Challenging IBD Cases...Case Presentation • 33 yo female G2P1 25 week gestation pregnancy with 3...
16
Challenging IBD Cases Nancy McGreal, MD Associate Professor of Medicine and Pediatrics Divisions of Adult and Pediatric Gastroenterology Duke University Medical Center
Transcript of Challenging IBD Cases...Case Presentation • 33 yo female G2P1 25 week gestation pregnancy with 3...

Challenging IBD Cases
Nancy McGreal, MDAssociate Professor of Medicine and Pediatrics
Divisions of Adult and Pediatric GastroenterologyDuke University Medical Center

Disclosures
• None

Case Presentation
• 33 yo female G2P1 25 week gestation pregnancy with 3 days of sharp RLQ abd pain; no known hx of IBD
• Initially - no fevers, chills, nausea, vomiting, diarrhea
• OSH: WBC 15.8K with mild left shift, reassuring fetal US
- RUQ US – normal, no cholelithiasis or cholecystitis
- Abd MRI – no appendicitis
• Develops fever 102 F, worsening RLQ abd pain, nausea
• No contractions or leakage of fluid; good fetal movement

Case Presentation
• PMHx: endometriosis, infertility, shingles
• PSHx: T&A, ORIF arm fx, ovarian cyst removal, I&D perianal abscess 11 years prior
• Meds: Prenatal vitamin, Omega-3 fatty acid
• FHx: CAD, HTN; no IBD or colorectal cancer
• SHx: Healthcare worker, non-contributory

Case Presentation
• PE: T 100.2 F other VSS, gravid abdomen, mild tenderness in RLQ without peritoneal signs
• Work-up:- WBC 14.6K with left shift- US appendix – non-diagnostic- Abd MRI – terminal ileitis
• Diarrhea develops on day of MRI – stool cx, C. diff PCR negative
• Fevers persist to 102 F despite IV piperacillin/tazobactam
• Repeat abd MRI 3 days later shows thickened TI compatible with possible Crohn’s disease

Next Steps?
• Is this infectious ileitis vs. new onset Crohn’s disease?
• If you are concerned this is a new diagnosis of Crohn’s disease in a pregnant patient, do you:
- Perform a colonoscopy for tissue diagnosis?
- Treat empirically for Crohn’s disease? Which medication?

Colonoscopy with Biopsy
PATHOLOGY: ILEAL MUCOSA WITH MODERATE CHRONIC ACTIVE ILEITIS, ULCERATION AND FEATURES MOST CONSISTENT WITH MARKED REACTIVE LYMPHOID HYPERPLASIA; NEGATIVE CD3/CD20 STAINING (NO LYMPHOMA); NORMAL COLON BIOPSIES

Case Presentation
• Started on IV solumedrol with response and transitioned to budesonide
• Recrudescence of RLQ abd pain; budesonide → prednisone
• Seen in GI clinic to discuss initiation of biologic therapy
• Re-admitted a few days later with fever 102 F, abdominal pain, WBC 15K, thrombocytosis

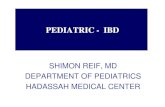
Abdominal MRI
• Percutaneous drainage → 3 liters purulent fluid with cx + for MSSA and anaerobes
• One blood cx + MSSA; endocarditis evaluation negative
AbscessAir-fluid level in abscess
Abscess

Next Steps?
• Management of Crohn’s disease complicated by intra-abdominal abscess in pregnancy:
- Antibiotic considerations
- Drainage/surgery in gravid abdomen
• Biologic therapy in the setting of intra-abdominal abscess/pelvic sepsis:
- Timing of initiation
- Management of biologics in the 3rd trimester

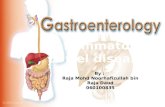
Management of Intra-abdominal Abscess in Crohn’s Disease
Carvalho A et al. J Coloproctology 2018; 38(2):158-163

Non-Obstetric Abdominal Surgery in Pregnancy
• 2% of women require surgery for non-obstetric indications during pregnancy (appendectomy, cholecystectomy)
• lBD
- CD: perforation, obstruction, bleeding, perianal abscess
- UC: medically refractory disease
• Laparoscopic and open approaches are both feasible and need to be individualized to the clinical scenario
• Perioperative considerations
- Positioning in left lateral decubitus 2nd/3rd trimesters
- Pre and post-op fetal heart monitoring at viability
- Tocolytic agents if risk of pre-term labor
- VTE prophylaxisKilleen S et al. Colorectal Dis 2016; 19:123-138SAGES May 2017

Mahadevan U et al. Gastroenterology 156(5): 1508-1524

Management of Biologics and Small Molecules in Pregnancy
Mahadevan U et al. Gastroenterology 156(5): 1508-1524

Case Presentation
• Treated with 4 weeks of ertapenum; drains removed
• Adalimumab initiated at conclusion of ertapenum course
• Healthy 37 week infant delivered 6 weeks after initiation of adalimumab
• 2 months post delivery the patient developed recurrent intra-abdominal fluid collections and underwent drainage followed by ileocecal resection
• Remains in clinical and endoscopic remission 4 years later on adalimumab 40 mg Q 2 weeks (6-MP added and withdrawn after one year of treatment)

Thank You for Your Time and Attention