Challenge TB - Indonesia Year 3 Quarterly Monitoring ...pdf.usaid.gov/pdf_docs/PA00MPX8.pdf ·...
67
Challenge TB - Indonesia Year 3 Quarterly Monitoring Report January – March 2017 Submission date: April 28, 2017
Transcript of Challenge TB - Indonesia Year 3 Quarterly Monitoring ...pdf.usaid.gov/pdf_docs/PA00MPX8.pdf ·...

Challenge TB - Indonesia
Year 3
Quarterly Monitoring Report
January – March 2017
Submission date: April 28, 2017
2
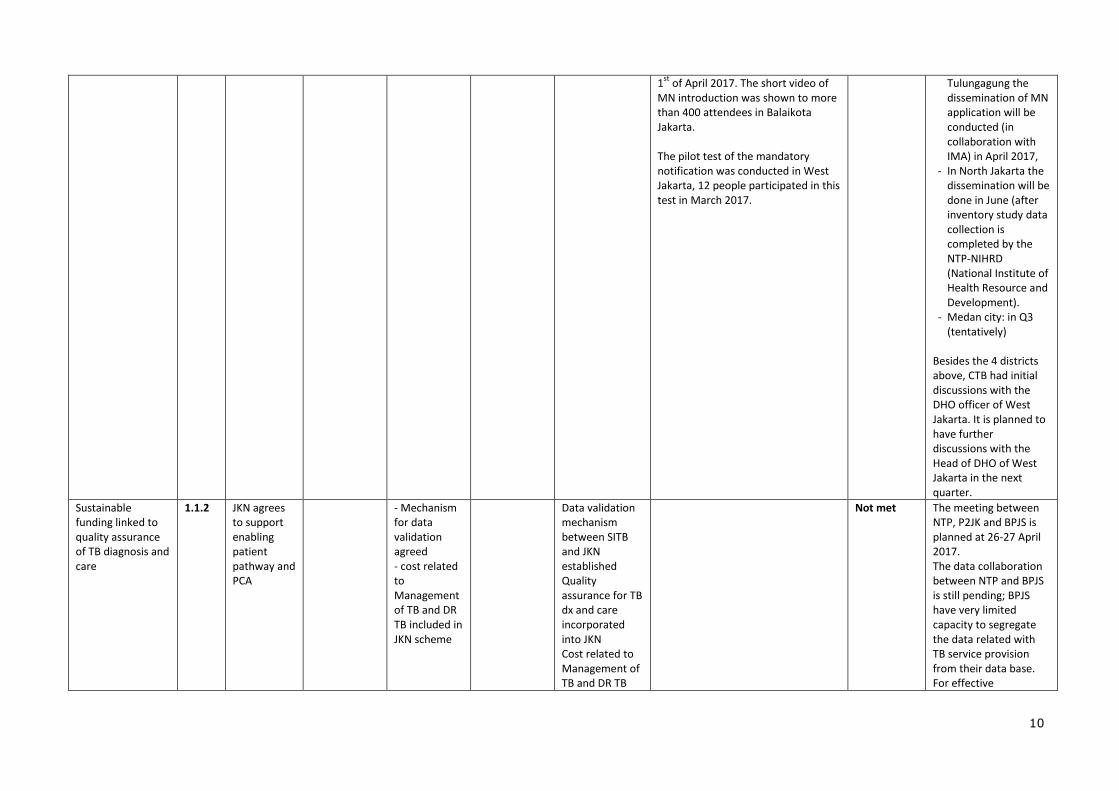
Table of Contents
1. QUARTERLY OVERVIEW 3
2. YEAR 3 ACTIVITY PROGRESS 9
3. CHALLENGE TB’S SUPPORT TO GLOBAL FUND IMPLEMENTATION IN YEAR 3 47
4. SUCCESS STORIES – PLANNING AND DEVELOPMENT 48
5. QUARTERLY REPORTING ON KEY MANDATORY INDICATORS 50
6. CHALLENGE TB-SUPPORTED INTERNATIONAL VISITS (TECHNICAL AND MANAGEMENT-RELATED TRIPS) 53
7. QUARTERLY INDICATOR REPORTING 57
Cover photo: "NTP Manager, DR. Asik Surya, MPPM was giving a token of appreciation to B.J. Habibie The 3rd President of Indonesia during the ceremonial opening of TBgraphy. The ceremonial opening of TBgraphy was opened by Joseph R. Donovan, US Ambassador for Indonesia (left) and USAID Mission Director, Erin McKee (right). (credit: Teuku Nasrullah)
This report was made possible through the support for Challenge TB provided by the United States Agency for International Development (USAID), under the terms of cooperative agreement number AID-OAA-A-14-00029.
Disclaimer
The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.

3
1. Quarterly Overview
Country Indonesia
Lead Partner KNCV
Other partners FHI360, WHO, IRD, ATS
Work plan timeframe October 2016 – September 2017
Reporting period January – March 2017
Most significant achievements: The TBGRAPHY event attended by the third (former) President of Indonesia and the Ambassador of the USA to Indonesia.
TBGRAPHY is a photo exhibition resulting from a contest, that shows photos of tuberculosis patients
and those who work to fight the disease in the country. The exhibit also highlighted various technologies used to detect tuberculosis infections, and the often lengthy and complex process involved in diagnosis and treatment. The exhibition was aimed at raising awareness of tuberculosis by placing emphasis on the importance of cooperation between institutions to combat the disease. The ceremonial opening of TBGRAPHY was attended by Joseph R. Donovan, US Ambassador for
Indonesia, Erin McKee, Mission Director for USAID/Indonesia, Asik Surya, NTP Manager, Ministry of Health, Arifin Panigoro, the chairman of the Stop TB Partnership Indonesia, and B.J. Habibie, the third President of Indonesia. Ambassador Donovan officially started the TBGRAPHY with an opening speech, followed by Dr. Asik and Mr. Habibie who is a former TB patient, having been diagnosed with TB while studying in Germany many years ago. Joint External Monitoring Mission 2017
The Joint External Monitoring Mission for tuberculosis (TB) control (JEMM TB), January 6-16, 2017, was undertaken by Indonesian experts from the Ministry of Health (MOH), the National Tuberculosis Program (NTP), universities, the non-governmental sector, community service organizations, and external experts from Indonesia’s partners in the fight against TB. CTB partners (WHO, KNCV, FHI360, ATS and IRD) were actively involved in the JEMM 2017. CTB also organized the visit in CTB provinces.
The mission aimed to provide an analysis of the TB situation, of Indonesia’s TB control efforts, and to provide recommendations for further strengthening of TB control services to reach the targets of the National TB Plan, 2015-2019, the End TB Strategy, and the Sustainable Development goals and targets which pertain to TB. The mission undertook field visits to DKI Jakarta, Central Java, West Sumatra, South Kalimantan, and South-East Sulawesi and held discussions with key agencies in the health field in the country.
Key recommendations of JEMM were presented to the Minister and high ranking officers of MoH: 1. In order to increase case finding, notifications and access to care, the JEMM strongly advises
the MoH to drive massive engagement of private providers - and shift treatment from hospitals to the primary care level - by adjusting payment mechanisms in both primary (FKTP) and hospital (FKRTL) systems of JKN. This would capitalize on the extraordinary opportunity created by expansion of JKN to transform TB control in Indonesia.
2. The JEMM strongly advises the MoH to greatly increase the public sector focus on engaging all
care providers and civil society. 3. The JEMM urges the MoH and NTP to double current funding and mobilize the human
resources necessary for full implementation of the NSP, 2016-2020, ensuring high quality of service provision. The NTP has to reach out to other agencies, directorates and entities within and outside the MoH to implement the NSP.
4. To improve the reporting of diagnosed cases, the JEMM urges the NTP to invest in swiftly and significantly improving the SITT and expediting mechanisms to capture all TB cases, in both
public and private sectors, including prisons. A TB module should be integrated with the future eHealth environment in Indonesia (SIP).
5. The JEMM urges the country to explore a Presidential Initiative on TB in order to enable and accelerate the multi-sectoral response to this preventable and treatable epidemic and ensure, in advance of the 2018 UN High Level Meeting on TB, that Indonesia is making the necessary investments to end TB.
The JEMM recommendations are utilized by NTP to revise and update current NTP policies and strategies, including the strategy for new the GF grant proposal 2018-2020.

4
The Mandatory Notification application officially launched by Minister of Health of Indonesia on World TB Day. Wajib Notifikasi (WIFI- Mandatory Notification) is a mobile application for primary clinics and private practitioners to notify TB cases to the NTP. During the World TB day peak event, the Minister of Health
of Indonesia, Prof. Dr. Nila Djuwita F. Moeloek, SpM (K) officially launched the WIFI application in Balaikota Jakarta, on the 1st of April 2017. On this occasion, the WIFI video introduction was shown to around 400 attendees from the Ministry of Health, the Provincial Health Office and other Ministries, Non-Profit Organizations in TB (international and local), TB stakeholders and professional organizations, International Development Organization and provincial staff of DKI Jakarta including health facilities and hospital staff.
This mobile application will support the Mandatory Notification implementation for private practitioners by providing a user-friendly reporting system. It gives private practitioners a reminder to follow up on a particular patient and his treatment and provides status-recommendations in a particular time
period. A notification will be sent to the respective Puskesmas (Public Health Center) and District Health Office through a SMS alert through which they will be able to monitor the report via web- based interface.
This application is free of charge and available at Google Play Store under the name “Wajib Notifikasi TB’ since the 23rd of February 2017. Up to now the application is downloaded by 100+ people. Before the official launch, the application was piloted in West Jakarta, 12 users participated in this pilot in March 2017. The project is still improving the user guide and is actively following up the dissemination of the app and the experiences of the “early adopters”, to ensure user-friendliness and effectiveness of the app.
PMDT site expanded from 21 (in Year 2), to 29 (in Q2 Year 3) sites in six CTB provinces In Year 3, up to March 2017, 7 new sub referral PMDT centers were established, which brings the total number of PMDT sites in CTB provinces to 29 (please see table below for more details). Additionally,
three sub-referral sites in Central Java were improved to be referral sites, and are now able to conduct initial treatment. Provinces Referral Site *)
Sub referral *) Progress during APA 3 up to
March 2017
North Sumatera
1 (RSUP. H. Adam Malik)
2 (RSUD Djasemen Saragih Siantar, RSUD Rantau Prapat (Labuan Batu)
2 new PMDT sub referral sites established (RSUD Djasemen Saragih Siantar, RSUD Rantau Prapat (Labuan Batu)
DKI Jakarta
1 (RSUP Persahabatan)
4 (RSI Cempaka Putih, RSUK Kalideres, RSPI Sulianti Saroso, RSUK Mampang)
3 new PMDT sub referral sites established (RSUK Kalideres, RSPI Sulianti Saroso and RSUK Mampang)
West Java 1 (RSHS) 3 RSPG Cisarua Bogor, BBKPM Bandung, RSUD Gunungjati Cirebon
Central Java
5 (RSUD dr. Moewardi, RSUP dr. Kariadi, RSUD Kardinah Tegal, RS Paru Ario Wirawan Salatiga, RSUD Cilacap,)
2 (RSUD Kudus, RSUD Temanggung )
3 Sub referral PMDT sites were strengthened to be referral sites (RSUD Kardinah Tegal, RS Paru Ario Wirawan Salatiga, RSUD Cilacap)
East Java 2 (RSUD Dr. Soetomo Surabaya & RSUD Saiful Anwar Malang)
5 (RS Paru Jember, RSUD Soedono Madiun, RSUD Dr. Iskak Tulungagung, RSUD Ibnu Sina Gresik, RSUD Jombang)
Papua 1 (RSUD Jayapura)
2 (RSUD Nabire and RSUD Merauke)
2 new PMDT sub referral sites established (RSUD Nabire and RSUD Merauke)
*) The role of MDR referral and sub-referral site is similar: identification of patients at risk of having DR TB, diagnosis of MDR TB, initiation of MDR-TB treatment, monitoring and managing side effects, treatment evaluation, recording & reporting, and also in logistic management. However, sub referral centers may not have all disciplines represented in their multi-disciplinary DRTB team, may not have the capacity and medicines to manage all intermediate and serious side effects, and some sub-referral hospitals do not have a ward for admission of DR-TB patients or complete laboratory for baseline tests. Referral centers

5
are currently being equipped and trained for the management of patients on BDQ containing regimens; the sub-referral centers not yet. Satellite sites are engaged in case finding, treatment continuation and organization of patient support, monitoring of side effects, logistic management, and recording.
The mass screening in total 11 prisons/detention centers was completed.
CTB facilitated active case finding in prisons. Next to increased case notification, the screening was also intended to show the Directorate General (DG) of Correction and the Ministry of Law and Human Rights, that TB screening should be implemented alongside routine TB case finding and care. After the results of the CTB screening in 11 prisons were reviewed, the DG of Correction agreed to use the remainder of APA3 to strengthen routine case finding based on cough surveillance, instead of only
relying on TB mass screening. In Q3, CTB will support the DG of Correction to prepare and conduct a workshop in collaboration with the NTP, to discuss health program sustainability to secure more
funding and human resources for TB control in prisons from the national level and to provide clearer guidance for the collaboration between the civilian and prison health services at facility level. Result from these 11 prisons (from Year 2 up to Q2 Year 3) are:
# Inmates screened (symptomatic + X-ray) = 10,594
% inmates screened are presumptive TB = 17% (1,908/10,954) % inmates able to collect sputum among presumptive = 77% (1,477/1,908) % inmates-sputum sent for Xpert examination = 100% (1,477/1,477) % inmates tested with Xpert are diagnosed with TB = 13% (193/1,477) % inmates diagnosed TB put on TB treatment = 100% (193/193)

6
Progress on CTB end-of-project SMART expected achievements:
CTB end-of-project SMART expected achievement
Baseline
(2014)
Actual Result
2015
Actual Result
2016
Remarks (progress to date, challenges, achievements)
A patient/case-based, real-time electronic recording & reporting system. functions at national and sub-national levels for both TB and MDR-TB
3=a patient/case-based, real-time ERR system functions at national and sub-national levels for both TB and MDR-TB
3=a patient/case-based, real-time ERR system functions at national and sub-national levels for both TB and MDR-TB
3=a patient/case-based, real-time ERR system functions at national and sub-national levels for both TB and MDR-TB
There are 2 electronic reporting systems, SITT (Comprehensive TB System Information) for TB sensitive patients and E TB Manager (ETM) for DRTB. Both SITT and ETM are patient/case based and developed as online (real time) system.
Challenges: Most facilities don’t input the data into the SITT in
real time (usually quarterly basis). Therefore aggregate reporting will continue to be important for the coming years.
Achievements:
- The systems have adopted the WHO new definition
- The newest version of
SITT now complies with the latest country policy changes and reflects the latest WHO definitions.
By the end of Challenge TB, 100% of presumptive DR-TB patients will be tested with GeneXpert
78%
(3,457/4,412)
88%
(5,513/6,235)
Challenge: data on the testing of presumptive DR-TB using GeneXpert is currently only available in ETM and through aggregate reports from Xpert sites. The newest version of SITT includes a feature for Xpert reporting and will be used starting in the 3rd quarter (where SITT is available on-site). Aggregate reporting will continue to be important.
Number of MDR-TB patients initiating second-line treatment increased from 996 in 2014 to 9,752 in 2019 in 6 CTB provinces (stratified by regimen)
996 1,136 1,317 CTB will focus on implementation of the shorter regimen (TA to procurement, adjustment of guidelines etc.) Beginning in July 2017. It is anticipated that with the introduction of ND&R…

7
Technical/administrative challenges and actions to overcome them: For APA3, a total number of 123 staff members were planned. At the end of quarter two there were still 18 vacancies to fill. The most challenging position to find suitable candidates for is the position of Technical Officer Lab (TO Lab). We therefore decided to lower the requirements for this position and
use our existing lab team to strengthen the capacity of the new candidates. As a result, we found TO Labs for all provinces with vacancies, except for East Java. That position, as well as the other outstanding vacancies, will be filled in quarter three. The Papua provincial team is still not fully formed yet. Despite four rounds of advertisements, recruitment of a provincial coordinator and senior technical officer has not been successful. Currently FHI is conducting the 5th round for recruitment for these positions; in the interim one national level
staff was temporarily based in Jayapura to support and accelerate CTB implementation in the three Papua districts. One M&E officer was successfully recruited and joined the Papua office in February 2017.
We have faced procurement delays for extended warranties on Xpert machines and SL-LPA tests due to protracted negotiations with MedQues and BioMerieux respectively, who do not adhere to the
preferential pricing provided by the producers (Cepheid for warranties and Hain LS for the 2nd line LPA). After extensive negotiations with both vendors and both Cepheid and Hain LS, the contract with MedQues will be signed in quarter three; BioMerieux has indicated they will not be able to partner on these purchases and thus cannot support with their import registration. Therefore, we will procure through GDF and import through USAID in quarter 3.
.

8

9
2. Year 3 activity progress
Sub-objective 1. Enabling environment
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 – Mar 2017
Piloting Mandatory Notification
1.1.1 GIS mapping of private providers in 4 districts available
MN app for PSPs piloted in 4 districts
MN implemented in 4 pilot districts
- evaluation of the result from MN piloting documented and disseminated - MN result is documented and disseminated to other districts
Lesson learnt from MN pilot feed into national policy and scale-up plans
PPs Mapping Results of the data analysis of private providers (PPs) mapping in Bandung city (conducted in Q4 APA 2) is now available. Lessons learned were identified to improve the next PPs mapping activities (questionnaire, method and data validation mechanism). CTB will collaborate with IMA (Indonesia Medical Association) to conduct the PPs mapping in Medan City, Tulungagung and West Jakarta. IMA will also take the spatial data of another health service (e.g. lab, pharmacist) to support the urban TB control implementation. Mandatory Notification Application
1
The implementation guideline and user guidance for MN application was finalized in March 2017 through coordination meetings with the NTP. The MN application, named WIFI (Wajib Notifikasi) was officially launched by the Minister of Health on World TB Day celebrated on the
Partially met
The delay of the MN pilot/implementation was caused by the delay in the official launch. Medan City and North Jakarta couldn’t be included yet, because they are part of the inventory study (IS). The pilot in these two places is postponed until data collection for the IS is completed in June), in order to avoid “external factors” impacting the result of the study. The pilot testing of the MN application was discussed with the DHO of Bandung City, Medan City, Tulungagung and North Jakarta. The following timeline was the result of that discussion: - In Bandung city and
1 The MN application is a user-friendly reporting system using mobile application for PPs and primary clinics. Its provides private practitioners a reminder to follow up the patient and treatment
outcome status-should be in a particular time period. A notification will be sent to Puskesmas (Public Health Center) and District Health Office at their respective area through SMS alert and they are
also able to monitor the report via web based console.
10
1st
of April 2017. The short video of MN introduction was shown to more than 400 attendees in Balaikota Jakarta. The pilot test of the mandatory notification was conducted in West Jakarta, 12 people participated in this test in March 2017.
Tulungagung the dissemination of MN application will be conducted (in collaboration with IMA) in April 2017,
- In North Jakarta the dissemination will be done in June (after inventory study data collection is completed by the NTP-NIHRD (National Institute of Health Resource and Development).
- Medan city: in Q3 (tentatively)
Besides the 4 districts above, CTB had initial discussions with the DHO officer of West Jakarta. It is planned to have further discussions with the Head of DHO of West Jakarta in the next quarter.
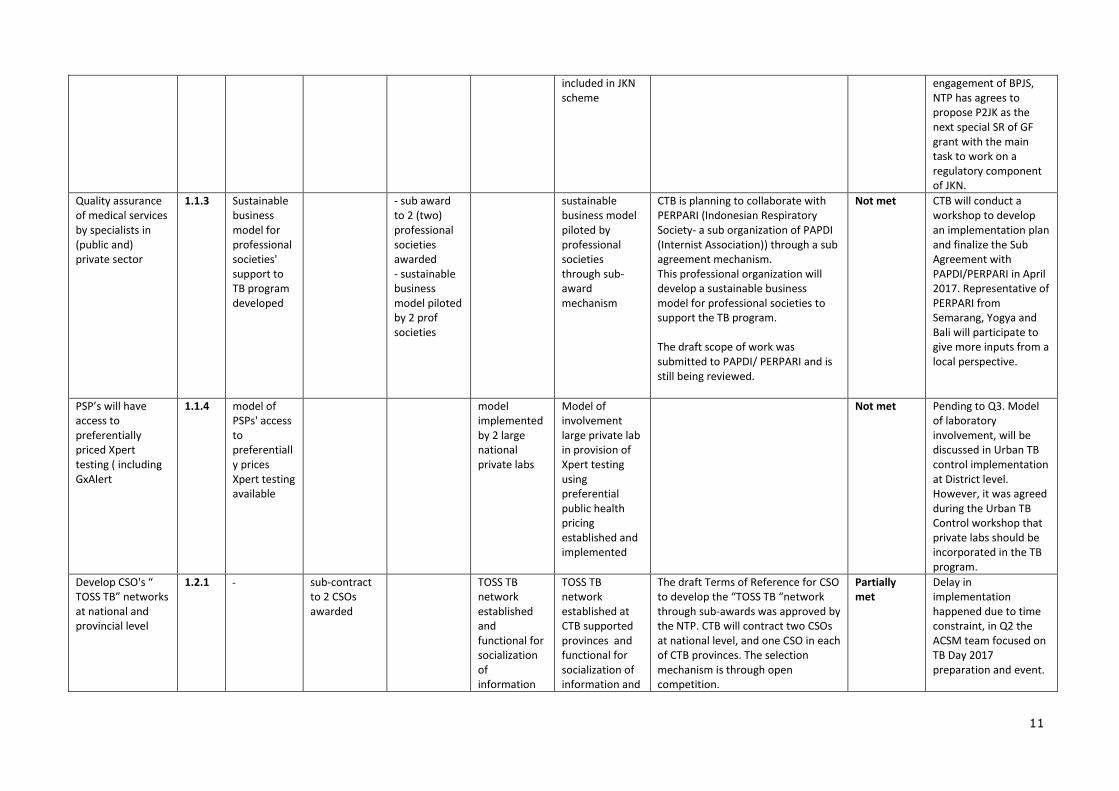
Sustainable funding linked to quality assurance of TB diagnosis and care
1.1.2
JKN agrees to support enabling patient pathway and PCA
- Mechanism for data validation agreed - cost related to Management of TB and DR TB included in JKN scheme
Data validation mechanism between SITB and JKN established Quality assurance for TB dx and care incorporated into JKN Cost related to Management of TB and DR TB
Not met The meeting between NTP, P2JK and BPJS is planned at 26-27 April 2017. The data collaboration between NTP and BPJS is still pending; BPJS have very limited capacity to segregate the data related with TB service provision from their data base. For effective
11
included in JKN scheme
engagement of BPJS, NTP has agrees to propose P2JK as the next special SR of GF grant with the main task to work on a regulatory component of JKN.
Quality assurance of medical services by specialists in (public and) private sector
1.1.3 Sustainable business model for professional societies' support to TB program developed
- sub award to 2 (two) professional societies awarded - sustainable business model piloted by 2 prof societies
sustainable business model piloted by professional societies through sub-award mechanism
CTB is planning to collaborate with PERPARI (Indonesian Respiratory Society- a sub organization of PAPDI (Internist Association)) through a sub agreement mechanism. This professional organization will develop a sustainable business model for professional societies to support the TB program. The draft scope of work was submitted to PAPDI/ PERPARI and is still being reviewed.
Not met CTB will conduct a workshop to develop an implementation plan and finalize the Sub Agreement with PAPDI/PERPARI in April 2017. Representative of PERPARI from Semarang, Yogya and Bali will participate to give more inputs from a local perspective.
PSP’s will have access to preferentially priced Xpert testing ( including GxAlert
1.1.4 model of PSPs' access to preferentially prices Xpert testing available
model implemented by 2 large national private labs
Model of involvement large private lab in provision of Xpert testing using preferential public health pricing established and implemented
Not met Pending to Q3. Model of laboratory involvement, will be discussed in Urban TB control implementation at District level. However, it was agreed during the Urban TB Control workshop that private labs should be incorporated in the TB program.
Develop CSO's “ TOSS TB” networks at national and provincial level
1.2.1 sub-contract to 2 CSOs awarded
TOSS TB network established and functional for socialization of information
TOSS TB network established at CTB supported provinces and functional for socialization of information and
The draft Terms of Reference for CSO to develop the “TOSS TB “network through sub-awards was approved by the NTP. CTB will contract two CSOs at national level, and one CSO in each of CTB provinces. The selection mechanism is through open competition.
Partially met
Delay in implementation happened due to time constraint, in Q2 the ACSM team focused on TB Day 2017 preparation and event.
12
and behavioral change communication on TB based on national Advocacy, communication and media strategy
behavioral change communication on TB based on national Advocacy, communication and media strategy
This quarter a new patient group has been established in Gresik, East Java, named PETIR (Pejuang TB MDR) with CTB facilitation.
Sub-objective 2. Comprehensive, high quality diagnostics
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges) Oct-Dec 2016 Jan-Mar 2017
Apr-Jun 2017
Jul-Sep 2017
Year end Oct 2016 to March 2017
13
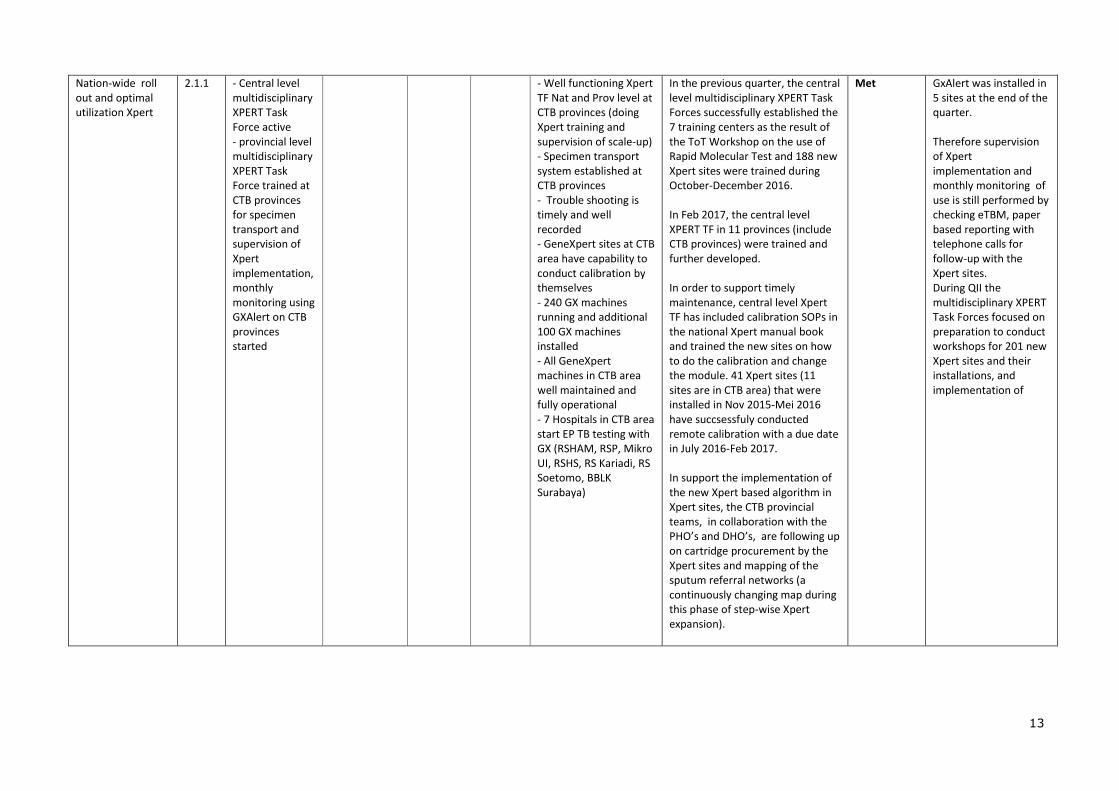
Nation-wide roll out and optimal utilization Xpert
2.1.1 - Central level multidisciplinary XPERT Task Force active - provincial level multidisciplinary XPERT Task Force trained at CTB provinces for specimen transport and supervision of Xpert implementation, monthly monitoring using GXAlert on CTB provinces started
- Well functioning Xpert TF Nat and Prov level at CTB provinces (doing Xpert training and supervision of scale-up) - Specimen transport system established at CTB provinces - Trouble shooting is timely and well recorded - GeneXpert sites at CTB area have capability to conduct calibration by themselves - 240 GX machines running and additional 100 GX machines installed - All GeneXpert machines in CTB area well maintained and fully operational - 7 Hospitals in CTB area start EP TB testing with GX (RSHAM, RSP, Mikro UI, RSHS, RS Kariadi, RS Soetomo, BBLK Surabaya)
In the previous quarter, the central level multidisciplinary XPERT Task Forces successfully established the 7 training centers as the result of the ToT Workshop on the use of Rapid Molecular Test and 188 new Xpert sites were trained during October-December 2016. In Feb 2017, the central level XPERT TF in 11 provinces (include CTB provinces) were trained and further developed. In order to support timely maintenance, central level Xpert TF has included calibration SOPs in the national Xpert manual book and trained the new sites on how to do the calibration and change the module. 41 Xpert sites (11 sites are in CTB area) that were installed in Nov 2015-Mei 2016 have succsessfuly conducted remote calibration with a due date in July 2016-Feb 2017. In support the implementation of the new Xpert based algorithm in Xpert sites, the CTB provincial teams, in collaboration with the PHO’s and DHO’s, are following up on cartridge procurement by the Xpert sites and mapping of the sputum referral networks (a continuously changing map during this phase of step-wise Xpert expansion).
Met GxAlert was installed in 5 sites at the end of the quarter. Therefore supervision of Xpert implementation and monthly monitoring of use is still performed by checking eTBM, paper based reporting with telephone calls for follow-up with the Xpert sites. During QII the multidisciplinary XPERT Task Forces focused on preparation to conduct workshops for 201 new Xpert sites and their installations, and implementation of

14
Figure 1. SOP Calibration Rapid Test Molecular TB
- Instruction leaflet/SOP for Calibration printed and distributed to all GeneXpert sites
CTB supported NTP in providing instruction/SOPs for calibration of Xpert machines (how to do the calibration and change the module). A dummy of desk flipcharts for Xpert calibration was submitted to NTP for final review, and will be printed after approval from NTP.
Met
Capacity building to support the implementation of GxAlert, provision of bar code printers,
2.1.2 GX Alert well implemented in 6 CTB supported provinces
Surveillance of Xpert implementation takes place at national level
- Xpert results are automatically entered eTB manager and linkage established between GX and SITT - Xpert results is notified to provider and patient - GX utilization data available at central level
The total sites planned for GxAlert is 16. In the first phase, CTB has provided technical assistance to install GxAlert in 5 Labs (4 hospitals, 1 National Reference Lab) in 3 CTB provinces. These are Mikrobiologi UI, Persahabatan Hospital, and Cempaka Putih Hospital in DKI Jakarta; Hasan Sadikin Hospital in West Java, and BBLK Surabaya in East Java. A truncated TOT was also given to
Partially met
NTP already acknowledges the benefits of GxAlert, following also the JEMM recommendation. The price and procurement are the issues that need to be solved before NTP can allocate resources for countrywide implementation.

15
a small in-country team during the installation. After the first installation conducted by an international consultant, the in-country team conducted site installations #2 to #5. The installation success rate was 100% and all data was transferred. The in-country team also experimented with LAN, local WiFi, various modems/routers, and multiple WiFi dongles/tech and was successful with global sims (Vodafone) and local sims (Telkomsel). With GxAlert 5 GeneXpert machines are connected across 3 provinces. It also allows the results of GeneXpert tests (include data error), information related to cartridges (stock, utilization) to be accessed from a website.
The other 11 sites planned under CTB Year 3 will be installed in phase II (Q3 Year 3).
Support maintenance and PSM of Xpert
2.1.3 - Maintenance contract for 17 GX machines finalized - 17 XpertCheck for CTB Xpert machines procured, calibration done as per due date
- Logistic Management and Information System related to Xpert introduced and implemented -Upgrading GxDx software started at CTB areas
calibration at CTB areas done as per due date
calibration at CTB areas done as per due date
- 17 CTB GX machines are calibrated in time and operational - National logistic management & information system related to Xpert implemented - MTB/RIF Ultra rolled out (depending on availability early 2017 and NTP approval)
- Significant increase in Xpert installation in the last 6 months from 82 machines by the end of 2016, to 277 machines by the end of March 2017 in 34 provinces in Indonesia. 216 GeneXpert machines will be installed in Q3.
- After a series of meetings and negotiations, CTB reached an agreement with Chepeid and PT. Medquest for an extended warranty of 17 GX machines:
1. A 3-year contract which started (dated) on the 1st January 2017, and covers all Xpert machines that are already broken (need
Partially met
The maintenance contract for 17 GX machines was delayed due to a protracted negotiation process related to price and services.
16
modules replacement) at this moment
2. The package includes: Xpert Check kits, spare part replacement, local courier, remote assistance, and onsite intervention (if needed)
- Logistic Management and Information System related to Xpert accommodated by GxAlert implementation in 5 sites (see 2.1.2). GxAlert provide information of Xpert cartridge –stock and utilization.
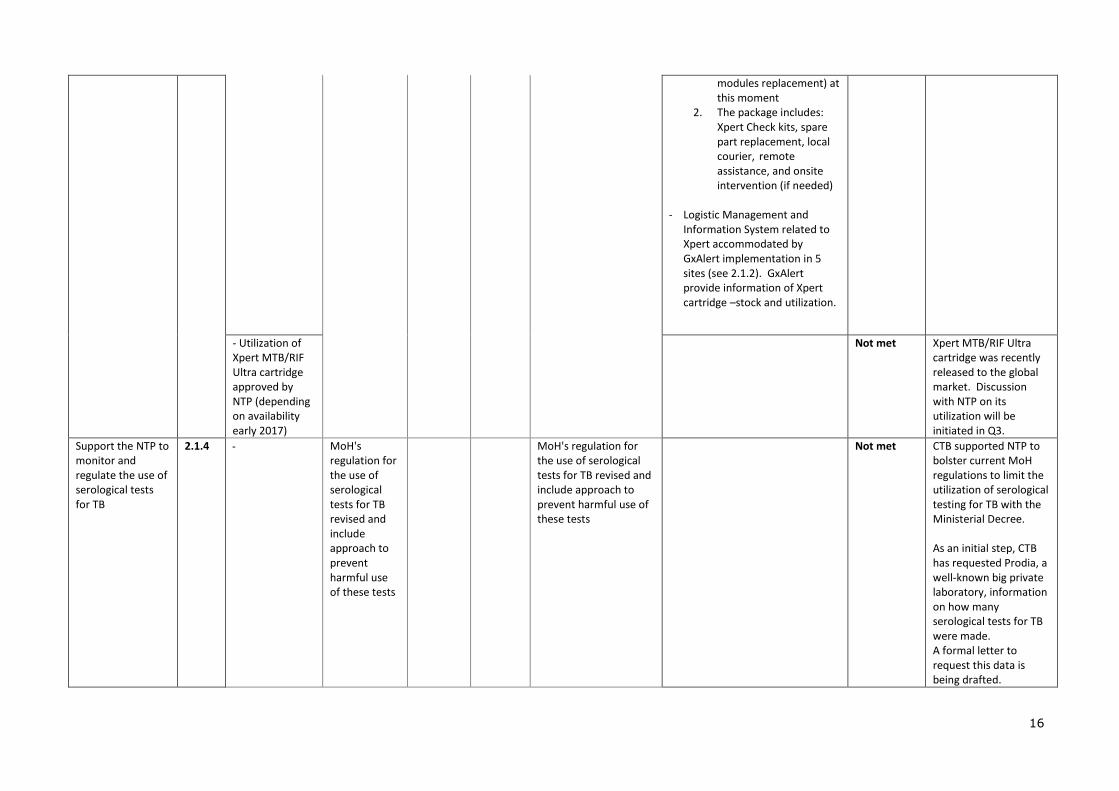
- Utilization of Xpert MTB/RIF Ultra cartridge approved by NTP (depending on availability early 2017)
Not met Xpert MTB/RIF Ultra cartridge was recently released to the global market. Discussion with NTP on its utilization will be initiated in Q3.
Support the NTP to monitor and regulate the use of serological tests for TB
2.1.4 MoH's regulation for the use of serological tests for TB revised and include approach to prevent harmful use of these tests
MoH's regulation for the use of serological tests for TB revised and include approach to prevent harmful use of these tests
Not met CTB supported NTP to bolster current MoH regulations to limit the utilization of serological testing for TB with the Ministerial Decree. As an initial step, CTB has requested Prodia, a well-known big private laboratory, information on how many serological tests for TB were made. A formal letter to request this data is being drafted.

17
Pilot for using children’s stool samples for use in Xpert
2.1.5 - SOP for GX testing using stool samples available and distributed to selected Xpert sites
interim result of piloting documented and shared to NTP, Pediatric TWG/KOMLI for further policy recommendation
CTB introduced the GX testing using stool samples to Childhood TB to TWG and NTP in August 2016. The TWG is planning a workshop in the 4
th week of April to develop
recommendations and a way forward on the subject. Draft SOPs were developed and in the final process. A workshop will be conducted with related experts (Childhood TB TWG, Lab team) in April, to decide on how the national TB program will continue with implementation of stool sample for childhood TB.
Partially met
The dissemination of GX testing using stool samples is awaiting the childhood TB TWG and Lab team result meeting.
Introduction of LQMS system (NRLs, provincial labs, IRL’s CTB provinces. districts)
2.2.1 - 3 NRLs are able to implement LQMS
- LQMS implementation policy available
- 3 National Reference labs in CTB area implement LQMS - Lessons learned and recommendation to improve implementation of LQMS
An open competition for the trainer for LQMS training started in March 2017. Training is planned to be conducted from 15th-19th May 2017. CTB, 3NRLs and representative of directorate of medical service will participate in the training.
Partially met
LQMS implementation in the 3 NRLs and a meeting to discuss broader implementation will follow after the training.
EQA and capacity building of the sputum smear network
2.2.2 - Accreditation tools for SS network according to GLI is available
- NTP/Medical Service are advocated on GLI standard for SS network
- Map of SS network in 6 CTB provinces available - Implementation of EQA System in
- Accreditation of SS network document and policy for accreditation from MoH are available - SS network in CTB provinces functioning well - e-TB 12 utilized in CTB area to improve Microscopy EQA - EQA system for SS
CTB translated an accreditation tool for TB Microscopy Laboratory Network according to GLI 11 Standards and adjusted it to the local context/country situation. The tool was presented to the MoH (NTP and Sub-directorate Quality &Accreditation) and NRLs to obtain inputs and finalized.
Met

18
- Revised eTB12 and new EQA RR Pathway disseminated to NRL and MoH
PMDT sites reviewed and take lessons learned for improvement
established in PMDT site at CTB areas
CTB has provided TA to revise eTB12 and SOP of EQA.
Met The new EQA-SOP will be disseminated by the NTP in National Money meeting in April.
- Revised eTB12 disseminated in CTB provinces and districts
Revised eTB 12 and SOPs were disseminated to lab technicians and IRLs in 2 CTB districts (Medan City and Deli Serdang).
Partially met
Dissemination to other CTB provinces will continue in Q3.
- Data on Satelite SS Labs in PMDT sites available
CTB provided TA to map out Sputum Smear (SS) labs in PMDT sites. CTB collected information on performance of SS labs in PMDT sites which will examine/monitor the progress of therapy results. Questionnaires for mapping were drafted and submitted to NTP for review. They consist of questions related to lab resources, work load, internal quality assurance and external quality assurance. The result of the mapping will be followed up with capacity building if needed.
Partially met
The result is expected to be completed in Q3.
SL-LPA introduction
2.3.1 - LPAsl starter kit procured
- Services for SL LPA available - EQA for LPA started
Procurement of SL LPA starter kit is delayed due to very high price offered by the distributor. In a meeting conducted by NTP in February 2017, BioMeureux and PT Enseval Medika Prima as principal of Hain product/LPA and distributor respectively agreed to revise the price.
Partially met
Unfortunately, the revised price was still considered too expensive. Therefore, re-negotiation with the principal/distributor of SL LPA is needed. SL LPA kit is already registered in this country. Therefore NTP/CTB will need permit letters from the principal/distributor to
19
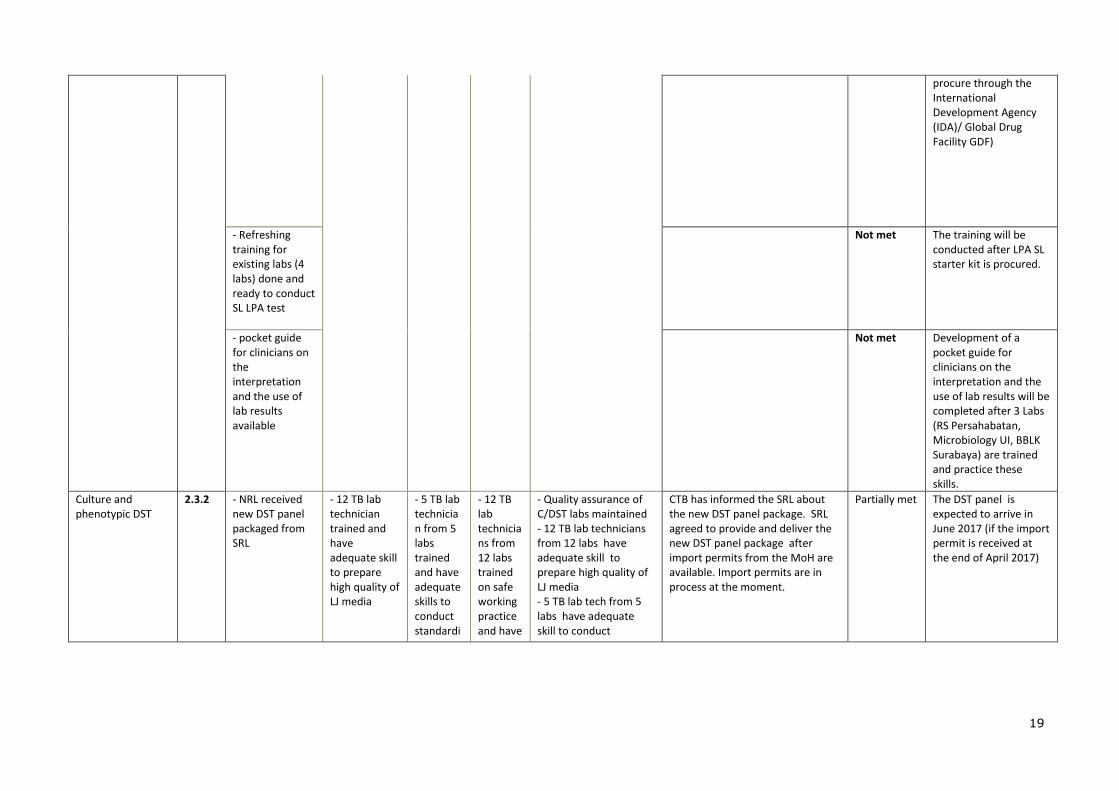
procure through the International Development Agency (IDA)/ Global Drug Facility GDF)
- Refreshing training for existing labs (4 labs) done and ready to conduct SL LPA test
Not met The training will be conducted after LPA SL starter kit is procured.
- pocket guide for clinicians on the interpretation and the use of lab results available
Not met Development of a pocket guide for clinicians on the interpretation and the use of lab results will be completed after 3 Labs (RS Persahabatan, Microbiology UI, BBLK Surabaya) are trained and practice these skills.
Culture and phenotypic DST
2.3.2 - NRL received new DST panel packaged from SRL
- 12 TB lab technician trained and have adequate skill to prepare high quality of LJ media
- 5 TB lab technician from 5 labs trained and have adequate skills to conduct standardi
- 12 TB lab technicians from 12 labs trained on safe working practice and have
- Quality assurance of C/DST labs maintained - 12 TB lab technicians from 12 labs have adequate skill to prepare high quality of LJ media - 5 TB lab tech from 5 labs have adequate skill to conduct
CTB has informed the SRL about the new DST panel package. SRL agreed to provide and deliver the new DST panel package after import permits from the MoH are available. Import permits are in process at the moment.
Partially met The DST panel is expected to arrive in June 2017 (if the import permit is received at the end of April 2017)

20
zed TB culture
adequate skill to start implementation on lab safety in TB culture/DST lab
standardized TB culture - Maintenance manual for DST labs established - DST labs certified for new DST package - NRL certified for new DST package - DST service for CAP and Mox available - 12 TB lab technicians from 12 labs trained and have adequate skill to work in TB culture/DST lab safely
LJ media preparation training was successfully done on 07-10 March 2017 with CTB facilitation. It was conducted at the NRL Culture/DST Lab (BBLK Surabaya) with 12 TB lab technicians (M:7; F:5) from 12 labs in CTB provinces as participants. Outputs of the training were that participants have adequate skills to prepare high quality TB culture/LJ media including the reagents and perform internal quality assurance (PMI) for media.
Met
Sub-objective 3. Patient-centered care and treatment
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Ensuring uptake of Xpert testing: TOT and mentoring PHO and DHO’s and professional societies to ensure uptake of Xpert testing following the updated national diagnostic algorithms and the Xpert roll-out
3.1.1 80% utilization rate of Xpert in CTB supported districts
At least 80% utilization of Xpert
North Sumatra (3 machines; 16 modules) Q2 = 22%
DKI (12 machines; 65 modules) Q2 = 29%
Central Java (7 machines; 32 modules) Q2 = 46%
West Java (4 machines; 42 modules) Q2 = 52%
East Java (8 machines; 44 modules) Q2 = 96%
Papua (3 machines; 8 modules) Q2 = 2%
Low reported utilization is related to poor recording and reporting (RR), manual
Choose an item.
21
and/or electronic, in several sites. Collecting excel based statistic reports from the machines could be one option to get more representative data. Ensuring each site is implementing the new TB algorithm and developing specimen referral networking will be the main strategy to increase Xpert utilization.
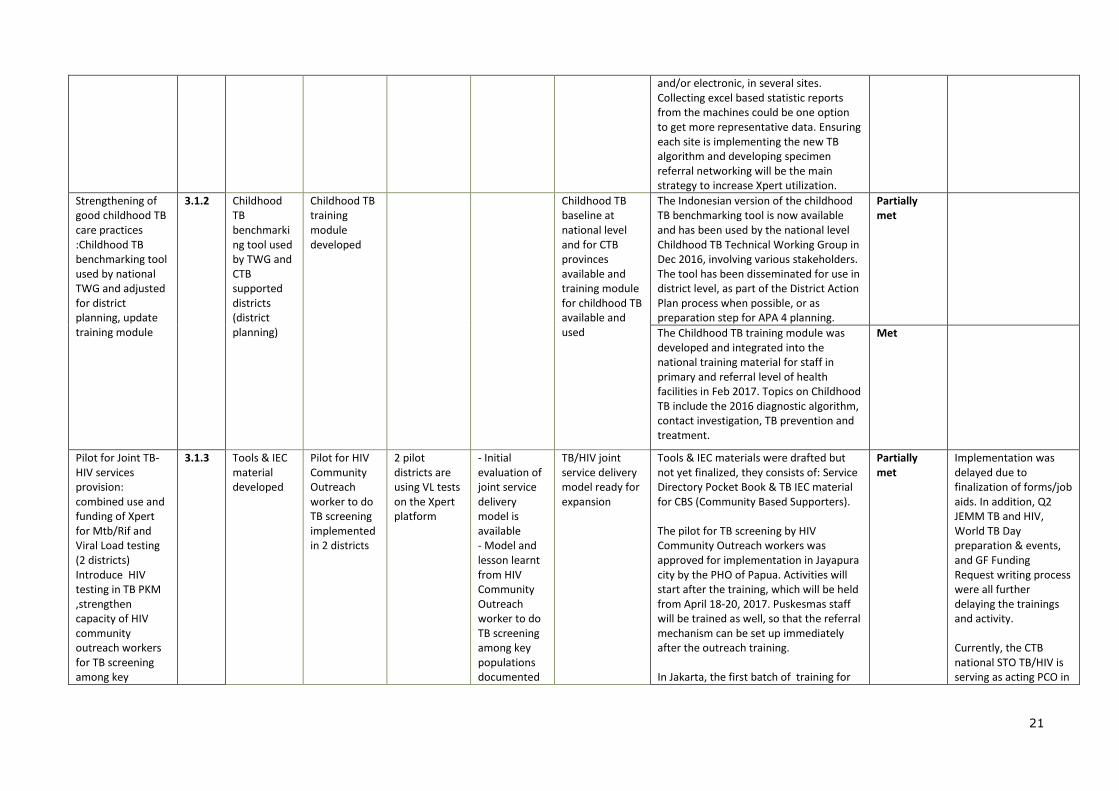
Strengthening of good childhood TB care practices :Childhood TB benchmarking tool used by national TWG and adjusted for district planning, update training module
3.1.2 Childhood TB benchmarking tool used by TWG and CTB supported districts (district planning)
Childhood TB training module developed
Childhood TB baseline at national level and for CTB provinces available and training module for childhood TB available and used
The Indonesian version of the childhood TB benchmarking tool is now available and has been used by the national level Childhood TB Technical Working Group in Dec 2016, involving various stakeholders. The tool has been disseminated for use in district level, as part of the District Action Plan process when possible, or as preparation step for APA 4 planning.
Partially met
The Childhood TB training module was developed and integrated into the national training material for staff in primary and referral level of health facilities in Feb 2017. Topics on Childhood TB include the 2016 diagnostic algorithm, contact investigation, TB prevention and treatment.
Met
Pilot for Joint TB-HIV services provision: combined use and funding of Xpert for Mtb/Rif and Viral Load testing (2 districts) Introduce HIV testing in TB PKM ,strengthen capacity of HIV community outreach workers for TB screening among key
3.1.3 Tools & IEC material developed
Pilot for HIV Community Outreach worker to do TB screening implemented in 2 districts
2 pilot districts are using VL tests on the Xpert platform
- Initial evaluation of joint service delivery model is available - Model and lesson learnt from HIV Community Outreach worker to do TB screening among key populations documented
TB/HIV joint service delivery model ready for expansion
Tools & IEC materials were drafted but not yet finalized, they consists of: Service Directory Pocket Book & TB IEC material for CBS (Community Based Supporters). The pilot for TB screening by HIV Community Outreach workers was approved for implementation in Jayapura city by the PHO of Papua. Activities will start after the training, which will be held from April 18-20, 2017. Puskesmas staff will be trained as well, so that the referral mechanism can be set up immediately after the outreach training. In Jakarta, the first batch of training for
Partially met
Implementation was delayed due to finalization of forms/job aids. In addition, Q2 JEMM TB and HIV, World TB Day preparation & events, and GF Funding Request writing process were all further delaying the trainings and activity. Currently, the CTB national STO TB/HIV is serving as acting PCO in
22
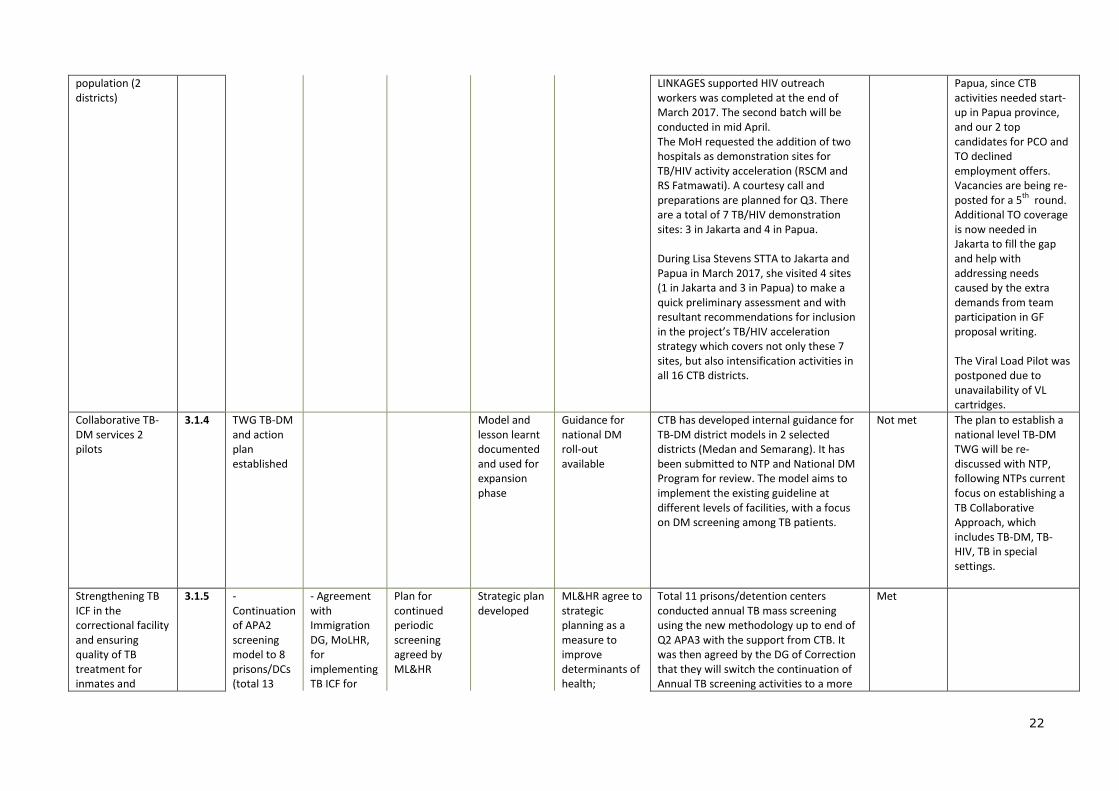
population (2 districts)
LINKAGES supported HIV outreach workers was completed at the end of March 2017. The second batch will be conducted in mid April. The MoH requested the addition of two hospitals as demonstration sites for TB/HIV activity acceleration (RSCM and RS Fatmawati). A courtesy call and preparations are planned for Q3. There are a total of 7 TB/HIV demonstration sites: 3 in Jakarta and 4 in Papua. During Lisa Stevens STTA to Jakarta and Papua in March 2017, she visited 4 sites (1 in Jakarta and 3 in Papua) to make a quick preliminary assessment and with resultant recommendations for inclusion in the project’s TB/HIV acceleration strategy which covers not only these 7 sites, but also intensification activities in all 16 CTB districts.
Papua, since CTB activities needed start-up in Papua province, and our 2 top candidates for PCO and TO declined employment offers. Vacancies are being re-posted for a 5
th round.
Additional TO coverage is now needed in Jakarta to fill the gap and help with addressing needs caused by the extra demands from team participation in GF proposal writing. The Viral Load Pilot was postponed due to unavailability of VL cartridges.
Collaborative TB-DM services 2 pilots
3.1.4 TWG TB-DM and action plan established
Model and lesson learnt documented and used for expansion phase
Guidance for national DM roll-out available
CTB has developed internal guidance for TB-DM district models in 2 selected districts (Medan and Semarang). It has been submitted to NTP and National DM Program for review. The model aims to implement the existing guideline at different levels of facilities, with a focus on DM screening among TB patients.
Not met The plan to establish a national level TB-DM TWG will be re-discussed with NTP, following NTPs current focus on establishing a TB Collaborative Approach, which includes TB-DM, TB-HIV, TB in special settings.
Strengthening TB ICF in the correctional facility and ensuring quality of TB treatment for inmates and
3.1.5 - Continuation of APA2 screening model to 8 prisons/DCs (total 13
- Agreement with Immigration DG, MoLHR, for implementing TB ICF for
Plan for continued periodic screening agreed by ML&HR
Strategic plan developed
ML&HR agree to strategic planning as a measure to improve determinants of health;
Total 11 prisons/detention centers conducted annual TB mass screening using the new methodology up to end of Q2 APA3 with the support from CTB. It was then agreed by the DG of Correction that they will switch the continuation of Annual TB screening activities to a more
Met

23
addressing determinants of health; enhanced monitoring of TB performance in prison Develop pilot with Immigration services for ICF
prisons/DCs in CTB areas) - APA2 first 5 prisons' screening analyzed
immigration detainees to piloting the model in DKI Jakarta
routine case finding based on cough surveillance for the rest of APA3. Results from these 11 prisons are: # inmates screened
(symptomatic + X-ray) = 10,594 % inmates screened are
presumptive TB = 17% (1,908/10,954)
% inmates able to collect sputum among presumptive= 77% (1,477/1,908)
% inmates-sputum sent for Xpert examination = 100% (1,477/1,477)
% inmates tested with Xpert are diagnosed with TB = 13% (193/1,477)
% inmates diagnosed TB put on TB treatment = 100% (193/193)
CTB successfully introduced the TB Intensified Case Finding (ICF) strategy to the immigration division. CTB had one courtesy meeting with the head of immigration division from Ministry of Law and Human Rights (MoLHR) Jakarta Provincial Office and he has given the “green light” to support the plan for implementing TB ICF in one immigration detention center in Jakarta as a model. Activities consist of preliminary assessment, workshop and TB screening for approximately 200 immigration detainees, this will be conducted in Q3.
24
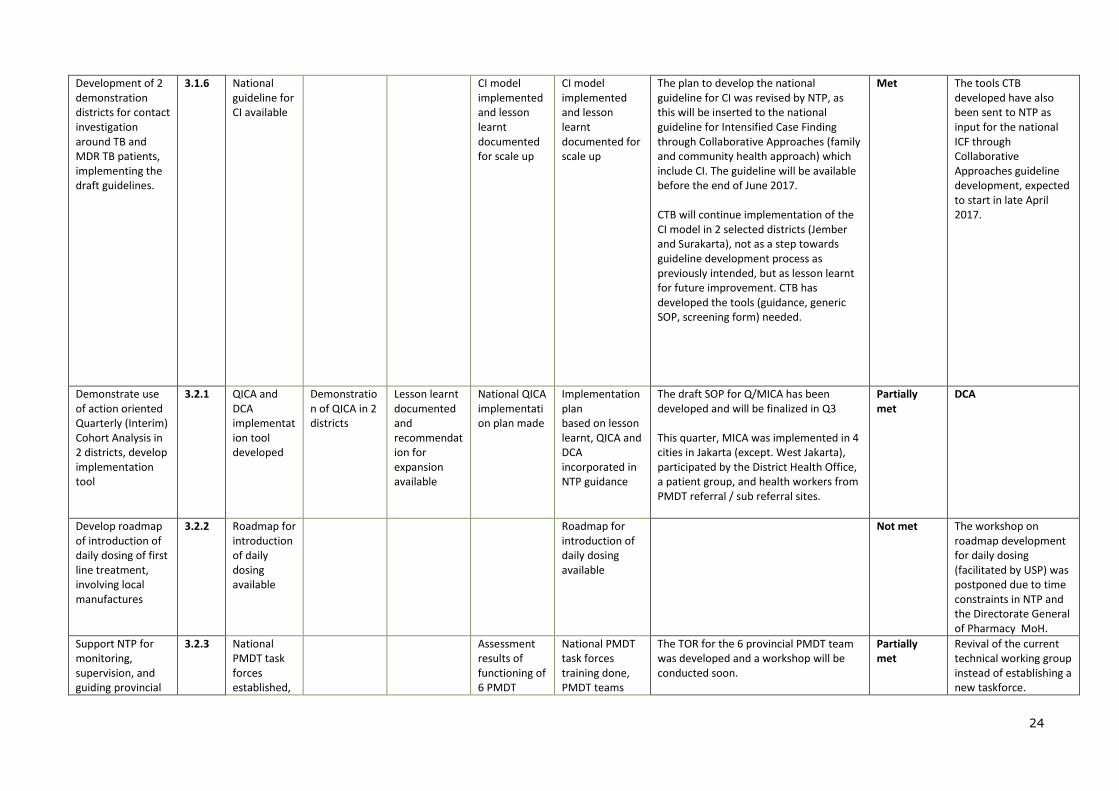
Development of 2 demonstration districts for contact investigation around TB and MDR TB patients, implementing the draft guidelines.
3.1.6 National guideline for CI available
CI model implemented and lesson learnt documented for scale up
CI model implemented and lesson learnt documented for scale up
The plan to develop the national guideline for CI was revised by NTP, as this will be inserted to the national guideline for Intensified Case Finding through Collaborative Approaches (family and community health approach) which include CI. The guideline will be available before the end of June 2017. CTB will continue implementation of the CI model in 2 selected districts (Jember and Surakarta), not as a step towards guideline development process as previously intended, but as lesson learnt for future improvement. CTB has developed the tools (guidance, generic SOP, screening form) needed.
Met The tools CTB developed have also been sent to NTP as input for the national ICF through Collaborative Approaches guideline development, expected to start in late April 2017.
Demonstrate use of action oriented Quarterly (Interim) Cohort Analysis in 2 districts, develop implementation tool
3.2.1 QICA and DCA implementation tool developed
Demonstration of QICA in 2 districts
Lesson learnt documented and recommendation for expansion available
National QICA implementation plan made
Implementation plan based on lesson learnt, QICA and DCA incorporated in NTP guidance
The draft SOP for Q/MICA has been developed and will be finalized in Q3 This quarter, MICA was implemented in 4 cities in Jakarta (except. West Jakarta), participated by the District Health Office, a patient group, and health workers from PMDT referral / sub referral sites.
Partially met
DCA
Develop roadmap of introduction of daily dosing of first line treatment, involving local manufactures
3.2.2 Roadmap for introduction of daily dosing available
Roadmap for introduction of daily dosing available
Not met The workshop on roadmap development for daily dosing (facilitated by USP) was postponed due to time constraints in NTP and the Directorate General of Pharmacy MoH.
Support NTP for monitoring, supervision, and guiding provincial
3.2.3 National PMDT task forces established,
Assessment results of functioning of 6 PMDT
National PMDT task forces training done, PMDT teams
The TOR for the 6 provincial PMDT team was developed and a workshop will be conducted soon.
Partially met
Revival of the current technical working group instead of establishing a new taskforce.
25
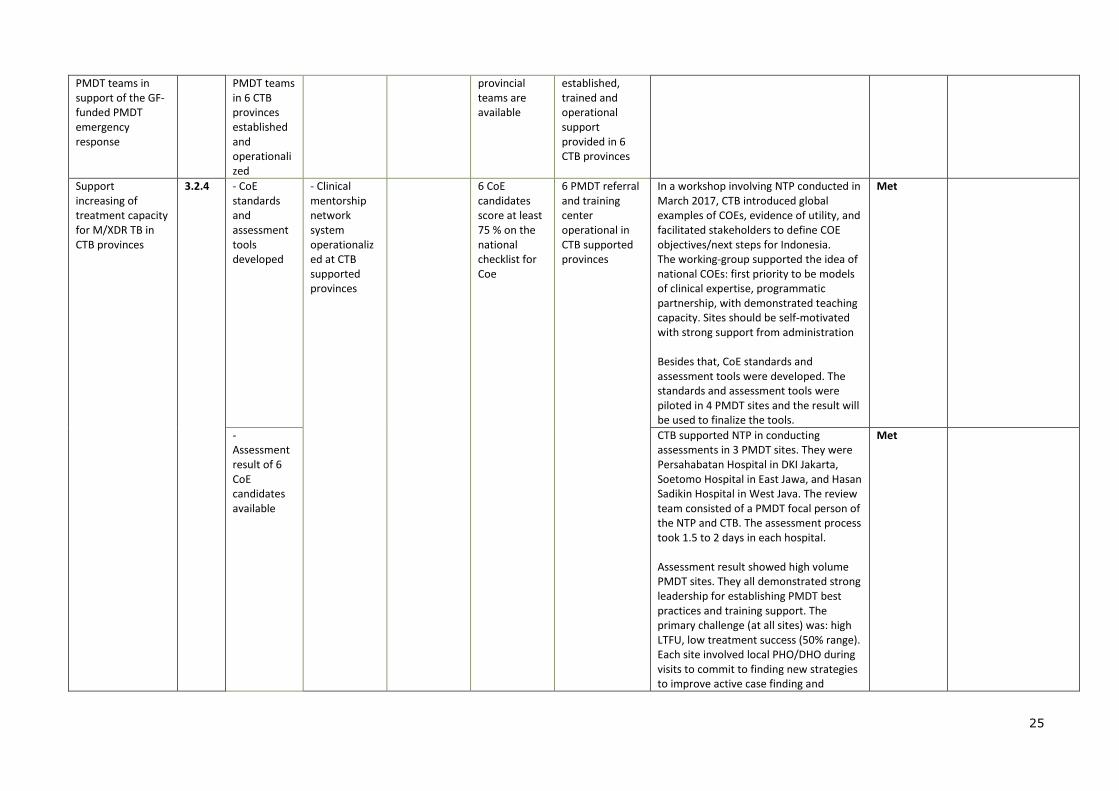
PMDT teams in support of the GF-funded PMDT emergency response
PMDT teams in 6 CTB provinces established and operationalized
provincial teams are available
established, trained and operational support provided in 6 CTB provinces
Support increasing of treatment capacity for M/XDR TB in CTB provinces
3.2.4 - CoE standards and assessment tools developed
- Clinical mentorship network system operationalized at CTB supported provinces
6 CoE candidates score at least 75 % on the national checklist for Coe
6 PMDT referral and training center operational in CTB supported provinces
In a workshop involving NTP conducted in March 2017, CTB introduced global examples of COEs, evidence of utility, and facilitated stakeholders to define COE objectives/next steps for Indonesia. The working-group supported the idea of national COEs: first priority to be models of clinical expertise, programmatic partnership, with demonstrated teaching capacity. Sites should be self-motivated with strong support from administration Besides that, CoE standards and assessment tools were developed. The standards and assessment tools were piloted in 4 PMDT sites and the result will be used to finalize the tools.
Met
- Assessment result of 6 CoE candidates available
CTB supported NTP in conducting assessments in 3 PMDT sites. They were Persahabatan Hospital in DKI Jakarta, Soetomo Hospital in East Jawa, and Hasan Sadikin Hospital in West Java. The review team consisted of a PMDT focal person of the NTP and CTB. The assessment process took 1.5 to 2 days in each hospital. Assessment result showed high volume PMDT sites. They all demonstrated strong leadership for establishing PMDT best practices and training support. The primary challenge (at all sites) was: high LTFU, low treatment success (50% range). Each site involved local PHO/DHO during visits to commit to finding new strategies to improve active case finding and
Met

26
retention for PMDT. In addition to that, an assessment in Sulianti Saroso Hospital in DKI Jakarta was also conducted and resulted in the initiation of the first MDR patient on treatment in that site.
- CoEs trained in all aspects of PMDT
The Introduction of clinical mentorship to the NTP was conducted during ATS’ mission debriefing on 23 March 2017. As further follow up, CTB will assess the readiness of communication / video conference equipment in PMDT sites in the next quarter.
Partially met
Supporting the NTP in PMDT management
3.2.5 good drug PSCM implemented with result of zero stock-out in CTB supported provinces
System of exchange experience agreed and implemented
good drug PSCM implemented with result of zero stock-out in CTB supported provinces
In Q2, CTB provided TA to the NTP on quantification, early warning systems and supply planning using Quant TB and eTB Manager software, and actively assisted the NTP in the GDF mission in September-October 2016 . CTB also provided TA to NTP to finalize the MDR logistic module, it is already n used for MDR TB training. CTB also supported the NTP to monitor Xpert machines, including cartridges and the utilization.
Partially met
The mechanism of exchange experience between PMDT sites will do by video conference (same with clinical mentorship). Due to PMDT site readiness for communication equipment, this activity is planned to be done in Q4.
Support implementation of ND/R by recruitment of experienced M/XDR TB clinician, expansion of BDQ treatment, develop supporting materials for
3.2.6 - M/XDR clinician recruited
- Triage approach and SR implemented - 1st patient at SR enrolled
- aDSM implemented in all PMDT sites in supported districts, BDQ treatment available in 6 PMDT priority provinces, implementation of SR started
CTB continues to support the NTP to improve quality of M/XDR treatment by recruiting an M/XDR clinician. The clinician will provide technical assistance in ensuring the treatment of DR TB patients in 6 hospitals are in line with National TB DR TB guidelines, and a clinical consultancy to the newly implemented DR TB treatment center and low performance centers as requested by
Not met

27
introduction shorter regimen, simplify aDSM for wider use, training in triage for doctors dealing with MDR, training and mentoring SR introduction and BDQ
the NTP. The ToR of the recruitment is available. However, it still needs to be discussed with the NTP PMDT team. The NTP and GF agreed to start STR implementation countrywide, by July 2017. The first shipment of STR drugs will arrive in the country by mid-June 2017. CTB provide support to finalize the guideline of STR (which also include the triage approach). The development of a shorter version of the guideline and a timeline of implementation will be conducted in early May 2017.
- aDSM policy and SOP available
CTB has prepared a draft guideline of aDSM and discussed the concept of aDSM with the Food and Drug Agency (FDA) and the NTP in March 2017. From the discussion, the NTP and the FDA prefer to use the current guideline that was released by the FDA (which is general for TB drugs either First Line and Second Line) and make adjustments or update it instead of using the new guideline developed by CTB which is focuses on second line drugs.
Partially met Further discussion is needed to identify the necessary adjustment and update.
Strengthening TB-HIV Care & Treatment by development of clinical HIV/TB care manual and mentoring SOP
3.2.7 Clinical TB/HIV care manual developed
Provincial and district clinical mentor group established and trained in mentoring in 2 provinces/districts
Provincial and district level mentor groups regularly review TB/HIV patients
It has been agreed with the NTP and the NAP that information on clinical mentoring for TB/HIV will be a part of a comprehensive HIV clinical mentoring manual. The team will meet by the end of April to finalize the TB/HIV section for integration into the HIV clinical mentoring manual. Provincial and district clinical mentor group establishment will be conducted after the TB/HIV section for integration into the HIV clinical mentoring manual is
Not met Discussions with the National MoH (NAP and NTP) showed that there were discrepant perceptions on the tools. The NAP has already developed the clinical mentoring tools for HIV and the NTP can use those for TB/HIV activities. However, the NAP did not agree to add TB/HIV specific
28
finalized.
material to enhance it. The NTP is therefore considering developing a separate manual. Discussions are ongoing.
Sub-objective 5. Infection control
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Support TB IC implementation in the framework of PMDT roll-out
5.1.2 Assessment result on TB IC at PMDT sites in CTB supported provinces available
70% of PMDT sites in CTB supported provinces implemented standard of TB IC (pass the national TB IC assessment tool)
IC assessment will be included as one of the standards in the self-assessment tool for DR TB facilities, currently being finalized. The earlier version of the tool has been tried in 3 PMDT hospitals.
Partially met Once the tool is finalized, it will be distributed for use in other PMDT facilities in CTB working area.
Develop national biosafety protocol for laboratory system
5.1.3 National TB lab BS leaflet developed and offered to MOH
National TB Lab BS leaflet developed and disseminated to TB Lab
Choose an item.
Operationalize TB surveillance among HCW, based on TBCAREI SOP’s and pilots
5.2.1 recommendation from lessons learnt workshop available
revised model of TB surveillance among HCWs adopted by NTP and implemented
No activities or progress related to this in Q2.
Not met This discussion to formulate the policy and implementation of TB HCW screening was delayed due to other priorities and time constraints.
Sub-objective 6. Management of latent TB infection

29
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Development of innovations in preventive treatment: introduction of HP treatment in pilot setting:
6.1.1 Plan for HRpt introduction available
Road-map of HRpt implementation established
The Minister of Health decree no. 67/2016 on TB Control, stated that Rifapentine is one option for TB preventive treatment . Introduction of the use of 3HP for child contacts was done to Childhood TB TWG in Dec 2016. However, there is no specific recommendation or plan for stepwise implementation yet. During Q2, CTB was involved in meetings related to the 3HP implementation plan. The NTP requires Sanofi to register Rifapentine in the country prior to any implementation, and this process started in December 2016.The process will take around 2 years by regular track. The NTP and Sanofi are discussing options to accelerate the process through fast tracking, for instance by the NTP sending a letter of support to the MoH Directorate of Pharmaceutical Service. At the same time CTB is exploring the possibility of using 3HP under study conditions ( feasibility study, looking at operational aspects of introduction of 3HP) Under the next FR proposal, CTB supports the NTP to propose funding for introduction of Rifapentine under the TB prevention module.
Partially met
Sub-objective 7. Political commitment and leadership

30
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status
Milestone met? (Met,
partially, not met)
Remarks (reason for not
meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun
2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Support and facilitate capacity building for district planning 6 provinces, 16 districts
7.2.1 16 districts task force appointed and trained on DAP formulation Draft of situation analysis, including baseline information and target-indicator setting, draft activity plan available in 16 district and feed into CTB APA 3B workplan
CTB APA3B Workplan approved and implementation started
DAP completed in 16 districts
legalized DAP available and integration into 2018 local government budget
priority activities in DAP integrated into 2018 local government budget
CTB facilitated the DAP (District Action Plan) financing scheme workshop with key stakeholders conducted in Semarang City & Surakarta City (Central Java). The next step to finalize the DAP is writing the narration of the whole DAP document and Municipality Regulation, then legalize the document to ensure the local budget for 2018 will accommodate the DAP. Below is further info for DAP: Table 1. DAP monitoring table
Key Item progress District- achieved
Socialization and preparation meeting with PHO/DHO and Local Planning Board (BAPPEDA), to appoint DAP Task force
Jayapura, Jayawijaya, Mimika (April)
Situation Analysis (setting initial indicator and target) and 1
st Draft
District Action Plan (indicators and target setting)
Jember, Bandung, Bogor (April) Jayapura, Jayawijaya, Mimika (May)
Finalization of Log frame Medan, Deli Serdang (April) Jember, Bandung, Bogor (April- May) Jayapura, Jayawijaya, Mimika (May)
Developing DAP Tulungagung (April)
Met
31
financing scheme Medan, Deli Serdang (May) Jember, Bandung, Bogor (May) Jayapura, Jayawijaya, Mimika (June, July)
Finished DAP process Semarang, Surakarta
The further DAP planning in DKI will be undertaken over the period April-May; due to the centralized nature of DKI Jakarta government, the planning will take place with close guidance from the PHO; the Log frames are expected by the end of May for mobilization of inter-sectoral resources.
Further progress of government support is a circular letter issued by the Governor West as the further follow up from Ministry of Home Affair. The letter is addressed to all districts/municipality mayors/leaders.
Figure 2. Circular letter from West Java Governor, to support acceleration to eliminate TB
In March 2017, the CTB Workplan APA3B was approved
32
Figure 3. DAP progress monitoring table
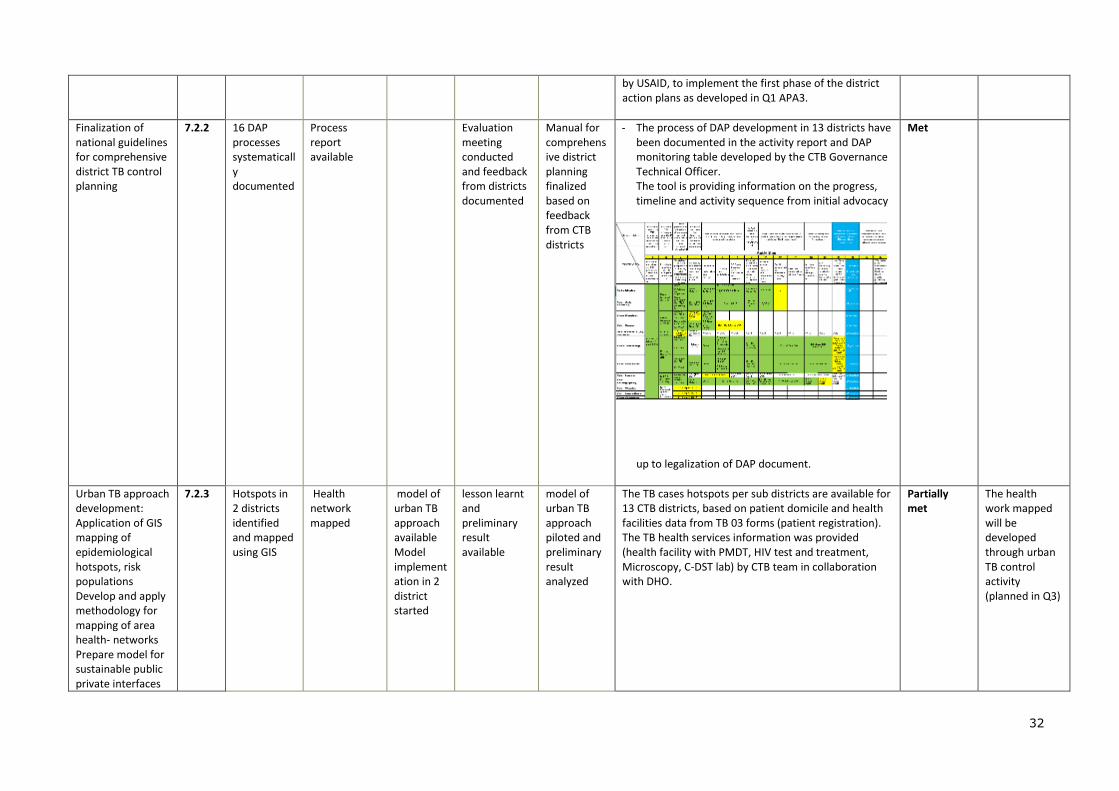
by USAID, to implement the first phase of the district action plans as developed in Q1 APA3.
Finalization of national guidelines for comprehensive district TB control planning
7.2.2 16 DAP processes systematically documented
Process report available
Evaluation meeting conducted and feedback from districts documented
Manual for comprehensive district planning finalized based on feedback from CTB districts
- The process of DAP development in 13 districts have been documented in the activity report and DAP monitoring table developed by the CTB Governance Technical Officer. The tool is providing information on the progress, timeline and activity sequence from initial advocacy
up to legalization of DAP document.
Met
Urban TB approach development: Application of GIS mapping of epidemiological hotspots, risk populations Develop and apply methodology for mapping of area health- networks Prepare model for sustainable public private interfaces
7.2.3 Hotspots in 2 districts identified and mapped using GIS
Health network mapped
model of urban TB approach available Model implementation in 2 district started
lesson learnt and preliminary result available
model of urban TB approach piloted and preliminary result analyzed
The TB cases hotspots per sub districts are available for 13 CTB districts, based on patient domicile and health facilities data from TB 03 forms (patient registration). The TB health services information was provided (health facility with PMDT, HIV test and treatment, Microscopy, C-DST lab) by CTB team in collaboration with DHO.
Partially met
The health work mapped will be developed through urban TB control activity (planned in Q3)

33
(notification, monitoring, training components)
Figure 4. TB Hotspot and TB services map
Currently, we are in progress to enrich the database with information of DOTS facility with HIV testing. The urban TB control (UTC) workshop was conducted in Jakarta, January 2017, participated and supported by the NTP, DHO staff from 10 cities (Jakarta, Bandung, Medan, Malang, Surabaya, Makassar, Semarang, Palembang, Batam and Pekanbaru); Professional organization, CSO, USAID representatives from the USAID mission as well as William Wells (USAID Washington), Michael K and Netty Kamp (KNCV-PMU). Key of results were: 1). Draft of action plan for urban TB control in 10 cities. 2). Draft of stepwise implementation
a. start from small scale (sub district) b. using GIS to build the health network c. The MoU should be developed as the approach
for TB patient governance in sub districts; between Public health center and PPs, private labs, and pharmacist.

34
Sub-objective 8. Comprehensive partnerships and informed community involvement
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Support the Indonesia Stop TB partnership and the NTP to make an analysis of the TB stakeholders landscape
8.1.1 TB partner landscape document available
TB partner landscape document available
Not met A meeting with Aisyiyah and NTP will be held in Q3 to finalize the TB partner landscape document which provide information data and role of each TB partner. The document is expected to be available before the 23
rd of May when the
Funding Request proposal is submitted. CCM will hold a special meeting for the TB partner landscape after 25 April 2017.
Support development of the advocacy, communication and media strategy
8.1.2 Overall national advocacy, communication and media strategy developed
Target group-specific strategies developed
Coherent advocacy, communication and media guide available
World TB Day Campaign as part of the national communication strategy has been implemented. A consultant to provide TA to develop national advocacy, communication and media strategy was hired last quarter. Messages for target group (male, urban, age 25-34, economic status middle lower- based on prevalence survey 2013 and basic health research 2013 ) has been defined as part of campaign objective. The message will implement through
Partially met
The delay on finalization of national advocacy, communication and media strategy was due to time constraints and conflicting priorities with TB Day preparation (expected to be finalized in Q4).

35
public service announcement (TV ads etc).
Development of CTB strategy on advocacy, communication
8.1.3 Joint CTB Advocacy, Communications and Media Strategy developed
CTB ACMS strategy disseminated in the organization
Media messaging regularly distributed
CTB facilitated the TB Day event 2017 by leading the photos festival, titled TBGRAPHY in Kota Tua, DKI Jakarta. The ceremonial opening of TBGRAPHY was attended by Joseph R. Donovan, US Ambassador for Indonesia, Erin McKee, Mission Director for USAID/Indonesia, Asik Surya, NTP Manager, Ministry of Health, Arifin Panigoro, the chairman of the Stop TB Partnership Indonesia, and B.J. Habibie, the third President of Indonesia. Ambassador Donovan officially started the TBGRAPHY with an opening speech, followed by Dr. Asik and Mr. Habibie who is a former TB patient, having been diagnosed with TB while studying in Germany many years ago. Some of media coverage regarding TBGRAPHY:
1. http://www.klikdokter.com/info-sehat/read/2912834/tbgraphy-mengenal-tuberkulosis-lewat-fotografi
2. https://www.youtube.com/watch?v=KLoTm7loLgM
3. http://thepresidentpostindonesia.com/2017/03/30/menderita-tb-di-umur-20-habibie-tegaskan-indonesia-bebas-tb-tahun-2050-di-pameran-tbgraphy-galeri-fatahillah/
4. https://lifestyle.sindonews.com/read/1192543/155/mengenal-tuberkulosis-
Partially met
36
lewat-fotografi-1490788910
5. http://lifestyle.bisnis.com/read/20170330/106/641154/perkenalkan-tuberculosis-lewat-pameran-fotografi
6. http://www.jakartaglobe.beritasatu.com/arts/photography-exhibition-raises-awareness-of-tuberculosis/
7. http://www.thejakartapost.com/news/2017/04/01/talk-the-week-us-ambassador-to-indonesia-opens-tuberculosis-themed-photo-exhibition.
8. http://fk.unair.ac.id/dr-asik-surya/
9. http://indonesia.shafaqna.com/ID/ID/4823392
https://www.pressreader.com/indonesia/kompas/20170330/281758449126265 Besides, in the peak event TB Day in Balaikota Jakarta, attended by around 800 people, CTB participated in the booth exhibition among another 15 participants. In CTB’s booth, through a game, CTB disseminated information related to TB to the community, TB cadres who visited the CTB booth.
http://www.jakartaglobe.beritasatu.com/arts/photography-exhibition-raises-awareness-of-tuberculosis/
http://www.jakartaglobe.beritasatu.com/arts/photography-exhibition-raises-awareness-of-tuberculosis/
http://www.jakartaglobe.beritasatu.com/arts/photography-exhibition-raises-awareness-of-tuberculosis/

37
Figure 5. People interested to visit CTB booth
Support JEMM 2017
8.1.4 recommendation from JEMM available and feed into development CN for GF
recommendation from JEMM available and feed into development CN for GF
Final JEMM 2017 recommendations are available to the NTP and the FR Writing Team, key recommendations were fed in into development of the FR for GF. The wider scale dissemination is waiting further approval from the Director of Prevention and CD Control. Based on JEMM 2017’s recommendations for TB/HIV, CTB supported the NTP and the NAP to develop an HIV test acceleration plan for TB patients, which will be focused on 42 districts in 2017. This plan will be scaled up in a step-wise fashion to 141 districts by 2019 and is already included in the 2018-2020 GF Funding Request/Concept Note.
Met
Support CCM and GF Technical Working Group
8.2.1 Monthly update reports by Provincial CTB teams on Xpert expansion, PMDT enrolment, TB/HIV testing and
Monthly update reports by Provincial CTB teams on Xpert expansion, PMDT enrolment, TB/HIV testing and
Monthly update reports by Provincial CTB teams on Xpert expansion, PMDT enrolment, TB/HIV testing and
Monthly update reports by Provincial CTB teams on Xpert expansion, PMDT enrolment, TB/HIV testing and
PRs of GF Indonesia rating improved (A2)
Monthly update reports on Xpert expansion, PMDT enrolment, TB/HIV testing and ART coverage, and action taken on findings have been incorporated into the CTB province monthly report template. Besides, CTB developed a district performance dashboard to monitor progress of districts with score card methods. Progress of districts is
Partially met
Updated monthly report template will be available from April 2017.
38
ART coverage, action taken on findings
ART coverage, action taken on findings
ART coverage, action taken on findings
ART coverage, action taken on findings
indicated by colors.
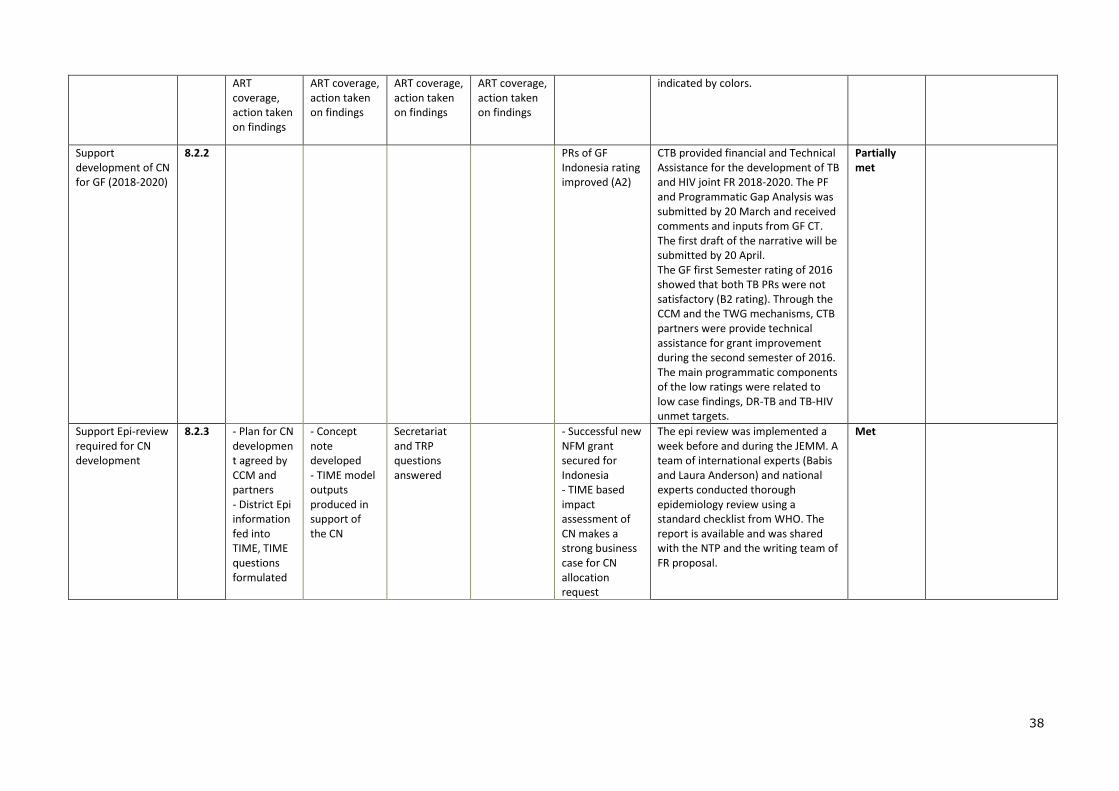
Support development of CN for GF (2018-2020)
8.2.2 PRs of GF Indonesia rating improved (A2)
CTB provided financial and Technical Assistance for the development of TB and HIV joint FR 2018-2020. The PF and Programmatic Gap Analysis was submitted by 20 March and received comments and inputs from GF CT. The first draft of the narrative will be submitted by 20 April. The GF first Semester rating of 2016 showed that both TB PRs were not satisfactory (B2 rating). Through the CCM and the TWG mechanisms, CTB partners were provide technical assistance for grant improvement during the second semester of 2016. The main programmatic components of the low ratings were related to low case findings, DR-TB and TB-HIV unmet targets.
Partially met
Support Epi-review required for CN development
8.2.3 - Plan for CN development agreed by CCM and partners - District Epi information fed into TIME, TIME questions formulated
- Concept note developed - TIME model outputs produced in support of the CN
Secretariat and TRP questions answered
- Successful new NFM grant secured for Indonesia - TIME based impact assessment of CN makes a strong business case for CN allocation request
The epi review was implemented a week before and during the JEMM. A team of international experts (Babis and Laura Anderson) and national experts conducted thorough epidemiology review using a standard checklist from WHO. The report is available and was shared with the NTP and the writing team of FR proposal.
Met
39
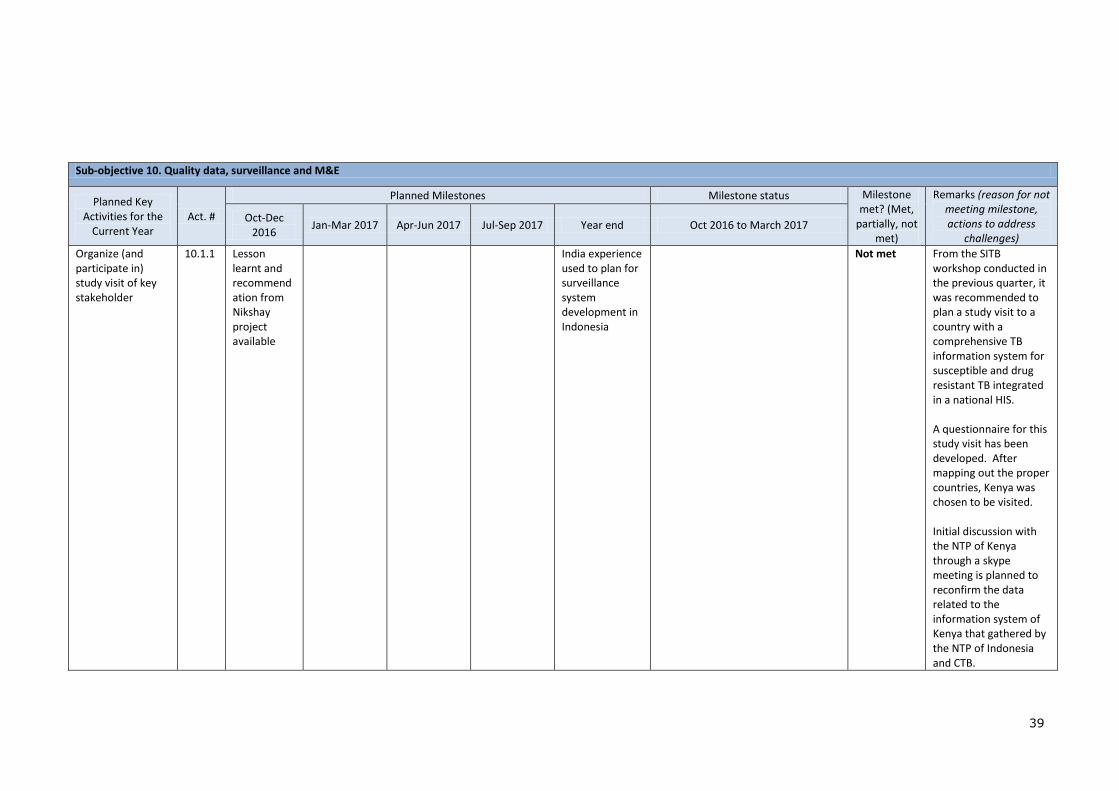
Sub-objective 10. Quality data, surveillance and M&E
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Organize (and participate in) study visit of key stakeholder
10.1.1 Lesson learnt and recommendation from Nikshay project available
India experience used to plan for surveillance system development in Indonesia
Not met From the SITB workshop conducted in the previous quarter, it was recommended to plan a study visit to a country with a comprehensive TB information system for susceptible and drug resistant TB integrated in a national HIS. A questionnaire for this study visit has been developed. After mapping out the proper countries, Kenya was chosen to be visited. Initial discussion with the NTP of Kenya through a skype meeting is planned to reconfirm the data related to the information system of Kenya that gathered by the NTP of Indonesia and CTB.

40
Update the package of functional requirements and specifications for the new SITB
10.1.2 Functional requirements and specifications for the new SITB agreed by stakeholders
CTB facilitated the NTP to assess implementation of SITT and eTB Manager in 14 districts/cities in 7 provinces and followed up the findings with SITB workshop in November 2016. In this workshop, the functional requirements and specifications for the new SITB was agreed by stakeholders. And in this period, the final draft of the high level document was developed.
Met Next step is the exposure visit to another country, tentatively Kenya to learn from their experiences.
Support to planning of SITB development
10.1.3 Dissemination workshop conducted and SITB development plan agreed
- SITB development plan agreed - Funding secured for effective development of SITB
Not met This activity is postponed until after the study visit
Support existing TB information system (SITT and ETB) including system maintenance
10.1.4 Provincial HIS team established in CTB supported provinces
Lesson learned and success story of CTB project
- Provincial HIS team fully operationalized in providing troubleshooting locally; - Interoperability with SIHA done -Lesson learned and success story of CTB project
The NTP has agreed on the provincial HIS team establishment in CTB supported provinces. The teams are responsible in troubleshooting SITT and eTB Manager and training on SITT and eTB manager. The team will include wasor and System Information staff in the provincial health office. CTB has developed the draft of training material and this will be finalized after dissemination of SITT 10.0.4, the newest version of SITT that complies with the latest country policy changes and reflects the latest WHO definitions. Training of the provincial HIS team is planned for Q3
Partially met
The provincial HIS team will be established in Q3.
41
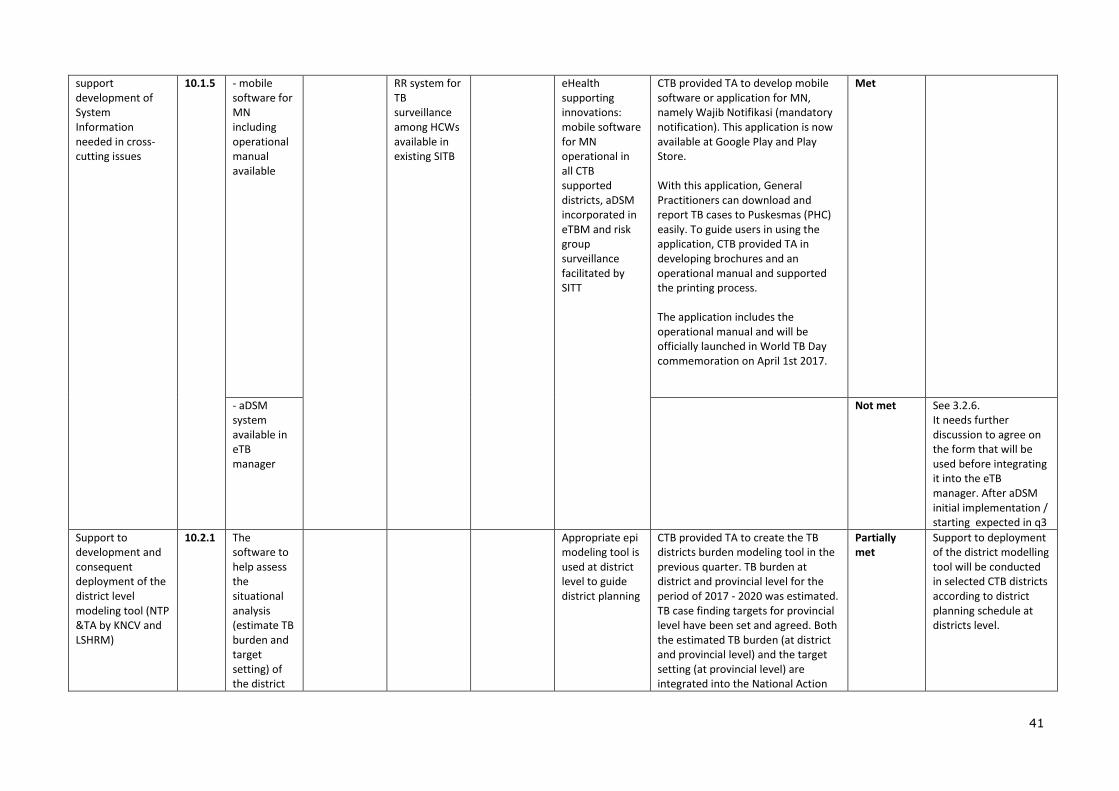
support development of System Information needed in cross-cutting issues
10.1.5 - mobile software for MN including operational manual available
RR system for TB surveillance among HCWs available in existing SITB
eHealth supporting innovations: mobile software for MN operational in all CTB supported districts, aDSM incorporated in eTBM and risk group surveillance facilitated by SITT
CTB provided TA to develop mobile software or application for MN, namely Wajib Notifikasi (mandatory notification). This application is now available at Google Play and Play Store. With this application, General Practitioners can download and report TB cases to Puskesmas (PHC) easily. To guide users in using the application, CTB provided TA in developing brochures and an operational manual and supported the printing process. The application includes the operational manual and will be officially launched in World TB Day commemoration on April 1st 2017.
Met
- aDSM system available in eTB manager
Not met See 3.2.6. It needs further discussion to agree on the form that will be used before integrating it into the eTB manager. After aDSM initial implementation / starting expected in q3
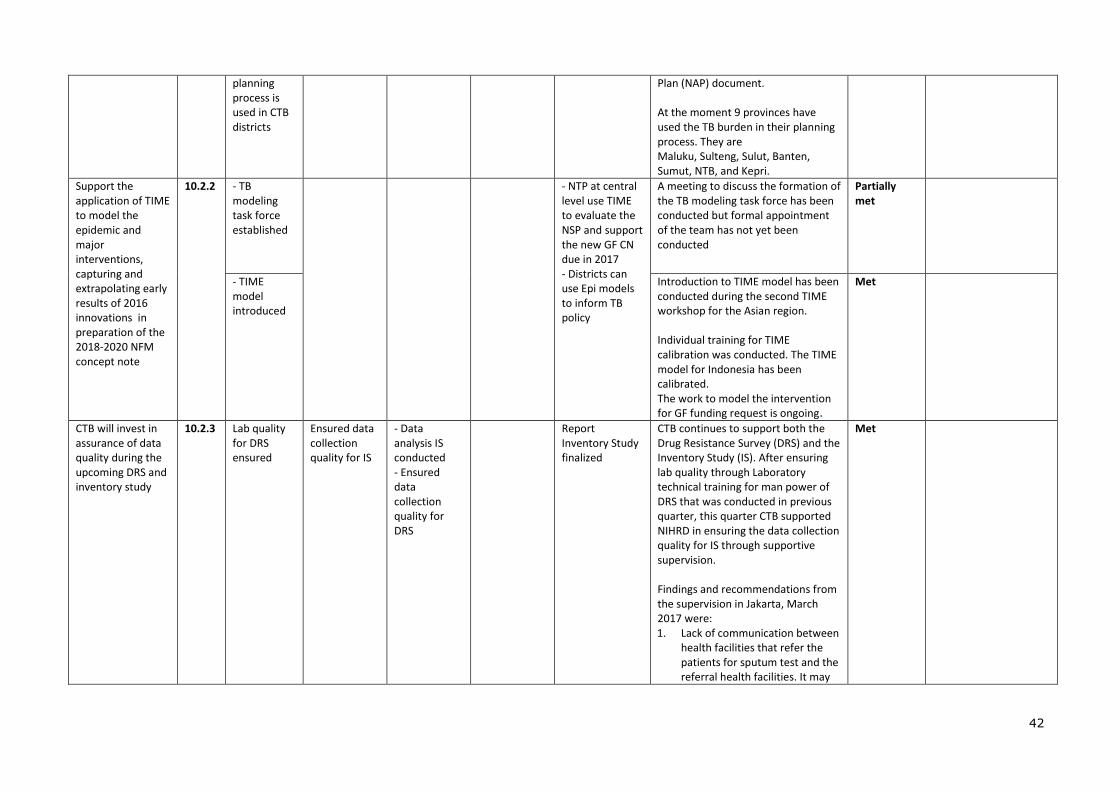
Support to development and consequent deployment of the district level modeling tool (NTP &TA by KNCV and LSHRM)
10.2.1 The software to help assess the situational analysis (estimate TB burden and target setting) of the district
Appropriate epi modeling tool is used at district level to guide district planning
CTB provided TA to create the TB districts burden modeling tool in the previous quarter. TB burden at district and provincial level for the period of 2017 - 2020 was estimated. TB case finding targets for provincial level have been set and agreed. Both the estimated TB burden (at district and provincial level) and the target setting (at provincial level) are integrated into the National Action
Partially met
Support to deployment of the district modelling tool will be conducted in selected CTB districts according to district planning schedule at districts level.
42
planning process is used in CTB districts
Plan (NAP) document. At the moment 9 provinces have used the TB burden in their planning process. They are Maluku, Sulteng, Sulut, Banten, Sumut, NTB, and Kepri.
Support the application of TIME to model the epidemic and major interventions, capturing and extrapolating early results of 2016 innovations in preparation of the 2018-2020 NFM concept note
10.2.2 - TB modeling task force established
- NTP at central level use TIME to evaluate the NSP and support the new GF CN due in 2017 - Districts can use Epi models to inform TB policy
A meeting to discuss the formation of the TB modeling task force has been conducted but formal appointment of the team has not yet been conducted
Partially met
- TIME model introduced
Introduction to TIME model has been conducted during the second TIME workshop for the Asian region. Individual training for TIME calibration was conducted. The TIME model for Indonesia has been calibrated. The work to model the intervention for GF funding request is ongoing.
Met
CTB will invest in assurance of data quality during the upcoming DRS and inventory study
10.2.3 Lab quality for DRS ensured
Ensured data collection quality for IS
- Data analysis IS conducted - Ensured data collection quality for DRS
Report Inventory Study finalized
CTB continues to support both the Drug Resistance Survey (DRS) and the Inventory Study (IS). After ensuring lab quality through Laboratory technical training for man power of DRS that was conducted in previous quarter, this quarter CTB supported NIHRD in ensuring the data collection quality for IS through supportive supervision. Findings and recommendations from the supervision in Jakarta, March 2017 were: 1. Lack of communication between
health facilities that refer the patients for sputum test and the referral health facilities. It may
Met
43
lead to missing cases as the reporting of the result relies on patients. It was recommended for the enumerators to check the result of the test to the referral health facilities proactively.
2. Enumerators did not compare the number of cases of health facilities to the estimated cases that was obtained from the previous mapping. So, advance investigation that may be needed was not captured. It was recommended for enumerators to compare the number of cases to the estimation and do advance investigation if needed.
3. For the hospitals, it was recommended to visit the potential sources of TB cases (inpatients and outpatients departments, MCH clinics, etc) to ensure all TB cases were recorded instead of rely on medical record only.
4. Some questionnaires were not completely filled (date of birth, NIK). It was recommended to put more effort to complete the questionnaire especially for the essential information. Some missing information could be asked to the patients in the next visit.
It was also recommended to conduct routine enumerator’s coordination meeting as part of the quality assurance.
Inclusion of public health research institutes in the
10.2.4 Network established
4 study protocols developed
4 CTB relevant study questions are addressed
Not met The long delayed workshop to develop a national TB research
44
research network activities ( epi training, including support to protocol development, mentoring of study implementation , analysis and international publications by local PI’s)
by local staff, mentored by PH research institutes with CTB TA
network will be conducted in Bogor by Mid-April 2017. The meeting will be financially supported by WHO. CTB provides TA to establish the network and workplan.
Operational Research on better screening algorithms for diagnosis of TB at PKM
10.2.5 Ethical approved obtained
OR started Data analysis finalized
- Most optimal combination of symptoms/risk group and TB screening and diagnosis algorithm for Puskesmas level is identified. - Preparation for Phase 2 started
A series of discussions were conducted between the study team, NTP and the Bogor district health office to finalize the study goals, protocol, tools and the study team structure. Tools were developed: screening forms (informed consent, patient flow card, patient characteristics and screening form, result form), costing tools and qualitative analysis tools. These tools are currently under final review for a pilot in May 2017. Protocol and ethical review forms were filled and are to be submitted to Universitas Padjajaran, West Java, by end of April 2017.
Partially met The study will engage local researchers from several universities (from Universitas Padjajaran West Java as principal investigator, from University of Indonesia as costing analysis expert, and from Sebelas Maret University as qualitative expert).
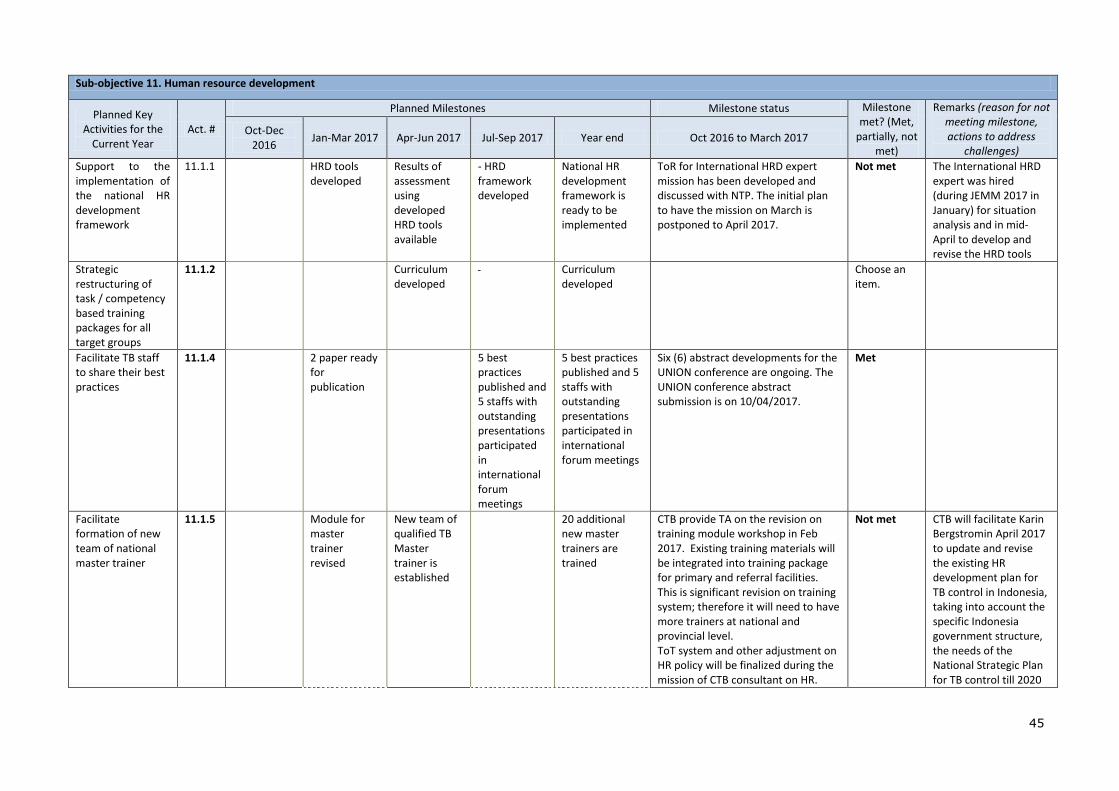
45
Sub-objective 11. Human resource development
Planned Key Activities for the
Current Year Act. #
Planned Milestones Milestone status Milestone met? (Met,
partially, not met)
Remarks (reason for not meeting milestone, actions to address
challenges)
Oct-Dec 2016
Jan-Mar 2017 Apr-Jun 2017 Jul-Sep 2017 Year end Oct 2016 to March 2017
Support to the implementation of the national HR development framework
11.1.1 HRD tools developed
Results of assessment using developed HRD tools available
- HRD framework developed
National HR development framework is ready to be implemented
ToR for International HRD expert mission has been developed and discussed with NTP. The initial plan to have the mission on March is postponed to April 2017.
Not met The International HRD expert was hired (during JEMM 2017 in January) for situation analysis and in mid-April to develop and revise the HRD tools
Strategic restructuring of task / competency based training packages for all target groups
11.1.2 Curriculum developed
Curriculum developed
Choose an item.
Facilitate TB staff to share their best practices
11.1.4 2 paper ready for publication
5 best practices published and 5 staffs with outstanding presentations participated in international forum meetings
5 best practices published and 5 staffs with outstanding presentations participated in international forum meetings
Six (6) abstract developments for the UNION conference are ongoing. The UNION conference abstract submission is on 10/04/2017.
Met
Facilitate formation of new team of national master trainer
11.1.5 Module for master trainer revised
New team of qualified TB Master trainer is established
20 additional new master trainers are trained
CTB provide TA on the revision on training module workshop in Feb 2017. Existing training materials will be integrated into training package for primary and referral facilities. This is significant revision on training system; therefore it will need to have more trainers at national and provincial level. ToT system and other adjustment on HR policy will be finalized during the mission of CTB consultant on HR.
Not met CTB will facilitate Karin Bergstromin April 2017 to update and revise the existing HR development plan for TB control in Indonesia, taking into account the specific Indonesia government structure, the needs of the National Strategic Plan for TB control till 2020

46
and the 8 factors described in the background sections.
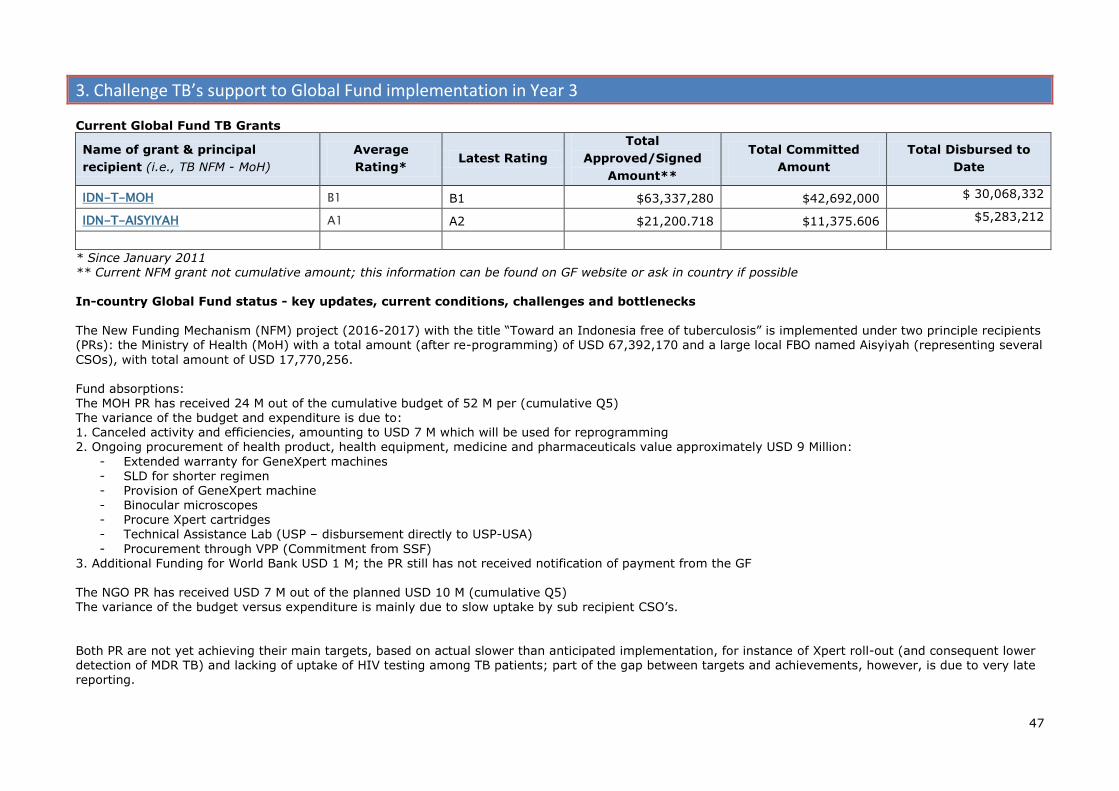
47
3. Challenge TB’s support to Global Fund implementation in Year 3
Current Global Fund TB Grants
Name of grant & principal
recipient (i.e., TB NFM - MoH)
Average
Rating* Latest Rating
Total
Approved/Signed
Amount**
Total Committed
Amount
Total Disbursed to
Date
IDN-T-MOH B1 B1 $63,337,280 $42,692,000 $ 30,068,332
IDN-T-AISYIYAH A1 A2 $21,200.718 $11,375.606 $5,283,212
* Since January 2011 ** Current NFM grant not cumulative amount; this information can be found on GF website or ask in country if possible In-country Global Fund status - key updates, current conditions, challenges and bottlenecks The New Funding Mechanism (NFM) project (2016-2017) with the title “Toward an Indonesia free of tuberculosis” is implemented under two principle recipients (PRs): the Ministry of Health (MoH) with a total amount (after re-programming) of USD 67,392,170 and a large local FBO named Aisyiyah (representing several
CSOs), with total amount of USD 17,770,256. Fund absorptions: The MOH PR has received 24 M out of the cumulative budget of 52 M per (cumulative Q5) The variance of the budget and expenditure is due to: 1. Canceled activity and efficiencies, amounting to USD 7 M which will be used for reprogramming 2. Ongoing procurement of health product, health equipment, medicine and pharmaceuticals value approximately USD 9 Million:
- Extended warranty for GeneXpert machines - SLD for shorter regimen - Provision of GeneXpert machine
- Binocular microscopes - Procure Xpert cartridges - Technical Assistance Lab (USP – disbursement directly to USP-USA)
- Procurement through VPP (Commitment from SSF) 3. Additional Funding for World Bank USD 1 M; the PR still has not received notification of payment from the GF The NGO PR has received USD 7 M out of the planned USD 10 M (cumulative Q5) The variance of the budget versus expenditure is mainly due to slow uptake by sub recipient CSO’s.
Both PR are not yet achieving their main targets, based on actual slower than anticipated implementation, for instance of Xpert roll-out (and consequent lower detection of MDR TB) and lacking of uptake of HIV testing among TB patients; part of the gap between targets and achievements, however, is due to very late reporting.
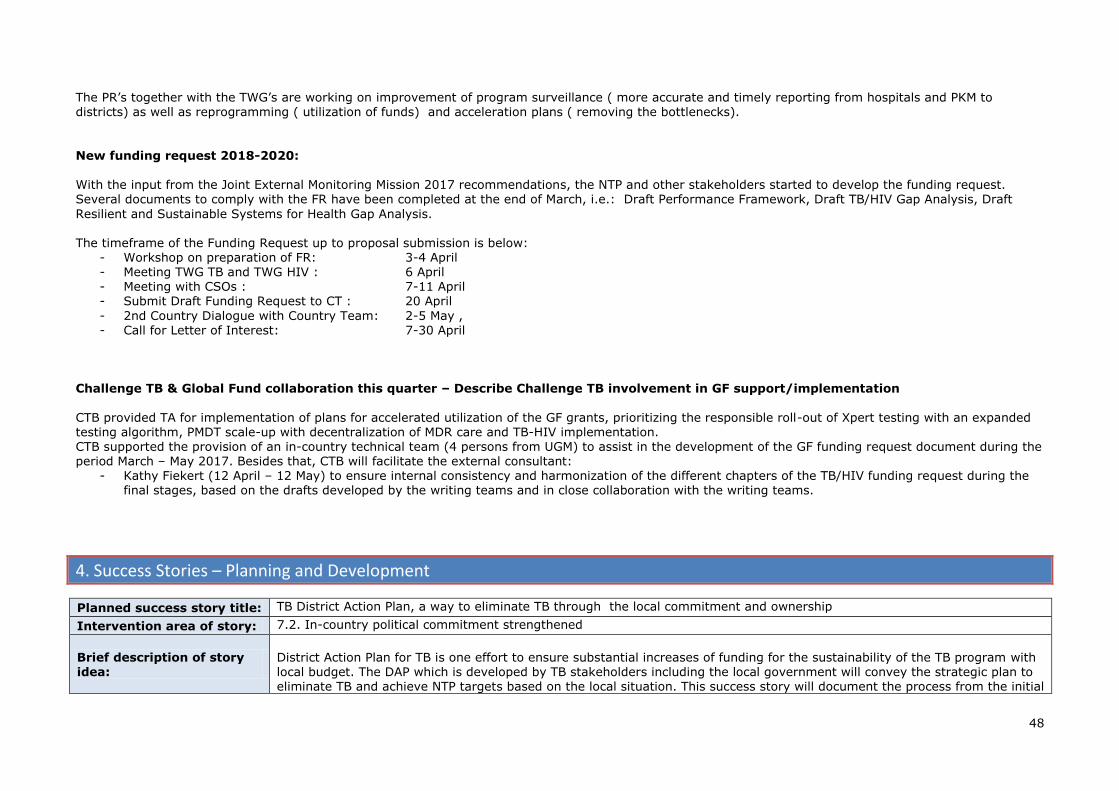
48
The PR’s together with the TWG’s are working on improvement of program surveillance ( more accurate and timely reporting from hospitals and PKM to districts) as well as reprogramming ( utilization of funds) and acceleration plans ( removing the bottlenecks).
New funding request 2018-2020: With the input from the Joint External Monitoring Mission 2017 recommendations, the NTP and other stakeholders started to develop the funding request. Several documents to comply with the FR have been completed at the end of March, i.e.: Draft Performance Framework, Draft TB/HIV Gap Analysis, Draft
Resilient and Sustainable Systems for Health Gap Analysis. The timeframe of the Funding Request up to proposal submission is below:
- Workshop on preparation of FR: 3-4 April - Meeting TWG TB and TWG HIV : 6 April - Meeting with CSOs : 7-11 April - Submit Draft Funding Request to CT : 20 April
- 2nd Country Dialogue with Country Team: 2-5 May , - Call for Letter of Interest: 7-30 April
Challenge TB & Global Fund collaboration this quarter – Describe Challenge TB involvement in GF support/implementation
CTB provided TA for implementation of plans for accelerated utilization of the GF grants, prioritizing the responsible roll-out of Xpert testing with an expanded testing algorithm, PMDT scale-up with decentralization of MDR care and TB-HIV implementation. CTB supported the provision of an in-country technical team (4 persons from UGM) to assist in the development of the GF funding request document during the period March – May 2017. Besides that, CTB will facilitate the external consultant:
- Kathy Fiekert (12 April – 12 May) to ensure internal consistency and harmonization of the different chapters of the TB/HIV funding request during the final stages, based on the drafts developed by the writing teams and in close collaboration with the writing teams.
4. Success Stories – Planning and Development
Planned success story title: TB District Action Plan, a way to eliminate TB through the local commitment and ownership
Intervention area of story: 7.2. In-country political commitment strengthened
Brief description of story idea:
District Action Plan for TB is one effort to ensure substantial increases of funding for the sustainability of the TB program with local budget. The DAP which is developed by TB stakeholders including the local government will convey the strategic plan to eliminate TB and achieve NTP targets based on the local situation. This success story will document the process from the initial

49
advocacy up to the document is legalized and accommodated into the local budget.
Status update (including estimated date of completion):
13 out of 16 districts of CTB area started to develop the District Action Plan. Development stage of each district varies, to
achieve the legalized District Action Plan. 2 cities (Semarang and Solo) finalized the DAP documents and are in the stage to legalize the documents. The Governor of West Java has published the circular letter to all head of districts/cities. The expected time for Solo and Semarang’s DAP process are completed in August 2017.
Planned success story title: Mandatory Notification Apps, raise the case notification by simplify the reporting
Intervention area of story: 10.1. Well-functioning case or patient-based electronic recording and reporting system is in place
Brief description of story
idea:
One of the reasons for private providers unwillingness to notify cases, is because the TB reporting and recording system is not simple. CTB initiated the development of a simple mobile app of TB RR, as the answer of PPs assumption that the TB form is complicated. Through this app, CTB will monitor the participation of PPs, and their contribution in TB case notification
Status update (including estimated date of
completion):
The Mandatory Notification application was officially launched during the TB Day peak event, by the Minister of Health
Republik of Indonesia. The application is available on Google Play Store since February 2017. Before it was launched, 12 PPs has tested this application in West Jakarta. In Q3, CTB will implement the MN app in 5 pilot sites (Bandung City, West
Jakarta, North Jakarta (tentative), Tulungagung, and Medan City). The pilot test is expected to be completed in August 2017.
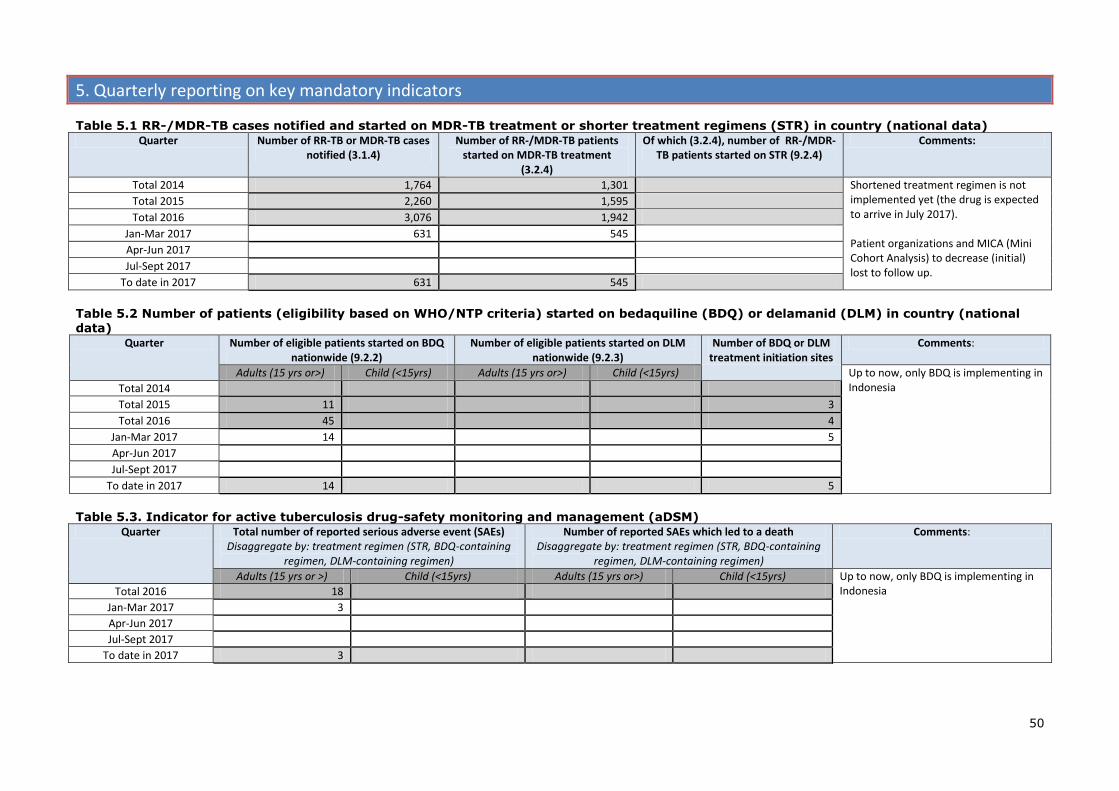
50
5. Quarterly reporting on key mandatory indicators
Table 5.1 RR-/MDR-TB cases notified and started on MDR-TB treatment or shorter treatment regimens (STR) in country (national data) Quarter Number of RR-TB or MDR-TB cases
notified (3.1.4) Number of RR-/MDR-TB patients
started on MDR-TB treatment (3.2.4)
Of which (3.2.4), number of RR-/MDR-TB patients started on STR (9.2.4)
Comments:
Total 2014 1,764 1,301 Shortened treatment regimen is not implemented yet (the drug is expected to arrive in July 2017). Patient organizations and MICA (Mini Cohort Analysis) to decrease (initial) lost to follow up.
Total 2015 2,260 1,595
Total 2016 3,076 1,942
Jan-Mar 2017 631 545
Apr-Jun 2017
Jul-Sept 2017
To date in 2017 631 545
Table 5.2 Number of patients (eligibility based on WHO/NTP criteria) started on bedaquiline (BDQ) or delamanid (DLM) in country (national data)
Quarter Number of eligible patients started on BDQ nationwide (9.2.2)
Number of eligible patients started on DLM nationwide (9.2.3)
Number of BDQ or DLM treatment initiation sites
Comments:
Adults (15 yrs or>) Child (<15yrs) Adults (15 yrs or>) Child (<15yrs) Up to now, only BDQ is implementing in Indonesia Total 2014
Total 2015 11 3
Total 2016 45 4
Jan-Mar 2017 14 5
Apr-Jun 2017
Jul-Sept 2017
To date in 2017 14 5
Table 5.3. Indicator for active tuberculosis drug-safety monitoring and management (aDSM) Quarter Total number of reported serious adverse event (SAEs)
Disaggregate by: treatment regimen (STR, BDQ-containing regimen, DLM-containing regimen)
Number of reported SAEs which led to a death Disaggregate by: treatment regimen (STR, BDQ-containing
regimen, DLM-containing regimen)
Comments:
Adults (15 yrs or >) Child (<15yrs) Adults (15 yrs or>) Child (<15yrs) Up to now, only BDQ is implementing in Indonesia Total 2016 18
Jan-Mar 2017 3
Apr-Jun 2017
Jul-Sept 2017
To date in 2017 3
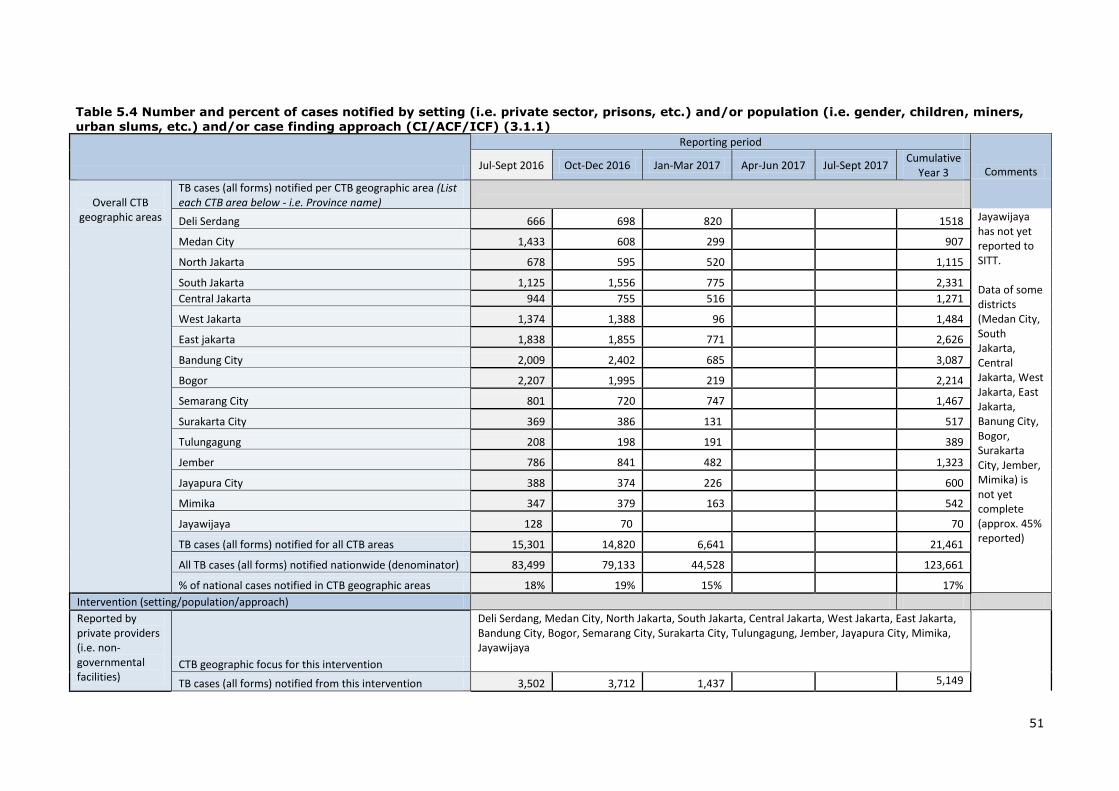
51
Table 5.4 Number and percent of cases notified by setting (i.e. private sector, prisons, etc.) and/or population (i.e. gender, children, miners,
urban slums, etc.) and/or case finding approach (CI/ACF/ICF) (3.1.1)
Reporting period
Comments Jul-Sept 2016 Oct-Dec 2016 Jan-Mar 2017 Apr-Jun 2017 Jul-Sept 2017
Cumulative Year 3
Overall CTB
geographic areas
TB cases (all forms) notified per CTB geographic area (List each CTB area below - i.e. Province name)
Deli Serdang 666 698 820 1518 Jayawijaya has not yet reported to SITT. Data of some districts (Medan City, South Jakarta, Central Jakarta, West Jakarta, East Jakarta, Banung City, Bogor, Surakarta City, Jember, Mimika) is not yet complete (approx. 45% reported)
Medan City 1,433 608 299 907
North Jakarta 678 595 520 1,115
South Jakarta 1,125 1,556 775 2,331
Central Jakarta 944 755 516 1,271
West Jakarta 1,374 1,388 96 1,484
East jakarta 1,838 1,855 771 2,626
Bandung City 2,009 2,402 685 3,087
Bogor 2,207 1,995 219 2,214
Semarang City 801 720 747 1,467
Surakarta City 369 386 131 517
Tulungagung 208 198 191 389
Jember 786 841 482 1,323
Jayapura City 388 374 226 600
Mimika 347 379 163 542
Jayawijaya 128 70 70
TB cases (all forms) notified for all CTB areas 15,301 14,820 6,641 21,461
All TB cases (all forms) notified nationwide (denominator) 83,499 79,133 44,528 123,661
% of national cases notified in CTB geographic areas 18% 19% 15% 17%
Intervention (setting/population/approach)
Reported by private providers (i.e. non-governmental facilities)
CTB geographic focus for this intervention
Deli Serdang, Medan City, North Jakarta, South Jakarta, Central Jakarta, West Jakarta, East Jakarta, Bandung City, Bogor, Semarang City, Surakarta City, Tulungagung, Jember, Jayapura City, Mimika, Jayawijaya
TB cases (all forms) notified from this intervention 3,502 3,712 1,437 5,149

52
All TB cases notified in this CTB area (denominator) 15,301 14,820 6,641 21,461
% of cases notified from this intervention 23% 25% 22% 24%
Children (0-14)
CTB geographic focus for this intervention
Deli Serdang, Medan City, North Jakarta, South Jakarta, Central Jakarta, West Jakarta, East Jakarta, Bandung City, Bogor, Semarang City, Surakarta City, Tulungagung, Jember, Jayapura City, Mimika, Jayawijaya
TB cases (all forms) notified from this intervention 1,693 2,158 543 2,701
All TB cases notified in this CTB area (denominator) 15,301 14,820 6,641 21,461
% of cases notified from this intervention 11% 15% 8% 13% Other (specify)
CTB geographic focus for this intervention
Deli Serdang, Medan City, North Jakarta, South Jakarta, Central Jakarta, West Jakarta, East Jakarta, Bandung City, Bogor, Semarang City, Surakarta City, Tulungagung, Jember, Jayapura City, Mimika, Jayawijaya
TB-HIV ( PLWHIV registered in TB recording-reporting)
TB cases (all forms) notified from this intervention 317 356 162
518
All TB cases notified in this CTB area (denominator) 15,301 14,820 6,641
21,461
% of cases notified from this intervention 2% 2% 2.4%
2.4%

53
6. Challenge TB-supported international visits (technical and management-related trips)
# Partner Name of consultant
Planned quarter Specific mission
objectives
Status (cancelled, pending,
completed)
Dates completed Additional Remarks (Optional) Q1
Q2
Q3
Q 4
1 KNCV Petra de Haas 12 days
1. International TA, stool sample piloting
2. Introduction of LIMS 3. Guiding the way forward re sequencing
Pending It is rescheduled to May 2017
2 KNCV Edine Tiemersma 10 days
1. OR on ICF phase 1 Data Collection and preparation for phase2
2. Drafting interim result of CEM PV BDQ
Pending International TA is scheduled to be done around study pilot phase to allow optimal preparation before Phase 1 implementation (around May-June 2017)
3 KNCV External Consultant TBD
14 days
1. International consultant to support national focal point in developing media and communication strategy for TB control program
Cancelled CTB contracted the local consultant to develop the media and communication strategy.
4 KNCV (2 persons) Kitty van Weezenbeek, Michael Kimerling, TBD
11 days each
CTB will participate in the JEMM in preparation of the new GF concept note development: Kitty van Weezenbeek PMDT and overall NTP, intensified case finding, Michael Kimerling Private sector and research (TBD ON LAB OR IC MOVED TO GF HUB)
Complete 30 Jan – 2 Feb 2017 • Kitty van Weezenbeek • Maarten Van Cleeff
5 KNCV KNCV HQ staff (TBD) 6 days
1.Provide training of Subaward management: staff of 2 GF PR's and CTB project management staff trained, resulting in adequate knowledge and tools to manage subgrants
Cancelled
6 KNCV Job van Rest & Ali Habib
14 days
International Consultant to develop master plan and national landscape/ stakeholders' needs analysis, 2 times
Complete 21-26 November 2016
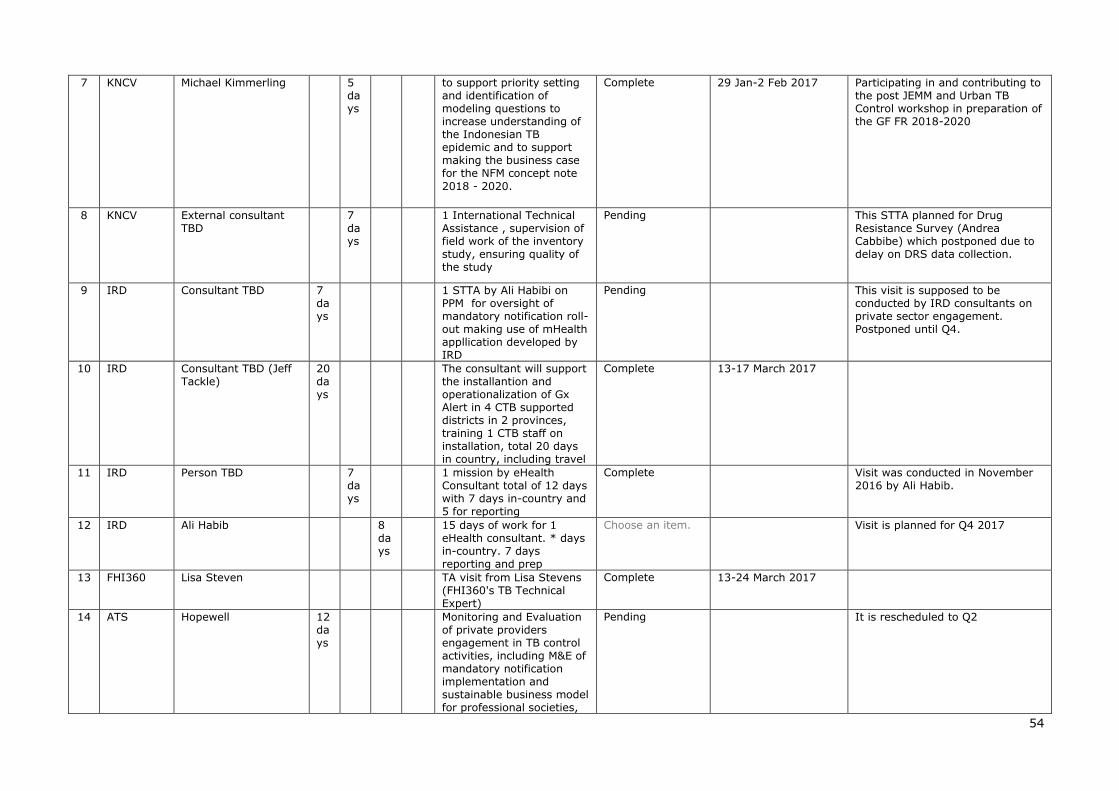
54
7 KNCV Michael Kimmerling 5 days
to support priority setting and identification of modeling questions to increase understanding of the Indonesian TB epidemic and to support making the business case for the NFM concept note
2018 - 2020.
Complete 29 Jan-2 Feb 2017 Participating in and contributing to the post JEMM and Urban TB Control workshop in preparation of the GF FR 2018-2020
8 KNCV External consultant TBD
7 days
1 International Technical Assistance , supervision of field work of the inventory study, ensuring quality of the study
Pending This STTA planned for Drug Resistance Survey (Andrea Cabbibe) which postponed due to delay on DRS data collection.
9 IRD Consultant TBD 7 days
1 STTA by Ali Habibi on PPM for oversight of mandatory notification roll-out making use of mHealth appllication developed by IRD
Pending This visit is supposed to be conducted by IRD consultants on private sector engagement. Postponed until Q4.
10 IRD Consultant TBD (Jeff Tackle)
20 days
The consultant will support the installantion and operationalization of Gx Alert in 4 CTB supported districts in 2 provinces, training 1 CTB staff on installation, total 20 days in country, including travel
Complete 13-17 March 2017
11 IRD Person TBD 7 days
1 mission by eHealth Consultant total of 12 days with 7 days in-country and 5 for reporting
Complete Visit was conducted in November 2016 by Ali Habib.
12 IRD Ali Habib 8 days
15 days of work for 1 eHealth consultant. * days in-country. 7 days reporting and prep
Choose an item. Visit is planned for Q4 2017
13 FHI360 Lisa Steven TA visit from Lisa Stevens (FHI360's TB Technical Expert)
Complete 13-24 March 2017
14 ATS Hopewell 12 days
Monitoring and Evaluation of private providers engagement in TB control activities, including M&E of mandatory notification implementation and sustainable business model for professional societies,
Pending It is rescheduled to Q2
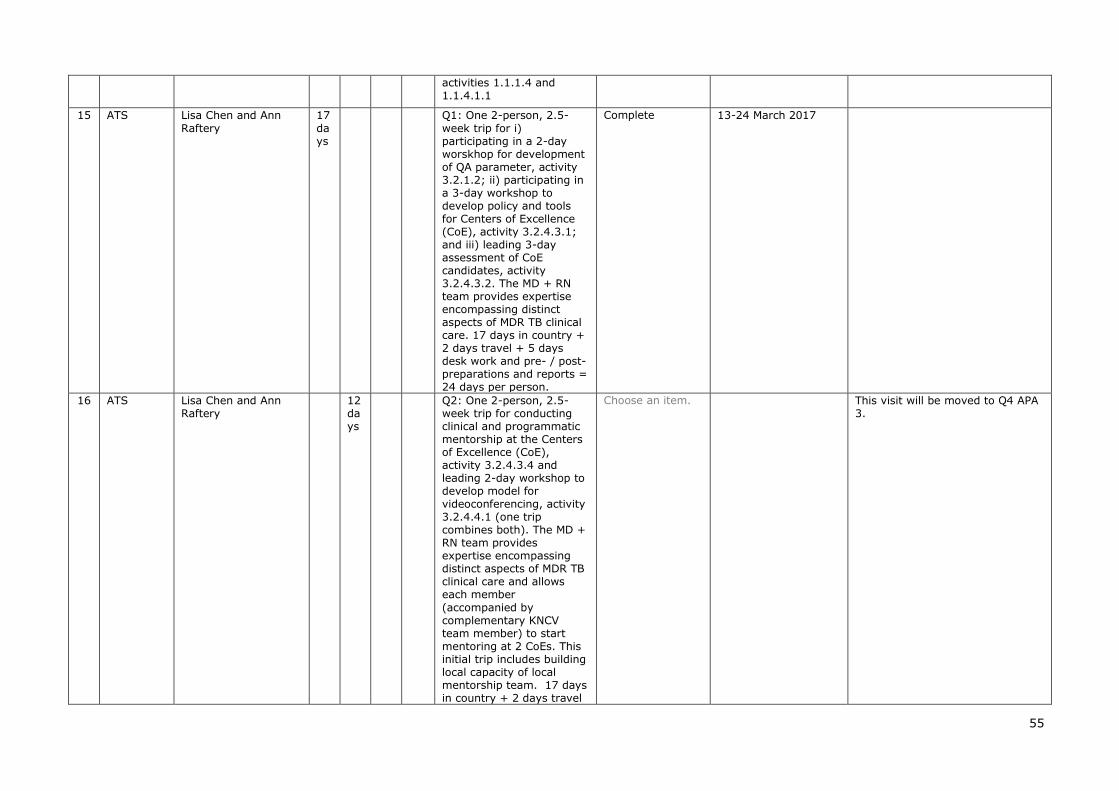
55
activities 1.1.1.4 and 1.1.4.1.1
15 ATS Lisa Chen and Ann
Raftery
17
days
Q1: One 2-person, 2.5-
week trip for i) participating in a 2-day worskhop for development of QA parameter, activity 3.2.1.2; ii) participating in a 3-day workshop to develop policy and tools for Centers of Excellence (CoE), activity 3.2.4.3.1; and iii) leading 3-day assessment of CoE candidates, activity 3.2.4.3.2. The MD + RN team provides expertise encompassing distinct aspects of MDR TB clinical care. 17 days in country + 2 days travel + 5 days desk work and pre- / post- preparations and reports = 24 days per person.
Complete 13-24 March 2017
16 ATS Lisa Chen and Ann Raftery
12 days
Q2: One 2-person, 2.5-week trip for conducting clinical and programmatic mentorship at the Centers of Excellence (CoE), activity 3.2.4.3.4 and leading 2-day workshop to develop model for videoconferencing, activity 3.2.4.4.1 (one trip combines both). The MD + RN team provides expertise encompassing distinct aspects of MDR TB clinical care and allows each member
(accompanied by complementary KNCV team member) to start mentoring at 2 CoEs. This initial trip includes building local capacity of local mentorship team. 17 days in country + 2 days travel
Choose an item. This visit will be moved to Q4 APA 3.

56
+ 4 days desk work and pre- / post- preparations and reports = 23 days per person.
17 ATS 2 person, TBD 12 days
Q4: One 2-person, 2-week trip for continuing clinical and programmatic mentorship at the Centers of Excellence (CoE), activity 3.2.4.3.4 and assessing CoE performance, activity 3.2.4.3.4. The MD + RN team provides expertise encompassing distinct aspects of MDR TB clinical care and allows each member (accompanied by complementary KNCV team member) to conduct assessment of 3 CoEs each then reconvene for next steps. 12 days in country + 2 days travel + 4 days desk work and pre- / post- preparations and reports = 18 days per person.
Choose an item.
Total number of visits conducted (cumulative for fiscal year) 6
Total number of visits planned in approved work plan 17
Percent of planned international consultant visits conducted 35% (6/17)

57
7. Quarterly Indicator Reporting
Sub-objective: 1. Enabling Environment
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
1.1.1. % of notified TB cases, all forms, contributed by non-NTP providers (i.e. private/non-governmental facilities)
CTB Geographical Areas (16 Districts) 1. Non NTP- Public 2. Non NTP-Private
quarterly 16 CTB Districts (2015) Case notification: 58, 847 Non NTP - Public: 31% (18,024/58,847) Non NTP- Private: 20% (11,802/58, 847)
Case notification all form increased 17 % (refer to NTP National Action Plan. Percentage of Non NTP contribution increased at least 5 % from baseline
16 CTB districts Jul-sep 2016 Non NTP Private 23% (3,502/15,301) Non NTP Public 29% (4426/15,301) Oct-Dec 2016 Non NTP private 25% (3,712/14,820) Non NTP Public 28% (4,202/14,820) Jan-Mar 2017 Non NTP private 22% (1,437/6,641) Non NTP Public 23% (1,535/6,641)
Data for Jan-March is uncompleted. Will be updated in next quarter
1.2.1. # of current/ex-TB patient groups engaged at the community level and also linked with the NTP
CTB Geographical Areas ( 6 provinces)
annually 7 (2016) at least 16 Measured Annually
Sub-objective: 2. Comprehensive, high quality diagnostics
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
2.1.2. A current national TB laboratory operational plan exists and is used to prioritize, plan and implement interventions.
National annually 2016 1= operational plan available
3= Operational plan available, implemented and shows progress towards annual targets. If #3 selected, include the proportion of targets in the plan being met at the time of reporting. Possible
Measured Annually
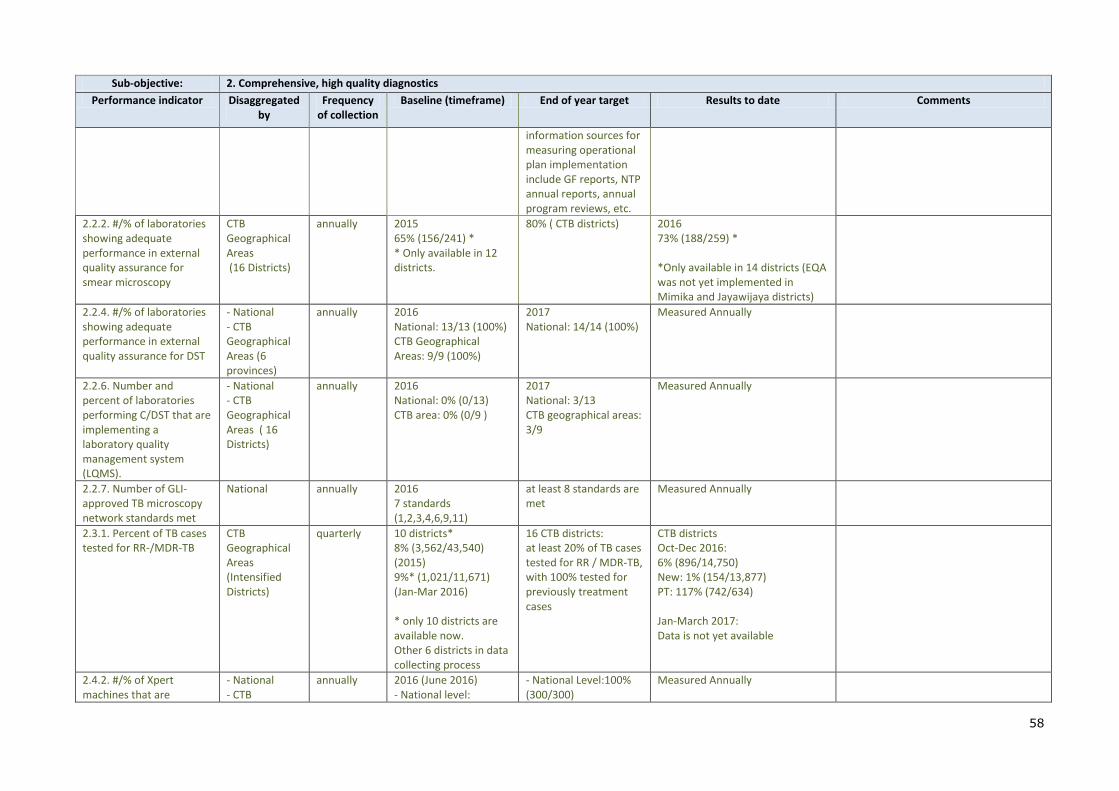
58
Sub-objective: 2. Comprehensive, high quality diagnostics
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
information sources for measuring operational plan implementation include GF reports, NTP annual reports, annual program reviews, etc.
2.2.2. #/% of laboratories showing adequate performance in external quality assurance for smear microscopy
CTB Geographical Areas (16 Districts)
annually 2015 65% (156/241) * * Only available in 12 districts.
80% ( CTB districts) 2016 73% (188/259) * *Only available in 14 districts (EQA was not yet implemented in Mimika and Jayawijaya districts)
2.2.4. #/% of laboratories showing adequate performance in external quality assurance for DST
- National - CTB Geographical Areas (6 provinces)
annually 2016 National: 13/13 (100%) CTB Geographical Areas: 9/9 (100%)
2017 National: 14/14 (100%)
Measured Annually
2.2.6. Number and percent of laboratories performing C/DST that are implementing a laboratory quality management system (LQMS).
- National - CTB Geographical Areas ( 16 Districts)
annually 2016 National: 0% (0/13) CTB area: 0% (0/9 )
2017 National: 3/13 CTB geographical areas: 3/9
Measured Annually
2.2.7. Number of GLI-approved TB microscopy network standards met
National annually 2016 7 standards (1,2,3,4,6,9,11)
at least 8 standards are met
Measured Annually
2.3.1. Percent of TB cases tested for RR-/MDR-TB
CTB Geographical Areas (Intensified Districts)
quarterly 10 districts* 8% (3,562/43,540) (2015) 9%* (1,021/11,671) (Jan-Mar 2016) * only 10 districts are available now. Other 6 districts in data collecting process
16 CTB districts: at least 20% of TB cases tested for RR / MDR-TB, with 100% tested for previously treatment cases
CTB districts Oct-Dec 2016: 6% (896/14,750) New: 1% (154/13,877) PT: 117% (742/634) Jan-March 2017: Data is not yet available
2.4.2. #/% of Xpert machines that are
- National - CTB
annually 2016 (June 2016) - National level:
- National Level:100% (300/300)
Measured Annually

59
Sub-objective: 2. Comprehensive, high quality diagnostics
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
functional in country (stratified by Challenge TB, other)
Geographical Areas (6 provinces)
98% (80/82) - CTB Geographical Areas (6 provinces) 96% (27/28)
- CTB : 100% (245/245)
2.4.5. % unsuccessful Xpert tests
CTB Geographical Areas (6 provinces)
quarterly 2015 - National: 6% (1,001/17,253) - CTB Area (6 provinces): 6% (691/11,510) 2016 (Jan-June 2016) - National : 3,5 % (355/10,180) - CTB area ( 6 Provinces) : 3,1 % (218/6951)
< 5% 6 CTB provinces Okt-Dec 2016: 7% (329/5,037) Jan-Mar 2017 6% (339/6,070)
Sub-objective: 3. Patient-centered care and treatment
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
3.1.1. Number and percent of cases notified by setting (i.e. private sector, pharmacies, prisons, etc.) and/or population (i.e. gender, children, miners, urban slums, etc.) and/or case finding approach
CTB Geographical Areas (16 Districts) By Case Finding Approach 1. TB-DM 2. TB-HIV 3. TB Children 4. CI
quarterly 2015 • TB-DM*: 1% (65/4,714) (only available in Semarang City and Surakarta City) • TB-HIV 2% (742 /43,540) • TB Children 12% (5,222/43,540) • CI: UN
* TB -DM: 5% (in 2 selected districts) * TB HIV: 6% * TB in children: 12% * CI: 1% (in 2 selected districts)
TB-DM Oct-Dec 2016: Data is not available Jan-Mar 2017: 13 (data available only available in 1 hospital & 1 Public Health Center in Semarang city) TB-HIV(16 CTB Districts) Oct-Dec 2016: 2% (356/14,820) Jan-March 2017: 2.4 % (162/6,641) Childhood TB (16 CTB Districts) Oct-Dec 2016: 15% (2,158/14,820) Jan-Mar 2017:
Data Jan-March still not complete.
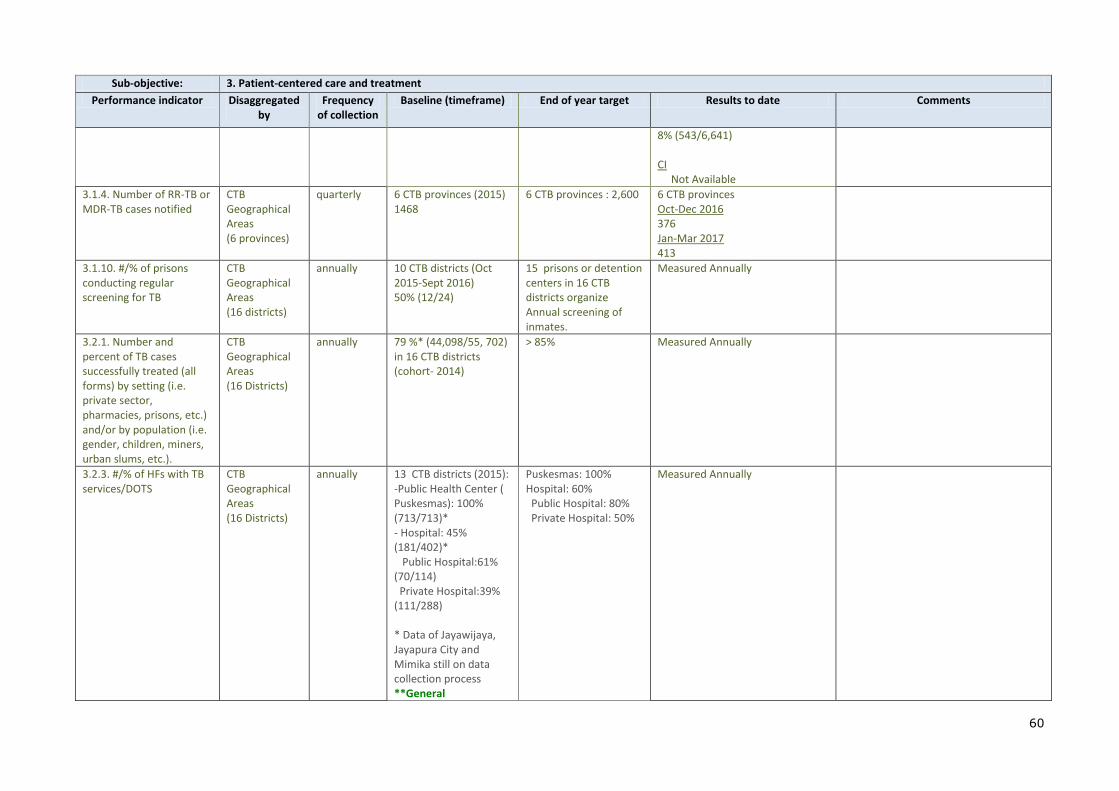
60
Sub-objective: 3. Patient-centered care and treatment
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
8% (543/6,641) CI Not Available
3.1.4. Number of RR-TB or MDR-TB cases notified
CTB Geographical Areas (6 provinces)
quarterly 6 CTB provinces (2015) 1468
6 CTB provinces : 2,600 6 CTB provinces Oct-Dec 2016 376 Jan-Mar 2017 413
3.1.10. #/% of prisons conducting regular screening for TB
CTB Geographical Areas (16 districts)
annually 10 CTB districts (Oct 2015-Sept 2016) 50% (12/24)
15 prisons or detention centers in 16 CTB districts organize Annual screening of inmates.
Measured Annually
3.2.1. Number and percent of TB cases successfully treated (all forms) by setting (i.e. private sector, pharmacies, prisons, etc.) and/or by population (i.e. gender, children, miners, urban slums, etc.).
CTB Geographical Areas (16 Districts)
annually 79 %* (44,098/55, 702) in 16 CTB districts (cohort- 2014)
> 85% Measured Annually
3.2.3. #/% of HFs with TB services/DOTS
CTB Geographical Areas (16 Districts)
annually 13 CTB districts (2015): -Public Health Center ( Puskesmas): 100% (713/713)* - Hospital: 45% (181/402)* Public Hospital:61% (70/114) Private Hospital:39% (111/288) * Data of Jayawijaya, Jayapura City and Mimika still on data collection process **General
Puskesmas: 100% Hospital: 60% Public Hospital: 80% Private Hospital: 50%
Measured Annually
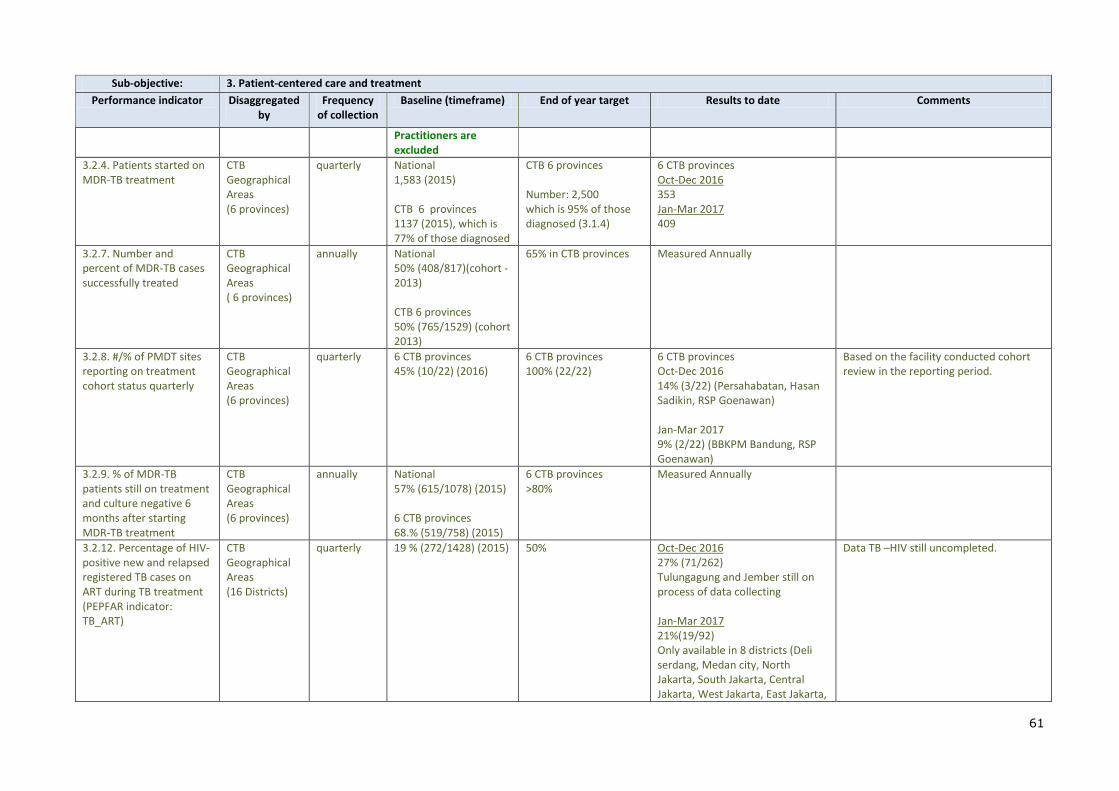
61
Sub-objective: 3. Patient-centered care and treatment
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
Practitioners are excluded
3.2.4. Patients started on MDR-TB treatment
CTB Geographical Areas (6 provinces)
quarterly National 1,583 (2015) CTB 6 provinces 1137 (2015), which is 77% of those diagnosed
CTB 6 provinces Number: 2,500 which is 95% of those diagnosed (3.1.4)
6 CTB provinces Oct-Dec 2016 353 Jan-Mar 2017 409
3.2.7. Number and percent of MDR-TB cases successfully treated
CTB Geographical Areas ( 6 provinces)
annually National 50% (408/817)(cohort -2013) CTB 6 provinces 50% (765/1529) (cohort 2013)
65% in CTB provinces Measured Annually
3.2.8. #/% of PMDT sites reporting on treatment cohort status quarterly
CTB Geographical Areas (6 provinces)
quarterly 6 CTB provinces 45% (10/22) (2016)
6 CTB provinces 100% (22/22)
6 CTB provinces Oct-Dec 2016 14% (3/22) (Persahabatan, Hasan Sadikin, RSP Goenawan) Jan-Mar 2017 9% (2/22) (BBKPM Bandung, RSP Goenawan)
Based on the facility conducted cohort review in the reporting period.
3.2.9. % of MDR-TB patients still on treatment and culture negative 6 months after starting MDR-TB treatment
CTB Geographical Areas (6 provinces)
annually National 57% (615/1078) (2015) 6 CTB provinces 68.% (519/758) (2015)
6 CTB provinces >80%
Measured Annually
3.2.12. Percentage of HIV-positive new and relapsed registered TB cases on ART during TB treatment (PEPFAR indicator: TB_ART)
CTB Geographical Areas (16 Districts)
quarterly 19 % (272/1428) (2015) 50% Oct-Dec 2016 27% (71/262) Tulungagung and Jember still on process of data collecting Jan-Mar 2017 21%(19/92) Only available in 8 districts (Deli serdang, Medan city, North Jakarta, South Jakarta, Central Jakarta, West Jakarta, East Jakarta,
Data TB –HIV still uncompleted.
62
Sub-objective: 3. Patient-centered care and treatment
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
and Semarang city)
3.2.13. Percentage of registered new and relapse TB cases with documented HIV status (PEPFAR indicator: TB_STAT)
CTB Geographical Areas (16 Districts)
quarterly 18 % (10,354/58, 847) (2015)
50% Oct-Dec 2016 16% (2,364/14,602) Tulungagung and Jember still on process of data collecting Jan-Mar 2017 26%(1037/3,924) Only available in 8 districts (Deli serdang, Medan city, North Jakarta, South Jakarta, Central Jakarta, West Jakarta, East Jakarta, and Semarang city)
Data TB –HIV still uncompleted.
Sub-objective: 5. Infection control
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
5.1.3. #/% of health facilities implementing FAST
CTB Geographical Areas (Intensified Districts)
annually 0% (0/22) 70% of PMDT sites in CTB supported districts implement FAST
Measured Annually
5.2.3. Number and % of health care workers diagnosed with TB during reporting period
CTB Geographical Areas (Intensified Districts)
annually Data not available yet in the system surveillance.
Not Applicable to set the target
Measured Annually
Sub-objective: 6. Management of latent TB infection
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
6.1.7. #/% eligible PLHIV with LTBI started on preventive treatment
CTB Geographical Areas (16 Districts)
annually 55% (163 /299) (2014) CTB districts
75% Measured Annually
6.1.11. Number of CTB annually TBD (available after at least 500 in CTB Measured Annually

63
Sub-objective: 6. Management of latent TB infection
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
children under the age of 5 years who initiate IPT
Geographical Areas (16 Districts)
district planning) areas.
Sub-objective: 7. Political commitment and leadership
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
7.2.1. % of NTP budget financed by domestic resources
CTB Geographical Areas (Intensified Districts)
annually 2016 Local budget allocation for TB : USD 291,774 (13 districts)* *)Data only available on local goverment budget, other source not available. Data for Jayapura city, Jayawijaya and Mimika are not available yet."
at least 10% increase for 2018 budget
Measured Annually
7.2.3. % of activity budget covered by private sector cost share, by specific activity
CTB Geographical Areas (Intensified Districts)
annually 2016 : 0% No activity budget covered by private sector yet in APA 2/2016
at least 5% of specific activity of CTB covered by private sector
Measured Annually
Sub-objective: 8. Comprehensive partnerships and informed community involvement
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
8.1.3. Status of National Stop TB Partnership
National annually 1= National Stop TB Partnership established, and has adequate organizational structure; and a secretariat is in place that plays a facilitating
3= National Stop TB Partnership established, has adequate organizational structure, has developed detailed charter/plan, meets
Measured Annually

64
Sub-objective: 8. Comprehensive partnerships and informed community involvement
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
role, and signed a common partnering agreement with all partners; but does not have detailed charter/plan, and does not meet regularly/ produce deliverables;
regularly and critical deliverables are produced
8.1.4. % of local partners' operating budget covered by diverse non-USG funding sources
CTB Geographical Areas
annually Unavailable ( will be available after local partners contracted-estimated after APA 3 WP approved)
<50% Measured Annually
8.2.1. Global Fund grant rating
National annually June 2016 - MoH: B1 - Aisyiyah: A1
- MoH : A2 - Aisyiyah: A1
Measured Annually
Sub-objective: 9. Drug and commodity management systems
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
9.1.1. Number of stock outs of anti-TB drugs, by type (first and second line) and level (ex, national, provincial, district)
CTB Geographical Areas (16 Districts) 1. FLD ( District Level) 2. SLD (District Level)
quarterly Jan-Mar 2016 (10 CTB districts) 1.FLD (District Level) Cat 1: 0 Cat 2: 1 city (Bandung City) Children: 1 (Bandung City) 2. SLD (District Level)= 1 city (Semarang City) New 6 additional districts in progress of data collection
No stock out in CTB areas (16 Districts)
CTB districts Oct-Dec 2016: FLD Cat 1: 0 Cat 2: 0 Children: 0 SLD: 0
9.2.2. Number of patients (eligibility based on
National quarterly National (2015) 16 patients
>100 National 2016

65
Sub-objective: 9. Drug and commodity management systems
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
WHO/NTP criteria) started on bedaquiline
45 2017 14
9.2.3. Number of patients (eligibility based on WHO/NTP criteria) started on delamanid
National quarterly 0 20 NA Treatment with Delamanid has not initiated yet
9.2.4. Number of MDR-TB patients started on shortened treatment regimens
National quarterly 0 800 NA Treatment with shorter regiment has not initiated yet
Sub-objective: 10. Quality data, surveillance and M&E
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
10.1.4. Status of electronic recording and reporting system
National annually 3=a patient/case-based, real-time ERR system functions at national and subnational levels for both TB and MDR-TB
4= a patient/case-based, real-time ERR system is functional at national and subnational levels for both TB and MDR-TB completely and meets WHO standard for TB surveillance data quality - i.e., data in the national database are accurate, complete, internally consistent, within timelines set, validated and free of duplicates and a data quality audit system is put in place (source: Standards and Benchmarks for
Measured Annually

66
Sub-objective: 10. Quality data, surveillance and M&E
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
Tuberculosis Surveillance and Vital Registration Systems – Checklist and User Guide, WHO, 2014).
10.2.1. Standards and benchmarks to certify surveillance systems and vital registration for direct measurement of TB burden have been implemented
National annually Latest assessment in 2013
2017 Measured Annually
10.2.6. % of operations research project funding provided to local partner (provide % for each OR project)
CTB Geographical Areas
annually 0 (2015) TBD Measured Annually
10.2.7. Operational research findings are used to change policy or practices (ex, change guidelines or implementation approach)
CTB Geographical Areas
annually 0 8 Measured Annually
Sub-objective: 11. Human resource development
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
11.1.3. Number of healthcare workers trained, by gender and technical area
CTB Geographical Areas (16 Districts)
quarterly TBD ( after district planning)
not applicable to set the target
Jan-Mar 2017 M: 49 F: 162
SO M F
1 12 10
2 37 152
11.1.5. % of USAID TB funding directed to local
CTB Geographical
annually unavailable not applicable to set the target
Measured Annually
67
Sub-objective: 11. Human resource development
Performance indicator Disaggregated by
Frequency of collection
Baseline (timeframe) End of year target Results to date Comments
partners Areas (16 Districts)