Systems Support: Care Management Protocols, Disease Registries, and Other Tools
Upload
dale-sandersCategory
view
1.981download
1
Disease Registries: Translating P4P and other Quality Measures into EpicCare
September 20, 2007
Users’ Group Meeting
The Faculty Practice Plan of Northwestern’s Feinberg School of Medicine

2
Agenda
NMFF Overview
Epic Implementation History
Patient Registries History and Overview
Our Experience building a Disease Registry
After the Build
Lessons learned

3
Chicago Shoreline

4
Feinberg Pavilion (Inpatients) & Ambulatory Care Center

5
Prentice Women’s Hospital: Opening October 2007

6
Our MissionNorthwestern Medical Faculty Foundation is the
regionally and nationally recognized physician group at the Feinberg School of Medicine, Northwestern University. Our physicians and staff use innovative
clinical practices and technology and a multidisciplinary approach to provide optimal patient
care and service. We support the clinical and academic activities of the Feinberg School and create an environment where the best medical
practices are demonstrated and learned.

7
About Northwestern Medical Faculty Foundation (NMFF)
Private, independent academic faculty practice plan founded in 1980
Multi-specialty group practice for over 600 member physicians who are all full-time faculty of Northwestern University’s Feinberg School of Medicine (NU FSM)
Physician led
Not for profit
Provides care for indigent patients
NMFF Overview

8
Northwestern Medical Faculty Foundation Facts
Over 600 physicians and 1,101 staff at the end of FY06
17 departments, 34 specialties
Just under 571,000 outpatient encounters in FY06
Total clinical revenue $346 million in FY06
We occupy roughly 268,000 square feet of clinical space for outpatient care in the Ambulatory Care Center (ACC)
NMFF Overview

9
Relationship to Northwestern University Feinberg School Of Medicine (NU FSM)
NMFF members are full-time NU FSM faculty
• Clinical care of patients
• Ground breaking clinical research
• Training next generation of physicians
Faculty for over 600 medical students and 500 residents and fellows (11,000 hours of teaching)
NMFF’s Ambulatory Care Center provides the venue for outpatient teaching and clinical research
NMFF Overview

10
Epic Implementation History• Pilot: 1996 NLM Project to Pilot EpicCare in GIM
• Awards: 1998 Davies Award Winner
• Implementation in 31 specialty practices (2001 – 2006)
• 97% Implemented in 32 specialties (2007)• Non-Implemented Specialties
• Reproductive Endocrinology and Infertility• Ophthalmology• Trauma/Critical Care
• Epic Products: Bridges, Clarity, EpicCare, Identity, MyChart
• Epic Version: Epic Fall 2006 version (Spring 2007 IU1 upgrade scheduled for October 2007)
• 3057 Active user accounts
Epic Implementation History

11
EpicCare Implementations in Specialty & Sub-Specialty Areas Allergy
Anesthesia/Pain Medicine
Cardiology
CardioThoracic Surgery
Dermatology
Endocrine/Metabolism
Gastroenterology
General Internal Medicine*
General Neurology
General OB/GYN
Geriatrics
GI-Endocrine Surgery
Gynecology Oncology
Gynecologic Surgery
Hematology Oncology
Hepatology
Immunotherapy
Interventional Radiology
Lynn Sage Breast Center
Maternal Fetal Medicine
Nephrology
NeuroBehavior
NeuroSurgery
Northwestern Ovarian Cancer Early Detection Program
Orthopedics/Sports Medicine
Otolaryngology
Plastics Surgery
Psychiatry
Pulmonary
Reproductive Genetics
Rheumatology
Surgical Oncology
Travel Medicine/Immunizations
UroGynecology
Urology*
Vascular Surgery*MyChart Department
Epic Implementation History

12
Agenda
NMFF Overview
Epic Implementation History
Patient Registries History and Overview
Our Experience building a Disease Registry
After the Build
Lessons learned

13
Patient Registry Definitions
“A database designed to store and analyze information about the occurrence and incidence of a particular disease, procedure, event, device, or medication and for which, the inclusion criteria are defined in such a manner that minimizes variability and maximizes precision of inclusion within the cohort.”
--- Dale Sanders, Northwestern University Medical Informatics Faculty, 2005
“Computer Applications used to capture, manage, and provide information on specific conditions to support organized care management of patients with chronic disease.”
--”Using Computerized Registries in Chronic Disease Care”; California Healthcare Foundation and First Consulting Group, 2004.
Patient Registries History & Overview

14
AHRQ’s Patient Registry Definition
“A patient registry is an organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure and that serves one or more predetermined scientific, clinical, or policy purposes.”
The National Committee on Vital and Health Statistics describes registries used for a broad range of purposes in public health and medicine as "an organized system for the collection, storage, retrieval, analysis, and dissemination of information on individual persons who have either a particular disease, a condition (e.g., a risk factor) that predisposes [them] to the occurrence of a health-related event, or prior exposure to substances (or circumstances) known or suspected to cause adverse health effects."
http://effectivehealthcare.ahrq.gov/reports/registry/registry.htm
Patient Registries History & Overview

15
History of Patient Registries
Historically, the term implies stand-alone, specialized products and clinical databases
Long precedence of use and effectiveness in Cancer
• 1926: First cancer registry at Yale-New Haven hospital
• 1935: First state, centralized cancer registry in Connecticut
• 1973: Surveillance, Epidemiology, and End Results (SEER) program of National Cancer Institute, first national cancer registry
• 1993: Most states pass laws requiring cancer registries
Pioneered by GroupHealth of Puget Sound in the early 1980s for diseases other than cancer
• “Clinically related information system”
Patient Registries History & Overview

16
Types of Registries
Product Registries• Patients exposed to a health care product, such as a drug or a device.
Health Services Registries• Patients by clinical encounters such as
–Office visits–Hospitalizations–Procedures–Full episodes of care
Referring Physician Registry• Facilitates coordination of care
Primary Care Physician Registry
• Facilitates coordination of care
Patient Registries History & Overview

17
Types of Registries
Scheduling Events Registry
• Facilitates analysis for Patient Relationship Management (PRM)• Can drive reminders for research and standards of care protocols
Mortality registry
• An important thing to know about your patients
Research Patient Registry
• Clinical Trials• Consent
Disease or Condition Registries
• Disease or condition registries use the state of a particular disease or condition as the inclusion criterion.
Combinations
Patient Registries History & Overview

18
Varying Benefits
Clinicians
Registries
Drug Manufacturer
Physician Organization Consumer
How do I analyze patient trends and outcomes for a disease?
How are my clinicians managing diseases?
How does my drug perform in disease prevention and cure?
How do I know which drug/procedure works best for me?
Patient Registries History & Overview

19
Uses for Patient Registries
To observe the course of disease
To understand variations in treatment and outcomes
To examine factors that influence prognosis and quality of life
To describe care patterns, including appropriateness of care and disparities in the delivery of care
To assess effectiveness
To monitor safety
Patient Registries History & Overview

20
Current Trends measuring Quality using Registries
The IOM defines quality as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”
Quality-focused registries are being used increasingly to assess differences between providers or patient populations based on performance measures that compare:
• Treatments provided or outcomes achieved with “gold standards” (e.g., evidence-based guidelines)
• Comparative benchmarks for specific health outcomes (e.g., risk-adjusted survival or infection rates)
Patient Registries History & Overview

21
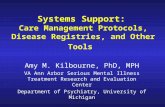
Quality Management Reporting - Example
Eligible Satisfied Rate
Preventive Services Cervical Cancer Screen 223 146 65%
Mammogram 138 83 60%
Colorectal Cancer Screen 355 143 40%
Pneumonia Vaccine 144 33 23%
Osteoporosis Screened or on Treatment 75 44 59%
Cardiovascular Disease HTN: good BP control (mean or last <= 140/90) 310 196 63%
CAD: antiplatelet medication 62 54 87%
CAD: lipid lowering medication 65 54 83%
CAD: Beta blocker post-MI 12 10 83%
CAD: ACE/ARB if DM or LVSD + CAD 25 19 76%
CHF: anticoagulation for AF + HF 6 5 83%
CHF: ACE/ARB if LVSD 3 3 100%
CHF: beta blocker if LVSD 3 3 100%
Diabetes Last Hba1c <= 7 87 37 43%
Last Hba1c <= 9 87 66 76%
Good BP control (mean or last BP <= 130/80) 83 39 47%
Good LDL control (<100) 87 49 56%
Nephropathy: screened or on ACE/ARB 87 64 74%
Patient Registries History & Overview

22
Getting the most out of your disease registry (Our Interpretation)
Consistent profiling for prospective, predictive intervention
• The goal is to keep people off of disease registries, but first you have to know how those who are on the registry, got there…
Outreach communication to patients
• Reminders about care and intervention
Ensuring a common understanding for inclusion, exclusion and disease management.
Quality of care reporting (e.g. P4P)
• Cost effective & treatment efficacy to payers & employers
• Feedback reports to physicians about their care practices
Process improvement projects for service line clinical programs
• Use trend analysis to find possible process deficiencies that affect patient care
Population reporting and analysis for research (e.g. Epidemiology)
Patient Registries History & Overview

23
Agenda
NMFF Overview
Epic Implementation History
Patient Registries History and Overview
Our Experience building a Disease Registry
After the Build
Lessons learned

24
Target Disease Registries
– Amyotrophic Lateral Sclerosis– Alzheimer's– Asthma– Breast cancer– Cataracts– Chronic lymphocytic leukemia– Chronic obstructive pulmonary disease– Colorectal cancer– Community acquired bacterial
pneumonia– Coronary artery bypass graft– Coronary artery disease– Coumadin management– Diabetes– End stage renal– Gastro esophageal reflux disease– Glaucoma– Heart failure– Hemophilia– Stroke (Hemorrhagic and/or Ischemic)– High risk pregnancy– HIV– Hodgkin's Disease
– Hypertension
– Lower back pain
– Systemic Lupus– Macular degeneration– Major depression– Migraines– MRSA/VRE– Multiple myeloma– Myelodysplastic syndrome & acute leukemia– Myocardial infarction– Obesity– Osteoporosis– Ovarian cancer– Prostate cancer– Rett Syndrome– Rheumatoid Arthritis– Scleroderma– Sickle Cell– Upper respiratory infection (3-18 years)– Urinary incontinence (women over 65)– Venous thromboembolism prophylaxis
Our Experience Building a Disease Registry

25
Patients exist in one of three states, relative to a patient registry
On Registry: The patient is a member of a particular registry; i.e., they fit the inclusion criteria
Off Registry: Patient was once a member of a registry and fit the inclusion criteria, but is now excluded. The exclusion could be “disease free.”
At Risk: The patient fits the profile that could lead to inclusion on the registry, but does not yet meet the formal inclusion criteria, e.g. obesity as a precursor to membership on the diabetes and or hypertension registry.
Off RegistryAt Risk On Registry
Disease Registry
Our Experience Building a Disease Registry

26
Patient Registry Vision
LAB RESULTS
CPT CODES
ICD9 CODES
MEDICATIONS
CLINICAL OBS
PROBLEMLIST
PATIENT VALIDATION
CLINICIAN VALIDATION
PATH
DISEASEREGISTRY
MORTALITY
REGISTRATION
SCHEDULING
INCLUSIONCRITERIA &
STRUCTURED EXCLUSION
CODES
PATIENT PROVIDER
RELATIONSHIP
* DISEASE MANAGEMENT* OUTCOMES ANALYSIS* RESEARCH* P4P REPORTING* CLINICAL TRIALS ENROLLMENT
RAD RESULTS
TUMOR REG
COSTS & REIMBURSEMENT
DATA
CARDIOLOGYIMAGING
• How do we define a particular disease? • Who has the disease?• What is their demographic profile?
• Are we managing these patients according to accepted best protocols?• Which patients had the best outcomes and why?• Where is the optimal point of cost vs. outcome?
Our Experience Building a Disease Registry

27
Disease Registry Exclusions
The industry will need standard vocabularies for excluding patients
• Removing patients from the registry whose data would otherwise skew the data profile of the cohort
“Why should this patient be excluded from this registry, even though they appear to meet the inclusion criteria?”
– Patient has a conflicting clinical condition
– Patient has a conflicting genetic condition
– Patient is deceased
– Patient is no long under the care of this facility or physician
– Patient is voluntarily non-compliant with the care protocol
– Patient is incapable of complying with the care protocol
Off RegistryAt Risk On Registry
Disease Registry
Our Experience Building a Disease Registry

28
Our disease registry is populated by patient care cycle
Disease Registry
Patient Data(Clinical, Business, etc)
Pay for Performance
measures
Pay for Performance
measuresPt. included in Disease Reg.
off Original Diagnosis
How do I build this?
Original Diagnosis Continued Care Continued Care Cured
Our Experience Building a Disease Registry

29
The Healthcare Process and Transactional Systems at NMFF
Diagnostic systemsLab SystemRadiologyImagingPathologyCardiologyOthers
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
ADT SystemMaster Patient Index
Pharmacy ElectronicMedical Record
SurveysResults
Billing and ARSystem
Claims ProcessingSystem
Patient Data lies in various data sources

30
The Northwestern Campus : Multiple, Collaborative, Organizations
EDWA single data perspective
on the patient care process
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index•ADT System•Master Patient Index
PharmacyPharmacy ElectronicMedical Record
ElectronicMedical Record
SurveysSurveys•Diagnostics•Pharmacy•Diagnostics•Pharmacy
Billing and ARSystem
Billing and ARSystem
Claims ProcessingSystem
Claims ProcessingSystem
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index•ADT System•Master Patient Index
PharmacyPharmacy ElectronicMedical Record
ElectronicMedical Record
SurveysSurveys•Diagnostics•Pharmacy•Diagnostics•Pharmacy
Billing and ARSystem
Billing and ARSystem
Claims ProcessingSystem
Claims ProcessingSystem
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
Diagnostic systems•Lab System•Radiology•Imaging•Pathology•Cardiology•Others
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index
Pharmacy ElectronicMedical Record
Surveys•Diagnostics•Pharmacy
Billing and ARSystem
Claims ProcessingSystem
DiagnosisRegistration &
SchedulingPatient
PerceptionOrders &
ProceduresResults & Outcomes
Billing &Accounts
Receivable
Claims Processing
EncounterDocumentation
•ADT System•Master Patient Index•ADT System•Master Patient Index
PharmacyPharmacy ElectronicMedical Record
ElectronicMedical Record
SurveysSurveys•Diagnostics•Pharmacy•Diagnostics•Pharmacy
Billing and ARSystem
Billing and ARSystem
Claims ProcessingSystem
Claims ProcessingSystem
Physician Office X
Hospital YPhysician Office Z

31
Disease Registry
Patient Data(Clinical, Business, etc)
Pay for Performance
measures
Pay for Performance
measuresPt. included in Disease Reg.
off Original Diagnosis
Original Diagnosis Continued Care Continued Care Cured
How do I build this?
Our Experience Building a Disease Registry

32
Basic steps to build a disease registry
Identify stakeholders
Identify data points necessary to define, include and exclude in disease registry
Identify source of data points
Build registry
Address data quality issues
Our Experience Building a Disease Registry

33
Identifying Data Points & Data Sources
Inclusion codes based entirely on ICD9, which is a good place to start, but not specific enough• Heart failure codes for study inclusion
– 398.91, 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 428.xx
• Exclusion criteria for beta blocker use†– Heart block, second or third degree: 426.0, 426.12, 426.13, 426.7– Bradycardia: 427.81, 427.89, 337.0– Hypotension: 458.xx– Asthma, COPD: see above– Alzheimer's disease: 331.0– Metastatic cancer: 196.2, 196.3, 196.5, 196.9, 197.3, 197.7, 198.1, 198.81, 198.82, 199.0,
259.2, 363.14, 785.6, V23.5-V23.9
• † Exclusion criteria were only assessed for patients who did not have a medication prescribed; Thus, if a patient was prescribed a medication but had an exclusion criteria, the patient was included in the numerator and the denominator of the performance measure. If a patient was not prescribed a medication and met one or more of the exclusion criteria, the patient was removed from both the numerator and the denominator.Acknowledgements to Dr. David Baker, NU Feinberg School of Medicine
Our Experience Building a Disease Registry

34
What does a Diabetes Disease Registry Look Like Elsewhere?
Our Experience Building a Disease Registry

35
University of Washington Physicians Network
Our Experience Building a Disease Registry

36
Harvard Vanguard
Our Experience Building a Disease Registry

37
Harvard Vanguard (continued)
Our Experience Building a Disease Registry

38
Our First Design
Keep it as flat as possible
Use consistent naming standards throughout
Keep design minimalist
Our Experience Building a Disease Registry

39
Our Extensible Design
Key Design Considerations
Used clinician input for building & defining institutional definition of the disease
Stakeholders input in defining inclusion & exclusion criteria
Disease Registry metadata contains inclusion, exclusion criteria
Added a reason for inclusion description for disease registry
The disease registry data model was built to tie the patient identity back to data points in the data warehouse which includes all EMR data sources.
Motives
Consistent profiling for prospective, predictive intervention
Outreach communication to patients
Quality of care reporting (e.g. P4P)
Process improvement projects for service line clinical programs
Population reporting and analysis for research (e.g. Epidemiology)
Our Experience Building a Disease Registry

40
Building our Disease Registry (i.e. Diabetes)
diabetes (registries_dm)
mrd_pt_id int
birth_dt datetime
death_dt datetime
gender_cd varchar(20)
problem_list_diabetes... int
encntrs_diabetes_dx_... int
orders_diabetes_dx_n... int
meds_diabetes_dx_num int
last_hba1c_val float
last_hba1c_dts datetime
max_hba1c_val float
max_hba1c_dts datetime
min_hba1c_val float
min_hba1c_dts datetime
tobacco_user_flg varchar(50)
alcohol_user_flg varchar(50)
last_encntr_dts datetime
last_bmi_val decimal(18, 2)
last_height_val varchar(50)
last_weight_val varchar(50)
data_thru_dts datetime
meta_orignl_load_dts datetime
meta_update_dts datetime
meta_load_exectn_guid uniqueidentifier
Column Name Data Type Allow Nulls
Problem List
Orders
Encounters
Epic-Clarity
Problem List
Orders
Encounters
Cerner
CPT’s Billed
Billing Diagnosis
IDX
Inclusion and
Exclusion Criteria
for Specific Disease Registry
ETL Package

41
Our First Disease Registry
Our Experience Building a Disease Registry

42
Agenda
NMFF Overview
Epic Implementation History
Patient Registries History and Overview
Our Experience building a Disease Registry
After the Build
Lessons learned

43
Analyzing Disease Registry Data
After the Build

44
Recognizing Bad Data
After the Build

45
Investigating Bad Data
3345 kg = 7359 lbs
Hello, CNN?
After the Build

46
Strategies for managing bad data
Reactive Measures
Define the ability to flag erroneous data in the data marts (disease registries)
Eliminate erroneous data from analytical reporting
Proactive Measures
Define feedback mechanism to report bad data in the source system to the appropriate data owner.
Prevent future input of bad data in the source systems
• Add data validations in the user interface.
After the Build

47
Tying it all together
Improvement Opportunity
After the Build

48
Tying Disease Registries back to Point of Care
Ideally disease registry information should be available at point of care
• Guideline-based intervals for tests, follow-ups, referrals
• Interventions that are overdue
• “Recommend next HbA1C testing at 90 days because patient is not at goal for glucose control.”
How do you implement this in Epic?
• Invoke web services within epic programming points to display information inside epic
• Invoke external web solutions within hyperspace
• Write data back in epic
–FYI Flags
–CUIs
–Health Maintenance Topics
–Etc.
After the Build

49
Agenda
NMFF Overview
Epic Implementation History
Patient Registries History and Overview
Our Experience building a Disease Registry
After the Build
Lessons learned

50
Lessons Learned
Clinical Sponsorship is necessary.
Agile development methods are useful in getting user buy-in
• They are quick
• They demonstrate work product
Defining registries shouldn’t be limited to only ICD-9 defined diseases
Try to include the reason a patient is added into a registry.
Measure and Insight can be equally significant to registries other than disease based
Need to prioritize which data sources have highest value (esp. when you have more than one EMR source)
Creating a “data bus” to traverse all available data points will create new opportunities for discovery and research.
After the Build


















