
CHF Winter
36
HealthcareFacilities Journal of Canadian Healthcare Engineering Society INSIDE Canadian Volume 35 Issue 1 Winter/hiver 2014/2015 PM#40063056 Canadian HealthcareFacilities CHES’ National Healthcare Facilities & Engineering Week LED Lighting Retrofits: Sooner or later? HAI Reduction CHES’ National Healthcare Facilities & Engineering Week LED Lighting Retrofits: Sooner or later? HAI Reduction SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS
-
Upload
rick-evangelista -
Category
Documents
-
view
226 -
download
2
description
Â
Transcript of CHF Winter
HealthcareFacilitiesJournal of Canadian Healthcare Engineering Society
INSIDE
Canadian
Volume 35 Issue 1 Winter/hiver 2014/2015
PM#
4006
3056
Canadian
HealthcareFacilities
Fall/automne 2013 1
CHES’ National Healthcare Facilities & Engineering WeekLED Lighting Retrofits: Sooner or later?HAI Reduction
CHES’ National Healthcare Facilities & Engineering WeekLED Lighting Retrofits: Sooner or later?HAI Reduction
SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS
SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS
ASCO: your partner in power.
ASCO Power Technologies Canada • Airport Road PO Box 1238, Brantford, Ontario N3T 5T3Tel: (519) 758-8450 • Fax: (519) 758-0876 • www.asco.com • Division of Emerson Electric Canada Limited Network Power
Call ASCO today foy foy f r morerer infofof rmation on making the switch to smarter powowo ewew r.r.r 519.758.84848 50.
®
At ASCO, we have the products and the expertise to meet all your power challenges: issues like high summer demand for electricity and risks to the environment. By using high-technology power transfer switches to “parallel” your power source, you can manage electricity costs more effectively than ever.
ASCO recently put a solution like this to work for Toronto Hydro, to meet consumers’ needs during summer afternoons when electricity demand and costs are at their peak. By fuel-ing an ASCO power switch with used cooking oil, Toronto Hydro has cut consumption of expensive diesel fuel and significantly reduced emissions. It’s a solution that makes sense...and a switch that could work for you, too.
LO
WER EMISSIONS
EN
ERGY EFFICIENT
UN
M
ATCHED EXPERTISE
LO
WER EMISSIONS
Y EFF
EN
ERGY EFFICIENT
HED E
UN
M
ATATACHED EXPERTIS
E
HED E
ASCOPower-CHES-Summer_Solisco.pdPage 1 5/22/07 11:51:52 AM

Experience and expertise to help you minimize the risk of Legionella
• Copper Silver Ionization: Proven effi cacy, residual protection and easy to maintain.
Terry Runka, Technical Sales Manager253 Orenda Road, Brampton, ON, L6T 1E6905-327-6492 or 1-800-268-0838 x [email protected]
• Safe on-site Chlorine Dioxide Generators: Well documented reduction of biofi lm and Legionella.
• Point of Use Filters: Proven effectiveness during boil water advisories against gram negative bacteria, fungi, and parasites.
• In Line Point of Use Filters: Eliminate water as a source of contamination in making ice and rinsing disinfected parts.
Find out which is the best solution for you:
Water Treatment SolutionsTM
Chem-Aqua offers expertise in…
ChemAqua_CHF_Winter_2014/15.indd 1 15-01-20 12:57 PM
contents
ARTICLES
12 Spotlight on 2014 Canadian Healthcare Projects Looking back on successes that will shape 2015
20 Scenes from the National Healthcare Facilities & Engineering Week Snapshots from across the country
22 Health Sciences Centre's Open House Opening the doors to energy efficiency
24 Engineering Healthcare Acquired Infection Reduction
New innovations for a healthier tomorrow
28 LED Lighting Retrofit: Sooner or later? A case study in retrofit decision making
CANADIAN HEALTHCARE FACILITIES IS PUBLISHED BY UNDER THE PATRONAGE OF THE
CANADIAN HEALTHCARE ENGINEERING SOCIETY
PUBLISHER Kevin Brown e-mail: [email protected]
EDITOR Matthew Bradford e-mail: [email protected]
ADVERTISING SALES Sean Foley, Stephanie Philbin Melissa Valentini MediaEdge Communications 416-512-8186 e-mail: [email protected]
SENIOR DESIGNER Annette Carlucci
DESIGNER Jennifer Carter
PRODUCTION Rachel Selbie MANAGER
SCISS JOURNAL TRIMESTRIEL PUBLIÉ PAR MEDIAEDGE COMMUNICATIONS INC. SOUS LE PATRON-AGE DE LA SOCIÉTÉ CANADIENNE D’INGÉNIERIE DES SERVICES DE SANTÉ
ÉDITEUR Kevin Brown e-mail: [email protected]
RÉDATRIC INTÉRIMAIRE Matthew Bradford e-mail: [email protected]
PUBLICITAIRE Sean Foley, Stephanie Philbin Melissa Valentini MediaEdge Communications 416-512-8186 e-mail: [email protected]
PUBICITÉ Annette Carlucci
COORDINATEUR DE Rachel Selbie PRODUCTION
CHES SCISSCanadian HealthcareEngineering Society
Société canadienne d'ingénieriedes services de santé
PRESIDENT Peter Whiteman
VICE-PRESIDENT Mitch Weimer
PAST PRESIDENT J.J. Knott
TREASURER Robert Barss
SECRETARY Randy Cull
EXECUTIVE DIRECTOR Donna Dennison
CHAPTER CHAIRMEN Maritime: Robert Barss Alberta: Tom Howard B.C.: Steve McEwan Ontario: Allan Kelly Manitoba: Craig Doerksen Newfoundland & Labrador: Brian Kinden
FOUNDING MEMBERS H. Callan, G.S. Corbeil, J. Cyr, S.T. Morawski CHES 4 Cataraqui Street, Suite 310 Kingston, Ontario K7K 1Z7 Telephone (613) 531-2661 Fax (866) 303-0626 e-mail: [email protected] CHES Home Page: www.ches.org Canada Post Sales Product Agreement No. 40063056 ISSN # 1486-2530
Canadian Healthcare FacilitiesVolume 35 Number 1
24
21
13
DEPARTMENTS
6 Publisher's Message
8 Message from the President
10 Chapter Reports
11 CHES Awards: Call for Nominations
01 OPA_10232590_Can_Healthcare_Facilities_VFD CYAN
10232590 B2B Canadian Healthcare Facilities VFD CANADIAN HEALTHCARE FACILITIES
MAGENTA
8.125"x10.875" YELLOW
100% OPA 8.75"x"11.375 BLACK
Bruce E 10232590 7"x9.5"
June 16/14 tl 100% N/A
Blee
d
Trim
Live
Bleed
Trim
Live
Once he reduced his energy costs by 55% after installing a VFD, savings in other parts of his business went into overdrive.Once you start seeing the benefits from our incentives for
installing premium efficiency motors and VFDs, you’ll want
to look into making other areas of your facility like lighting,
HVAC and building automation more efficient too. When you
do, you’ll be joining institutions like Kingston General Hospital,
St. Thomas-Elgin Hospital and Hotel Dieu Hospital who are
already enjoying the energy savings that our incentives deliver.
Take a look at their stories and our incentives at saveonenergy.ca/canadian-healthcare
Subject to additional terms and conditions found at saveonenergy.ca. Subject to change without notice.OMOfficial Mark of the Ontario Power Authority.
6 Canadian Healthcare Facilities
Change. Progress. Potential. With a new year comes fresh opportunities and a chance to reflect on the people, ideas, and achievements that have carried the Canadian healthcare industry forward. That's why we're proud to dedicate a sizeable portion of this first issue of 2015 to the promising developments and events on our radar, while spotlighting just some of the healthcare projects that defined 2014.To begin, Canadian Healthcare Facilities welcomes the return of its Top Canadian Healthcare Projects feature, which highlights a handful of the past year's successes. From the development of the new Hay River Regional Health Centre in the Northwest Territories to the redevelopment of Selkirk Regional Health Centre in Manitoba, and water reduction efforts at the Nova Scotia Hospital Central Laundry to lighting retrofits at Ontario's University Health Network, the projects on display in these pages are sure to inspire. Also in this issue, we look back on the success of CHES' 2014 National Engineering Week and share snapshots from the Health Sciences Centre open house in Winnipeg. Looking ahead, we discuss the future of healthcare acquired infection prevention, take a glimpse at CHES' 2015 National Conference, and review other CHES initiatives.2015 also brings changes to the CHF team, as this will mark my final issue as editor. Since assuming the role in 2011, I have greatly enjoyed collaborating with many of you on content for CHES' Journal, whether it's been working on award articles, project profiles, industry news, or simply helping to bring news of the industry's many successes. The CHES community has been extremely welcoming and knowledgeable, and I'm happy to have had a chance to be part of it.Moving forward, the editor role will fall to Clare Tattersall, a MediaEdge veteran who's experience, enthusiasm, and creativity will bring a fresh energy to this publication.Thank you for your support and warm wishes for the year(s) ahead,
Matthew Bradford
Editor – MediaEdge
Editor's Message
Embracing change, celebrating success
Reproduction or adoption of articles appearing in Canadian Healthcare Facilities is authorized subject to acknowledgement of the source. Opinions expressed in articles are those of the authors and are not necessarily those of the Canadian Healthcare Engineering Society. For information or permission to quote, reprint or translate articles contained in this publication, please write or contact the editor.Canadian Healthcare Facilities Magazine RateExtra Copies (members only) $25 per issueCanadian Healthcare Facilities (non members) $30 per issueCanadian Healthcare Facilities (non members) $80 for 4 issues A subscription to Canadian Healthcare Facilities is included in yearly CHES membership fees.
La reproduction ou l’adaptation d’articles parus dans le Journal trimestriel de la Société canadienne d’ingénierie des services de santé est autorisée à la condition que la source soit indiquée. Les opinions exprimées dans les articles sont celles des auteurs, qui ne sont pas nécessairement celles de la Société canadienne d’ingénierie des services de santé. Pour information ou permission de citer, réimprimer ou traduire des articles contenus dans la présente publication, veuillez vous adresser à la rédactrice.Prix d’achat du Journal trimestrielExemplaires additionnels (membres seulement) 25 $ par numéroJournal trimestriel (non-membres) 30 $ par numéroJournal trimestriel (non-membres) 80 $ pour quatre numérosL’abonnement au Journal trimestriel est inclus dans la cotisation annuelle de la SCISS.
IS YOUR BOTTOM LINE FEELING THE HEAT?
TAKE AIM ON ENERGY AND HEAT LOSS.
IS YOUR BOTTOM LINE FEELING THE HEAT?
TAKE AIM ON ENERGY AND HEAT LOSS.
Properly installed mechanical insulation
saves energy and tons of money. Schedule
an energy audit with one of our techs.
We can quickly show you the savings and
payback using data from the thermal
imaging gun which is uploaded to the
3e Plus Energy Software.
IS YOUR FACILTY WASTING MONEY?
PAYBACKS IN AS LITTLE AS 3 MONTHS!
WE’RE SHOVEL READY TO SAVE, ARE YOU?
INSULATION SAVES AMERICA VALUABLE ENERGY 855-88-ISAVE www.iSAVETEAM.org
The Team
0114 isave ad.qxp_Layout 1 1/14/15 2:38 PM Page 1
8 Canadian Healthcare Facilities
I want to take this opportunity to wish everyone the best this new year, with hopes 2015 brings only the best of health, happiness, and prosperity for you, your family, and loved ones.
I believe “Healthcare Sustainability” is defined as meeting the needs of the present, without compromising the ability of future generations to meet their own needs. Now, there are many contributing factors. Most notably, these are ecological, economics, political, and cultural, which all affect and influence our sustainability. The challenge is adapting and adjusting to these every changing dynamics.
Our healthcare systems are in a constant state of change and are continuously evolving to meet the needs of our stakeholders. Sustainability is most definitely a concern and a priority all across Canada and North America, to which I’m constantly amazed and fascinated by the ingenuity and resourcefulness of our healthcare teams to endure and thrive while developing new processes and technologies to meet this social challenge.
I’m convinced education is paramount in our efforts to develop the skills necessary to meet these ever-changing needs, codes, and standards. Our facility maintenance and operating engineers require interdisciplinary and infrastructure systems thinking capabilities to fully understand what the service requirements are and how we manage our systems to meet these needs effectively.
I also believe the healthcare industry has to be one of the most change-driven industries; technology advancements, codes and standards, programs and services, and environmental and public policy all drive facility management service pressures. To position ourselves to meet these needs, the dissemination of knowledge and the development of skills are absolutely critical and will determine our success in this constantly evolving environment.
The resourcefulness of our facility leaders meeting this challenge coast to coast has been nothing short of phenomenal. Facilities management personnel are always rising to meet these change pressures in a positive and proactive manner all across Canada and North America, providing education sessions in many different formats, from conferences and in-service sessions to web-based distant learning opportunities.
We as an organization need to continue to develop these opportunities. As facility management representatives, we need to ensure our personnel have every opportunity for personal and professional development.
Kindest Regards. Have a great year, work hard, and play hard.
Peter Whiteman CEMPresident CHES National
Message from the President
Making a difference in an “Environment of Excellence”
crit ical th inking
Improve the efficiency and comfort in your health care district? Let the Internet-connected products of Reliable Controls® help you do the analysis. We deliver high performing energy management and control systems for health care districts all across Canada.
Visit our website to request a quote from a Reliable Controls®
Authorized Dealer™ near you and let us help you do some critical thinking.
We are the people and technology you can rely on.
Reliable Controls CorporationHealthare Facilities Magazine - - full page ad dimensions (single page full bleed [8.375” x 11.125”]) - 02.09.09 rev-B
www.reliablecontrols.com
LEED™ 5 year™
w a r r a n t yBACnet® CHES™
m e m b e r
C
M
Y
CM
MY
CY
CMY
K
CHCF mag ad rev-B 2009.pdf 3/25/09 2:55:13 PM

MA
RITI
ME
CHA
PTER
November 4, 2014 was the first meeting of the new
CHES Maritime Chapter Executive. The 2015 Maritime
Spring Conference planning is underway. It will be
held in Halifax. The dates, venue, and theme are being
investigated and will be announced shortly. The chapter
is also investigating the possibility of an Education Day
for mid-winter.
Concerning finances, the present account balance is
$12,000. We expect some additional revenue from the
National Conference surplus. It is worth remembering
that a large portion of the chapter's account money was
used to fund registration of the National Conference
and CHES webinars, contributing greatly to member
PD and certainly increasing chapter attendance at the
conference.
Robert Barss, Maritime Chapter Chair
Chapter ReportsM
AN
ITO
BA C
HA
PTER
ALB
ERTA
CH
APT
ER
I challenge everyone who attended the Saint John, NB CHES National
Conference and those who participated via the tele-conference
last session to do a winter check-up. What have you followed up on
regarding what you saw and heard about at the conference? I know
I still have my checklist, and I have been working on two of the five
things. The value of CHES comes from not just hearing and seeing great
things, but taking them back and putting them into action.
With that in mind, the CHES Manitoba Chapter Executive have
been working further to make the Education Day on Wednesday,
April 21, 2015 into another excellent day where our attendees
will also generate a list of takeaways and implement positive
changes in healthcare. This year’s theme will continue to focus
on maintenance; specifically, with a look at nearly every aspect of
building envelopes, including wall systems, windows, doors, roofs,
below grade water proofing, and humidity control.
The goal is to have attendees take away easy maintenance activities
they can start implementing immediately, or long-term strategic ideas
they can take back to their facilities to begin looking at in terms of
feasibility or funding. We want this year's Education Day to build on the
great ones of the past.
Elsewhere, we plan to continue cooperating with the Canadian
Centre for Healthcare Facilities (CCHF) as they plan for a Manitoba
session to coincide with the MB Education Day.
Craig B. Doerksen, Manitoba Chapter Chair
Hello from Alberta and the new executive team. They include myself,
Tom Howard (chair), Peter Jarvis (vice-chair), Chantel McGeachy
(secretary), Randy Badry (treasurer), and Preston Kostura (past chair).
Honourable mention goes to Ken Herbert who transitioned out of the
past chair spot.
We hosted our annual Clarence White Conference in Red Deer from
November 24 – 25, and it was a huge success. We sold out our 60-plus
booths (as well as turned away a couple late registrants); hosted over
225 delegates; and served meals for 325 guests, including delegates
and vendors staff. It was a great way to set things up for the 2015
National Conference, which is coming to Edmonton from September
20-22, 2015 at the Shaw Conference Centre. Vendor and sponsor
spots are filling up fast for that, so if anyone is interested, don’t delay
in registering.
We will be hosting the CanHCC course in Calgary from June 16-17,
2015. Look for registration information online.
Have a safe and happy New Year with your friends and family!
Tom Howard, Alberta Chapter Chair
10 Canadian Healthcare Facilities
� Structural Engineering
� Building Science
� Structural Restoration
� Parking Facility Design
� Audits & Studies
rjc.ca
South Health Campus: Calgary, AB
BC Cancer Centre for the North: Prince George, BC
New Oakville Hospital: Oakville, ON
ON
TARI
O C
HA
PTER The Ontario Chapter has been extremely busy since my last report. I
have thoroughly enjoyed the position of chapter chair for the last four
years and will hand over the gavel to Roger Hollis at our May conference
in Ottawa.
Our chapter conference will be held in Ottawa from May 24 - 26,
2015, at the Ottawa Conference and Event Centre. The theme of the
conference is “Ideas Start Here”, so please send us your ideas and the
hot topics would you like to see presented. We are hoping to fill the
trade show space with 70 exhibitor booths and, of course, there will be
the great CHES golf game on Sunday to kick it off. We hope to see you
there, and I would like to thank Ron Durocher for taking this on. All the
information is on the CHES website on the Ontario home page.
Our education chair, Rick Anderson, is negotiating with Sheridan
College and will be contributing a $15,000.00 bursary in the coming
months. We are looking at doing a couple of education sessions before
and after our May conference. We will include the details in an e-blast
once they are finalized.
I would like to congratulate Rick Anderson on receiving a Lifetime
Membership Award. This award was presented by Peter Whiteman,
our national president, at the National Annual General Meeting in Saint
John, New Brunswick this past September. We will also be honouring
Rick at our gala banquet in Ottawa for our members who could not
make it to New Brunswick.
This year is an election year. Please consider running for an executive
position as the rewards are infinite. We will be looking for a secretary,
treasurer, and vice chair. Ron Durocher will send the information out to
all members in the new year. The new executive will be introduced at
the May conference in Ottawa
CHES Ontario continues to market and promote this great
organization. We will be having a booth at the Long Term Care Show in
Toronto in April. We hope to attract some long-term care members who
face the same operational problems that other hospitals face on a daily
basis. This year, we will partner with the Canadian Coalition of Green
Healthcare (CCGH). Thanks to Jeff, Jim, and Richard for promoting this.
Membership remains steady and through our education efforts we
are seeing new members join CHES because they see value in what we
do and what we stand for.
Jim Durocher is the new communications chair and will replace
Allen Leyte, who has moved on. Thank you Jim for stepping up to the
challenge and Allen for your past support.
The executive has established a bursary which is open to all
immediate family members of active regular and associate members.
CHES Ontario is very supportive of our colleges who will turn out future
facility managers and support workers for our hospitals. CHES Ontario
wants to give back to our members; with the high cost of education,
this scholarship will help in providing some funds in order to help them
through their education. There will be five $1000.00 bursaries given
out, and the deadline to submit is March 31 of each year. I would like
to thank the committee, led by Rick Anderson, for their hard work on
putting this together. Please visit the CHES website where you'll find all
the information on the Ontario home page.
Lastly, our finances remain strong. The proceeds from our
conferences have allowed us to give back to the members. I would
like to thank Ed Davies for his meticulous accounting processes and
for keeping us on track.
In closing, I want to say that I am very proud of the current executive
for all the hard work they do and look forward to working with the new
executive.
Allan Kelly, Ontario Chapter Chair
Winter/hiver 2014/2015 11
CALL FOR NOMINATIONS FOR AWARDS2015
Hans Burgers AwardFor Outstanding Contribution to Healthcare
Engineering
DEADLINE: March 31, 2015
To nominate:• Please use the nomination form posted on the
CHES website and refer to the Terms of Reference.
Purpose• The award shall be presented to a resident
of Canada as a mark of recognition of outstanding achievement in the field of healthcare engineering.
2015Wayne McLellan Award of ExcellenceIn Healthcare Facilities Management
DEADLINE: April 30, 2015
To nominate:• Please use the nomination form posted on the
CHES website and refer to the Terms of Reference.
Purpose• To recognize hospitals or long-term care facilities that have
demonstrated outstanding success in completion of a major capital project, energy efficiency program, environmental stewardship
program, or team building exercise.
Award sponsored by
For Nomination Forms, Terms of Reference, criteria, and past winners www.ches.org / About CHES / AwardsSend nominations to; CHES National Office [email protected] Fax: 613-531-0626

12 Canadian Healthcare Facilities
THE NEW HAY RIVER REGIONAL HEALTH CENTREBY ERIN GRIFFITHS Delivering healthcare “North of 60˚” was once described as challenging, remote, dangerous, and incredibly unique. As the north evolves and the modernization of healthcare continues, the area remains geographically and culturally unique. While gone are the traditional days of using fishing boats, canoes, and dog sled teams to transport patients, the face of northern healthcare today includes a territorial electronic medical records system, med flights, and aboriginal healing circles.
Hay River, known as the “Hub of The North”, is located in the Northwest Territories (N61˚, W116˚) on the south shore of Great Slave Lake. The community has a population of 3,600 people, with a catchment area of 6,000. The history of health care in the community began with the first settlement of the Dene and the establishment of the Anglican Church in the late 1800s. Health care continued to advance throughout the years from a small room in a local church to a nursing station and then, in 1965, to the current facility, the H.H. Williams Memorial Hospital
H.H. Williams Memorial Hospital has evolved over the years from a six-bed to a 24-bed facility. It has expanded over the last five decades to include a variety of services, such as mental health services, social services, mammography, dialysis, and midwifery. This now aging infrastructure will be replaced by a new state of the art health centre.
The new facility will be a modern health centre designed to support a wide range of services for residents of Hay River and surrounding communities. Construction of the building began in April 2013, with an anticipated completion date in the summer of 2015.
The design-build project budget is approximately $55 million, which will allow the construction of a health centre approximately 6,800 m². The design of the new Hay River Regional Health Centre incorporates the provision of a wide range of health care services such as wellness, health promotion, and prevention. The new Health Centre will be more than a hospital; it will incorporate a primary care clinic; diagnostic services, including mammography; and easier access to, and delivery of, services like the dialysis unit to support the community.
One of the design principles of the new Health Centre is the organization of the flow of staff. A corridor which services the public is considered the “front of house” corridor, while the other major corridor is largely a staff-only service corridor and is considered a “back of house” corridor.
The design has used some of the program space assigned for waiting rooms and placed waiting areas in the “sunny street” to develop bright, open areas with visual connection to the exterior. Clients entering the building will be received by a receptionist.
“Sunny Street has been developed as the main organizing structure of the new Hay River Regional Health Centre,” explains Jan Pierzchajlo from Rockliff Pierzchajlo Architects &
SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS2014 marked another important year in the growth of Canada's healthcare network. It saw a number of new projects, innovations, and redevelopments take shape throughout the country – each advancing the quality of care in their respective regions. And while Canadian Healthcare Facilities has featured a number of these projects within its pages, there are always more to highlight. Here are just a few more successes on our radar...
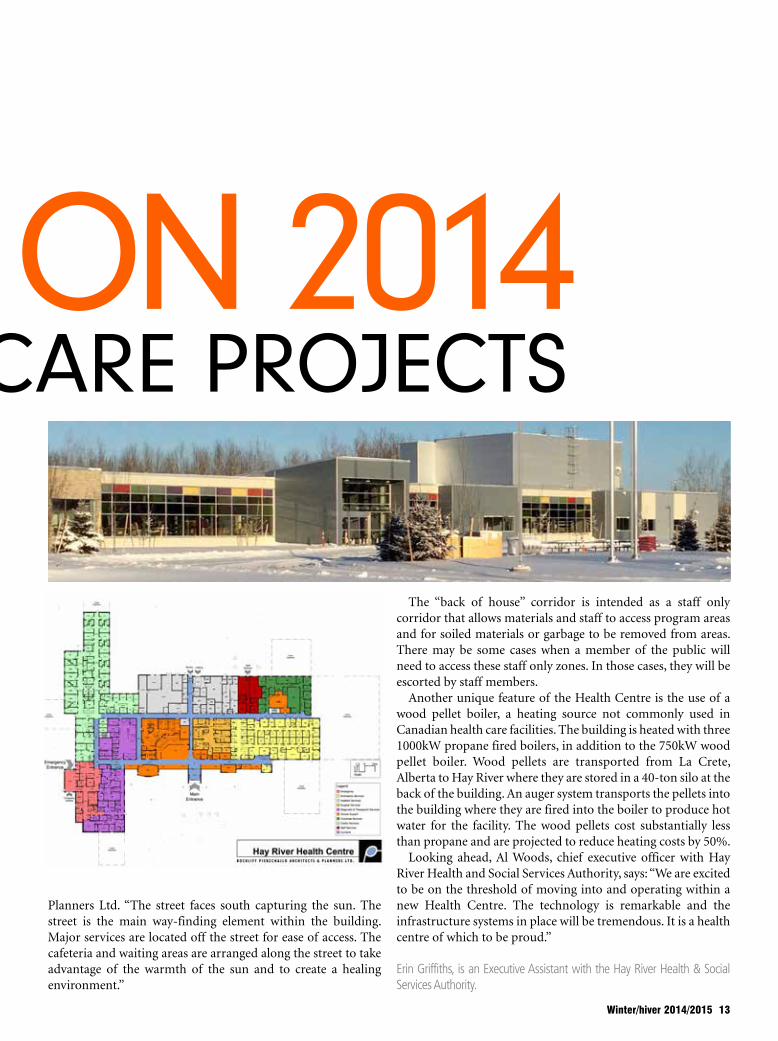
Planners Ltd. “The street faces south capturing the sun. The street is the main way-finding element within the building. Major services are located off the street for ease of access. The cafeteria and waiting areas are arranged along the street to take advantage of the warmth of the sun and to create a healing environment.”
The “back of house” corridor is intended as a staff only corridor that allows materials and staff to access program areas and for soiled materials or garbage to be removed from areas. There may be some cases when a member of the public will need to access these staff only zones. In those cases, they will be escorted by staff members.
Another unique feature of the Health Centre is the use of a wood pellet boiler, a heating source not commonly used in Canadian health care facilities. The building is heated with three 1000kW propane fired boilers, in addition to the 750kW wood pellet boiler. Wood pellets are transported from La Crete, Alberta to Hay River where they are stored in a 40-ton silo at the back of the building. An auger system transports the pellets into the building where they are fired into the boiler to produce hot water for the facility. The wood pellets cost substantially less than propane and are projected to reduce heating costs by 50%.
Looking ahead, Al Woods, chief executive officer with Hay River Health and Social Services Authority, says: “We are excited to be on the threshold of moving into and operating within a new Health Centre. The technology is remarkable and the infrastructure systems in place will be tremendous. It is a health centre of which to be proud.”
Erin Griffiths, is an Executive Assistant with the Hay River Health & Social Services Authority.
SPOTLIGHT ON 2014 CANADIAN HEALTHCARE PROJECTS
Winter/hiver 2014/2015 13

14 Canadian Healthcare Facilities
CAPITAL HEALTH'S LAUNDRY WATER REDUCTIONBY DAVE BLIGHThe Nova Scotia Hospital Central Laundry is the largest laundry operation in Nova Scotia and one of the largest in the Maritimes, operating 364 days per year since the early 1980s with 110 unionized employees. The facility is located on Pleasant St. in Dartmouth and washes, dries, irons, and folds linens for hospitals, long-term care facilities, and commercial clients across Nova Scotia.
The Central Laundry processes an estimated 900,000 lbs of laundry each month, or about 10,800,000 lbs last year. The cleaning process uses approximately 1,600,000 US gallons of water each month, as well as vast quantities of synthetic detergent and weak alkali and acid agents.
Water is heated by steam from the adjacent central heating plant, which usually burns natural gas in three large boilers and supplies the entire Nova Scotia Hospital campus with heat, hot water, and humidification.
In the fall of 2013, the Crothall Healthcare Canada management team at the laundry suggested that it may be possible to reduce the amount of water being used in the laundry process. A review with participants from the Central Heating Plant, Halifax Water
The Nova Scotia Hospital Central Laundry
AquaRecycle System
Commission, Efficiency Nova Scotia, and Engineering and Maintenance concluded that a water recycling system could substantially reduce the amount of steam and water needed, while maintaining the quality of the final product. The Nova Scotia Department of Health and Wellness agreed to provide approximately $300,000 to finance the initiative as a capital project in 2013-2014, and a system built by AquaRecycle was selected for the project.
Five industrial-sized washing machines called washer-extractors run constantly to process such a huge volume of laundry. They work just like consumer models, filling with hot water and detergent and agitating the load, and draining the water when the cycle is complete. The Central Laundry also has an efficient tunnel washing machine, which uses less than one-third of the water needed by the washer-extractors for the same load, but unfortunately is not big enough to handle the all the dirty laundry by itself. Before the recycling system was installed, this water and all the heat it contained would be lost down the drain.
Now, the hot water coming out of the washer-extractors is sent through a series of insulated filtration tanks that remove lint, particulates, oil, soap, and other contaminants. The water is circulated through these tanks and then through a final pass under UV lights to kill any bacteria or viruses that remain by several small efficient pumps.
The system is installed and functioning as expected, with a running average recycle rate of 77% since its commissioning in the spring of 2014. This means that only 23% of the water needed to operate the washer-extractors is being purchased from the utility.
It is difficult to project the annualized savings from the reduction of steam usage due to the volatile nature of natural gas prices, but they are substantial as the water temperature is maintained above 100°F through the recycling process. As less steam is required to heat the process water to the right temperature (165 °F), we can conservatively estimate the monthly savings as approximately 800 GJ, or about $6,500 at current rates. The monthly water utility bills show an average reduction of about 3000 m3 per month ($7,000 at current rates) for a total monthly savings of about $13,500.
With water rates likely to rise again in the near future, this has been a wise and timely investment.
Dave Bligh is an Onsite Energy Manager with Efficiency Nova Scotia
A diagram of the AquaRecycle system

SELKIRK REGIONAL HEALTH CENTRE REDEVELOPMENTBY MATT BRADFORDResidents of Selkirk, Manitoba and its surrounding regions are anticipating the arrival of a new and enhanced healthcare facility under the Interlake Eastern Regional Health Authority (RHA) banner. Planned for completion in spring 2017, the new Selkirk Regional Health Centre will replace the existing Selkirk & District General Hospital with a brand new facility offering more room, a greater slate of services, and access to MRI services.
“The existing infrastructure is just not meeting the needs of the community, so our goal with the new facility is to meet those needs and expand on them in a variety of areas,” says Ron Van Denakker, vice president of corporate services with Interlake-Eastern RHA.
The new centre will be double the size of the existing Selkirk Regional Health Centre at 180,506 square feet. In addition to housing an MRI facility, it will provide a wide range of services, including surgery, obstetrics, medicine, emergency, diagnostics imaging, rehabilitation, community cancer outreach, dialysis, and palliative care.
Construction of the new facility is being led by EllisDon, with designs provided by architectural firms LM Architectural Group and Stantec. It will embrace a more holistic approach to patient care, incorporating natural interior and exterior features, an abundance of natural lighting, and an exterior courtyard which will serve as the central focal point for the centre.
“The amount of natural light in this project is going to be remarkable,” says Andrew Brimble, associate and architect with LM Architectural Group. “What the horizontal approach afforded us is the opportunity to get more natural light throughout the facility, because we can put more things around the exterior itself. Too often,
you lose that light when you get to the middle of a hospital, and you're unable to appreciate the natural exterior, whereas in this hospital, patients and staff will get that as they travel through the corridor systems.”
Other highlights include exterior decks for end-of-life care rooms; an emergency department designed to facilitate faster and more comfortable care; the use of local materials to create a familiar and natural environment, and other holistic elements throughout.
“The design principals were based on providing not only treatment, but also the concept of treating the whole body,” says Van Denakker. “That's embedded in the functional document through the entire building.”
The Selkirk Regional Health Centre is aiming to meet and exceed LEED Silver standards. It will include a number of sustainable features such as high-performance building cladding systems; geothermal fields and heat-pump technology; recycled content building materials; improved indoor air quality measures; and highly efficient plumbing and lighting fixtures.
“LEED Silver is hard to achieve in health care, but the design team has really gone the extra mile in striving to achieve this goal,“ says Gary Dandeneau, regional director of capital planning and facility management.
To date, EllisDon crews have completed 10% of construction, with structural steel installation and exterior wall framing to occur over the winter.
Looking ahead, Van Denakker notes: “We're very proud of the work we're doing, and it's taken a lot of time to get here. It's going to be an absolutely gorgeous facility that's just going to make you feel really good.”
Development moves ahead over the winter on the Selkirk Regional Health Centre
Winter/hiver 2014/2015 15
16 Canadian Healthcare Facilities
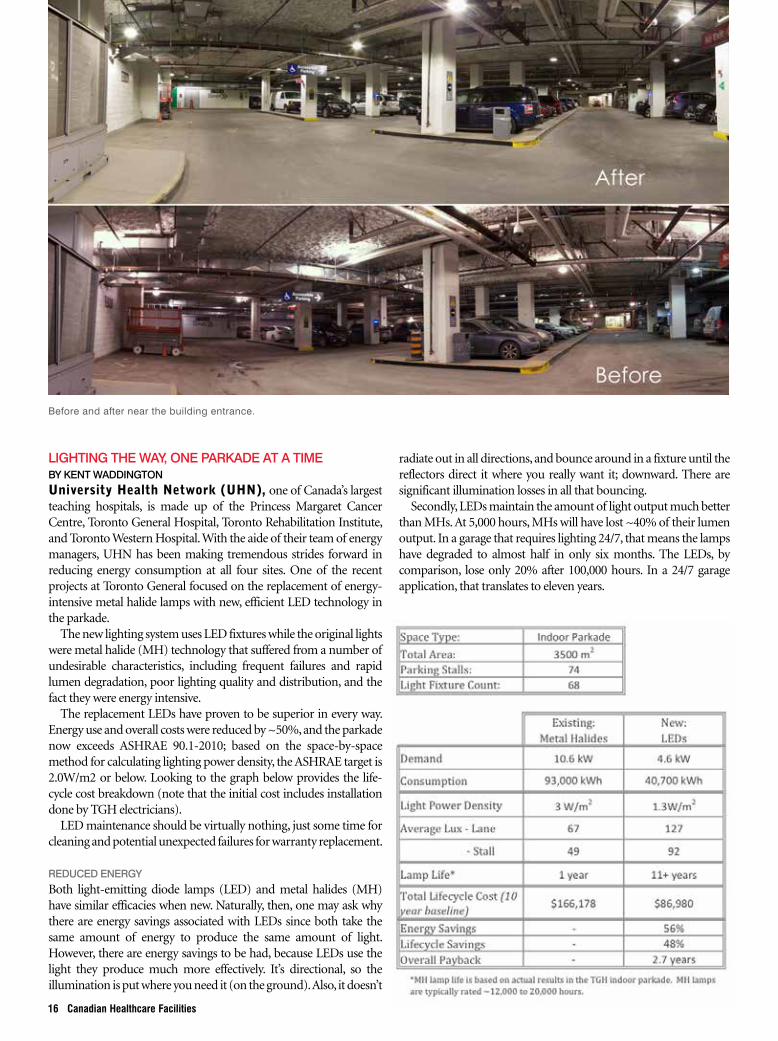
LIGHTING THE WAY, ONE PARKADE AT A TIMEBY KENT WADDINGTONUniversity Health Network (UHN), one of Canada’s largest teaching hospitals, is made up of the Princess Margaret Cancer Centre, Toronto General Hospital, Toronto Rehabilitation Institute, and Toronto Western Hospital. With the aide of their team of energy managers, UHN has been making tremendous strides forward in reducing energy consumption at all four sites. One of the recent projects at Toronto General focused on the replacement of energy-intensive metal halide lamps with new, efficient LED technology in the parkade.
The new lighting system uses LED fixtures while the original lights were metal halide (MH) technology that suffered from a number of undesirable characteristics, including frequent failures and rapid lumen degradation, poor lighting quality and distribution, and the fact they were energy intensive.
The replacement LEDs have proven to be superior in every way. Energy use and overall costs were reduced by ~50%, and the parkade now exceeds ASHRAE 90.1-2010; based on the space-by-space method for calculating lighting power density, the ASHRAE target is 2.0W/m2 or below. Looking to the graph below provides the life-cycle cost breakdown (note that the initial cost includes installation done by TGH electricians).
LED maintenance should be virtually nothing, just some time for cleaning and potential unexpected failures for warranty replacement.
REDUCED ENERGYBoth light-emitting diode lamps (LED) and metal halides (MH) have similar efficacies when new. Naturally, then, one may ask why there are energy savings associated with LEDs since both take the same amount of energy to produce the same amount of light. However, there are energy savings to be had, because LEDs use the light they produce much more effectively. It’s directional, so the illumination is put where you need it (on the ground). Also, it doesn’t
Before and after near the building entrance.
radiate out in all directions, and bounce around in a fixture until the reflectors direct it where you really want it; downward. There are significant illumination losses in all that bouncing.
Secondly, LEDs maintain the amount of light output much better than MHs. At 5,000 hours, MHs will have lost ~40% of their lumen output. In a garage that requires lighting 24/7, that means the lamps have degraded to almost half in only six months. The LEDs, by comparison, lose only 20% after 100,000 hours. In a 24/7 garage application, that translates to eleven years.
Replacing the old 180 and 125 watt MH fixtures with 79 and 53 watt LEDs resulted in not only energy savings of 56% but greatly increased light quality as seen in the images throughout this case study.
*MH lamp life is based on actual results in the TGH indoor parkade. MH lamps are typically rated ~12,000 to 20,000 hours.
FREEING RESOURCES Previously, the MH lamps would last up to one year before needing to be replaced with some lasting only a few months. This meant UHN staff had to constantly monitor which ones had burnt out and be ready to replace them. Replacement, however, was not a straightforward task; it required timing it so there wasn’t a car below the fixture, getting a lift jack in place, wrestling off the heavy class covering, and swapping out the failed bulb whenever one of the 68 fixtures failed.
Less frequently, staff also have to replace the ballasts. With so many other items to attend do on a day-to-day basis, having to spend all this time on garage lighting was an unwelcome time sink. There was also the cost of bulbs to be factored in at $35 each, and the cost of ballasts at $60.
The new LEDs come with a ten year warranty and a L80 life of 100,000 hours. That means they should still be shining brightly eleven years from now, with virtually zero maintenance cost. It’s quite a difference.
BETTER LIGHTThis is perhaps the most important benefit of the new LED lights. When people first arrive at the hospital, staff want it to be a comfortable and safe experience. In the parking garage, this is assisted through proper lighting, which the previous MH lighting failed to provide. Too many parking stalls were dark, lighting was uneven as lamps burnt out, poor light
distribution resulted in bright spots under the lamps which quickly fell off to dark patches, displays and signs were difficult to read, side entrances were always in the shadows, and there were real concerns raised about tripping hazards.
It may sound a little bleak, but this was the reality for some visitors and patients to the hospital -- primarily, people who have difficulty with their mobility or vision, and older patients who need more light as they age. As people age, their eyes need better light to navigate through spaces, therefore improving the light quality was a must.
During the preliminary stage of the project, staff established that the parkade suffered from poor lighting and that it needed to be improved, but they needed to figure out
Offset drain positionkeeps water from splashing directly into drain and aerosolizing contents of the trap.
Oversized backsplashhas coved edges and helps to keep water contained and flowing toward drain.
Sloped rear basin wall minimizes splashing of water stream and creates circuitous flow to drain.
ADACompliant
WILLOUGHBY WICS SERIES
© 20
14 W
illoug
hby I
ndus
tries
Inc.
Designed specifically to minimize splashing
and reduce the spread of infectious disease.
» Information sheet and REVIT files are available at willoughby-ind.com
Sandstone Grey Granite
Bone Glacier White
Red Coral Nocturnal Blue
White Granite
Black Granite
Sea Green
800.428.4065 | www.willoughby-ind.com
Aquasurf® solid surface color options:
Infection Control Sink
Winter/hiver 2014/2015 17

18 Canadian Healthcare Facilities
Rx FOR HOSPITALSECURITY
www.commissionaires.ca/healthcare1 877 322 6777
Protect your hospital environment. Keep your patients, staff and visitors safe with the Commissionaires team of dedicated security profes-sionals.
Commissionaires offers:
• Security Guarding• Parking Control• Mobile Patrol• Access Control/Reception• Courteous, professional customer
assistance
You can count on Commissionaires. Many are former military and ex-RCMP, superbly trained and experienced to respond to your security needs.
exact ly how they would def ine ‘improvement’. To do that, they needed to know what good lighting really was, and then use that information to establish some goals and targets.
First, they looked at standards for covered and enclosed parking areas as articulated by IESNA (Illumination Engineering Society of North America), the Ontario Building Code, and the Toronto Municipal Code; all of which it was learned have similar minimum requirement of 50 lux for general parking areas (IESNA lists 54).
IESNA clarifies that recent practice suggests a target between 85 and 110 lux is more suitable for a well- designed facility. They further provide targets for specific areas such as ramps, corners, entrance areas, and stairs. From this information, UHN created the following specific workable targets: • Parking stalls – 85 to 110 lux (absolute
minimum 50+ lux) • Driving lanes and pathways - 100+ lux
Next, the team looked at how light was distributed through the space with the
goal of improving lighting uniformity. The existing fixtures produced quite the patchwork of light, with relatively well lit areas clashing with dimly lit areas, both on the floor and on the ceiling. Numerous dark walls and corners made the parkade seem even darker than it was.
Light distribution was the problem; that, and fixtures that kept burning out. Lighting fixtures need to work in conjunction with the space, since they rely on surfaces in the space to reflect the light around and back into our eyes. In the case of the Peter Munk Building , they were faced with predominantly grey concrete walls and a ceiling of fibrous grey fireproofing; the light didn’t stand a chance. What they needed were light fixtures that provided light directly where it was needed, in a wide angle of distribution, and with minimal light bouncing off walls and ceilings.
After numerous sample tests, the Philips QLP G3 LED fixture they have installed now proved to be the preferred solution, providing a wide distribution and a visually-pleasing light throughout the entire space. Enough light even
bounces back up so that the ceiling isn’t too dark.
Post-installation measurements verified that the targeted lux values were all met and exceeded, the floor was well lit, the walls and corners illuminated, and the entrances were bright and inviting. The LED upgrade greatly improved light quantity and quality, freed up maintenance resources, saved energy, and helped further reduce UHN’s ecological footprint.
With assistance from Toronto Hydro, UHN also applied for and received a financial retrofit incentive through the Ontario Power Authority’s saveONenergy program. They pursued the Custom Lighting Retrofit incentive which proved to be a very straightforward application process that resulted in a total incentive of $2,615, or $0.05/kWh.
Kent Waddington is Communications Director with the, Canadian Coalition for Green Health Care. Thanks to Chad Berndt, P.Eng, CEM, LEED AP, Energy Project Manager at University Health Network for providing the photographs and content for this case study.

The CHES 2015 National Conference will be held in Edmonton AB at the Shaw Conference Centre, September 20-22, 2015.
The theme of the 2015 conference is “HEALTHCARE FACILITIES AND THE TECHNOLOGY HIGHWAY” The CHES 2015 Education Program will once again be jam-packed with talks on relevant industry topics from high-profile experts in the field.
Our Conference will commence with the Opening Reception at the At Gallery of Alberta on Sunday September 20, 2015, join us for food, friends and fun! Again, in 2015, we will be holding the Great CHES Golf Tournament on Sunday September 20, 2015 at Northern Bear Golf Course – A Jack Nicklaus Signature Course! Join us for the CHES President’s Reception and Gala Banquet again in 2015! We will again celebrate the accomplishments of our peers at the Award Dinner.
We look forward to seeing you in Edmonton in 2015!
For more info visit our website at www.ches.org
Follow us on Twitter!
@CHES_SCISS
SCENES FROM NATIONAL HEALTHCARE FACILITIES &
ENGINEERING WEEK ENGINEERS ON DISPLAY ACROSS CANADA
This October, healthcare engineers and professionals across Canada took to the hallways, boardrooms, and mechanical rooms in celebration of National Healthcare Facilities & Engineering Week (NHFEW).
20 Canadian Healthcare Facilities
Held between October 19 to 25 at numerous facilities across the country, the week was held to expose non-engineering professionals to the engineering staff, systems, and processes that drive their facilities forward. Each event included onsite tours, expert-led presentations, and networking events throughout the day.
Over at St. Michael's Hospital in Toronto, Ontario for example, Quinton D'Mello, manager of engineering and plant services, and his planning team oversaw an Engineering Week event which included a staff breakfast, tours to the mechanical and electrical room tours, awareness videos on themes like “water hammering”, educational displays, and tours of key facility systems.
“The event is very important to the industry because it brings awareness
South Shore Regional Hospital (Bridgewater, NS): Tom Hanley, Steve Robar, Billy Peck, John Mulley, Dave Ackman
SCENES FROM NATIONAL HEALTHCARE FACILITIES &
ENGINEERING WEEK ENGINEERS ON DISPLAY ACROSS CANADA The staff at St. Michael's Hospital gather for National Engineering Week. The planning team included Quinton D'Mello, How-Yune Chong, Nancy
Dempsey, Ron Shakespeare, Maurice Rotsaert, and Ken Jones
Queens General Hospital (Liverpool, NS): Ryan McCarthy, Randall Harnish
Fishermen’s Memorial Hospital (Lunenburg, NS): Tim Chiasson, Ron Hatt, Steve Mader, Andrew Frelick, Danny Dares, John Mulley
Winter/hiver 2014/2015 21
to non-engineering staff and visitors in a hospital environment,” said D'Mello. “All of our staff were very impressed with what we do. For instance, we had our building automation system on display and staff were very fascinated by how we control their workspace, temperature, and humidity level.”
Other CHES teams experienced similar successes. Enjoy the snapshots from various healthcare facilities in this spread and look for upcoming details on National Healthcare Facilities & Engineering Week (NHFEW)

Presented by the
Canadian Healthcare Engineering Societyin partnership with ASHE.
St. John’s NL – May 26-27, 2015Whistler BC – June 10-11 2015Calgary AB – June 16-17, 2015Toronto ON – October 21-22, 2015
Check website www.ches.org for other dates & locations that may be offered in the future.Registration is available online.
For further information:CHES National Offi ceTel: 613-531-2661 | Fax: [email protected] | www.ches.org4 Cataraqui Street, Suite 310Kingston ON K7K 1Z7 Canada
www.ches.org
Canadian Healthcare Construction Course
22 Canadian Healthcare Facilities22 Canadian Healthcare Facilities
On October 2, 2014 Health Sciences Centre in Winnipeg opened the doors of their leading , energ y ef f ic iency second Central Energy Plant for staff and community tours. The grand opening featured self-guided tours through six stops in the facility, along with a trivia ballot about the plant's d e s i g n , o p e r a t i o n , a n d efficiency.
Over 200 visitors toured the facility, asking HSC staff and design engineers technical questions while learning how the fac i l i t y suppor t s the campus. Manitoba Hydro and SMS Engineering were also at the opening to highlight their involvement in the success of the project.
Overall, the 34,000-square-foot building and its technical systems are expected to save HSC $185,000 a year. Read the full case study in the summer 2 0 1 4 i s s u e o f C a n a d i a n Healthcare Facilities.
Christie Nairn is Environmental Sustainability Coordinator with Health Sciences Centre Winnipeg.
By Christie Nairn
HEALTH SCIENCES CENTRE OPEN HOUSE
HSC and MB Hydro work together to optimize efficiency at the energy plant.
The official switch flipped by HSC’s Chief Operating Engineer, Gerry Hebert with support from (left to right) Dale Friesen (Manitoba Hydro), Craig Doerksen (Facility Management, HSC), Dana Erickson (Chief Operating Officer, HSC) and Andy Lohse (SMS Engineering).
Presented by the
Canadian Healthcare Engineering Societyin partnership with ASHE.
St. John’s NL – May 26-27, 2015Whistler BC – June 10-11 2015Calgary AB – June 16-17, 2015Toronto ON – October 21-22, 2015
Check website www.ches.org for other dates & locations that may be offered in the future.Registration is available online.
For further information:CHES National Offi ceTel: 613-531-2661 | Fax: [email protected] | www.ches.org4 Cataraqui Street, Suite 310Kingston ON K7K 1Z7 Canada
www.ches.org
Canadian Healthcare Construction Course
ENGINEERING HEALTHCARE ACQUIRED INFECTION REDUCTION
Healthcare Acquired Infections (HAIs) are the fourth leading cause of death in Canada after heart attacks, cancer, and stroke. Thirty years ago, the chance of catching an HAI as an in-patient in a Canadian hospital was about 2%. Today, it’s over 10%.
By Barry Hunt
Unless we take action, the odds of becoming infected in thirty years will be one in four. Moreover, the cost of treatment for each infected person has risen from a few hundred dollars to over $20,000 with no end in sight. By 2050, the total cost of treatment for HAIs in Canada could approach $40 billion dollars.
For years, we have focused primarily on asking staff to wash their hands and wear gowns and gloves for known infectious cases. Obviously, we need to do more. Albert Einstein once said:
“The definition of insanity is doing the same thing over and over and expecting different results”. In the 90s, Dr. Robert Weinstein also said the following about infection control: “Given the choice of improving technology or improving human behaviour, technology is the better choice”.
I would agree, but argue that we need to combine both technology and behaviour change. Also, thought. Therefore, we need engineering.
The Coalition for Healthcare Acquired Infection Reduction
24 Canadian Healthcare Facilities
Bacteria Distance 5’ 6’ 7’ 8’ 9’ 10’
mW/cm2 1314 999 778 620 504 417Klebs Pneumonia Seconds 18 24 30 42 48 60
VRE Seconds 30 36 42 54 66 78
MRSA Minutes 1.2 1.6 2.1 2.6 3.2 3.8
C diff Minutes 4.6 6.0 7.7 9.7 11.9 14.4
(CHAIR) has identified several practical and cost-effective strategies to achieve the goal of reducing 80% of HAIs in Canada by 2024. The top three strategies involve both technology and engineering, and each strategy has recently been shown to reduce HAIs by over 50%.
Combining these three engineering strategies with cultural, clinical and practice changes throughout the hospital is key to achieving the goal of an 80% reduction.
1. INTERMITTENT SURFACE DISINFECTION USING UVCCurrent housekeeping practice generally budgets 15 minutes for daily room cleaning, 30 minutes for terminal cleaning between patients, and 45 minutes for terminal cleaning for isolation cases. This results in less than half of surfaces being cleaned, and the surfaces which are cleaned are disinfected to a level sufficient to prevent regrowth, usually within hours with the materials in use today.
The risk of infection can be double if the prior occupant of a patient room had an infection. We need to achieve a Log6 level of disinfection of all surfaces within the patient room to protect incoming patients. UVC can do this easily. In fact, two independent studies published in 2013 showed >50% reduction
in HAIs when a Log6 level of UVC was used to supplement room cleaning between patients.
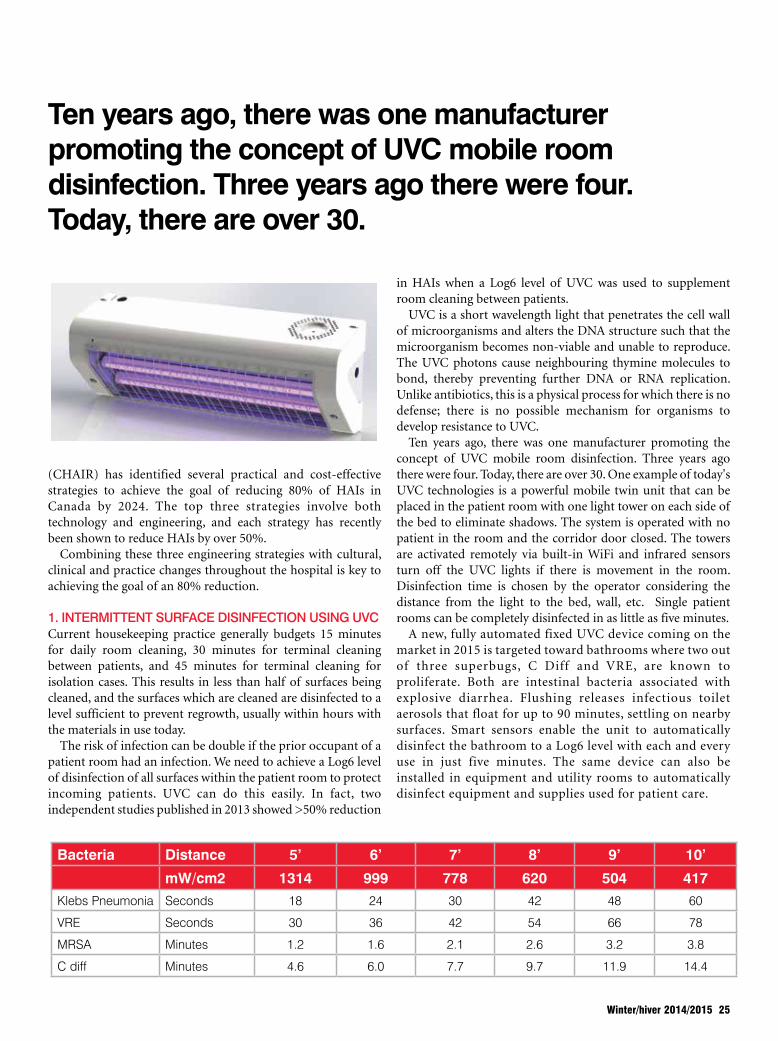
UVC is a short wavelength light that penetrates the cell wall of microorganisms and alters the DNA structure such that the microorganism becomes non-viable and unable to reproduce. The UVC photons cause neighbouring thymine molecules to bond, thereby preventing further DNA or RNA replication. Unlike antibiotics, this is a physical process for which there is no defense; there is no possible mechanism for organisms to develop resistance to UVC.
Ten years ago, there was one manufacturer promoting the concept of UVC mobile room disinfection. Three years ago there were four. Today, there are over 30. One example of today's UVC technologies is a powerful mobile twin unit that can be placed in the patient room with one light tower on each side of the bed to eliminate shadows. The system is operated with no patient in the room and the corridor door closed. The towers are activated remotely via built-in WiFi and infrared sensors turn off the UVC lights if there is movement in the room. Disinfection time is chosen by the operator considering the distance from the light to the bed, wall, etc. Single patient rooms can be completely disinfected in as little as five minutes.
A new, fully automated fixed UVC device coming on the market in 2015 is targeted toward bathrooms where two out of three superbugs, C Diff and VRE, are known to proliferate. Both are intestinal bacteria associated with explosive diarrhea. Flushing releases infectious toilet aerosols that float for up to 90 minutes, settling on nearby surfaces. Smart sensors enable the unit to automatically disinfect the bathroom to a Log6 level with each and every use in just five minutes. The same device can also be installed in equipment and utility rooms to automatically disinfect equipment and supplies used for patient care.
Ten years ago, there was one manufacturer promoting the concept of UVC mobile room disinfection. Three years ago there were four. Today, there are over 30.
Bacteria Distance 5’ 6’ 7’ 8’ 9’ 10’
mW/cm2 1314 999 778 620 504 417Klebs Pneumonia Seconds 18 24 30 42 48 60
VRE Seconds 30 36 42 54 66 78
MRSA Minutes 1.2 1.6 2.1 2.6 3.2 3.8
C diff Minutes 4.6 6.0 7.7 9.7 11.9 14.4
Winter/hiver 2014/2015 25
2. PERSISTENT SELF-SANITIZING SURFACESIn a groundbreaking clinical trial at three major US hospitals, the use of copper on six high touch surfaces (bed rail, IV pole, over-bed table, chair arms, computer keyboard, and monitor) resulted in an HAI reduction of MRSA and VRE of 58% in the ICUs of these hospitals.
The clinical trial was published in the Infection Control and Epidemiology Journal, May 2013. Subsequently, copper and copper alloys have been registered with the US EPA and Health Canada as an antimicrobial product providing Log3 disinfection in less than two hours.
Innovators in this category have developed a copper alloy coating process for hospital furniture surfaces and medical devices. The coating is permanent, won’t tarnish, can be applied to most surfaces and is available in a variety of colours and finishes. These can provide up to Log6 disinfection in as little as 30 minutes.
The success of the US copper trial in preventing infections was due in large part to the fast action of copper ions on the membranes and DNA of bacteria and viruses. 97% of the time, when randomly tested, the surfaces in the ICU trial did not have enough remaining viable organisms to effect transmission. There are many other antimicrobial agents on the market in addition to copper such as titanium dioxide, silver, etc. Generally, however, they are slower to act and often do not show a comparable level of disinfection. Slower-acting, persistent, self-sanitizing surfaces however may be appropriate as an adjunct to copper for floors, walls, and ceilings and other low-touch surfaces.
3. ENGINEERING HVACGenerally speaking, infection comes primarily from the air recirculated within the hospital, not from outside air. However, if HVAC coils, evaporation pans, and filters are not maintained, they can actually add directly to the bioburden of incoming air as well.
Within the hospital, infected patients, visitors and staff shed organisms in patient rooms and bathrooms. Viruses in particular can be airborne in nature (cold, flu, measles, TB) or can become airborne in the form of droplet nuclei when released directly from a patient (sneezing, coughing, talking, suctioning) or from toilet and sink aerosols. Viruses can also be liberated from surfaces where they have previously settled (turbulent air flow, movement of bed linens, curtains and gowns, foot traffic, etc.). Return air provides a path to spread
viruses throughout the hospital as viruses pass through most filters. Studies have also shown that the same organisms found in HVAC ducts settle on the surfaces in patient rooms and are the same organisms found in the tracheas of patients. Return air vents should be filtered at the point of entry to reduce the bioload of pathogens from infected patients, and return air should be treated with UVC to eliminate the viruses which pass through the filters.
Low humidity in indoor air is a major contributor to virus transmission. The total level of virus shedding from patients increases with low humidity. The percent of small particles, known as “droplet nuclei”, expelled with each cough or sneeze also increases with low humidity. Droplet nuclei travel a lot further and persist in the air a lot longer than larger particles. The combined effect is an exponential increase in virus “spreadability” when the humidity drops.
To make matters worse, patients become dehydrated easily in low humidity environments. Their membranes are more easily breached and their immune system responses are compromised resulting in an increase in “susceptibility”. The combined effect of increased spreadability and increased susceptibility is the reason we have a winter “flu season” and “cold season”.
Both spreadability and susceptibility are lowest at ~52% relative humidity (RH). Some facilities already have a policy in place to require 50% RH for burn units, bone marrow transplant units, and ORs, usually at the insistence of clinicians based on their experience with patient outcomes. We should be engineering and operating our HVAC systems to provide 50% RH year round to protect all of our patients.
Reducing the organisms in the HVAC supply reduces infections, particularly in areas with ventilated patients. As reported in the Journal of Perinatology in 2011, the HVAC to the NICU at Buffalo Women’s & Children’s Hospital was supplemented with UVC resulting in a 62% reduction in treatment costs for Ventilator-Associated infections (VAIs). This engineered solution now saves the hospital $850,000 per year.
Another US study on disinfecting HVAC supply air said: “In conclusion, we confirmed the results of two previous studies that demonstrated that an automated UVC device significantly reduced environmental contamination on high touch surfaces in patient rooms.”
In 2009, ASHRAE published its “Top 10” priority list for research into “Airborne Infectious Disease Engineering Control Strategies”. The top 3 items were UVC surface disinfection, UVC disinfection of HVAC air, and UVC disinfection of upper room air in high-traffic public access areas like cafeterias and waiting rooms. The evidence to support both the first and second are already in. Now, it’s time to act.
In the words of Google, engineering is “the branch of science and technology concerned with the design, building, and use of engines, machines, and structures; 2) the work done by, or the occupation of, engineers; 3) the action of working artfully to bring something about”. In the hospital world, it’s time for us to utilize science and technology to work artfully to reduce HAIs.
Barry Hunt is Chairman of the Coalition for Healthcare Acquired Infection Reduction (CHAIR). For more information visit www.chaircanada.org
26 Canadian Healthcare Facilities
Low humidity in indoor air is a major contributor to virus transmission.

Contact Clinicair today to schedule medical-grade duct cleaningand indoor air quality assessment servicesfrom Canada’s only professional airquality specialists.
For a free estimate call 647-777-1044Toll Free: 1-877-318-3588
clinicair.ca
truth is, we’ve made our buildings so energy efficient that dust, humidity, volatile organic compounds and hidden gases are trappedindoors. and unless treated properly and regularly, the air in yourbuildings can become a reservoir for dirt and potentially dangerouscontaminants and a source of irritation for your tenants.
Clinicair is here to help with a specially selected suite of the lateststate-of-the-art services and products to identify and resolve iaQ
problems in multi-unit buildings, businesses, andmedical and dental offices. and every member ofthe Clinicair team attends rigorous training and iscertified by Healthy indoors Partnership (HiP), theCanadian professional iaQ association.
Putting the “quality”back in “air quality.”
Because if your building’s not healthy,neither are your tenants.
CliniCair is Proud to offer
Proud MeMber of
NAT034 Clinicair Air Ad FNL V3_Layout 1 16/08/12 1:33 PM Page 1

Owners are continually faced with questions concerning facility renewals and the right time to proceed. The challenge is deciding whether or not the project meets the corporate criteria. That said, one of the common decisions in today's world is whether they should proceed with LED lighting projects.
To proceed with LED upgrades in the mid 2000s was the same question we asked in the early 1990s when looking at T8 technology. Technology was new, expensive, untested in all areas of use, and did not have the full line of products and features that the other lighting products of the day provided. Now, LED versus T8 or T12 is similar to the question of T8 versus T12 raised in the 1990s.
By Robert Hutton
28 Canadian Healthcare Facilities
LED LIGHTING RETROFIT:
SOONER OR LATER?
Today, however, LED products are coming down in cost. In addition, the quality criteria are much more accepted and tested, the energy requirements are reduced, and product lines now match the varying needs of work spaces.
Turning back to the original question, then, when should you proceed with an LED retrofit? Sooner or later? Perhaps reviewing a parking garage scenario will be helpful for answering this question.
A RETROFIT SCENARIOConsider a recent case study dealing with a parking garage

that was constructed in the early 1970s with a basic, semi-open concrete structure format. It was approximately 200,000 square feet with six floors. The lighting consisted of 370, T12 eight-foot HO fixtures (F96T12/120V), and the condition of the fixtures as of 2009 was poor-to-medium with rust and deteriorating wiring.
Before the retrofit, lighting levels varied from a low of 0.5 fc (foot candles) to a high of 1 fc, which did not meet minimum illumination levels of the building code and engineering best practice/design recommendations for parking structures. Light trespass into the neighbourhood and day lighting controls were also concerns that could be resolved with the current technology. Furthermore, the T12 lighting was obsolete and non-serviceable since legislation banned T12 lamps and ballast production, effective June 2010. In this case study, it was also noted that maintenance was increasing in frequency and cost.
After a lighting survey, LED fixtures were chosen as a replacement strategy and it was determined that 200 new fixtures would be required to replace the T12 units. As a result, predicted benefits included improved lighting levels, therefore meeting the standard, significantly reducing maintenance, and reducing energy costs. Also, it
was understood that LED technology provided a method of lighting control that makes the most use of day lighting, as well as reduces light trespass into the neighbourhood. Lastly, the technology has a 60 to 80K hours of life expectancy before replacement, providing significant operational energy and maintenance savings.
Grant applications for this project from various utility and government agencies were aggressively pursued for both the design and implementation of the project. In Ontario, the Ontario Power Authority has a program which for this scenario would be a ~10% grant, which we included in the costing as a credit to the project cost.
The retrofit project goals were to reduce energy consumption and costs, reduce maintenance costs, reduce CO2 impact, and improve the lighting experience. An LED system would meet these goals.
Replacement of the fixtures with a new LED system would result in a 270421 kWh/year or 75% savings in energy consumption and a 159.1 Tonnes of CO2 reduction. There would be a corresponding energy cost savings.
T12 lamps have an average life of 12000 hours and an average ballast life of five years. Based on a project life of nine years, this would result in a $36,000 cost for
Do you know the quality of medical air being piped to your patients right now?
Quality control for medical air made on‑site is mandatory.
Our unique quality control service provides real‑time, full time traceability and off‑spec prevention.
Ask us how. Contact us 1‑888‑629‑0202.
Winter/hiver 2014/2015 29
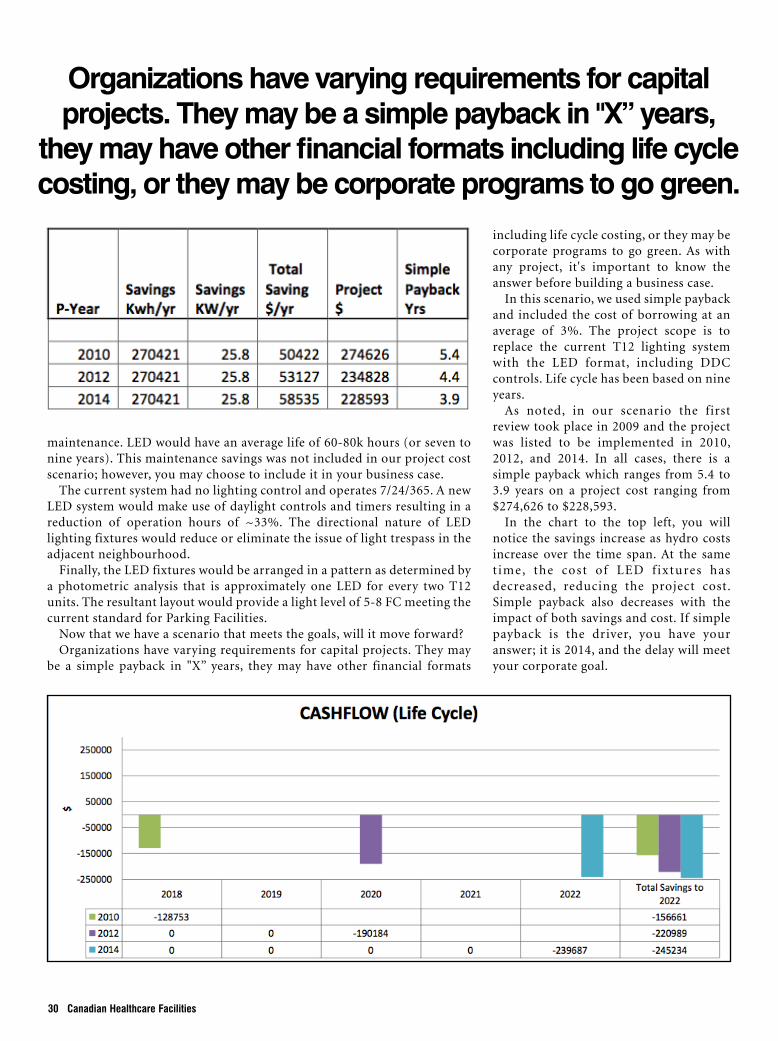
maintenance. LED would have an average life of 60-80k hours (or seven to nine years). This maintenance savings was not included in our project cost scenario; however, you may choose to include it in your business case.
The current system had no lighting control and operates 7/24/365. A new LED system would make use of daylight controls and timers resulting in a reduction of operation hours of ~33%. The directional nature of LED lighting fixtures would reduce or eliminate the issue of light trespass in the adjacent neighbourhood.
Finally, the LED fixtures would be arranged in a pattern as determined by a photometric analysis that is approximately one LED for every two T12 units. The resultant layout would provide a light level of 5-8 FC meeting the current standard for Parking Facilities.
Now that we have a scenario that meets the goals, will it move forward?Organizations have varying requirements for capital projects. They may
be a simple payback in "X” years, they may have other financial formats
30 Canadian Healthcare Facilities
including life cycle costing, or they may be corporate programs to go green. As with any project, it's important to know the answer before building a business case.
In this scenario, we used simple payback and included the cost of borrowing at an average of 3%. The project scope is to replace the current T12 lighting system with the LED format, including DDC controls. Life cycle has been based on nine years.
As noted, in our scenario the first review took place in 2009 and the project was listed to be implemented in 2010, 2012, and 2014. In all cases, there is a simple payback which ranges from 5.4 to 3.9 years on a project cost ranging from $274,626 to $228,593.
In the chart to the top left, you will notice the savings increase as hydro costs increase over the time span. At the same t ime, the cost of LED f ixtures has decreased, reducing the project cost. Simple payback also decreases with the impact of both savings and cost. If simple payback is the driver, you have your answer; it is 2014, and the delay will meet your corporate goal.
Organizations have varying requirements for capital projects. They may be a simple payback in "X” years,
they may have other financial formats including life cycle costing, or they may be corporate programs to go green.

FUEL YOUR KNOWLEDGE
Quench your thirst for industry news and information. With brand new features every day, REMI will nourish your mind, while replenishing your system’s need to be in-the-know. If you’re thirsty for expert advice, our articles will help you excel and give you the stamina to stay ahead of the game.
Canada’s leading news and information source servicing the Real Estate Management Industry
MERGING INDUSTRY LEADING BRANDS
REMI_Fuel_Logos_2014.indd 1 14-09-29 4:11 PM
32 Canadian Healthcare Facilities
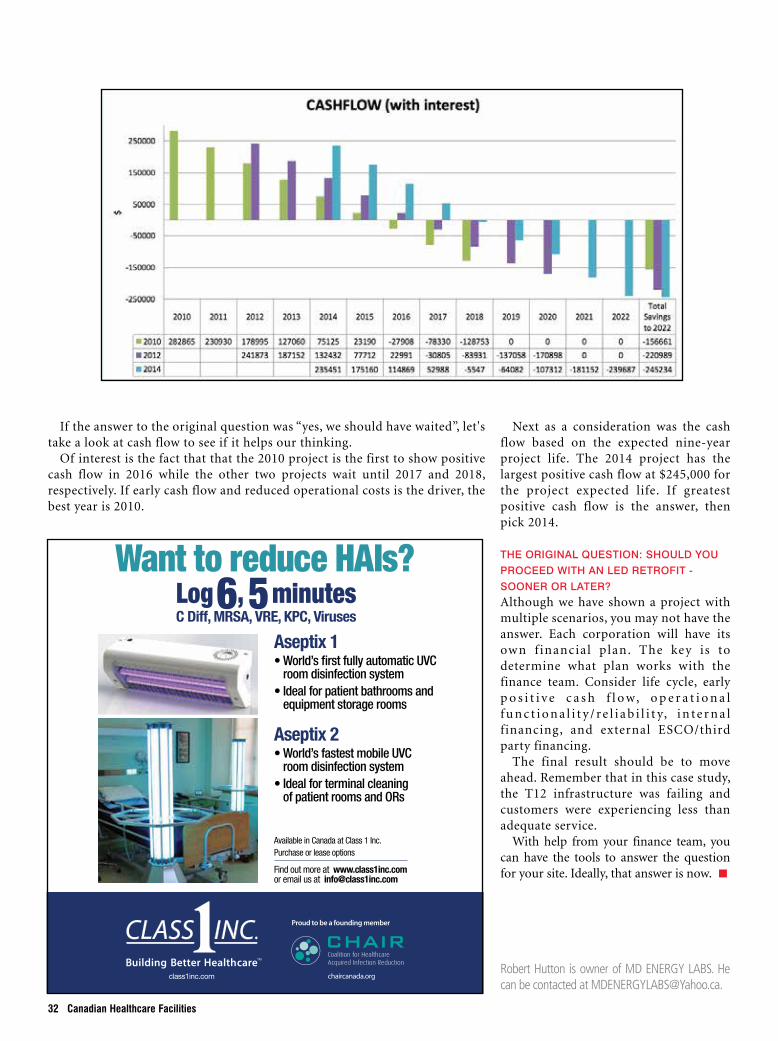
Next as a consideration was the cash flow based on the expected nine-year project life. The 2014 project has the largest positive cash flow at $245,000 for the project expected life. If greatest positive cash flow is the answer, then pick 2014.
THE ORIGINAL QUESTION: SHOULD YOU PROCEED WITH AN LED RETROFIT - SOONER OR LATER?Although we have shown a project with multiple scenarios, you may not have the answer. Each corporation will have its own f inancial plan. The key is to determine what plan works with the finance team. Consider life cycle, early p o s i t i v e c a s h f l o w, o p e r a t i o n a l f u n c t i o n a l i t y / re l i a b i l i t y, i n te r n a l financing, and external ESCO/third party financing.
The final result should be to move ahead. Remember that in this case study, the T12 infrastructure was failing and customers were experiencing less than adequate service.
With help from your finance team, you can have the tools to answer the question for your site. Ideally, that answer is now.
Robert Hutton is owner of MD ENERGY LABS. He can be contacted at [email protected].
Class 1 Inc.Publication: Canadian Journal of Infection ControlSize: 1/3 page horizontal (4.5625” x 4.75”)
Want to reduce HAIs?C Diff, MRSA, VRE, KPC, Viruses
class1inc.com
Proud to be a founding member
chaircanada.org
Log6, 5minutes
Aseptix 2•World’sfastestmobileUVC
roomdisinfectionsystem•Idealforterminalcleaning
ofpatientroomsandORs
Aseptix 1•World’sfirstfullyautomaticUVC
roomdisinfectionsystem•Idealforpatientbathroomsand
equipmentstoragerooms
Available in Canada at Class 1 Inc. Purchase or lease options
Find out more at www.class1inc.com or email us at [email protected]
If the answer to the original question was “yes, we should have waited”, let's take a look at cash flow to see if it helps our thinking.
Of interest is the fact that that the 2010 project is the first to show positive cash flow in 2016 while the other two projects wait until 2017 and 2018, respectively. If early cash flow and reduced operational costs is the driver, the best year is 2010.
The Water Spec ia l i s ts
WWW.KLENZOID.COM
265 Watline Avenue, Mississauga, Ontario L4Z 1P3 Tel: (888) 712-40005830 Côte de Liesse, Suite 100, Ville Mont-Royal, Québec H4T 1B1 TÉL : (514) 342-2121
Proven Solutions for Healthcare Facilities through Service-Intense Water Management Programs
Is your
waterGETTING THE
treatmentIT DESERVES?
www.norspec.comMuira_CHF_Winter_2014-15_FINAL.pdf 1 15-01-15 1:25 PM
Winter/hiver 2014/2015 33
WESTERN FILMMAKER Advertising ProofSuite 121 - 9801 King George Blvd., Surrey, BC V3T 5W5Tel: (604) 581-0559 Fax: (604) 581-5116
PLEASE CHECK: NAmE, AddrESS, TELEPHoNE NumBErS, ALL SPELLiNG. YouR pRooF IS TIME SENSITIvE. Please reply by e-mail or fax to 604-581-5116 upon receipt.
Specifications:Ad Size: 1/4 Vertical Colours: CmYK
proof #: 1
i have carefully proofread this ad and accept full responsibility, with any changes as shown on this proof. i understand that Western Filmmaker is not responsible for any errors or omissions overlooked on my proof if i choose not to sign and return my proof, or after it has been signed. All changes and/or corrections must be clearly indicated and returned by the above date. No reply will result in your ad being printed as shown.
CLiENT SiGNATurE: dATE SiGNEd:
pLEASE RETuRN YouR SIGNED pRooFWESTERN FILMMAKER FAX: (604) 581-5116
❑ APProVEd AS SHoWN, No CHANGES ❑ CorrECTioNS / PLEASE SENd NEW ProoF❑ CorrECTioNS / No ProoF rEQuirEd
AuTHoriZATioN
Proofing Method: Sent by ❑ Fax ❑ mail n E-mail
Client: Caster Town Ltd.Contact: Scott Cluthe
invoice#: WFCC 244
Phone: 604 251 3151E-mail: [email protected]
dATE SENT: 05/11/2014 REpLY BY: 11/11/2014
VANCOUVER1-800-689-1441
CALGARY1-800-665-1348
CasterTown_CHF_Winter_2014/15.indd 1 15-01-20 2:41 PM
2015 Webinar Series
Time: 0900 BC/1000 AB & SK/1100 MB/1200 ON & QC/1300 NS & NB/1330 NL
One hour in length
Wednesday March 25, 2015
Medical Air, What You Need to Know Speaker: Paul Edwards, BCom, Vice President, Sales, Marketing & Business Development, Air Liquide Healthcare
Wednesday April 29, 2015
Energy Efficiency, condensation control and personal protection starts with inspecting mechanical insulation Speaker: Steve Clayman, B.Comm., Director of Energy Initiatives, Thermal Insulation Association of Canada Wednesday October 28, 2015
Combustible Piping in Health Care Facilities Speaker: Patrick McQuire, Technical Represenative, IPEX Wednesday November 25, 2015
Proposed requirements for Z317.2‐15 (HVAC) Speaker: Gordon Burrill, President, Teegor Consulting Inc. Speaker: Nick Stark, Vice President Knowledge Management, HH Angus & Associates Limited
Registration
CHES Member: Non‐Member: Single: $30 + $3.90 HST = $33.90 (per webinar) Single: $40 + $5.20 HST = $45.20 (per webinar)
Series: $90 + $11.70 HST = $101.70 (per series) Series: $120 + $15.60 HST = $135.60 (per series)
Register online:
www.ches.org Professional Development
34 Canadian Healthcare Facilities
www.thermogenicsboilers.com905.727.1901
Untitled-1 1 14-10-30 10:52 AM
We are pleased to announce that Ventcare now monitors 50 plus hospitals in the Ontario region.
Labour Canada has fully “acknowledged” the scope of work provided in the semi-annual inspection program. In addition, the written documentation contributes greatly to the hospital accreditation programs.
Further we are always pooling the knowledge resources of Infection Control and Engineering Groups like CHES, the ventilation inspection program is in a constant evolution to meet future healthcare needs for patients and staff.
The location and inspection of the hospital ventilation fire doors may be part of
your building audit this year. Some of you have already taken advantage
of our new software program which in conjunction with our patented robotics, allows us to minimize ceiling access requirements.
To date, of the thousands of fire doors inspected approximately 30% are not humanly accessible from traditional ceiling
access points. Our patented robot overcomes
this obstacle, allowing complete documentation of all
fire doors within the ventilation system. Further, of the total, 7%
have been found defective, blocked with wood, wired up, or simply closed
shutting off airflow.
Ventilation MonitoringBandy II
“Setting the Standard for Commercial Ventilation Care”
Fire Door Inspection
HEALTHCAREVENTILATION SYSTEMS
What’s really in yours?
75
176 Bullock Drive, Unit 14, Markham, ON L3P 7N1 Tel: 905-201-7887 Fax: 905-201-1340www.ventcare.com
We are pleased to announce that Ventcare now monitors 50 plus hospitals in the Ontario region.
Labour Canada has fully “acknowledged” the scope of work provided in the semi-annual inspection program. In addition, the written documentation contributes greatly to the hospital accreditation programs.
Further we are always pooling the knowledge resources of Infection Control and Engineering Groups like CHES, the ventilation inspection program is in a constant evolution to meet future healthcare needs for patients and staff.
The location and inspection of the hospital ventilation fire doors may be part of
your building audit this year. Some of you have already taken advantage
of our new software program which in conjunction with our patented robotics, allows us to minimize ceiling access requirements.
To date, of the thousands of fire doors inspected approximately 30% are not humanly accessible from traditional ceiling
access points. Our patented robot overcomes
this obstacle, allowing complete documentation of all
fire doors within the ventilation system. Further, of the total, 7%
have been found defective, blocked with wood, wired up, or simply closed
shutting off airflow.
Ventilation MonitoringBandy II
“Setting the Standard for Commercial Ventilation Care”
Fire Door Inspection
HEALTHCAREVENTILATION SYSTEMS
What’s really in yours?
Ventcare CHF.indd 1 27/04/10 2:26 PM


















