Childhood Brain Tumors · Each year, more than 4,000 brain and central nervous system (CNS) tumors...
18
Childhood Brain Tumors John Crawford, MD, MS* Author Disclosure Dr Crawford has disclosed no financial relationships relevant to this article. This commentary does contain a discussion of an unapproved/ investigative use of a commercial product/ device. Educational Gap Brain tumors are the most common solid tumor of childhood and the No. 1 cause of death among all childhood cancers. The pediatrician is pivotal in both the diagnosis and long- term management of brain tumors. A lack of awareness of the clinical signs and symp- toms of brain tumors may delay diagnosis and worsen patient outcomes. Objectives After completing this article, readers should be able to: 1. Recognize the presenting signs of brain tumor (eg, headache, deteriorating school performance, ataxia, emesis). 2. Recognize the signs and symptoms of craniopharyngioma. Introduction Each year, more than 4,000 brain and central nervous system (CNS) tumors are reported in children age 0 to 19 years in the United States, according to the most recent data from the Central Brain Tumor Registry of the United States. (1) Although the incidence of five per 100,000 person-years is rare compared with other childhood malignancies, brain tumors are the most common solid tumor of childhood. Most importantly, brain tumors are the No. 1 cause of death among all childhood cancers, according to surveillance, epidemiology, and survival data. (2) Childhood brain tumors represent an anatomically and biologically diverse group of neoplasms that can present with both common and unusual symptoms. A lack of awareness of the clinical signs and symptoms of brain tumors may lead to a delayed diagnosis by clinicians. The pediatrician is pivotal in both the diagnosis and long-term management of brain tu- mors. This primary care–focused review will offer a practical overview of childhood brain tu- mors, including diagnosis, classification, management, and both early and late effects. Potential late effects of therapy include neurocognitive deficits, endocrinopathies, vasculopathies, and de- velopment of secondary neoplasms. A greater awareness of the clinical and neurologic warning signs associated with the presence of a brain tumor may allow earlier diagnosis and possibly affect outcomes. Brain Tumor Classification, Epidemiology, and Pathogenesis The current classification of primary brain tumors is based on histologic criteria presented by the World Health Organization (WHO). (3) Brain tumors are broadly classified according to the cell of origin and most commonly are neuroepithelial de- rived. WHO classification categories of primary brain tumors include tumors of the neuroepithelium, cranial nerves, menin- ges, and sella, as well as those of hematopoietic and germ cell origin. Among the neuroepithelial tumors, gliomas are the most common brain tumors of childhood, occurring at an incidence of 1.16 per 100,000 person-years. (1) Gliomas are astrocyte- derived tumors and are graded 1 through 4, according to increasing degree of aggressiveness. Juvenile pilocytic astrocy- toma and diffuse fibrillary astrocytoma represent the majority of low-grade gliomas (WHO grades I and II), whereas anaplastic Abbreviations CNS: central nervous system CSF: cerebrospinal fluid CT: computed tomography MRI: magnetic resonance imaging NF-1: neurofibromatosis type 1 NF-2: neurofibromatosis type 2 WHO: World Health Organization *University of California San Diego and Rady Children’s Hospital, San Diego, CA. Article central nervous system Pediatrics in Review Vol.34 No.2 February 2013 63 by 1617003 on May 11, 2020 http://pedsinreview.aappublications.org/ Downloaded from
Transcript of Childhood Brain Tumors · Each year, more than 4,000 brain and central nervous system (CNS) tumors...

Childhood Brain TumorsJohn Crawford, MD, MS*
Author Disclosure
Dr Crawford has
disclosed no financial
relationships relevant
to this article. This
commentary does
contain a discussion of
an unapproved/
investigative use of
a commercial product/
device.
Educational Gap
Brain tumors are the most common solid tumor of childhood and the No. 1 cause of death
among all childhood cancers. The pediatrician is pivotal in both the diagnosis and long-
term management of brain tumors. A lack of awareness of the clinical signs and symp-
toms of brain tumors may delay diagnosis and worsen patient outcomes.
Objectives After completing this article, readers should be able to:
1. Recognize the presenting signs of brain tumor (eg, headache, deteriorating school
performance, ataxia, emesis).
2. Recognize the signs and symptoms of craniopharyngioma.
IntroductionEach year, more than 4,000 brain and central nervous system (CNS) tumors are reported inchildren age 0 to 19 years in the United States, according to the most recent data from theCentral Brain Tumor Registry of the United States. (1) Although the incidence of five per100,000 person-years is rare compared with other childhood malignancies, brain tumors arethe most common solid tumor of childhood. Most importantly, brain tumors are the No. 1cause of death among all childhood cancers, according to surveillance, epidemiology, andsurvival data. (2) Childhood brain tumors represent an anatomically and biologically diversegroup of neoplasms that can present with both common and unusual symptoms. A lack ofawareness of the clinical signs and symptoms of brain tumors may lead to a delayed diagnosisby clinicians.
The pediatrician is pivotal in both the diagnosis and long-term management of brain tu-mors. This primary care–focused review will offer a practical overview of childhood brain tu-mors, including diagnosis, classification, management, and both early and late effects. Potentiallate effects of therapy include neurocognitive deficits, endocrinopathies, vasculopathies, and de-velopment of secondary neoplasms. A greater awareness of the clinical and neurologic warningsigns associated with the presence of a brain tumor may allow earlier diagnosis and possiblyaffect outcomes.
Brain Tumor Classification, Epidemiology, and PathogenesisThe current classification of primary brain tumors is based on histologic criteria presented bythe World Health Organization (WHO). (3) Brain tumors are broadly classified according to
the cell of origin and most commonly are neuroepithelial de-rived. WHO classification categories of primary brain tumorsinclude tumors of the neuroepithelium, cranial nerves, menin-ges, and sella, as well as those of hematopoietic and germ cellorigin.
Among the neuroepithelial tumors, gliomas are the mostcommon brain tumors of childhood, occurring at an incidenceof 1.16 per 100,000 person-years. (1) Gliomas are astrocyte-derived tumors and are graded 1 through 4, according toincreasing degree of aggressiveness. Juvenile pilocytic astrocy-toma and diffuse fibrillary astrocytoma represent themajority oflow-grade gliomas (WHO grades I and II), whereas anaplastic
Abbreviations
CNS: central nervous systemCSF: cerebrospinal fluidCT: computed tomographyMRI: magnetic resonance imagingNF-1: neurofibromatosis type 1NF-2: neurofibromatosis type 2WHO: World Health Organization
*University of California San Diego and Rady Children’s Hospital, San Diego, CA.
Article central nervous system
Pediatrics in Review Vol.34 No.2 February 2013 63
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

astrocytoma and glioblastomamultiforme represent thema-lignant variants (WHO grades III and IV).
Although there is no histologic distinction betweenadult and pediatric gliomas, there are striking differencesin their epidemiology. Glioblastomamultiforme representsthe most common glioma of adulthood (3.19 per 100,000person-years), whereas juvenile pilocytic astrocytoma is themost common glioma of childhood (0.8 per 100,000 per-son-years). (1)
Three commonly encountered neurogenetic syndromesdiagnosed in childhood (neurofibromatosis type 1 [NF-1],neurofibromatosis type 2 [NF-2], and tuberous sclerosis)have a predisposition for low-grade glioma formationbased on their respective genetic mutations. In the caseof NF-1, children may develop low-grade gliomas of theoptic pathway, cerebrum, cerebellum, and spinal cord.Children who have NF-2 are also at risk for glioma forma-tion but more commonly develop meningiomas, ependy-momas, and acoustic schwannomas. Children who havetuberous sclerosis may develop subependymal giant cell as-trocytomas (WHO grade I) that can obstruct the foramenof Monro, leading to obstructive hydrocephalus.
Aside from a few genetic syndromes with a predisposi-tion for developing CNS tumors (ie, NF-1, NF-2, tuber-ous sclerosis, Li-Fraumeni syndrome, Gardner syndrome,Turcot syndrome, Gorlin syndrome), brain tumor patho-genesis is largely unknown. Brain tumor genesis is mostlikely a consequence of inherited, acquired, and epigeneticphenomena.
In general, patient characteristics such as age and genderare not associated with a predisposition to a brain tumor,with a few exceptions. For instance, CNS germ cell tumorsoccur more commonly in boys (twofold), and pituitary tu-mors are more common in girls (threefold). Although en-vironmental and other epigenetic causes are under intenseinvestigation, there is no proven cause of childhood braintumors aside from the known associated genetic syndromesmentioned earlier.
Tumors of young children (age 0–4 years) most com-monly are of embryonal origin and often are located inthe posterior fossa. The differential diagnosis of posteriorfossa tumors in this age group, listed by decreasing fre-quency, include medulloblastoma, juvenile pilocytic astro-cytoma, ependymoma, and atypical teratoid rhabdoidtumor. In older children, juvenile pilocytic astrocytoma isthe most common posterior fossa tumor, followed bymedulloblastoma.
Across all ages, medulloblastoma (WHO grade IV) isthe most common malignant brain tumor of childhood(0.51 per 100,000 person-years) and the most commonprimary brain tumor in children age 0 to 4 years.
Medulloblastoma is derived from tumor stem cells ofthe external granular layer of the cerebellum and can becategorized according to distinct histologic variants (clas-sic, nodular desmoplastic, and anaplastic large-cell). Re-cent studies have divided medulloblastoma into distinctmolecular subgroups that can potentially be used to pre-dict survival and provide risk-adapted therapies. (4)(5)
A histopathologic and neuroradiographic mimicker ofmedulloblastoma, the atypical teratoid rhabdoid tumor isa highly malignant tumor related to the rhabdoid tumorof the kidney that most often occurs in children age youn-ger than 2 years. (6) Atypical teratoid rhabdoid tumor iscategorized molecularly by a mutation/deletion of thehSNF5/INI-1 gene on chromosome 22q11.2 and can oc-cur outside of the CNS in the kidney and soft tissues.Atypical teratoid rhabdoid tumors can occur in both infra-tentorial and supratentorial locations. The diagnosis is con-firmed by an immunohistochemical lack of INI-1 proteinexpression that distinguishes it from the histologicallysimilar medulloblastoma. The distinction betweenmedullo-blastoma and atypical teratoid tumor is critically importantbecause atypical teratoid rhabdoid tumors can be more ag-gressive, may have poorer survival rates, and may requiremore aggressive therapy than classic medulloblastomas.
Ependymomas are the second most common embryo-nal tumor of childhood (0.29 per 100,000 person-years)and are derived from ependymal cells within the CNS.Ependymoma can be of varying grades (WHO grades Iand III) and locations. They are found more commonlyin the posterior fossa; however, these tumors also can oc-cur in the supratentorial region and in the spinal cord.
With more than 30 histopathologic classifications ofprimary pediatric brain tumors, establishing a diagnosiscan be challenging even for the most experienced pediatricneuropathologist. The current WHO classification systemis helpful with regard to establishing a uniform guidelinefor brain tumor classification and grading, but it is byno means complete. Advances in molecular genetics haveimproved our ability to classify brain tumors based on bi-ologic markers but likely will not replace our current his-topathologic classification for many years. Unfortunately,not all brain tumors are “created equal,” making diagnos-tic and management strategies nonuniform and highly in-dividualized at times.
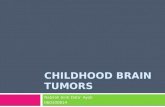
The morbidity and mortality associated with child-hood brain tumors are multifactorial and depend not onlyon tumor pathology but also on location and treatment.Figure 1 lists some of the more common pediatric braintumors according to neuroanatomic location. This list isfar from exhaustive and is meant to demonstrate the di-versity of tumor types based on location. It is also meant
central nervous system brain tumors
64 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

to provide the primary care physician with a general dif-ferential diagnosis in children suspected of having a braintumor in the context of abnormal results on neurologicexamination.
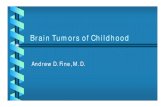
Signs and SymptomsThe presenting signs and symptoms of pediatric brain tu-mors can be incredibly diverse and elusive to the patient,parent, and clinician alike. In general, symptoms arise fromthe neuroanatomic pathways that are disrupted by the tu-mor, as illustrated in Fig 2. The most common symptomreported by children with a newly diagnosed brain tumor isheadache. Headache occurs in approximately one third ofpediatric patients newly diagnosed as having brain tumors.(7) Headache in the absence of other symptoms associatedwith normal neurologic findings does not have reliablepositive predictive value in the diagnosis of a brain tumor.Therefore, the presence of headache alone should not bea “red flag” for this diagnosis.
Nausea and vomiting may occur in approximately onethird of children newly diagnosed as having a brain tumor.(7) However, children who have systemic illnesses such asgastroenteritis, viral meningitis, and childhood migraine allcan present with similar symptoms, and these are far morecommon illnesses than brain tumors.
Children will often present with the triad of headache,nausea or vomiting, and gait imbalance that develops overweeks to months. This triad, with progression of signs
and symptoms, should alert the clinicianto the likelihood of cerebrospinal fluid(CSF) obstruction secondary to a brain tu-mor. In 15% of children newly diagnosedas having a brain tumor, papilledema alsomay be present.
The triad of headache, nausea or vom-iting, and gait imbalance is the mostcommon presentation of posterior fossatumors and is usually accompanied byearly morning vomiting as the definingfeature. The pathophysiology of earlymorning vomiting is related to noctur-nal hypoventilation, hypercarbia, vaso-dilation of cerebral vessels, increasedcerebral blood volume, and increasedCSF production, all during recumbentsleep. Posterior fossa tumors also maypresent with head tilt and torticollis, par-ticularly when there is invasion of theforamen of Luschka.
One of the most difficult presentingsigns of pediatric brain tumors to detect clinically is a visualfield deficit. These defects can be associated with a varietyof suprasellar and optic pathway tumors, including cranio-pharyngioma, optic glioma, and low-grade glioma, toname a few. Often, the visual field deficits in childrenare subacute or chronic and are not readily noticed bythe child or caregiver, regardless of age, until progressionto extreme papilledema and subsequent optic nerve palloror infarction develops.
Similar to visual field deficits, signs and symptoms re-lated to endocrine dysfunction may be present severalmonths before a diagnosis of a brain tumor is made.The more common signs of endocrine dysfunction associ-ated with brain tumors include precocious or delayed pu-berty, anorexia, and excessive urination. These symptomslocalize to a tumor in the region of the hypothalamic-pituitary axis and include pituitary adenomas, germinomas,and low-grade gliomas.
The presence of a new-onset seizure, particularly of focalonset, may be seen in up to 40% of children diagnosed withcortical-based tumors. (7) Although seizures are a commonpresenting feature of brain tumors, the vast majority of sei-zures are due to other systemic or genetic influences. Over-all, a new childhood brain tumor is associated with less than4% of all new-onset seizure presentations.
Occasionally, patients may present with tics, tremors,movement disorders, or learning disabilities that can beconfused with other postinfectious, demyelinating, or neu-rodegenerative diseases. CNS germinomas or low-grade
Figure 1. Common pediatric brain tumor subtypes according to anatomic location.
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 65
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

gliomas of the basal ganglia, midbrain, or deep whitematter in particular are associated with atypical symptoms.
Young children who have brain tumors often are themost challenging patients to diagnose. These childrenwill present with macrocephaly (40%), vomiting (30%),irritability (25%), and lethargy (20%). (7) Macrocephalyusually is detected on routine health visit screeningsand must be distinguished from other familial, traumatic,and neurogenetic causes. Two signs that can be over-looked in young children are failure to thrive and earlyhandedness. In the case of failure to thrive, childrenmay have a prolonged history of poor weight gain with-out an identifiable cause, and despite an exhaustive gas-trointestinal evaluation, eventually neuroimaging revealsa midline tumor. In cases of diencephalic syndrome (aconstellation of severe emaciation, normal or precociousintellectual development, and normal linear growth),a hypothalamic/chiasmatic tumor is present on neuroi-maging that is almost always a low-grade glioma (withor without hydrocephalus). Remarkably, after treatmentwith surgery or chemotherapy, there is marked improve-ment in weight gain that correlates with tumor shrinkage.Early or changing handedness can be a sign of upper mo-tor neuron injury and may be seen with both cortical-based and spinal cord tumors. A list of some of the morecommon warning signs in the presentation of childhoodbrain tumors that may warrant neuroimaging is shown inTable 1.
Neurologic ExaminationA thorough neurologic examination isof paramount significance in the assess-ment of a child suspected of having abrain tumor. The majority of childrendiagnosed as having a brain tumor haveabnormal findings on neurologic ex-amination at presentation. (7) In a busypediatric practice, a focused historyand neurologic examination based onsymptoms can be adequate to raisesuspicion of a brain tumor. The keycomponents of the neurologic ex-amination include evaluation of mentalstatus, cranial nerves, motor skills, sen-sation, reflexes, coordination, and gait(Table 2).
In terms of mental status, an in-creased degree of encephalopathy willmost likely prompt emergent neuroim-aging. However, in patients who havechronic hydrocephalus secondary to
a midbrain tectum low-grade glioma, a history of slowbut steady decline in school performance may be the onlywarning sign.
Examining extraocular movements can be a sensitivecomponent of brain tumor detection, particularly in casesof midbrain, pineal, cerebellar, and brainstem tumors. Par-inaud syndrome, a constellation of findings that includeparalysis of upgaze, pupils that are mid-dilated and poorlyreactive to direct light, convergence or retraction nystag-mus, and eyelid retraction, is commonly seen with dorsalmidbrain tumors. Children who have cerebellar tumors,especially with involvement of the floculonodular lobe, willpresent with nystagmus in any direction. Limited upgazeor upgaze nystagmus is always pathologic and shouldprompt further evaluation.
Another syndrome presenting with abnormal eyemovements worth mentioning in the context of pediatricneuro-oncology is opsoclonus myoclonus syndrome.This syndrome represents a paraneoplastic phenomenoncharacterized by involuntary conjugate eye movements oflarge amplitude and myoclonic jerks; it is usually associ-ated with an extra-CNS neuroblastoma. These childrencan present with a cerebellar syndrome (eg, fast oscillat-ing nystagmus, tremor, ataxia, dysmetria, irritability) inthe absence of neuroimaging findings that may mimica postinfectious syndrome.
As mentioned, visual field abnormalities are common intumors involving the optic pathway (eg, nerves, chiasm,
Figure 2. Common symptoms of pediatric brain tumors according to anatomic location.
central nervous system brain tumors
66 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

tracts, thalamus, radiation, visual cortex) and, if not testedfor, can be missed. (8) The easiest way to assess visual fieldsin young patients is to use two colorful objects. Whilemaintaining central fixation with one object, the secondobject should be placed in each of the four quadrants whilemonitoring for tracking. In older, more cooperative pa-tients, it is necessary that each eye be tested individuallywhile maintaining central fixation to test accurately for vi-sual fields.
A fundoscopic examination is crucial not only in assess-ing for papilledema but also in detecting disc pallor, com-monly seen in tumors involving the optic nerve and chiasmand indicative of optic nerve damage. Both the con-ventional and panoptic ophthalmoscope may be used toperform the fundoscopic examination. The panoptic oph-thalmoscope allows for visualization of the entire disc andgenerally is regarded as more user-friendly than the con-ventional ophthalmoscope. Regardless of the equipmentused, in an uncooperative or young child, a formal dilatedexamination performed by an ophthalmologist may be re-quired to obtain accurate results.
Patients afflicted with brainstem tumors can presentwith a multitude of cranial neuropathies. Facial nervepalsy is a common presentation of most brainstem tu-mors involving the pons. Often confused with havingBell’s palsy, these patients may have other cranial neu-ropathies (eg, esotropia, decreased hearing, drooling,dysphagia) specifically involving abducens, vestibulo-cochlear, glossopharyngeal, vagus, and hypoglossalnerves in isolation or in various combinations. Any pa-tient presenting with new-onset facial palsy should havea thorough neurologic examination to exclude other
cranial neuropathies that wouldraise suspicion for a brainstem tu-mor and prompt immediateneuroimaging.
In terms of motor testing, themost important procedure is to as-sess for possible asymmetries in bulk,tone, and strength. Children whohave longstanding upper motor neu-ron injury secondary to a low-gradecortical, subcortical, or brainstem tu-mor involving the cortical spinaltracts will have increased tone as wellas hemiatrophy of the affected limb.These physical findings can provideuseful clinical insight with regard totumor grade and biologic behavior,because hemiatrophy and hypertoniarepresent longstanding upper motor
neuron injury and correlate with low-grade tumor pathol-ogy. In young children, in whom individual muscle groupsare difficult to test, one can look for hand preference whengrasping for objects. In older children, the presence ofa pronator drift when the arms are extended in supinationwith the hands open is a sensitive test for extremityweakness.
Asymmetries in sensation (cold, light touch, and pin-prick) can be clues to cortical tumors, spinal cord tumors,and, in the case of facial sensation, dysfunction of the di-visions of the trigeminal nerve located throughout thebrain stem.
Evaluation of reflexes can be very helpful, especially ifthere are asymmetries. The upper extremity reflexes (bi-ceps, triceps, and brachioradialis) generally are more diffi-cult to obtain in young children; however, asymmetries arepathologic and can be clues to tumor location. In thelower extremities, asymmetries in the patellar and Achillesreflexes are generally associated with a Babinski response,indicative of upper motor neuron dysfunction.
Coordination testing is extremely important in childrenwho have suspected cerebellar and brainstem tumors. Theclassic finger-to-nose testingmust be performed to assess forcerebellar dysmetria. It is critical for the child to extend theextremity fully and reach for the examiner’s finger. Cerebel-lar testing can be done in both the arms and the legs. Alter-natively, the patient may hold out a finger and mirror theexaminer’s finger movements in the extended position. Thismirror testing is extremely sensitive in assessing cerebellardysfunction, and in the case of patients who have cerebellartumors, will result in an “overshoot” of the movement. Arather quick and sensitive screening test that can be
Table 1. Signs and Symptoms Associated WithDelayed Diagnosis of Childhood Brain Tumors
Signs and Symptoms Tumor Location
Early morning vomiting, recurrentvomiting, enlarging head
Posterior fossa, ventricular system
Failure to thrive, anorexia Suprasellar, hypothalamicVisual complaints, abnormal eyemovements
Optic pathway, suprasellar, brainstem, posterior fossa
Tics, tremor, movement disorder Basal ganglia, thalamus, midbrainEarly handedness Cortex, subcortical, brain stem, spinal
cordFacial nerve palsy Brain stem, cerebellar pontine angleHearing loss Cerebellar pontine anglePrecocious puberty, nocturnal enuresis SuprasellarHead tilt, torticollis Cerebellar pontine angle,
cervicomedullary junction
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 67
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

performed easily is to have the child rapidly tap his fingersagainst his thumbs and his feet on the floor. Asymmetries ofthese fine motor movements may be indicative of cerebellardysfunction, focal motor weakness, or both.
Gait assessment is an important part of the neurologicexamination and can be accomplished solely by observa-tion. Patients who have cerebellar tumors, particularly thoseinvolving themidline cerebellum, will exhibit a classic wide-based ataxic gait, as well as an inability to perform tandemstraight-line walking. Children who have cortical spinaltract involvement will exhibit a hemiparetic gait, with cir-cumduction of the leg and asymmetries in the swing phaseof the arms. In all cases of gait disturbance, it is important toconsider spinal cord tumors in the differential diagnosis.
Finally, it is always prudent to perform a thorough skinexamination, looking for neurocutaneous stigmata of dis-ease. In particular, the presence of café au lait macules andaxillary freckling should raise suspicion for neurofibromatosisand trigger fundoscopic examination and assessment for vi-sual deficits (NF-1) and hearing deficits (NF-2). Patientswho have ash leaf spots, shagreen patches, and facial angio-matosis should undergo head circumference measurementand a fundoscopic examination. In children who haveknown or suspected tuberous sclerosis who present withheadache, vomiting, or irritability, the diagnosis of obstruc-tive hydrocephalus secondary to a subependymal giant cellastrocytoma should be considered.
Neuroimaging Features of Childhood BrainTumorsAny child who has an abnormal result on neurologic exam-ination in the setting of the aforementioned symptomsshould have neuroimaging to rule out a brain tumor. Thechoice of neuroimaging depends on the urgency of thesymptoms and the degree of neurologic abnormality. Chil-drenwhomanifest alteredmental status, behavioral changes,or cognitive decline associated with headache, nausea, vom-iting, and ataxia in the absence of infection should be re-ferred to the emergency department. In these situations,a noncontrast computed tomography (CT) scan of the headgenerally is performed based on availability and urgency.
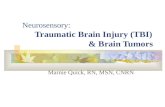
It is important to note that some tumors, particularlytumors of the brainstem, cerebellum, and suprasellar re-gion as well as infiltrative tumors of the white matter,can be missed on CT neuroimaging. Figure 3 shows exam-ples of the CT appearances of various pediatric brain tu-mors with their associated signs and symptoms. CTneuroimaging is sensitive in detecting both blood and cal-cification and continues to have a role in the ongoing man-agement of pediatric brain tumors, often because theremay be no sedation requirement because the length oftime for the procedure is short. Both coronal and sagittalreformatting of CT sequences are available at most centersand can provide additional anatomic information.
Table 2. Key Components of the Neurologic Examination in a Child WhoHas a Suspected CNS Tumor
Examination Pertinent Findings Suggestive of a Tumor
Mental status (level of alertness, speech and language) Encephalopathy, progressive neurocognitive declineCranial nerve 2 (visual fields, fundoscopic examination) Visual field deficit, papilledemaCranial nerves 3, 4, 6 (extraocular movements, efferentpupillary function)
Nystagmus (upgaze in particular), gaze paralysis in anydirection, mid-position, poorly reactive pupils
Cranial nerve 7 (facial symmetry) Facial weakness (upper versus lower motor neurondistribution)
Cranial nerve 8 (hearing, balance) Decreased hearing to finger rub (unilateral or bilateral),vertigo
Cranial nerves 9, 10, 12 (palate elevation, swallowing,tongue movements)
Drooling, dysphagia
Motor examination (bulk, tone, proximal and distal strength) Early handedness, delayed motor milestones, pronator drift,focal changes in tone with associated atrophy
Reflexes (biceps, triceps, brachioradialis, patellar, Achilles) Hyperreflexia with Babinski signCerebellar function (finger to nose testing, mirror testing,rapid finger and toe tapping)
Dysmetria, overshoot on mirror testing, marked asymmetryof finger and/or toe tapping (must be differentiated fromweakness)
Gait (heel, toe, tandem straight line) Wide-based unsteady gait, inability to perform straight-linetest, circumduction of gait
Sensory examination Sensory deficits in a focal anatomic distribution
central nervous system brain tumors
68 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

A CT scan with contrast is rarely necessary in the emer-gency setting of a patient suspected of having a brain tu-mor unless an infectious cause (eg, cerebral abscess) is inthe differential diagnosis. Despite the utility of a CT scanin the emergency setting, magnetic resonance imaging(MRI) is the standard of care for all children who havea known or suspected brain tumor. MRI is the most sen-sitive neuroimaging modality for detecting a brain tumor,with and without intravenous gadolinium contrast. Al-though not every CNS tumor shows enhancement, the ga-dolinium is particularly helpful in detecting those patientswho have disseminated leptomeningeal metastatic diseaseat presentation. Therefore, all children who have newlydiscovered brain tumors on neuroimaging should rou-tinely have an MRI with contrast of the entire spinal axis.Occasionally, abnormalities will be encountered on anMRI that could be consistent with other disorders, suchas demyelinating or postinfectious diseases, which may in-volve the deep white matter, basal ganglia, or thalamus.Under these circumstances, additional MRI sequences,
such as MRI perfusion and spectroscopy, can be used todifferentiate tumor from mimickers. Although not usedroutinely in every case, it is hoped that additional MRI se-quences can be used reliably to distinguish a tumor fromradiation necrosis and help to predict responses to radia-tion, chemotherapy, or biologic therapy.
Although the MRI is an extremely valuable tool in thepractice of neuro-oncology, it has its limitations. For ex-ample, in patients who have orthodontic braces, there isoften magnetic susceptibility artifact that can limit the in-terpretation of suprasellar tumors in particular. In smallchildren, sedation is required to obtain an adequate studybecause motion artifact is common in this age group.
MRIs have been notoriously ineffective at detectingblood and mineralization; however, this limitation is cir-cumvented with newer sequences, including susceptibil-ity weighted imaging. The most significant limitation ofMRI is its inability to render a pathologic diagnosis. Al-though there are specific neuroimaging features of the var-ious pediatric brain tumor subtypes, there is tremendous
Figure 3. Computerized tomography neuroimaging findings and associated symptoms of childhood brain tumors.
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 69
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

overlap, and therefore a specific diagnosis cannot be achievedbased on MRI appearance alone.
With the exception of the CNS germinoma, which candisplay elevations of serum andCSFmarkers (a-fetoproteinand b-human chorionic gonadotropin), the final diag-nosis of a brain tumor is made by histologic examinationafter biopsy or resection.
Examples of MRI neuroimaging features of pediatricbrain tumors with associated symptoms are shown in Fig 4.
Acute Management of the Newly DiagnosedPatientThe management of the child newly diagnosed as havinga brain tumor usually begins in the emergency depart-ment after neuroimaging. In general, the managementof neuro-oncology patients is no different from that ofpatients who have other acute neurologic emergencies.Establishing an airway, sufficient breathing, and effectivecirculation remain the most crucial immediate priorities.
In cases of acute obstructive hydrocephalus with her-niation syndrome, emergent neurosurgical consultationfor either surgical resection or emergent temporizingventricular decompression is required. Preoperative labo-ratory testing should include a complete blood cell count,coagulation studies, and blood type and cross-matching.In the case of suprasellar tumors, it is extremely helpful toobtain baseline electrolytes and endocrine studies beforesurgery, because patients who have large suprasellar tu-mors often have multiple endocrinopathies of both ante-rior and posterior pituitary function.
A baseline ophthalmologic evaluation, including visualfield testing and fundoscopic evaluation, is important inpreoperative evaluations because most patients do notcomplain of visual field deficits at presentation. Depend-ing on the degree of vasogenic edema, intravenous cor-ticosteroids with a gastrointestinal-protective agent aregiven conventionally before and after surgery. Althoughthere is little evidence to support the use of corticoste-roids with regard to overall outcome, corticosteroidscan relieve headache, nausea, and vomiting and remaina generally accepted treatment.
If the diagnosis is based on CT imaging alone, a pre-operative MRI of the brain and spine (with and withoutgadolinium) is necessary for surgical planning and stag-ing. A general schematic of acute management strategiesin patients newly diagnosed with a brain tumor is listed inTable 3.
Equally important in the management of newly diag-nosed patients is providing psychosocial support duringthe initial confirmation of the diagnosis. It is beyond
the scope of the primary care physician or emergency de-partment team to discuss tumor histology, treatmentstrategies, and outcomes. However, it is important tokeep the patients (when appropriate) and parents in-formed of the diagnostic process. This task generally isperformed best in a conference room setting, where neu-roimages can be reviewed with the family and the neuro-surgical/neuro-oncology team may be introduced.
It is common for parents to have extraordinary guiltwhen a brain tumor is diagnosed. It must be emphasizedthat brain tumors occur in children of all ages, races, andgeographic locations, and there is no single cause for devel-oping a brain tumor, a disorder that cannot be prevented.
Parents and clinicians often are plagued with guilt bydelayed diagnosis due to unusual or vague symptoms.There has been no study to date that has correlated earlydetection of pediatric brain tumors with changes in over-all or event-free survival. Children generally present formedical attention when their neurologic symptoms im-pede their ability to play.
Social workers, child life specialists, and neuropsychol-ogists provide critical support to families and patientsduring diagnosis and throughout the course of care.Once a pathologic diagnosis is firmly established, a multi-disciplinary conference is required to review the diagno-sis, treatment plan, and prognosis.
Therapeutic Strategies and OutcomesNeurosurgery generally is the first and most important in-tervention for children newly diagnosed as having a braintumor. The ultimate goal of surgery is to obtain a com-plete resection without postoperative complications.Sometimes a complete resection is not feasible due to tu-mor location, in which case a subtotal resection or biopsyis performed. In children who have posterior fossa tumors(eg, medulloblastoma, juvenile pilocytic astrocytoma,ependymoma), a gross total resection correlates with im-proved event-free and overall survival.
However, the posterior fossa is a potentially dangerouslocation and prone to postoperative complications. Pos-terior fossa mutism syndrome, a constellation of mutism,hypotonia, and irritability, can occur in the immediatepostoperative period and is presumed to be due to mid-line cerebellum connection disruption. Posterior fossamutism can be partially or completely reversible overweeks to months and has been reported with varying de-grees of severity in up to 10% to 20% of children who un-dergo posterior fossa surgery.
In children who have cortical-based tumors (eg, low-grade astrocytoma, ependymoma, oligodendroglioma,
central nervous system brain tumors
70 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

mixed glioneuronal tumors), the goal is to achieve grosstotal resection. In those patients who have high-grade tu-mors of any location, maximum tumor resection and ad-juvant therapy are required, based on the high rate ofreoccurrence and dissemination. In children who havedeep-seated tumors (ie, thalamic, basal ganglia, pineal-tectal tumors), a biopsy often is sufficient to achieve a di-agnosis, and tumor debulking is performed in cases inwhich there is significant mass effect.
In the case of CNS germinoma, a diagnosis can bemade on the basis of elevation of serum or CSF tumormarkers (a-fetoprotein and b-human chorionic gonado-tropin) alone. A biopsy, although generally favored, isnot always required to establish a diagnosis ofCNS germinoma. A gross total resection in childrenwho have extensive craniopharyngiomas can be cura-tive; however, gross total resection is often associ-ated with resulting visual field deficits and multipleendocrinopathies.
Children diagnosed with tectal or pineal tumors oftenundergo a biopsy approach, given the potential risk ofsurgical morbidity, and frequently also receive a CSF di-versional procedure (ventricular peritoneal shunt versusendoscopic third ventriculostomy) in cases of obstructivehydrocephalus. The decision to place a shunt in a childwho has a malignant brain tumor with associated hydro-cephalus sometimes is based on medical necessity, but theprocedure carries a 5% to 7% risk of extraneural seeding.Those who have large posterior fossa tumors frequentlyrequire a CSF diversional procedure because prolongedCSF obstruction is associated with papilledema and po-tential optic nerve infarction.
Despite the precarious location of the tumor, childrenwho have brainstem tumors can undergo safe resection toachieve cure in cases of dorsal exophytic cervicomedullarytumors. Patients who have diffuse intrinsic pontine gli-oma, the most malignant of childhood brain tumors,generally do not undergo biopsy unless enrolled in
Figure 4. Magnetic resonance imaging findings and associated symptoms of childhood brain tumors. CNS[central nervous system.
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 71
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

a clinical trial, because the diagnosis can be made by theappearance of a characteristic expansile mass centered inthe pons with minimal or no contrast enhancement onMRI. Occasionally, a biopsy is warranted in these cases,especially when there are focal, well-defined enhancinglesions, to exclude infectious or demyelinating mimickersof brainstem gliomas.
An additional tumor, optic nerve glioma, can be diag-nosed on the basis of neuroradiographic features alone.These tumors often are low-grade gliomas associated withNF-1 and are seen easily on dedicated MRI sequences ofthe optic nerves. Very rarely, meningiomas and metastaticdisease can present with optic nerve pathology. Childrendiagnosed as having optic nerve gliomas (with or withoutneurofibromatosis) are treated conservatively with observa-tion but undergo chemotherapy if they demonstrate visualdysfunction or tumor progression. In summary, theoutcome for children who have brain tumors is very muchdependent on skilled neurosurgical management toachieve a gross total resection whenever feasible, and suchmanagement remains the ultimate goal for successfultreatment.
Once neurosurgical intervention and sufficient healingof surgical wounds are achieved, additional treatmentsmay be required, including chemotherapy, radiation ther-apy, or a combination of both. These adjunct therapiesare chosen based on the pathologic diagnosis and amountof residual tumor. The nonsurgical management of child-hood brain tumors is complex and depends on the age of
the patient, pathologic diagnosis,degree of residual tumor, presenceor absence of dissemination, andavailability of clinical trials. If thereader is interested in the manage-ment of a specific tumor type, thereare numerous textbooks, publishedclinical trials, and review articles thatoutline the evidence-based manage-ment strategies and controversies ofspecific pediatric tumor subtypes.
For tumors of low-grade histo-logic type in which gross total resec-tion is achieved, no further treatmentis necessary. Children who have re-sidual low-grade tumors generallyare observed for progression. If theydemonstrate growth on surveillanceneuroimaging (every 4–6 months),they are treated with further surgery,chemotherapy, or radiation therapy,depending on age, tumor location,
degree of recurrence, and symptoms. Children who havemalignant gliomas require radiation therapy postopera-tively, in combination with the experimental biologicagents (eg, molecular-based targeted therapy) or oral che-motherapy agents such as temozolomide. The most prom-inent role of chemotherapy is in children who haveembryonal tumors or CNS germinomas and in youngerchildren who have progressive low-grade gliomas.
Based on strong research evidence, (1) it has been shownthat a combination of chemotherapy involving either a two-drug regimen (carboplatin and vincristine) or a four-drugregimen (procarbazine, thioguanine, lomustine, and vincris-tine) can improve event-free survival in children diagnosedwith progressive low-grade glioma. (9)
In children who have embryonal tumors (medulloblas-toma, ependymoma, or atypical teratoid rhabdoid tu-mors), chemotherapy is often used in conjunction witheither focal or craniospinal radiation, depending on theage, degree of dissemination, and tumor pathology. Inchildren who have average-risk medulloblastoma (age>3 years, <1.5-cm2 residual disease, nondisseminated dis-ease, and nonanaplastic histology), a combination of cra-niospinal radiation with adjuvant chemotherapy followedby maintenance chemotherapy is used. Chemotherapycan be used either at standard doses or at higher dosesto achieve greater CNS penetration that would require au-tologous stem cell support secondary to myeloablativechemotherapy. Current trials are underway to investigatethe utility of a reduced dose of craniospinal radiation to
Table 3. General Management Strategy of NewlyDiagnosed Pediatric Brain Tumors
Airway, breathing, circulation stabilizationNeurosurgery/neuro-oncology consultationNPOPresurgical laboratory tests (electrolytes, CBC, coagulation studies, blood type andcross-matching)
Intravenous steroids (dexamethasone) with GI-protective agentMagnetic resonance imaging of the brain and spine with and without intravenouscontrast
Preoperative endocrine laboratory tests for suprasellar tumorsOphthalmologic examinationSeizure prophylaxis for patients presenting with or at high risk for convulsionsSocial work consultation
Lumbar puncture for CSF cytology and tumor markers (for suspected CNSgerminoma) is generally performed 7 to 10 days postoperatively if there are nocontraindications.
CBC¼complete blood cell count, CNS¼central nervous system, CSF¼cerebrospinal fluid,GI¼gastrointestinal, NPO¼nothing by mouth.
central nervous system brain tumors
72 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

prevent long-term sequelae of radiation therapy withoutcompromising survival.
Patients who have high-risk medulloblastomas requirehigh-dose craniospinal radiation of 3,600 cGy with a pos-terior fossa boost, whereas patients who have average-riskmedulloblastomas require either 1,800 or 2,340 cGy ofcraniospinal radiation with a similar posterior fossaboost. Current management strategies of children whohave average-risk medulloblastomas have led to improve-ments of 5-year event-free survival that approach 85% inmultiple international studies. Patients who have high-risk medulloblastomas, unfortunately, have much lowersurvival rates (40%–65%) and are the focus of intenseinvestigation.
The results of adjuvant chemotherapy in patients whohave posterior fossa ependymoma are less convincing thanfor medulloblastoma. Children can achieve durable re-sponses to postoperative radiation alone. Previous studiesin young children who delayed or avoided radiation dem-onstrated recurrence of ependymoma in up to two thirdsof children treated with chemotherapy alone. Phase IIIclinical trials are being conducted to determine whethera combination of focal radiation and chemotherapy willhave synergistic effects.
Children younger than 3 years provide additional chal-lenges for the clinician, regardless of the tumor histology.The long-term effects of craniospinal and possibly evenfocal radiation have led to various management strategiesto avoid or delay radiation therapy. In children who haveembryonal tumors, higher doses of chemotherapy toachieve greater CNS penetrability have been used to de-lay or avoid radiation in a subset of children who haveembryonal tumors. However, high-dose chemotherapyregimens are myeloablative, require autologous stem cellrescue during therapy, and have been associated withtreatment-related morbidity and mortality in a small per-centage of patients. One management strategy currentlyunder investigation is to treat young children whohave posterior fossa embyronal tumors with adjuvantmethotrexate-based chemotherapy followed by involved-field-only radiation therapy, with the option of usingcraniospinal therapy for progressive disease.
Children who have CNS germinomas can be cured byusing a combination of chemotherapy and involved-fieldlower dose radiation that involves the ventricular system, at-taining cure rates of greater than 90%. The malignant coun-terpart of a CNS germinoma, the nongerminomatous germcell tumor (embyronal, immature teratoma, choriocarci-noma, and mixed germ cell tumor), requires a combinationof chemotherapy and craniospinal radiation and is associ-ated with approximately 20% lower 5-year overall survival.
Children diagnosed with diffuse intrinsic pontine gli-oma have the worst survival rate, with greater than 90%mortality by 2 years despite radiation therapy and use ofinvestigational agents. A variety of radiosensitizing bio-logic and chemotherapic agents have been used aloneand in various combinations without improvement insurvival. It is important to realize that not every brain-stem tumor carries this dismal prognosis. Childrenwho have exophytic brainstem tumors can be curedwith surgery or radiation therapy. Children who havefocal brainstem tumors can become long-term survivorsand presumptively have tumors with low-gradepathologic characteristics. Children who have high-gradegliomas in general have similar poor survival rates asthe adult patients and are the focus of numerous clinicaltrials.
Because cranial and craniospinal radiation is com-monly used in both initial treatment regimens and salvagetherapy at relapse, clinicians should be aware of the twomajor types of radiation treatments: photon and protonbeam radiation. Both photon and proton beam irradia-tion use high-energy irradiation to create free radicalsthat deliver preferential damage to tumor DNA becausetumor cells do not have competent enzymatic repaircapabilities. Both modalities use frameless stereotacticnavigation to provide three-dimensional conformal in-tensity-modulated radiation, in which radiation beamsare formed to match the tumor shape. During inten-sity-modulated radiation therapy, the intensity of radia-tion is changed during treatment to spare normalsurrounding tissues.
The concern for photon beam radiation is that therecan be damage to normal surrounding tissue due tothe intrinsic properties of the high-energy particle. Thiseffect is important when targeting sensitive areas suchas the cochlea, temporal lobes, and, in the case of spinalirradiation, the abdominal cavity.
Because of the physical nature of the proton, the radi-ation dosage deposited inadvertently in normal tissues(termed the exit dose) is less and therefore may spare vitalorgans. Children who have suprasellar and malignantposterior fossa tumors theoretically are good candidatesfor proton beam therapy from a neurocognitive stand-point. (10) Only a small number of proton beam centersexist in the United States, however, and therefore notevery child can be treated with proton beam irradia-tion. Ongoing studies are being performed to deter-mine whether there are any benefits of proton beamtherapy with regard to survival or incidence of lateeffects, but these studies will not be completed for manyyears.
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 73
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

Management of Progressive or RecurrentDiseaseThe management of progressive brain tumor disease posessignificant challenges, and pediatricians should be aware ofthe issues that patients and families face. Despite combinedsurgery, chemotherapy, and radiation treatments, a signif-icant proportion of children will have progressive or recur-rent disease. The risk of disease recurrence is dependent onthe patient’s age, tumor pathology, extent of resection,and previous treatment. In children who experience localrelapse, surgery generally is offered, depending on the an-atomic site of relapse. If patients have not received radia-tion therapy to the affected area, radiation generally isoffered. Even when a patient has received previous radia-tion, radiosurgery techniques (stereotactic, highly focusedradiation) have been used to prolong survival.
Most commonly, as with other malignancies, childrenwho experience progressive or recurrent disease are of-fered enrollment in clinical trials. Most clinical trials oftreatments for recurrent childhood brain cancer involvePhase I studies, designed to test a new drug’s safetyand tolerability. The decision to enroll in a clinical trialis a personal one and involves myriad factors, includinggeography, tolerability and mode of delivery of theagents, and quality of life. All clinical trials in the UnitedStates and many international trials are registered onwww.clinicaltrials.gov. These clinical trials can be re-searched by patients, families, and clinicians. Each trialconsists of both inclusionary and exclusionary criteria thatmust be met before enrollment.
Neuro-oncology therapy is changing constantly, andnew clinical trials are added weekly. In patients for whomclinical trials are not an option, combinations of biologicand chemotherapic regimens, with or without radiation,have been used, with varying degrees of success in delay-ing the progression of the disease.
Acute and Subacute Effects of TreatmentThe primary care physician should understand the acuteand long-term effects of brain tumor treatment. Patientsmay have acute treatment-related effects from surgery,radiation, and chemotherapy, depending on the tumortype and therapy received. In the case of surgery, patientscan experience headaches after the surgical procedure.Headaches generally are relieved with anti-inflammatorymedications; however, if fever is present, an abscess or in-fection due to CSF leak must be considered.
Children receiving chemotherapy might experience al-lergic reactions or acute neurologic complaints, such asfoot drop or cranial neuropathies. Children who have
CNS tumors may experience seizures at any time duringtheir treatment. Administering non–enzyme-inducinganticonvulsants (eg, levetiracetam) whenever possible isa requirement for many clinical trials involving investiga-tional drugs.
Children undergoing cranial radiation may experiencefatigue, nausea, or vomiting during their treatment. Onoccasion, stimulant and nonstimulant medications canbe used to treat radiation somnolence. In the case of ra-diation or chemotherapy-related emesis, antiemetic med-ications or low-dose corticosteroids can be very helpful incontrolling symptoms.
The neuro-oncology team manages the usual adverseeffects of chemotherapy on the hematopoietic system(neutropenia, anemia, and thrombocytopenia); however,it is crucial that the primary care physician be aware ofwhen the patient is undergoing treatment to recognizepotential complications of therapy. In children who arereceiving craniospinal radiation, complete blood cellcounts are performed weekly because of the risk for ane-mia associated with marrow disruption due to radiation.
Late Effects of TreatmentImproved patient survival has presented a new era of lateeffects of tumor therapies that the primary care providermust be able to recognize. As with other pediatric malig-nancies, treatment with chemotherapy poses a potentialrisk for future hematogenous malignancies. In childrenwho have received craniospinal radiation, subsequentthyroid cancers, skin cancers, meningiomas, and second-ary high-grade gliomas all have been reported. (11) Un-der these circumstances, a compelling argument can bemade for performing yearly MRI examinations in chil-dren who have undergone previous cranial radiationand are long-term survivors.
Children who have received any form of chemotherapyfor the treatment for a brain tumor are at risk for both he-matogenous and systemic secondary malignancies. High-frequency hearing loss is extremely prevalent in childrenwho have received platinum-based chemotherapies, andsuch children must have routine audiometric evaluations.Other potential late effects of chemotherapy on organfunction include disruption of cardiac, renal, pulmonary,and hepatic function. The effect of chemotherapy on fer-tility of both genders is the subject of current investigation.
Radiation therapy, despite its critical role in the manage-ment of pediatric brain tumors, has the highest number oflong-term sequelae that the primary care physician shouldrecognize. (12)(13)(14)(15) The most common, and per-haps most significant, effect of radiation therapy is its
central nervous system brain tumors
74 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

impact on neurocognition. Children younger than 8 yearsare at the highest risk for radiation-related neurocognitiveinjury. Those patients who receive craniospinal radiationare at risk for declines in IQ of 2 to 4 points per year(10–20 points overall), depending on radiation dosage, tu-mor location, and age of the child. Subsequently, thesechildren often have difficulty with learning and memoryand may require special education services. Studies are on-going to determine whether pharmacologic interventionshave any impact on improving neurocognition in this pop-ulation of children.
Endocrinopathies are commonly seen in patients whohave received either whole brain or suprasellar boosts of ra-diation. Although the hypothalamic-pituitary axis hor-mones often are measured before, during, and aftertherapy, the long-term consequences of treatment-relatedendocrinopathies acquired during childhood are unknown.
Another important long-term neurologic complica-tion specific to children who have received cranial radia-tion is neurovascular disease. Depending on the radiationdose and location, children are at increased risk for cere-bral vasculopathy, including Moyamoya disease, whichincreases the risk for a future stroke. The mechanism ofradiation-related vasculopathy is not entirely known butis different from the atherosclerotic or cardioembolicpathophysiology of stroke seen in adults. Unfortunately,pharmacologic intervention is difficult to apply due to thelack of data on whether preventive therapy (eg, aspirin,cholesterol-lowering drugs, antiplatelet agents) decreasesthe risk of radiation-associated childhood strokes.
Children who have been treated with either chemo-therapy or radiation therapy for a brain tumor may havechronic headaches. These headaches can have features ofmigraines, tension-type headaches, cluster headaches, ora combination of all three. The exact pathophysiologicmechanism and true incidence are not fully understood.A certain proportion of patients will develop chronic dailyheadaches and require both prophylactic and abortiveheadache regimens. Unfortunately, in some cases, it isdifficult to determine whether the headache is relatedto the disease or to the sequelae of treatment. It is impor-tant to recognize that headaches could be a sign of dis-ease recurrence and may be present before there isMRI evidence of progressive or recurrent disease. A thor-ough headache history may be helpful in distinguishingwhether there is a change in the headache pattern frombaseline that warrants neuroimaging.
Less understood late effects of brain tumor treatmentare depression and other psychosocial consequences. Awide range of patients of all ages, with all tumor types,tumor locations, and therapies, are at risk for depression.
It is unclear whether this condition is due to a direct ef-fect of the tumor diagnosis or of therapy. Regardless, pa-tients should be screened routinely for signs and symptomsof depression. Screening can be performed by both theneuro-oncology team and the pediatrician. When depres-sion is suspected, a referral to child psychiatry or initiationof antidepressant therapy may be warranted. In terms ofthe psychosocial consequences of brain tumors, a high di-vorce rate among parents, disrupted sibling relationships,and problems with peer-to-peer interactions have been ob-served. A summary of the common late effects of brain tu-mor therapy is shown in Table 4.
Future of Pediatric Neuro-OncologyThe field of pediatric neuro-oncology is evolving rapidly,thanks in part to the advances in molecular biology. Manycommon primary brain tumors now can be categorizedaccording to molecular markers, which someday soonwill serve as the basis of risk stratification in clinical trials.Our improved knowledge of the molecular mechanismsof neuro-oncogenesis has led to the discovery of an enor-mous number of molecular-targeted therapies (ie, bio-logic agents) that currently are being studied in clinicaltrials for recurrent or refractory disease. These drugsare designed specifically to disrupt known tumor-specificmolecular signaling pathways. It is the hope that one day,more specific targeted biologic therapies will replace con-ventional chemotherapy or radiation in the treatment ofchildhood brain tumors.
One of the great limitations in achieving success of bi-ologic-based treatments is the ability of these drugs to crossthe blood–brain barrier. To overcome this gatekeeper,a number of treatment strategies, including gene-based de-livery systems, immunotherapies, and convection-baseddrug delivery, currently are being investigated.
Advances in radiation oncology are necessary for im-proving neurocognitive outcomes without sacrificing ther-apeutic efficacy. It is unknown whether proton beamtherapy will be superior to conventional photon beam ther-apy, and results may not be known for many years. An im-proved understanding of the molecular mechanisms ofradiation-related neurocognitive injury will allow for the de-velopment and implementation of neuroprotective agents atthe initiation of therapy. Likewise, advances in neu-roimaging will allow detection of tumor reoccurrence ear-lier and more accurate differentiation of treatment-relatedchanges from disease reoccurrence.
Determining the genetic underpinnings of neuro-oncologic disease includes understanding epigenetic fac-tors that govern neuro-oncogenesis. Today, a variety ofmouse models exist that spontaneously and at great
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 75
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

frequency form brain tumors similar to childhood disease.Primary tumor cell cultures have been established for a va-riety of pediatric brain tumors and are being used to studyindividual tumor growth patterns, as well as the potentialresponsiveness of tumors to a variety of chemotherapeu-tic and biologic therapies. As our knowledge of the role ofstem cells in disease formation and progression improves,innovative stem cell therapies may play a role in the futureof neuro-oncologic treatment. It is our belief that one orall of these advances in molecular medicine will allow usto achieve individualized brain tumor therapies for ourpatients and give the best hope for cure.
Role of the PediatricianPediatric brain tumors are a rare but serious disease ofchildhood that require a multidisciplinary approach to di-agnosis, ongoing management, and recognition of lateeffects of treatment. The role of the pediatrician is ex-tremely important in all aspects of brain tumor manage-ment. A heightened awareness of the signs and symptomsof childhood brain tumors in conjunction with a focusedneurologic examination may lead to an earlier diagnosis.Children who are long-term survivors of brain tumors faceunique challenges with regard to a multitude of potentiallate effects of therapy and therefore require meticulouscontinuity of care beyond childhood and into adulthood.
The pediatrician serves as a crucial liaison between pediat-ric and adult medicine in providing continuity of care. It isthe hope that improved understanding of the biology ofdisease will translate into novel therapies and improvedsurvivals of children diagnosed with brain tumors.
References1. CBTRUS, Central Brain Tumor Registry of the United States.CBTRUS statistical report: primary brain and central nervoussystem tumors diagnosed in the United States in 2004-2008.Available at: www.cbtrus.org. Accessed July 12, 20122. Howlader N, Noone AM, Krapcho M, et al, eds. SEER CancerStatistics Review, 1975-2008, Bethesda, MD: National CancerInstitute. Available at: http://seer.cancer.gov/csr/1975_2008/.Accessed July 12, 20123. Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHOclassification of tumours of the central nervous system. ActaNeuropathol. 2007;114(2):97–1094. Leary SE, Olson JM. The molecular classification of medullo-blastoma: driving the next generation clinical trials. Curr OpinPediatr. 2012;24(1):33–395. Kool M, Korshunov A, Remke M, et al. Molecular subgroups ofmedulloblastoma: an international meta-analysis of transcriptome,genetic aberrations, and clinical data of WNT, SHH, Group 3, andGroup 4 medulloblastomas. Acta Neuropathol. 2012;123(4):473–4846. Ginn KF, Gajjar A. Atypical teratoid rhaboid tumor: currenttherapy and future directions. Front Oncol. 2012;2:1147. Wilne S, Collier J, Kennedy C, Koller K, Grundy R, Walker D.Presentation of childhood CNS tumours: a systematic review andmeta-analysis. Lancet Oncol. 2007;8(8):685–6958. Harbert MJ, Yeh-Nayre LA, O’Halloran HS, Levy ML, andCrawford JR. Unrecognized visual field deficits in children withprimary central nervous system brain tumors. J Neurooncol. 2012;107(3):545–549
Table 4. Potential Late Effects ofPediatric Brain Tumor Therapy
1. Endocrinopathy (hypothyroidism, growth hormonedeficiency, corticotropin deficiency, precocious ordelayed puberty, diabetes insipidus)
2. Secondary neoplasms (hematogeneous, skin, thyroid,CNS)
3. Cerebral vasculopathy (stroke, Moyamoya disease,angiitis)
4. Neurocognitive effects (learning, memory, IQ)5. Sensorineural hearing loss6. Scoliosis7. Osteopenia8. Primary headache disorder9. Epilepsy10. Infertility/dysmenorrhea11. Depression/anxiety12. Obesity/diabetes13. Neuropathy14. Ocular effects (vision loss, amblyopia, cataracts)15. Cardiomyopathy16. Renal insufficiency
CNS¼central nervous system.
Summary
• Based on strong evidence, brain tumors, although rare,are the No. 1 cause of death among all childhoodcancers.
• Based on consensus, the morbidity and mortalityassociated with childhood brain tumors aredetermined by many factors, particularly tumorpathology, anatomic location, and treatment.
• Based on strong evidence, headache occurs inapproximately one third of patients newly diagnosedwith pediatric brain tumors.
• Based on consensus, brain tumors are managed bysurgery, chemotherapy, or radiation, depending ontumor type, location and dissemination, and age.
• Based on strong evidence, in treating brain tumors,chemotherapy places the child at risk for futuremalignancies and radiation therapy places the child atrisk for developing neurocognitive deficits.
central nervous system brain tumors
76 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

9. Ater JL, Zhou T, Holmes E, et al. Randomized study of twochemotherapy regimens for treatment of low-grade glioma inyoung children: a report from the Children’s Oncology Group.J Clin Oncol. 2012;30(21):2641–264710. Merchant TE, Hua CH, Shukla H, Ying X, Nill S, Oelfke U.Proton versus photon radiotherapy for common pediatric braintumors: comparison of models of dose characteristics and theirrelationship to cognitive function. Pediatr Blood Cancer. 2008;51(1):110–11711. Armstrong GT, Liu Q, Yasui Y, et al. Long-term outcomesamong adult survivors of childhood central nervous systemmalignancies in the Childhood Cancer Survivor Study. J NatlCancer Inst. 2009;101(13):946–95812. Reimers TS, Ehrenfels S, Mortensen EL, et al. Cognitivedeficits in long-term survivors of childhood brain tumors:identification of predictive factors. Med Pediatr Oncol. 2003;40(1):26–34
13. Spiegler BJ, Bouffet E, Greenberg ML, Rutka JT, Mabbott DJ.Change in neurocognitive functioning after treatment with cranialradiation in childhood. J Clin Oncol. 2004;22(4):706–71314. Mulhern RK, Merchant TE, Gajjar A, Reddick WE, Kun LE.Late neurocognitive sequelae in survivors of brain tumours inchildhood. Lancet Oncol. 2004;5(7):399–40815. Armstrong GT, Stovall M, Robison LL. Long-term effects ofradiation exposure among adult survivors of childhood cancer:results from the Childhood Cancer Survivor Study. Radiat Res.2010;174(6):840–850
Suggested ReadingGupta N, Banerjee A, Haas-Kogan D, eds. Pediatric CNS Tumors.
New York, NY: Springer-Verlag; 2010Keating RF, Goodrich JT, Packer RJ, eds. Tumors of the Pediatric
Nervous System. New York, NY: Thieme Medical Publishers Inc;2001
PIR QuizThis quiz is available online at http://www.pedsinreview.aappublications.org. NOTE: Learners can take Pediatrics in Review quizzes and claim creditonline only. No paper answer form will be printed in the journal.
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physician’s Recognition Award (PRA) and credit system, a minimum performancelevel must be established on enduring material and journal-based CME activities that are certified for AMA PRA Category 1 CreditTM. In order tosuccessfully complete 2013 Pediatrics in Review articles for AMA PRA Category 1 CreditTM, learners must demonstrate a minimum performance levelof 60% or higher on this assessment, which measures achievement of the educational purpose and/or objectives of this activity.
In Pediatrics in Review, AMA PRA Category 1 CreditTM may be claimed only if 60% or more of the questions are answered correctly. If you score lessthan 60% on the assessment, you will be given additional opportunities to answer questions until an overall 60% or greater score is achieved.
1. The symptom that most warrants emergent neuroimaging for a suspected brain tumor in a previously well 4-year-old child is:
A. Episodic vomiting.B. Newly discovered myopia.C. Occasional isolated headache.D. Progressive ataxia.E. Single generalized seizure.
2. A 3-year-old boy presents with a 4-week history of headache, morning vomiting, and a wide-based gait. Hisexamination reveals papilledema, ataxia, and dysmetria. He is most likely to have a:
A. Craniopharyngioma.B. Frontal lobe glioma.C. Medulloblastoma.D. Migraine headache.E. Optic glioma.
3. A 6-year-old girl has been noted to have progressive deterioration of her coordination over the past month andis no longer interested in play. On examination, you note palsy of her left abducens and facial nerves. Yoususpect a brainstem glioma. The best choice as an initial neuroimaging study is:
A. Head computed tomography scan with contrast.B. Head computed tomography scan without contrast.C. Lumbar puncture for opening pressure.D. Magnetic resonance imaging spectroscopy.E. Magnetic resonance imaging with and without contrast.
central nervous system brain tumors
Pediatrics in Review Vol.34 No.2 February 2013 77
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

4. Neurosurgery is an integral part of diagnosis and management of most brain tumors. However, there are twotypes of brain tumors for which surgery is not required to establish a diagnosis. Diffuse intrinsic pontine gliomais one. The other is:
A. Choroid plexus carcinoma.B. Central nervous system germinoma.C. Medulloblastoma.D. Optic glioma.E. Supratentorial ependymoma.
5. The parents of a 12-year-old boy who has received both chemotherapy and radiation for a brain tumor ask youabout late sequelae of those treatments. You explain that hematogenous and secondary systemic malignanciesare a threat to any child receiving chemotherapy, whereas the most common effect specifically attributable toradiation therapy is:
A. Cerebral vasculopathy.B. Chronic headache.C. Depression.D. Impaired learning.E. Seizures.
central nervous system brain tumors
78 Pediatrics in Review Vol.34 No.2 February 2013
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.34-2-632013;34;63Pediatrics in Review
John CrawfordChildhood Brain Tumors
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/34/2/63including high resolution figures, can be found at:
References
1http://pedsinreview.aappublications.org/content/34/2/63.full#ref-list-This article cites 13 articles, 2 of which you can access for free at:
Subspecialty Collections
ogic_disorders_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/neurolNeurologic Disordersogy_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/neurolNeurologyneoplastic_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/cancer:Cancer/Neoplasticlogy:oncology_subhttp://classic.pedsinreview.aappublications.org/cgi/collection/hematoHematology/Oncology_cmehttp://classic.pedsinreview.aappublications.org/cgi/collection/journalJournal CMEfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pedsinreview.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.34-2-632013;34;63Pediatrics in Review
John CrawfordChildhood Brain Tumors
http://pedsinreview.aappublications.org/content/34/2/63located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0191-9601. Illinois, 60143. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by 1617003 on May 11, 2020http://pedsinreview.aappublications.org/Downloaded from