Chapter 1: Developmental, Cellular, and Molecular …...Chapter 1: Developmental, Cellular, and...
21
Chapter 1: Developmental, Cellular, and Molecular Basis of Human Breast Cancer Jose Russo, Yun-Fu Hu, Xiaoqi Yang, Irma H. Russo Breast cancer, which is the most common neoplastic disease in females and accounts for up to one third of all new cases of women’s cancer in North America, continues to rise in incidence. In addition, the mortality caused by this disease has remained almost unchanged for the past 5 decades, be- coming only second to lung cancer as a cause of cancer- related death. The failure in eradicating this disease is largely due to the lack of identification of a specific etiologic agent, the precise time of initiation, and the molecular mechanisms responsible for cancer initiation and progres- sion. Despite the numerous uncertainties surrounding the origin of cancer, there is substantial evidence that breast cancer risk relates to endocrinologic and reproductive fac- tors. The development of breast cancer strongly depends on the ovary and on endocrine conditions modulated by ovarian function, such as early menarche, late menopause, and par- ity. However, the specific hormone or hormone combina- tions responsible for cancer initiation have not been identi- fied, and their role as protective or risk factors is still incompletely understood. A highly significant female hor- mone is estrogen, which is involved in the development of a variety of cancers, but it is still unclear whether estrogens are carcinogenic to the human breast. An understanding of whether estrogens cause mutations, and, if so, whether they act through hormonal effects activated by receptor binding, cytochrome P450-mediated metabolic activation, or compro- mise the DNA repair system, is essential for determining whether this steroid hormone is involved in the initiation or progression of breast cancer. This knowledge has to be based on a multidisciplinary approach encompassing studies of the development of the breast, influence of hormones on the differentiation of individual structures, and their interrela- tions in the pathogenesis of breast cancer. The analysis of the mechanisms involved would require confirmation in the ad- equate in vitro models and determination of the role played by genomic alterations in both cancer initiation and progres- sion. [J Natl Cancer Inst Monogr 2000;27:17–37] Breast cancer accounts for up to one third of all new cases of women’s cancer in North America, representing the most com- mon neoplastic disease in the female (1). The incidence rates of this disease have been approximately level during the past de- cade, and breast cancer mortality is declining in the United States and in certain industrialized areas. However, these favor- able trends have not been observed in nations with lower breast cancer incidence, and societies traditionally known to have low breast cancer incidence are experiencing an increase in both incidence and mortality (1,2). Even though the U.S. mortality rates in females decreased an average of approximately 1.7% per year from 1990 through 1995, breast cancer retains the first place as a cause of cancer-related death in nonsmoking women (1,2). The failure in eradicating this disease is largely due to the lack of identification of a specific etiologic agent, the precise time of initiation, and the molecular mechanisms responsible for cancer initiation and progression. Despite the numerous uncer- tainties surrounding the origin of cancer, intensive epidemio- logic, clinical, and genetic studies have identified a number of biologic and social traits as risk factors associated with breast cancer (2–5). Principal among them are the evidence of BRCA1 and BRCA2 susceptibility genes; familial history of cancer in the breast, ovary, or endometrium; individual history of breast diseases; advanced age; higher socioeconomic status; excess ionizing radiation exposure; tallness in adult life; consumption of alcohol; and a variety of endocrinologic and reproductive factors (2–5). These latter factors include early onset of men- struation, nulliparity or delayed first childbirth, short duration of breast-feeding, late menopause, postmenopausal obesity, ex- tended use of oral contraceptives, and prolonged estrogen re- placement therapy (2–5). Among the hormonal influences, a major role has been at- tributed to the unopposed exposure to elevated levels of estro- gens (6), as has been indicated for a variety of female cancers, namely vaginal, hepatic, and cervical carcinomas (7–12). How- ever, the mechanisms through which this phenomenon occurs have not been completely understood (6). In fact, it is still un- clear whether estrogens are carcinogenic to the human breast. Most of the current understanding of the carcinogenicity of es- trogens is based on clinical observations of a greater risk of endometrial hyperplasia and neoplasia associated with estrogen supplementation (10–12) and experimental data (13–15). At least three mechanisms are considered to be responsible for the carcinogenicity of estrogens; the most widely recognized is the receptor-mediated hormonal activity, which is generally related to stimulation of cellular proliferation, resulting in more oppor- tunities for accumulation of genetic damage leading to carcino- genesis (16,17). The second mechanism is the cytochrome P450- mediated metabolic activation, which elicits direct genotoxic effects by increasing mutation rates (18–43), and a third mecha- nism is postulated to compromise the DNA repair system, re- sulting in the accumulation of lesions in the genome essential to estrogen-induced tumorigenesis (13). Disappointingly, the molecular mechanisms underlying the development of breast cancer in general, and estrogen-associate breast carcinogenesis in particular, are not completely under- stood. It is generally believed that the initiation of breast cancer results from uncontrolled cellular proliferation and/or aberrant programmed cell death or apoptosis as a consequence of cumu- Affiliation of authors: Breast Cancer Research Laboratory, Fox Chase Cancer Center, Philadelphia, PA Correspondence to: Jose Russo, M.D., Breast Cancer Research Laboratory, Fox Chase Cancer Center, 7701 Burholme Ave., Philadelphia, PA (e-mail: [email protected]). See “Note” following “References.” © Oxford University Press Journal of the National Cancer Institute Monographs No. 27, 2000 17
Transcript of Chapter 1: Developmental, Cellular, and Molecular …...Chapter 1: Developmental, Cellular, and...

Chapter 1: Developmental, Cellular, and Molecular Basisof Human Breast Cancer
Jose Russo, Yun-Fu Hu, Xiaoqi Yang, Irma H. Russo
Breast cancer, which is the most common neoplastic diseasein females and accounts for up to one third of all new casesof women’s cancer in North America, continues to rise inincidence. In addition, the mortality caused by this diseasehas remained almost unchanged for the past 5 decades, be-coming only second to lung cancer as a cause of cancer-related death. The failure in eradicating this disease islargely due to the lack of identification of a specific etiologicagent, the precise time of initiation, and the molecularmechanisms responsible for cancer initiation and progres-sion. Despite the numerous uncertainties surrounding theorigin of cancer, there is substantial evidence that breastcancer risk relates to endocrinologic and reproductive fac-tors. The development of breast cancer strongly depends onthe ovary and on endocrine conditions modulated by ovarianfunction, such as early menarche, late menopause, and par-ity. However, the specific hormone or hormone combina-tions responsible for cancer initiation have not been identi-fied, and their role as protective or risk factors is stillincompletely understood. A highly significant female hor-mone is estrogen, which is involved in the development of avariety of cancers, but it is still unclear whether estrogensare carcinogenic to the human breast. An understanding ofwhether estrogens cause mutations, and, if so, whether theyact through hormonal effects activated by receptor binding,cytochrome P450-mediated metabolic activation, or compro-mise the DNA repair system, is essential for determiningwhether this steroid hormone is involved in the initiation orprogression of breast cancer. This knowledge has to be basedon a multidisciplinary approach encompassing studies of thedevelopment of the breast, influence of hormones on thedifferentiation of individual structures, and their interrela-tions in the pathogenesis of breast cancer. The analysis of themechanisms involved would require confirmation in the ad-equate in vitro models and determination of the role playedby genomic alterations in both cancer initiation and progres-sion. [J Natl Cancer Inst Monogr 2000;27:17–37]
Breast cancer accounts for up to one third of all new cases ofwomen’s cancer in North America, representing the most com-mon neoplastic disease in the female (1). The incidence rates ofthis disease have been approximately level during the past de-cade, and breast cancer mortality is declining in the UnitedStates and in certain industrialized areas. However, these favor-able trends have not been observed in nations with lower breastcancer incidence, and societies traditionally known to have lowbreast cancer incidence are experiencing an increase in bothincidence and mortality (1,2). Even though the U.S. mortalityrates in females decreased an average of approximately 1.7% peryear from 1990 through 1995, breast cancer retains the firstplace as a cause of cancer-related death in nonsmoking women(1,2).
The failure in eradicating this disease is largely due to thelack of identification of a specific etiologic agent, the precisetime of initiation, and the molecular mechanisms responsible forcancer initiation and progression. Despite the numerous uncer-tainties surrounding the origin of cancer, intensive epidemio-logic, clinical, and genetic studies have identified a number ofbiologic and social traits as risk factors associated with breastcancer (2–5). Principal among them are the evidence of BRCA1and BRCA2 susceptibility genes; familial history of cancer inthe breast, ovary, or endometrium; individual history of breastdiseases; advanced age; higher socioeconomic status; excessionizing radiation exposure; tallness in adult life; consumptionof alcohol; and a variety of endocrinologic and reproductivefactors (2–5). These latter factors include early onset of men-struation, nulliparity or delayed first childbirth, short duration ofbreast-feeding, late menopause, postmenopausal obesity, ex-tended use of oral contraceptives, and prolonged estrogen re-placement therapy (2–5).
Among the hormonal influences, a major role has been at-tributed to the unopposed exposure to elevated levels of estro-gens (6), as has been indicated for a variety of female cancers,namely vaginal, hepatic, and cervical carcinomas (7–12). How-ever, the mechanisms through which this phenomenon occurshave not been completely understood (6). In fact, it is still un-clear whether estrogens are carcinogenic to the human breast.Most of the current understanding of the carcinogenicity of es-trogens is based on clinical observations of a greater risk ofendometrial hyperplasia and neoplasia associated with estrogensupplementation (10–12) and experimental data (13–15). Atleast three mechanisms are considered to be responsible for thecarcinogenicity of estrogens; the most widely recognized is thereceptor-mediated hormonal activity, which is generally relatedto stimulation of cellular proliferation, resulting in more oppor-tunities for accumulation of genetic damage leading to carcino-genesis (16,17). The second mechanism is the cytochrome P450-mediated metabolic activation, which elicits direct genotoxiceffects by increasing mutation rates (18–43), and a third mecha-nism is postulated to compromise the DNA repair system, re-sulting in the accumulation of lesions in the genome essential toestrogen-induced tumorigenesis (13).
Disappointingly, the molecular mechanisms underlying thedevelopment of breast cancer in general, and estrogen-associatebreast carcinogenesis in particular, are not completely under-stood. It is generally believed that the initiation of breast cancerresults from uncontrolled cellular proliferation and/or aberrantprogrammed cell death or apoptosis as a consequence of cumu-
Affiliation of authors: Breast Cancer Research Laboratory, Fox Chase CancerCenter, Philadelphia, PA
Correspondence to: Jose Russo, M.D., Breast Cancer Research Laboratory,Fox Chase Cancer Center, 7701 Burholme Ave., Philadelphia, PA (e-mail:[email protected]).
See “Note” following “References.”
© Oxford University Press
Journal of the National Cancer Institute Monographs No. 27, 2000 17

lative genetic damages that lead to genetic alterations that resultin activation of proto-oncogenes and inactivation of tumor sup-pressor genes (44,45). Genetic alterations, in turn, can be inher-ited as germline mutations or acquired as somatic mutations.These latter ones might occur as a result of exposure to envi-ronmental carcinogens, either physical (e.g., excess ionizing ra-diation), chemical (e.g., polycyclic hydrocarbons or nitro-soureas), and/or biologic (e.g., viruses) (5). The classic two-stageanimal model of chemical carcinogenesis has constituted thebasis for the generally accepted conclusions that the altered ge-notype of an initiated cell is irreversible and that the expressionof transformed phenotypes requires further genetic or epigeneticchanges (46). Tumor progression, the second stage of carcino-genesis in this model, involves exclusively epigenetic changesthat are considered to be reversible (46). It remains to be deter-mined whether this is true in breast cancer. The mechanismthrough which endocrinologic factors, such as hormone replace-ment therapy, influence cancer initiation and progression inwomen has not been clarified as yet. The development of breastcancer entails multiple events; unfortunately, the two main fac-tors elucidated in the experimental animal model, the causativeagent and the time of initiation, are unknown in the humanpopulation (47,48). The elucidation of whether estrogens act asendogenous carcinogenic agents requires a better understandingof the normal development of the breast under the influence ofphysiologic conditions, which in turn is important for under-standing the pathogenetic pathway leading to preneoplastic le-sions and cancer. The analysis of pure populations of humanbreast epithelial cells (HBECs) at various stages en route tomalignancy would be the direct approach to understanding thecellular and molecular processes of breast carcinogenesis (49).However, it has been extremely difficult to establish primarycultures of HBECs from breast lesions representing variousstages of neoplastic progression, and no cell lines at the inter-mediate stages of neoplastic transformation are available formechanistic studies (49). It is expected that an in vitro system ofHBECs that can reproduce the main steps of the in vivo situation,such as cell immortalization and transformation, would consti-tute an adequate tool for determining what genomic changes areimportant in the initiation and progression of the neoplastic pro-cess (50–62). It is, therefore, predicted that an in vitro system ofthis nature will allow us to test whether estrogens are endog-enous carcinogens and whether they play an essential role in theinitiation and/or the promotional phase of breast cancer.
DEVELOPMENTAL PATTERN OF THE HUMAN BREAST
FROM ADOLESCENCE TO MATURITY
The development of the breast, which is rigorously controlledby the ovary, can be defined by several parameters, such as itsexternal appearance, total area, volume, degree of branching,number of structures present in the mammary gland, and degreeof differentiation of individual structures, i.e., lobules and al-veoli (63–68).
The breast undergoes changes that are progressive from birthto early childhood, becoming striking at puberty. The adolescentperiod begins with the first signs of sexual change at puberty,which in American females sets in between the ages of 10 and12 years, and terminates with sexual maturity (64–66). Althoughpuberty is often considered to be the point of initiation of ovarianfunction, the development of the ovary is a gradual process thatdepends on pituitary gonadotropins. Receptors for the pituitary
luteinizing hormone (LH) and follicle-stimulating hormone(FSH) are present in the ovary even during the infantile period,when they stimulate the secretion of androgens after binding toand activating their respective receptors (69). FSH and LH in-teract with growth hormone (GH) and prolactin in modulatingovarian steroidogenesis, a function that is also influenced byepinephrine, secreted by the adrenal medulla. The release ofFSH is, in turn, modulated by inhibin and activin, glycoproteinhormones secreted by the ovary (69).
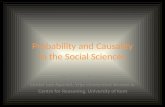
The mammary ductal tree undergoes progressive elongationand branching during childhood and puberty. These processesare positively regulated by GH, although its exact mechanism ofaction is unclear. GH directly stimulates ductal growth in hy-pophysectomized–ovariectomized rats, and it might act as wellthrough its local mediator, the insulin-like growth factor I. Nor-mal ductal development, however, requires the presence of es-trogen and progesterone, the two ovarian steroid hormones thatact on the mammary gland through their respective receptors. Aspuberty approaches, the rudimentary mamma begins to showgrowth activity both in the glandular tissue and in the surround-ing stroma. Glandular increase is due to the growth and divisionof small bundles of primary ducts originated during intrauterinelife from invaginations of the superficial ectoderm (63,65–67).The ducts grow and divide through a combination of dichoto-mous and sympodial branching, forming at the distal epithelial–stromal boundary a club-shaped terminal end bud. Each terminalend bud bifurcates into two smaller ductules or alveolar buds(67,70). The term alveolar bud applies to those structures thatappear morphologically more developed than the terminal endbud. With further branching, alveolar buds become smaller andmore numerous, and then they are called ductules. When anaverage of 11 alveolar buds/ductules cluster around a terminalduct, they form the lobule type 1 (Lob 1) or virginal lobule (Fig.1) (67). Terminal ducts and ductules are lined by a two-layeredepithelium, whereas terminal end buds in the human fetus arelined by an epithelium composed of up to four layers of cells.Lobule formation in the female breast occurs within 1–2 yearsafter onset of the first menstrual period. Afterward, the ulteriordevelopment of the gland varies greatly from woman to woman.Full differentiation of the mammary gland is a gradual process
Fig. 1. Whole mount preparation of breast tissue of an 18-year-old nulliparouswoman showing lobule 1. Toluidine blue, ×25.
18 Journal of the National Cancer Institute Monographs No. 27, 2000

taking many years, and it can be assumed that in all women inwhom pregnancy did not supervene, it was never attained (63).
The normal breast tissue of adult women contains two otheridentifiable types of lobules in addition to the Lob 1 describedabove. These are designated lobule type 2 (Lob 2) and type 3(Lob 3) (Figs. 2 and 3). The transition from Lob 1 to Lob 2 andof these to Lob 3 is a gradual process of sprouting of newductules, which increase in number from approximately 11 inLob 1 to 47 and 80 in Lob 2 and Lob 3, respectively (Fig. 3,Table 1). As the number of ductules increases, so does the sizeof the lobules, even though individual ductules appear reducedin size (Table 1) (63,68).
The breast of nulliparous women contains more undifferen-tiated structures, such as terminal ducts and Lob 1, although Lob2 and Lob 3 are occasionally observed. These characteristics arenot influenced by age or menopausal status (Fig. 4). In parouspremenopausal women, the predominant structure is the mostdifferentiated Lob 3, whose number peaks during the early re-productive years. They start to decrease after the fourth decadeof life, as the proportion of Lob 1 increases, and, when meno-pause sets in, they reach the same values observed in nulliparouswomen (Fig. 4). In the breast of nulliparous women, the Lob 2is present in moderate numbers during the early years, sharplydecreasing after age 23 years, whereas the number of Lob 1remains significantly higher. This observation suggests that acertain percentage of Lob 1 might have progressed to Lob 2, butthe number of Lob 2 progressing to Lob 3 is significantly lowerin nulliparous women as compared with parous women. In thecase of parous women, it is interesting to note that a history ofparity between the ages of 14 and 20 years is associated with asignificant increase in the number of Lob 3 that remains presentas the predominant structure until the age of 40 years, the timeat which a decrease in the number of Lob 3 occurs, probablybecause of their involution to predominantly Lob 1 (Fig. 4)(63,68).
HORMONAL INFLUENCES ON THE DEVELOPMENT OF
THE BREAST
The breast is a hormone-responsive organ by excellence. Itsdevelopment is influenced by a myriad of hormones and growth
factors, responding selectively to given hormonal stimuli witheither cell proliferation or differentiation. The type of responseelicited is, in turn, modulated by specific topographic character-istics of the mammary parenchyma (70–78). In either case, theresponse of the mammary gland to these complex hormonal andmetabolic interactions results in developmental changes that per-manently modify both the architecture and the biologic charac-teristics of the gland (72,73). Among all of the complex hor-monal influences, estrogens are considered to play a major rolein promoting the proliferation of both the normal and the neo-plastic breast epithelium (71,72). Estradiol acts locally on themammary gland, stimulating DNA synthesis and promoting budformation. Although the influence of estrogens on the prolifera-tive activity of mammary epithelial cells has been traditionallyconsidered to be mediated by at least three different mecha-nisms, a receptor-mediated (79–85), an autocrine/paracrine loop(85), and/or a negative feedback (86), it is generally acceptedthat the biologic activities of estrogens are mediated by thenuclear estrogen receptor (ER) that, on activation by cognateligands, forms a homodimer with another ER-ligand complexand activates transcription of specific genes containing the es-trogen response elements (87). According to this classic model,the biologic responses to estrogens are mediated by a well-characterized ER.
Fig. 2. Whole mount preparation of human breast tissue of a 24-year-old nul-liparous woman showing lobule 2. Toluidine blue, ×25.
Fig. 3. Whole mount preparation of human breast tissue of a 35-year-old parouswoman containing lobule 3. Toluidine blue, ×25.
Table 1. Characteristics of the lobular structures of the human breast
StructureLobular
area,* mm2No. of ductules
per lobule†Area of each
ductule,‡ mm2No. of cells/
cross-section§
Lob 1 0.048 ± 0.044 11.2 ± 6.3 0.232 × 10−2 32.4 ± 14.1Lob 2 0.060 ± 0.026 47.0 ± 11.7 0.167 × 10−2 13.1 ± 4.8Lob 3 0.129 ± 0.049 81.0 ± 16.6 0.125 × 10−2 11.0 ± 2.0
*Student’s t tests were done for all possible comparisons. Lobular (Lob) areasshowed significant differences between Lob 1 versus Lob 3 and Lob 2 versusLob 3 (P<.005).
†The number of ductules per lobule was different (P<.01) in all the compari-sons.
‡The area of each ductule per cross-section was significantly different inductules of Lob 1 versus Lob 2 and Lob 3 (P<.01).
§The number of cells per cross-section was significantly different in ductulesof Lob 1 versus Lob 2 and Lob 3 (P<.01). Modified from (63).
Journal of the National Cancer Institute Monographs No. 27, 2000 19

The recent cloning of a new type of ER, the ER� from the rat(88), mouse (89), and human (90) tissues, has required research-ers to rename the traditional ER as ER�. The presence of ER�in target tissue or cells is essential to their responsiveness toestrogen action. In fact, the expression levels of ER� in a par-ticular tissue have been used as an index of the degree of estro-gen responsiveness (91). A vast majority of human breast car-cinomas are initially positive for ER�, and their growth can bestimulated by estrogens and inhibited by antiestrogens (92–94).ER� and ER� share high sequence homology, especially in theregions or domains responsible for specific binding to DNA andthe ligands (88–90). ER� can be activated by estrogen stimula-tion and blocked with antiestrogens (88,90,95). On activation,ER� can form homodimers as well as heterodimers with ER�(95–99). The existence of two ER subtypes and their ability toform DNA-binding heterodimers suggests three potential path-ways of estrogen signaling: via the ER� or ER� subtype intissues exclusively expressing each subtype and via the forma-tion of heterodimers in tissues expressing both ER� and ER�(97). In addition, estrogens and antiestrogens can induce differ-ential activation of ER� and ER� to control transcription ofgenes that are under the control of an AP1 element (100).
The importance of the integrity of ER� in the mammarygland has been clearly elucidated by using the �-ER knock-out(KO) mice (101). The mammary glands of these animals arepoorly developed. Nonetheless, the �-ERKO mammary glandappears to possess the intrinsic tissue components necessary forpubertal development and pregnancy-induced maturation, but itfails to develop because of the loss of multiple stimuli that aredownstream of ER� action (101). Unlike the dramatic underde-velopment observed in the mammary gland of the �-ERKOmouse, no such phenotype is observed in adult �-ERKO females(101). Although these studies are important for our understand-ing of the role of both ERs, extrapolation to the human breast
needs to be carefully done because these genetic-engineeredmice reflect only a portion of the functional complexity of thehuman situation.
Progesterone is another major, although controversial, playerin mammary gland biology. This ovarian steroidal hormone alsoacts, in conjunction with estrogen, through its specific receptorPgR in the normal epithelium for regulating breast development.The role of these hormones on the proliferative activity of thebreast, which is indispensable for its normal growth and devel-opment, has been for a long time, and still is, the subject ofheated controversies. Although estrogen is known to stimulatecell proliferation, the breast epithelium of sexually mature andnormally cycling women does not exhibit maximal proliferationduring the follicular phase of the menstrual cycle (77,78,102–106), when estrogens reach peak levels of 200–300 pg/mL andprogesterone is less than 1 ng/mL (107). Instead, the breastepithelium exhibits its maximal proliferative activity during theluteal phase, when progesterone levels reach 10–20 ng/mL andestrogen levels are twofold to threefold lower than those ob-served during the follicular phase (107). These observations arepuzzling when analyzed to the light of in vitro and experimentaldata because estrogen stimulates the proliferation of culturedbreast cells and breast tissues implanted in athymic nude mice.Progesterone, however, has no effect or even inhibits cell growthin the same models (105,106).
In addition to its response to circulating hormones, the pro-liferative activity of the mammary epithelium in both rodentsand humans varies with the degree of differentiation of the mam-mary parenchyma (68,71–74,108,109). In humans, the highestlevel of cell proliferation is observed in the undifferentiated Lob1 present in the breast of young nulliparous females (71–74).The progressive differentiation of Lob 1 into Lob 2 and Lob 3,occurring under the hormonal influences of the menstrual cycle,and the full differentiation into lobules type 4 (Lob4) as theresult of pregnancy leads to a concomitant reduction in the pro-liferative activity of the mammary epithelium (68,71–74,108,109).
The relationship of lobular differentiation, cell proliferation,and hormone responsiveness of the mammary epithelium is justbeginning to be unraveled. Of interest, the content of ER� andPgR in the lobular structures of the breast is directly proportionalto the rate of cell proliferation. These three parameters are maxi-mal in the undifferentiated Lob 1, decreasing progressively inLob 2, Lob 3, and Lob 4 (Fig. 5, Table 2). The determination ofthe rate of cell proliferation, expressed as the percentage of cellsthat stain positively with Ki67 antibody, has revealed that pro-liferating cells are predominantly found in the epithelium liningducts and lobules and less frequently in the myoepithelium andin the intralobular and interlobular stroma. Ki67-positive cellsare most frequently found in Lob 1 (Fig. 5, Table 2). The per-centage of positive cells is reduced by threefold in Lob 2 and bymore than 10-fold in Lob 3 (Figs. 5 and 6, Table 2) (73,110).ER�- and PgR-positive cells are found exclusively in the epi-thelium; the myoepithelium and the stroma are totally devoid ofsteroid receptor-containing cells. The highest number of cellspositive for both receptors is found in Lob 1, decreasing pro-gressively in Lob 2 and Lob 3 (Fig. 5, Table 2) (110).
To clarify the relationship between steroid receptor-positivecells and proliferating cells, we used a double-staining proce-dure, combining in the same tissue section anti-Ki67 and ER�,Ki67 and PgR, or ER� and PgR antibodies. Each antibody was
Fig. 4. Percentage of lobules (Lob) type 1 (Lob 1), type 2 (Lob 2), and type 3(Lob 3) in the breasts of parous premenopausal (Pre-Men.), parous postmeno-pausal (Post-Men), and of nulliparous premenopausal and postmenopausal (Pre& Post-Men) women.
20 Journal of the National Cancer Institute Monographs No. 27, 2000

identified by its color reaction, brown with 3,3�-diaminobenzi-dine-HCl (DAB) or red with the alkaline phosphatase-vector red(110). This procedure allowed us to quantitatively determine thespatial relationship between those cells that are proliferating andthose that react with either ER� or PgR antibodies. It was foundthat a higher percentage of cells reacted simultaneously withboth ER� and PgR, appearing purple red in color (Fig. 6),whereas the number of cells positive for both ER� and Ki67or PgR and Ki67 was very low (Table 2). The highest percentageof ER�-, PgR-, and Ki67-positive cells was observed in Lob 1(Fig. 6, Table 2). The percentages of Ki67-, ER�-, and PgR-positive cells was reduced to 1.6%, 3.8%, and 0.7% in Lob 2,respectively. Their percentages became negligible in Lob 3(Table 2).
Of interest was the observation that even though there weresimilarities in the relative percentages of Ki67-, ER�- and PgR-positive cells and in the progressive reduction in the percentageof positive cells as the lobular differentiation progressed, thosecells positive for Ki67 were not the same that reacted positivelyfor ER� or PgR (Fig. 6) (110). Very few cells, less than 0.5% in
Lob 1 and even fewer in Lob 2 and Lob 3, were positive for bothKi67 and ER� (Ki67+ER) or Ki67 and PgR (Ki67+PgR) (Table2). Despite their low percentage, still double-labeled (Ki67+ER)cells were more numerous in Lob 1, decreasing gradually in Lob2 and Lob 3. The percentage of cells exhibiting double labelingwith Ki67 and PgR, however, were more numerous in Lob 2than in Lob 1 but decreased to the same levels observed for ER�in Lob 3 (Table 2).
The simultaneous immunocytochemical detection of prolif-erating cells and of those containing ER� and PgR in normalbreast tissue led us to conclude that their number varies with thedegree of lobular development of the organ and that steroidreceptor content is linearly related to the rate of cell prolifera-tion. The use of a double-labeling immunocytochemical tech-nique has allowed us to demonstrate that the expression of thereceptors occurs in cells other than the proliferating cells, con-firming results reported by others (104). The findings that pro-liferating cells are different from those that are ER� positive andPgR positive support data that indicate that estrogen controls cellproliferation by an indirect mechanism. This phenomenon hasbeen demonstrated with the use of a supernatant of estrogen-treated ER�-positive cells that stimulates the growth of ER�-negative cell lines in culture. The same phenomenon has beenshown in vivo in nude mice bearing ER-negative breast tumorxenografts (111,112). ER�-positive cells treated with antiestro-gens secrete tumor growth factor-� that inhibits the proliferationof ER�-negative cells (113). The fact that the highest prolifera-tive activity and the highest percentage of ER�- and PgR-positive cells are present in Lob 1 provides a mechanistic ex-planation for the higher susceptibility of these structures to betransformed by chemical carcinogens in vitro (47,114), support-ing as well the observations that Lob 1 is the site of origin ofductal carcinomas (115).
ARCHITECTURAL PATTERN OF THE NORMAL BREAST
AT MENOPAUSE
Menopause supervenes as the consequence of the atresia ofmore than 99% of the 400 000 follicles that are present in theovaries of a female fetus of a gestational age of 5 months (69).Gonadotropin-releasing hormone secretion is also implicated inthis phenomenon, indicating that a hypothalamic process is in-volved in the development of menopause. The most character-istic sign of menopause is amenorrhea, which is the result of thealmost complete cessation of ovarian estrogen and progesteroneproduction. The years leading to the final menstrual period, untilmenopause sets in, generally at around the age of 51 years,constitute the perimenopause. During this period, many women
Table 2. Distribution of Ki67, ER-�, and PgR-positive cells in the lobular structures of the human breast
Lobule type No. cells Ki67 ER PgR Ki67 + ERn Ki67 + PgRo
Lob 1 19 339a 4.72 ± 1.00d,e 7.46 ± 2.88h 5.70 ± 1.36k 0.48 ± 0.28 0.09 ± 0.01Lob 2 8490b 1.58 ± 0.45f 3.83 ± 2.44i 0.73 ± 0.57l 0.31 ± 0.21 0.28 ± 0.27Lob 3 17 750c 0.40 ± 0.18g 0.76 ± 0.04j 0.09 ± 0.04m 0.01 ± 0.01 0.01 ± 0.01
aTotal number of cells counted in lobule 1 (Lob 1) in breast tissue samples of 12 donors; btotal number of cells counted in Lob 2 in breast tissue samples of 5donors; ctotal number of cells counted in Lob 3 in breast tissue samples of three donors; dproliferative activity determined by the percentage of cells Ki67 positive,expressed as the mean ± standard deviation. Differences were significant in eLob 1 versus flob 2 (t � 1.98; P<.05), fLob 2 versus gLob 3 (t � 2.27; P<.04), andeLob 1 versus gLob 3 (t � 2.56; P<.01). Estrogen receptor (ER)-positive cells were significantly different in hLob 1 versus iLob 2 and jLob 3 (t � 2.04; P<.05).Progesterone receptor (PgR)-positive cells were significantly different in kLob 1 versus lLob 2 (I � 2.27; P<.05) and in kLob 1 versus mLob 3 (t � 2.60; P<.03).nPercentage of cells positive for both Ki67 and ER, expressed as the mean ± SD. oPercentage of cells positive for both Ki67 and PgR, expressed as themean ± standard deviation. Reprinted with permission by Kluwer Academic Publishers (110).
Fig. 5. Percentage of cells positive for estrogen receptor (ER), for progesteronereceptor (PgR), for proliferating cells (Ki67), and for both ER and Ki67(ER+Ki67), or PgR and Ki67 (PgR+Ki67) (ordinate). Cells were quantitated inlobule 1 (Lob 1), Lob 2, and Lob 3 of the breast (abscissa). Reproduced withpermission by Kluwer Academic Publishers (110).
Journal of the National Cancer Institute Monographs No. 27, 2000 21

ovulate irregularly, either because the rise in estrogen during thefollicular phase is insufficient to trigger a LH surge or becausethe remaining follicles are resistant to the ovulatory stimulus(69). The increase in human longevity occurring in our societyhas caused a considerable increment in the number of womenthat will live one third or more of their lives after menopause, aperiod characterized by profound ovarian hormone deprivation.
After menopause the breast undergoes regression in both nul-liparous and parous women. This regression is manifested as anincrease in the number of Lob 1 and a concomitant decline in thenumber of Lob 2 and Lob 3. At the end of the fifth decade of life,the breast of both nulliparous and parous women is composedpredominantly of Lob 1 (Fig. 4) (68). These observations haveled us to conclude that the understanding of breast developmentrequires a horizontal study in which all different phases ofgrowth are taken into consideration. For example, the analysis ofbreast structures at a single given point, i.e., age 50 years, wouldlead one to conclude that the breasts of both nulliparous andparous women are identical. However, the phenomena occurringin prior years might have imprinted permanent changes in thebreast, which affect its susceptibility to carcinogenesis but are nolonger morphologically observable. Thus, from a quantitativepoint of view, the regressive phenomenon occurring in the breastat menopause differs between nulliparous and parous women. Inthe breast of nulliparous women, the most predominant structureis the Lob 1, which comprises 65%–80% of the total lobule typecomponents and their relative percentage is independent of age.Second in frequency is the Lob 2, and the least frequent structureis the Lob 3, which represent 10%–35% and 0%–5% of the total
lobular population, respectively. In the breast of premenopausalparous women, however, the predominant lobular structure isthe Lob 3, which comprises 70%–90% of the total lobular com-ponent. Only after menopause the number of Lob 3 declines andthe relative proportion of the three lobular types approaches thatobserved in nulliparous women. Full lobular differentiation onlyoccurs in the parous women, especially in those completingfull-term pregnancy at a young age, but lobular differentiation innulliparous women seldom reaches the Lob 3 and never the Lob4 stages (68). These differences in the pattern of breast devel-opment between nulliparous and parous women greatly explainthe protective effect induced by pregnancy from breast cancerdevelopment. They also highlight the need to determine whetherthe undifferentiated Lob 1 of nulliparous women differ fromthose of the parous postmenopausal woman in their ability tometabolize estrogens or in the ability of the cells to repair geno-toxic damage (116,117).
ARCHITECTURAL PATTERN OF THE BREAST WITH
PROLIFERATIVE DISEASE
Our studies of the pattern of breast development in tissuesdevoid of mammary pathology, such as those obtained fromreduction mammoplasties, led us to establish certain criteria ofnormality specific for a given age and parity status of the donors.In these tissues, we identified parenchymal structures exhibitingvariations in the degree of differentiation, rate of cell prolifera-tion, and content of ER� and PgR (118). To answer the questionof whether breast lesions of either benign, premalignant, or ma-
Fig. 6. Ductal epithelium of the human breast. (A) Single-layered epithelium ofa lobule 1 (Lob 1) ductule contains Ki67 positive cells (brown nuclei) andestrogen receptor (ER)-positive cells (red purple nuclei; ×40); (B) the single-layered epithelium lining the ductule contains brown Ki67-positive cells, and redpurple PgR-positive cells. The specificity of the reaction was verified by invert-
ing the order of the stains, i.e., (C) and (D) ER-positive cells, brown, Ki67-positive cells, purple red; (E) brown nuclei of PgR-positive cells and a Ki67-positive cell in mitosis appears stained purple red (DAB-Hematoxylin; ×40).Reproduced with permission by Kluwer Academic Publishers (110).
22 Journal of the National Cancer Institute Monographs No. 27, 2000

lignant nature develop as a reflection of the stage of develop-ment of the breast, we compared parenchymal structures presentin 33 reduction mammoplasty specimens with those found in 45breast biopsies performed because of mammographic abnor-malities or clinically suspicious breast masses (Table 3). Be-cause the initiation of the neoplastic process is inversely relatedto the degree of differentiation of the breast, which in turn is afunction of reproductive history, the patient populations weresubdivided according to parity status (Table 3). In this study, weconfirmed previous observations that in the reduction mammo-plasty specimens (RM) the breast of nulliparous women of allages was composed predominantly of Lob 1, whereas the breastof parous premenopausal women contained a higher concentra-tion of Lob 3 (Table 3) (118). Those breast tissues obtained frombiopsies had an architectural pattern different from that obtainedfrom RM for women of comparable parity status because parouswomen that had a breast biopsy contained a higher percentage ofLob 1 and a lower percentage of Lob 3 than the parous popu-lation of the RM group (Table 3) (118).
The patient population that had breast biopsies was also sub-divided into subgroups, based on the histopathologic diagnosisof their lesions. One group of 21 patients had no pathologypresent (normal breast or control group), one group of 15 pa-tients had ductal hyperplasia (DH group), four patients had bluntduct adenosis (BDA group), and five patients had sclerosingadenosis (SAD group) (Table 4). Tissue sections from all thesegroups were analyzed for lobular architecture, type of pathologiclesions, and proliferative activity of the breast (Figs. 7 and 8)(118). The breast tissues of the groups classified as normalbreast (control) and DH had a significantly higher percentage ofLob 1 than Lob 2 and Lob 3 (P<.0008 and P<.0001, respec-tively) (Fig. 7). The breast tissues containing BDA were alsocharacterized by having a higher percentage of Lob 1, whereasthe SAD group had a higher percentage of Lob 2 (Table 4, Fig.7) (118). In all of the groups, the percentage of Lob 3 wassignificantly lower than that of Lob 1, although the relativepercentage of Lob 3 was significantly higher in breast biopsieswith BDA and SAD than in the normal breast biopsies or inthose diagnosed with DH (P<.05) (Fig. 7) (118).
The number of proliferating epithelial cells, determined byimmunostaining of the Ki67 nuclear antigen, was higher in Lob1 than in Lob 2 and Lob 3 (P<.001), with a similar pattern in thenormal breast, DH, and SAD groups, although the differenceswere not statistically significant between Lob 1 and Lob 2 in theSAD group (Fig. 8). In the BDA group, however, the rate of cellproliferation was higher in Lob 2 (P<.01) than in Lob 1 and Lob3 (Fig. 8) (118). Although the proliferative activity was on anaverage higher in Lob 1 than in Lob 3, the differences were not
statistically significant (Fig. 8) (118). These data allowed us toconclude that breast tissues obtained from biopsies performedbecause of mammographic or clinical abnormalities, even in theabsence of cancer, have architectural and cell kinetic patternsdifferent from the normal breast tissues obtained from reductionmammoplasties. More important is the observation that even inthose cases in which no pathology or only benign lesions werediagnosed, the pattern of breast development in biopsies wasmore similar to that of the cancer-bearing breast than it is tothe population not requiring a biopsy. Our findings that inDH-containing biopsies Lob 1 are the most frequent structurespresent and have the highest rate of cell proliferation support ourpostulate that DH originates from Lob 1 (115). Lob 2 and Lob 3,which are the sites of origin of more differentiated lesions, suchas BDA and SAD, are more prominently represented and aremore proliferative in those biopsies containing these typesof pathologic lesions. It is of importance to clarify that paritydoes not seem to influence the pattern of development inDH-containing breast tissues. A similar observation has beenmade in cancer-bearing breasts or in breasts of nulliparouswomen in terms of lobular composition.
BREAST DEVELOPMENT, HORMONES, AND THE
PATHOGENESIS OF BREAST CANCER
From our studies associating normal breast development andthe pathogenesis of both experimental and spontaneous mam-mary carcinogenesis emerged an important concept: that the Lob1, the most undifferentiated structure found in the breast ofyoung nulliparous women, is equivalent to the terminal ductallobular unit, a structure originally identified by Wellings et al.(119) as the site of origin of ductal carcinomas (Fig. 9) (63,70).This observation was supported by comparative studies of nor-mal and cancer-bearing breasts obtained at autopsy. We ob-served that the nontumoral parenchyma of those breasts that haddeveloped a malignancy contain a significantly higher numberof hyperplastic terminal ducts, atypical Lob 1, and ductal carci-nomas in situ originating from Lob 1 than those breasts free ofmalignancies. These findings indicate that the Lob 1 is affectedby both preneoplastic and neoplastic processes (115). More dif-ferentiated lobular structures have been found to be affected byneoplastic lesions as well, although they originate tumors whosehistologic type and malignancy are in an inverse relationshipwith the degree of differentiation of the parent structure(52,115,120,121). The finding that the most undifferentiatedstructures originate the most aggressive neoplasms is clinicallyimportant because these structures are more numerous in thebreasts of nulliparous women who are, in turn, at a higher risk ofdeveloping breast cancer (68).
Table 3. Lobular architecture of the breast—comparison of percentages of structures found in reduction mammoplasties and breast biopsies with proliferativebreast disease
Group (parity) No. of cases Age, y Lob 1 (%) Lob 2 (%) Lob 3 (%)
RM (all) 33 29.4 ± 8.2 22.45 ± 23.7a 37.25 ± 28.61c 38.41 ± 34.22e
RM (nulliparous) 9 22.9 ± 6.7 45.87 ± 27.40 47.17 ± 22.01 6.94 ± 7.01RM (parous) 24 31.9 ± 2.3 16.92 ± 8.26g 35.45 ± 3.14i 47.86 ± 33.4k
PBD (all) 45 46.6 ± 1.5 65.66 ± 34.15b 24.64 ± 20.64d 9.68 ± 6.31f
PBD (nulliparous) 10 42.5 ± 10.3 70.99 ± 33.3 25.26 ± 24.74 3.75 ± 1.6PBD (parous) 35 48.9 ± 11.8 65.25 ± 37.3h 21.10 ± 8.07 j 13.62 ± 3.10l
The differences between a and b is P<.0000005; the difference between c and d is P<.04; between e and f is P<.00009; between g and h P<1 × 10−7; between i andj is P<.07, and between k and l is P<.0003. RM � reduction mammoplasty; PBD � proliferative breast disease. Reprinted with permission by JAI Press (118).
Journal of the National Cancer Institute Monographs No. 27, 2000 23

The analysis of the nontumoral breast tissues from cancer-bearing lumpectomy or mastectomy specimens reveals that thebreasts in nulliparous women have an architecture dominated byLob 1, being their overall architecture similar to that of nullip-arous female free of mammary pathology (120,122). Althoughthe breast tissues of parous women from the general populationcontain predominantly Lob 3 and a very low percentage of Lob1, in those parous women who have developed breast cancer,their breast tissues have also the Lob 1 as the predominantstructure, appearing in this sense similar to those of nulliparouswomen. It is of interest that all of the parous women in ourstudies who had developed breast cancer had a history of latefirst full-term pregnancy or a family history of breast cancer.The analysis of these samples allowed us to conclude that thearchitecture of the breast of parous women with breast cancerdiffers from that of parous women without cancer. The similari-ties found between the architecture of the breast of nulliparouswomen and that of parous women with cancer support our hy-pothesis that the degree of breast development is of importancein the susceptibility to carcinogenesis and, furthermore, that par-
ous women who develop breast cancer might exhibit a defectiveresponse to the differentiating influence of the hormones ofpregnancy (52,115,120–122).
Breast cancer is a hormone-dependent malignancy. The riskof developing breast cancer has been traditionally linked to ex-posure to estrogen, mainly because a majority of breast cancerscontain receptors for this hormone. The ER� content of a tumoris considered to be a parameter of prognostic significance(123,124). There is no information available as yet of the prog-nostic significance of the ER� content of a tumor. The presenceof ER�-positive and ER�-negative cells and of proliferatingcells, regardless of the receptor status of the normal breast, mayhelp to elucidate the genesis of ER�-positive and ER�-negativebreast cancers (125,126). It has been suggested that ER�-negative breast cancers result from either the loss of the ability
Table 4. Lobular structures found in breast biopsies
Group Patient’s age, y No. Lob 1 (%) Lob 2 (%) Lob 3 (%)
Normal control 42.28 ± 6.66 21 71.95 ± 7.09 23.02 ± 5.47 5.11 ± 3.17Ductal hyperplasia 44.06 ± 11.37 15 87.76 ± 3.16 11.85 ± 3.10 0.24 ± 0.94Blunt duct adenosis 37.25 ± 11.64 4 58.39 ± 19.93 31.57 ± 11.75 9.82 ± 9.82Sclerosing adenosis 37.00 ± 3.16 5 37.92 ± 15.52 48.95 ± 15.65 11.31 ± 9.97
The ages of the patients in the four groups under study did not differ significantly. In the normal breast or control group, the percentage of lobule 1 (Lob 1) wassignificantly different from Lob 2 and Lob 3 (P<.0008); Lob 2 was significantly different from Lob 3 (P<.07). In the group with ductal hyperplasia, the percentageof Lob 1 was significantly different from Lob 2 and Lob 3 (P<.000001) and so were the differences between Lob 2 and Lob 3 (P<.02). The percentages of Lob 2in the groups with sclerosing adenosis and blunt duct adenosis were significantly higher than those of the control (P<.07) and ductal hyperplasia (P<.001) groups.The percentage of Lob 3 was significantly higher in the groups with sclerosing adenosis (P<.05) and blunt duct adenosis (P<.05) than in those breast tissuescontaining ductal hyperplasia. Reprinted with permission by JAI Press (118).
Fig. 7. Histogram showing the relative percentage of lobule 1 (Lob 1), Lob 2,and Lob 3 (ordinate) present in breast biopsies of women with proliferativelesions. D.H. � ductal hyperplasia; B.D.A. � blunt duct adenosis, and S.A.D.� sclerosing adenosis. Reproduced with permission by JAI Press (118). Fig. 8. Histogram showing the proliferative activity, determined as the percent-
age of cells reacting positively with Ki67 antibody, in the epithelium of lobule1 (Lob 1), Lob 2, and Lob 3 (ordinate) present in breast biopsies of women withproliferative lesions. D.H. � ductal hyperplasia; B.D.A. � blunt duct adenosis,and S.A.D. � sclerosing adenosis. Reproduced with permission by JAI Press(118).
24 Journal of the National Cancer Institute Monographs No. 27, 2000

of the cells to synthesize ER� during the clinical evolution ofER�-positive cancers or that ER�-positive and ER�-negativecancers are different entities (125,127).
We have observed that Lob 1 contains at least three cell
types: ER�-positive cells that do not proliferate, ER�-negativecells that are capable of proliferating, and a small proportion ofER�-positive cells that can proliferate as well (Fig. 10) (110).Therefore, estrogen might stimulate ER�-positive cells to pro-
Fig. 9. Whole mount preparations showing a lobule type 1 (Lob 1)(A) and a ductal carcinoma in situ involving several terminal ductsand Lob 1 (B). Toluidine blue, ×4.
Fig. 10. Schematic representation of the postulated pathways of estrogen actionson breast epithelial cells. Three different types of cells can be considered to bepresent in the mammary epithelium: Estrogen receptor negative (ER−) prolifer-ating cells (Ki67+), ER positive (ER+) cells that do not proliferate (Ki67−), anda small proportion of ER+ and Ki67+ cells. Estrogen might stimulate ER+ cells
to produce a growth factor that, in turn, stimulates neighboring ER− cells capableof proliferating. ER+Ki67+ cells that can proliferate and could be stimulated byestrogen to originate ER+ daughter cells or probably tumors. ER− cells mayconvert to ER+ cells during neoplastic transformation. Adapted from (110).
Journal of the National Cancer Institute Monographs No. 27, 2000 25

duce a growth factor that might, in turn, stimulate neighboringER�-negative cells to proliferate (Fig. 10) (110). In the samefashion, the small proportion of cells that are ER�-positive andcan proliferate could be the source of ER�-positive tumors. Thepossibility exists, as well, that the ER�-negative cells convert toER�-positive cells. The newly discovered ER� opens the pos-sibility that those cells traditionally considered to be negative forER might be positive for ER� (88–90,128–131). It has recentlybeen found that ER� is expressed during the immortalizationand transformation of ER-negative human breast epithelial cells(Fig. 11) (131), supporting the hypothesis of a conversion fromnegative to positive receptor cell. The functional role of ER�-mediated estrogen signaling pathways in the pathogenesis ofmalignant diseases is essentially unknown. ER�-mediatedmechanisms have been implicated in the increased PgR expres-sion in the dysplastic acini of the dorsolateral rat prostate inresponse to treatment with testosterone and estradiol-17� (132).ER� has been detected either alone or co-expressed with ER� in
both normal and cancerous human breast tissues and breast celllines (129–131). These observations suggest the possibility thatER� and ER� proteins interact with each other and discriminatebetween target sequences leading to differential responsivenessto estrogens. In addition, estrogen responses mediated by ER�and ER� may vary with different composition of their co-activators that transmit the effect of ER-ligand complex to thetranscription complex at the promoter of target genes (133).
Although the receptor-mediated mode of estrogen action isthe most widely studied and accepted, evidence is mounting thata membrane receptor, coupled to alternative second messengersignaling mechanisms, is operational and may stimulate the cas-cade of events leading to cell proliferation (134,135). Thisknowledge suggests that ER�-negative cells found in the humanbreast may respond to estrogens through this one pathway orother known or as yet undiscovered pathways. Definitively morestudies need to be done in this direction, especially when takinginto consideration that, in the normal breast, the proliferatingand steroid hormone receptor-positive cells are not the same.This finding has opened new possibilities for clarifying themechanisms through which estrogens stimulate cell proliferationfor initiating the cascade of events leading to cancer.
There is evidence as well that estrogen may not need toactivate its nuclear receptors to initiate or promote breast carci-nogenesis. The metabolic activation of estrogens can be medi-ated by various cytochrome P450 (CYP) complexes, generatingthrough this pathway reactive intermediates that elicit directgenotoxic effects by increasing mutation rates [(18–43), Chap-ters 4 and 5]. The two major endogenous estrogens, estradiol-17� (E2) and estrone (E1), are continuously interconverted by17�-hydroxylase. They are generally metabolized via two majorpathways: hydroxylation at C-16� position and at the C-2 or C-4positions (16,20,21). The carbon position of the estrogen mol-ecules to be hydroxylated differs among various tissues, andeach reaction is probably catalyzed by various CYP isoforms(136). For example, in MCF-7 human breast cancer cells, whichproduce catechol estrogens (CE) in culture (23,34), CYP IA1catalyzes hydroxylation of E2 at C-2, C-15�, and C-16�, CYPIA2 predominantly at C-2 (22), and a member of the CYP IBsubfamily at C-4 (24–26). The hydroxylated estrogens are CEthat have a very short half-life in vivo because of rapid inacti-vation via monomethylation at the 2-, 3- or 4-hydroxy (OH)groups catalyzed by blood-borne catechol-O-methyltransferase(COMT) [(20,27,28), Chapter 6]. Steady-state concentrations ofCE are determined by the CYP-mediated hydroxylations of es-trogens and COMT-catalyzed methylation of catechols (22). Anincrease in CE because of either elevated rates of synthesis orreduced rates of monomethylation will easily lead to their au-toxidation to semiquinones and subsequently quinones. Thesetwo compounds are electrophiles capable of covalently bindingto nucleophilic groups on DNA via a Michael addition and, thus,serve as the ultimate carcinogenic reactive intermediates in theperoxidatic activation of CE (29). This pathway still needs to bedemonstrated in normal breast epithelial cells.
Collectively, the alternative pathways described above offernew paradigms for determining the role of estrogens as endog-enous carcinogens and for clarifying whether they act as initia-tors or promoters of the neoplastic process. Many questionsremain to be answered, such as are there differences in the levelsof aromatases, sulfotransferases, CYP IA1, or CYP IB1 presentin the differentiated breast of parous women and those found in
Fig. 11. Expression of ER� or ER� in mortal, immortal, chemically transformed,and neoplastic human breast epithelial cells. (A) Representative picture of the gelfor ER� or ER� reactions. (B) Plots represent the average value from threeindependent RT-polymerase chain reaction reactions for each cell line. Signalintensities of the ER� or ER� products for each cell line were normalized usingglyceraldehyde phosphate dehydrogenase (GAPDH) products to produce arbi-trary units of relative abundance. Reproduced with permission by the Interna-tional Journal of Oncology (131).
26 Journal of the National Cancer Institute Monographs No. 27, 2000

the poorly differentiated gland of young nulliparous women? Bythe same token, are the oxidative adduct byproducts of the me-tabolism of estrogens to CEs, semiquinones, and quinones dif-ferent in various types of lesions found in the breast? These areimportant questions that need to be answered to fully understandthe role of estrogens in breast carcinogenesis.
THE IN VITRO MODEL OF BREAST CANCER
Culture of Human Breast Epithelial Cells In Vitro
Under in vitro conditions, HBECs have a life span compa-rable to that of adult human fibroblasts (30–64 doublings) whencultured in a medium supplemented with bovine pituitary extractand a standard concentration of calcium (1.05 mM) (53,54).However, when the concentration of calcium (Ca2+) in the me-dium is reduced to 0.04 mM (low Ca2+), the growth and popu-lation longevity of the cells are profoundly affected (56–59).HBECs cultured under low Ca2+ conditions divide for periods ofmore than 1000 days and for more than 50 generations of lineargrowth, without expressing terminal differentiation. Similar ef-fects have been observed in other cell types, such as WI-38(137), mouse epidermal (138–140), and rat esophageal epithelialcells (141). In addition, under these conditions HBECs maintaina normal diploid karyotype and human breast epithelial charac-teristics, including morphologic and ultrastructural features, aswell as formation of domes and duct-like structures in collagen.They also express specific keratin filaments and milk fat globulemembrane antigen (50,53,57). The behavior of HBECs in vitro,however, is in great part modulated by the biologic conditions ofthe breast from which they were obtained. Cells obtained fromlobules varying in their degree of differentiation show variationsin their in vitro growth properties (53,57,58,114). The number ofdoublings is higher in those HBECs derived from less differen-tiated breast tissues, i.e., the Lob 1 of young nulliparous women,which also exhibit a greater rate of cell proliferation (47,114).Furthermore, these HBECs are more susceptible to be trans-formed in vitro by etiologically important environmental chemi-cal carcinogens, a phenomenon that does not occur in cells ob-tained from the more differentiated Lob 3 of older and parouswomen (47,114). These observations indicate that both the invitro growth characteristics of HBECs and their susceptibility tobe transformed by chemical carcinogens are profoundly influ-enced by the degree of lobular differentiation and the rate of cellproliferation of the breast epithelium in vivo.
Immortalization of Human Breast Epithelial Cells
As previously indicated, normal HBECs maintained in vitrosenesce after 10–20 passages. Very few immortal breast epithe-lial cell lines of nonmalignant origin have been established(50,142–145). Among them, MCF-10, a HBEC line derivedfrom a primary culture of sample S#130, designated as MCF-10M, became immortalized after culture in low Ca2+ medium formore than 2 years. Two immortal cell lines arose spontaneously,MCF-10A and MCF-10F (50,145). The immortalization of thesecells was characterized by their continuous growth in conven-tional, 1.05 mM Ca2+ (also called high Ca2+ medium) withoutentering into senescence after more than 20 passages in vitro.Although the growth curves of MCF-10M, MCF-10A, andMCF-10F cells were similar when grown in low- and high-Ca++
media, MCF-10M cells were unable to continue growing inhigh-Ca++ medium after the 20th passage, whereas the immortalMCF-10A and MCF-10F cells grew indefinitely under highCa++ conditions. An important difference between MCF-10Mand its immortalized derivatives was their survival efficienciesin soft agar (Table 5), even though there were no significantdifferences in survival efficiencies among these cell types whenthey were seeded in agar-methocel (Table 5). None of the threecell types formed colonies in soft agar or in agar-methocel.Instead, the neoplastic breast epithelial cell line MCF-7 had asignificantly higher survival efficiency, and they formed colo-nies in both culture conditions (Table 5).
The immortalized cells MCF-10A and MCF-10F are bonafide HBECs, expressing epithelial sialomucins and keratins usu-ally reported in human breast (50,145). Ultrastructurally, thecells appear low cuboidal, with their lateral borders joined bynumerous desmosomes and the free surfaces are lined by shortmicrovilli. When plated on plastic surfaces, they grow in mono-layers forming domes. In a collagen matrix and under the controlof hormones and growth factors the cells form ductular struc-tures. They lack anchorage-independent growth and are not tu-morigenic in severe compromised immune deficient mice. Cy-togenetic analysis of MCF-10M cells showed a normal diploidkaryotype, whereas the immortalized MCF-10A and MCF-10Fcells had a near diploid karyotype. Genotypically, these cellswere demonstrated to be of human origin by DNA hybridizationwith probes for highly polymorphic sequences, such as the hy-pervariable single-copy gene PUM. The relationship of MCF-10A and MCF-10F cells to a specific donor was demonstrated byhybridization of identical size HaeIII fragments with a M13
Table 5. Growth characteristics of HBEC grown in soft agar and in agar-methocel*
Cells
Plating efficiency (%) Survival efficiency (%) Colony efficiency (%)
SA AM SA AM SA AM
MCF-10M 26.3 ± 8 31.1 ± 9 51.8 ± 21 93.9 ± 45 0.0 0.0MCF-10A 41.7 ± 1 44.5 ± 14 212.1 ± 20 62.9 ± 43 0.0 0.0MCF-10F 9.8 ± 5 21.0 ± 7 180.0 ± 96 91.9 ± 34 0.0 0.0MCF-7 42.8 ± 6 50.7 ± 14 468.4 ± 57 672.1 ± 53 3.6 ± 0.8 6.72 ± 1.2
*The mortal human breast epithelial cells (HBECs) MCF-10M, immortal MCF-10A and MCF-10F, and malignant MCF-7 cells (1 × 104/well) in 0.28% agar (softagar; SA) or 0.8% methylcellulose (agar-methocel; AM) were seeded in 24-well plates in which the flat polystyrene had been precoated with a solidified layer of0.9% agar in culture medium without supplements. The plates were incubated at 37 °C and the median replenished twice a week. Twenty-four hours after planting,all cultures were examined for cell aggregates that might bias the final results. Twenty-one days after planting, viable cells and colonies ranging in size from 50 to250 �m in diameter, as determined with a micrometer disc, were counted under an inverted phase contrast microscope. The results were expressed as platingefficiency (i.e., number of cells 24 hours after plating per 100 cells plated), survival efficiency (i.e., number of cells survived 21 days after plating per 100 cellsplated), and colony efficiency (i.e., number of colonies formed 21 days after plating per 100 cells plated).
Journal of the National Cancer Institute Monographs No. 27, 2000 27

probe that detects multiple hypervariable minisatellites (145).The immortal MCF-10 cells do not have amplification ofc-erbB2/HER-2-neu, erbA-1, int-2, int-1 or mutated c-Ha-ras-1gene and do not contain SV40 antigen. These characteristicsmake this cell line the most near to a normal HBEC line avail-able. Undoubtedly, the establishment of the immortal cell lineMCF-10F that arose spontaneously from the mortal diploidHBECs without viral or chemical intervention provides an im-portant tool for understanding how chemical carcinogens areable to induce transformation phenotypes. At the same time, italso provides the basis for understanding the differences in theprocesses that control senescence, immortalization, and malig-nancy.
Neoplastic Transformation of Human Breast EpithelialCells With Chemical Carcinogens
Exposure of primary cultures of HBECs to chemicals such asbenzo[a]pyrene (BP), N-methyl-N-nitrosourea (NMU), and7,12-dimethylbenz[a]anthracene (DMBA), all known to be car-cinogenic in animals (115), reveals that their susceptibility to betransformed is modulated by host factors and by specific char-acteristics of the cells. Treatment of MCF-10F cells with BP andDMBA has given rise to a series of chemical-carcinogen-initiated cell lines, each one expressing a well-defined trans-formed phenotype. The transformed cells express anchorage in-dependence, loss of ductule-like formation in collagen gel, andincrease in chemotactic and invasive properties, tumorigenicityin heterologous hosts (e.g., BP1E tumor cell lines) (47,49,146).Thus, the highest susceptibility of HBECs to be transformed hasbeen found to be associated with a high rate of cell proliferationand undifferentiated condition of the donor organ in vivo (114),immortalization prior to exposure to the carcinogens (47), andinherited predisposition to breast cancer, as revealed by our stud-ies of HBECs obtained from prophylactic mastectomies per-formed in women with familial history of breast cancer andgenetic predisposition, as evidenced by linkage analysis (147).
Primary cultures established from outgrowths of organoidsobtained from prophylactic mastectomies received two 24-hourtreatments with BP or DMBA in a week. After 30 days, the cellswere plated in agar-methocel for evaluation of anchorage-independent growth. By day 21 postplating, viable cells andcolonies, ranging in size from 50 to 250 mm in diameter, werecounted. Results were expressed as survival efficiency, colonyefficiency, and colony size. Survival efficiency (Fig. 12, A) andcolony efficiency (Fig. 12, B) in agar-methocel were calculatedas number of cells that survived per 100 cells plated and asnumber of colonies formed per 100 cells plated, respectively.The average size of the colonies was measured with a microm-eter disc under an inverted phase contrast microscope (Fig. 13).
BP and DMBA did not affect survival efficiency but signifi-cantly increased colony efficiency of treated cells. The coloniesformed by treated cells showed considerable anchorage-independent growth during the 21-day assay period (Fig. 12, Aand B) (147). Because the formation of colonies in agar is gen-erally construed as an indication of anchorage-independentgrowth, a hallmark of neoplastic cells, our results clearly indi-cated that HBECs from women with familial history of breastcancer manifested phenotypic changes indicative of initial stagesof neoplastic transformation in response to the treatment withcarcinogens (147). In contrast, the same treatments when appliedto HBECs of women without familial history of breast cancer
induced phenotypic alterations indicative of partial transforma-tion only, such as increased survival efficiency in agar methocel(Fig. 12, A and B), which is perceived to precede the acquisitionof anchorage independence.
Our observations led us to conclude that genetic predisposi-tion in women with familial history of breast cancer confersinherited susceptibility to environmental chemical carcinogens(147). However, induction of the full spectrum of transformedphenotypes by chemical carcinogens requires immortalization ofthe cells prior to exposure to the carcinogens. It is not knownhow estrogens or other endocrine disrupters influence the sus-ceptibility of the epithelial cells to undergo neoplastic transfor-mation, or whether these cells will express transformation phe-notypes when estrogen is metabolized or interacts with specificnuclear receptors.
Molecular Basis of Cell Immortalization and NeoplasticTransformation
Genomic Alterations
Genomic analysis of MCF-10F cells, using single-strand con-formational polymorphism technique revealed the presence of avariant band in one of the heterozygous alleles of TP53. On
Fig. 12. Survival efficiency (A) and colony efficiency (B) in agar-methocel ofchemical carcinogen-treated human breast epithelial cells (HBECs) from womenwith or without familial history of breast cancer (mean ± SD). Survival effi-ciencies were calculated as a percentage of the values of controls for each sampleto minimize derivations in responses among samples and to compare with thevalues of two previous studies on carcinogen-treated HBECs from women withno familial history of breast cancer. Reproduced with permission by the Societyfor In Vitro Biology (147).
28 Journal of the National Cancer Institute Monographs No. 27, 2000

DNA sequencing, a point mutation (TAG → TTA) of codon 254in exon 7 of this gene was detected (Table 6) (148). There wasa coexistence of a mutation of TP53 and instability of microsat-ellite DNA in the intragenic TP53 in these cells, manifested byadditional bands with slower mobility. We used polymerasechain reaction (PCR) amplification of microsatellite DNA lengthpolymorphism to detect allelic loss as well as microsatelliteinstability (MSI). These microsatellites are highly polymorphic,flanked by unique sequences that can serve as primers for PCRamplification. They have been proven to be useful markers forinvestigating multiple areas of MSI and loss of heterozygosity(LOH) and should be applicable to allelotyping as well as re-gional mapping of deletions in specific chromosomal regions.We have studied 466 markers that represent approximately 4.6%of the 10 000 microsatellite markers identified. MicrosatellitePCR analysis of MCF-10F cells did not reveal LOH with any ofthe markers analyzed in this study when compared with theirparental MCF-10M cells. However, MCF-10F cells did showMSI in chromosome 11 in the locus D11S392 and in chromo-some 17 in the loci represented by markers D17S849, TP53,D17S786, and D17S520 (149).
Neoplastic transformation of MCF-10F cells with chemicalcarcinogens (e.g., BP1 and BP1E cells) is associated with ge-netic instability on chromosomes 11 and 13, in addition to thatobserved on chromosome 17, which has been detected in asso-ciation with immortalization (150–153). MSI was found onchromosome 11 by using marker D11S912 and expressed as anallelic expansion in the BP1 and BP1E cells, representing anadditional location affected in the early stage of transformationof HBECs (Fig. 14) (151). On chromosome 13, MSI was foundin both BP1 and BP1E cells by using markers D13S260 andD13S289 at 13ql2–13 (flanking the BRCA2 locus) (Fig. 14)(150). In addition, we have also observed other genomic alter-ations on chromosomes 9 and 16 (154).
Activation of Telomerase in the Immortalized MCF-10F Cells
There is evidence that the repetitive TTAGGG sequenceslocated at the ends of human chromosomes (i.e., telomeres) mayact as a molecular mitotic clock (155). It is generally believedthat each successive genomic replication is accompanied bygradual shortening of 50–200 base pairs (bp) because of incom-plete replication of the 3� ends, and cellular senescence occurs
when telomeres reach a critically short length that replication ofthe genome cannot be maintained (156). The stabilization of thetelomeric sequences at the ends of chromosomes, which is re-quired for the continuous proliferation of immortal cells, in-volves the activation of the enzyme telomerase, which addsTTAGGG repeats to the 3� ends of chromosomes (157,158). Thegenetic nature of cellular senescence implicates activation oftelomerase as a key element of cell immortalization (144,158).Elevated levels of telomerase activities have been detected in anumber of immortal cell lines and human tumor tissues(159,160). We have observed telomerase activity in immortalMCF-10F but not in the mortal MCF-10M cells (161), suggest-ing that telomerase activation may play a role in the spontaneousimmortalization of MCF-10F cells.
Increase of H-Ferritin in MCF-10F Cells
In efforts to identify genes underlying the process of immor-talization, we have performed subtractive hybridization and dif-ferential display analysis between immortal MCF-10F and itsparental mortal MCF-10M cells. With the use of a 10F(+)/10M(−) subtractive complementary DNA (cDNA) library, weisolated more than 15 clones, one of which contains sequencesidentical to H-ferritin (162). We observed marked increases inmessenger RNA (mRNA) levels of ferritin H in immortal MCF-10F cell lines (particularly in late passages) (Fig. 15) and intissues exhibiting an increase in growth rate, such as ductalhyperplasia, carcinoma in situ, and invasive carcinoma (Fig. 16)(162). An increase in transcript signal was also confirmed by insitu hybridization of breast tissues containing lesions represen-tative of progressive stages of neoplastic evolution (Fig. 17).The levels of expression were undetectable in normal tissues;they increased progressively from moderately elevated in DH, astage of cell progression from normal to neoplasia that may bea histopathologic parallel of cell immortalization, greater expres-sion in carcinoma in situ, with the highest transcript levels beingdetected in infiltrating ductal carcinoma (Fig. 17).
Ferritin is a large protein found in most cell types of verte-brates, as well as of invertebrates, plants, and bacteria (163). Themain function of ferritin is iron storage. This function, in turn,can be subdivided into iron storage for other cells (specialized-cell ferritin), iron storage for intracellular needs (normal house-keeping ferritin), and iron storage for intracellular protection
Fig. 13. Representative colonies formed in agar-methocel by chemically transformed primary cultures of human breast epithelial cells obtained from women withfamilial history of breast cancer. The cells were treated with the chemical carcinogens benz[a]pyrene (BP) or 7,12-dimethylbenz[a]anthracene (DMBA) prior toplating (phase contrast photograph, ×508). Reproduced with permission by the Society for In Vitro Biology (147).
Journal of the National Cancer Institute Monographs No. 27, 2000 29

from iron overload (stress housekeeping ferritin) (163). Iron isrequired for DNA synthesis necessary for cell growth and mul-tiplication (164–166). It is also required for electron transportand for oxygen metabolism, generating harmful activated oxy-gen species capable of damaging DNA, lipids, and proteins(167). The iron-catalyzed conversion of H202 is a major route tothe synthesis of highly reactive OH radicals that inflict damageon the nucleotide bases of DNA, inducing mutations and in-creasing the risk of cancer (42,168).
Normally, the concentration of iron capable of catalyzingthese reactions is tightly controlled and regulated, and a criticalhomeostatic balance is achieved by the synthesis of ferritin(163,169). Many compounds, such as flavins and xanthine oxi-dase, are capable of reductively releasing iron from ferritin(170,171). Once released from ferritin, iron in the ferrous (Fe++)state is capable of participating in free-radical reactions (Fentonreactions) leading to oxidative damage (Fig. 18). Thus, a dis-ruption in normal iron homeostasis may lead to an increase in thelevel of reactive iron and to a corresponding increase in oxygenfree-radical generation and DNA damage (172). Oxidative stresshas also been implicated in metastasis, because it results in lossof cell adhesion, a prerequisite for cell detachment and subse-quent host tissue invasion (173,174).
Progression of invasive breast cancer to the metastatic state is
Fig. 15. Northern analysis of primary cultures of breast epithelial cells S#130,240, and 229; immortal MCF-10F cells; benz[a]pyrene-transformed cells BP1Eand BP1ET; dimethylbenz[a]anthracene-transformed S3 and D31 cells; and theneoplastic cell lines MCF-7, HBL-100, BT-20, and T-47D. An increased signalfor H-ferritin messenger RNA is observed in MCF-10F cells; a much higherintensity in BP1E, BP1ET, D3, and D3-1; and the highest signal intensity isobserved in the malignant cell lines MCF-7, HBL-100, BT-20, and T-47D.Reproduced with permission by Wiley-Liss, Inc., a subsidiary of John Wiley &Sons, Inc. (162).
Table 6. Comparison of the sequence of p53 exon 7 in MCF-10M and MCF-10F cells
Cells
Codon No.
253 254 255 256 257 258 259 260 261 262 263
MCF-10M*Antisense TGG TAG TAG TGT GAC CTT CTG AGG TCC agt cctSense ACC ATG ATG ACA CTG GAA GAC TCC AGG tca ggaAminoacid Thr Ileu Ileu Thr Leu Glu Asp Ser Ser
MCF-10F†Antisense TGG TTA GTA GTG TGA CCT TCT GAG GTC CAG TCCSense ACC AAT CAT CAC ACT GGA AGA CTC CAG GTC AGGAminoacid Thr Asn His His Thr Gly Arg Leu Gln Val Arg
*MCF-10M cells exhibit a wild-type sequence.†MCF-10F cells show a frame-shift mutation by insertion of a base at codon 254. Reprinted with permission from International Journal of Oncology (148).
Fig. 14. Microsatellite instability detected in chromosome 11 and 13 with markers D11S9129 (left panel), D13S260 (central panel), and D13S289 (right panel) inMCF-10M (p22), lane 1; MCF-10F (P130), lane 2; BP1 (p27, p52), lane 3; BP1E (p25), lane 4; BP1E (p30), lane 5, and BP1E (P60), lane 6.
Fig. 16. Northern analysis of total RNA from breast cancer tissue (M1 and M2),normal tissue from the same patient (B1 and B2), normal control breast tissue(N1 and N2), and tissue with ductal hyperplasia (H1 and H2). A high signalintensity is seen in the malignant tissue, very low levels are detected in normaltissue samples, and an increase in signal above normal levels is seen in tissueshowing ductal hyperplasia. Reproduced with permission by Wiley-Liss, Inc., asubsidiary of John Wiley & Sons, Inc. (162).
30 Journal of the National Cancer Institute Monographs No. 27, 2000

linked to OH radical-induced DNA damage (175–177). Thus,ferritin-dependent oxidative damage to DNA may be one of themechanisms contributing to immortalization of HBECs. An in-crease in ferritin H chain levels may provide iron necessary forthe clonal selection and uncontrolled growth of cells. It has beenshown that iron and its binding proteins participate in a varietyof reactions required for cell proliferation (56,178) and are criti-cal for the activity of the enzyme ribonucleotide reductase, arate-limiting enzyme in DNA synthesis (165,179). Ferritin hasbeen shown to have an immunosuppressive effect on host im-mune response in cancer patients (180,181). Placental isoferritin,an acidic form of ferritin, and its p43 super heavy chain have
been reported to be synthesized by breast cancer cells but areabsent in normal breast epithelium (182). Breast cancer-associated p43 induces alterations in the expression of cell-surface molecules in neoplastic cells, which in turn could havean effect on the modulation of the cells’ adhesive interactions(183). Cytokines, such as tumor necrosis factor, interleukin-1�,and the NF-�B family of transcription factors, specifically in-duce synthesis of ferritin H by selectively increasing ferritin Htranscription (Fig. 18) (183–185).
Our observations that the immortalization of HBECs wasassociated with an increased ferritin H chain gene transcriptionled us to postulate that this increase might have contributed to
Fig. 17. In situ hybridization (upper row) and Northern blot analysis of Ferritin H chain messenger RNA (lower row) in normal breast lobules (Normal Breast), DuctalHyperplasia, Ductal Carcinoma in situ, and Invasive Carcinoma. Tissue sections were counterstained with hematoxylin and photographed in dark field (finalmagnification ×100).
Fig. 18. The possible role of increased ferritin H chain gene in the neoplastic transformation of human breast epithelial cells. Adapted from (162).
Journal of the National Cancer Institute Monographs No. 27, 2000 31

the immortalization of HBEC; probably through one or more ofthe following mechanisms: a) providing a source of iron re-quired by rapidly dividing cells for clonal expansion, b) provid-ing iron capable of participating in free-radical reactions leadingto oxidative DNA damage and mutation, or c) affecting immunesurface antigens and thus providing immortal cells a growthadvantage by allowing them to escape immune surveillance (Fig.18). However, the possibility that ferritin H chain gene inductionmay be a consequence of the immortalized condition of the cells,rather than its cause, cannot be ruled out. In either instance, itmay prove to be a valuable marker of cell immortalization or anearly indicator of malignant transformation.
Reversion of Immortalized and Transformed Phenotypes
To investigate the functional role of genomic changes onchromosomes 11 and 17 that were detected in the immortalizedand transformed cells, single normal human fibroblast A9-derived chromosome 11 or 17, tagged with a neomycin-resistantgene, was transferred into 6 × 106 transformed BP1E cells. Sur-viving cells or clones of microcell hybrids from chromosome 11or 17 were designated BP1E-11neo or BP1E-17neo cells. A totalof 16 colonies was isolated from BP1E-11neo and BP1E-17neocells each. The transfer efficiency in BP1E cells was approxi-mately 2.6 × 10−6 cells (149). During a selection period of up to6 months, BP1E-17neo cells, and to a lesser degree BP1E-11neocells, exhibited altered cellular morphology and growth pattern,such as contact inhibition and cellular senescence (149). In ad-dition to the acquired ability to survive in the G-418 selectionmedium that indicates the active function of the neomycin-resistance gene tagged on the donor chromosome 11 or 17,the physical presence of these chromosomes was further con-firmed by dual-color fluorescence in situ hybridization (FISH)analysis. As shown in Fig. 19, A and B, the metaphases of theBPlE-11neo#145 cells were confirmed to contain an extra chro-mosome 11 that had a stronger signal with the painting probe(red). Anchorage-independent growth in agar-methocel gelwas reduced from 17% in control BP1E cells to 7% in theBP1E-11neo#145 cells, whereas BP1E-17neo D100 cells failed
to form any colony (100% reduction), reflecting a more potentsuppression of the BP1E cells by chromosome 17 than that bychromosome 11. These data indicated that the introduced chro-mosome 11 caused a partial growth inhibition, whereas chromo-some 17 produced a nearly complete growth suppression of theBP1E cells (149). Another phenotypic reversion induced by thechromosome transfer was the recovery of the ability of cells toform ductule-like structures in collagen gel, a property exhibitedby BP1E-17neo D100 cells, similar to that of MCF-10F cells,whereas BP1E cells grew in loosely arranged clusters or asisolated cells. These observations confirmed the reversion of thetransformed phenotype by chromosome 17 transfer.
Microsatellite analysis showed that the preexisting instabilityin the parental BP1E cells at loci D17S849 (17pl3.3), TP53(17p13.1), D17S786 (17pl3.1), and D17S520 (17pl2.0) wasreverted in BP1E-17neo D100 cells, which acquired an allelicpattern similar to that of the mortal MCF-10M cells. In con-trast, the instability of these markers was not restored in theBPlE-11neo #145 cells. These data indicated a specific effectassociated with transfer of chromosome 17. Surprisingly, noneof the corresponding donor alleles observed in the A9–17neocells could be detected in the BPlE-17neo D100 cells, suggestingthat other untested regions of the donor chromosome 17 mightbe the responsible ones for the phenotypic reversion and therestored microsatellite stability.
In summary, our data provide supportive evidence for thehypothesis that MSI within or near genes can confer instabilityto these genes and alter their expression or functions. However,further investigation is required for determining what is theirfunctional role in the initiation and progression of neoplasia.TP53 has been considered as the guardian of the genome byallowing cells to undergo DNA repair prior to entering a newcell cycle (186–188). The observation that introduction of anunaffected chromosome 17 can correct instability on the corre-sponding chromosome, including that of marker TP53, in addi-tion to the reversion of transformed phenotypes in the trans-formed BP1E cells, suggests that other important genes onchromosome 17 may control this process.
FUTURE PERSPECTIVES
In the paradigm described above, it is clear that if estrogensplay a role in the early stages of cell immortalization and trans-formation, this experimental system will allow us to demonstratesuch phenomena. The demonstration of the ability of the mam-mary epithelial cells to metabolize estradiol and/or to accumu-late “genotoxic” metabolites could profoundly influence our un-derstanding of the neoplastic transformation of the mammaryepithelium (189). Metabolic biotransformation of estradiol oc-curs in human mammary explant cultures composed of a mixtureof epithelial and stromal cells (190,191). Treatment of normalmouse mammary epithelial cells with the mutagenic polycyclichydrocarbon DMBA results in production of 16�-hydroxy-estrone. This predominant metabolite of estrogen increases un-scheduled DNA synthesis, cellular proliferation, and anchorage-independent growth, all phenomena indicative of preneoplastictransformation (192). Because normal HBECs are susceptibleto be transformed by environmental carcinogens that requiremetabolic activation (116,117) and many of the enzymes (e.g.,CYP IA1) that catalyze the oxidation of drugs, alkaloids, andenvironmental pollutants also catalyze the hydroxylation of es-trogens (136,193,194), we hypothesize that HBECs, regardless
Fig. 19. Dual-color fluorescence in situ hybridization (FISH) for the detection ofchromosome 11 in metaphases of BP1E-1neo #145 cells. (A) A representativefield of a metaphase spread showing a pair of host chromosome 11 (red stained)and a donor (partial) chromosome 11 (red stained with green signal). This clonecontained one extra donor chromosome 11, in addition to the pair of host chro-mosome 11. (B) Representative field of a metaphase spread showing a pair ofchromosome 11 (red stained) in BP1E cells.
32 Journal of the National Cancer Institute Monographs No. 27, 2000

of their ER status, are capable of metabolic activation of estro-gen and, thus, susceptible to estrogen-induced carcinogenesis. Itis possible that the rates of metabolic activation of estrogenmight vary among HBECs with different carcinogenic suscep-tibility. We postulate that the susceptibility of cells to be trans-formed by estrogens would depend on their rate of proliferation,genetic predisposition, and mortal status of the cells, rather thantheir ER contents, similar to what has been observed with chemi-cal carcinogens (47,114,146,147). If these assumptions are true,the efficiency and extent of estrogen-induced neoplastic trans-formation will be high in immortalized MCF-10F cells, moder-ate in those HBECs derived from breasts of women with familyhistory of breast cancer, and low in cells derived from the breastof parous women and of those women with no family history ofbreast cancer. The independence of ER contents in estrogen-induced carcinogenesis would support the postulate that meta-bolic activation of estrogen is involved in the neoplastic trans-formation of susceptible HBECs. Alternatively, estrogen or itsmetabolites may not initiate neoplastic transformation, but theymay act by promoting neoplastic progression in chemicallytransformed HBECs by increasing the genomic instability of thecells. In essence, estrogen, on metabolic activation, might serveas an initiator and/or as a promoter of carcinogenesis in thehuman breast. However, the metabolism of estrogen in normalHBECs and the carcinogenic potential of estrogen and its me-tabolites in the human breast are virtually unknown.
REFERENCES
(1) Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics, 1999. CACancer J Clin 1999;49:8–31.
(2) Mettlin C. Global breast cancer mortality statistics. CA Cancer J Clin1999;49:138–44.
(3) Pike MC, Spicer DV, Dahmoush L, Press MF. Estrogens, progestogens,normal breast cell proliferation, and breast cancer risk. Epidemiol Rev1993;15:17–35.
(4) Bernstein L, Ross RK. Endogenous hormones and breast cancer risk.Epidemiol Rev 1993;15:48–65.
(5) Hu, YF, Russo IH, Russo J. Prevention of human breast cancer. J Wom-en’s Cancer. In press 2000.
(6) Henderson BE, Ross R, Bernstein L. Estrogens as a cause of humancancer: the Richard and Hinda Rosenthal Foundation award lecture. Can-cer Res 1988;48:246–53.
(7) Greenwald P, Barlow JJ, Nasca PC, Burnett WS. Vaginal cancer aftermaternal treatment with synthetic estrogens. N Engl J Med 1971;285:390–2.
(8) Nissen ED, Kent DR. Liver tumours and oral contraceptives. Obstet Gy-necol 1975;46:460–7.
(9) Herbst AL. Clear cell adenocarcinoma and current status of DES-exposedfemales. Cancer 1981;48(2 suppl):484–8.
(10) Shaw RW. Adverse long-term effects of oral contraceptives: a review. BrJ Obstet Gynaecol 1987;94:889–94.
(11) Chilvers C, Mant D, Pike MC. Cervical adenocarcinoma and oral contra-ceptives. Br Med J 1987;295:1446–7.
(12) Beral V, Hannaford P, Kay C. Oral contraceptive use and malignancies ofthe genital tract. Results from the Royal College of General Practitioners’Oral Contraceptive Study. Lancet 1988;2:1331–5.
(13) Yan ZJ, Roy D. Mutations in DNA polymerase � mRNA of stilbeneestrogen-induced kidney tumors in Syrian hamster. Biochem Mol Biol Int1995;37:175–83.
(14) Zhu BT, Liehr JG. Quercetin increases the severity of estradiol-inducedtumorigenesis in hamster kidney. Toxicol Appl Pharmacol 1994;125:149–58.
(15) Tsutsui T, Barrett JC. Neoplastic transformation of cultured mammaliancells by estrogens and estrogenlike chemicals. Environ Health Perspect1997;105(suppl 3):619–24.
(16) Adlercreutz H, Gorbach SL, Goldin BR, Woods MN, Dwyer JT, Ha-
malainen E. Estrogen metabolism and excretion in Oriental and Caucasianwomen. J Natl Cancer Inst 1994;86:1076–82.
(17) Nandi S, Guzman RC, Yang J. Hormones and mammary carcinogenesis inmice rats and humans: a unifying hypothesis. Proc Natl Acad Sci U S A1995;92:3650–7.
(18) Liehr JG, Ulubelen AA, Strobel HW. Cytochrome P-450-mediated redoxcycling of estrogens. J Biol Chem 1986;261:16865–70.
(19) Roy D, Liehr JG. Temporary decrease in renal quinone and reductaseactivity induced by chronic administration of estradiol to male Syrianhamsters. Increased superoxide formation by redox cycling of estrogen. JBiol Chem 1988;263:3646–51.
(20) Ball P, Knuppen R. Catecholestrogens (2- and 4-hydroxyoestrogens):chemistry, biosynthesis, metabolism, occurrence and physiological sig-nificance. Acta Endocr Suppl (Copenh) 1980;232:1–127.
(21) Zhu BT, Bui QD, Weisz J, Liehr JG. Conversion of estrone to 2- and4-hydroxyestrone by hamster kidney and liver microsomes: implicationsfor the mechanism of estrogen-induced carcinogenesis. Endocrinology1994;135:1772–9.
(22) Ashburn SP, Han X, Liehr JG. Microsomal hydroxylation of 2- and4-fluoroestradiol to catechol metabolites and their conversion to methylethers: catechol estrogens as possible mediators of hormonal carcinogen-esis. Mol Pharmacol 1993;43:534–41.
(23) Brueggemeier RW, Katlic NE, Palmer CW Jr, Stevens JM. Catecholestrogen formation in MCF-7 cell culture and effects of bromoestrogeninhibitors. Mol Cell Endocrinol 1989;64:161–7.
(24) Niwa T, Bradlow HL, Fishman J, Swaneck GE. Determination of estradiol2- and 16-alpha-hydroxylase activities in MCF-7 human breast cancercells in culture using radiometric analysis. J Steroid Biochem 1989;33:311–4.
(25) Spink DC, Hayes CL, Young NR, Christou M, Sutter TR, Jefcoat CR, etal. The effects of 2,3,7,8-tetrachlorodibenzo-�-dioxin on estrogen metabo-lism in MCF-7 breast cancer cells: evidence for induction of a novel17�-estradiol 4-hydroxylase. J Steroid Biochem Mol Biol 1994;51:251–8.
(26) Liehr JG, Ricci MJ. 4-Hydroxylation of estrogens as a marker of humanmammary tumors. Proc Natl Acad Sci U S A 1996;93:3294–6.
(27) Knuppen R, Ball P, Emons G. Importance of A-ring substitution of es-trogens for the physiology and pharmacology of reproduction. J SteroidBiochem 1986;24:193–8.
(28) Creveling CR, Inoue K. Catechol-O-methyltransferase: factors relating tothe carcinogenic potential of catecholestrogens. Polycyclic AromatCompd 1994;6:253–9.
(29) Dwivedy I, Devanesan P, Cremonesi P, Rogan E, Cavalieri E. Synthesisand characterization of estrogen 2,3- and 3,4-quinones. Comparison ofDNA adducts formed by the quinones versus horseradish peroxidase-activated catechol estrogens. Chem Res Toxicol 1992;5:828–33.
(30) Stalford AC, Maggs JL, Gilchrist TL, Park BK. Catecholestrogens asmediators of carcinogenesis: correlation of aromatic hydroxylation of es-tradiol and its fluorinated analogs with tumor induction in Syrian ham-sters. Mol Pharmacol 1994;45:1259–67.
(31) Weisz J, Bui QD, Roy D, Liehr JG. Elevated 4-hydroxylation of estradiolby hamster kidney microsomes: a potential pathway of metabolic activa-tion of estrogens. Endocrinology 1992;131:655–61.
(32) Bunyagidj C, McLachlan JA. Catechol estrogen formation in mouseuterus. J Steroid Biochem 1988;31:795–801.
(33) Paria BC, Chakraborty C, Dey SK. Catechol estrogen formation in themouse uterus and its role in implantation. Mol Cell Endocrinol 1990;69:25–32.
(34) Bui Q, Weisz J. Identification of microsomal, organic hydroperoxide-dependent catechol estrogen formation: comparison with NADPH depen-dent mechanism. Pharmacology 1988;36:356–64.
(35) Zhu BT, Liehr JG. Inhibition of the catechol-O-methyltransferase-catalyzed O-methylation of 2- and 4-hydroxyestradiol by catecholamines:implications for the mechanism of estrogen-induced carcinogenesis. ArchBiochem Biophys 1993;304:248–56.
(36) Zhu BT, Liehr JG. Inhibition of catechol O-methyltransferase-catalyzedO-methylation of 2- and 4-hydroxyestradiol by quercetin. Possible role inestradiol-induced tumorigenesis. J Biol Chem 1996;271:1357–63.
(37) Bradlow HL, Fishman J, Telang NT, Osborne MP. Re: Estrogen metabo-lism and excretion in Oriental and Caucasian women [letter]. J Natl Can-cer Inst 1994;86:1643–5.
Journal of the National Cancer Institute Monographs No. 27, 2000 33

(38) Schneider J, Kinne D, Fracchia A, Pierce V, Anderson KE, Bradlow HL,et al. Abnormal oxidative metabolism of estradiol in women with breastcancer. Proc Natl Acad Sci U S A 1982;79:3047–51.
(39) Bradlow HL, Hershcopf J, Martucci C, Fishman J. 16�-hydroxylation ofestradiol: a possible risk marker for breast cancer. Ann N Y Acad Sci1986;464:138–51.
(40) Osborne MP, Bradlow HL, Wong GY, Telang NT. Upregulation of es-tradiol C-16�-hydroxylation in human breast tissue: a potential biomarkerof human breast cancer risk. J Natl Cancer Inst 1993;85:1917–20.
(41) Malins DC, Haimanot R. Major alterations in the nucleotide structure ofDNA in cancer of the female breast. Cancer Res 1991;51:5430–2.
(42) Malins DC, Holmes EH, Polissar NL, Gunselman SJ. The etiology ofbreast cancer. Characteristic alteration in hydroxyl radical-induced DNAbase lesions during oncogenesis with potential for evaluating incidencerisk. Cancer 1993;71:3036–43.
(43) Sipe HJ Jr, Jordan SJ, Hanna PM, Mason RP. The metabolism of 17�-estradiol by lactoperoxidase: a possible source of oxidative stress in breastcancer. Carcinogenesis 1994;15:2637–43.
(44) Black DM. The genetics of breast cancer. Eur J Cancer 1994;30A:1957–61.(45) Van de Vijver MJ. Molecular genetic changes in breast cancer. In: Wein-
berg RA, editor. Oncogenes and the molecular origins of cancer. ColdSpring Harbor (NY): Cold Spring Harbor Press; 1993. p. 25–6.
(46) Murray AW, Edwards EM, Hii CS. Tumor promotion: biology and mo-lecular mechanisms. In: Cooper CS, Grove PL, editors. Chemical carci-nogenesis and mutagenesis. Berlin (Germany): Springer Verlag; 1990. p.135–49.
(47) Russo J, Calaf G, Russo IH. A critical approach to the malignant trans-formation of human breast epithelial cells with chemical carcinogens. CritRev Oncog 1993;4:403–17.
(48) Russo J, Barnabas N, Zhang PL, Adesina K. Molecular basis of breast celltransformation. Radiat Oncol Investig 1996;3:424–9.
(49) Russo J, Yang X, Hu YF, Bove BA, Huang Y, Silva ID, et al. Biologicaland molecular basis of human breast cancer. Front Biosci 1998;3:D944–60.
(50) Tait L, Soule H, Russo J. Ultrastructural and immunocytochemical char-acterization of an immortalized human breast epithelial cell line, MCF-10.Cancer Res 1990;50:6087–94.
(51) Russo J, Russo IH. A comprehensive approach to mammary carcinogen-esis. Proc Int Assoc Breast Cancer Res 1989;1:5.
(52) Russo J, Russo IH. Role of differentiation on transformation on humanbreast epithelial cells. In: Medina D, Kidwell W, Heppner G, Anderson E,editors. Cellular and molecular biology of mammary cancer. New York(NY): Plenum Publishing; 1987. p. 399–417.
(53) Russo J, Mills MJ, Moussalli MJ, Russo IH. Influence of human breastdevelopment on the growth properties of primary cultures. In Vitro CellDevelop Biol 1989;25:643–9.
(54) Ham RG, McKeehan WL. Development of improved media and cultureconditions for clonal growth of normal diploid cells. In Vitro 1978;14:11–22.
(55) Hammond SL, Ham RG, Stampfer MR. Serum-free growth of humanmammary epithelial cells: rapid clonal growth in defined medium andextended serial passage with pituitary extract. Proc Natl Acad Sci U S A1984;81:5435–9.
(56) McGrath CM, Soule HD. Calcium regulation of normal human mammaryepithelial cell growth in culture. In Vitro 1984;20:652–62.
(57) Mills MJ, Mousalli MJ, Russo J. DNA-labeling index and in vitro growthof mammary epithelium are modulated by the stage of gland development.Proceedings of the International Association of Breast Cancer Research;1987; Miami.
(58) Mousalli MJ, Mills MJ, Russo J. Influence of mammary gland develop-ment on its epithelium’s growth potential in tissue culture. Proceedings ofthe International Association of Breast Cancer Research; 1987; Miami.
(59) Soule HD, McGrath CM. A simplified method for passage and long-termgrowth of human mammary epithelial cells. In Vitro Cell Dev Biol 1986;22:6–12.
(60) Briand P, Peterson OW, Van Deurs B. A new diploid nontumorigenichuman breast epithelial cell line isolated and propagated in chemicallydefined medium. In Vitro Cell Dev Biol 1987;23:181–8.
(61) Gaffney EV. A cell line (HBL-100) established from human breast milk.Cell Tissue Res 1982;227:563–8.
(62) Steuer AF, Rhim JS, Hentosh PM, Ting RC. Survival of human cells inthe aggregate form: potential index of in vitro cell transformation. J NatlCancer Inst 1977;58:917–21.
(63) Russo J, Russo IH. Development of human mammary gland. In: NevilleMC, Daniel CW, editors. The mammary gland development regulationand function. New York (NY): Plenum Publishing; 1987. p. 67–93.
(64) Tanner JM. The development of the reproductive system. In: Tanner JM,editor. Growth at adolescence with a general consideration of the effect ofhereditary and environmental factors upon growth and maturation frombirth to maturity. Oxford (UK): Blackwell Scientific; 1962. p. 28–39.
(65) Vorherr H. Development of the female breast. In: Vorherr H, editor. Thebreast: morphology, physiology and lactation. New York (NY): AcademicPress; 1974. p. 1–18.
(66) Dabelow A. die Milchdruse. In: Bargmann W, editor. Handbuch der mik-roskopishen anatomic des menschen. Vol 3, Part 3 haut and sinnes organs.Berlin (Germany): Springer-Verlag; 1957. p. 277–485.
(67) Russo J, Tay LK, Russo IH. Differentiation of the mammary gland andsusceptibility to carcinogenesis. Breast Cancer Res Treat 1982;2:5–73.
(68) Russo J, Rivera R, Russo IH. Influence of age and parity on the devel-opment of the human breast. Breast Cancer Res Treat 1992;23:211–8.
(69) Edwards RG, Howles CM, Macnamee C. Clinical endocrinology of re-production. In: Baulieu EE, Kelly PA, editors. Hormones: from moleculesto disease. New York (NY): Chapman and Hall; 1990. p. 457–76.
(70) Russo IH, Russo J. Mammary gland neoplasia in long-term rodent studies.Environ Health Perspect 1996;104:938–67.
(71) Russo J, Russo IH. Role of hormones in human breast development: themenopausal breast. In: Progress in the management of menopause. Lon-don (UK): Parthenon Publishing; 1997. p. 1–10.
(72) Russo IH, Russo J. Role of hormones in cancer initiation and progression.J Mammary Gland Biol Neoplasia 1998;3:49–61.
(73) Russo J, Russo IH. Role of differentiation in the pathogenesis and pre-vention of breast cancer. Endocr Related Cancer 1997;4:7–21.
(74) Calaf G, Alvarado ME, Bonney GE, Amfoh KK, Russo J. Influence oflobular development on breast epithelial cell proliferation and steroidhormone receptor content. Int J Oncol 1995;7:1285–8.
(75) Lippman ME, Dickson RB, Gelmann EP, Rosen N, Knabbe C, Bates S, etal. Growth regulation of human breast carcinoma occurs through regulatedgrowth factor secretion. J Cell Biochem 1987;35:1–16.
(76) Meyer JS. Cell proliferation in normal human breast ducts fibroadenomasand other ductal hyperplasias measured by nuclear labeling with tritiatedthymidine. Effects of menstrual phase, age, and oral contraceptive hor-mones. Hum Pathol 1977;8:67–81.
(77) Masters JR, Drife JO, Scarisbrick JJ. Cyclic variations of DNA synthesisin human breast epithelium. J Natl Cancer Inst 1977;58:1263–5.
(78) Ferguson DJ, Anderson TJ. Morphological evaluation of cell turnover inrelation to the menstrual cycle in the “resting” human breast. Br J Cancer1981;44:177–81.
(79) Anderson TJ, Ferguson DJ, Raab GM. Cell turnover in the “resting”human breast: influence of parity, contraceptive pill, age and laterality. BrJ Cancer 1982;46:376–82.
(80) Russo J, Russo IH. Estrogens and cell proliferation in the human breast.J Cardiovasc Pharmacol 1996;28 Suppl 5:19–23.
(81) Kumar V, Green S, Stack G, Berry M, Jin JR, Chambon P. Functionaldomains of the human estrogen receptor. Cell 1987;51:941–51.
(82) King RJ. Effects of steroid hormones and related compounds on genetranscription. Clin Endocrinol (Oxf) 1992;36:1–14.
(83) Huseby RA, Maloney TM, McGrath CM. Evidence for a direct growth-stimulating effect of estradiol on human MCF-7 cells in vitro. Cancer Res1984;44:2654–9.
(84) Huff KK, Knabbe C, Lindsey R, Kaufman D, Bronzert D, Lippman ME,et al. Multihormonal regulation of insulin-like growth factor-I-related pro-tein in MCF-7 human breast cancer cells. Mol Endocrinol 1988;2:200–8.
(85) Dickson RB, Huff KK, Spencer EM, Lippman ME. Induction of epider-mal growth factor-related polypeptides by 17�-estradiol in MCF-7 humanbreast cancer cells. Endocrinology 1986;118:138–42.
(86) Soto AM, Sonnenschein C. Cell proliferation of estrogen-sensitive cells:the case for negative control. Endocr Rev 1987;8:44–52.
(87) Tsai MJ, O’Malley BW. Molecular mechanisms of steroid/thyroid recep-tor superfamily members. Annu Rev Biochem 1994;63:451–86.
(88) Kuiper GG, Enmark E, Pelto-Huikko M, Nilsson S, Gustaffson JA. Clon-
34 Journal of the National Cancer Institute Monographs No. 27, 2000

ing of a novel receptor expressed in rat prostate and ovary. Proc Natl AcadSci U S A 1996;93:5925–30.
(89) Tremblay GB, Tremblay A, Copeland NG, Gilbert DJ, Jenkins NA, La-brie F, et al. Cloning, chromosomal localization, and functional analysisof the murine estrogen receptor �. Mol Endocrinol 1997;11:353–65.
(90) Mosselman S, Polman J, Dijkema R. ER �: identification and character-ization of a novel human estrogen receptor. FEBS Lett 1996;392:49–53.
(91) Katzenellenbogen BS. Dynamics of steroid hormone receptor action.Annu Rev Physiol 1980;42:17–35.
(92) Topper J, Freedman C. Multiple hormone interactions in the developmen-tal biology of the mammary gland. Physiol Rev 1980;60:1049–60.
(93) Dickson RB, Lippman ME. Cellular and molecular biology: In: LippmanME, Dickson RB, editors. Breast cancer. Boston (MA): Kluwer AcademicPublishers; 1988. p. 119–65.
(94) Jordan VC. Tamoxifen: the herald of a new era of preventive therapeutics.J Natl Cancer Inst 1997;89:747–9.
(95) Kuiper GG, Carlsson B, Grandien K, Enmark E, Haggblad J, Nilsson S,et al. Comparison of the ligand binding specificity and transcript tissuedistribution of estrogen receptors � and �. Endocrinology 1997;138:863–70.
(96) Cowley SM, Hoare S, Mosselman S, Parker MG. Estrogen receptors �
and � form heterodimers on DNA. J Biol Chem 1997;272:19858–62.(97) Kuiper GG, Gustafsson JA. The novel estrogen receptor-� subtype: po-
tential role in the cell- and promotor-specific actions of estrogens andanti-estrogens. FEBS Lett 1997;410:87–90.
(98) Pace P, Taylor J, Suntharalingam S, Coombes RC, Ali S. Human estrogenreceptor � binds DNA in a manner similar to and dimerizes with estrogenreceptor �. J Biol Chem 1997;272:25832–8.
(99) Ogawa S, Inoue S, Watanabe T, Hiroi H, Orimo A, Hosoi T, et al. Thecomplete primary structure of human estrogen receptor � (hER�) and itsheterodimerization with ER � in vivo and in vitro. Biochem Biophys ResCommun 1998;243:122–6.
(100) Paech K, Webb P, Kuiper GG, Nilsson S, Gustafsson J, Kushner PJ, et al.Differential ligand activation of estrogen receptors ER� and ER� at AP1sites. Science 1997;277:1508–10.
(101) Couse JF, Korach KS. Estrogen receptor null mice: what have we learnedand where will they lead us? Endocr Rev 1999;20:358–417.
(102) Going JJ, Anderson TJ, Battersby S, MacIntyre CC. Proliferative andsecretory activity in human breast during natural and artificial menstrualcycles. Am J Pathol 1988;130:193–204.
(103) Potten CS, Watson RJ, Williams GT, Tickle S, Roberts SA, Harris M, etal. The effect of age and menstrual cycle upon proliferative activity of thenormal human breast. Br J Cancer 1988;58:163–70.
(104) Clarke RB, Howell A, Potten CS, Anderson E. Dissociation betweensteroid receptor expression and cell proliferation in the human breast.Cancer Res 1997;57:4987–91.
(105) Laidlaw IJ, Clarke RB, Howell A, Owen AW, Potten CS, Anderson E.The proliferation of normal human breast tissue implanted in athymicnude mice is stimulated by estrogen but not progesterone. Endocrinology1995;136:164–71.
(106) Clarke RB, Howell A, Anderson E. Estrogen sensitivity of normal humanbreast tissue in vivo and implanted into athymic nude mice: analysis of therelationship between estrogen-induced proliferation and progesterone re-ceptor expression. Breast Cancer Res Treat 1997;45:121–33.
(107) Goodman HM, editor. Basic medical endocrinology. 2nd ed. New York(NY): Raven Press; 1994. p. 288–90.
(108) Russo J, Russo IH. Influence of differentiation and cell kinetics on thesusceptibility of the rat mammary gland to carcinogenesis. Cancer Res1980;40(8 Pt 1):2677–87.
(109) Russo J, Russo IH. Biology of disease. Biological and molecular bases ofmammary carcinogenesis. Lab Invest 1987;57:112–37.
(110) Russo J, Ao X, Grill C, Russo IH. Pattern of distribution of cells positivefor estrogen receptor � and progesterone receptor in relation to prolifer-ating cells in the mammary gland. Breast Cancer Res Treat 1999;53:217–27.
(111) Clarke R, Dickson RB, Lippman ME. Hormonal aspects of breast cancer.Growth factors, drugs and stromal interactions. Crit Rev Oncol Hematol1992;12:1–23.
(112) Knabbe C, Lippman ME, Wakefield LM, Flanders KC, Kasid A, DerynckR, et al. Evidence that transforming growth factor-� is a hormonally
regulated negative growth factor in human breast cancer cells. Cell 1987;48:417–28.
(113) Dickson RB, Lippman ME. Growth factors in breast cancer. Endocr Rev1995;16:559–89.
(114) Russo J, Reina D, Frederick J, Russo IH. Expression of phenotypicalchanges by human breast epithelial cells treated with carcinogens in vitro.Cancer Res 1988;48:2837–57.
(115) Russo J, Gusterson BA, Rogers A, Russo IH, Wellings SR, van ZwietenMJ. Comparative study of human and rat mammary tumorigenesis. LabInvest 1990;62:244–78.
(116) Tay LK, Russo J. Formation and removal of 7,12-dimethylbenz[a]-anthracene–nucleic acid adducts in rat mammary epithelial cells withdifferent susceptibility to carcinogenesis. Carcinogenesis 1981;2:1327–33.
(117) Tay LK, Russo J. In vitro metabolism of 7,12-dimethylbenz[a]anthracenein mammary epithelial cells from rats with different susceptibilities tocarcinogenesis. Carcinogenesis 1983;4:733–8.
(118) Russo J, Russo IH. Differentiation and breast cancer development. In:Heppner G, Bittar ED, editors. Advances in oncobiology. Greenwich(CT): JAI Press; 1998. p. 1–10.
(119) Wellings SR, Jensen HM, Marcum RG. An atlas of subgross pathology ofthe human breast with special reference to possible precancerous lesions.J Natl Cancer Inst 1975;55:231–73.
(120) Russo J, Russo IH. Development pattern of human breast and suscepti-bility to carcinogenesis. Eur J Cancer Prev 1993;2(suppl 3):85–100.
(121) Russo J, Russo IH. Toward a physiological approach to breast cancerprevention. Cancer Epidemiol Biomarker Prev 1994;3:353–64.
(122) Russo J, Romero AL, Russo IH. Architectural pattern of the normal andcancerous breast under the influence of parity. Cancer Epidemiol Biomar-ker Prev 1994;3:219–24.
(123) Khan SA, Rogers MA, Khurana KK, Meguid MM, Numann PJ. Estrogenreceptor expression in benign breast epithelium and breast cancer risk. JNatl Cancer Inst 1998;90:37–41.
(124) Molino A, Micciolo R, Turazza M, Bonetti F, Piubello Q, Corgnati A, etal. Prognostic significance of estrogen receptors in 405 primary breastcancers: a comparison of immunohistochemical and biochemical methods.Breast Cancer Res Treat 1997;45:241–9.
(125) Habel LA, Stanford JL. Hormone receptors and breast cancer. EpidemiolRev 1993;15:209–19.
(126) Harlan LC, Coates RJ, Block G, Greenberg RS, Ershow A, Forman M, etal. Estrogen receptor status and dietary intakes in breast cancer patients.Epidemiology 1993;4:25–31.
(127) Moolgavkar SH, Day NE, Stevens RG. Two-stage model for carcinogen-esis: epidemiology of breast cancer in females. J Natl Cancer Inst 1980;65:559–69.
(128) Vladusic EA, Hornby AE, Guerra-Vladusic FK, Lupu R. Expression ofER� in breast cancer cells: does it play an important role? Proc Am AssocCancer Res 1997;38:297a.
(129) Dotzlaw H, Leygue E, Watson PH, Murphy LC. Expression of estrogenreceptor-� in human breast tumors. J Clin Endocrinol Metab 1997;82:2371–4.
(130) Vladusic EA, Hornby AE, Guerra-Vladusic FK, Lupu R. Expression ofestrogen receptor � messenger RNA variant in breast cancer. Cancer Res1998;58:210–4.
(131) Hu YF, Lau KM, Ho SM, Russo J. Increased expression of estrogenreceptor � in chemically transformed human breast epithelial cells. Int JOncol 1998;12:1225–8.
(132) Lau KM, Leav I, Ho SM. Rat estrogen receptor-� and -�, and progester-one receptor mRNA expression in various prostatic lobes and microdis-sected normal and dysplastic epithelial tissues of the Nobel rats. Endo-crinology 1998;139:424–7.
(133) Watanabe T, Inoue S, Ogawa S, Ishii Y, Hiroi H, Ikeda K, et al. Agonisticeffect of tamoxifen is dependent on cell type, ERE-promotor context, andestrogen receptor subtype: functional difference between estrogen recep-tors � and �. Biochem Biophys Res Commun 1997;236:140–5.
(134) Aronica SM, Kraus WL, Katzenellenbogen BS. Estrogen action via thecAMP signaling pathway: stimulation of adenylate cyclase and cAMP-regulated gene transcription. Proc Natl Acad Sci U S A 1994;91:8517–21.
(135) Pappas TC, Gametchu B, Watson CS. Membrane estrogen receptors iden-tified by multiple antibody labeling and impeded-ligand binding. FASEBJ 1995;9:404–10.
Journal of the National Cancer Institute Monographs No. 27, 2000 35

(136) Spink DC, Eugster HP, Lincoln DW 2nd, Schuetz JD, Schuetz EG,Johnson JA, et al. 17�-estradiol hydroxylation catalyzed by human cyto-chrome P450 IAl: a comparison of the activities induced by 2,3,7,8-tetrachlorodibenzo-�-dioxin in MCF-7 cells with those from heterologousexpression of the cDNA. Arch Biochem Biophys 1992;293:342–8.
(137) Cristofalo VJ, Wallace JM, Rosner BA. Glucocorticoid enhancement ofproliferative activity in WI-38 cells. In: Sata SD, Ross R, editors. Hor-mones and cell culture book B. Cold Spring Harbor (NY): Cold SpringHarbor Laboratory; 1979. p. 875–87.
(138) Hennings H, Michael D, Cheng C, Steinert P, Holbrook K, Yuspa SH.Calcium regulation of growth and differentiation of mouse epidermal cellsin culture. Cell 1980;19:245–54.
(139) Hennings H, Holbrook K. Extracellular calcium regulates growth andterminal differentiation of cultured mouse epidermal cells. In: BoyntonAL, McKeehan WL, Whitfield JF, editors. Symposium on ions, cell pro-liferation, and cancer. New York: Academic Press; 1982. p. 497–514.
(140) Hennings H, Kruszewski FH, Yuspa SH, Tucker RW. Intracellular cal-cium alterations in response to increased external calcium in normal andneoplastic keratinocytes. Carcinogenesis 1989;10:777–80.
(141) Stoner GD, Babcock MS. Influence of growth factors on proliferation ofnormal and chemically transformed rat esophageal epithelial cells. ProcAm Assoc Cancer Res 1982;23:42a.
(142) Huschtscha LI, Holiday R. Limited and unlimited growth of SV40-transformed cells from human diploid MRC-5 fibroblasts. J Cell Sci 1983;63:77–99.
(143) Linder S, Marshall H. Immortalization of primary cells by DNA tumorviruses. Exp Cell Res 1990;191:1–7.
(144) Shay JW, Wright WE, Werbin H. Defining the molecular mechanisms ofhuman cell immortalization. Biochim Biophys Acta 1991;1072:1–7.
(145) Soule HD, Maloney TM, Wolman SR, Peterson WD Jr, Brenz R, Mc-Grath CM, et al. Isolation and characterization of a spontaneously im-mortalized human breast epithelial cell line, MCF-10. Cancer Res 1990;50:6075–86.
(146) Calaf G, Russo J. Transformation of human breast epithelial cells bychemical carcinogens. Carcinogenesis 1993;14:483–92.
(147) Hu YF, Russo IH, Zalipsky U, Lynch HT, Russo J. Environmental chemi-cal carcinogens induce transformation of breast epithelial cells fromwomen with familial history of breast cancer. In Vitro Cell Dev Biol Anim1997;33:495–8.
(148) Barnabas N, Moraes R, Calaf G, Estrada S, Russo J. Role of p53 inMCF-10F cell immortalization and chemically-induced neoplastic trans-formation. Int J Oncol 1995;7:1289–96.
(149) Yang X, Tahin Q, Hu YF, Russo IH, Balsara BR, Mihaila D, et al.Functional roles of chromosomes 11 and 17 in the transformation ofhuman breast epithelial cells in vitro. Int J Oncol 1999;15:629–38.
(150) Huang Y, Bove B, Wu Y, Russo IH, Yang X, Zekri A, et al. Microsatelliteinstability during the immortalization and transformation of human breastepithelial cells in vitro. Mol Carcinog 1999;24:118–27.
(151) Huang Y, Bove B, Russo IH, Yang X, Russo J. Microsatellite instabilityis induced by benzo[a]pyrene and 7,12-dimethyl benz[a]anthracene inhuman breast epithelial cells in vitro. Proc Am Assoc Cancer Res 1998;39:537.
(152) Yang X, Huang Y, Russo IH, Barrett JC, Russo J. Chromosomes 11 and17 revert transformed phenotypes induced by benzo[a]pyrene (BP) inhuman breast epithelial cells. Proc Am Assoc Cancer Res 1998;39:1263a.
(153) Yang XQ, Russo IH, Huang YJ, Russo J. Microsatellite instability ofD17S513 on chromosome 17 is associated with progression of breastcancer. Int J Oncol 1997;11:41–6.
(154) Wu Y, Barnabas N, Russo IH, Yang X, Russo J. Microsatellite instabilityand loss of heterozygosity in chromosomes 9 and 16 in human breastepithelial cells transformed by chemical carcinogens. Carcinogenesis1997;18:1069–74.
(155) Harley CB. Telomere loss: mitotic clock or genetic time bomb? Mutat Res1991;256:271–82.
(156) Hopfer U, Jacobberger JW, Gruenert DC, Eckert RL, Jat PS, Whitsett JA.Immortalization of epithelial cells. Am J Physiol 1996;270(1 Pt 1):C1-C11.
(157) Blackburn EH. Structure and function of telomeres. Nature 1991;350:569–73.
(158) Shay JW, Wright WE. The reactivation of telomerase activity in cancerprogression. Trends Genet 1996;12:129–31.
(159) Shay JW, Bacchetti S. A survey of telomerase activity in human cancer.Eur J Cancer 1997;33:787–91.
(160) Avilion AA, Piatyszek MA, Gupta J, Shay JW, Bacchetti S, Greider CW.Human telomerase RNA and telomerase activity in immortal cell lines andtumor tissues. Cancer Res 1996;56:645–50.
(161) Higgy NA, Russo J, Mgbonyebi P, Salicioni AM, Russo IH. Humanchorionic gonadotropin inhibits telomerase activity in human breast epi-thelial cells in vitro. Proc Am Assoc Cancer Res 1998;39:3678a.
(162) Higgy NA, Salicioni AM, Russo IH, Zhang PL, Russo J. Differentialexpression of human ferritin H chain gene in immortal human breastepithelial MCF-10F cells. Mol Carcinog 1997;20:332–9.
(163) Theil EC. Ferritin: structure, gene regulation, and cellular function inanimals, plants, and microorganisms. Annu Rev Biochem 1987;56:289–315.
(164) Anison P. Current concepts in iron metabolism. Clin Lab Haematol 1982;11:241–57.
(165) Reichard P, Ehrenberg A. Ribonucleotide reductase—a radical enzyme.Science 1983;221:514–9.
(166) Ponka P, Schulman HM, Cox TM. Iron metabolism in relation to hemesynthesis. In: Dailey HA, editor. Biosynthesis of heme and chlorophyllus.New York (NY): McGraw-Hill; 1990; p. 393–405.
(167) Reif DW. Ferritin as a source of iron for oxidative damage. Free RadicBiol Med 1992;12:417–27.
(168) Guyton KZ, Kensler TW. Oxidative mechanisms in carcinogenesis. BrMed Bull 1993;49:523–44.
(169) Klausner RD, Rouault TA, Harford JB. Regulating the fate of mRNA: thecontrol of cellular iron metabolism. Cell 1993;72:19–28.
(170) Dognin J, Crichton RR. Mobilisation of iron from ferritin fractions ofdefined iron content by biological reductants. FEBS Lett 1975;54:234–6.
(171) Biemond P, Swaak AJ, Beindorf CM, Koster JF. Superoxide-dependentand -independent mechanisms of iron mobilization from ferritin by xan-thine oxidase. Implications for oxygen-free-radical-induced tissue de-struction during ischaemia and inflammation. Biochem J 1986;239:169–73.
(172) Zhao MJ, Jung L. Kinetics of the competitive degradation of deoxyriboseand other molecules by hydroxyl radicals produced by the Fenton reactionin the presence of ascorbic acid. Free Radic Res 1995;23:229–43.
(173) Fidler IJ, Nicolson GL. Concepts and mechanisms of breast cancer me-tastasis. In: Bland KI, Copeland EM, editors. The breast: comprehensivemanagement of benign and malignant diseases. Philadelphia (PA): Saun-ders; 1991. p. 395–408.
(174) Kohn EC, Liotta LA. Molecular insights into cancer invasion: strategiesfor prevention and intervention. Cancer Res 1995;55:1856–62.
(175) Malins DC, Polissar NL, Gunselman SJ. Progression of human breastcancers to the metastatic state is linked to hydroxyl radical-induced DNAdamage. Proc Natl Acad Sci U S A 1996;93:2557–63.
(176) Han X, Liehr JG. Microsome-mediated 8-hydroxylation of guanine basesof DNA by steroid estrogens: correlation of DNA damage by free radicalswith metabolic activation to quinones. Carcinogenesis 1995;16:2571–4.
(177) Frenkel K, Wei L, Wei H. 7,12-dimethylbenz[a]anthracene induces oxi-dative DNA modification in vivo. Free Radic Biol Med 1995;19:373–80.
(178) Weinberg ED. Roles of iron in neoplasia. Promotion, prevention, andtherapy. Biol Trace Elem Res 1992;34:123–40.
(179) Fan H, Villegas C, Wright JA. A link between ferritin gene expression andribonucleotide reductase R2 protein, as demonstrated by retroviral vectormediated stable expression of R2 cDNA. FEBS Lett 1996;382:145–8.
(180) Moroz C, Lahat N, Biniaminov M, Ramot B. Ferritin on the surface oflymphocytes in Hodgkin’s disease patients. A possible blocking substanceremoved by levamisole. Clin Exp Immunol 1977;29:30–5.
(181) Keown P, Descamps-Latscha B. In vitro suppression of cell-mediatedimmunity by ferroproteins and ferric salts. Cell Immunol 1983;80:257–66.
(182) Rosen HR, Moroz C, Reiner A, Reinerova M, Stierer M, Svec J, et al.Placental isoferritin associated p43 antigen correlates with features of highdifferentiation in breast cancer. Breast Cancer Res Treat 1992;24:17–26.
(183) Rosen HR, Flex D, Stierer M, Moroz C. Monoclonal antibody CM-H-9detects circulating placental isoferritin in the serum of patients with vis-ceral metastases of breast cancer. Cancer Lett 1991;59:145–51.
(184) Kwak EL, Larochelle DA, Blaumont C, Torti SV, Torti FM. Role ofNF-�B in the regulation of ferritin H by tumor necrosis factor-�. J BiolChem 1995;270:15285–93.
36 Journal of the National Cancer Institute Monographs No. 27, 2000

(185) Rogers JT. Ferritin translation by interleukin-6: the role of sequencesupstream of the start codons of the heavy and light subunit genes. Blood1996;87:2525–37.
(186) Kastan MB, Onyekwere O, Sidransky D, Vogelstein B, Craig RW. Par-ticipation of p53 protein in the cellular response to DNA damage. CancerRes 1991;51:6304–11.
(187) el-Deiry WS, Harper JW, O’Connor PM, Velculescu VE, Canman CE,Jackman J, et al. WAF1/CIP1 is induced in p53-mediated G1 arrest andapoptosis. Cancer Res 1994;54:1169–74.
(188) Agarwal ML, Taylor WR, Chernov MV, Chernova OB, Stark GR. Thep53 network. J Biol Chem 1998;273:1–4.
(189) Russo J, Hu YF, Ao X, Grill C, Russo IH. Critical appraisal of estrogensas carcinogenic agents. In: Birkhauser MH, Rosenbaum H, editors. IVEuropean Congress on Menopause. Paris: Editions ESKA; 1998. p.279–87.
(190) Telang NT, Axelrod DM, Bradlow HL, Osborne MP. Metabolic biotrans-formation of estradiol in human mammary explant cultures. Ann N YAcad Sci 1990;586:70–8.
(191) Fishman J, Osborne MP, Telang NT. The role of estrogen in mammarycarcinogenesis. Ann N Y Acad Sci 1995;768:91–100.
(192) Telang NT, Suto A, Wong GY, Osborne MP, Bradlow HL. Induction byestrogen metabolite 16�-hydroxyestrone of genotoxic damage and aber-rant proliferation in mouse mammary epithelial cells. J Natl Cancer Inst1992;84:634–8.
(193) Ryan DE, Thomas PE, Reik LM, Levin W. Purification, characterizationand regulation of five rat hepatic microsomal cytochrome P-450 enzymes.Xenobiotica 1982;12:727–44.
(194) Wilson NM, Christou M, Turner CR, Wrighton SA, Jefcoate CR. Bindingand metabolism of benzo[a]pyrene and 7,12-dimethylbenz[a]anthraceneby seven purified forms of cytochrome P-450. Carcinogenesis 1984;5:1475–83.
NOTE
Supported by Public Health Services grants R01CA6728 (National CancerInstitute) and ES07280 (National Institute of Environmental Health Sciences),National Institutes of Health, Department of Health and Human Services.
Journal of the National Cancer Institute Monographs No. 27, 2000 37