Chest Pain Chest Pain Differentiating Causes and Patient Presentations June 2009.
Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
1
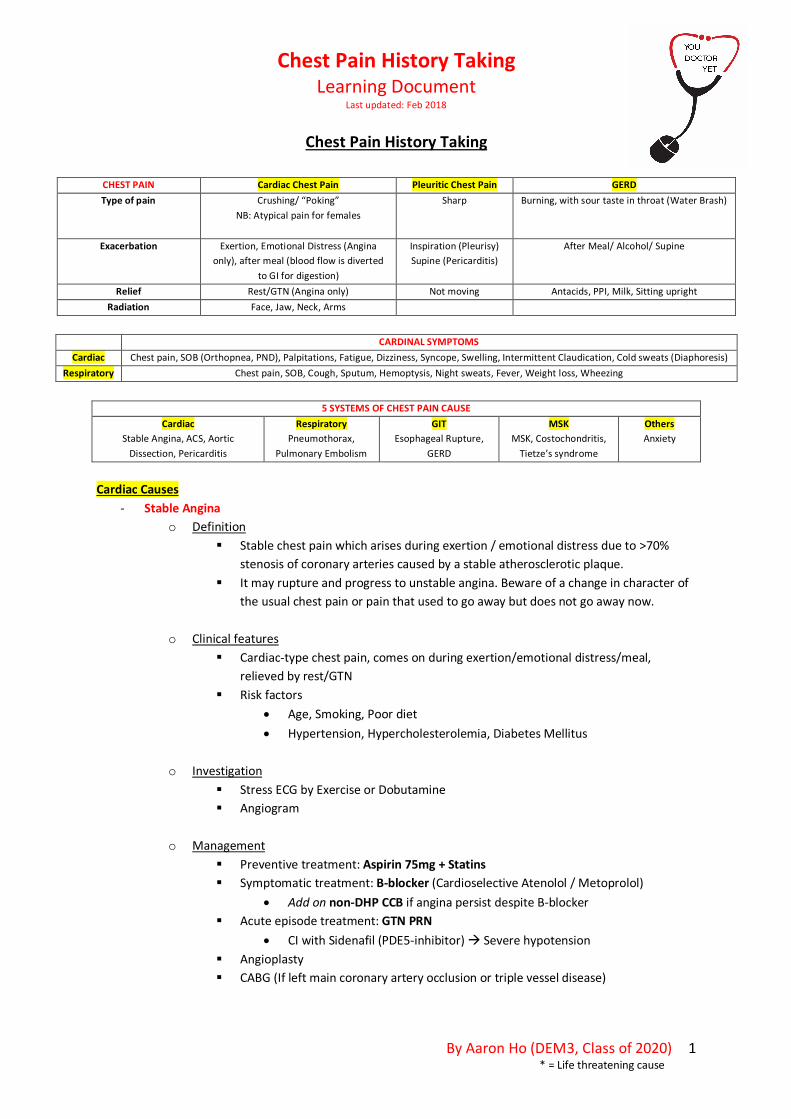
Chest Pain History Taking
CHEST PAIN Cardiac Chest Pain Pleuritic Chest Pain GERD Type of pain Crushing/ “Poking”
NB: Atypical pain for females
Sharp Burning, with sour taste in throat (Water Brash)
Exacerbation Exertion, Emotional Distress (Angina only), after meal (blood flow is diverted
to GI for digestion)
Inspiration (Pleurisy) Supine (Pericarditis)
After Meal/ Alcohol/ Supine
Relief Rest/GTN (Angina only) Not moving Antacids, PPI, Milk, Sitting upright Radiation Face, Jaw, Neck, Arms
CARDINAL SYMPTOMS
Cardiac Chest pain, SOB (Orthopnea, PND), Palpitations, Fatigue, Dizziness, Syncope, Swelling, Intermittent Claudication, Cold sweats (Diaphoresis) Respiratory Chest pain, SOB, Cough, Sputum, Hemoptysis, Night sweats, Fever, Weight loss, Wheezing
5 SYSTEMS OF CHEST PAIN CAUSE
Cardiac Stable Angina, ACS, Aortic
Dissection, Pericarditis
Respiratory Pneumothorax,
Pulmonary Embolism
GIT Esophageal Rupture,
GERD
MSK MSK, Costochondritis,
Tietze’s syndrome
Others Anxiety
Cardiac Causes
- Stable Angina o Definition
§ Stable chest pain which arises during exertion / emotional distress due to >70% stenosis of coronary arteries caused by a stable atherosclerotic plaque.
§ It may rupture and progress to unstable angina. Beware of a change in character of the usual chest pain or pain that used to go away but does not go away now.
o Clinical features § Cardiac-type chest pain, comes on during exertion/emotional distress/meal,
relieved by rest/GTN § Risk factors
• Age, Smoking, Poor diet • Hypertension, Hypercholesterolemia, Diabetes Mellitus
o Investigation
§ Stress ECG by Exercise or Dobutamine § Angiogram
o Management
§ Preventive treatment: Aspirin 75mg + Statins § Symptomatic treatment: B-blocker (Cardioselective Atenolol / Metoprolol)
• Add on non-DHP CCB if angina persist despite B-blocker § Acute episode treatment: GTN PRN
• CI with Sidenafil (PDE5-inhibitor) à Severe hypotension § Angioplasty § CABG (If left main coronary artery occlusion or triple vessel disease)

Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
2
- ACS*
o Definition § An umbrella term for unstable angina, STEMI and NSTEMI, in which there is an
occlusion of the lumen by thrombus secondary to rupturing of atherosclerotic plaque
§ STEMI = Transmural Infarct, while NSTEMI = Endocardial Infarct
o Clinical features § Cardiac-type chest pain, which is persistent and not relieved by rest/GTN,
associated with sympathetic features of nausea, vomiting, sweating and cardiac features of palpitations and dyspnea
§ Risk Factors • Hypertension, Hypercholesterolemia, Diabetes Mellitus • Personal and Family Hx (<55yo) of ACS • Smoking
o Investigation
§ 12-lead ECG § Cardiac enzymes Troponin T, I, CKMB
• Repeat ECG every 10 mins if normal
o Management § STEMI
• Initial management (MOAT) o Morphine IV 2.5mg + Metaclopramide IV 10mg o Oxygenation o Aspirin 300mg PO o Ticagrelor 180mg PO
• Ultimate Goal
o Primary PCI within 90 mins o If Primary PCI unavailable within 120 mins, thrombolysis is
indicated.
§ Unstable angina or NSTEMI • Risk stratification with TIMI risk score
o ≥5 = High risk § Ticagrelor 180mg PO § Early PCI
o ≤2 = Low risk § Clopidogrel (Plavix) 600mg PO
o Differentiating Unstable Angina, NSTEMI, STEMI
§ Unstable Angina: Cardiac enzymes not raised § STEMI: Cardiac enzymes raised + STE on ECG § NSTEMI: Cardiac enzymes raised + Non-STE on ECG (ECG can be normal)

Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
3
- Aortic Dissection*
o Definition § A tear in the intimal layer of the aorta, allowing blood to flow through it and cut
through the medial layer
o Clinical features § Excruciating tearing chest pain of very sudden onset, radiates to the back between
scapulae, max pain at onset and improves overtime § Migratory pain to abdomen/legs if anterograde
o Risk Factors
§ HTN § Connective Tissue Disorders (Marfan’s, Ehlers Danlos)
o Classification
§ DeBakey Classification (Site of origination) • Type I: Ascending aorta, Aortic arch, Descending aorta • Type II: Only ascending aorta • Type III: Only descending aorta
§ Stanford Classification (Site of involvement)
• Type A: Involves ascending aorta (Managed surgically) • Type B: Does not involve ascending aorta (Managed medically)
o Origin of occlusion
§ Carotid origin • Neurological symptoms: Syncope, TIA, Stroke
§ Subclavian origin • Unequal blood pressures and pulses (Radio-radial + Radio-femoral delay)
o Management
§ Pain control § Anti-impulse control (Reduce LV contraction)
• IV beta-blockers (Labetalol, Esmolol) o If CI, Non-DHP CCB (Verapamil, Diltiazem) is indicated o If SBP remains < 100 mmHg, nitroprusside is indicated
- Pericarditis
o Definition § Inflammation of the pericardium
o Clinical features
§ Pleuritic chest pain, worsened lying down and relieved sitting forward
o Causes § Infectious: Virus, Bacteria, Fungi (Fever)

Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
4
§ Previous MI associated with Dressler’s syndrome § Autoimmune disease (SLE, RA, Sarcoidosis)
o Management § Pain relief
• Ibuprofen 400mg TDS PO (max 1200mg/day) § Treat underlying cause
Respiratory Causes
- Tension Pneumothorax* o Definition
§ Air in the pleural space
o Clinical features § Pleuritic chest pain of very sudden onset, associated with SOB
o Risk Factors
§ Young marfanoid patients § Elderly smoker with COPD/Asthma (Emphysematous bullae) § Post-chest trauma
o Investigation
§ Physical Exam • Tracheal deviation away (Only in tension pneumothorax) , Hyperresonant
percussion note, Decreased breath sounds
§ CXR o Management
§ First, IV cannula at 2nd intercostal space, mid-clavicular line § Followed by Chest drain § If recurrent pneumothorax, surgical options like pleurectomy and Talc pleurodesis
can be considered
- Pulmonary Embolism* o Definition
§ Clot in the pulmonary arterial tree, most common origin from a proximal DVT. • Other rarer causes can be air, fat, amniotic fluid, neoplasm
o Clinical features § Pleuritic chest pain of very sudden onset § Associated with SOB, Hemoptysis, Collapse, Fever
o Risk factors (Virchow Triad + History)
§ Stasis • Immobility (Paralysis, Stroke, long bus/plane rides) • Venous pooling (Heart failure, Chronic venous insufficiency)
§ Endothelial damage • Post-op • Trauma

Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
5
§ Hyper-coagulation • Cancer + Cancer Treatment • Increased estrogen (e.g. Liver failure, HRT, OCP, Pregnancy) • Coagulopathies (Factor V Leiden, Protein C/S deficiency, Antithrombin III
deficiency, Antiphospholipid syndrome) § + Personal or Family Hx of DVT/PE
o Well’s score
§ < 4.0 = PE unlikely (<10%) § > 4.5 = PE likely (20-40%)
o Investigation
§ Well’s score < 4.0 = Age-adjusted D-dimer to exclude PE § Well’s score > 4.5 = CTPA (Gold standard)
o Management (Anticoagulation is the mainstay medication)
§ Hemodynamically stable • Anticoagulation with LMWH, with simultaneously Warfarin bridging
§ Hemodynamically unstable • ABCDE + Resuscitation + Oxygen and Morphine • Thrombolysis with Alteplase • Anticoagulation with LMWH, with simultaneously Warfarin bridging
- Pneumonia
o Definition § Acute lower respiratory tract infection (LRTI), affecting the pulmonary parenchyma
o Clinical features
§ Pleuritic chest pain, associated with systemic features like fever, malaise and resp features like SOB
o Investigations § CURB-65
• 0-1: Send home on antibiotics • 2: Admit to Hospital • ≥3: Admit to ICU
§ Bloods – WCC and differentials, CRP § CXR – Consolidation § ABG – Type I or II respiratory failure
o Management (Subjected to local antibiotics guidelines. Given below is for Cork patients)
§ CURB 0-1 = Amoxicillin 500mg TDS PO § CURB 2-3 = Co-amoxiclav 1.2g TDS IV + Clarithromycin 500mg BD PO § CURB 4-5 = Ceftriaxone 2g OD IV + Clarithromycin 500mg BD PO
GIT Causes - Esophageal rupture*

Chest Pain History Taking Learning Document
Last updated: Feb 2018
By Aaron Ho (DEM3, Class of 2020) * = Life threatening cause
6
o Retrosternal chest pain following violent vomiting or recent esophageal endoscopy
- GERD o Retrosternal burning chest pain, brought on from meal/alcohol/supine and relieved by
antacids
MSK Cause
- MSK o Sharp pleuritic chest pain, able to pin-point location of pain, exacerbated by pressure over
area - Costochondritis
o Sharp pleuritic chest pain with tenderness but no swelling - Tietze’s syndrome
o Sharp pleuritic chest pain with tenderness and swelling Others
- Anxiety/Panic attacks o Sense of impending doom, anxious personality o Recurrent episodes triggered by a stimulus (Social stimulus like crowds, public speaking)
Extra
ECG Criteria for STEMI STE ≥ 1mm in >2 contiguous limb leads (II, III, aVF or I, aVL)
STE ≥2mm >2 contiguous precordial leads (V1-V6) New LBBB according to Sgarbossa’s Criteria
- STE ≥1mm concordant with QRS in any leads (5 pts) - STD ≥1mm in any lead from V1-V3 (3 pts)
- STE >5mm discordant with QRS in any leads or STE: S-wave ratio > 25% (Modified) (2pts)
Posterior MI: - Reciprocal STD and Tall R waves in V1 from Posterior STE and Q waves
- Posterior leads must be done to confirm diagnosis