
CHAPTER -4 ANALYSIS AND FINDINGS -...
98
77 CHAPTER -4 ANALYSIS AND FINDINGS This chapter brings out data analysis and interpretations. The data collected from different sources have been organized in order to bring out effective findings and conclusions. The main sources of data collection are the nursing staff, heads of nursing and hospital, hospital records, and observed field data. This chapter is organized into three major main parts namely Part – 1. Demographic Profile and Job Characteristics, Part – 2 Working conditions and facilities provided to the nursing staff, Part – 3 Over view of Quality indicators. Part I of this chapter is “Demographic Profile and job characteristics”. This provides the findings about the nursing staff background and their work related characteristics. The information presented in this segment is based on the structured interview scheduled administered with 317 nursing staff, data collected from administrative and nursing heads of the sample hospitals (key informant interview) by guided interview schedule and data obtained from the hospital records (secondary data). Part II of this chapter is “Working conditions and facilities provided to the nursing staff”. This presents the findings of the variables like physical facilities, organisational policies, professional development, work teams, respectful relationship, supervision and management, and service quality and patient safety. The information provided in this segment is based on the structured interview scheduled administered with 317 nursing staff, data collected from head of the hospitals and nursing heads of the sample hospitals by unstructured in depth interview. Part III of this chapter is “Quality of work life indicators”, this part covers variables like work life balance, absenteeism, work stress, communication, job satisfaction, organisational culture and climate, and nursing staff’ perception on their work performance. There are seven variables covered in this segment.
Transcript of CHAPTER -4 ANALYSIS AND FINDINGS -...

77
CHAPTER -4
ANALYSIS AND FINDINGS
This chapter brings out data analysis and interpretations. The data collected from
different sources have been organized in order to bring out effective findings and
conclusions. The main sources of data collection are the nursing staff, heads of
nursing and hospital, hospital records, and observed field data. This chapter is
organized into three major main parts namely Part – 1. Demographic Profile and
Job Characteristics, Part – 2 Working conditions and facilities provided to the
nursing staff, Part – 3 Over view of Quality indicators.
Part I of this chapter is “Demographic Profile and job characteristics”. This
provides the findings about the nursing staff background and their work related
characteristics. The information presented in this segment is based on the structured
interview scheduled administered with 317 nursing staff, data collected from
administrative and nursing heads of the sample hospitals (key informant interview)
by guided interview schedule and data obtained from the hospital records
(secondary data).
Part II of this chapter is “Working conditions and facilities provided to the nursing
staff”. This presents the findings of the variables like physical facilities,
organisational policies, professional development, work teams, respectful
relationship, supervision and management, and service quality and patient safety.
The information provided in this segment is based on the structured interview
scheduled administered with 317 nursing staff, data collected from head of the
hospitals and nursing heads of the sample hospitals by unstructured in depth
interview.
Part III of this chapter is “Quality of work life indicators”, this part covers variables
like work life balance, absenteeism, work stress, communication, job satisfaction,
organisational culture and climate, and nursing staff’ perception on their work
performance. There are seven variables covered in this segment.

78
Chapter – 5 covers the effect of job characteristics and working conditions and
facilities on quality of work life of the nursing staff”. In this chapter the findings of
key variables of Part-1 and Part-2 are cross examined with Part-3 Quality of Work
Life indicators variables to understand “the effect of job characteristics and working
conditions and facilities on the quality of work life of nursing staff”. The effect on
quality of work life of nursing staff due to demographic profile of nurses, job
characteristics, working conditions and facilities is analysed by applying statistical
tools like chi-square tests, logistic regression and correlation. Also the data are
analysed and presented in the form of cross tables.
The final chapter of analysis is “Chapter-6 Key Informant Interviews on nursing
work environment”. In this segment the views shared by the heads of the nursing
department like matron, assistant matron and hospital head medical superintendent
or chief medical officer examined. A guided interview schedule was used to collect
the information from theses respondents. These respondents also called key
informants, as they have shared information with regard to nursing staff problems,
challenges, work related issues, factors affecting their routine work, working
conditions and facilities provided to the nursing staff etc.
Overall in this chapter some of the statistical tools used for analyzing data were
percentages, mean, standard deviation, chi-square test etc. Also two way tables
were used to describe the variables of the study. In addition to this, a multivariate
tool of Logistic regression, has been used to bring out appropriate findings and meet
the requirement of study objectives from the available data. In brief these statistical
tools have played vital role in exploring the important aspects of the phenomenon
and analyzing all important variables of this research study.

79
PART-1 DEMOGRAPHIC PROFILE AND JOB CHARACTERISTICS
Section – ‘A’ Demographic Profile of the respondents
This section provides useful information to understand the demographic profile and
job characteristics of the respondents. The respondents are 317 nursing staff who
have completed three years of experience in Municipal Peripheral hospitals in
Mumbai. The findings below relate to significant aspects of the respondents’ social,
economic and job related characteristics.
Age, Education and Experience
Age: The nursing staff age, education and their experience are presented in table
1.1. The mean age of respondents is 42. The standard deviation of age (8) indicates
that large numbers of respondents have reached middle age. The middle age group
has its own behaviour and associated issues like health, adjustment to working
conditions and facilities, promotions and other opportunities. As they grow older
the nurses are expected to have improved knowledge and skills, maturity, and
commitment to the work. It is also expected that patients would feel confident when
the staff which is present is older in age. Also the senior staff would be good
sources for providing coaching and training to the young staff at the ward level.
They command respect from coworkers and other groups. On the other hand they
might resist changes like computerisation, or modernization including use of latest
technology because they need to acquire new skills which would be difficult for
them to acquire at a older age.
Experience: The mean total experience of respondents is 19 years. The total years
of experience of the nursing staff include their current experience in the present
hospital and experience in similar BMC peripheral hospitals. The mean years of
experience in the present hospital is 15 years. It is clear that the work age of
beginner nurses is 23 years (mean age is 42 minus mean total experience 19 equal
to 23 years) and before they took up the current positions they had worked on an
average of 4 years (total mean experience 19 years minus mean present hospital
experience 15 years) in other hospitals including BMC hospitals. The nursing staff
have gained long years of experience in the same hospitals. Even though the
nursing staff have various opportunities and scope to work in other places including

80
abroad, they have not moved away. Also it indicates that there is hardly any nursing
staff turnover in these hospitals. Since the majority of the staff have continued to
serve in the same hospitals it helps the staff to understand the value system of the
hospitals and patients’ behaviour, and this facilitates better coordination between
the patients and the staff. The nursing staff are able to easily understand the patient
background, cultural and social requirement of the patients at the early stage of
patients’ stay. As a result, the patients get appropriate support right from the time of
their admission into the hospital.
Education: Among the respondents, a majority of the nursing staff, nearly 71 per
cent, are qualified with a nursing diploma with Higher Secondary Course (HSC)
which is the currently considered as minimum educational eligibility for a staff
nurse position. However, 28 per cent of the nursing staff have a diploma in nursing
with Secondary School Leaving certificate (SSLC) or Standard X. These nurses are
relatively older nurses and had joined the hospitals before the introduction of HSC
as a requirement. There is only one per cent of staff who have a degree with nursing
diploma or Degree in nursing courses as seen in the sample hospitals. It is seen that
there is no necessity for the nursing staff to carry on higher studies as there is no
perceived benefit associated with higher qualification. Also there is a reason to
believe that majority of the staff have middle age health factors and family
responsibilities that undermine any effort of upgrading their qualifications. It is
reported that the Indian Nursing Council is trying to bring degree in nursing as the
basic qualifications for nursing services where the present qualifications of Staff
nurses (diploma in nursing) will be replaced by the degree holders as and when
these nursing staff retire. One of the matrons in the study hospitals pointed out that
“by 2010 new recruitment will start with only degree in nursing candidates”. In the
near future the diploma in general nursing and midwifery holders will be no longer
potential candidates in the public hospitals. Also the nursing educational institutions
are likely to stop training diploma nurses in the coming years.

81
TABLE -1.1 Respondents Age, Education, and Experiences
Age of the respondents Present designation Total Staff Nurse Sister
incharges Below 30 yrs 27 (10.2) 1 (1.9) 28 (8.8)31-35 yrs 48 (18.2) 2 (3.8) 50 (15.8) 36-40 yrs 58 (22.0) 5 (9.4) 63 (19.9) 41-45 yrs 63 (23.9) 7 (13.2) 70 (22.1) 46-50 yrs 42 (15.9) 3 (5.7) 45 (14.2) 51 & above 26 (9.8) 35 (66.0) 61 (19.2)Education X2 = 90.73 P=.000 SSLC with Nursing Diploma 55 (20.8) 34 (64.2) 89 (28.1)H Sc with Nursing Diploma 205 (77.7) 19 (35.8) 224 (70.7)Others 4 (1.5) 0 (0.0) 4 (1.3)Total years of experience X2 = 41.21 P=.000 Up to 5 yrs 30 (11.4) 0 (0.0) 30 (9.5)6-10 yrs 36 (13.6) 3 (5.7) 39 (12.3)11-15 yrs 89 (33.7) 7 (13.2) 96 (30.3)16-20 yrs 58 (22.0) 5 (9.4) 63 (19.9)21-25 yrs 42 (15.9) 12 (22.6) 54 (17.0)26- & above yrs 9 (3.4) 26 (49.1) 35 (11.0)Experience in present hospital X2 = 102.39 P=.000 Up to 5 yrs 41 (15.5) 15 (28.3) 56 (17.7)6-10 yrs 30 (11.4) 5 (9.4) 35 (11.0)11-15 yrs 70 (26.5) 2 (3.8) 72 (22.7)16-20 yrs 80 (30.3) 4 (7.5) 84 (26.5)21-25 yrs 30 (11.4) 7 (13.2) 37 (11.7)26 & above 13 (4.9) 20 (37.7) 33 (10.4)Total 264 (100) 53 (100) 317 (100) X2 = 68.67 P=.000
(Figures in brackets indicate the percentage of nursing staff) N=317
Family Size and Background
The size of the family includes adults, children and dependents. The details are
presented in Table -1.2 Adults, children and dependents. The mean number of adult
in the nursing staff family is 3 and the standard deviation is 1. Nursing staff family

82
size is one of important factors to decide on a professional career because being a
female worker they have greater responsibilities to take care of the family members
particularly the young children and elderly persons in the family. It is expected that
if the family members are adults and are able to manage themselves, the nursing
staff have slightly less home responsibilities. Also the adult members are able to
understand the nature of nursing profession and try to extend support and
cooperation to the nursing staff. Another advantage is that there is a possibility to
get financial support from the adult members subject to their earning capacity.
However, the nursing staff do have certain responsibilities of supporting the adult
members in terms of providing financial support if they are pursuing higher studies,
unemployed or any other reason that adds to the tension of the nursing staff.
The mean number of children in the nursing staff family is 1.7 and the standard
deviation is 0.6. Nearly 38 per cent have only one child and 57 per cent have two
children in the present scenario. A majority of the nursing staff have followed the
governmental norm of “we two, ours two”. This is because of the nursing staff’s
high awareness on family planning, living in an urban environment, more oriented
towards having small and compact families. Another reason for having only one or
two children is most of the nuclear family set up wherein the family consists of only
the husband and wife and there are no other members, elders or relatives or trust
worthy persons, to take care of their off spring. It is to be noted that some the
nursing staff mentioned that “young and school going children take much of our
time and give us more challenges by demanding more attention, and support.”
Another issue is that the nursing staff have to pay more attention to their work
because of the above reasons and the nursing have consciously avoided having a
larger family.

83
TABLE -1.2
Nursing Staff Family Members: Adults, Children and Dependents
Number of Adults Present designation
Total Staff Nurse Sister incharges Up to 2 102 (38.6) 13 (24.5) 115 (36.3)
3-4 134 (50.8) 26 (49.1) (50.5)160
5-6 25 (9.5) 14 (26.4) (12.3)39
7+ 3 (1.1) 0 (0.0) (0.9)3
Number of children 1 70 (38.3) 12 (38.7) 82 (38.3)
2 106 (57.9) 15 (48.4) 121 (56.5)
3+ 7 (3.8) 4 (12.9) 11 (5.2)
Number of dependents X2 = 13.35 P=.004 1 49 (20.8) 15 (32.6) 64 (22.7)
2 122 (51.7) 23 (50.0) 145 (51.4)
3 46 (19.5) 6 (13.0) 52 (18.4)
4 14 (5.9) 1 (2.2) 15 (5.3)
5 3 (1.3) 0 (0.0) 3 (1.1)
6 2 (0.8) 1 (2.2) 3 (1.1)
Total 236 (100) 46 (100) 282(100) X2 = 7.28 P=.063
(Figures in brackets indicate the number of nursing staff) N=317
The mean number of dependents in the nursing staff family is 2. Nearly 46 per cent
of the nursing staff have two dependents, 20 per cent have only one dependent.
These dependents are mostly their own children and in-laws who are staying with
the nursing staff. Other than caring for elders and the children who require more
attention and well being the nursing staff also provide economic and monetary
support to these dependents.
Economic conditions of nursing staff
The smooth functioning of a family unit is connected with various requirements
including financial support. In the nursing staff family there are few members
earning and providing support. The details of economic support and other aspects
are presented in table Table1.3

84
Majority of nursing staff 74 per cent have two earning members in the family which
include self and their spouse. Nearly 13 per cent of the staff have a single earning
member that is mostly self income. However, the mean earning member in the
nursing staff family is 2 and the standard deviation is 0.7. In normal circumstances,
it is expected every male has to work in Indian traditional families. If it is
considered the male has to work in addition to that the female member also working
so every nursing staff family is supposed to have two earners in a family which
brings in an additional economic support for the family.
Nearly 59 per cent of the nursing staff receive a salary between Rs.14000 to
Rs.17000 which is a reasonable salary as per the Indian economy, but to earn this
salary the staff have to put in at least an average of 19 years of service in the
hospitals. The system is such that more the years of experience of the nursing staff,
the higher the salary due to yearly increments. The nursing staff average self
income is Rs.15,301 per month per person and the standard deviation is Rs.2049.
However, the mean income is not the actual take home salary. There are some
standard deductions applicable like professional tax, contribution to provident fund,
loan recovery, LIC, Income tax etc.
Nearly 39 per cent of staff have a family income of Rs.20001 to Rs.25000. The
mean income of the family is Rs.22,831. The difference between the self-income
and family income is Rs.7530 per month. It means, on an average, extra income
other than self generated is Rs.7530 per month. In other words, the spouses’ earning
is really low when compared to that of the nursing staff. In such situations if the
nursing staff do not work, the family is likely to face economical crises. Even
though there is an average of two persons who earn in the nursing staff family,
many nursing families depend on the nursing staff income as main source of
income. Therefore, even if a nurse wishes to leave her job she cannot leave the job.
The total family members are 1742 which includes 1024 adults and 359 children.
The per capita income of the family members is Rs.4155 person per month which
include the both the self and spouse. If the children are excluded from the
calculation of per capita income it works out Rs.7068. While comparing the

85
nursing staff family members’ per capita income Rs.4155 with national per capita
income Rs.3333 per month per person (World Bank Report, 2007) the nursing staff
family members have a higher per capita income per month.
TABLE1.3
Economic Support and Income Status of the Staff
Occupation of spouse Present designation
Total Staff Nurse Sister incharges Unsecured job 179 (73.7) (34.7)17 196 (67.1)
Secured job 51 (21.0) (30.6)15 66 (22.6)
Retired 13 (5.3) (34.7)17 30 (10.3)
Number of earning members in the family X2 = 55.94 P=.000 1 32 (12.1) 8 (15.1) 40 (12.6)
2 205 (77.7) 29 (54.7) 234 (73.8)
3 15 (5.7) 10 (18.9) 25 (7.9)
4 8 (3.0) 4 (7.5) 2 (3.81)
5 3 (1.1) 2 (3.8) 5 (1.6)
6 1 (0.4) 0 (0.0) 1 (0.3)
Monthly self income X2 = 17.71 P=.003 Up to Rs. 8000/- 3 (1.1) 0 (.0) 3 (.9)
Rs.8001-11000/- 7 (2.7) 0 (.0) 7 (2.2)
11001-14000 82 (31.1) 4 (7.5) 86 (27.1)
14001-17000 158 (59.8) 31 (58.5) 189 (59.6)
17001 & above 14 (5.3) 18 (34.0) 32 (10.1)
Monthly family income X2 = 46.930 P=.000 Rs.10000 -15,000 17 (6.4) 1 (1.9) 18 (5.7)
Rs.15001 to Rs.20000 68 (25.8) 11 (20.8) 79 (24.9)
Rs.20001to Rs.25000 106 (40.2) 17 (32.1) 123 (38.8)
Rs.25001to Rs.30000 51 (19.3) 21 (39.6) 72 (22.7)
Rs.30001 to Rs.35000 9 (3.4) 2 (3.8) 11 (3.5)
Rs.35001 and above 13 (4.9) 1 (1.9) 14 (4.4)
Total 264 (100) 53 (100) 317 (100) X2 = 11.74 P=.038
(Figures in brackets indicate the number of nursing staff) N=317
Nearly 51.7 per cent of the spouses are working in private companies and 14.5 per
cent work in Government organisations. Further, the jobs are classified under
secured and not so secured to have clear view about the nature of job and how they
meaningfully support the nursing staff family. It is found that nearly 59.3 per cent

86
of the spouses of the nursing staff are working in private companies and the casual
work sector that are both unsecured. However 20.8 per cent of the spouses of
nursing staff are working in secured positions like government job, corporations,
banks etc. Secured job and unsecured job makes lot of difference in the nursing
staff mindset. It has been observed that some nursing staff are very happy to
mention the occupational status of their husband only if he possesses a secured or
white-collar job or runs his own business. On the other hand, if the staff’s spouse
has a job in the private sector or in employed in a temporary occupation, the staff
mentions their spouse’s occupation with some hesitation. Some of the staff stated
that their husbands are not willing to take up a job. This increases their mental
tension and there is no financial support from their spouse.
Nursing staff’s Marital Status, Religion and State of Origin
Nursing staff’s marital status, their religion and the state of origin is presented in
table number 1.4. Among the respondents nearly 92 per cent are married and only 6
per cent are unmarried. Married nursing staff have many problems which include
time pressure, developing professionalism, raising and managing the children and
other work related issues. Some of the nursing staff mentioned that their children
are latch-key kids. It is because there are no facilities in the work place or there is
nobody is to take care of the children at home and childcare facilities are either
easily available or expensive. Many senior nursing staff have reported that because
of the work shifts they have missed out on enjoying quality time with their children.
The majority of the nursing staff i.e. 84.5 per cent belongs to Hindu religion and
nearly 13 per cent of the staff are Christian. The nursing profession and religion are
traditionally closely associated. Nursing services were introduced in India by
missionaries and later it was recognised as a profession in the country. Since the
beginning Christians used to take up nursing as a profession and make it their career
choice. It is perceived that there is no practice of taking nursing as a career choice
in Hindu communities. But in the study of hospitals it has been found that majority
are belonging to Hindu religion. It shows that the religion is no long longer a factor
when choosing the nursing profession and secondly that Hindu families have
accepted that their children have a right to choose nursing as profession. Another

87
reason for accepting nursing a career choice is that it gives enough employment
opportunities for women in private, government and corporations which in turn
provides a constant source of income to the family. Moreover, the women
irrespective of any religion who takes up nursing profession get satisfaction while
serving the community.
The majority of the staff (91 per cent) are Maharashtrians and only 6 per cent hail
from Kerala. It shows that the recruitment is restricted to only within the state of
Maharashtra. The Maharashtrians being localities can understand the local
languages of the state, the difficulties of the patients and are able to communicate
with the patients without any language barrier. However, there are certain issues
associated with the present system – in case the hospitals need more number of
nursing candidates to compensate the existing shortage or additional requirements if
any it would be difficult to identify workforce within the state because there may be
inadequate number of nursing candidates who are trained within the state and there
is scope for such candidate to migrate aboard.
TABLE – 1.4 Nursing Staff Marital Status, Religion and State of origin
Variables
Present designation
Total Staff Nurse Sister incharges Current marital status Unmarried 17 (6.4) 2 (3.8) 19 (6.0)
Married 243 (92.0) 49 (92.5) 292 (92.1)
Widowed 3 (1.1) 2 (3.8) 5 (1.6)
Divorced 1 (0.4) 0 (0.0) 1 (0.3)
Religion Hindu 222 (84.1) 46 (86.8) 268 (84.5)
Muslim 4 (1.5) 1 (1.9) 5 (1.6)
Christian 36 (13.6) 5 (9.4) 41 (12.9)
Others 2 (0.8) 1 (1.9) 3 (0.9)
State of origin Maharashtra 242 (91.7) 47 (88.7) 289 (91.2)
Kerala 13 (4.9) 5 (9.4) 18 (5.7)
Karnataka 3 (1.1) 0 (0.0) 3 (0.9)
Other states 6 (2.3) 1 (1.9) 7 (2.2)
Total 264 (100) 53 (100) (100)317(Figures in brackets indicate the number of nursing staff) N=317

88
Travelling between the workplace and residence and related matters
The details of place of stay, travel distance, mode of transport, duration of travel
and amount spent on travel are discussed in table 1.5. Most of the respondents stay
in different locations and are spread all over Mumbai and its suburban areas. The
respondents stay in nearly 60 different locations. Nearly 13.6 per cent of the
respondents stay in Borivili. This is the highest concentration of staff in a single
location. Many respondents stay far away from their work place. In Mumbai most
of the areas are well connected with the transport facilities. Since the nursing staff
follow the shift system and the duty timings are different from non-peak hours it
would be possible for them to travel easily. The nursing staff are not provided with
quarters. Hardly any staff have got accommodation within the hospitals. Even if the
hospitals provide quarters some of the staff members hesitate to occupy such
facilities because they have to work as substitutes or relievers and have to be
available 24 hours on call. In fact, a few nursing staff complained that “they have
been used very frequently as a substitute for absentees”.
A majority of the nurses, nearly 55 per cent, stay close to their work place, within 5
kilometers, and another 11 per cent of the staff stay between 16 – 20 kilometers.
The mean distance between workplace and the place of residence is 11 kilometers
and the standard deviation is 18 kilometers. The nursing staff have an option of
choosing from a variety of modes of transport. Nearly 43.8 per cent of the nursing
staff travel by train while 29.3 per cent travel by bus. Usually, the nursing staff use
multiple modes of transport to reach the hospital. The nursing staff use train and
auto or train and bus etc. because the work place is far away from the railway
station or sometimes the residence is far away from the railway station. Using
multiple modes of transport increases travel fatigue and this results in an attitudinal
change in the work place as well in the family set up. The nursing staff that use only
trains as their mode of transport feel that is faster and cost effective but are
uncomfortable to the overcrowding that Mumbai trains are famous for.

89
TABLE-1.5
Travel to Work Place and Related Issues
Variables
Present designation
Total Staff Nurse Sister incharges
Mode of transport Walk (8.7)23 5 (9.4) 28 (8.8)
Auto (2.3)6 1 (1.9) 7 (2.2)
Bus (29.5)78 11 (20.8) 89 (28.1)
Train (44.7)118 28 (52.8) 146 (46.1)
Train and Auto (1.1)3 0 (0.0) 3 (0.9)
Bus and Train (11.0)29 8 (15.1) 37 (11.7)
Own vehicle (2.7)7 0 (0.0) 7 (2.2)
Distance between the work place and residence Upto 5 kms 150 (56.8) 23 (43.4) 173 (54.6)
6-10 kms 25 (9.5) 5 (9.4) 30 (9.5)
11-15 kms 19 (7.2) 4 (7.5) 23 (7.3)
16-20 kms 27 (10.2) 8 (15.1) 35 (11.0)
21-25 kms 13 (4.9) 1 (1.9) 14 (4.4)
26-30 kms 4 (1.5) 1 (1.9) 5 (1.6)
31-35 kms 5 (1.9) 1 (1.9) 6 (1.9)
35+ kms 21 (8.0) 10 (18.9) 31 (9.8)
4-5 hours 17 (6.4) 4 (7.5) 21 (6.6)
5 & above hours 26 (9.8) 8 (15.1) 34 (10.7)
Amount spent on travel No expenses 25 (9.5) 3 (5.7) 28 (8.8)
Up to Rs.200 32 (12.1) 5 (9.4) 37 (11.7)
Rs.201-400 96 (36.4) 15 (28.3) 111 (35.0)
Rs.401-600 64 (24.2) 16 (30.2) 80 (25.2)
Rs.601 & above 47 (17.8) 14 (26.4) 61 (19.2)
Total duration of away from residence 8-9 hours 49 (18.6) 4 (7.5) 53 (16.7)
9-10 hours 172 (65.2) 37 (69.8) 209 (65.9)
11-12 hours 37 (14.0) 10 (18.9) 47 (14.8)
13 & above hours 6 (2.3) 2 (3.8) 8 (2.5)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the number of nursing staff) N=317
The mean time spent on travel is 1.4 hours (table1.6). Nearly 32 per cent of staff
stay close to the hospital hence they spend just about 15 minutes on travel to and

90
from the workplace. Nearly 28 per cent of the staff spend one hour on travel and
another 21 per cent spend two hours on travel. Many nursing staff have their own
houses in suburban areas. They have got these houses in suburban areas because the
cost of flats is relatively cheaper there, but these places are considerably far from
their work place. It is to be noted that a majority of study hospitals located in
suburban areas and all the hospitals have been well connected with transport
systems and this saves a lot travelling time. However, the nursing staff have to face
a crowd while travelling even though they may travel in non-peak hours. There are
many occasions the staff face traffic problems especially when they travel by bus.
This delays them when reaching the hospital or home. The nursing staff spend a
reasonable amount of their income on travel since majority of the respondents travel
by train which is relatively cheaper and faster transport service.. The mean travel
expenses is Rs.455 per month and the standard deviation is Rs.305. Nearly 30 per
cent of the staff spend Rs.201 to Rs.400 as monthly travel expenses. Only 11 per
cent of the staff spend less than Rs.200 as monthly travel expenses.
The nursing staff spend more than one third of the day away from their family. The
usually are at work or are travelling and these two constitute the total time spent
away from the residence. The nursing staff’s mean time away from the residence is
9 hours and 40 minutes and standard deviation is 1 hour 30 minutes. Nearly 32 per
cent of the nursing staff have indicated that they spend up to 8 hours in the hospital
and another 31 per cent of the staff spend 8-9 hours in the hospital. In fact, nearly
63 per cent of the above two categories 32 +31 of the nursing staff reported that
they spend less than 9 hours which is comparatively lower than the mean time. It is
reported that staying longer hours away from the residence affects the personal life
particularly managing the children’s education, emotional support and well being. It
is to be noted that when the mother is away for longer hours, children are likely to
get upset and learn abnormal behaviour. There is significant association between
the travel time and distance traveled by the nursing staff (r = 0.513). The table 1.6
presents the summary of statistics used in chapter-4 Section -A.

91
Table 1.6 Summary Table
Variables Mean Median Mode S D Mini mum
Maxi mum
Age 42.0 43 45 8.3 24 58
Total years of work 18.9 18 15 7.4 3.5 36
Years in Present Hospital 14.8 15 15 7.8 0 33
No. of Adults 3.2 3 2 1.4 1 13
Children below 14years 1.7 2 2 0.6 1 4
No. of dependent members 2.1 2 2 0.9 1 6
No. of earning members in the family 2.1 2 2 0.7 1 6
Monthly Self income 15327 16000 17000 2018 7000 19000
Monthly Family income 22831
Distance between workplace and residence 11.3 3 0 18.2 0 200
Total duration away from the residence in a day 9.6 9 9 1.3 7.3 14
Travel hours 1.6 1 1 1.2 0.3 6
Amount spend on travel 456.3 400 400 304.5 0 1500
Section B: Job Characteristics
1. Nursing organisation in the sample hospitals
Nursing department in Peripheral hospitals follows a simple organisational
structure. The structure consists of only five categories and the details are presented
in chart-1. The highest position in the hierarchy is Matron. She is the overall In-
charge of all the functions of the nursing department as well the nursing care system
in the hospital. The second in command in the hierarchy is Assistant Matron. She
provides administrative support in terms of supervising, organisation of functions,
interacting with all ward staff, taking the charge of all the nursing functions in the
absence of Matron. The third level is sister In-charge. She reports to assistant
matron or matron. She is provided with a set of responsibilities which will be
carried out on day-to-day basis. The sister in charge is a ward level staff and
provides support and facilitation to the staff nurses. The next category is staff nurse
position. Staff nurse carries out the nursing duties at the ward level and she is
responsible for the implementation pf the entire nursing programme. The last rung
of the hierarchy ladder is the ANM staff. The ANM staff assist in wards,

92
particularly labour wards and maternity wards, in some hospitals. Once the ANM
staff get retired they are replaced by staff nurse.
Chart-1 Nursing organisational chart in BMC Peripheral Hospital
The matron and the assistant matron were interviewed separately through in-depth
interviews to bring out insights of study variables. The sister in-charge and staff
nurses were interviewed through structured questionnaires. The number of
respondents (sisters in-charge and staff nurses) participated in the study is presented
in chart-2. The information shared by matron and assistant matron along with head
of the hospitals is presented separately.
Chart-2 Percentage of staff participated in the study
Representation of staff for the study
17%
83% Sister in charge
Staff Nurse
Among the respondents nearly 83 per cent are staff nurses and 17 per cent are sister
incharges. The sister incharges are senior staff work in the ward along the
supervisory responsibilities. While comparing the staff nurse and sister incharges,
the staff nurses are higher in number as they are the field staff. Accordingly, the
Matron
Assistant Matron
Sister in charge
Staff Nurse
Auxiliary Nursing Midwife (ANM)

93
adequate and appropriate representation of these categories participated in the
study.
The nursing staff from various departments which include Outpatient Services,
Casualty, Operation Theatre, Burns Ward, Intensive care Unit (ICU), Medical
Intensive Care Unit (MICU), Pediatric Intensive Care Unit (PICU), Premature
Ward, Pediatric Ward, Trauma Intensive Care Unit (TICU), Male Surgical ward,
Male Medical ward, Male Ortho ward, Eyes Ear Throat ward (ENT), Female
Surgical Ward, Female Medical Ward, Female Ortho ward, Labour ward, Obstrics
and Gynecology ward (OBG), etc. participated in the study. For the purpose of
analysis all these wards are classified into five major categories. They are General
wards, Critical care units, Operation Theatre (OT), Emergency Services and OPD
services. The departments representation are presented in chart-3.
Chart-3 Present departments of the participants of the study
Nursing staff present departments
7%
55%7%
17%
14% Out Patient ServicesGeneral Ward ServicesEmergency ServicesOperation Theatre ServicesCritical Care Services
It is found that there is an appropriate representation from each department for the
study.
Nearly 55 per cent from general wards, 17 per cent from operation theatre, 14 per
cent from critical care units, 7 per cent from emergency services and 7 per cent
from OPD services nurse have participated in the study. In every hospital usually 5
to 10 per cent of the beds are provided for critical care services, and nearly 80 per
cent of the beds are general wards. The staff distribution is done in accordance with
the nature of care provided by the hospital.

94
2. Nursing work activities
The nursing staff are trained in three and half years in professional training
institutions. During this period they are provided with appropriate training in all the
areas of clinical and some aspects of non-clinical services so that they can easily
handle the patient care. When they join hospitals they are provided with variety of
opportunities in various work settings like different wards including general wards,
critical care wards, operation theatre and outpatient services. Even though the
nursing staff are capable of doing multiple tasks but they cannot do all the work at a
time. So it is important to prioritise work logically. Sometimes they continue to
perform a variety of complex functions and across various chains of activities so it
is very important to specify what work they have to do and when they are supposed
to do them. This specification can be called job description. The nursing staff’
duties and responsibilities are clearly specified in the job description. This ensures
that the staff can work in a focused way and that their time is utilised effectively to
achieve better patient care. The nursing staff job description is enclosed in appendix
-4.
Keeping this in view, the nursing staff are asked to spell out whether they are doing
their work as per their job descriptions or not. Nearly 19 per cent of nursing staff
reported that they do work other than the nursing work. The details are presented in
Table 1.7. It is observed that many nursing staff do non-nursing work and they
consider these tasks are part of the nursing care such as clerical work, inventory
management, handling of patient visitors, management of class IV staff etc.
Table 1.7 Nursing staff working as per your designation/job description
Are you doing work as per your designation/job description?
Present designation
Total Staff Nurse Sister incharges No 49 (18.6) 11 (20.8) 60 (18.9)Yes 215 (81.4) 42 (79.2) 257 (81.1)Total 264 (100.0) 53 (100.0) 317 (100.0)
(Figures in brackets indicate the percentage of nursing staff) N=317
This is because of lack of clarity of proper guidelines about the work they suppose
to carry out. In the absence of specific guidance or written guidelines the staff
managing their work based on the basic training received from nursing school
during their studentship. As a result these nurses continue to provide service with

95
their age old practices and there is no possibility of ushering in modern methods of
nursing practice. Details of non-nursing activities performed are presented in
Table1.8
Table 1.8
List of selected non-nursing activities performed by the nursing staff
Non-nursing activities performed by the nursing staff
Present designation Total
Staff Nurse Sister incharges Blood transfusion, inserting I V to the patients
19 (38.8) 5 (45.4) 24 (40.0)
Controlling the visitors, shifting patients one place to another
2 (4.1) 0 (0.0) 2 (3.3)
Election duty, and other government work 3 (6.1) 1 (9.1) 4 (6.7)
Giving kidney tray, pulling the Oxygen cylinder
11 (22.4) 2 (18.2) 13 (21.7)
Indenting of material, and maintenance of inventory in the ward
6 (12.2) 2 (18.2) 8 (13.3)
More clerical work includes reports, registers and formats
6 (12.2) 0 (0.0) 6 (10.0)
Taking lecture on cleanliness, and hand washing procedures
2 (4.1) 1 (9.1) 3 (5.0)
Total 49 (100.0) 11 (100.0) 60 (100)(Figures in brackets indicate the percentage of nursing staff) N=60 As mentioned in table 1.8 the nursing staff carry out some of the work which are
not in their regular profile, however, they have continue to do so because it became
their practice. The nursing staff feel that all these non-nursing work may be a part
of the job description of the doctors or the house keeping staff or the administrative
staff. The usual non-nursing work which the nursing staff regularly perform are
blood transfusion, inserting the IV, giving kidney tray, pulling the Oxygen cylinder,
controlling the visitors, shifting patients one place to another clerical work, election
duty, providing training, lecture to class IV staff etc. It is confirmed that the
hospitals have documents formalising the job descriptions and the staff have seen
such documents but do not have copy of this document in hand. In the absence of
formal guidance or standards the nursing staff are unable to compare or conclude
whether they do more or less or optimal work or the work they do which really is
part of their formal work profile.
96
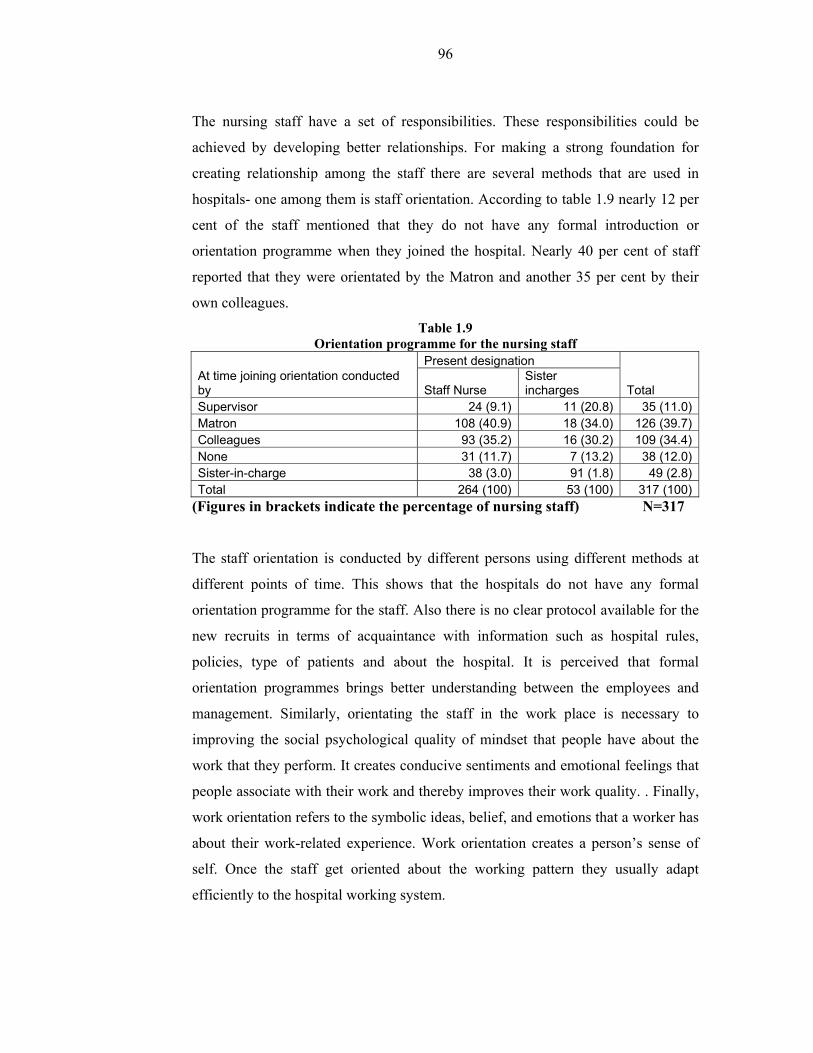
The nursing staff have a set of responsibilities. These responsibilities could be
achieved by developing better relationships. For making a strong foundation for
creating relationship among the staff there are several methods that are used in
hospitals- one among them is staff orientation. According to table 1.9 nearly 12 per
cent of the staff mentioned that they do not have any formal introduction or
orientation programme when they joined the hospital. Nearly 40 per cent of staff
reported that they were orientated by the Matron and another 35 per cent by their
own colleagues.
Table 1.9 Orientation programme for the nursing staff
At time joining orientation conducted by
Present designation
Total Staff Nurse Sister incharges
Supervisor 24 (9.1) 11 (20.8) 35 (11.0)Matron 108 (40.9) 18 (34.0) 126 (39.7)Colleagues 93 (35.2) 16 (30.2) 109 (34.4)None 31 (11.7) 7 (13.2) 38 (12.0)Sister-in-charge 38 (3.0) 91 (1.8) 49 (2.8)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
The staff orientation is conducted by different persons using different methods at
different points of time. This shows that the hospitals do not have any formal
orientation programme for the staff. Also there is no clear protocol available for the
new recruits in terms of acquaintance with information such as hospital rules,
policies, type of patients and about the hospital. It is perceived that formal
orientation programmes brings better understanding between the employees and
management. Similarly, orientating the staff in the work place is necessary to
improving the social psychological quality of mindset that people have about the
work that they perform. It creates conducive sentiments and emotional feelings that
people associate with their work and thereby improves their work quality. . Finally,
work orientation refers to the symbolic ideas, belief, and emotions that a worker has
about their work-related experience. Work orientation creates a person’s sense of
self. Once the staff get oriented about the working pattern they usually adapt
efficiently to the hospital working system.

97
Organisation of work shift and Duty System
In the study hospitals the duty roster is prepared systematically and distributed in
each ward. According to table 1.10 almost all the nursing staff (98 per cent) say
that there is a duty roster and it is followed without fail. Usually the duty list is
prepared for one full month by the matron. Once the duty roster is ready, it is put in
place and everybody follows the duty roster without fail. In case the staff fail follow
the duty roster they are punished with salary deduction or being marked as absent
for two days known as double day absent. Sometimes it may be difficult for the
staff to follow as per the schedule. In such a situation it is necessary to bring some
flexibility to modify or change their shift timings. It has been found that nearly 68.8
per cent of the nursing staff feel that they had an opportunity to modify or change
the shift for meeting their requirements. The remaining members did not have a
chance to modify their shits for their personal emergencies. Developing quality
work environment needs flexibility in the work schedule.
Since the nursing staff follow the shift system they usually have some problems.
The nursing staff considers that doing shift duty particularly night duty is a major
drawback of nursing profession. Keeping this in view, the nursing staff were asked
to report on this issue. In case they get an opportunity to choose the duty, the
majority of the respondents (nearly 83 per cent as per table 1.10) would prefer to do
morning shift and nearly 16 per cent have given their preference to do afternoon
shift while hardly any staff (less than one per cent) is interested in doing night duty.
It shows that nursing staff are doing their duty mostly against their wishes.
However, their service is needed 24 hours and somebody has to be there with the
patients. So there is no option for staff to withdraw from doing night duty or shift
duties. Another interesting observation is that the younger nurses like to do morning
shift due to their family commitments. Similarly, the elder nurses feel that they
should be given morning shift because they have served several years round the
clock services and at this stage of life in their middle age or old age with the
attendant health issues they should get some relief from doing night shifts. It is very
difficult for the nursing management to handle these issues.

98
Table 1.10 Nursing of Duty system and Flexibility
Variables
Present designation
Total Staff Nurse Sister incharges
Do you have duty roster? No (1.9)5 (1.9)1 (1.9)6Yes (98.1)259 (98.1)52 (98.1)311Which shift do you prefer? Morning (82.2)217 (86.8)46 (83.0)263After noon (17.0)45 (13.2)7 (16.4)52Night shift (0.8)2 (0.0)0 (0.6)2Do you have an opportunity to modify or change your shift timings for an emergency or family reason? No (32.6)86 (24.5)13 (31.2)99Yes (67.4)178 (75.5)40 (68.8)218How many times have you been able to avail this? Never (55.7)147 (39.6)21 (53.0)168Sometimes (34.1)90 (39.6)21 (35.0)111Frequently (5.7)15 (9.4)5 (6.3)20Very frequently (4.5)12 (11.3)6 (5.7)18Total (100)264 (100)53 (100)317
(Figures in brackets indicate the percentage of nursing staff) N=317
Shift timings and Official break between the shifts
The nursing department maintains proper working system by preparing a duty list,
leave plan and allocating the staff to respective wards. Table 1.11 shows the clear
plan on the timings between each shifts (duration for each shift).
Table 1.11
Shift Timings S.N Duty Shift Timings Applicable to Remarks
1 Morning Shift 7.00 am - 2.30 pm Staff Nurse Circle duty staff
2 Evening Shift 2.00 pm – 9.30 pm Staff Nurse Circle duty staff
3 Night Shift 9.00 pm – 7.30 pm Staff Nurse Circle duty staff
4. General Shift 8.00 am – 4.00 pm Staff Nurse Only for OPD/OT
5 General Shift 7.00 am – 3.00 pm Sister in charge S/I of each ward/OT
6 Evening Shift 1.00 pm – 9.00 pm Sister in charge S/I evening
supervisor
7 Evening Shift 9.00 pm – 7.00 am Sister in charge S/I Night duty
supervisor
(Sources: Attendance registers of nursing staff, at the matron office)

99
Sister in charge and senior staff nurse usually do general duty which consists of 8
hours. In addition to some of the staff nurses who are young mothers, older nurses
with lots of years of experience (on the ground of health problems) are given
general duty as per the decision of matron office.
The nursing staff is expected to work a minimum of 24 days in different shifts in a
month and the remaining 6 days are given as day-off generally in between a shift
change. Each shift has specific duration for example night shift has 10 hours duty
and day duties usually last 7.30 hours. The system is rotated to ensure that all the
staff nurses and the sister incharge shall undergo a similar system for every month.
The details are presented in the table as given below:
Table 1.12 Work shift hours for a Month
Sl.No Duty
shift No. of days
Actual work hours of Staff Nurse
Actual work hours of Sister in-charge
1 Night shift 06 days 10 hours per shift 10 hrs x 6 days = 60 hours
10 hours per shift 10 hrs x 6 days = 60 hours
2. Morning shift
12 days 7 and half hours per shift 7.5 hrs x 12 days = 90 hours
8 hours per shift 8 hrs x 12 days = 96 hours
3. Evening shift
06 days 7 and half hours per shift 7.5 hrs x 6 days = 45 hours
8 hours per shift 8 hrs x 6 days = 48 hours
4. Day off 06 days - - Total 30 days 195 hours in a month Total hours = 204 – 16 =
188 hours* * Half day leave @4 hours per day for 4 weeks (4hrs x 4 days) =16 hours (Sources: Duty Roster, at the matron office)
Circle duty system is common in all the hospitals. The sister incharges do mostly
morning shift and night duty weekly once. The night duty may increase or decrease
depending on sister incharges positions available in the hospital. As per the current
nursing duty roster the nursing staff do which include day and night duty for 195
hours and sister incharge 188 hours in a month. The sister in-charge is provided
with half a day leave every week in addition to their four offs in a month.
Official Break: Break is essential for the staff in between the hectic work schedule.
It is found that different practices are followed in the hospitals. In fact there is no
clear rule which specify the break between the work shifts. In this regard nearly

100
58.4 per cent of the nursing staff reported that they have the privilege of getting
official break during shift and another 38.5 per cent of the staff reported that they
have no official break during the shift. The details are presented in Table 1.13
Number of breaks during the shifts: Nearly 59 per cent of the respondents enjoy
one break in the morning shift as per table 1.13. Nearly 99 per cent say that there is
no official break in the afternoon and night duty. It shows that there is a lack of
clear guidance regarding providing breaks to the nursing staff in the hospitals. The
reason for not providing official break is because the nursing staff are expected to
provide patient care 24 hours and leaving the patients may hamper the treatment.
Therefore, there is no official break or fixed time of break during the shift. A
practice followed in the hospitals is that if there is an adequate number of staff
present in the ward, there is an increased likelihood for the staff members to get a
break during their shifts. Also there is a possibility of getting a break if there is a
reliever who will come and take over the duty. Even though there is no official
break the nursing staff are permitted to take a break anytime during their shift
unofficially when there is less work load in the ward.
Duration of Break: The respondents have indicated that the mean duration of
break is 31 minutes in the morning shift. It ranges between15 minutes to 60
minutes. It is very important to note the break is given only in the morning shift and
general shift and there is no break in the afternoon or night shift.
Table 1.13 Break in between the shifts and frequency of breaks
Opportunity for getting break between the shifts
Present designation Total Staff Nurse Sister incharges
No (39.8)105 (32.1)17 38.5)122Yes (56.8)150 (66.0)35 58.4)185Morning shift: No. of Breaks No break (40.9)108 (30.2)16 39.1)124One break (59.1)156 (69.8)37 60.9)193Average Duration of each-Morning Shift 15 minutes (0.6)1 0.0)0 0.5)130 minutes (95.5)149 86.5)32 93.8)18140 minutes (3.2)5 13.5)5 5.2)1060 minutes (0.6)1 0.0)0 0.5)1Total (100)264 100)53 100)317
(Figures in brackets indicate the percentage of nursing staff) N=317

101
Practical constraints and suggestions regarding break: The staff members are unable to enjoy the break because it does not have official
status. On the other hand, even if the hospital allows them to take a break; it would
not be possible for them to take a break because of the non-availability of relievers
for the staff. In addition to that if the nursing staff work load is heavy in the busy
wards, the patients need constant attention of the nursing staff and it would be
difficult for the nurses to move away from their wards. These are the practical
constraints which affect the nursing staff and do not allow them even a break to
relax form their work pressures.
The staff nurses and sister incharges suggest that one break of 30 minutes should be
provided in each shift or at least 15-30 minutes should be given as a break in
between the shift particularly in the afternoon shift. Nursing staff also should be
given break like any other administrative staff. Some of the staff feel that the
present system of giving one break in the morning shift and no breaks in the other
shifts should be continued. However, it is not acceptable to some of the other staff
members. Furthermore, some of the nursing staff suggest that the break should be
according to the work load and if there is less or no work load then the staff is likely
to get a break. Giving official breaks or increasing their frequency may affect
patient care. There is a lack of unanimous consensus among the nursing staff about
the changes needed in the break system.
Double duty
In BMC hospitals double duty is common. Double duty means the staff has to
continue to work one shift after another for two shifts in single day. In other words,
the staff does two work shifts without having any break. In the study hospitals a
majority of the staff (80 per cent) reported that they do double duty in a single day.
The double duty is a convenient tool for the nursing management to make up for the
immediate shortage of staff or absenteeism. There are various reasons for the staff
doing double duty in the hospitals, such as shortage of workforce, increased work
load in the hospital (work load increases whereas actual number of staff is remain
the same), staff members’ frequent absenteeism either for short period or due to

102
long leave, lack of substitutes to meet the additional staff requirements, etc. It is
observed that at a given point of time nearly 10 to 15 per cent of the staff are on
long leave. Also, the double duty depends on seasonal requirements, particularly
during the children’s Board examinations, summer and festival seasons as during
this period a large number of staff apply for leave. The hospital management finds it
very difficult to put strict rules in place against the staff wishes. Nearly 66.7 per
cent of the staff report that they do double duty occasionally, 29.6 per cent say that
they are required to do so once or twice in a month and another 3.6 per cent say that
they have to do double duty every week. It shows that double duty has become
inevitable in the hospitals. If the hospital avoids double duty then the patient care
may get affected due to non-availability of the staff during the shift. At the same
time if the double duty norm continues, the staff get tired and there is a possibility
of adverse effects in the ward like compromise on quality of patient care and lack of
attention given to the patients. Also there is a possibility that with less number of
staff posted in the ward the staff present have to take on the entire work load and
work under a lot of pressure.
Table 1.14 Double duty, compensation for double duty
Variables
Present designation
Total Staff Nurse Sister incharges
Are you doing double duty? No 44 (16.7) (37.7)20 64 (20.2)Yes 220 (83.3) (62.3)33 253 (79.8)How often do you do double duty? Weekly once 9 (4.1) (0.0)0 9 (3.6)Monthly once /twice 64 (29.1) (21.2)7 71 (28.1)Occasionally 47 (66.8)1 (78.8)26 173 (68.4)In what ways is the double duty was compensated? Day off 224 (97.8) (100.0)42 266 (98.2)Monetary 5 (2.2) 0.00 5 (1.8)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317 The staff double duty is compensated by providing a compensatory off. There is no
monetary support for doing double or extra duties in the hospital. Providing
compensatory off has its own side effect in that a staff who does double duty would
take the compensatory off along with her regular off creating a larger gap in a

103
situation already overwrought with lack of human resources that led to the existing
staff having to do double duty in the first place. This means the cycle of double
duty will never end. Since there is a heavy shortage of nursing staff in the hospital
and very less scope for avoiding double duty in the hospitals it becomes necessary
for the hospital to keep attractive incentives for the staff who do double duty. In
this way the hospital can avoid work pressure among the staff and would able to
cope with the situation.
Nursing work force, work load and job rotation
Hospitals are facing an acute shortage of work forces. There are several reasons for
this shortage. The shortage of staff really affects the patient care, however, the
hospitals do try to provide patient care with the available resources. On the other
hand, it may be difficult to provide even minimum level care when the number of
staff is reduced beyond a certain limit as it creates distress among the staff. At this
stage it has become very important to look at the work force of the study hospitals.
BMC has provided certain guidelines with regard to minimum staffing requirement
i.e. sanctioned posts for these hospitals. Sanctioned post is the minimum number of
staff who should be available to accomplish the tasks (work load) of the hospitals.
The details of staff position in the study hospitals are presented in table 1.15 There
is always some vacant position exist in the hospitals. The current situation in the
study hospitals is presented in table 1.15.
Table 1.15
Nursing workforce in the Study Hospitals
Hospital
Staff nurse Sister in charge Total
SP FP VP SP FP VP SP FP VP Bhagawathi Hospital, Borivili 135 124 11 19 17 2 154 141 13 V N Desai Hospital, Santacruz 81 74 7 13 10 3 94 84 10 K B Bhabha Hospital, Kurla 80 70 10 12 12 0 92 82 10 M T Agarwal Hospital, Mulund 51 43 8 15 12 3 66 55 11
Satapti Hospital, Govandi 67 56 11 8 7 1 75 63 12
Total 414 367 47 67 58 9 481 425 56 SP=Sanctioned posts, FP= Filled posts, VP= Vacant Posts Sources: Hospital records of study hospitals
104
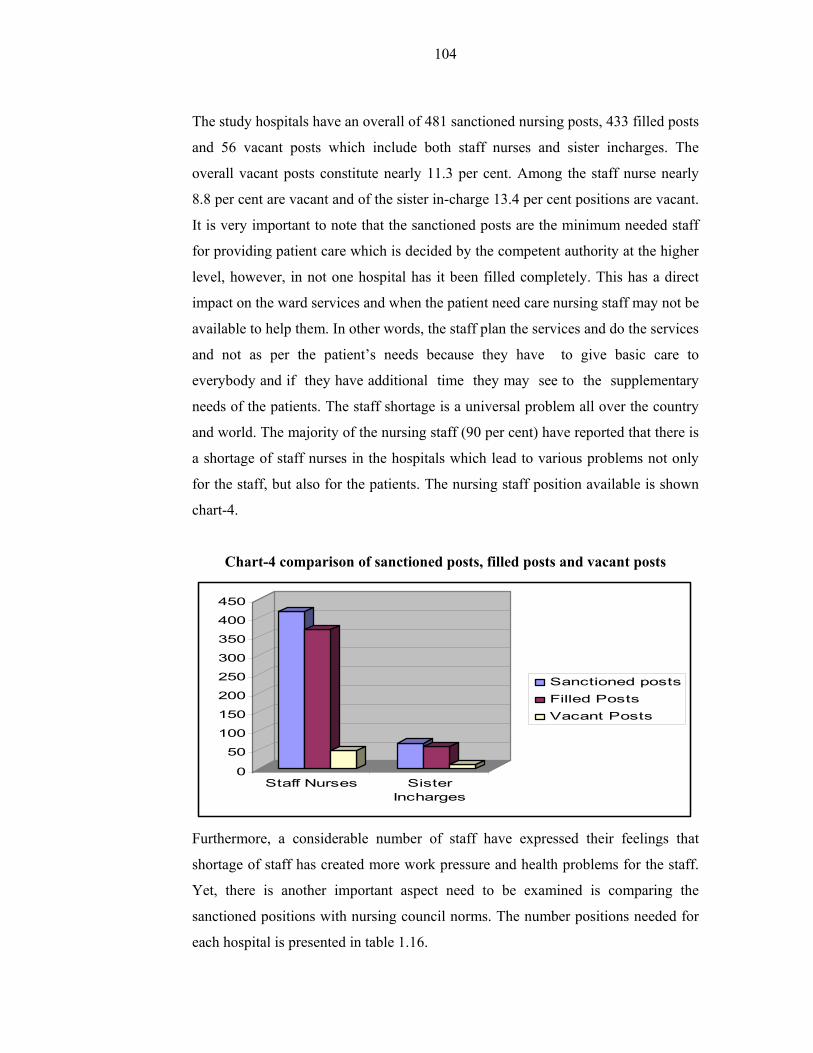
The study hospitals have an overall of 481 sanctioned nursing posts, 433 filled posts
and 56 vacant posts which include both staff nurses and sister incharges. The
overall vacant posts constitute nearly 11.3 per cent. Among the staff nurse nearly
8.8 per cent are vacant and of the sister in-charge 13.4 per cent positions are vacant.
It is very important to note that the sanctioned posts are the minimum needed staff
for providing patient care which is decided by the competent authority at the higher
level, however, in not one hospital has it been filled completely. This has a direct
impact on the ward services and when the patient need care nursing staff may not be
available to help them. In other words, the staff plan the services and do the services
and not as per the patient’s needs because they have to give basic care to
everybody and if they have additional time they may see to the supplementary
needs of the patients. The staff shortage is a universal problem all over the country
and world. The majority of the nursing staff (90 per cent) have reported that there is
a shortage of staff nurses in the hospitals which lead to various problems not only
for the staff, but also for the patients. The nursing staff position available is shown
chart-4.
Chart-4 comparison of sanctioned posts, filled posts and vacant posts
0
50
100
150
200
250
300
350
400
450
Staff Nurses SisterIncharges
Sanctioned postsFilled PostsVacant Posts
Furthermore, a considerable number of staff have expressed their feelings that
shortage of staff has created more work pressure and health problems for the staff.
Yet, there is another important aspect need to be examined is comparing the
sanctioned positions with nursing council norms. The number positions needed for
each hospital is presented in table 1.16.

105
Table 1.16 Nursing staff requirement as per the nursing council norms
Hospital Number of beds
Ope
ratio
n th
eatr
e Average OPD per
day
Nursing staff requirement as per
MCI norms including 30 per cent reserve To
tal
General Critical Nursing staff
Sister in charge
Bhagawathi Hospital, Borivili
373 12 13 1019 268 64 332
V N Desai Hospital, Santacruz
284 - 5 1333 160 46 206
K B Bhabha Hospital, Kurla
306 - 4 1241 165 50 215
M T Agarwal Hospital, Mulund
225 10 8 643 172 41 213
Satapti Hospital, Govandi
210 10 9 1095 175 41 216
Total 1398 52 39 5331 940 242 1182 While comparing the actual posts (filled) positions with nursing council norms the
number of staff needed is 200 per cent. The details of nursing norms enclosed in
appendix 5. When comparing the sanctioned positions with nursing council norms,
the sanctioned post is an average of 40.6 per cent of nursing council norms,
similarly, comparing the filled posts and the nursing council norms, the filled posts
amount to a mere 36 per cent of the nursing council norms. A comparative table is
presented along with graph in table 1.17 as given below.
Table 1.17 Comparison between the sanctioned posts with nursing council
norms
Positions Staff Nurses Sister incharges Total
Sanctioned positions 414 67 481
As per nursing council norms 940 242 1182

106
0100200300400500600700800900
1000
Staff Nurses SisterIncharges
Sanctioned posts
Filled Posts
Staff needed asper nursing councilnorms
Keeping the above data in view, it becomes necessary to examine the staff-patient
ratio in actual situations. The data that has been collected through the structured
questionnaire is presented in table 1.18. In the hospitals the staff allotment is based
on the wards and number of beds. The wards are categorised as: small ward about
25 beds, medium size 26 -35 beds and bigger wards up to 45 beds. It is observed
that in many hospitals renovation work is in progress so the hospital authorities
have combined two wards or three wards together. Sometimes there would be
possibilities of allotting the staff based on number of patients in case the workload
increases. The staff are distributed among Operation Theatres, Critical Care Units,
the various types of Wards and Out Patient Services. It is found that nearly 29 per
cent of staff are allocated to the operation theatre services while 71 per cent are
distributed among the wards and the OPD services. During the interviews in the
study hospitals the nursing staff managed a number of patients. The details are
presented in table 1.18. The nursing staff report that nearly 18 per cent attend to less
than 10 patients while another 16 per cent attend 21 to 30 patients in a single shift.
Moreover, nearly 10 per cent attend to 31 to 40 patients in their shift. The mean
current nursing staff and patient ratio is 1:13 i.e. one staff member is responsible for
thirteen patients. Ideally, 1 staff is to 5 patients is the required ratio in every shift.
But in the sample hospitals the number of patients for each nurse to care for is much
higher. It shows that the nursing staff are really required do more work and handle a
large number of patient in their shifts so that they concentrate on the minimum
patient care essential for the wellbeing of the patients.

107
Table 1.18 Number of patients seen by nursing staff during their the shift
In your duty you over see-Patients Staff NursesSister
incharges TotalOT services 75 (28.4) 23 (43.4) 98 (30.9)Less than 10 pts 49 (18.6) 8 (15.1) 57 (18.0)11-20 pts 42 (15.9) 6 (11.3) 48 (15.1)21-30 pts 43 (16.3) 7 (13.2) 50 (15.8)31-40 pts 29 (11.0) 3 (5.7) 32 (10.1)41-50 pts 19 (7.2) 4 (7.5) 23 (7.3)50 pts and above 7 (2.7) 2 (3.8) 9 (2.8)In your duty you over see-Wards OT 67 (25.4) 21 (39.6) 88 (27.8)1 Ward 180 (68.2) 23 (43.4) 203 (64.0)2 wards 12 (4.5) 4 (7.5) 16 (5.0)3 wards 5 (1.9) 5 (9.4) 10 (3.2)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
The hospitals have no provision to provide extra staff when the workload increases
in the ward and other areas. As seen in Table 1.19, nearly 68 per cent of nursing
staff mentioned that the hospitals do not provide any extra staff in such situations. It
is to be noted that the hospitals are already facing shortage of staff and there is no
possibility of providing extra staff.
Table 1.19 Additional staff are provided if the work load increases
Does the organisation provide for extra staff if workload increases? Staff Nurses Sister incharges TotalNo 179 (67.8) 37 (69.8) 216(68.1)Yes 85 (32.2) 16 (30.2) 101(31.9) 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff N=317
All the study hospitals follow the strategy of job rotation for a specific period of
time. Job rotation shall help the staff gain experience in a variety of conditions and
also lead to the acquisition of multi-skills. This also helps the hospital make an
arrangement for substitute in any ward irrespective of staff crunch so that the work
will not suffer. Job rotation has created an opportunity for the nurses to work in
Operation Theatre, Critical Care Services and special and general wards. As seen in
Table 1.20 nearly 90 per cent of staff say that they have been rotated on the job
every year and another 5 per cent reported that they are rotated in once in two years.

108
At the outset the job rotation fulfills the aim of the nursing staff of being
professionals with multi skills.
Table 1.20 Nursing staff Job Rotation
How frequently you are shifted to one ward to another? Staff Nurses
Sister incharges Total
Daily 4 (1.5) 3 (5.7) (2.2)7
Yearly 259 (98.1) 28 (52.8) 287
(90.5)One in 2 yrs 1 (0.4) 14 (26.4) 15 (4.7)One in 3 yrs 0 (0.0) 8 (15.1) 8 (2.5) 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff N=317
Work activities and Time spent for each activity
Nursing staff are engaged in several activities during their duty (single shift) which
is, generally, 7 hours 30 minutes in a day. Some of the activities that are performed
are directly connected with patient care and some of the activities are indirectly
associated with patient care. The staff nurse utilises nearly 50 per cent of her time
for direct patient care. The rest of the time is spent on other activities. The non-
nursing work can be done by others instead of the nursing staff so that the nurse can
devote her full time to patient care. If such an arrangement is made the current
nursing shortage can be managed to some extent.
Table 1.21 Time Utilisation by Staff Nurse
Activities performed by Staff Nurse Time spent for each activity
Out of 450 minutes Per cent
Patient care (medication, communicating with patients, bed making, handing over taking over, rounds with doctors, planning of work)
225 50
Clerical work (writing a case file, Preparing report, indent, etc) 71 16
Inventory management, ,collecting, checking items from stores etc 31 7
Telephone conversation for work purpose 14 3 Handling visitors / relatives and others 27 6 Internal training (case discussion, and other learning) 23 5 Traveling to various places in the hospital for work purposes 18 4
Break (coffee, tea, and lunch) 27 6 Talking to the friends, and colleagues other than the work matters 14 3
109
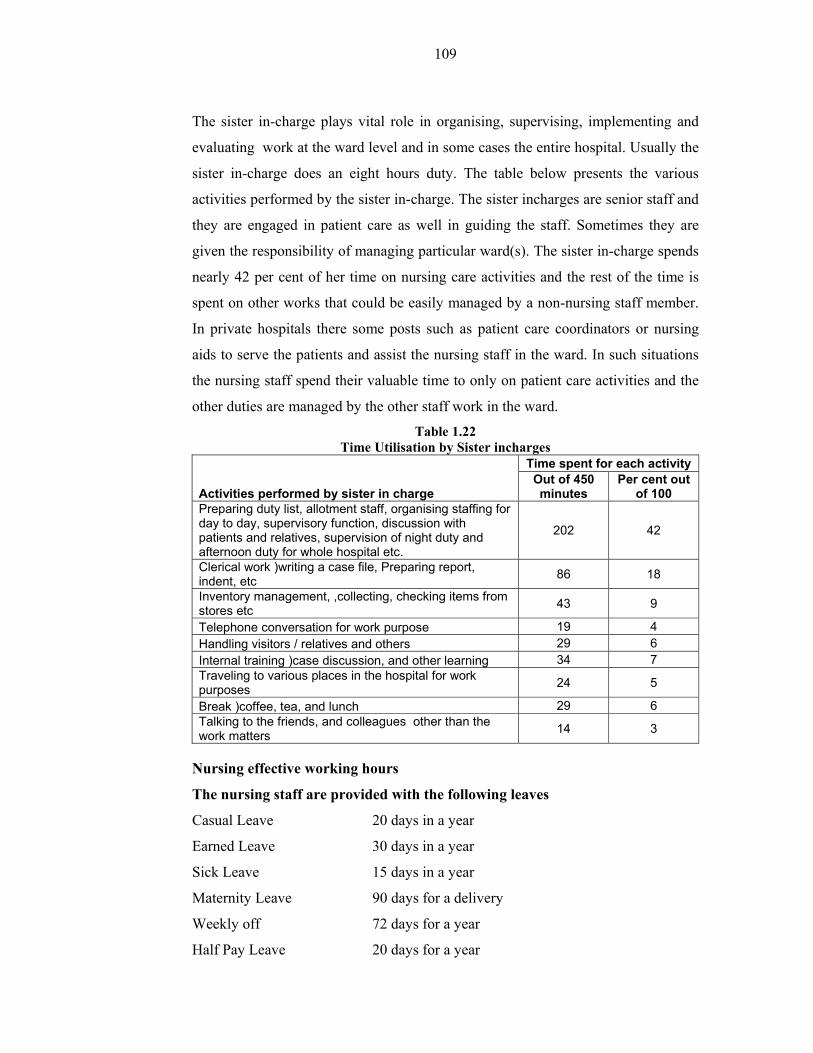
The sister in-charge plays vital role in organising, supervising, implementing and
evaluating work at the ward level and in some cases the entire hospital. Usually the
sister in-charge does an eight hours duty. The table below presents the various
activities performed by the sister in-charge. The sister incharges are senior staff and
they are engaged in patient care as well in guiding the staff. Sometimes they are
given the responsibility of managing particular ward(s). The sister in-charge spends
nearly 42 per cent of her time on nursing care activities and the rest of the time is
spent on other works that could be easily managed by a non-nursing staff member.
In private hospitals there some posts such as patient care coordinators or nursing
aids to serve the patients and assist the nursing staff in the ward. In such situations
the nursing staff spend their valuable time to only on patient care activities and the
other duties are managed by the other staff work in the ward.
Table 1.22 Time Utilisation by Sister incharges
Activities performed by sister in charge
Time spent for each activity Out of 450 minutes
Per cent out of 100
Preparing duty list, allotment staff, organising staffing for day to day, supervisory function, discussion with patients and relatives, supervision of night duty and afternoon duty for whole hospital etc.
202 42
Clerical work )writing a case file, Preparing report, indent, etc 86 18
Inventory management, ,collecting, checking items from stores etc 43 9
Telephone conversation for work purpose 19 4 Handling visitors / relatives and others 29 6 Internal training )case discussion, and other learning 34 7 Traveling to various places in the hospital for work purposes 24 5
Break )coffee, tea, and lunch 29 6 Talking to the friends, and colleagues other than the work matters 14 3
Nursing effective working hours
The nursing staff are provided with the following leaves
Casual Leave 20 days in a year
Earned Leave 30 days in a year
Sick Leave 15 days in a year
Maternity Leave 90 days for a delivery
Weekly off 72 days for a year
Half Pay Leave 20 days for a year

110
In addition to the above there is a provision for abortion leave for the staff and two
permissions for at least 1-2 hours of absence each is granted to the staff in a month.
The sister incharges and senior staff get a weekly one day and half day leave
respectively. Considering the number of off-days and other requirements the
nursing staff’s effective working hours is calculated.
Staff Nurse
Total number of days available in a year = 365 days
Number of days leave in a year 147 days
Net working days = 218 days
As per the above analysis the staff nurses devote 50 per cent of the time for patient
care so the net working time goes to patient care is 109 days i.e. 30 per cent of the
time in the year to patient care, but the staff are paid for the full year. In this case it
is important to note that the working system, organisational ability and old practices
are the primary instruments responsible for not using the working days of staff
efficiently.
As per the above analysis the sister incharges devote 42 per cent of the time for the
core purposes and direct work related issues so the net working time for patient care
is 92 days i.e. 25 per cent of the year for patient care but the staff are paid for the
full year. In this case, too it is important to note that the working system,
organisational ability and old practices are primary responsible instrument for not
using the net working days of staff.
Considering the actual situation, the nursing staff have reported their satisfaction
with regard to time devoted to nursing supervisory and patient care processes. It is
understood that the nursing staff do not allot sufficient time to patient care. It is also
evident in Table 1.23 that only 32 per cent of the staff feel that the time devoted to
patient care is satisfactory and the rest of the respondents feel that non-nursing work
takes more time. Also some of the nursing staff feel that due to the heavy work load
the time spent on each patient is nominal. There are two issues affecting the nursing

111
staff satisfaction with regard to time devoted the patient care process: (1.) There are
more non nursing jobs and (2.) Inadequate time devoted to the patients due to work
pressure.
Table 1.23 Nursing staff satisfaction regarding the time devoted to patient care
What extent do you satisfied with the time you give for patient care?
Present designation
Total Staff Nurse Sister incharges
Not at all (6.8)18 (5.7)3 (6.6)21To some extent (62.5)165 (56.6)30 (61.5)195To a large extent (30.7)81 (37.7)20 (31.9)101Total (100)264 (100)53 (100)317
(Figures in brackets indicate the percentage of nursing staff) N=317
Analysis of nursing tasks
Nursing tasks are considered to be significant ones. There is no doubt that the
nursing staff really contribute to the patient care process meaningfully. However,
the nursing staff do many jobs which are not specific to their profession. In such
cases it may affect the quality of nursing specific work as well decrease the
intensity level of their work. Also there is a scope for developing the perception a
low value is assigned to the nursing profession. Every nurse can choose to do the
job that challenges, is interesting and makes her feel proud. If the staff have an
opportunity to do such kinds of job she is motivated, satisfied and achieves a good
performance. Theoretically speaking the workplace where the employees perform
high complexity tasks shows that there is very low absenteeism Turner and
Lawrence identify five job characteristics and their relationship to personal and
work outcomes. According to the experience and practice of the staff members on
the job activities may rate each characteristic high or low.
1. Skill variety: the degree to which the nursing job requires a variety of
different activities so the nurse can use a number of different skills and
talent
2. Task identity: the degree to which the nursing job requires completion of a
whole and identifiable piece of work.
3. Task significance: the degree to which the nursing job has a substantial
impact on the lives or work of other people

112
4. Autonomy: the degree to which the nursing job provides substantial
freedom, independence, and discretion to the individual in scheduling the
work and in determining the procedures to be used in carrying it out.
5. Feedback: the degree to which carrying out the nursing work activities
required by the nursing job results in the individual obtaining direct and
clear information about the effectiveness of her performance.
These job characteristics such as skill variety, task identity, task significance,
autonomy and feedback or low feedback on the job of nursing can be rated as low
or high for example low skill variety or high skill variety on so on.
Skill variety
As evident in Table 1.24 nearly 69.4 per (very frequently 30.3 per cent and
frequently 39.1 per cent) of staff feel that their job provides opportunities to update
their skills. When the job demands very frequent updates the nursing staff get
involved with a number of jobs or a variety of jobs that could also involve a new
one. In such a case they would require a very high level of skills variety to
accomplish such tasks. Even experienced nurses report that there are many changes
in nursing techniques, work automation and computerisation etc. which are really
challenging for them. In fact, they should be able to tap into their reservoir of
knowledge to tackle the new tasks or use it as a stepping board to update their
knowledge to tackle such tasks. The nursing profession has been undergoing many
changes and demands always high skill variety.
Task identity:
Table 1.24 depicts that nearly 65 per cent (very frequently 24.6 per cent plus
frequently 40.4 per cent) of the staff feel that they are engaged in important jobs
which are identifiable with their own contribution. Since nursing is an activity that
lasts for 24 hours it is mandatory that in each shift the respective nursing staff
accomplish their tasks within their shift timings. Individual work is well-
coordinated and is incorporated in the whole patient care process and it is possible
to identify the particular staff member who is responsible for a particular procedure
which impacted patient care positively. Thus, while the staff members accomplish

113
patient care through collective efforts, every staff member’s contribution is
identifiable in the entire patient care process. The task identity brings significance
clarity on the efforts of nursing patient care.
Task significance:
As seen in Table 1.24 nearly 64 per cent (very frequently 40.70 per cent and
frequently 23.70 per cent) of the staff feel that the nursing job (current work) makes
them feel proud. The nursing staff usually serve the needy and are responsible for
the essential patient care. Patient care has always been considered a significant job.
However, while it is generally expected that the nursing staff would consider the
task nursing highly significant, only about 64 per cent of the staff described their
job thus. This finding is in line with the nursing staff’s opinion about the nursing
profession as lacking when it comes to commanding respect and getting recognition
within the hospital despite years of experience. However the task significance
directly associated with necessity of such tasks to be performed as well the outcome
of such tasks.
Autonomy
That 59 per cent (very frequently 23.70 per cent plus frequently 35.30 per cent) of
the nurses feel that they enjoy a high degree of autonomy to decide their work
schedule and carry out their routine work is also seen in Table 1.24. The job high
autonomy leads to responsibility-oriented staff and ensures that the staff take
personal responsibility for the results. On the other hand, as nearly 41 per cent of
the nursing staff hope that they are not provided with adequate autonomy and in this
case the staff may not take personal responsibility for their own actions. It may be
possible that these nursing staff did not have such exposure. In fact, the nursing
staff are restricted to decisions regarding very few aspects of their routine work.
The staff should follow the instructions of doctors, nursing administration.
Feedback
As visible in Table 1.24 nearly 52 per cent (very frequently 20.8 per cent and
frequently 31.5 per cent) of the staff feel that they get feedback from their superiors
from time to time. A large number of staff, nearly 48 per cent, state that there is no

114
feedback from their superiors. In fact, it is observed that there is no proper system
of monitoring or checking the work done by the staff nurses in the ward. In such an
organisation there is no way to provide feedback to the staff and this also adds to
the difficulty of understanding the nursing staff’s performance from the
management point of view.
Table 1.24
Nursing Job characteristics
Frequency of updating skills and abilities (Skill variety)
Present designation
Total Staff Nurse Sister incharges
Very frequently 80 (30.3) 16 (30.2) 96 (30.3)Frequently 103 (39.0) 21 (39.6) 124 (39.1)Some times 63 (23.9) 10 (18.9) 73 (23.0)Never 18 (6.8) 6 (11.3) 24 (7.6)Task accomplished recognisable easily or identified by you or others (Task Identity) Very frequently 59 (22.3) 19 (35.8) 78 (24.6)Frequently 112 (42.4) 16 (30.2) 128 (40.4)Some times 69 (26.1) 12 (22.6) 81 (25.6)Never 24 (9.1) 6 (11.3) 30 (9.5)Tasks which makes feel proud of being nurse and the task being useful to the hospital Very frequently 105 (39.8) 24 (45.3) 129 (40.7)Frequently 63 (23.9) 12 (22.6) 75 (23.7)Some times 54 (20.5) 6 (11.3) 60 (18.9)Never 42 (15.9) 11 (20.8) 53 (16.7)Frequency of job allows to decide the work schedule, and plan your work with freedom Very frequently 56 (21.2) 19 (35.8) 75 (23.7)Frequently 98 (37.1) 14 (26.4) 112 (35.3)Some times 63 (23.9) 11 (20.8) 74 (23.3)Never 47 (17.8) 9 (17.0) 56 (17.7)Frequency of job/superiors provides feedback about the staff progress and performance Very frequently 52 (19.7) 14 (26.4) 66 (20.8)Frequently 86 (32.6) 14 (26.4) 100 (31.5)Some times 89 (33.7) 17 (32.1) 106 (33.4)Never 37 (14.0) 8 (15.1) 45 (14.2) 264 (100) 100(53) 100(317)
(Figures in brackets indicate the percentage of nursing staff) N=317 Table 1.24(A) clearly evidences that nearly 80 per cent of the staff get oral
feedback. In the absence of a formal mechanism of feedback system the nursing
staff have no way to understand their level of performance.

115
Table 1.24 (A)
Method of feedback to the nursing staff Method the feedback was delivered
Present designation Total Staff Nurse Sister incharges Staff Nurse
Oral 215 (81.4) 39 (73.6) 254 (80.1)Written 0 (0.0) 2 (3.8) 2 (0.6)Both 12 (4.5) 4 (7.5) 16 (5.0)No feed back 37 (14.0) 8 (15.1) 45 (14.2) 264 (100.0) 53 (100.0) 317 (100.0)
(Figures in brackets indicate the percentage of nursing staff) N=317
Meaningfulness of nursing work
The meaningfulness of nursing work means the nursing staff should feel that at the
end of day they have done a useful job and it has really benefited the patients. The
meaningfulness of a job is identified by adding the three variables skill variety, task
identity, and task significance, if these three characteristics exist in the job. It is then
possible to predict whether the incumbent will view the job as important, valuable,
and worthwhile. The following table represents the meaningfulness of nursing
work:
Table 1.25 Meaningful job
Meaningfulness of job High Low TotalSkill Variety 214 (69 ) 103 (31 ) 317 (100)Task Variety 206 (65 ) 111 (35 ) 317 (100)Task Identity 204 (64 ) 113 (26 ) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
It is clear in Table 1.25 that the nursing staff have rated that the tasks which they
perform involves high levels of skill variety (69 per cent), task variety (65 per cent)
and task identity (64 per cent). While the figures are not very high, it can be
concluded that the nursing staff consider that their current job is meaningful and
that nursing does involve meaningful work.
Motivating Potential Score (MPS)
The motivating potential score is computed to identify the significance of the
nursing task. It is computed by adding the scores of skill variety, task identity and
task significance and divide this sum by three and multiply the resulting figure with
autonomy and feedback. The formula for computing MPS is as given below:

116
MPS = skill variety, task identity and task significance x Task identity x Feedback
3
After computing the score, it is further recoded as high or low in the SPSS
programme as is shown in Table 1.26.
Table 1.26
Motivating Potential Score Motivating Potential Score Per centLow 145 (45.7 )High 172 (54.3 )Total 317 (100.0)
(Figures in brackets indicate the percentage of nursing staff) N=317
Jobs that are high on motivating potential score must be high on at least one of the
three factors that lead to experienced meaningfulness (skill variety, task identity and
task significance), and the score must be high on both autonomy and feedback. As
found in Table 1.25 all three factors combine together to form meaningfulness (skill
variety, task identity and task significance) an average score is 64 per cent and the
autonomy score is 59 per cent and feedback 52.3 per cent. It is found that the
autonomy and feedback scores are less than the meaningfulness score.
Further, it could be understood that if the motivating potential score is high, the
motivation, performance and satisfaction will be positively affected, whereas the
likelihood of absenteeism and staff turnover will be lessened. As per the scores in
this table the score is on the higher side at 54 per cent so there must be a slight
impact on employee satisfaction, performance and motivation levels.
Furthermore, there is a need to confirm to the extent the MPS has relationship with
absenteeism, the nursing staff’s self perception on performance and their job
satisfaction. Table 1.27 compares MPS with absenteeism and it is found that when
the MPS is high, absenteeism is low (47.7 per cent). This means that the
motivational potential score does lead to lower levels of absenteeism.
In Table 1.27, while comparing MPS with self perception of nursing staff it is
found that when the MPS is high the nursing staff self perception is slightly high

117
(50.6 per cent). It shows that the motivational potential score leads to some
improvement in the way they look at their own performance. While comparing
MPS with job satisfaction of nursing staff it is found that when the MPS is
relatively high and the nursing staff job satisfaction is also relatively high (64.5 per
cent). This clearly indicates that a high motivational potential score leads to high
job satisfaction among the nurses. In other words, a well designed and challenging
job would increase job satisfaction among the nursing staff.
Table1.27 Comparison of MPS with absenteeism, Self perception and Job satisfaction
Motivating Potential Score (MPS)
AbsenteeismTotal High Low
Low 67 (46.2) 78 (53.8) 145 (100.0) High 90 (52.3) 82 (47.7) 172 (100.0)Total 157 (49.5) 160 (50.5) 317 (100.0) X2 = 1.178 P=0.277
Motivating Potential Score (MPS)
Self perception
Total Low High Low 68 (46.9) 77 (53.1) 145 (100.0) High 85 (49.4) 87 (50.6) 172 (100.0)Total 153 (48.3) 164 (51.7) 317 (100.0) X2 = 0.200 P=0.654
Motivating Potential Score (MPS)
Job Satisfaction
TotalLow High Low 76 (52.4) 69 (47.6) 145 (100.0) High 61 (35.5) 111 (64.5) 172 (100.0)Total 137 (43.2) 180 (56.8) 317 (100.0) X2 = 9.209 P=0.002
(Figures in brackets indicate the percentage of nursing staff) N=317
Nursing work related Problems
The nursing staff have to work with various categories of the people in the hospital.
Usually they work with patients, the patient’s relatives, visitors, doctors, class IV
staff, co-workers and the administrative staff. While working with a variety of
personalities they are likely to face some problems. These problems basically relate
to work procedures, systems, work pressure, non-cooperation from colleagues and
misunderstanding about the context. The details of some of the problems are
discussed below.

118
Problem faced with patients
When the question about patient related problems was posed to the nursing staff a
majority of the nursing staff replied “In the ward we face many problems from the
patient’s side”. It is a unanimous opinion among the nursing staff. The nursing staff
have highlighted some of the major problems like consumption of alcohol,
shouting at the staff, arguments, asking for special care, smoking, lack of patience,
not allowing completion of certain procedures essential to patient care, lack of
communication, language problems, demanding more time and facilities, frequently
being irritating , creating tension in the ward, not paying their dues for operation
and medicinal purchases, encouraging visitors during non-visiting hours, arguing
about or fighting for medicines that are not available , non co-operation, not
following the given restrictions or procedures, absconding from the ward,
overcrowded wards, lack of satisfaction for the services extended, complaining
about everything, use abusive language, troubling/ threatening the staff with
political connections to satisfy their own whims. Most of these problems are
chronic and recurrent and it is very difficult to curb them. The staff need more
support from the management to solve many of these problems. Also, the nursing
department should focus on the issues which affect the nursing staff directly or
indirectly.
Problems faced with Patients’ relatives
The patient relatives present more problems than the patients themselves. The usual
problems are vociferous arguments due to non-availability of medicines, arrogant
behaviour, involving political bigwigs (corporators), visiting at any time and not
following the visiting hours schedule, using foul language, disturbing other patients
in the ward, not attempting to understand the explanations given by the nursing
staff due to lack of basic knowledge and yet interfering with the nursing work,
fighting with the nursing staff, not listening to the requests of the staff, over-
crowding, etc. These problems are daily affairs for most of the nursing staff. In fact,
the visitors behave as per their own wishes and norms, disregarding hospital rules.
It is found that the nursing staff have given up on their efforts to control the visitors
in the ward because it has become a routine for the visitors to enter the hospital at
any time and not abide by hospital rules.

119
Problems faced with Class IV staff
It is expected that the class IV staff extend complete support to the nursing staff, but
the reality is just the opposite in the study hospitals. The nursing staff face several
problems in day-to-day management of the ward because of the class IV staff.
Some of the usual problems faced by the nursing staff are that the class IV staff
periodically abscond from the work place, absenteeism, engage in open rebellion of
the nurses, do not follow given instructions, consume alcohol while on duty, sleep
while on duty, don’t follow the activities logically, , exhibit arrogant behaviour,
indulge in unacceptable practices that are unethical at times , etc. It is observed
that there is a strong union for class IV staff in every hospital. It is therefore
difficult to take any kind of disciplinary action against them. The current situation
seems to be uncontrollable and at any given point of time the hospital management
can face serious problems due to the lack of cooperation and support from the class
IV staff in the study hospitals.
Problems faced with peer groups
The nursing staff stated that did face some problems with their colleagues. The
usual problems include colleagues reporting late for duty or substitution ,
occasional absenteeism which leads to double duty, lack of communications
resulting in misunderstandings and shortage of staff which adds to the work
pressure, becoming sick, inability to leave for long periods of time .
Problems faced with doctors
The doctors usually come late and (re)write the patient care orders which affect
routine work of the nursing staff. The late arrival of most doctors leads to the nurses
having to answer patients’ queries that might lead to arguments and fights.
Sometimes there is no support extended to the nursing work by the doctors for work
related issues. Some of the young doctors do not understand the ground reality of
the system wherein the nursing staff faces a few problems with both the
administration and the patients.

120
Problems faced with administration
The administration fails to provide even the minimum work facilities. They are
unable to understand the practical issues that the nurses have to grapple with. They
are unable to organise the required supplies for the patient care, for which the
nurses bear the brunt of the patients’ ire. They are often uncooperative even on
work related matters and maltreat the nurses at times.
Supervisory Responsibilities
Sister in charge supervisory responsibilities
The Sister incharges are responsible for supervising the nursing staff in the ward.
The number of persons to be supervised based on the ward size and the number of
staff they supervise because of the nursing staff allocation is based on the number
of beds occupied in each ward and the ward size.
Table1.28 Number of staff supervised by sister in charge
Supervision of Nursing staff Per cent
Up to 2 staff 14 (26.4)2-4 staff 12 (22.6)5-6 staff 12 (22.6)7 and above 15 (28.3)Total 53 (100.0)(Figures in brackets indicate the percentage of nursing staff) N=317
Usually the senior staff supervises two to seven nursing staff in her wards.
However, in actuality, nearly 28 per cent of the sister incharges supervise more than
seven nursing staff members. When the number of staff needing supervision is high
the sister incharges have to pay more attention to the ward and the management of
the staff nurses in addition to the class IV staff and the management of inventories
in the ward is a huge burden that befalls them. There are several difficulties in
supervising the staff in the hospital. The sister incharges face certain problems at
their level just as the nursing staff face some problems at their level. The sister
incharges have to manage certain issues absenteeism of staff nurses, arrangement
for substitutes, management of long leave for various staff members , ensuring
material supply, checking up on class IV staff availability, coordinating between
the staff and the matron office, etc.

121
Supervisory role of staff nurses
The staff nurses have to supervise some of the other staff nurses and the class IV
staff while discharging their duty. It is found that a considerable number nursing
staff have put in long years of services but did not get promoted and such nursing
staff are given supervisory responsibilities establishing them as senior nurses. The
senior nurse position is not an official one. In this case the senior nursing staff shall
supervise the nursing staff. Nearly 48 per cent of the senior staff supervises one or
two staff nurses and the class IV staff. Nearly 10.6 per cent of the staff nurses
supervise 5-6 class IV staff during their duty hours. It is observed that supervisory
responsibilities lead to tension. Some of the usual problems associated with class IV
staff supervision are absconding from the work place, disobedience, drinking and
sleeping while on duty, trouble-making, and non-cooperation.

122
PART-2. WORKING CONDITIONS AND FACILITIES
This part of the chapter is based upon findings and analysis of working conditions
and facilities provided by the hospitals for the nursing staff to carry out the
functions.
2.1 Physical Facilities
Healthcare delivery is a dynamic process which involves use of appropriate inputs.
The inputs include various resources like human resources, material resources and
financial resources. The human resources concern doctors, nursing staff, technical
staff, maintenance staff, housekeeping staff, etc. The material resources include
medical, surgical and consumable items and other technical support necessary for
patient care. In order to provide better patient care hospitals need to maintain their
equipments and possess the right quantity of material supply Quality material made
available at the right time is very important for proper healthcare delivery. At the
same time, adequate facilities like drinking water, sanitation, communication
facilities will help the staff members achieve patient care goals. The hospitals
should be in a position to provide these items in a timely and efficient manner. The
non-availability of physical facilities may affect healthcare delivery as well as bring
down the performance levels of the nursing staff and their job satisfaction.
Keeping this in view, a structured questionnaire was administered to the nursing
staff to understand the current situation with regard to material availability. The
nursing staff’s comments on the status of physical facilities availability in the
study hospitals. is presented in Table 2.1
Equipment availability is one of the major concerns in the study hospitals. All these
hospitals have been provided with the bare minimum equipments which are
essentially needed for providing patient care. However, the respondents working in
different departments reported that there has been inadequate provision of
equipment to meet even the minimum requirement of patient care. The majority of
the respondents, nearly 80 per cent, feel that there is a need for an increase in the
availability of equipments as well as an improvement in their functionality and
maintenance to provide adequate patient care. It should be noted that there is a

123
slight difference of opinion between the staff nurses and the sister incharges in
terms equipment availability and that the sister incharges are more positive than the
staff nurses.
Table 2.1
Grading the facilities available in the hospital
Physical Facilities Grading Staff Nurse Sister incharges
Total
Equipment Not at all 12 (4.5) 0 (0.0) 12 (3.8)To some extent 212 (80.3) 43 (81.1) 255 (80.4)To a large extent 40 (15.2) 10 (18.9) 50 (15.8)
Material supply Not at all 7 (2.7) 0 (0.0) 7 (2.2)To some extent 220 (83.3) 45 (84.9) 265 (83.6)To a large extent 37 (14.0) 8 (15.1) 45 (14.2)
Safe drinking water Not at all 67 (25.4) 12 (22.6) 79 (24.9)To some extent 96 (36.4) 17 (32.1) 113 (35.6)To a large extent 101 (38.3) 24 (45.3) 125 (39.4)
Basic sanitation facilities
Not at all 38 (14.4) 7 (13.2) 45 (14.2)To some extent 97 (36.7) 17 (32.1) 114 (36.0)To a large extent 129 (48.9) 29 (54.7) 158 (49.8)
Communication facilities
Not at all 23 (8.7) 2 (3.8) 25 (7.9)To some extent 90 (34.1) 21 (39.6) 111 (35.0)To a large extent 151 (57.2) 30 (56.6) 181 (57.1)
Place for dining Not at all 59 (22.3) 7 (13.2) 66 (20.8)To some extent 83 (31.4) 14 (26.4) 97 (30.6)To a large extent 122 (46.2) 32 (60.4) 154 (48.6)
Dress changing room Not at all 20 (7.6) 1 (1.9) 21 (6.6)To some extent 95 (36.0) 17 (32.1) 112 (35.3)To a large extent 149 (56.4) 35 (66.0) 184 (58.0)
Total 264 (100.0) 53 (100.0) 317 (100)(Figures in brackets indicate the percentage of nursing staff) N=317
Similarly, it is expected that the supply of material should be regular, without any
delay as well adequate in quantity. The majority of the respondents, nearly 84 per
cent, opinion that the hospital material supply such as medicine, linen and other
consumables are not sufficiently provided by the administration. In other words, the
material supply is inadequate for the staff to manage even the basic requirement of
patient care and definitely not up to the standards that would satisfy the patients
with the level of care that they have been provided with. Here too the sister
incharges exhibit a more positive outlook than the staff nurses.
With regard to other facilities like safe drinking water provided in the hospital only
39 per cent of the staff feel that they have adequate safe drinking water facility.

124
Nearly one fourth of staff report that there is no provision for safe drinking water in
their wards. The basic sanitation facilities are adequate according to nearly 50 per
cent of the staff. However, nearly 14 per cent of the staff mentioned that they do not
have any provision for basic sanitation facilities in their wards. There is just a
slight variation in the opinions of the staff nurse and the sister incharges. Nearly 38
per cent of staff nurse and 45 per cent of the sister in charge feel that drinking water
facilities are adequate, and nearly 49 per cent of staff nurse and 55 per cent sister in
charge feel that the basic sanitation facilities adequately provided. It is to be noted
that the staff are working long hours nearly eight hours in day shifts and ten hours
in night shift and sometimes the staff do double duty and need to use these
facilities. The absence of such facilities situation lead to poor hygiene and also
affect the health of the staff. In addition to the above, there is a possibility for lack
of sanitation to lead to an increase in sources for infection in the very place where
patients are in a condition most susceptible to them. It has been observed that in the
initial planning of the hospital’s basic building structure there had been no
provision made for adequate toilet facilities in some of the important locations
including the wards and in the officers’ rooms. That the current buildings could
support an increase in toilets or water cooler areas is doubtful. However, the
management has to seriously focus on these issues and support the staff as much as
possible.
The communication system is a part of the patient care delivery system in the
hospital. Internal communication facilities like intercom facility, and telephone
connection to local hospitals are extremely essential and useful to the staff while
working in a ward. All the study hospital have made adequate provisions for better
communication facilities in the hospitals. Nearly 57 per cent of the staff feel that
they have been adequately provided with communication facilities.
Nearly 49 per cent of the staff opined that they have adequate place for dining while
21 per cent stated that they do not have any provision for dining facilities in their
ward or in the hospital. There is a significant variation in the opinions of the staff
nurses, nearly 46 per cent, and the sister incharges, 60 per cent, who report that the
dining facilities are adequate. In some of the hospitals the nursing staff are allowed

125
to use the dining hall located in nursing students’ hostel which is little away from
the wards.
Since the majority of the staff stay far from the hospital and travel long distances,
they prefer to come to the hospital in civilian clothes. They prefer changing to their
uniforms before signing the attendance register and this is the norm in all the
hospitals. Nearly 58 per cent of the staff nurses have reported that they have been
provided with changing rooms. Regarding the adequacy of the changing rooms
nearly 56 per cent of the staff nurses as compared to 66 per cent of the sister in-
charge reported that they have adequate changing room facilities in the hospitals.
The overall opinion of the staff regarding the availability of the physical facilities
has been presented in Chart 2.1
Chart 2.1
Nursing staff’s opinion on the physical facilities available in the study hospitals
Nursing staff opinion on physical facilities
4 2
2514 8
217
80 84
36 36 35 31 3516 14
3950 57
4958
0102030405060708090
Equi
pmen
ts
Mat
eria
ls s
uppl
y
Safe
drin
king
wat
er
Basi
c sa
nita
tion
faci
litie
s
Com
mun
icat
ion/
int
erco
m
Plac
e fo
r din
ing
Dre
ss c
hang
ing
room
Not at allTo a some extentTo a large Extent
Chat-2.1 indicates that none of facilities meet the compete requirement of the staff.
However communication facilities and dress changing room has exceed above 50
per cent and the other facilities have no significant contribution to the nursing staff
requirement.
In addition to the availability of material, it is also important that the material be
accessible at the right time. Sometimes the material may be stocked in the storage
areas, but they may not be accessible to the staff due to various reasons such as

126
lengthy procedure, lack of authority, or similar reasons. Among the respondents the
sister incharges are expected to have better access to inventory because of
supervisory and administrative requirements. The opinions of the staff nurses and
the sister incharges on physical facilities presented in Table 2.2.
Table2.2
Overall Opinion of nursing staff with regard to physical facilities
Designation
Opinion on Physical facilities availability Total
Low High
Staff Nurse 56.1 43.9 100
Sister In-charge 47.2 52.8 100
Total 54.6 45.4 100
Only 44 per cent of the staff feel that the physical facilities provided rate high in
adequacy whereas 53 per cent of the sisters incharge feel that the physical facilities
availability is high. It is clear that the sister incharges who are of the opinion that
they could access physical facilities are in a better position. This is in line with the
functional authority of the sister incharges. In other words, the sister incharges are
responsible for the management of wards and they directly deal with the
administration and management of material and therefore seem to have fewer
problems with the accessibility of material than the staff nurses.
2.2 Managing the patients in case of non-availability of facilities
Nearly 51 per cent of the staff feel that the patients have suffered due to non-
availability of material in the ward and the hospital. Comparing the staff nurses and
the sister incharges opinions on the issue of the negative effect of non-availability
of physical facilities on patient treatment it is evident that while nearly 50 per cent
of the staff nurses state that patient care suffered due to the non-availability of
material, only 43 per cent of sister incharges feel the patient care was affected by
the non-availability of physical facilities. Overall, 49 per cent of the nursing staff
have reported that patient care suffered due to the lack of availability of material in
the hospitals.

127
Table 2.3
Impact of lack of facilities on patient care
Do you have an experience in the past where
due to non availability of material the patient
care was suffered irrespective all your efforts?
Present designation
Total Staff Nurse
Sister
incharges
No 133 (50.4) 30 (56.6) 163 (51.4)
Yes 131 (49.6) 23 (43.4) 154 (48.6)
Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
Since the nursing staff are in direct contact with the patients and they have the
responsibility to provide facilities, guidance and support to the patients during the
course of their entire stay at the hospital, it becomes necessary for the staff to take
some steps to improve the conditions in case the material supply is inadequate or
there is a complete lack of the same in the ward. The nursing staff’s experiences of
managing patients in case there are no medicines or linen or any other facility
available in the ward is shown in Table 2.4.
Table 2.4 Management of patients incase of non-availability facilities
Sl. No. Nursing staff action against non availability of facilities Percentage
1 To follow as per the direction of supervisors/doctors 34
2 Ask the patients or relatives to bring items (medicines, surgical items etc) incase of shortage and they buy from outside
63
3 Only inform superiors and they shall manage 21 4 Incase of need for equipments shall be taken from wards 15
5 Transfer the patient if no service available or higher level of treatment is required to other hospital as per doctor’s instruction
49
6 Give prescriptions to the patients and referring to medical social worker for any other support
76
7 To maintain some material for emergency and take it from other ward
35
In case some of the facilities are not available in the ward or in the hospitals, the
nursing staff ask the patient or their relatives to get such material from outside. If
the facility are complex such as a higher level of treatment , the patients will be
shifted to medical college hospitals because peripheral hospitals are not tertiary care
centers and hence, these hospitals have only limited facilities. It is to be noted that

128
in the study hospitals, facilities like ICU, blood bank, emergency care, diagnostic
equipments like CT Scan, MRI, etc. are not available as per regulatory standards.
2.3 Additional facilities needed for Nursing staff and Patients
Facilities needed for Patients
The nursing staff is of the opinion that there is a need for adequate material supply
for the patients. As indicated earlier, a large number of staff feel that the material
supply is inadequate in the hospitals. Nursing staff feel that some material like
linen, medicines, good diet, disposables, advanced technological machines; number
of beds, antibiotics should be available adequately. Apart from this, the staff also
feel that there is a need for additional services like blood bank, X-ray facilities and
lab services at night, CT scan, MRI, ECG facilities, ICU services, dressing rooms,
drinking water, stationery, blood investigations injections, clean place, proper
educational means and methods for the patients, channels to provide emotional
support to the patients are essential. In addition to the above, free treatment for poor
patients and adequate security guards to control overcrowding in the hospitals
should be provided.
Facilities need for nursing staff
The nursing staff feel that the primary requirement is adequate staff as per staff
nursing council norms (better staff-patient ratio), safe drinking water facilities with
purified aquaguard water, baby-sitting support, bank concession for 2 hours (to do
personal banking work), card swiping instead of manual logging in of arrival and
departure, training and educational facilities for the staff, educational and loan
support for the staff’s children, adequate bathroom and toilet facilities, canteen
facilities, removal of double duty, changing room, locker facilities, common room,
concession on medical treatment, dining room at one or two locations (inpatient or
outpatient areas), official lunch break, rooms for the staff to rest in between their
duty, staff quarters, good salary, additional staff as relievers, more support from
class IV staff, good management, increase in uniform allowance, cabin or locker
for the staff, sick rooms (specialty), time bound promotions, proper nursing stations,
adequate stationeries, suitable duty hours, patient-safety material, staff learning
opportunities, schools of nursing, safety and security for staff particularly from

129
alcoholics, respect for the staff, presence of adequate Class IV staff, free tea, dinner
and breakfast for the night staff and reasonable work hours for those on afternoon
and night In addition to the above, the nursing staff expect to be given authority to
discharge (after getting doctor’s discharge instructions) the poor patients (subject to
confirm with proper records as their poor status) in case they are unable to pay at
any time.
2.4 Safety and Security for the nursing staff
Safety and security is very important not only for the staff but also for the patients.
The nursing staff primarily need safety and security in the workplace. Since the
nursing staff provide round-the-clock services, and work in an environment that is
accessible to any and everyone they are naturally concerned about their
vulnerability to physical and psychological threats. Nearly 44 per cent of the staff
have mentioned that they have no confidence in the safety and security measures in
the hospital premises. The nursing staff’s opinion on this issue is presented in
Table 2.5.
Table 2.5 Safety and Security of nursing staff
Security and safety for staff
Present designation
Total Staff Nurse Sister incharges
Not at all 118 (44.7) 20(37.7) 138 (43.5)To a some extent 75 (28.4) 17 (32.1) 92 (29.0)To a large Extent 71 (26.9) 16 (30.2) 87 (27.4)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317 Safety and security is considered to be an important issue in any work place.
However, the hospitals that are supposed to cater to the well-being of the patients
seem to be grossly negligent of the well-being of the staff as a considerable number
of the staff are emphatic about this lack, particularly, those involved in night shifts
and those working in the male wards. While the sister incharges also expressed
similar feelings, only 38 per cent say that there is a lack of safety and security in the
work place. It is a major challenge for the hospitals. Few hospital administrators
have indicated that there is a lack of security personnel in the hospital due to which
the lack of security will be exacerbated.

130
2.5 Hospital Policies and Rules
All hospitals under the BMC including the study hospitals have been following the
guidelines of BMC health policies. Most of the rules are the same across the
hospitals. However, certain rules are designed such that they are specifically
applicable to the peripheral hospitals of the BMC. The rules governing the hospital
should be known to the staff so that they may able to follow them properly. Also the
employees should be made to understand the implementation of the rules is uniform
and that there is no discrimination. The respondents have given their opinion in this
regard which is presented in Table 2.6.
Table 2.6 Nursing staff’s opinion on hospital rules
Opinion on Rules Yes/No Staff Nurse Sister
incharges Total
Are you aware of leave rules? No 12 (4.5) 1 (1.9) 13 (4.1)Yes 252 (95.5) 52 (98.1) 304 (95.9)
Are you satisfied with the leave rules?
No 37 (14.0) 4 (7.5) 41 (12.9)Yes 227 (86.0) 49 (92.5) 276 (87.1)
Are you aware of transfer policies?
No 35 (13.3) 3 (5.8) 38 (12.1)Yes 228 (86.7) 49 (94.2) 277 (87.9)
Are you satisfied with the transfer policies?
No 44 (18.4) 12 (23.5) 56 (19.3)Yes 195 (81.6) 39 (76.5) 234 (80.7)
Are you aware of Promotional policies?
No 40 (15.2) 1 (1.9) 41 (12.9)Yes 224 (84.8) 52 (98.1) 276 (87.1)
Are you satisfied with the promotional policies?
No 152 (57.6) 33 (62.3) 185 (58.4)Yes 112 (42.4) 20 (37.7) 132 (41.6)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the percentage of nursing staff) N=317
Nearly 96 per cent of the staff are aware of the leave rules which are applicable to
them and which are followed in the hospital. Nearly 87 per cent of the staff are
satisfied with the leave rules. The nursing staff are provided with an adequate
number of leaves. They usually take leave and hence are clear on the same.
However, the need for some additional provisions with regard to leave is felt as has
been mentioned in Table 2.7. Nearly 88 per cent of the staff are aware of the transfer rules as applicable
according to the hospital they work in. Nearly 82 per cent of the staff are satisfied
with transfer rules (Table 2.6). The staff members feel that certain provisions which
are applicable to the staff with regard to transfer is dissatisfactory because it affects
their seniority. It is also opined that when the staff are transferred from the medical

131
college hospital to the peripheral hospitals, their records are not properly
transferred, there are a few incidents narrated by the staff wherein their transfer
records got misplaced by the hospital authorities. In such cases the staff have to
travel in between their duties to these hospitals to sort out the issue. It affects the
nursing staff’s morale. One of the hospital administrators confessed that the BMC
rule that any person transferred from the medical college to a peripheral hospital
shall lose their seniority is to dissuade the staff from applying for a transfer because
getting an adequate number of trained staff for medical colleges is difficult. There
are certain concerns expressed by the nursing staff with regard to transfer policies
as mentioned in Table 2.7.
As seen in table 2.6 nearly 87 per cent of the staff are aware of the promotion rules
that are applicable to them as per their hospital regulations. Nearly 42 per cent of
the staff are satisfied with the promotion rules. Promotion is considered a major
issue for the management as well for the employees. According to the employees
they expect promotions to be time bound and based on seniority or experience.
Whereas the Government expects certain formalities that need to be completed,
certain procedures and regulatory measures followed,. with regard to promotions
the staff members would like some additional provisions which have been
mentioned in Table 2.7.
Table 2.7 Suggested changes in the Hospital Rules
Leave Rules
Maternity leave should be provided for at least six months, every six months the staff should be given 10-15 days as a long holiday, leave should be sanctioned as per the staff’s needs, second and fourth Saturday should be declared a holiday, sick leave should be increased, staff should not be denied leave or forcefully asked to work when there is a shortage of staff.
Transfer Rules
Transfer of staff should be taken into consideration based on experience, staff working in BMC healthcare institutions should get transfers immediately without losing their seniority, mutual transfers should be accepted, transfer policies should be more transparent, and transfer policies should include the provision of nearest distance from home, transfer should not be linked with promotion, staff personal records particularly after transfer from one hospital to another should be kept in safe custody, administration should follow the rules as they are.
Promotion Rules
Promotion should be given based on higher education, experience, and seniority, after every 10 years of service the staff nurse should be promoted to the next level, promotion should be based on experience and performance, common test should be introduced for promotion, State and Central Governments’ rules need to be followed for promotions, promotion should be given without transfer, caste based reservation policies should not be considered for promotion.

132
2. Professional Development
A person professionally trained will be have adequate knowledge in her areas of
work. The work knowledge includes theoretical, practical, and clinical aspects. She
would apply such knowledge based on evidence or theoretical inputs. She would
able to share or communicate such knowledge to colleagues, clients and others to
bring out the best outcome. The professionally oriented person is usually open-
minded, interested in refinement of existing knowledge, striving to define patterns
of responses from patients, hospital authorities, and committed to life-long learning.
The professionals show accountability by understanding and following, ethical
standards, self-regulation and rules in practice in her work place. She shows
commitment to her patients and strives to achieve desired results and is actively
engaged in enhancing the quality of services provided. The professional staff
member exercises autonomy by independently, taking decisions, understanding the
limitations of autonomy and tackling the barriers to autonomy and seek remedy for
a particular situation. Since the nursing staff are considered to be professionals, they
posses all the said qualities. However, in the current situation the nursing staff’s
ability to align personal and organisational goals with ethical and professional
standards that include a responsibility to the patient and the community, a service
orientation, and a commitment to life-long learning and improvement have become
the major concerns. Continuous learning will lead to a better understanding of the
work process whereby the staff are able to provide patient care up to the requisite
standards. The nursing staff have expressed their opinion on the importance of
continuous training that would useful to them in Table 2.8.
Table 2.8 Nursing staff’s opinion on continuous training
How important do you think continuous
training is useful for nurses? Present designation Total Staff Nurse Sister incharges
Not Very important 4 (1.5) 3 (5.7) 7 (2.2)Not important 6 (2.3) 1 (1.9) 7 (2.2)Neither or nor important 6 (2.3) 2 (3.8) 8 (2.5)Important 118 (44.7) 14 (26.4) 132 (41.6)Very important 130 (49.2) 33 (62.3) 163 (51.4)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets Percentage the number of nursing staff) N=317

133
It is expected that the nursing staff will act with bearing in mind the perspectives of
their patients, continue to learn the needs of the patients, take initiatives to enhance
the knowledge about their patients, and try to establish adequate policies for their
work areas.
Nearly 51 per cent of the staff feel that continuous learning and training is very
important for professional development also 42 per cent of the staff feel that the
training and development will be very useful to achieve greater performance at
work. Even though the nursing staff are very keen on learning and enthusiastic
about professional development there are few opportunities provided to the nursing
staff, the details of which are provided in Table 2.9.
Table 2.9 Professional development opportunities provided to the nursing staff
Sufficient opportunities provided for continued professional development by the hospital management to nursing staff
Present designation Total Staff Nurse
Sister incharges
No 113 (42.8) 11 (20.8) 124 (39.1)Yes 151 (57.2) 42 (79.2) 193 (60.9) 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317 Nearly 39 per cent of the nursing staff expressed that they did not have an
opportunity to continue their learning in the hospital. However, when considering
the number of staff that have attended training programmes it is found that nearly
37.8 per cent have attended only one programme and 48.7 per cent have attended
two programmes. The training programmes organised by the hospitals are given
below.
2.1 Title of training programmes
The hospitals have organized few training programmes for the nursing staff and the
nursing staff attended the same during the last two to three years. The training
programmes were: management of HIV-AIDS patients, waste disposal systems and
management; bio-Medical waste management system; burns care and management;
basic computer training; breast feeding; diabetics management, pediatrics care;
cancer care management; disaster management; domestic violence; gadget
Suturing; NICU; premature management; RCH training; eye donation; ventilator
management; personality development; RNTCP; Safe delivery and stapler method.

134
It is understood that the majority of the programmes were organized in the hospitals
basically focused on infection control, communicable diseases management, and
meeting certain legal requirement and personal safety of the staff.
2.2 Employer support for training programme
Usually it is expected from the hospital management to provide necessary support
like financial support, leave with pay, sponsorship etc. for training and professional
development of the nursing staff. Most of the training programmes are organized
within the hospital or within Mumbai. Very few nurses have gone outside trainings.
The hospitals have provided support in terms of finance and leave-with-pay for the
staff.
In addition to the above, it is very important to note that the quality of training and
usefulness of the training programmes. Sometimes the same is repeated or there is
no importance given to the latest developments or an advanced course in nursing
does not make any sense to the nursing staff. It has been observed that a majority of
the past training focused on the nursing staff and patient safety related topics. Few
programmes were organised to strengthen the knowledge and the skills of the
nursing staff. Keeping this in view, a structured questionnaire was administered to
the respondents to give their areas of interest for future training programmes. The
majority of the staff expressed interest in different topics for training. The details
are given below.
2.3 Future (next 2 to 3 years) Training needs for the nursing staff
Technical Areas: Advanced nursing information technology; patient safety and
computerization; biomedical engineering; ECG reading and recording; operation
theatre techniques and management, latest technology and medicines; modern
technology and equipment handling techniques; sterilization and fumigation.
Advanced Nursing courses: Advanced nursing care techniques; BCG training;
advanced ICU nursing; breast feeding; pediatrics nursing procedures; hygiene
practices; cardiology nursing; emergency management; HIV-AIDS management;
developing creative nursing care; health malnutrition; ICCU nursing care

135
management; neurology; latest update of nursing; neonatal care; family planning;
oncology; pediatric and premature; refresher course on advance nursing; etc.
Other Areas: communication skills; motivational techniques; health education;
cleanliness; infection disease management and control; medical law and medical
legal aspects; waste disposal management; administrations and ward management;
stress management. It is found that all the above areas are very important fields
which are highly essential aspects of professional development. Keeping this in
mind, the nursing staff were requested to report on the present conditions that exist
in the hospitals enabling learning and development. The nursing staff’s responses
are presented in Table 2.10
2.4 Enabling climate for nursing professional development in the hospital
The current situation in the hospitals about the nursing professional development is
discussed as follows:
Table 2.10 Organisational Support regarding professional development
Opinion on Rules Yes/No Staff
Nurse Sister incharges
Total
Does your superior encourage your new ideas
No 65 (24.6) 15 (28.3) 80 (25.2)Yes 199 (75.4) 38 (71.7) 237 (74.8)
Have you been encouraged to develop your full potential as a nurse
No 86 (32.6) 20 (37.7) 106 (33.4)Yes 178 (67.4) 33 (62.3) 211 (66.6)
Have you been given your personal career development as high priority by superiors
No 107 (40.5) 25 (47.2) 132 (41.6)
Yes 157 (59.5) 28 (52.8) 185 (58.4)Have you been supported if applied for study leave
No 122 (46.2) 26 (49.1) 148 (46.7)Yes 142 (53.8) 27 (50.9) 169 (53.3)
(317)100 100 (317) 100 (317)(Figures in brackets indicate the percentage of nursing staff) N=317
The majority of the nursing staff (74.8 per cent) feel that their superiors encourage
their new ideas and permit their use in work related matters. Nearly 66.6 per cent of
the staff feel that the superior staff have been encouraging to develop themselves up
to their full potential as nurses. Nearly 58.4 per cent of the nursing staff feel that the
superiors give importance to the nursing staff’s personal career development.
Nearly 53 per cent of the staff feel that they get study leave for pursuing higher

136
studies if they apply for it. Further, to understand the overall climate for
professional development details are presented in Table 2.11.
Table 2.11
Enabling climate for professional development
Enabling climate
Present designation
Total Staff Nurse
Sister
incharges
Low (42.4)112 (47.2)25 (43.2)137
High (57.6)152 (52.8)28 (56.8)180
Total (100.0)264 (100.0)53 (100.0)317
(Figures in brackets indicate the percentage of nursing staff)
N=317
Overall the enabling climate for professional development is slightly better (nearly
57 per cent) in the hospital.
2.5 Performance Appraisals
Performance appraisal is not only a formal procedure to assess the performance of
the staff but also a means of providing feedback to them to improve their
performance. However, an effective performance appraisal system can be difficult
to implement, especially if front-line supervisors are responsible for large numbers
of nursing staff as is the case with the nursing supervisor. Therefore, the employees’
understanding about performance appraisal systems and how it is perceived by the
employees for professional development is important. In practice there are some
methods of performance appraisals. They are self appraisal, formal interview of the
staff by a competent team and writing confidential reports. Nearly 99 per cent of the
staff say that writing a confidential report is the only means of performance
appraisal system in their hospitals. There is no other effective performance
appraisal system in place in the hospitals. The confidential report is written by the
superior on the performance of the subordinates. This system is lacking as it
offers no scope for giving appropriate feedback to the staff so that they may
improve. The confidential report is written for every year for each nursing staff and
once in two years for sister incharges. However, of the nursing staff nearly 19 per
cent have mentioned that there was no confidential report writing as per the

137
schedule in the last six years. Many staff nurses also confirmed that there is no
effective feedback from the higher authorities that would enable the nursing staff to
improve their performance. It is observed that it is not a matter of concern to the
nursing staff or the superiors or the hospital administration because there are too
many aspects to handle.
3. Collaborative relationship and team work
A team is a collection of individuals who are interdependent in their tasks, who
share responsibilities for outcomes, who see themselves and who are seen by others
as an intake social entity embedded in one or more larger social systems, and who
manage their relationships across organisational boundaries. Work teams are
continuing work units like operation theatre, wards, critical care units and other
important areas responsible for producing goods or providing services. Work teams
are directed by superiors who make most of the decisions about what is done, how
it is done and who does it.
Healthcare services are expanding their reach in different directions due to various
aspects like specialties, research and development and other complexities. These
aspects demand more understanding, participation and interaction and cordial
relationships. It would be possible to achieve the desired output (better patient care)
only by effective interaction, collaborative relationships and effective
communication among the various professionals and non-professionals working in
the hospital. The situation is such that healthcare cannot be provided by a single
individual. In a large sized hospital several persons are a part of the patient care
delivery system. The team work and collaborative relationships complement each
other.
Team work reflects on how the people working together in an organised setup have
opportunities to participate in the team process. Similarly, the collaborative
relationship reflects the existence of good communication, faith among the
members and respect for each other. These aspects are discussed in Table 2.12.

138
Table 2.12 Working together in collaborative manner to achieve the team effectiveness
Work team relations Grading Staff Nurse Sister incharges
Total
Doctors, nursing staff, class IV employees and administrative staff work together as a team
Not at all 6 (2.3) 0 (0.0) 6 (1.9)To some extent 155 (58.7) 23 (43.4) 178 (56.2)To a large extent
103 (39.0) 30 (56.6) 133 (42.0)There is an opportunity to participate in meetings, discussions, sharing information related to nursing work
Not at all 27 (10.2) 2 (3.8) 29 (9.1)To some extent 124 (47.0) 21 (39.6) 145 (45.7)To a large extent
113 (42.8) 30 (56.6) 143 (45.1)The team members communicate freely with one another
Not at all 12 (4.5) 1 (1.9) 13 (4.1)To some extent 132 (50.0) 20 (37.7) 152 (47.9)To a large extent 120 (45.5) 32 (60.4) 152 (47.9)
The work load shared equally among us
Not at all 23 (8.7) 6 (11.3) 29 (9.1)To some extent 110 (41.7) 15 (28.3) 125 (39.4)To a large extent 131 (49.6) 32 (60.4) 163 (51.4)
Staff expertise is respected by the team members
Not at all 20 (7.6) 2 (3.8) 22 (6.9)To some extent 135 (51.1) 23 (43.4) 158 (49.8)To a large extent 109 (41.3) 28 (52.8) 137 (43.2)To a large extent 122 (46.2 ) 32 (60.4) 154 (48.6 )
Total 264 (100.0) 53 (100.0)
317 (100.0 )
(Figures in brackets indicate the percentage of nursing staff) N=317
A nursing staff is involved in collaborative relationships, acting as mentor, student,
coach, and support for professional growth of others as per the needs of the patients.
She is ethically informative, is good at decision making and practices values she
and her hospital subscribe to. She communicates, critically thinks and follows
ethical guidelines concerning clinical and professional practices. Only 40 per cent
of the staff nurses and 57 per cent of the sister incharges feel that they are working
together with doctors, class IV staff, and other administrative staff in an organized
manner. However, the degree of cooperativeness depends on the cases, such as
emergency, routine and non routine patient care services. It is to be noted that the
quality of healthcare services could be achieved mostly by the means of team work.
It is reported by 43 per cent of staff nurse, 57 per cent of the sister incharges and 45
per cent across both categories that there is an opportunity to participate in
meetings, discussions and sharing the information with the team regarding the

139
assignment carried out by the team. This statistic reflects that only half of the staff
is comfortable with the existing situation and there is a high scope for improving
participation through team discussions on the matters related to teamwork. Hence
there are greater opportunities for the team members to get an opportunity in
planning and executing work in their field. This shows that there is inadequate
attention focussed on the autonomy of the staff working as a team. This also has
bearing on the team members’ communication with each other. Nearly 46 per cent
of the staff nurse and 60 per cent of the sister incharges feel that they communicate
freely with one another. Regarding the other important aspects like sharing work
load it has been reported that 50 per cent of the staff nurse, 60 per cent of the sister
incharges feel that the work is distributed equally among them. Similarly, 46 per
cent of the sister incharges and 60 per cent of the sister incharges feel that their
expertise is effectively used and is respected. The nurse staff are part of the team
but they do not have adequate opportunities to participate in the team processes.
This can be understood from the Table 2.13. The overall score of the five
dimensions of team work clearly reflects that the team effectiveness marginally
high at 53 per cent.
Table 2.13
Nursing staff opinion on team effectiveness score
Collaborative Relationship for Team
Effectiveness
Present designation
Total Staff Nurse
Sister
incharges
Low (50.0)132 (33.9)18 (47.3)150
High (50.0)132 (66.0)35 (52.6)167
Total (100)264 (100)53 (100)317
(Figures in brackets indicate the Percentage of nursing staff) N=317
On a positive note nearly 66 per cent of the sister incharges say that they have many
opportunities to take decisions, as they are given opportunities at various levels and
on various occasions. Whereas the nursing staff are seen participating in their team
only at the routine team activities like work in the operation theatre, ICU, and other
some areas and not mainly at the administrative level of team management.

140
D. Respectful Relationships
Respectful relationship can be considered to be one of the needs of the staff
members. On a day-to-day basis getting adequate respect from colleagues and
coworkers facilitate effective teamwork in the hospitals. Individuals gain respect
because of their unique individual qualities apart from the job they do. If the job
provides dignity to the nursing staff and makes them feel comfortable then the staff
will really enjoy a high degree of respect. As it is understood that employees should
command respect and not demand respect, it is assumed that the nursing job is
recognised as a significant job and contribute to the process of healthcare delivery;
however, it is lacking in order to achieve appropriate status amongst the
professionals and the beneficiaries. To understand the current status of nursing staff
respectfulness, the nursing staff were asked to report their opinions on the same and
these details are presented in Table 2.14. It is reported that only one fourth of the
staff nurse and nearly 30 per cent of sister incharges feel that they are respected by
the patients and relatives. A majority of the staff, (73 per cent) feel that they do not
get respect from the patients and relatives. The nursing staff get adequate respect
from their superiors (nearly 60 per cent), colleagues and coworkers (nearly 72 per
cent), and medical staff (nearly 63 percent). It is seen that the nursing staff get most
respect from their colleagues and the least respect from patients and relatives.
Further the findings reveal that the nursing staff get a lot more respect from medical
staff then their own superiors (sister incharges, assistant matron and matron).
Comparing the sister incharges with staff nurses, the staff nurses feel that they get
lower status than their senior colleagues. The patient and their relatives treat both
categories at the same level. This is because the patients and relatives most likely do
not know the difference between these two categories, unlike the staff members in
the hospital who understand the job profiles and designations.

141
Table 2.14 Nursing staff opinion on respect they get from their patients and colleagues
Respectable relationship with stakeholders
Grading Staff Nurse Sister incharges
Total
Patient and relatives Not at all (8.3)22 (13.2)7 (9.1)29
To some extent (65.5)173 (56.6)30 (64.0)203
To a large extent (26.1)69 (30.2)16 (26.8)85Class IV and other housekeeping staff
Not at all (8.3)22 (11.3)6 (8.8)28
To some extent (59.81)58 (54.7)29 (59.0)187
To a large extent (31.8)84 (34.0)18 (32.2)102Superiors Not at all (2.3)6 (3.8)2 (2.5)8
To some extent (37.9)100 (30.2)16 (36.6)116
To a large extent (59.8)158 (66.0)35 (60.9)193Colleagues and Coworkers
Not at all (0.4)1 (1.9)1 (0.6)2
To some extent (27.3)72 (30.2)16 (27.8)88
To a large extent (72.3)191 (67.9)36 (71.6)227Medical staff Not at all (1.1)3 (1.9)1 (1.3)4
To some extent (36.4)96 (32.1)17 (35.6)113
To a large extent (62.5)165 (66.0)35 (63.1)200Total (100 )264 (100)53 (100 )317
(Figures in brackets indicate the percentage of nursing staff) N=317
It is culturally/commonly understood that an elderly person always get more respect
than their younger counter- parts. Table 2.15 presents the nursing staff’s opinions
on the status of respect.
Table 2.15
Respect accorded as per age: Nurses’ opinions
Age
Respectful Relationship with Nursing Staff Total
Low High
Below 30 yrs 15 (53.6) 13 (46.4) 28 (100.0)
31-35 yrs 22 (44.0) 28 (56.0) 50 (100.0)
36-40 yrs 26 (41.3) 37 (58.7) 63 (100.0)
41-45 yrs 32 (45.7) 38 (54.3) 70 (100.0)
46-50 yrs 17 (37.8) 28 (62.2) 45 (100.0)
51 & above 28 (45.9) 33 (54.1) 61 (100.0)
Total 140 (44.2) 177 (55.8) 317 (100.0)
(Figures in brackets indicate the percentage of nursing staff N=317

142
It is seen that the age group of 30 to 40 years receives a high degree of respect
while the age group of 51 and above opine that they are accorded less respect than
the age group of 46- 50 years. The conclusion is that those who belong to the older
age group are not happy with the respect they get from the co-workers and other
colleagues. Similarly, it is possible to compare whether nurses with more
experience get respect in a direct proportion or not. The table 2.16 gives
information on this.
Table 2.16
Respect accorded as per experience
Years in Present Hospital
Respectful Relationship with Nursing Staff Total
Low High
Up to 5 yrs 26 (46.4) 30 (53.6) 56 (100.0)
6-10 yrs 15 (42.9) 20 (57.1) 35 (100.0)
11-15 yrs 28 (38.9) 44 (61.1) 72 (100.0)
16-20 yrs 35 (41.7) 49 (58.3) 84 (100.0)
21-25 yrs 17 (45.9) 20 (54.1) 37 (100.0)
26 & above 19 (57.6) 14 (42.4) 33 (100.0)
Total 140 (44.2) 177 (55.8) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
It is further possible to trace the link between experience and the respect accorded
to nurses in hospitals. It is seen that from 0 years of experience to 15 years of
experience 54 per cent to 61 per cent of the staff feel that they are given a lot of
respect which is a positive trend. Whereas those with more than 16 years of
experience, that is the senior level staff, indicated a decline in the level of respect
from the hospital staff and others (58 per cent to 42 per cent). This shows that there
is a lack of cultural indoctrination in the hospitals. Moreover, either the
organisational hierarchy or the chain of command is unclear or is not followed in
the least. In such a case the senior staff seem to be unable to command respect in
the organisation and this would result in a few problems in accomplishing tasks.
There would be no control over the staff on the lower rungs across the organisation.

143
E. Supervision and Management
Nursing staff expect their superiors to engage in a positive relationship and be
caring, competent, and supportive. It is understood that most of the nursing
supervisors have learnt to apply certain skills based on their experience as a nursing
leader. Basically, the nursing supervisors are staff nurses who got a promotion and
became nursing supervisors and they have not gone through any formal training to
improve their leadership qualities.
Table 2.17 Supervisors’ support and encouragement to the nursing staff
The immediate supervisor is really
Grading Staff Nurse Sister incharges
Total
Creating harassment free work environment
Not at all 34 (12.9) 9 (17.0) 43 (13.6)
To some extent 116 (43.9) 20 (37.7) 136 (42.9)
To a large extent 114 (43.2) 24 (45.3) 138 (43.5)
Motivate, and support under critical situations
Not at all 20 (7.6) 6 (11.3) 26 (8.2)
To some extent 109 (41.3) 21 (39.6) 130 (41.0)
To a large extent 135 (51.1) 26 (49.1) 161 (50.8)
Encouraging the innovative work
Not at all 31 (11.7) 3 (5.7) 34 (10.7)
To some extent 115 (43.6) 28 (52.8) 143 (45.1)
To a large extent 118 (44.7) 22 (41.5) 140 (44.2)
Helpful to solve the work and family related problems
Not at all 65 (24.6) 12 (22.6) 77 (24.3)
To some extent 98 (37.1) 20 (37.7) 118 (37.2)
To a large extent 101 (38.3) 21 (39.6) 122 (38.5)
Total 264 (100.0) 53 (100.0) 317 (100.0 )
(Figures in brackets indicate the percentage of nursing staff) N=317
At this stage it becomes necessary to understand that the nursing supervisors are
able to create a better environment for the staff nurses at the workplace and these
supervisors are supportive, helpful and encourage the staff to do good work etc. as
is discussed in Table 2.17.
It is a fact that employees have their own limitations in terms of knowledge,
attitude, and commitment to work. It is the responsibility of the supervisors to
understand the employees individually and as a group and extend their support
according to their subordinates’ requirements. The supervisors are the immediate

144
contact for the staff members to share their work related concerns. The supervisors
should be easily accessible to the staff members, and motivate them in case any
critical situation crops up. Table 2.18 presents certain important variables like
harassment-free work environment, motivating the staff, encouragement for
innovative work and solving their work and family related issues. It is reported that
nearly 43.5 per cent of the staff feel that their immediate supervisors create a
harassment-free work environment to a large extent. Nearly 50.8 per cent of the
staff report that they get motivated and are supported in critical situations to a large
extent. Nearly 45 per cent staff feel that their immediate supervisors encourage their
innovative work to some extent and 44 per cent of the staff state that their
immediate supervisors encourage the innovative work to a large extent. Nearly 38.5
per cent of the staff opine that their immediate supervisors are helpful to solve even
family related problems to a large extent. These are very important issues which
need to be addressed by the nursing supervisors in order to promote a good work
environment with stress-free employees.
Nursing supervisors are considered to be more task oriented. Among the four
variables, only the last variable (supervisor’s support in helping solve family and
work related problems) is considered more sensitive by both the staff nurse and the
sister incharges. The staff nurses feel there is no need to share their family related
issues with their nursing supervisors and at the same time the supervisors feel that
the nursing staff’s family issues are a private aspect and hence there is no need to
focus on these issues. However, family problems have a direct impact on the
nursing staff’s peace of mind which may affect their routine work schedule.
Table 2.18
Nursing staff’s opinion on supervisors’ support
Supervisor Support for the work
achievement
Present designation Total
Staff Nurse Sister incharges
Low (45.5)120 (45.3)24 (45.4)144
High (54.5)144 (54.7)29 (54.6)173
(100)264 100(53) 100(317)
(Figures in brackets indicate the percentage of nursing staff) N=317

145
Overall, it is clearly spelt out in Table 2.18 that both the nursing staff and the sister
incharges (nearly 55 per cent) share the opinion that they get support from their
respective supervisors. However, this alone is not adequate to keep up the morale of
the staff in the work environment.
2. Opportunities to share opinion and suggestions on the work related matters
The nursing staff have various assumptions with regard to their role in decision
making since the nursing staff’s role is to carry out only the doctors’ orders and
their routine functions which has been earmarked for them. However, in a given
situation they would be able to contribute to organisations in various ways. It could
be the responsibility of the management to accommodate such provisions from time
to time through certain means like asking the staff for suggestions on various
aspects such as maintenance of hospital, quality of care, documentation process of
patient care, team work, balancing work life and family responsibilities of the
nursing staff, etc. Table 2.19 presents the five dimensions of opportunities to
participate in the decision making process.
Table 2.19 Opportunities to participate on the decision making process
Opportunities for the staff to give opinion and suggestions on
Grading Staff Nurse Sister incharges
Total
Improving cleanliness, and safety of the hospital
Not at all 62 (23.5) (18.9)10 72 (22.7)To some extent 112 (42.4) (37.7)20 132 (41.6)To a large extent 90 (34.1) 23 (43.4) 113 (35.6)
Improving the quality patient care services
Not at all 67 (25.4) (28.3)15 82 (25.9)To some extent 108 (40.9) (34.0)18 126 (39.7)To a large extent 89 (33.7) 20 (37.7) 109 (34.4)
Improving the documentation, nursing work methods and processes
Not at all 82 (31.1) (32.1)17 99 (31.2)To some extent 86 (32.6) 18 (34.0) 104 (32.8)To a large extent
96 (36.4) 18 (34.0) 114 (36.0)Importance of working as a team
Not at all 83 (31.4) 22 (41.5) 105 (33.1)To some extent 115 (43.6) 19 (35.8) 134 (42.3)To a large extent 66 (25.0) 12 (22.6) 78 (24.6)
Methods (how to balance family and hospital requirement) for improving the work life balance
Not at all 113 (42.8) 26 (49.1) 139 (43.8)To some extent
76 (28.8) 13 (24.5) 89 (28.1)To a large extent
75 (28.4) 14 (26.4) 89 (28.1)Total 264 (100.0) 53 (100.0) 317 (100.0)
(Figures in brackets indicate the percentage of nursing staff) N=317

146
The management (management level just above that of the nursing staff) has to take
employees into confidence for decision making through various activities and
different methods which can help the nursing staff boost their morale. Also the
nursing staff are responsible to execute such jobs on a day-to-day basis or at least
periodically and hence involving them in the decision making process will make
them more accountable. One of the methods is taking their suggestions and opinions
for work related purposes which gives them an opportunity to participate in the
decision making process. Maintaining cleanliness is a very important aspect which
falls directly within the purview of the nursing staff. Nearly 35.6 per cent of the
staff feel that they had opportunities to give their opinion on improving cleanliness
and the safety of the hospital. As far as staff nurses are concerned nearly 34 per cent
of them feel that they have greater opportunities to participate on work related
decision making, particularly improving cleanliness, and 43 per cent of sister
incharges feel that they have greater opportunities to participate in the decision
making process of improving cleanliness.
If the hospital desires to improve the quality of care in the hospital, the most
important group which could contribute is the nursing staff because they are
instrumental in achieving better patient care. The nursing staff’s contribution in this
regard is most appreciated. Nearly 34 per cent of the staff opine that they have been
consulted to improve the quality of patient care services to a large extent. Nearly 34
per cent of the staff nurses and 38 per cent of the sister incharges were of the
opinion that their expertise was valued in this field.
Nearly 36 per cent of the staff nurse and 34 per cent of the sister incharges report
that they were consulted for improving documentation, nursing work methods and
processes to a large extent. Nursing staff are expected to do documentation in the
ward particularly with respect to admission register, discharge register, and
maintenance of case files. The practice of writing such work is done using
traditional, out-dated technologies and there is a lot of scope for improving such
practices. Nearly 25 per cent of the staff nurse and 22 per cent of the sister
incharges and 25 per cent as a group feel that they were consulted by their
supervisors or superiors about the importance of team work in the hospital. This

147
shows that team work is lacking in the hospitals as is reflected by the responses of
the nursing staff. Nearly 28 per cent of the staff nurse and 26 per cent of the sister in
charge testify that they were consulted by the supervisory staff on ways to improve
their work life balance. Work life balance involves various aspects especially
organising the nursing staff work in such a way that it does not affect the nursing
staff’s personal affairs while at the same time seeing to it that their family concerns
do not affect work related matters. It is expected some support from the
management with regard to work life balance of nursing staff however there has
been no effort in this regard.
3. Employees value on management
The employees join the organisations to achieve certain goals and satisfy some
needs within the organisation. To this end the employees expect help, support, etc.
from their organisation. They feel that the management should understand the
employees’ requirements without any pressure from the employee’s and satisfy
these needs. The employees judge the management based on the commitment
shown by the management towards satisfying the employees’ needs and
accordingly develop trust or faith in the organisation. The organisation is expected
to demonstrate fairness in the application of rules and regulations so that the
employees continue to give their best to the organisation. The nursing staff report
on the four dimensions, namely management interest in maintaining the dignity of
the patients, maintaining faith and trust of the employees, open and transparent
communication, and demonstrating that the employees are valued. The details of the
nursing staff responses on these dimensions are presented in Table 2.20

148
Table 2.20 Employees’ opinion on management
Variables Grading Staff Nurse
Sister incharges
Total
Hospital management is concerned with satisfying and up keeping dignity of patients
Not at all 41 (15.5) 5 (9.4) 46 (14.5)
To some extent 144 (54.5) 33 (62.3) 177 (55.8)
To a large extent 79 (29.9) 15 (28.3) 94 (29.7)
I have complete faith and trust on the hospital management’ s ability on justice )equity/ fairness to all
Not at all 81 (30.7) 8 (15.1) 89 (28.1)
To some extent 89 (33.7) 23 (43.4) 112 (35.3)
To a large extent 94 (35.6) 22 (41.5) 116 (36.6)
The hospital management maintains transferant and open communication on sharing information to all
Not at all 62 (23.5) 9 (17.0) 71 (22.4)
To some extent 115 (43.6) 24 (45.3) 39 (43.81)
To a large extent 87 (33.0) 20 (37.7) 107 (33.8)
I could see the hospital makes sure that the employees are valued
Not at all 52 (19.7) 7 (13.2) 59 (18.6)
To some extent 123 (46.6) 27 (50.9) 150 (47.3)
To a large extent 89 (33.7) 19 (35.8) 108 (34.1)
Total 264 (100.0 )
53 (100 ) 317 (100 )
(Figures in brackets indicate the percentage of nursing staff) N=317
The nursing staff give more value to the hospital management when the hospital
management treats its patients with dignity and aims to give them full satisfaction.
The nursing staff are engaged indirect patient care as per the policies of the hospital
management. In this regard, nearly 30 per cent of the nursing staff feel that the
hospital management is concerned with satisfying and maintaining the dignity of
the patients to a large extent. This indicates to the hospital management that there is
still a very large scope to improve the situation. Only 37 per cent of the nursing
staff feel that they have complete faith and trust in the hospital management’s
ability for justice (equity or fairness) accorded to all staff. This demonstrates that
the management needs to improve its record of taking employees into confidence
on issues concerning management affairs. This situation has to be considered
seriously. Nearly 34 per cent of the nursing staff feel that hospitals ensure open and
transparent communication of its affairs and share the information with all
concerned. However, this is not adequate because a large per cent of the staff feel
that the hospitals rarely pay attention to this aspect. Finally, nearly 34 per cent of

149
the staff feel that they feel that the hospital ensures that the employees know that
they are valued to a large extent but the major part of the respondents are not happy
with the management’s practices in this regard. It shows that the hospital
management lacks consideration for its employees who are the cogs in the wheel of
the organisation. Overall, the employee’s opinion about the management is not very
satisfactory. The employees face many problems which can be easily handled by
the hospital without much difficulty but the hospital management prolongs looking
into such problems and do not try solve it at once.
F. Service Quality and Patient Safety
The quality of patient care is the main concern for the patients as well as for the
hospitals. The quality of care depends on various important factors like quality of
resources, organizational processes, and methods of delivery. The nursing staff are
concerned with the quality of patient care and the safety of the patients. Another
key aspect in the hospital is patient safety. Patient safety includes physical safety,
reduction of medical errors, and appropriate safety culture. Table 2.21 provides
information on the three dimensions of quality of patient care and patient safety as
is reported on by the nursing staff.
Table 2.21 Opinion on nursing quality care and patient safety
Opinion on nursing quality care and patient safety
Grading Staff Nurse Sister incharges
Total
Every nurse has the opportunity to perform the types of work at their level best
Strongly disagree 17 (6.4) 2 (3.8) 19 (6.0)Disagree 57 (21.6) 10 (18.9) 67 (21.1)Agree 144 (54.5) 32 (60.4) 176 (55.5)Strongly agree 46 (17.4) 9 (17.0) 55 (17.4)
The overall quality of nursing care provided is high
Strongly disagree 14 (5.3) 3 (5.7) 17 (5.4)Disagree 81 (30.7) 13 (24.5) 94 (29.7)Agree 120 (45.5) 29 (54.7) 149 (47.0)Strongly agree 49 (18.6) 8 (15.1) 57 (18.0)
The hospital has provided enough facilities for protection of patients in the ward
Strongly disagree 38 (14.4) 8 (15.1) 46 (14.5)Disagree 94 (35.6) 15 (28.3) 109 (34.4)Agree 110 (41.7) 21 (39.6) 131 (41.3)Strongly agree 22 (8.3) 9 (17.0) 31 (9.8)
Total 264 (100.0) 53 (100.0)
317 (100.0 )
(Figures in brackets indicate the percentage of nursing staff) N=317

150
Nearly 72.4 per cent (agree 55.5 per cent + strongly agree 17.4 per cent) agree that
every nurse has the opportunity to perform various types of work at their level best.
It is to be noted that the nursing staff do not have many opportunities in terms of
decision making and participation in other important aspects but they do have
multiple opportunities to work in different areas of healthcare like ICU, OT, special
wards etc. which gives them a variety of experience due to the popular practice of
job rotation. Nearly 65per cent (agree 47 per cent + strongly agree 18 per cent)
agree that the overall quality of nursing care is high in the hospital. However, nearly
35 per cent of the nursing staff are unable to agree on the existence of high quality
of care in the hospital due to various reasons which include lack of material
availability, shortage of staff, lack of professional training and development in the
hospital. Only 51 per cent (agree 41 per cent + strongly agree 10 per cent) agree that
the hospital has provided enough facilities for protection of the patients in the
wards. On the other hand, nearly that many (49 per cent) disagree with the notion
that the hospital has provided enough facilities for the protection of the patients in
the wards. There is a lack of patient safety measures in the hospital. Also there is no
strong mechanism for bring patient safety culture in effect in the hospitals. This
reflects the organisation’s beliefs in the traditional practices of patient care delivery
and its inability to cope with the changes in the healthcare delivery models and the
modern patient’s requirements.

151
PART-3 QUALITY OF WORK LIFE INDICATORS
The third Part of the chapter 4 is organized based the analysis and findings and
details are as follows: Part 3 Overview of quality of work life Indicators” and has
seven major sections such as work life balance.
A. Work life Balance
It is commonly understood that nursing is a job that is mostly suitable for women as
it provides them greater opportunities. Due to an increase in educational
achievements by women, decreased family size, stagnant or declining wages for
men or unemployment of spouses, increased cost of maintaining a middle-class life
style, lengthening life span, and liberalization of attitudes concerning women's and
men's proper roles within the family structure an increasing number of women have
taken up nursing as a profession. In contrast, there is negligible agreement about
women's ability to function equally well in the two demanding arenas of work and
family. Men's ability to succeed at the same balancing feat has been taken for
granted because, historically, successful fulfillment of the worker role was
synonymous with successful fulfillment of the husband/father role. In practice, by
focusing heavily on women, work-family research had reflected the assumption that
work-family issues are solely women's issues – an assumption increasingly called
into question. In a given situation, the nursing staff have to handle both the family
and work. It is perceived that there is some difficulty in maintaining the family
without compromising on the work front or vice versa. Table 3.1 presents certain
key dimensions of balancing work and family by focussing on issues such as work
schedule, personal relationships, children’s education and well being, family and
personal engagements, travelling to and from the work place, and enjoying the work
place.

152
Table 3.1
Nursing staff opinion on work and life balancing issues
Nursing staff ability to make balance between
the work and family Grading Staff
Nurse Sister
incharges Total
My work schedule affects my family and personal relationships at home
Not at all 84 (31.8) 10 (18.9) 94 (29.7)
To some extent 25 (47.31) 28 (52.8) 53 (48.31)
To a large extent 55 (20.8) 15 (28.3) 70 (22.1)
My working life has greater impact on my children’s education, paying attention and their well being
Not at all 95 (36.0) 14 (26.4) 109 (34.4)
To some extent 109 (41.3) 26 (49.1) 135 (42.6)
To a large extent 60 (22.7) 13 (24.5) 73 (23.0)
I have enough time for my family, friends and other personal engagements
Not at all 47 (17.8) 15 (28.3) 62 (19.6)
To some extent 134 (50.8) 26 (49.1) 160 (50.5)
To a large extent 83 (31.4) 12 (22.6) 95 (30.0)
Journey between the workplace and home is hectic
Not at all 87 (33.0) 20 (37.7) 107 (33.8)
To some extent 103 (39.0) 23 (43.4) 126 (39.7)
To a large extent 74 (28.0) 10 (18.9) 84 (26.5)
Balancing between the work and family becomes difficult now
Not at all 75 (28.4) 12 (22.6) 87 (27.4)
To some extent 128 (48.5) 30 (56.6) 158 (49.8)
To a large extent 61 (23.1) 11 (20.8) 72 (22.7)
I am really enjoying the current work
Not at all 19 (7.2) 2 (3.8) 21 (6.6)
To some extent 126 (47.7) 22 (41.5) 148 (46.7)
To a large extent 119 (45.1) 29 (54.7) 148 (46.7)
Total 264 (100 ) 53 (100) (100)317(Figures in brackets indicate the percentage of nursing staff) N=317
Personal relationships form the basic foundation of a family. As an important
member of the family, the nursing staff member has to maintain strong relationships
with her spouse, children and the elders at home. As indicated in Table 3.1 nearly
70 per cent (some extent 48 per cent and large extent 22 per cent) of the nursing
staff have reported that the current work schedule of the hospital affects their
personal relationships. Since nursing involves a shift system and a hectic work load
which exhausts most of their time and energy.

153
Table 3.1 depicts that nearly 23 per cent of the nursing staff feel that their working
life has a greater impact on their children’s education and their well being than on
the other family members. It is to be noted that the respondents being ladies have
dynamically involved in family relationships and take more responsibility for their
children, especially the younger ones. On the other hand, nearly 34 per cent of the
staff report that their work life does not come in the way of managing their
children’s education. However, 66 per cent (not at all 43 per cent and to some
extent 23 per cent) of the nursing staff indicated that their working life had affected
their children education, and their well being. It means they are unable to pay
attention to their children’ education and their well being. Among the respondents,
the married women face more challenges than the unmarried women. The various
issues associated with married women are social issues, family issues and work
related matters. It is expected that the nursing staff have the ability to handle both
areas, that is work and home and maintain the balance between these two. It should
be noted that among the married women 34 per cent have indicated that the working
life has a greater impact on their children’s education and their well being which
has been presented in table3.2.
Table3.2
The working life impact on the married nursing staff
Current marital status:
My working life has greater impact on my children's education, paying attention and their
well being Total
Not at all To a some
extent To the large
extent
Unmarried 19 (100) 0 (0) 0 (0) 19 (100)
Married 100 (34.2) 126 (43.2) 66 (22.6) 292 (100)
Widowed 1 (20.0) 3 (60.0) 1 (20.0) 5 (100)
Divorced 1 (100) 0 (0) 0 (0) 1 (100)
Total 121 (38.2) 129 (40.7) 67 (21.1) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317, X2 =35.2, P=0.000
As is seen in Table 3.1, nearly 30 per cent of the nursing staff feel that they have
enough time for family, friends and other personal engagements. Nearly 70 per cent
(some extent 50 per cent and not at all 20 per cent) have indicated that there is no

154
scope for them to socialise. Socialisation is an important need of the nursing staff.
Most of nursing staff hail from Maharashtra while some of the staff are from
different states. Since a majority of the nurses have family ties in local areas they
are keen to attend family functions, festivals, personal engagements and so on. On
the other hand, the other staff nurses need to visit their home towns. Since a
considerable number of respondents indicated that they are unable to have adequate
time for the said purposes it is clear that organisational polices, hospital
management practices and other institutional difficulties like staff shortages are
major issues that need to be focussed upon.
It is seen in Table 3.1 nearly 66 per cent (some extent 40 percent plus large extent
26 percent) of the nursing staff feel that the journey between their workplace and
home is hectic to a large extent. Even though the nursing staff travel on a daily basis
to their workplace there are times when travel becomes very irritating due to
overcrowding in trains and buses, insufficient travel facilities and different shift
timings. This causes unnecessary tension may reflect in reduced effectiveness of the
staff at work and home.
As per table 3.1 nearly 73 per cent (some extent 40 percent plus large extent 23
percent) of the nursing staff feel that balancing work and family has become
difficult in modern times. However, 27 per cent of the staff feel that balancing
between the work and family is not at all difficult these days. Individuals work to
make life is comfortable but when work life becomes difficult it leads to adverse
consequences for the nursing staff’s health, managing the family and patient care.
Table 3.1 indicates that nearly 47 per cent of the staff feel that they are really
enjoying their current work to a large extent. Even though many factors have been
associated with balancing work with family, among all these factors work
enjoyment is considered a very important factor. This aspect is to some extent in
line with the motivational potential score. Work enjoyment is the major indicator
for work life balance. The analysis of the responses leads to the conclusion that only
47 per cent of the nursing staff have are able to balance their work life with their
family life.

155
Nursing staff preference and commitment to the work
The nursing staff were asked to list their preference if the situation demands them
to be present at the workplace while their presence is also required elsewhere such
as attending an important family function or an emergency at the hospital. The
nursing staff’s responses have been presented in Table 3.3.
Table 3.3
Nursing staff’s preferences and commitment to their work The nursing staff required to attend important family function or emergency at the hospital –what would be their preferences.
Present designation
Total Staff Nurse Sister incharges
Not sure 86 (32.6) 19 (35.8) 105 (33.1)Preference to work 125 (47.3) 27 (50.9) 152 (47.9)Preference to family 53 (20.1) 7 (13.2) 60 (18.9)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
As shown in Table 3.3 nearly 48 per cent of the staff give preference to work when
the situation demands that they are required to be at the work place as well
elsewhere such as their home. Nursing staff are attached to their work. It shows
that they are very committed to their work. It is to be noted that when the nursing
staff carry out their work whole heartedly on most occasions. Since the nursing staff
are highly dedicated to their profession, they naturally give more preference to their
work. However, nearly 33 per cent of the staff are unable decide on this matter
which clearly indicates that there are variations among the nurses and reflects the
changing attitudes towards the nursing profession. In these cases there is a kind of
mixed opinion among the nurses about commitment to their work.
B. Absenteeism
Absenteeism is one of the major issues in the hospital. Staff members being absent
from work causes various problems to the hospital which include work pressure for
existing staff, creating temporary shortage of the workforce, patients getting
affected to a large extent at the same time certain specific jobs handled by select
individuals that cannot be accomplished until the person responsible returns to

156
work. In the study hospitals absenteeism is one of the issues that are a primary
concern. The nursing administrators face many difficulties managing the nursing
staff’s absenteeism that is presented in Table 3.4. This table indicates the number of
days that staff members were absent in the course of last one year.
Table 3.4
Number of days nursing staff have remain absent for the work during the year
Absenteeism number of days recoded
Present designation Total
Staff Nurse Sister incharges
No absenteeism 17 (6.4) 2 (3.8) 19 (6.0)1-20 days 138 (52.3) 26 (49.1) 164 (51.7)21-40 days 95 (36.0) 22 (41.5) 117 (36.9)41-60 days 10 (3.8) 2 (3.8) 12 (3.8)61 & above days 4 (1.5) 1 (1.9) 5 (1.6)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
It is important to note that almost 94 per cent of the staff absented themselves from
work on one or the other occasion during the year and only 6 per cent had never
been absent during the year. Nearly 51 per cent of staff remained absent for 1-20
days in a year and 37 per cent for 21-40 days in a year. The mean number of days
for absenteeism is 22 days in a year and the standard deviation is 12.9. It means 94
per cent of the staff are not available 22 days in a year. The hospital has a policy
whereby the nursing staff can take leave 11 days earned leave at a time and for a
maximum of three times a year. This condition forces the nursing staff to restrict
their vacation to a short duration. Furthermore, the nurses face many problems is
getting their leave sanctioned the second or third time in the same year unless they
have strong justifications for their request. On the other hand, the hospital already
faces an acute shortage of the nursing workforce, hence it is impossible to sanction
more days off work for the nursing staff. Even some of the staff mentioned that the
in being permitted to ustilise their casual leave is due to the shortage of staff. This
shows that the hospital management tries to manage the situation by using the
existing workforces by compromising the leave benefits of the staff.

157
Some of the major reasons stated by the nursing staff for taking leave as mentioned
by the staff are family and personal reasons, heath related reasons, attending
functions, etc. These details are presented in Table 3.5.
Table 3.5 Reasons for nursing staff absenteeism
What were the reasons for such absenteeism? Present designation
Total Staff Nurse
Sister incharges
Personal and family reasons (54.3)134 (52.9)27 (54.0)161
Health related problems of self and family members (19.8)49 (11.8)6 (18.5)55
Social reasons like attending functions, festivals and others (6.5)16 (9.8)5 (7.0)21
Work related tension, tardiness, work stress and others (3.6)9 (2.0)1 (3.4)10
Don't feel like to attend the work due to lack of support (3.6)9 (9.8)5 (4.7)14
Leave travel concession (8.1)20 (11.8)6 (8.7)26
Children’s education (4.0)10 (2.0)1 (3.7)11
Total (100)247 (100)51 (100)298(Figures in brackets indicate the percentage of nursing staff) N=298
One of the major reasons for absenteeism among the respondents is personal and
family reasons. Nearly 54 per cent of the staff were absent for duty for personal and
family reasons. Nearly 18.5 per cent have reported that health issues concerning
themselves and their family members. There is a noticeable difference between the
staff nurses and the sister incharges concerning health related issues as reasons for
absenteeism. The sister incharges resorted to this reason only 12 per cent of the time
whereas the staff nurses used up this reason 20 per cent of the time. The reason for
this variation could be that the staff nurse generally have more responsibilities in
terms of taking care of their own and their family members’ health. Nearly 7 per
cent of the staff had taken leave for social reasons like attending functions, festivals
and others. In this case the nursing staff have already reported that there is little
scope for getting time off for the same. Nearly 9 per cent of the staff used their
leave to travel during their vacation. . Other than these reasons the nursing staff also
remained absent for like work related tension, tardiness, work stress , not wanting to
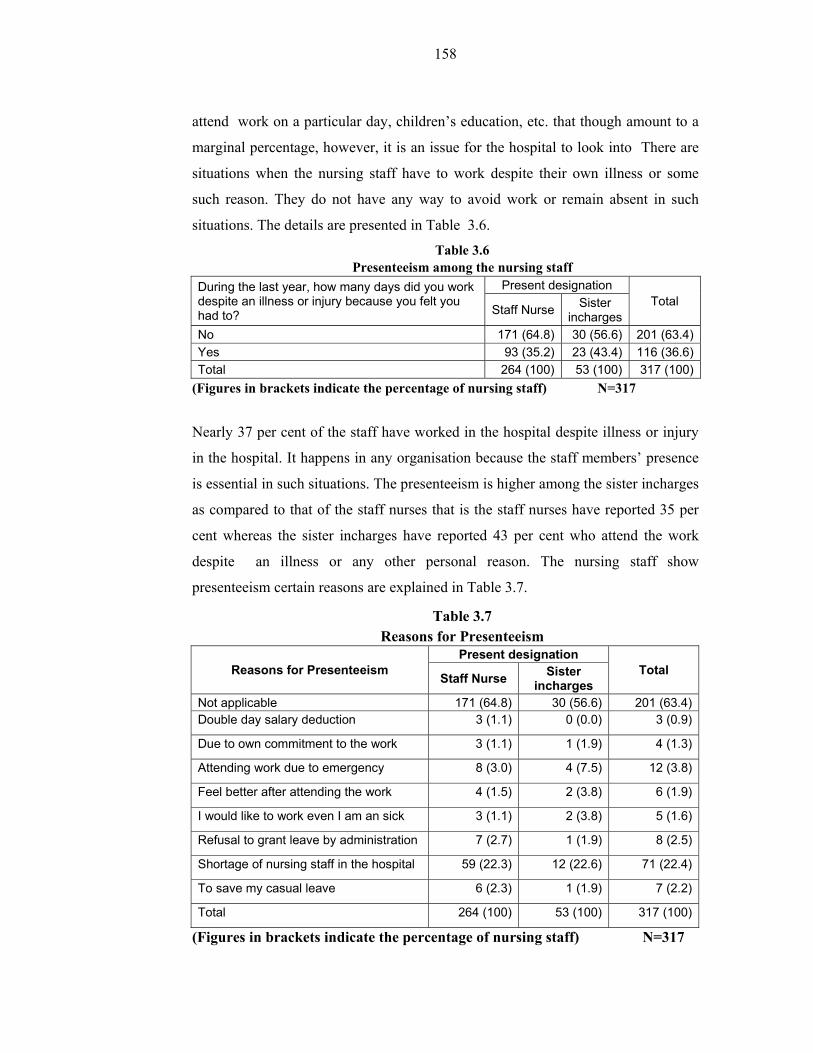
158
attend work on a particular day, children’s education, etc. that though amount to a
marginal percentage, however, it is an issue for the hospital to look into There are
situations when the nursing staff have to work despite their own illness or some
such reason. They do not have any way to avoid work or remain absent in such
situations. The details are presented in Table 3.6.
Table 3.6 Presenteeism among the nursing staff
During the last year, how many days did you work despite an illness or injury because you felt you had to?
Present designation Total
Staff Nurse Sister incharges
No 171 (64.8) 30 (56.6) 201 (63.4)Yes 93 (35.2) 23 (43.4) 116 (36.6)Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317
Nearly 37 per cent of the staff have worked in the hospital despite illness or injury
in the hospital. It happens in any organisation because the staff members’ presence
is essential in such situations. The presenteeism is higher among the sister incharges
as compared to that of the staff nurses that is the staff nurses have reported 35 per
cent whereas the sister incharges have reported 43 per cent who attend the work
despite an illness or any other personal reason. The nursing staff show
presenteeism certain reasons are explained in Table 3.7.
Table 3.7 Reasons for Presenteeism
Reasons for Presenteeism Present designation
Total Staff Nurse Sister incharges
Not applicable 171 (64.8) 30 (56.6) 201 (63.4)Double day salary deduction 3 (1.1) 0 (0.0) 3 (0.9)
Due to own commitment to the work 3 (1.1) 1 (1.9) 4 (1.3)
Attending work due to emergency 8 (3.0) 4 (7.5) 12 (3.8)
Feel better after attending the work 4 (1.5) 2 (3.8) 6 (1.9)
I would like to work even I am an sick 3 (1.1) 2 (3.8) 5 (1.6)
Refusal to grant leave by administration 7 (2.7) 1 (1.9) 8 (2.5)
Shortage of nursing staff in the hospital 59 (22.3) 12 (22.6) 71 (22.4)
To save my casual leave 6 (2.3) 1 (1.9) 7 (2.2)
Total 264 (100) 53 (100) 317 (100)
(Figures in brackets indicate the percentage of nursing staff) N=317

159
With reference to Table 3.7 the staff members have worked in the hospital in spite
of their illness or injury for a number of reasons like the administration may deduct
their salary, to avoid absenteeism, because there is a huge shortage of staff, the
authorities have refused to sanction leave, there is compulsory duty and fear of
deduction of double-day salary, in response to a disaster, due to their work
commitment, for emergency work, feeling better when on duty, feeling responsible
to the department, interested in work responsibility, already used up all the leaves,
interested in patient care, since the staff stay in quarters nursing administration calls
them to replace the absentee, to save their own casual leaves.
C. Work Stress
Nursing staff have the possibility of getting into stressful situations in the hospital.
The sources of stress may be moral factors when people are prevented from doing
‘good’ they may feel that they have not done what they ought to have or that they
have erred, thus giving rise to a troubled conscience. The nursing staff usually play
two roles, as professionals and as moral actors. In a situation the nursing staff’s
inability to function according to their conscience is associated with several
phenomena: a decreased well-being in nurses, shortages of nurses, burnout, and
distancing from patients. These negative consequences of a troubled conscience
make it imperative to understand more about situations that evoke it, in order to
help guide the personnel on how to relate to professional values and rules and their
personal conscience. There are various factors associated with nursing work stress
are external influences as well internal factors which are discussed in Table 3.8. The
nursing staff’s work stress consists of 11 dimensions as stated below.

160
Table 3.8 Factors contribute nursing staff work stress
Were you stressed by the following aspects
Yes/No Staff Nurse Sister incharges
Total
Forced to provide care that you feel wrong
No 71 (26.9) 17 (32.1) 88 (27.8)
Yes 193 (73.1) 36 (67.9) 229 (72.2)
Wrong medication by yourself No 96 (36.4) 28 (52.8) 124 (39.1)
Yes 168 (63.6) 25 (47.2) 193 (60.9)
Sometimes disagree with the care/medicines prescribed by a doctor
No 79 (29.9) 22 (41.5) 101 (31.9)
Yes 185 (70.1) 31 (58.5) 216 (68.1)
Seeing patients being insulted by others
No 45 (17.0) 11 (20.8) 56 (17.7)
Yes 219 (83.0) 42 (79.2) 261 (82.3)
Seeing patients being injured/falls/bedsore
No 59 (22.3) 16 (30.2) 75 (23.7)
Yes 205 (77.7) 37 (69.8) 242 (76.3)
Find yourself avoiding patients or family members who need help or support due to your work pressure
No 145 (54.9) 27 (50.9) 172 (54.3)
Yes 119 (45.1) 26 (49.1) 145 (45.7)
My family issues take more energy than the official work however I would like to devote myself to the work
No 158 (59.8) 29 (54.7) 187 (59.0)
Yes 106 (40.2) 24 (45.3) 130 (41.0)
I feel that I am unable to live up to others’ expectations of my work
No 134 (50.8) 34 (64.2) 18 (53.0)
Yes 130 (49.2) 19 (35.8) 19 (47.0)
The situations makes me lower my aspirations to provide good care
No 128 (48.5) 32 (60.4) 160 (50.5)
Yes 136 (51.5) 21 (39.6) 157 (49.5)
When I am badly treated No 70 (26.5) 16 (30.2) 86 (27.1)
Yes 194 (73.5) 37 (69.8) 231 (72.9)
My workload makes me to feel sick No 98 (37.1) 21 (39.6) 119 (37.5)
Yes 166 (62.9) 32 (60.4) 198 (62.5)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the percentage of nursing staff) N=317
Table 3.8 indicates that nearly 72 per cent of the staff feel that they are disturbed or
stressed when they are forced to provide care that they instinctively or through
experience feel is wrong. It is the situation in which the nursing staff have to
manage the patients which adds to the pressures on the nursing staff in the
workplace. If the pressure exceeds the nursing staff’s ability to handle them, the
staff member’s frustration levels increase to an extent that it affects their
professionalism. Nearly 60.9 per cent of the staff feel that they get stressed when

161
they give wrong medication to the patients. Giving wrong medicine usually does
not happen, however, there are many other factors that need the attention of the
nursing staff which does create a window for error in treating the patients. This
results in burnout for the nursing staff. Nearly 68 per cent of the staff feel that they
get stressed when they disagree with the care or medicines prescribed by the doctor.
Even though providing prescriptions are not the concern of the nursing staff but the
staff get become involved on moral grounds because the nursing staff play a vital
role in patient care management. Such situations may disturb the nursing ability to
function effectively.
Table 3.8 shows that nearly 82 per cent of the nursing staff feel that they get
stressed when they see their patient being insulted by anyone in the hospital. This
indicates that the nursing staff have a high degree of accountability and feel concern
for their patients. This create moral issues and dilemmas in the nursing staff’s
minds. Nearly 76 per cent of the staff feel stressed when they see the patient get
injured or fall from the beds or get bedsores. As a professional they would like to
provide better patient care to avoid such incidences. If the situation is such that they
are unable to provide the very best care the staff become stressed. This is a
professional issue that needs to be tackled.
Table 3.8 indicates that nearly 46 per cent of the staff are disturbed when they find
themselves avoiding patients or family members who need help or support due to
their work pressure. Since the nursing staff play multiple role as professionals, they
experience task pressure (number of task to be performed at a time) and being an
active member of their own family they experience time pressures which make
them compromise when providing service to the patients or taking care of the
family members which affects the nursing staff.
Table 3.8 indicates that nearly 41 per cent of staff feel that they are stressed out due
to their family issues and that these problems tax their energy more than the official
work, however, they would like to devote themselves to their work. More
specifically, if the nursing staff give more time to their family, they feel guilty. This
leads to ethical or moral dilemmas which affect the nursing staff’s routines. Nearly

162
50 per cent of the staff feel that they are suffer stress when they are unable to live
up to others’ expectations in their work front. People usually hope for a positive
opinion from others. If the nursing staff is unable to satisfy their patients’
expectations they feel dissatisfied with themselves on moral and ethical grounds.
Nearly 73 per cent of the nursing staff feel that they get stressed when they are
badly treated. Nursing is considered to be a noble profession and hence people
providing such services should be treated well by patients as well as the
management. If there is a situation when they are not given importance they feel
bad. Nearly 62.5 per cent of the staff feel that their work load makes them feel sick
which in turn adds to their stress. Work load is one of the major contributors to the
nursing staff’s stress. The nursing staff’s workload is the most frequently reported
stressor. Work overload in combination with inadequate resources (such as lack of
time and inadequate staffing) seems to be the greatest source of stress in health care.
A heavy workload typically entails not being able to perform duties to the nurse’s
own satisfaction.
When nurses are unable to fulfill the moral goals of nursing namely, to protect
patients from harm and to provide good care they experience moral distress.
Impediments to fulfilling these moral goals may be shortage of staff, inadequately
trained staff, or organizational constraints. Inability to act according to one’s values
leads to moral distress.
D. Communication
“Nurses must be as proficient in communication skills as they are in clinical skills.”
Clinical knowledge, skills, and judgment are not enough to achieve excellent
outcomes. Nurses must demonstrate the ability to be communicators in all aspects
of their professional work in order to achieve safe care and quality outcomes. The
nursing staff should have good communication skills be able to focus on finding
solutions, achieve desirable outcomes, seek to protect and advance collaborative
relationships among colleagues; invite and hear all relevant perspectives; develop
goodwill and mutual respect to build consensus and arrive at a common
understanding; demonstrate congruence between words and actions, and hold others
accountable for doing the same. Further, the nursing staff should have access to

163
understand and use communication technologies, be able to communicate clearly
about clinical, financial, and work environment outcomes and showcase high
performance on the professional front. To understand the nursing staff’s
communication status in the hospital there are eight dimensions that are used. The
details are explained in Table 3.9.
Table 3.9
Nursing staff communication
Variables Yes/No Staff Nurse Sister incharges Total
I could openly communicate on the mistakes which I committed
No 42 (15.9) 3 (5.7) 45 (14.2)
Yes 222 (84.1) 50 (94.3) 272 (85.8)
My superiors encouraged me to report the near- miss faults
No 104 (39.4) 13 (24.5) 117 (36.9)
Yes 160 (60.6) 40 (75.5) 200 (63.1)
My superiors use abusive language
No 192 (72.7) 43 (81.1) 235 (74.1)
Yes 72 (27.3) 10 (18.9) 82 (25.9)
My superiors never let me down in front of others.
No 184 (69.7) 40 (75.5) 224 (70.7)
Yes 80 (30.3) 13 (24.5) 93 (29.3)
The majority of my normal, daily activities on the job are guided by the written operating instructions
No 232 (87.9) 49 (92.5) 281 (88.6)
Yes 32 (12.1) 4 (7.5) 36 (11.4)
I get communication about latest technologies which are part of my routine work
No 210 (79.5) 42 (79.2) 252 (79.5)
Yes 54 (20.5) 11 (20.8) 65 (20.5)
I have difficulty in communicating with different patients who speak and understand different languages (language barrier)
No 64 (24.2) 13 (24.5) 77 (24.3)
Yes 200 (75.8) 40 (75.5) 240 (75.7)
Lack of availability of information in time
No 143 (54.2) 33 (62.3) 176 (55.5)
Yes 121 (45.8) 20 (37.7) 141 (44.5)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the percentage of nursing staff) N=317
There are some important dimensions of communications are discussed as follows;
the nursing staff have scope for making mistakes which may arise due to difficulty
in following directions, demonstrating poor clinical judgment, or inadequate
assessment of patients. Table 3.9 depicts that nearly 85 per cent of the nursing staff
reported that they could openly communicate about their mistakes they commit
during the work. Similarly, nearly 63 per cent of the staff feel that their superiors
encouraged them to report the near-miss mistakes or faults. This shows that the
superiors are open minded and accept the nursing staff’s mistakes and hence there is

164
scope for the nursing staff to get feedback from their superiors and improve their
clinical skills. Further, it strengthens the nursing staff’s ability to effectively triage
patients or set priority when caring for patients, identifying the critical symptoms or
test results, attempting to manage difficult situations with appropriate skill level or
competency.
Nearly 30 per cent of the staff feel that their superiors use abusive language. When
there is foul language used by the superiors when addressing their staff by and they
are condescending, rude, abrupt, insulting, aggressive and angry. Dismissive
behaviour such as telling others to shut up or not caring for what others think,
dismissive remarks about another’s role in the team, educational qualifications, or
lack of experience all have negative consequences on the nursing spirit; however,
nearly 70 per cent of the staff reported that their superior have never used abusive
language. This shows that there are a few exceptions among the superiors while the
majority is good in communicating with the staff. This can help the nursing staff
continue to maintain their spirit and motivation.
Nearly 29 per cent of the nursing staff reported that their superiors have let them
down in front of others. This shows that there is a lack of support that the nursing
staff receive from their superiors which include: unhelpful behaviours, refusing to
answer a question or providing needed patient information, impatience and making
it difficult for others to ask for assistance, complaining when asked to help or
refusal to assist others, or unhelpful critique of others. However, nearly 71 per cent
of the staff feel that their superiors never let them down in front of others in any
kind of situation. It shows that the majority of superior nursing staff have learnt the
art of communicating properly and uplifting the nursing staff’s spirits. This is also a
very important indicator that there is considerably good nursing leadership that
exists in the hospital.
The nursing staff should be guided with certain standard operating protocols so that
the staff can work without any difficulty. In the absence of superior staff or guides
the staff can function without any difficulty with the help of written rules. Nearly
86.4per cent of the staff reported that that their normal, daily activities on the job

165
are not guided by written operating instructions in the hospital. However, 20.5 per
cent feel there are some written rules which are available to guide them. This shows
that the staff members need regulations to be formally communicated to them to
prevent practice of any kind of regress procedure. It may lead to patients being
harmed. In the absence of standard procedure there is no way to understand a failure
and take the corrective steps. Even at this stage there is no verification or
confirmation by the superiors on the work carried out by the staff nurses.
Nearly 78 per cent of the staff feel that they are not informed about the latest
technologies which could impact their routine work. This shows that the nursing
staff do not have updates which would then result in incompetence. As a result, the
nursing work might include questionable interventions, inability to deliver a
standard of care, lack of critical thinking skills, or lack of knowledge and skills
required by one's position.. The senior doctors believe that the nursing staff should
only carry out the work which they have been told to do and therefore there is no
scope for the nursing staff to use their own ideas or the knowledge they possess.
Nearly 76 per cent of the staff feel that they have no difficulty in communicating to
different patients who speak and understand different languages (language barrier).
This shows that the nursing staff have knowledge of the various languages used in
Mumbai. Language barrier is an extremely important aspect for any individual. If a
person cannot speak well in a particular language when a majority are using, it
would be very difficult for the persons to deal with patients. However, 24 per cent
of the staff feel that they do have language difficulties when the patient speaks
something other than the locally used languages. At present the hospital
administration follows the rule that every nursing staff should be able to speak,
read, write as well clear a exam conducted by the Corporation. If any staff member
fails to pass that examination they will be penalised by having their increment
stopped. This provision is followed in the hospitals to ensure that the nursing staff
are helpful to the patients particularly as effective communicators because
communication plays a vital role in the patient care process.

166
Nearly 55.5 per cent of the staff feel that there is a lack of availability of
information and this results in a time lag for taking some decision or doing some
work. This shows that the nursing staff needs to wait for information for various
purposes including admission, medication, treatment procedures, discharge, and
other administrative issues. This also affects the teamwork of nursing staff, as non-
cooperative nurses may hinder the communication flow, not valuing or
acknowledging the contributions of others, unhealthy competition with others, not
being dependable, or looking good at other's expense. Timely information is
extremely important for proper patient care in the hospitals and the administration
should facilitate its smooth flow
E. Job Satisfaction
Job satisfaction is another important issue for professionals. Job satisfaction has a
number of facets such as satisfaction with: work, pay, supervision, quality of work
life, participation opportunities, organisational commitment, and organisational
climate. There are a number of factors associated with the measurement of job
satisfaction of the nursing staff, however, only a few dimensions have been used to
understand the job satisfaction of nursing staff in the study hospitals. The
dimensions are: satisfaction with the present job, employer value on the nursing
work, overall satisfaction of choice of nursing as a career and encouraging others to
become a nurse. The details are presented in Table 3.10.
37 per cent of the nursing staff have reported that the present job gives them
complete satisfaction. It is over one third of the respondents. However, 44 per cent
of the staff report that they are satisfied with the current job to some extent only.
Rather a large percentage (19 percent) report complete dissatisfaction. Hence it can
be said 44 percent plus 19 percents (63 percent) are some extent or totally
dissatisfied. This response does not give complete satisfaction and hence a large per
cent of the staff are not satisfied with their current position. Nearly 32 per cent of
the staff feel that their employer places a high value on the work they do. The other
49 per cent indicate that this is true to some extent. These responses indicate that
nurses do not find a strong value accorded to them.

167
Table 3.10 Nursing staff job satisfaction
Variables Grading Staff Nurse
Sister incharges
Total
The present job gives me complete satisfaction
To a large extent 96 (36.4) 22 (41.5) 118 (37.2)
To some extent 123 (46.6) 16 (30.2) 139 (43.8)
Not at all 45 (17.0) 15 (28.3) 60 (18.9)
My employer places a high value on the work I do
To a large extent 82 (31.1) 19 (35.8) 101 (31.9)
To some extent 140 (53.0) 16 (30.2) 156 (49.2)
Not at all 42 (15.9) 18 (34.0) 60 (18.9)
Overall, I am satisfied with my choice of nursing as a career
To a large extent 127 (48.1) 24 (45.3) 151 (47.6)
To some extent 75 (28.4) 11 (20.8) 86 (27.1)
Not at all 62 (23.5) 18 (34.0) 80 (25.2)
I would encourage others to become a nurse
To a large extent 133 (50.4) 32 (60.4) 165 (52.1)
To some extent 41 (15.5) 6 (11.3) 47 (14.8)
Not at all 90 (34.1) 15 (28.3) 105 (33.1)
Total 264 (100.0) 53 (100.0) 317 (100.0 )
(Figures in brackets indicate the percentage of nursing staff) N=317
The majority of the nursing staff feel that their employers do not give much
importance to the work they do. Nearly 48 per cent of the staff feel that overall they
are satisfied with their choice of nursing as a career. On the other hand, a
considerable number of the staff (25 per cent) regret that their choice of nursing as a
career. There are a number of reasons for such a response. The nursing staff
compare the modern nursing profession with the practices of the olden days. In
earlier days (15-20 years ago) the nursing job was respected by the patients, the
nursing staff were fully committed to the job, material supply was adequate, etc.
But these days the situation is very different which is not favourable. Only 52 per
cent of the nursing staff have reported that they would recommend others to become
a nurse as well. More than one third do not recommend it at all. This shows that the
existing nursing staff particularly the respondents are not in favour of youngsters to
choose nursing as a profession. The nursing staff indicate that the reasons for the

168
same are that the nursing job is plagued by a number of problems like continuous
duty, night shifts, lack of facilities, lack of management support, etc.
F. Organisational Culture and Climate
Culture is a set of norms and expectations that guide the organisation as a whole.
The organisational culture and climate should be favourable to the nursing staff for
effective functioning and patient care delivery. The organisational culture and
climate consists of various elements which are qualitative in nature. Of course, the
development and maintenance of the hospital’s organisational culture is the
responsibility of the various stakeholders of the organisations which include
doctors, nurses, management and patients, however, the key responsibility belongs
to the management. To understand the organisational culture of study hospitals
there are six dimensions used as presented in Table 3.11.
Nearly 33 per cent (strongly disagree 6.3 per cent and disagree 26.8 per cent) of the
staff disagree that the hospital extends complete support to the employees. It is
exactly one third of the respondents to say that the hospital does not support various
activities they perform, and provide physical and emotional support to the
employees. In the absence of proper support from the management the employees
find it more difficult to bring about changes or introduce standards, or initiate any
progressive activity.
Nearly 23 per cent (strongly disagree 3.8 per cent and disagree 19.2 per cent) of the
staff disagree with the notion that the hospital ensures that the staff is competent in
work processes and management of work. This shows that the hospitals are limited
in their approach towards developing the staff’s competency. There are no regular
programmes to monitor and evaluate the nurses’ performances, and provide
feedback to the employees, and there is an absence of regular training programmes
to train them. Learning organisations try to ensure that the employees constantly
learn and understand the various processes. Also the management should make sure
that the staff members are involved in developing the work processes and simplify
it for better management of patient care.

169
Table 3.11
Organisational culture
Variables Grading
Present designation
Total Staff Nurse Sister
incharges
The hospital extend the complete support to the employees
Strongly disagree 16 (6.1) 4 (7.5) 20 (6.3)
Disagree 72 (27.3) 13 (24.5) 85 (26.8)
Agree 53 (58.01) 30 (56.6) 183 (57.7)
Strongly agree 23 (8.7) 6 (11.3) 29 (9.1)
Hospital ensures that the staff competency in work process and management of work
Strongly disagree 12 (4.5) 0 (0.0) 12 (3.8)
Disagree 49 (18.6) 12 (22.6) 61 (19.2)
Agree 67 (63.31) 33 (62.3) 100 (63.1)
Strongly agree 36 (13.6) 8 (15.1) 44 (13.9)
We always work together in serve the patient
Strongly disagree 6 (2.3) 1 (1.9) 7 (2.2)
Disagree 7 (6.41) 3 (5.7) 20 (6.3)
Agree 155 (58.7) 26 (49.1) 181 (57.1)
Strongly agree 86 (32.6) 23 (43.4) 109 (34.4)
My hospital leadership is role model for other hospital in the same sector
Strongly disagree 40 (15.2) 5 (9.4) 45 (14.2)
Disagree 104 (39.4) 16 (30.2) 120 (37.9)
Agree 88 (33.3) 23 (43.4) 111 (35.0)
Strongly agree 32 (12.1) 9 (17.0) 41 (12.9)
The hospital provides effective communication to all concern and creates better interpersonal relations among the staff.
Strongly disagree 22 (8.3) 1 (1.9) 23 (7.3)
Disagree 71 (26.9) 13 (24.5) 84 (26.5)
Agree 133 (50.4) 29 (54.7) 162 (51.1)
Strongly agree 38 (14.4) 10 (18.9) 48 (15.1)
The hospital never break the rules and ethics which have laid down
Strongly disagree 22 (8.3) 3 (5.7) 25 (7.9)
Disagree 75 (28.4) 20 (37.7) 95 (30.0)
Agree 129 (48.9) 21 (39.6) 150 (47.3)
Strongly agree 38 (14.4) 9 (17.0) 47 (14.8)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the per cent of nursing staff) N=317
Nearly 91 per cent of the staff agreed that they work together to achieve patient
care. It shows that the nursing staff are unanimous in their feelings on working
together to achieve patient care. This is a good indicator. It could be noted that there
is a high scope for team work in the organisation. This culture has to be encouraged
and strengthened and used for better patient care.

170
Nearly 52 per cent (strongly disagree 14.2 per cent and disagree 37.9 per cent) of
the nursing staff disagree that their hospital leadership is the role model for other
hospitals in the same sector. It shows that the nursing staff expect some active role
and participation from the leadership to provide guidance, problem solving,
resource availability, professional development etc. Also the present organisational
climate and culture is not favorable. The role model emphasises various qualities
which are expected from the leadership of the hospital because the staff members
expect a good role model to follow for developing themselves.
Nearly 34 per cent (strongly disagree 7.3 per cent and disagree 26.5 per cent) of the
staff disagreed that the hospitals provide effective communication to all concerned
and create better interpersonal relationships among the staff. Effective
communication and interpersonal relations across the staff and between the staff
and patients is very important. These are the activities that usually the management
has to constantly focus on to maintain and develop the organisation. In the absence
of effective communication and interpersonal relations in the hospital there would
be a high demand for better patient care and a development of better culture.
Nearly 38 per cent (strongly disagree 7.9 per cent and disagree 30.0 per cent) of the
staff have disagreed that the hospitals never break the rules and ethics which have
been laid down. There is some possibility of a slight change in the rules while
applying them to the staff members. This may cause some resentment among the
staff. If the staff members continue to see or experience such a situation they get
frustrated and it will hamper patient care. This factor is also the source for
demotivation among the nursing staff. Further, it is a strong source for the
organisation’s cultural damage and there is no scope for developing or maintaining
a healthy culture within the organisation. Finally, the management is responsible for
introducing, maintaining and developing a better climate and culture within the
organisation.

171
G. Self-perception of performance
The nursing staff’s performance is basically the outcome of their own satisfaction,
patient satisfaction, and the achievement of the hospital objectives. Performance is
defined as “A quantitative measure characterizing a physical or functional attribute
relating to the execution of a mission/operation or function”. Similarly,
“performance is the accomplishment of work assignments or responsibilities and
contributions to the organizational goals, including behaviour and professional
demeanor (actions, attitude, and manner of performance) as demonstrated by the
employee’s approach to completing work assignments”. Accordingly the
performance is an employee's accomplishment of the assigned work as specified in
the criteria and as measured against the standards of the employee's position. The
key dimensions associated with the nursing staff performance are capacity to
perform, willingness to perform and the opportunity to perform. The nursing staff’s
capacity to perform depends on the nursing staff’s ability, age, health, skills,
intelligence, level of education, endurance, stamina, energy level and motor skills.
The willingness to perform depends on motivation, job satisfaction, job status,
anxiety, legitimacy of participation, attitude, perceived task characteristics, job
involvement, ego involvement, self-image, personality, norms, values, perceived
role expectations, feelings of equity,. the opportunity to perform, equipment,
material, and supplies; working conditions; action of coworkers; leader behaviour;
mentorism; organisational policies, rules and procedures; information; time; and
pay.
Performance measurement
Outcomes are often preferred for measuring system performance, but because many
factors can influence outcomes besides nursing care, correctly interpreting outcome
measures requires appropriate controls for these other factors, controls that can be
difficult to implement. At the other end of the spectrum, structural measures are
often viewed as too rigid and because many processes can affect how structure
influences outcomes, making structure an imperfect substitute for how the system is
performing. Process measures, like structural measures, are often easier to measure,
but their connection to patient outcomes must be validated (Eddy 1998) and their
strength is dependent on their association to clinically tested practice guidelines and

172
patient outcomes. This requires an evidence-based approach that is currently
limited.
There are four components which can help to measure performance that include
clinical utilization and outcomes, financial performance and condition, system
integration and change, and patient satisfaction (McGillis Hall 2002). A wide range
of factors have been proposed as key influencers in the performance of nursing.
They fall into four broad categories: nurse training and competencies, physical plant
and structure, nursing organization, and work environment and culture. Since all
these factors have wide ranges and need evidence based outcome, it is decided to
understand the nursing performance through self perception process. The key
dimensions that are used to understand self perception of the nursing staff’s
performance is knowledge, ability to handle the work load, ability to handle the
patients, punctuality and attendance, interpersonal relationship, and future potential
development of nurses. These details are presented in Table 3.12
Nearly 52 per cent of the nursing staff feel that their knowledge on their job is good,
while 39 per cent of the staff feel that their knowledge on their job is very good.
This indicates that the staff members are very positive about the knowledge they
posses. The knowledge level would help better nursing care and safety for the
patients. Nearly 44.2 per cent of the nursing staff feel good about their ability to
handle the work load placed upon them, while 53 per cent of the staff feel very
good about their ability to handle the work load placed on them. This shows that
the nursing staff are confident of their ability to handle the work load which they
are entrusted with from time to time. Since the majority of the nursing staff are
experienced they have learnt to manage the workload effectively.

173
Table 3.12 Nursing staff’ perception on their performance
Variables Grading Present designation
Total Staff Nurse Sister
incharges
Your knowledge about your job
Poor 1 (0.4) 0 (0.0) 1 (0.3)
Average 20 (7.6) 7 (13.2) 27 (8.5)
Good 140 (53.0) 24 (45.3) 164 (51.7)
Very good 103 (39.0) 22 (41.5) 125 (39.4)
Your ability to handle the work load placed upon you
Average 8 (3.0) 2 (3.8) 10 (3.2)
Good 120 (45.5) 20 (37.7) 140 (44.2)
Very good 136 (51.5) 31 (58.5) 167 (52.7)
Your ability to handle the patient
Average 5 (1.9) 2 (3.8) 7 (2.2)
Good 115 (43.6) 21 (39.6) 136 (42.9)
Very good 144 (54.5) 30 (56.6) 174 (54.9)
Your view about your punctuality and attendance at work
Poor 1 (0.4) 0 (0.0) 1 (0.3)
Average 12 (4.5) 6 (11.3) 18 (5.7)
Good 111 (42.0) 14 (26.4) 125 (39.4)
Very good 140 (53.0) 33 (62.3) 173 (54.6)
Your inter-personal relationship with colleagues and co-workers
Poor 0 (0.0) 2 (3.8) 2 (0.6)
Average 6 (2.3) 0 (0.0) 6 (1.9)
Good 108 (40.9) 19 (35.8) 127 (40.1)
Very good 150 (56.8) 32 (60.4) 182 (57.4)
Your estimate about your own potential to develop further as professional
Very poor 2 (0.8) 0 (0.0) 2 (0.6)
Poor 2 (0.8) 0 (0.0) 2 (0.6)
Average 28 (10.6) 4 (7.5) 32 (10.1)
Good 126 (47.7) 24 (45.3) 150 (47.3)
Very good 106 (40.2) 25 (47.2) 131 (41.3)
Total 264 (100) 53 (100) 317 (100)(Figures in brackets indicate the percentage of nursing staff) N=317
Nearly 43 per cent of nursing staff feel that their ability to handle the patients is
good while 55 per cent of the staff feel that their ability to handle the patient is very
good. This shows that the staff members are highly competent to take care of the
patients in their custody. Nearly 39 per cent of the nursing staff feel good about
their punctuality and attendance at work, and 55 per cent of the staff feel very good
for the same. This shows that the nursing staff are conscientious about their work,
value time, and are able to do their work in time.

174
Nearly 40 per cent of the nursing staff feel that their interpersonal relationships with
colleagues and co-workers is good, while 57 per cent of the staff feel that their
inter-personal relationship with colleagues and co-workers is very good. This shows
that the nursing staff are able to achieve team work and effect a better performance
through coordinated efforts. Nearly 47 per cent of the nursing staff feel that their
estimate about their own potential to develop further as a professional is good,
while 41 per cent of the staff opine that their potential is very good. This shows that
the nursing staff expect themselves to be better professionals and there is a high
scope for them to develop their skills and abilities.


















