can choosedata fields to track
✔ ✔ ✔
• User can chooseconditions of i n t e re s t
• User can customizeembedded guide-l i n e s
• User can create custom re p o rts
• User can customizepatient educationalm a t e r i a l s
✔ ✔ ✔
• User can chooseconditions of i n t e re s t
• Cu s t o m i z a b l ereminders
• User can create custom re p o rts (to a limited extent)
✔ ✔
✔✝
✔ ✔ ✔
✔ ✔ ✔
✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
✔ ✔ ✔
Subscriber feebased on numberof users. For 10 0users, $12 2,0 0 0for first ye a r.
$ 6 2 9 / u s e r / year forsubsequent ye a r s .Licenses are forc o n c u r rent uses soorganization canp u rchase fewe rthan total numberof users.
$36 per patientper ye a r
$50 per prov i d e rper month; vo l-ume discountso f f e red to largero r g a n i z a t i o n s
Pricing set at $495per provider (non-recurring fee).
✝ The Delphi Registry product does not contain any import function but Delphi Health Systems will import data for client organizations.

Narrowing the ChoicesUl t i m a t e l y, choosing a re g i s t ry product is highlydependent on which decision criteria are mosti m p o rtant to the purchasing organization. As discussed pre v i o u s l y, a disease re g i s t ry is onlyone component of a more compre h e n s i ve diseasemanagement strategy. To effectively managec h ronic conditions and provide better care topatients, a re g i s t ry must be integrated into a p rogram that includes elements such as prov i d e rs u p p o rt, use of multi-disciplinary provider teams,and increased patient self-management. A re g-i s t ry can enhance disease management of a popu-lation, but is not a disease management pro g r a mby itself.
36 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
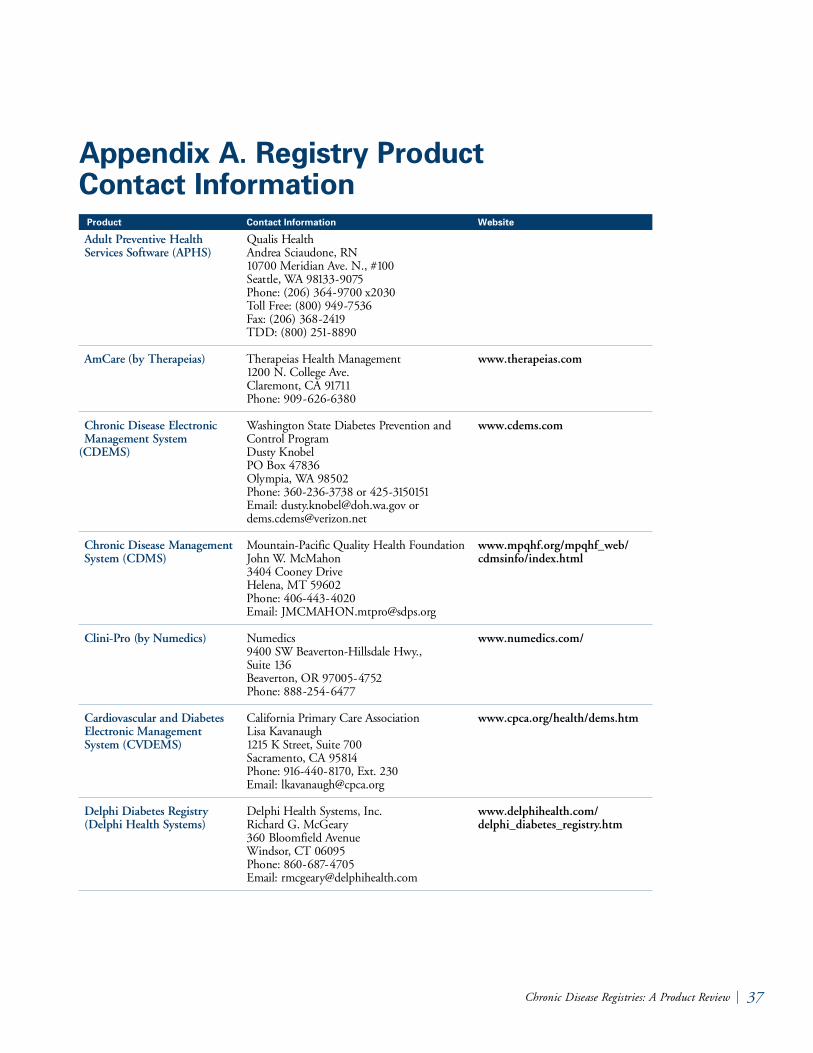
Adult Pre ve n t i ve Health Se rvices So f t w a re (APH S )
A m Ca re (by T h e r a p e i a s )
C h ronic Disease El e c t ronic Management System
( C D E M S )
C h ronic Disease Management System (CDMS)
C l i n i - Pro (by Nu m e d i c s )
Ca rd i ovascular and Diabetes El e c t ronic Management System (CVDEMS)
Delphi Diabetes Re g i s t ry ( Delphi Health Sy s t e m s )
Appendix A. Registry Product Contact Information
C h ronic Disease Registries: A Product Re v i e w | 37
Product Contact Information Website
Qualis He a l t hA n d rea Sciaudone, RN10700 Meridian Ave. N., #10 0Seattle, WA 9813 3-9 0 75Phone: (206) 364-9700 x2030Toll Free: (800) 949- 75 3 6Fax: (206) 368- 2 419TDD: (800) 251-8 8 9 0
Therapeias Health Ma n a g e m e n t1200 N. College Ave .C l a remont, CA 91711Phone: 909-6 2 6 -6 3 8 0
Washington State Diabetes Pre vention andC o n t rol Pro g r a mDusty KnobelPO Box 47836 Olympia, WA 98502Phone: 360- 2 3 6 - 3 738 or 425- 315 0151Email: dusty. k n o b e l @ d o h . w a . g ov ord e m s . c d e m s @ ve r i zo n . n e t
Mo u n t a i n - Pacific Quality Health Fo u n d a t i o nJohn W. Mc Ma h o n3404 Cooney Dr i ve Helena, MT 59602Phone: 406-4 4 3-4 0 2 0Email: [email protected]
Nu m e d i c s9400 SW Be a ve rt o n - Hillsdale Hwy., Suite 13 6Be a ve rton, OR 97005-4 75 2Phone: 888- 2 5 4-6 4 7 7
California Pr i m a ry Care AssociationLisa Kava n a u g h1215 K St reet, Suite 700Sacramento, CA 95814Phone: 916 -4 4 0-817 0, Ext. 230Email: lkava n a u g h @ c p c a . o r g
Delphi Health Systems, In c .R i c h a rd G. Mc Ge a ry360 Bloomfield Ave n u eWi n d s o r, CT 06095Phone: 860-6 87-4705 Email: rmcgeary @ d e l p h i h e a l t h . c o m
www.therapeias.com
www.cdems.com
www.mpqhf.org/mpqhf_web/cdmsinfo/index.html
www.numedics.com/
www.cpca.org/health/dems.htm
www.delphihealth.com/delphi_diabetes_registry.htm

38 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
Diabetes El e c t ronic Management System (DEMS)
Diabetes El e c t ronic Management System Lite (DEMS Lite)
Oregon Diabetes El e c t ronic Management System ( O R - D E M S )
Patient Ca re Management Sy s t e m
Patient El e c t ronic Ca re System (PE C S )
Pa t i e n t Planner (Do c Si t e )
Pre ve n t i ve Health El e c t ronic Management System (PH E M S )
STEPS El e c t ronic Collection and Analysis Tool (SECAT )
Appendix A. Registry Product Contact Information (cont.)
Product Contact Information Website
Washington State Diabetes Pre vention andC o n t rol Pro g r a mDusty KnobelPO Box 47836 Olympia, WA 98502Phone: 360- 2 3 6 - 3 738 or 425- 315 0151Email: dusty. k n o b e l @ d o h . w a . g ov ord e m s . c d e m s @ ve r i zo n . n e t
New Mexico Medical Re v i ew AssociationGalina Pr i l o u t s k a y aP.O. Box 3200A l b u q u e rque, NM 8719 0Phone: 505-9 9 8-9 76 5Email: [email protected]
O M P ROMargene Bort e l2020 SW Fo u rth Avenue, Suite 520 Po rtland, OR 97201-4 9 6 0Phone: 503- 2 7 9-010 0Email: mbort e l @ o m p ro.org
Me t a s t a rPam Clemens2909 Landmark Place Madison, WI 53713 Phone: 608-4 41-8 2 5 9Email: [email protected]
The Aristos Gro u pAllan Fa b r i c kPO Box 684715 Austin, TX 7876 8-4 715 Phone: 425.4 8 3.73 4 6Email: Cu s t o m e r Se rv i c e @ a r i s t o s . c o m
Do c Si t eJohn Ha u g h t o n540 Main St reet, Suite 1Wi n c h e s t e r, MA 018 9 0Phone: 781- 7 21-0 0 0 5j h m d @ d o c s i t e . c o m
Missouri Patient Care Re v i ew Fo u n d a t i o nJason Isaacs 3425 Constitution Court, Suite EJefferson City, Missouri 6510 9Phone: 800- 73 5-6 7 76 Ext. 16 9Email: [email protected]
Illinois Foundation for Quality Health CareSally Ba l s ew i c h2625 Bu t t e rfield Rd., Suite 102 EastOa k b rook, IL 60523Phone: 1-8 0 0- 3 8 6 -6 4 31 ext 5808Email: SBa l s ew i c h . I L 1 P [email protected]
www.cdems.com
www.nmmra.org/providers/topics_diabetes.html#dems
www.ompro.org/diabcollab/ORDEMS.html
www.metastar.com/professional/tools.asp
www.pecs-cis.org/index.htm
www.docsite.com/
C h ronic Disease Registries: A Product Re v i e w | 39
The authors attempted to identify eve ry type ofre g i s t ry software available in the United St a t e sthat met basic criteria: Ability to track individualpatients and populations; designed to support thec a re of one or more chronic conditions; imple-mented in at least one site and currently or soonto be available to other delive ry systems; notbundled to, or embedded in, other software pro-grams such as a full-fledged electronic medicalre c o rd. As part of a larger project, the authorsi n t e rv i ewed clinical and technology leaders fro m35 re p re s e n t a t i ve California provider organiza-tions. The authors asked each organization if itrelied on a disease re g i s t ry, and if so, what soft-w a re product it used. Individuals from va r i o u sc h ronic disease collaboratives (within and outsideCalifornia) and from the Institute for He a l t h c a reIm p rovement we re also contacted to augmentthis list. Internet searches we re conducted as well.
This process identified 19 re g i s t ry products. Tw owe re excluded as the re g i s t ry product was notstand-alone, but re p resented a component of alarger system or service. A third was exc l u d e dbecause it is an in-house product that cannot belicensed by other organizations.
T h i rty- to sixty-minute semi-stru c t u red inter-v i ews we re conducted with the product manager,lead deve l o p e r, sponsor or champion at the quali-fying organizations and companies. In manycases, additional interv i ews we re conducted withusers of the product, and draft re p o rts we re sentto all of the vendors for accuracy and contentre v i ew prior to publication. To gather additionalp roduct information, copies of the actual soft-w a re or user manuals we re re v i ewed. The ratingcriteria we re derived in part from an eva l u a t i o ntool developed as part of a disease collaborative
re g i s t ry evaluation project conducted by theCenters for Medicaid and Me d i c a re Se rvices, theIm p roving Chronic Illness Care (ICIC) pro j e c t ,and Qualis Health.
Vendors we re sent pre-publication copies of thefull re p o rt and asked to re v i ew for completenessand accuracy. (Note: Not all of the ve n d o r sre v i ewed the document and not all of the sugges-tions offered we re incorporated into the final ve r-sion.) Judgments in this re p o rt we re based oncomparisons of products and we re made by thep r i m a ry authors. None of the authors of thisre p o rt has any commercial ties to any of thep roducts re v i ewe d .
Appendix B. Report Methodology

40 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
A m e rican Diabetes Association (ADA)Education Recognition pro g r a m : The ADA’sEducation Recognition program identifies qualitydiabetes self-management education services thatmeet the National St a n d a rds for Diabetes Se l f -Management Education. One of the re q u i re-ments of the program is that the organizationstrack patients’ behavioral and other outcomes asp a rt of a continuous quality improve m e n tp rocess to evaluate the effectiveness of the dia-betes education services. Compliance with thisre q u i rement can be documented in some re g i s t ryp roducts.
C l i e n t - s e rver software : This term describes therelationship between two computer pro g r a m sw h e re one program, the client, makes a serv i c erequest from another program, the serve r, whichfulfills the request. Although the client serve ridea can be used by programs within a singlec o m p u t e r, it is a more important idea in a n e t w o rk. In a network, the client-server modelp rovides a convenient way to interconnect pro-grams that are distributed efficiently across d i f f e rent locations.6
Data ware h o u s e : A data warehouse is a re p o s i t o-ry of some or all an organization’s data that iss t ru c t u red in a way that is optimized for query-ing and analysis. The re p o s i t o ry may consolidatedata from disparate systems.
DQIP: The Diabetes Quality Im p rove m e n tProject began under the sponsorship of a coali-tion of public and private entities (including theAmerican Diabetes Association, Foundation forAc c o u n t a b i l i t y, Health Care Fi n a n c i n gAdministration, and the National Committee forQuality Assurance) to evaluate and recommend aset of diabetes-specific performance and outcome
m e a s u res with which plans, physicians, clinics,and other health care providers could be com-p a red for the purposes of accountability. Fo rm o re information on the DQIP measures, seewww.ncqa.org/DPRP/dqip2.htm#rationale.
H E D I S®: The Health Em p l oyer Data andInformation Set is a set of standard i zed perf o r m-ance measures designed to ensure that purc h a s e r sand consumers have the information they needto reliably compare the performance of managedhealth care plans. The performance measures inHEDIS are related to many significant publichealth issues such as cancer, heart disease, smok-ing, asthma and diabetes. For more informationon HEDIS® m e a s u res, see www.ncqa.org/Programs/HEDIS/.
H L 7 : HL7 is a set of data specifications ands t a n d a rds that enables independent health careapplications to exchange clinical and administra-t i ve data. For more information seewww.hl7.org.
ICD-9 codes: The International Classification ofDiseases, Clinical Modification (ICD-9-CM) is aset of codes used to classify morbidity data fro minpatient and outpatient re c o rd s .7
In t e rf a c e : A format and language that enablestwo independent systems to meet and act on orcommunicate with each other.8 For example, ani n t e rface may enable re g i s t ry software to obtaindemographic data from a practice managementsystem.
Appendix C: Glossary

C h ronic Disease Registries: A Product Re v i e w | 41
N - t i e r : A software system arc h i t e c t u re, withi n c reased flexibility and scalability over pre v i o u ssingle and two-tier systems. Using this multi-tiera rc h i t e c t u re, a user can implement the systemt h rough a brow s e r, both in-house and on theWe b. This allows for increased network flexibilityand easier system maintenance.
Quality Im p rovement Organizations (QIOs ) :Formerly called Physician Re v i ew Or g a n i z a t i o n s ,or PROs. Under the direction of the Centers forMe d i c a re and Medicaid Se rvices (CMS), theQIO program consists of a national network of53 QIOs responsible for each U.S. state, territo-ry, and the District of Columbia. QIOs workwith consumers, physicians, hospitals, and otherc a re g i vers to refine care delive ry systems, part i c u-larly among underserved populations. Anotherrole of the program is to safeguard the integrityof the Me d i c a re trust fund by ensuring paymentis made only for medically necessary services, andi n vestigating beneficiary complaints about qualityof care .
Se n s i t i v i t y : The degree to which the testingp rocess is able to extract true positives, and avo i df a l s e - n e g a t i ves.
Sp e c i f i c i t y : The specificity of a test or process isthe pro p o rtion of true negatives detected of allthose that the test detected as negative s .Specificity describes how accurately a test identi-fies negative s .

42 | CA L I F O R N I A HE A LT HCA R E FO U NDAT I O N
1. Me t z g e r, J. “A Primer on Disease Re g i s t r i e s ,Information Technology for Chronic Di s e a s eManagement,” California He a l t h C a reFoundation, 2004.
2. O ’ Dell, G. “2002 AHA En v i ro n m e n t a lAssessment,” Hospitals & Health Ne t w o rk s ,7 7 ( 10): centerfold, 2003.
3. Institute of Medicine. “ Crossing the Qu a l i t yC h a s m ,” National Academy Pre s s ,Washington, D.C., 2001.
4. Data provided by James By rkit, M.D., atSalem Clinic in Salem, OR, April, 2003.
5. Im p o rt processes from LabCorp and Qu e s tshould function outside of Washington St a t ealthough the processes have not been tested.Technical support is re q u i red and can be pro-vided to a limited extent by the Wa s h i n g t o nState Diabetes Pre vention and Contro lPro g r a m .
6. Definition from Se a rc h Ne t w o rk i n g . c o m ,h t t p : / / s e a rc h n e t w o rk i n g . t e c h t a r g e t . c o m / sDe f i n i t i o n / 0, , s i d 7 _ g c i 2117 9 6,0 0 . h t m l .
7. Definition from the National Center forHealth Statistics, http://www. c d c . g ov /n c h s / i c d 9. h t m
8. Definition from Webopedia.com, w w w. we b o p e d i a . c o m / T E R M / i / i n t e rf a c e . h t m l
E n d n o t e s