Ch 20 Manter Gatz s Essentials of Clinical Neuroanatomy and Neurophysiology
27
EDITION 10 Manter and Gatz’s Essentials of Clinical Neuroanatomy and Neurophysiology
description
um capítulo apenas.
Transcript of Ch 20 Manter Gatz s Essentials of Clinical Neuroanatomy and Neurophysiology

EDITION 10
Manter and Gatz’s Essentials ofClinical Neuroanatomy
and Neurophysiology
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 1/12 Pg: i COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 1/12 Pg: i BLACK Team:

EDITION 10
Manter and Gatz’s Essentials ofClinical Neuroanatomy
and Neurophysiology
Sid Gilman, MD, FRCPWilliam J. Herdman Professor and ChairDepartment of NeurologyUniversity of Michigan Medical SchoolAnn Arbor, Michigan
Sarah WinansNewman, PhDProfessor EmeritaDepartment of Anatomy and Cell BiologyUniversity of Michigan Medical SchoolCourtesy ProfessorPsychology DepartmentCornell UniversityIthaca, New York
Illustrations by Margaret Croup Brudon
F.A. Davis PublishersPhiladelphia
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 3/12 Pg: iii COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 3/12 Pg: iii BLACK Team:

F. A. Davis Company1915 Arch StreetPhiladelphia, PA 19103www.fadavis.com
Copyright 2003 by F. A. Davis Company
Copyright 1958, 1961, 1966, 1970, 1975, 1982, 1987, 1992, and 1996 by F.A. Davis Company. All rights reserved.This book is protected by copyright. No part of it may be reproduced, stored in a retrieval system, or transmitted inany form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without written permissionfrom the publisher.
Printed in the United States of America
Last digit indicates print number: 10 9 8 7 6 5 4 3 2 1
Acquisitions Editor: Margaret BiblisDevelopmental Editor: Anne SeitzProduction Editor: Nwakaego Fletcher-PerryCover Designer: Louis Forgione
As new scientific information becomes available through basic and clinical research, recommended treatments anddrug therapies undergo changes. The author(s) and publisher have done everything possible to make this book accu-rate, up to date, and in accord with accepted standards at the time of publication. The author(s), editors, and publisherare not responsible for errors or omissions or for consequences from application of the book, and make no warranty,expressed or implied, in regard to the contents of the book. Any practice described in this book should be appliedby the reader in accordance with professional standards of care used in regard to the unique circumstances that mayapply in each situation. The reader is advised always to check product information (package inserts) for changesand new information regarding dose and contraindications before administering any drug. Caution is especially urgedwhen using new or infrequently ordered drugs.
Library of Congress Cataloging-in-Publication Data
Gilman, Sid.Manter and Gatz’s essentials of clinical neuroanatomy and
neurophysiology.—10th ed. / Sid Gilman, Sarah Winans Newman.p. ; cm.
Includes bibliographical references and index.ISBN 0-8036-0772-5 (paper cover)1. Neuroanatomy. 2. Neurophysiology.[DNLM: 1. Nervous System—anatomy & histology. 2. Nervous System
Physiology. WL 100 G487m 2003] I. Title: Essentials of clinicalneuroanatomy and neurophysiology. II. Manter, John Tinkham, 1910- III.Gatz, Arthur John, 1907- IV. Newman, Sarah Winans. V. Title.
QM451 .G47 2003612.8—dc21 2002067443
Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, isgranted by F. A. Davis Company for users registered with the Copyright Clearance Center (CCC) Transactional Re-porting Service, provided that the fee of $.10 per copy is paid directly to CCC, 222 Rosewood Drive, Danvers, MA01923. For those organizations that have been granted a photocopy license by CCC, a separate system of payment hasbeen arranged. The fee code for users of the Transactional Reporting Service is:8036-0772/03 + $.10.
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 4/12 Pg: iv COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 4/12 Pg: iv BLACK Team:

Preface to the 10th Edition
In the six years since the ninth edition of this bookwas published, neuroscience has continued toprogress at an astonishingly rapid rate. Moreover,the remarkable advances in basic neuroscience ofthe past three decades have been translated intoclinical advances that have begun to change themanagement of many neurological diseases. Wenow have means of treating disorders that previ-ously defied even symptomatic benefit. For ex-ample, we have an array of medications availablefor Parkinson’s disease, epilepsy, stroke, sleepdisorders, multiple sclerosis, migraine headache,and neuromuscular disorders such as myastheniagravis, myositis, and peripheral neuropathy. Wealso have symptomatic treatments for Alzhei-mer’s disease, and from the current pace ofresearch in this disorder, it appears that preven-tive therapies will become available within thenext decade. The armamentarium for diagnosis ofneurological disorders has also advanced, includ-ing an array of imaging studies for examining thestructure and function of the nervous system.These approaches have proved invaluable notonly in the diagnosis of neurological disorders,but also in understanding some of the mostcomplex functions of the normal brain.
We undertook the present revision to updatethe book scientifically. To this end, we addedconsiderable new material concerning neuroanat-omy, neurophysiology, and neuropharmacology,and yet attempted to keep the book short andsuccinct. To accomplish this, we shortened andconsolidated some of the existing material, in-cluding the presentations of the structure andfunction of the brain stem and thalamus. We haverewritten literally every chapter. We changed
many of the illustrations in keeping with the newinformation presented, and added several newillustrations.
We also added two new features in keepingwith our longstanding aim of making the bookrelevant to clinical practice. We present a clinicalcase briefly at the beginning of many chapters toillustrate the practical utility of the informationcontained in that chapter. These real cases poseproblems of localization of disease process, typeof pathology causing the symptoms, and manage-ment of the patient. We present follow-up mate-rial on these cases at the end of the chapter. Wealso added magnetic resonance images takenfrom neurologically normal adult humans, both toillustrate structural relationships and to give ourreaders experience in viewing clinical imagingstudies. Throughout the current revision we haveemphasized physiological concepts within thecontext of the anatomic organization of thenervous system and pointed out the clinicalrelevance of the major anatomic structures. Wekept the book focused on the student who seeks abrief, clinically oriented overview of neuroanat-omy and neurophysiology that summarizes thematerial in more comprehensive textbooks. Weintended the book to be helpful to house officersin neurology, neurosurgery, otolaryngology, psy-chiatry, and physical medicine and rehabilitationwho wish to update their knowledge. We alsoprovided an approach that will be useful tophysical therapists, speech pathologists, andnurses.
Sid Gilman, MD, FRCPSarah Winans Newman, PhD
v
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 5/12 Pg: v COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 5/12 Pg: v BLACK Team:

Acknowledgments:Consultants for the 10th Edition
We thank the colleagues listed below who graciously gave us their valuable time to reviewmanuscript sections, suggest revisions, and advise us on appropriate references for updatingthis edition. We do not hold these individuals responsible for any material in the final revisionof this book. The authors take full responsibility.
We give special thanks to the Department of Radiology of the University of Michigan andto Dr. Diana Gomez-Hassan, who not only contributed her time and expertise, but also selectedthe magnetic resonance images of neurologically normal individuals and prepared them forour use.
We also thank Margaret Croup Brudon, who revised some of her previous illustrations andprovided new illustrations, all of which are superb.
Harold P. Adams, MDDepartment of NeurologyUniversity of Iowa Hospitals
James W. Albers, MD, PhDDepartment of NeurologyUniversity of Michigan Medical School
Roger L. Albin, MDDepartment of NeurologyUniversity of Michigan Medical School
Robert W. Baloh, MDReed Neurological Research CenterUniversity of California, Los Angeles
Louis R. Caplan, MDDepartment of NeurologyBeth Israel Deaconess Medical Center
Antonio R. Damasio, MD, PhDDepartment of NeurologyUniversity of Iowa
Norman L. Foster, MDDepartment of NeurologyUniversity of Michigan Medical School
Diana Gomez-Hassan, MD, PhDDepartment of RadiologyUniversity of Michigan Medical School
Susan Hickenbottom, MDDepartment of NeurologyUniversity of Michigan Medical School
Jaideep Kapur, MD, PhDDepartment of NeurologyUniversity of Virginia HSC
Golda Kevetter Leonard, PhDDepartment of OtolaryngologyUniversity of Texas Medical Branch, Galveston
Richard J. Krauzlis, PhDSalk Institute
Allan I. Levey, MD, PhDDepartment of NeurologyEmory University
William Z. Rymer, MD, PhDRehabilitation Institute of Chicago
Jeremy D. Schmahmann, MDDepartment of NeurologyMassachusetts General Hospital
Steven Telian, MDDepartment of OtolaryngologyUniversity of Michigan Medical School
Roy Twyman, MDR.W. Johnson Pharmaceutical Research Institute
vii
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 7/12 Pg: vii COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 7/12 Pg: vii BLACK Team:

Contents
Section 1 BASIC PRINCIPLES 1
Chapter 1 Introduction to the NervousSystem 1
Nerve Cells and Nerve Fibers 1Organization of Cells and Fibers in the
Nervous System 3Functionally Defined Fiber Groups in the
Peripheral Nerves 3Overview of the Gross Anatomy of the
Nervous System 4Internal Anatomy of the Spinal Cord 9Development of the Nervous System 11
Chapter 2 Physiology of Nerve Cells 15Resting Membrane Potential 15Ion Channels Control Membrane
Potential 16Action Potential 16Action Current 18Afterpotentials and Refractory Periods Follow
the Action Potential 18Synapses 19Neuromuscular Junction 21
Section 2 PERIPHERAL NERVOUSSYSTEM 23
Chapter 3 Fibers of the SpinalNerves 23
Functional Classification 23Physiologic Classification 25
Chapter 4 Spinal Reflexes and MuscleTone 27
Spinal Reflexes 27Muscle Spindles 27Alpha, Beta, and Gamma Motoneurons of the
Spinal Cord 29Stretch Reflex 30Golgi Tendon Organs and Their Reflexes 30Muscle Tone 31Reflexes of Cutaneous Origin 31
Chapter 5 Autonomic NervousSystem 33
The Autonomic Nervous System Has TwoDivisions 33
Sympathetic Nervous System 34Parasympathetic Nervous System 36Autonomic Innervation of the Genitourinary
System 36Autonomic Reflexes of Other Pelvic
Viscera 38
Section 3 ASCENDING ANDDESCENDING PATHWAYS 41
Chapter 6 Pain and Temperature 41Somatic Sensation 41Overview of the Pathways for Pain, Thermal
Sense, and Touch 42Dorsal Roots of the Spinal Nerves Supply
Dermatomes 42Adjacent Spinal Nerves Form Peripheral
Nerves 42Pain-Temperature Pathways 42Perception of Pain 47Temperature Sense 47Visceral Pain Pathways and Referred
Pain 47Effect of Cutting the Spinothalamic
Tract 48Sensory Effects of Dorsal Root Irritation 48Endogenous Analgesia 49Central Pain (Thalamic Syndrome) 49
Chapter 7 Proprioception, Touch, andTactile Discrimination 51
Central Nervous System Pathways 51Physiologic Aspects of Tactile
Discrimination 57Effect of Spinal Cord Lesions on Touch
Sensation 58
Chapter 8 Motor Pathways 60Motor Areas of the Cerebral Cortex 60
ix
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 9/12 Pg: ix COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 9/12 Pg: ix BLACK Team:

Descending Fibers from the Cerebral Cortexand Brain Stem Influence MotorActivity 61
Role of Lateral, Medial, and PropriospinalPathways in Spinal Cord Function 66
Chapter 9 Lesions of the Peripheral Nerves,Spinal Nerve Roots, and Spinal Cord 68
Degeneration and Regeneration of NerveCells and Fibers after Injury 68
Clinical Consequences of Peripheral NerveLesions 69
Lower Motoneuron Lesions: HypotonicParalysis of Muscles 69
Lesions of Dorsal Roots 69Upper Motoneuron Lesions: Spastic Paralysis
of Muscles 70Abnormal Reflexes Associated with Lesions
of the Motor Pathway 72Transection of the Spinal Cord 73Hemisection of the Spinal Cord (Brown-
Sequard Syndrome) 73Lesions of the Central Gray Matter of the
Spinal Cord 75Lesions Involving the Ventral Horns and the
Corticospinal Tracts 75Lesions Involving Dorsal and Lateral
Funiculi 75Thrombosis of the Anterior Spinal
Artery 75Tumors of the Spinal Cord 76
Section 4 BRAIN STEM ANDCEREBELLUM 77
Chapter 10 Organization of the Brain Stemand Cranial Nerves 77
Surface Anatomy of the Brain Stem 77Internal Structures at the Transition from
Spinal Cord to Brain Stem 82Classification of Cranial Nerve Nuclei and
Fibers according to their Functions 83Functionally Distinct Cranial Nerve Cell
Columns 84Reticular Formation 86Atlas of the Brain Stem: Transverse
Sections 88Blood Supply to the Brain Stem and
Cerebellum 95
Chapter 11 Cranial Nerves of theMedulla 97
Hypoglossal Nerve (XII) 97Accessory Nerve (XI) 97
Vagal System: Nervus Intermedius (VII),Glossopharyngeal (IX), Vagus (X) andCranial Accessory (XI) Nerves 98
Chapter 12 Cranial Nerves of the Pons andMidbrain 104
Abducens Nerve (VI) 104Trochlear Nerve (IV) 105Oculomotor Nerve (III) 105Facial Nerve (VII) 106Trigeminal Nerve (V) 107
Chapter 13 Lesions of the BrainStem 111
Principles of Localization 111Lesions of the Medulla 112Lesions of the Pons 114Lesions of the Midbrain 116Brain Stem Lesions Causing Coma and
‘‘Locked-in’’ Syndrome 118
Chapter 14 Hearing 119Ear 119Central Auditory Pathways 122Diagnosing Hearing Deficits from Nerve
Damage and from ConductiveDefects 124
Auditory Reflexes 125
Chapter 15 Vestibular System 127Vestibular Portion of the Inner Ear 127Vestibular Nerve and Its Central
Connections 129Vestibulocerebellar Connections 130Vestibulospinal Tracts 130Vestibulo-ocular Systems 131Vestibulothalamocortical Pathway 133Sensory Aspects of Vestibular
Stimulation 133
Chapter 16 Cerebellum 135Overview of Cerebellar Function 135Cerebellar Anatomy 135Peduncles 139Major Circuits 141Integration of the Cerebellum and Cerebral
Cortex in Movement and Cognition 143Clinical Signs of Cerebellar
Dysfunction 144Diseases 145
Section 5 FOREBRAIN 147
Chapter 17 Basal Ganglia 147Overview 147
x CONTENTS
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 10/12 Pg: x COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 10/12 Pg: x BLACK Team:

Components 149Connections of the Dorsal Striatum and
Pallidum with the Cerebral Cortex 150Connections of the Pallidum with the Brain
Stem 154Ventral Striatum and Pallidum 154Function and Dysfunction 154
Chapter 18 Vision 158Overview of the Visual Pathways 158Retina 158Visual Pathways 161Information Processing in the Visual
Pathways 163Effects of Lesions Interrupting the Visual
Pathway 164
Chapter 19 Optic Reflexes and EyeMovements 167
Light Reflexes 167Reflexes Associated with the Near-Point
Reaction 168Disorders of Pupillary Function 168Eye Movements 169
Chapter 20 Cerebral Cortex andThalamocortical Connections 174
Cerebral Cortex 174Cortical Cell Layers: The Basis for Structure
and Function Relationships within andbetween Cortical Areas 174
Cortical Networks and InformationProcessing 177
Thalamus 177Thalamocortical Connections 180Functional Cortical Regions 182Disorders of Cortical Networks 189
Chapter 21 Limbic System 193Overview 193Telencephalic Limbic System 193Hypothalamus 197Hypothalamic Functions 200Epithalamus 202
Chapter 22 Olfaction 204Olfactory Receptors 204Olfactory Bulbs and Their Projections 204Olfactory Cortical Areas 206Damage to Olfactory Structures 206
Chapter 23 ChemicalNeuroanatomy 207
Characteristics of NeurotransmitterMolecules 207
Functional Characterization ofNeurotransmitter Receptors 207
Acetylcholine 208Monoamines 209Neuropeptides 214Amino Acids 218
Section 6 CIRCULATION OF BLOODAND CEREBROSPINAL FLUID 221
Chapter 24 Cerebral Arteries Supplying theForebrain 221
Anterior Circulation 221Internal Carotid Artery and Its
Branches 221Posterior Cerebral Artery and Its
Branches 223Formation of the Circle of Willis and Its
Central Branches 225
Chapter 25 Cerebrospinal Fluid 227Formation and Circulation 227Composition and Function 228Blood-Brain Barrier 229Pressure 229
Section 7 APPROACHES TO PATIENTSWITH NEUROLOGIC SYMPTOMS 233
Chapter 26 Clinical Evaluation ofNeurologic Disorders 233
Patient History 234Physical Examination 236Neurologic Examination 236
Chapter 27 Neurologic Diagnostic Tests 241Cerebrospinal Fluid Analysis 241Electroencephalography and Evoked-
Potential Studies 242Nerve Conduction Studies,
Electromyography, and Muscle and NerveBiopsy 243
Anatomic Imaging Studies 244Physiologic Imaging Studies 245
Suggested Readings 247Index 249
CONTENTS XI
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 11/12 Pg: xi COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_fm 5/30/02 5 Pos: 11/12 Pg: xi BLACK Team:

20Cerebral Cortex
and Thalamocortical Connections
Case StudyA 55-year-old man suddenly develops weak-ness of his right arm and leg while at work.When he attempts to tell a coworker about hisweakness, he can speak only slowly and canproduce single words or brief phrases. Hefeels frustrated about his inability to commu-nicate and frightened about the suddenweakness of his limbs. His coworker takeshim immediately to hospital, where a neurolo-gist sees him promptly. On examination, theman can speak only single words such as‘‘weak’’ or short phrases such as ‘‘no painhead.’’ Nevertheless, he understands complexlanguage, as shown by his ability to carryout multiple tasks on command such as‘‘touch your left index finger to your right ear,then close your eyes, then open your mouth.’’The lower right side of his face appears weak,and his right arm and leg have approxi-mately 25% of the strength of his left arm andleg. Deep tendon reflexes on the right sideare decreased compared with the left, and theright plantar response is extensor, the leftflexor. Sensory testing with pinprick, lighttouch, cold, vibration sense, and positionsense reveals no abnormalities.
Where in the nervous system does this pa-tient have a lesion causing his speech diffi-culty and right-sided weakness? What wouldcause this? Is treatment available?
Cerebral CortexThe human brain possesses the capacity toundertake a vast number of intellectual and
cognitive functions. Performing these functionsrequires the circuits of the cerebral cortex to beengaged and to interact with other parts of thenervous system. The cerebral cortex participatesin many aspects of memory storage and recall. Itis necessary for the comprehension and executionof language and for certain special talents such asmusical and mathematic abilities. It participatesin processes responsible for attention, and itcontributes to the perception and conscious pro-cessing of all sensations, as well as to theintegration of sensory inputs from several modal-ities, providing recognition of individuals, ob-jects, and places. The cortex is necessary for theplanning and execution of complex motor activ-ities such as fine digit, hand, and phonatorymovements and for the planning of complexbehavior.
The cerebral cortex is a mantle of gray matteron the surface of the cerebral hemispheres. Withlimited exceptions, the thalamus provides theinput to the cortex, and corticothalamic projec-tions uniformly reciprocate the thalamocorticalconnections. This chapter therefore includes anoverview of the organization of the thalamus andsome details of the thalamocortical relationships.
Cortical Cell Layers: TheBasis for Structure andFunction Relationships withinand between Cortical AreasCells arranged in layers that follow the contoursof the gyri and sulci densely populate the cerebralcortex. The cortex can be divided into regions
174
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 1/19 Pg: 174 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 1/19 Pg: 174 BLACK Team:

based on differences in the number of cell layers.Isocortex contains six layers; allocortex hasthree; and mesocortex, which forms a zonebetween isocortex and allocortex, varies fromthree to six layers. The zone of mesocortex thatborders isocortex contains five to six layers, andthe mesocortex adjacent to allocortex has threeto four. Corticoid, or cortex-like, regions haveneurochemical features and neuronal connec-tions characteristic of cortex, but corticoid areascontain no clearly discernible layering of cells.
Isocortex
The Six Cell Layers of Isocortex Differin Cell Type and Connections
In the human brain, most of the cerebral cortexconsists of isocortex. From the pial surface, thecell layers of isocortex have been named: I,molecular; II, external granular; III, externalpyramidal; IV, internal granular; V, internalpyramidal; and VI multiform (or fusiform).These names refer to the size and shape of the celltypes that predominate in each layer, and thecells’ sizes and shapes, in turn, relate directly totheir input and output connections. Very smallcells (like grains of sand) fill the granular layers;the pyramidal layers contain large neurons withpyramidal shape; and the multiform layer consistsof a variety of cell types, but mostly spindle-shaped (fusiform).
A radial pattern of fibers to and from thecortex, and fibers making connections betweenthe layers of cells of the cortex, organizes thecortex into vertical columns. Afferent fibers tothe cortex run radially toward the surface (i.e.,along the length of the vertical columns). Theydistribute to the small stellate (star-shaped) cells,which can be found in all layers, but theyconstitute the predominant cell type in thegranular layers (II and IV). Input from thethalamus projects primarily to layer IV. Thestellate cells, which are interneurons, makeshort-axon connections within their verticalcolumn to form a great variety of closed process-ing loops.
Efferent projections of pyramidal cells in manylayers, especially those in layer III, coordinateneuronal processing in both adjacent and distantvertical columns of the cortex. These projectionsform interhemispheric connections through thecorpus callosum and intrahemispheric associa-
tion fibers that provide the backbone of func-tional cortical networks. The output of thecolumns to subcortical targets comes from thepyramidal cells of layer V. These cells project tothe basal ganglia, brain stem and spinal cord, andto those thalamic nuclei that have only subcorticaland diffuse cortical connections. Layer VI cellsproject back to the thalamic nuclei that provideinput restricted to a specific cortical area.
Functional Regions of Isocortex Vary inthe Relative Thickness of Their Cell Layers
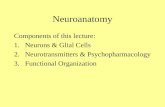
The relative thickness of each of the six corticallayers, and the density of neuron cell bodieswithin each layer vary in different regions of theisocortex. Recognized early in the 20th century,these histologic differences were thought toreflect functional differences. At that time, Brod-mann designated a total of 52 cytoarchitecturallydifferent areas of the isocortex, many of which arenow recognized as functionally distinct and canbe identified by number as part of the standardanatomic nomenclature of the cortex (Figs. 20–1and 20–2).
The term homotypic isocortex refers to iso-cortical areas that form the prototype pattern ofsix well-developed layers of cells, whereas theterm idiotypic isocortex designates those withextreme variations from the homotypic pattern.The primary motor area (MI) and the primarysensory areas consist of idiotypic cortex. MIcontains an enlarged layer V and reduced layers IIto IV, whereas the primary visual, somatosensory,and auditory areas have thick layers II, III, and IVand a relatively thin layer V.
The association areas of the cortex consist ofhomotypic isocortex. Unimodal association ar-eas surround (or lie adjacent to) the primary areas.In these areas, the cells process only one sensorymodality (e.g., visual, auditory, or somatosensoryassociation areas) or deal exclusively with pro-gramming movements (motor association cortex).Lesions of the unimodal sensory association areaslead to complex defects in sensory perception,with the elemental sensations remaining intact.
Heteromodal association areas receive inputfrom multiple unimodal areas. Thus, heteromodalassociation neurons deal with integrated sensoryor sensorimotor contingencies, or, in some cases,fire only in response to stimuli of motivationalsignificance. The heteromodal association areascan be found in the prefrontal region, the posterior
X Figs. 20-20-2
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 175
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 2/19 Pg: 175 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 2/19 Pg: 175 BLACK Team:

FIGURE 20–1. A lateral view of the surface of the brain, showing the numbered Brod-mann’s areas of the cerebral cortex.
FIGURE 20–2. A medial view of the surface of the cerebral hemisphere showing the num-bered Brodmann’s areas of the cerebral cortex.
176
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 3/19 Pg: 176 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 3/19 Pg: 176 BLACK Team:

parietal lobe, and the posterior parts of thetemporal lobe. The heteromodal association areasof the temporal lobe consist of extensions fromthe parietal lobe on both the medial and lateralsurfaces of the hemisphere. Lesions of theheteromodal areas result in complex defectsinvolving both cognitive and affective (emo-tional) components.
Mesocortex, Allocortex,and Corticoid AreasThe mesocortex consists of the paralimbicareas, which surround the medial and basal partsof the cerebral hemispheres. The five paralimbicareas are as follows:
1. Cingulate complex (cingulate gyrus, retro-splenial area, and subcallosal area, whichincludes the paraterminal gyrus).
2. Parahippocampal gyrus.3. Temporal pole.4. Insula.5. Caudal orbitofrontal cortex.
The mesocortex contains three to six layers ofneurons: six in zones that lie adjacent to isocortexand three in zones next to the allocortex. Theallocortex consists of the hippocampal forma-tion and the piriform or primary olfactorycortex. Allocortical areas contain three celllayers.
The corticoid areas include the septal region(deep to the paraterminal gyrus), the substantiainnominata, and parts of the amygdaloidcomplex. These regions lie at the base of theforebrain and contain simple, poorly differenti-ated cortex, which nonetheless shares the neu-rotransmitter and connectional characteristics ofother cortical areas. Allocortical and corticoidareas together make up the limbic telencephalon.(See Chapter 21.)
Cortical Networks andInformation ProcessingOur current understanding of information pro-cessing in the cerebral cortex stems from the con-cept of networks. This view has effectively re-placed the concept of serial, unidirectionalprocessing from primary sensory to association tomotor areas, in the manner of an elaborate reflex
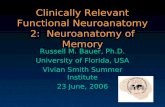
arc. With increasing knowledge of anatomic con-nections in the primate cortex, and the activitypatterns of various cortical areas from human im-aging studies, the concept of parallel processingin large-scale functional networks has emerged.This model of cortical function takes into accountthat heteromodal association areas interconnectreciprocally not only with the unimodal sensoryassociation areas and with each other, but alsowith the paralimbic and limbic areas necessary forlearning, memory, and motivation (Fig. 20–3).The resulting concept focuses on essentially si-multaneous activation of the various nodes in acortical network and in the related subcorticalstructures during cognitive tasks.
Separate but overlapping networks for lan-guage, attention, learning and memory, face-object recognition, and comportment have beenproposed. Functional imaging studies have as-sisted in clarifying not only the normal functionof these networks, but also the basis for neuro-logic and psychiatric disorders in their function.These studies reveal the integral relationship ofparticular cortical areas with specific parts of thethalamus (described here), the basal ganglia (seeChapter 17), and the cerebellum (see Chapter 16).
ThalamusThe diencephalon is an egg-shaped mass of graymatter deep in the brain rostral to the midbrain. Itscomponents include the thalamus, the largestsubdivision, the subthalamus (the subthalamicnucleus is described with the basal ganglia inChapter 17), and the hypothalamus and epithal-amus, both of which are described with the limbicsystem in Chapter 21.
The third ventricle separates the right half ofthe thalamus from the left half, and the telachoroidea, which forms the roof of this ventricle,bears a choroid plexus. In most, but not all,human brains, a small area called the massaintermedia or interthalamic adhesion joins thetwo halves of the thalamus.
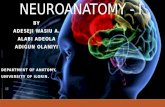
The internal medullary lamina subdividesthe thalamus of each hemisphere into threeunequal parts (Fig. 20–4). This band of myelin-ated fibers separates the medial and lateralnuclear groups from the ventral nuclear groupand bifurcates at its rostral extent to encompass ananterior nuclear group. The internal medullary
X Fig. 20-3
X Fig. 20-4
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 177
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 4/19 Pg: 177 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 4/19 Pg: 177 BLACK Team:

lamina encloses the centromedian and otherintralaminar nuclei. A thin sheet of cells calledthe thalamic reticular nucleus forms the lateralwall of the thalamus. This cell group separates thelateral group of nuclei from the posterior limb ofthe internal capsule. Another narrow band of cellsmaking up the midline nuclei resides on themedial wall of the thalamus, adjacent to the thirdventricle.
The thalamus serves as the station for process-ing and relaying neuronal activity from all typesof peripheral sensory receptors, from the basalganglia, and from the cerebellum to the cerebralcortex. With the exception of the reticular nu-cleus, all thalamic nuclei project to the cerebralcortex (thalamocortical fibers) and receive affer-ents (corticothalamic fibers) from the same cor-tical regions to which they project.
ISOCORTEX
MESOCORTEX
ALLOCORTEX
1 & 2 SENSORY
SENSORY UNIMODALASSOCIATION
HETEROMODALASSOCIATION
PARALIMBIC
LIMBIC
MOTOR UNIMODALASSOCIATION
1 MOTOR
FIGURE 20–3. A simplified view of information processing across the cerebral cortex. Thisdiagram contrasts the primarily unidirectional flow of sensory information through primaryand unimodal association areas with the heavily integrated processing within and betweenheteromodal association, paralimbic, and limbic areas. In the processing of long-termmemory, the flow of activation is bidirectional at every level. (Adapted from Mesulam, MM:Principles of Behavioral and Cognitive Neurology, ed 2. Oxford University Press, New York,2000.)
178 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 5/19 Pg: 178 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 5/19 Pg: 178 BLACK Team:

ILLD
LP
VPM
VL
VA
Ret
Put
C
CC
A
MDI
MDm
MiPI Pm
CCLGN
MGN
OFr
OFc
AC
DL
FEF
MA
1º M
1º SS
GUS
VEST
INS
1º Aud&
Aud A
TP
Vis A
PC
PH
1º Vis
VPL
FIGURE 20–4. Schematic diagram of the relationships of the nuclear groups of the thala-mus. (Right) The topographic thalamocortical projections of the anterior, medial, ventral,and lateral nuclear groups. Reciprocal corticothalamic connections are not shown. (Left)The relationship of reticular nucleus to the thalamocortical and corticothalamic con-nections of one nucleus (VL) is shown as an example. The intralaminar nuclei project to thestriatum (including the ventral striatum) and diffusely to the frontal, parietal, and temporallobes. The light-shaded area is the internal medullary lamina. A = anterior nuclear group;AC = anterior cingulated area; Aud = auditory cortex; AudA = auditory association cortex;C = caudate; cc = corpus callosum; DL = dorsolateral prefrontal cortex; FEF = frontal eyefield; GUS = gustatory cortex; IL = intralaminar nuclei; INS = insula; LD = lateral dorsal nucleus;LGN = lateral geniculate nucleus; LP = lateral posterior nucleus; M = motor cortex;MA = motor association cortex; MDl = lateral part of mediodorsal nucleus; MDm = medialpart of mediodorsal nucleus; MGN = medial geniculate nucleus; Mi = midline nuclei;OFc = caudal orbitofrontal cortex; OFr = rostral orbitofrontal cortex; PC = posterior cingulate;PH = parahippocampal cortex; Pl = lateral pulvinar; Pm = medial pulvinar; Put = putamen;Ret = reticular thalamic nucleus; SS = somatosensory cortex; TP = temporoparietal associa-tion cortex; VA = ventral anterior nucleus; VEST = vestibular cortex; Vis = visual cortex; VisA = visual association cortex; VL = ventral lateral nucleus; VPL = ventral posterolateralnucleus; VPM = ventral posteromedial nucleus. (Adapted from Nieuwenhuys, R, Voogd, J,and van Huijzen, C: The Human Central Nervous System, ed 3. Springer-Verlag, New York,1988.)
179
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 6/19 Pg: 179 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 6/19 Pg: 179 BLACK Team:

ThalamocorticalConnections
Topographic Patternof Thalamocortical ConnectionsThe pattern of the extensive reciprocal connec-tions between thalamus and cortex follows essen-tially a topographic distribution, with rostro-medial and caudolateral parts of the thalamusinterconnected with corresponding regions ofthe cortical mantle. Within this topographicorganization, however, individual thalamic nuclei(or more accurately, subdivisions of individualthalamic nuclei) subserve individual modality-specific, heteromodal, or paralimbic-limbic corti-cal regions.
Figure 20–4 provides a schematic diagramillustrating the topographic pattern of thalamo-cortical relations. Collectively, the midline, ante-rior, and medial nuclei of the thalamus intercon-nect with the limbic and paralimbic cortical areas,as well as with the heteromodal regions of theprefrontal cortex. The ventral thalamic nuclei
project in rostrocaudal order to the modality-specific areas of the frontal lobe (motor cortex),parietal lobe (somatosensory, taste, and vestibularcortices), temporal lobe (auditory cortex), andoccipital lobes (visual cortex). The nuclei of thelateral nuclear group reciprocate connections withthe heteromodal cortex of the posterior parietaland temporal lobes and the unimodal associationcortex for vision.
Internal CapsuleThe thalamocortical fiber system comprises onepart of the total of afferent and efferent fibers ofthe cerebral cortex. Beneath the cortex, theseascending and descending fibers form the coronaradiata in the medullary substance of the hemi-sphere. As they course ventrally from the frontallobe, the most rostral fibers pass down betweenthe head of the caudate nucleus and the rostral endof the lentiform nucleus, to form the anteriorlimb of the internal capsule. Caudally, fiberspassing between the thalamus and the lentiformnucleus form the posterior limb of the internal
FIGURE 20–5. A horizontal section through the cerebrum showing the location of the in-ternal capsule fibers (right) and the various bundles that make up the capsule (left).CC(g) = corpus callosum, genu; CC(s) = corpus callosum, splenium; C(h) = caudate head;C(t) = caudate tail; f = fornix; LV(a) = lateral ventricle, anterior horn; LV(p) = lateral ventri-cle, posterior horn; P = putamen; SP = septum pellucidum; Th = thalamus; III = third ventricle.
180 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 7/19 Pg: 180 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 7/19 Pg: 180 BLACK Team:

capsule. At the level of the interventricularforamen, the transition between the anterior andposterior limbs forms the genu (knee) of theinternal capsule (Figs. 20–5 and 20–6). Descend-ing fibers of the corticospinal tract pass throughthe posterior limb of the internal capsule. Thecorticobulbar fibers, which control the muscles ofthe head, run rostral to the corticospinal fibers.Motor fibers to the upper extremity pass rostral tothose to the lower extremity. Fibers passing to andfrom the frontal lobe, other than pyramidal fibers(e.g., connections of the midline, anterior, andmediodorsal thalamic nuclei with the prefrontalcortex), make up the anterior limb of the internalcapsule. Fibers connecting the ventral thalamuswith the parietal lobe occupy the posterior part ofthe posterior limb of the internal capsule. Opticradiation fibers occupy the retrolenticular por-tion of the internal capsule (i.e., ‘‘behind’’ thelentiform nucleus) (see Fig. 20–5 and 18–3).Auditory radiation fibers project through thesublenticular part of the internal capsule (i.e.,‘‘beneath’’ the lentiform nucleus), which is below
the plane of section in the brain slice pictured inFigure 20–5.
Thalamic Nuclei with Subcorticaland Diffuse Cortical ConnectionsThe midline nuclei of the thalamus consist ofdiffuse, small nuclei surrounding the third ven-tricle. They project to paralimbic and limbiccortices and to the limbic sector of the basalganglia, the ventral striatum.
The intralaminar nuclei consist of numerous,small, diffuse collections of nerve cells within theinternal medullary lamina. In the caudal aspect ofthe lamina, two circumscribed intralaminar nucleican be delineated: the centromedian nucleus,which lies adjacent to the ventral posterior com-plex, and the parafascicular nucleus, locatedjust medial to the centromedian nucleus. Like themidline nuclei, the intralaminar nuclei intercon-nect with basal ganglia circuits. The centrome-dian nucleus receives fibers from the globus palli-dus and area 4 of the cerebrum and projects to theputamen. The parafascicular nucleus receives fi-
f
CP
Th
SP
LV(p)
III
f
ANTERIOR LIMB,INTERNAL CAPSULE
POSTERIOR LIMB,INTERNAL CAPSULE
FIGURE 20–6. A T2-weighted magnetic resonance image of a neurologically normaladult in the axial plane. Compare with Figure 20–5.
Zgs. 20-5 &20-6
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 181
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 8/19 Pg: 181 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 8/19 Pg: 181 BLACK Team:

bers from area 6 of the cerebrum. Its axons projectto the caudate nucleus. In addition, both the cen-tromedian and parafascicular cell groups form to-pographically organized, diffuse projections tothe frontal and parietal lobes important in activat-ing the cortex. The intralaminar nuclei representthe rostral extent of the ascending reticular acti-vating system. They receive bilateral input fromthe brain stem reticular formation and the antero-lateral system of the spinal cord. (See Chapter 6.)
Actually derived from the subthalamus, thethalamic reticular nucleus consists of a thinlayer of cells sandwiched between the posteriorlimb of the internal capsule and the externalmedullary lamina. Unique among thalamic nu-clei, it does not project to the cerebral cortex, butrather, it sends fibers to the thalamic nuclei, thebrain stem reticular formation, and other parts ofthe thalamic reticular nucleus. Nearly all thalamicefferents to the cortex must pass through thislateral sheet of cells, and, in doing so, they sendcollaterals to its neurons. Similarly, corticotha-lamic projections to the thalamic nuclei passthrough the reticular nucleus, where collateralbranches form synapses with its cells. Thus,although not directly connected to the cortex, thereticular nucleus monitors both thalamocorticaland corticothalamic activity. Although still unde-fined, its function appears related to the regulationof thalamic activity. Many thalamic reticularnucleus neurons contain gamma-aminobutyricacid, a finding suggesting that these neurons havelargely inhibitory effects.
Functional Cortical RegionsThe specific connections of individual nuclei ofthe anterior, medial, ventral, and lateral thalamiccell groups are described in the following sec-tions, in connection with their cortical targets.
Primary Motor and MotorAssociation AreasMI corresponds to Brodmann’s area 4. Located inthe precentral gyrus on the convexity of thecerebral hemisphere, it extends from the fissure ofSylvius laterally into the interhemispheric fissuremedially. Neurons of MI influence the motorsystem directly through the corticospinal andcorticobulbar tracts and indirectly through their
projections to the red nucleus and the reticularformation. (See Chapter 8.) These neurons alsoproject to and, in turn, receive influences from,recurrent loops through the cerebellum (seeChapter 16) and the basal ganglia (see Chapter17). MI contains a somatotopic distribution ofneurons; that is, the arrangement of neuronsfollows a sequence reflecting their order ofterminations in the brain stem and spinal cord(Fig. 20–7). Nevertheless, unequal amounts ofcortex innervate various parts of the body. Theparts of the body capable of fine or delicatemovement possess a large cortical representation;large numbers of cortical neurons control them,whereas the parts capable only of gross move-ments have a small cortical representation.
In addition to the somatotopic arrangement, theorganization of the primary motor cortex includesradially arranged columns of neurons. Each verti-cal column consists of a functional entity respon-sible for directing a group of muscles acting on asingle joint. With this organization, the columnsof the cortex represent movements, not individualmuscles. Individual neurons within these clustersdo innervate individual muscles; hence clusters ofneurons in different combinations among the col-umns innervate individual muscles repeatedly.Neurons of the motor cortex having axons in thecorticospinal tract function chiefly in the controlof the distal muscles of the limbs.
The primary motor cortex interconnects recip-rocally with the caudal (posterior) part of theventral lateral nucleus of the thalamus. Thisportion of the ventral lateral nucleus receives itsmajor input from the deep cerebellar nuclei.
Lesions in MI result immediately in paresis ofthe contralateral musculature with hypotonia (i.e.,decreased resistance to passive manipulation) anddiminished muscle stretch reflexes. In a fewweeks, muscle strength partially recovers, theaffected musculature develops spasticity (i.e.,increased resistance to passive manipulation), themuscle stretch reflexes become enhanced, and anextensor plantar response (Babinski’s sign) ap-pears. In the chronic state, the affected hand andfingers show slowness of movement and loss ofdexterity. This is a kinetic apraxia, which isdescribed later in this chapter.
A unimodal cortex devoted to motor planning,the motor association cortex, consists of Brod-mann’s area 6 and parts of areas 8 and 44. The
X Fig. 20-7
182 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 9/19 Pg: 182 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 9/19 Pg: 182 BLACK Team:

motor association cortex includes the supplemen-tary motor area (MII), the premotor area, thefrontal eye fields, and the posterior part of Broca’sarea.
Located on the medial surface of the frontallobe in area 6, just anterior to the MI, MIIcontains a complete somatotopic representationof the body, as shown by the results of electricalstimulation in animals and humans. MII partici-pates in the advance planning and sequencing of
movements, particularly for movements involv-ing both sides of the body. Imaging studiesdemonstrate that this area becomes active when aperson thinks about a movement, in the absenceof any motor activation.
The premotor area in Brodmann’s area 6,is immediately in front of area 4 on the lat-eral surface of the hemisphere. Neurons in boththe premotor area and MII receive input fromsensory unimodal and heteromodal association
FIGURE 20–7. (A) Lateral surface of the left cerebral hemisphere. The precentral gyrus iscolored, and the functional organization of upper motor neurons is indicated. (B) A coronalsection taken through X to X´ provides a more detailed representation of the opposite sideof the body in the motor area. (Adapted from Penfield, W, and Rasmussen, H: The Cere-bral Cortex in Man. Macmillan, New York, 1950.)
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 183
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 10/19 Pg: 183 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 10/19 Pg: 183 BLACK Team:

cortices. Accordingly, they respond to sensorystimuli, but the response is determined more bythe type of movement elicited by the stimulusthan by the sensory characteristics of the stimu-lus. Both these areas also project to the primarymotor cortex and the basal ganglia, and they sendtheir axons into the corticospinal tract and thepontocerebellar projection system.
Parts of the motor association cortex, thefrontal eye fields, lie on the lateral surface of thehemisphere in the precentral sulcus and includethe caudal parts of the adjacent superior andmiddle frontal gyri. Stimulation of this arearesults in conjugate deviation of the eyes to theopposite side. This region interconnects with theparietal eye field and contributes to all volitionaland visually guided saccades, as well as to pursuitand vergence movements of the eyes. (SeeChapter 19.) The primary thalamic nucleus of themotor association cortex, the oralis portion ofthe ventral lateral nucleus, contains a small-celled component and a large-celled componentthat receive fibers from the globus pallidus andthe substantia nigra pars reticulata, respectively.
Lesions of the supplementary and premotorcortices result in complex defects of movement inthe absence of weakness. Experimental animalswith lesions in area 6 lose the ability to alter thetype of limb and body movement in response todifferent types of sensory inputs. Visual guidanceof motor performance also becomes impaired.Unilateral lesions that include the frontal eye fieldresult in defective scanning and exploration of theopposite side of the visual environment.
Primary Sensory and UnimodalSensory Association AreasThe sensory areas for somatic sensation, audition,and vision occupy large areas of the parietal,temporal, and occipital isocortex. Research onstructural and functional relationships in thecerebral cortex has rapidly changed our view ofits organization. For purposes of this discussion,the term primary sensory cortex refers to bothprimary and secondary areas of earlier descrip-tions. Each of these areas contains a topographicmap of the receptor surface (the body wall, organof Corti, and retina, respectively). The cells of theadjacent unimodal sensory areas exhibit funda-mentally different response characteristics, butthey also contain a topographic organization. Inprimates, these unimodal areas contain multiple
repetitions of the somatosensory, auditory, andvisual receptor surfaces, although the topographicresolution diminishes, and the extraction offeatures of categories and individual stimuliincreases.
The vestibular and gustatory cortices lie at theinterface between isocortical and mesocorticalareas in the operculum, where the parietal so-matosensory cortex merges with the insularcortex. The detailed structure and functions ofthese areas have been defined less fully than thosefor somatosensory, visual, and auditory areas.The olfactory cortex consists of an allocortical(three-layered) area on the ventral surface of thehemisphere. Its organization and pattern of con-nections necessarily differ markedly from thoseof the other sensory regions.
Primary Somatosensory and UnimodalSomatosensory Association Areas
The primary somatosensory area (SI) includesBrodmann’s areas 3, 1, and 2 on the postcentralgyrus. It lies in continuity with a secondary area(SII) on the operculum and dorsal insula. Theseareas receive projections from the posterior partof the ventral posterolateral nucleus and fromthe ventral posteromedial nucleus of the thala-mus. The ventral posterolateral nucleus transmitsinformation from the medial lemniscus and thespinothalamic tract, and the ventral posteromedialnucleus transmits information from the trigemi-nothalamic tract. Many cells in these thalamicnuclei have both place- and modality-specificresponses to stimuli and small receptive fields,and the functional organization of SI reflects thesecharacteristics. The somatotopic organization ofSI consists of a mirror image of the adjacent MI.Muscle spindle afferents activate neurons of area3a (the most rostral strip of area 3, in the depthsof the central sulcus), cutaneous afferents stimu-late area 3b (caudal to 3a) and area 1, and jointreceptors activate area 2. Active tactile explora-tion provides especially strong stimulation of theneurons of these areas. The cells of SII havelarger receptive fields and respond to touch,pressure, and position of the limbs and pain fromboth sides of the body. Lesions of SI result inimpairment of ‘‘cortical sensation,’’ or tactilediscrimination. This includes deficits in two-pointdiscrimination, precise localization of tactilestimuli, position sense, and stereognosis. Theability to recognize the primary modalities of
184 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 11/19 Pg: 184 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 11/19 Pg: 184 BLACK Team:

sensation (i.e., touch, pain, and temperature)remain preserved but poorly localized in humanpatients with lesions of SI.
The somatosensory unimodal associationarea lies in the superior parietal lobule (area 5 andthe anterior part of area 7). Most of the neurons inthis region respond only to somatosensorystimuli. They interconnect with the lateral pos-terior nucleus of the thalamus. This areasubserves touch localization, exploration of theenvironment with the body surface, synthesis ofpersonal and extrapersonal space, and memory ofthe somesthetic environment. Neurons of thisregion project to the heteromodal association areain the posterior part of area 7 and the inferiorparietal lobule.
Primary Auditory and Unimodal AuditoryAssociation Areas
The transverse temporal gyri (Heschl’s gyri) liewithin the lateral fissure, continuous with thesuperior part of the superior temporal gyrus.Brodmann’s area 41, the anterior gyrus, corre-sponds to the primary auditory area (AI). Area42, the secondary auditory area (AII), liesposterior to area 41, and it usually occupies themore posterior transverse gyrus and part of theadjacent planum temporale. Both these areasreceive auditory information through the auditoryradiations from the medial geniculate nucleus.AI contains a tonotopic organization; low-frequency sounds receive processing more ros-trally and laterally than do high-frequencysounds. Neurons of AI respond not only to thefrequency but also to the localization of sound.The ascending auditory pathway has many decus-sations in the brain stem; thus, the AI area of eachhemisphere receives information from both ears,although the input from the contralateral ear ismore heavily represented than input from theipsilateral ear. Unilateral lesions of AI cannot bedetected clinically and can be discovered onlywith specialized tests such as auditory evokedpotentials or dichotic listening tasks. Completecortical deafness results only from bilateral dam-age to the AI area and the adjacent auditoryassociation areas of both cerebral hemispheres.
The auditory unimodal association area liesin area 22 of the superior temporal gyrus. As inthe primary auditory cortex, the neurons in thisarea interconnect with the medial geniculatenucleus and respond only to auditory stimuli.
They discriminate auditory frequencies and thesequence, or pattern, of sounds. The area alsoparticipates in the retention of auditory informa-tion. Neurons in this region project to theheteromodal association areas in the prefrontaland temporoparietal areas of cerebral cortex andalso to the paralimbic and limbic structures of thetemporal lobe.
In the human, bilateral lesions of the auditoryassociation areas or a unilateral left-sided lesionthat disconnects area 22 from Wernicke’s arearesult in pure word deafness. Patients with thisdisorder cannot understand or repeat spokenlanguage, but they respond appropriately toenvironmental sounds (a finding indicating thatthey are not deaf), and they can understandwritten language (a finding indicating they are notaphasic).
Primary Visual and Unimodal VisualAssociation Areas
The striate cortex (area 17), which lies along thebanks of the calcarine fissure medially andextends onto the occipital pole, constitutes theprimary visual cortex. This area receives visualinput from the retina through the lateral genicu-late nucleus. The striate area of each hemispherereceives information from the contralateral half ofthe binocular visual field. The dorsal parts of thestriate cortex, in the cuneus, respond to stimuli inthe contralateral lower hemifield. The ventralparts of the striate cortex, in the lingual gyrus,respond to input from the contralateral upperhemifield. Neurons of the striate cortex integrateinformation from the homologous areas of thetwo eyes and respond to the shape of objects aswell as to their color, size, location, and directionof movement. The secondary visual cortex,Brodmann’s area 18, surrounds the striate cortex.It, too, contains a representation of the contralat-eral half of the visual field. In humans, focallesions of the striate cortex result in visual fielddefects that reflect this retinotopic organization ofthe cortex. (See Chapter 18.) Complete bilateraldestruction of the striate cortex results in corticalblindness. In this condition, the pupillary lightreflexes remain intact, but the patient possessesno useful vision. Some patients with corticalblindness claim that they can see when clearlythey cannot. This condition bears the termAnton’s syndrome and results from lesions that
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 185
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 12/19 Pg: 185 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 12/19 Pg: 185 BLACK Team:

destroy area 17 and the peristriate, unimodalvisual association cortex in areas 18 and 19.
The visual unimodal association area in-cludes the peristriate cortex (areas 18 and 19) andareas on the middle and inferior temporal gyri(areas 20, 21, and 37). Neurons in the visualunimodal association area respond only to visualstimuli and can respond to complex aspects ofvisual stimuli such as form, motion, and color.The middle temporal visual area at the occipito-temporoparietal junction (areas 19, 37, and 39)analyzes the speed and direction of movingstimuli. (See Chapter 19.) These areas receivethalamic input from the inferior and lateralparts of the pulvinar (Figs. 20–4 and 20–8). Inexperimental animals, lesions of this area result indefects of depth perception, distance judgment,movement, spatial orientation, and hue discrimi-nation thresholds. In humans, lesions in areas 20,21, and 37 can result in discrete deficits in namingof visual stimuli that affect some categories ofobjects and not others. For example, a patient mayeasily recognize and name manufactured tools butcannot identify correctly items of food or types ofanimals.
Primary Vestibular Areas
Experimental evidence indicates that areas at theboundaries of the somatosensory cortex, 3a
and 2V, respond to stimulation of the vestibularapparatus. These two areas of the somatosensorycortex also receive information about musclespindle stimulation and joint movement, respec-tively. They interconnect with the ventral pos-terolateral and ventral lateral thalamic nuclei.Other areas that have been implicated in theconscious sense of gravity and acceleration in-clude an area near SII, at the parietoinsularinterface, and a part of area 7 in the posteriorparietal lobe.
Primary Taste Area
The primary taste area or gustatory cortical arearesides in the parietal operculum and adjacentanterior insular cortex (Brodmann’s area 43; Fig.20–1). This area receives taste information fromthe ipsilateral side of the tongue through theparvocellular division of the ventral postero-medial nucleus of the thalamus (Fig. 20–4).
Primary Olfactory Area
In spite of its name, the primary olfactory cortexdiffers from the sensory areas discussed earlier inthe pattern of its connections. This area ofallocortex receives processed olfactory signalsfrom the olfactory bulb and relays these signalsdirectly to other limbic areas. The primaryolfactory cortex also relays olfactory signals
LATERAL VENTRICLE
FORNIX
PULVINARCEREBRAL AQUEDUCT
LATERAL GENICULATE NUCLEUS
HIPPOCAMPUS
FIGURE 20–8. A T1-weighted (spoiled gradient echo) magnetic resonance image from aneurologically normal adult. This coronal sequence shows the lateral geniculate nucleusand pulvinar in the posterior thalamus.
ZFig 20-8
186 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 13/19 Pg: 186 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 13/19 Pg: 186 BLACK Team:

directly to the lateral orbitofrontal cortex and topart of the insula, as well as to the magnocellularor medial portion of the mediodorsal nucleus ofthe thalamus, which reciprocally interconnectswith the orbitofrontal area of the isocortex. Theallocortical primary olfactory cortex thereforeprovides input into a set of thalamocortical-corticothalamic connections that resemble thoseof other sensory systems. In experimental ani-mals, lesions in the pathway from the primaryolfactory cortex through the thalamus to theorbitofrontal cortex have shown that this pathwayparticipates in complex olfactory discriminationlearning.
Heteromodal Association AreasMI, MII, SI, and SII and the unimodal associationareas participate only in single modality informa-tion processing. In the next stage of informationprocessing, termed heteromodal, several differentsensory modalities converge onto and can acti-vate single neurons. Many neurons in hetero-modal regions also change their discharge rateduring specific motor acts, a finding indicatingthat these neurons integrate complex sensoryinputs with motor output. Regions within the twomajor heteromodal association areas intercon-nect, and the networks of these connections formthe basis for a variety of cognitive processes,including language. The heteromodal corticesalso have extensive connections with paralimbicand limbic structures and therefore participate inlearning, memory, mood, and motivation. Injuryto heteromodal areas leads to complex neurologicdisorders with combinations of cognitive defectsand emotional disturbances. The two majorheteromodal association areas include (1) thetemporoparietal areas and (2) the prefrontal areas.
Temporoparietal Association Area
The temporoparietal heteromodal associationarea occupies a strip of cortex extending from themiddle and caudal superior temporal gyri into theinferior parietal lobule and the posterior part ofthe superior parietal lobe. It includes both lateraland medial surfaces of the posterior parietalcortex, and on the medial side it continues into theposterior part of the temporal lobe. This strip thusabuts the auditory cortex of the lateral temporallobe, the somatosensory cortex of the anteriorparietal lobe, the visual cortex of the occipital
lobe, and the paralimbic cortices on the medialsurface of the hemisphere. The temporoparietalassociation cortex receives input from all theseadjacent sensory areas and has both input andoutput relations with the paralimbic cortex. Theactivity of its cells reflects these connections,because many neurons within this region respondto a single sensory modality, whereas neighboringneurons respond to a single sensory modality ofanother type or to multiple types of sensorymodalities. In addition, many of these neuronsalter their responses during performance of taskswith a strong motivational component such as areward. The thalamic nuclei most heavily con-nected with the temporoparietal area include themedial part of the pulvinar nucleus and thelateral posterior nucleus.
In experimental animals, unilateral lesions inthese areas result in neglect of objects and stimuliin personal and extrapersonal space on thecontralateral side of the body. Bilateral lesions inanimals lead to impairment in exploring extra-personal space, with defects in determiningspatial relationships between objects and negoti-ating relatively simple mazes. Visual, auditory,and somatosensory perceptions remain intact, butthese sensory modalities cannot be integrated.
Lesions of the temporoparietal heteromodalassociation areas in the human result in complexdisturbances that depend on the side of the lesion.Damage in the left cerebral hemisphere leads todisorders of language and disturbed spatial inte-gration. An important part of the temporalheteromodal association area in the left hemi-sphere, Wernicke’s area, lies in the posterior partof the superior temporal gyrus (Brodmann’s area22). This area integrates the sensory modalitiesneeded to understand written and spoken lan-guage. Injury results in Wernicke’s aphasia,which is described later in this chapter. Complexdisorders result from left cerebral hemispherelesions that spare Wernicke’s area but damage theangular gyrus (Brodmann’s area 39) in theinferior parietal lobe. These consist of varyingcombinations of the following:
1. Alexia (inability to read).2. Anomia (inability to name objects).3. Constructional apraxia (inability to con-
struct simple figures such as a clock or ahouse with pencil and paper).
4. Agraphia (inability to write).
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 187
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 14/19 Pg: 187 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 14/19 Pg: 187 BLACK Team:

5. Finger agnosia (inability to name individualfingers).
6. Confusion between the left and right sidesof personal and extrapersonal space.
A subset of these disorders, the combination ofacalculia, agraphia, finger agnosia, and right-leftdisorientation, has been termed the Gerstmannsyndrome; however, it seldom appears in isola-tion. Lesions of the left cerebral hemisphere thatspare Wernicke’s area but affect the supramar-ginal gyrus (Brodmann’s area 40) in the inferiorparietal lobule result in conduction aphasia. Thisdisorder is described later.
Unilateral damage to the temporoparietal het-eromodal association area in the right cerebralhemisphere causes disturbances in the integrationof personal and extrapersonal space, referred to assensory neglect. Such lesions result in dressingapraxia (difficulty in dressing, particularly the leftside of the body), constructional apraxia (diffi-culty in constructing simple figures with penciland paper, usually with inattention to the left sideof the figure), neglect of the left side of personaland extrapersonal space, and lack of insight aboutthese difficulties.
Bilateral lesions of the temporoparietal hetero-modal association areas lead to complex disordersincluding visual, spatial, and language defects.One such disorder, Balint’s syndrome, usuallyresults from bilateral lesions of the posteriorparietal lobe. This consists of (1) inability to gazetoward the peripheral field (even though eyemovements are intact), (2) difficulty in reachingout and touching objects accurately with visualguidance, and (3) inattention to objects in theperipheral parts of the visual field.
In addition to the cognitive, perceptive, andmotor disturbances resulting from lesions of thetemporoparietal heteromodal association areas,affective disorders also appear. Mood alterationsranging from anger to apathy can be seen withthese disturbances. These emotional disturbancesresult from interruption of the connections be-tween heteromodal association areas and parts ofthe limbic system.
Prefrontal Cortex
The largest part of the frontal lobe, the prefrontalregion, lies rostral to the motor areas. Theprefrontal heteromodal association area makesup most of this region. It includes Brodmann’s
areas 8 through 10, parts of 11 and 12, and 45through 47. A small area on the ventral surface ofthe frontal lobe, the orbital cortex, interconnectsprincipally with the limbic lobe and is discussedas part of the paralimbic cortex. The prefrontalheteromodal association area has major connec-tions with other areas of cortex, notably thetemporoparietal association cortex and the motorassociation areas of the frontal lobe, as well as theparalimbic cortex. The prefrontal heteromodalarea interconnects reciprocally with the lateralpart of the mediodorsal nucleus of the thala-mus and with the ventral anterior nucleus,which receives input from the reticular formation.The prefrontal area also sends projections to thebasal ganglia through the head of the caudatenucleus.
The neurons of the prefrontal cortex respond tomany different types of sensory inputs and thuscan be characterized as heteromodal neurons, butthey also respond to the behavioral importance ofthe inputs. A neuron responding strongly to asensory input that has been associated with apleasant reward may respond differently when thesame input has been associated with a noxiousstimulus. Thus, the neurons of the prefrontalregion appear to integrate motivational eventswith complex sensory stimuli. Neurons in thisarea also serve to inhibit motor responses when atask requires delaying the response. The ventro-medial component of the prefrontal cortex par-ticipates in emotional processing and in planningand decision making.
Injury to the prefrontal cortex in experimentalanimals impairs the ability to perform tasksrequiring the animal to alternate responses tostimuli with a delay. Unilateral ablation of thefrontal eye fields in animals results in neglect ofstimuli in the opposite side of extrapersonalspace. In humans, lesions of the prefrontal cortexdisrupt some of the most complex aspects ofbehavior. Unilateral lesions of either side lead toneglect of the contralateral side of extrapersonalspace. Bilateral lesions cause markedly disturbedbehavior. These patients become unconcernedwith their illness and may appear depressed orinappropriately jocular. Their social graces andconcern for others disappear. They may eat fromthe floor, drop food on their clothing withoutconcern, and ignore the ordinary standards ofcleanliness. Often they appear apathetic, althoughthey may be irascible. They cannot exercise
188 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 15/19 Pg: 188 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 15/19 Pg: 188 BLACK Team:

foresight or good judgment and have essentiallyno insight. They can be distracted easily andcannot perform complex tasks requiring appro-priate sequencing of several actions or responses.These disorders have been termed the frontallobe syndrome and also the dysexecutive syn-drome.
Paralimbic AreasThe paralimbic areas consist primarily of me-socortical areas. With the limbic cortex, they forma continuous ring of tissue at the medial edge ofthe cerebral hemisphere (the limbic lobe) thatextends laterally to include the insula. The areasof Brodmann that make up this ring of cortexinclude the following:
1. The temporal pole (area 38).2. The insula.3. The caudal orbitofrontal cortex (caudal
parts of areas 11 and 12).4. The parahippocampal regions (areas 27, 28,
34, and 35).5. The retrosplenial area (areas 26, 29, and 30),
cingulate gyrus (areas 23, 24, 31, and 33),and the precallosal and subcallosal regions(areas 32 and 25).
The paralimbic areas receive information fromheteromodal association areas of the isocortex,limbic cortex, and anterior, laterodorsal, mid-line, and medial nuclei of the thalamus. Themedial nuclei heavily interconnected with theparalimbic cortex include the medial part ofthe mediodorsal nucleus and the medial part ofthe pulvinar.
The paralimbic areas participate in memoryand learning, drive and affect, and social behav-ior. Through their direct impact on the hypothal-amus, these areas influence homeostasis. (SeeChapter 21.) Damage to the parahippocampalcortex as well as to the hippocampus andamygdala leads to severe disorders of memory.Damage to the paralimbic areas of the orbitofron-tal region and to the amygdala results in changesin mood and social behavior. In some patients,this damage leads to severe apathy. The paralim-bic areas of the orbitofrontal and insular regionsalso participate in processing olfactory and gus-tatory information, as noted previously in thischapter.
Limbic AreasThe limbic cortex, which consists of allocortex,includes the (1) hippocampal formation and(2) primary olfactory (pyriform) cortex. Thecorticoid areas, which contain no discerniblelayering of cells, include the (1) amygdala,(2) septal area, and (3) substantia innominata.Many of these areas cannot be seen on the medialor ventral surface of the hemisphere because,although they are directly continuous with theparalimbic cortex, they are folded under, so theyappear deep to the medial edge of the paralimbiccortex.
A specific group of neurons extending throughseveral limbic areas provides excitatory choliner-gic innervation for the entire surface of thecerebral cortex, particularly the paralimbic areas.These include the medial septal nucleus, thevertical and horizontal nuclei of the diagonal bandof Broca, and the nucleus basalis of Meynert inthe substantia innominata. (See Fig. 23–1.)
Limbic structures participate in both explicitmemory (the hippocampus) and associative, oremotional, memory (the amygdala). The anteriorthalamic nuclei, the medial part of the me-diodorsal nucleus, and the medial pulvinarconnect directly to the hippocampus, primaryolfactory cortex, and amygdala. The limbic cortexprovides input to basal ganglia through projec-tions to the ventromedial part of the head of thecaudate nucleus and to the ventral striatum. (Foradditional discussion of the limbic areas of thecortex, see Chapter 21.)
Disorders of CorticalNetworks
AgnosiasThe process of comprehension (‘‘knowing’’ or‘‘gnosis’’) entails a comparison of present sen-sory phenomena with past experience. For exam-ple, the visual association areas must be called onwhen a person recognizes an old friend in acrowd. Agnosia consists of a failure to recognizestimuli when the appropriate sensory systemsfunction adequately. Agnosia commonly occursin visual, tactile, and auditory forms.
Visual agnosia can be defined as the failure torecognize objects visually in the absence of adefect of visual acuity or intellectual impairment.
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 189
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 16/19 Pg: 189 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 16/19 Pg: 189 BLACK Team:

The patient often can see the object clearly butcannot recognize or identify it visually. In a purevisual agnosia, the same object can be identifiedby other sensibilities such as touch. The moststriking example of this, prosopagnosia, consistsof an agnosia for familiar faces. Bilateral lesionsof the temporal aspect of visual unimodal asso-ciation areas usually underlie visual agnosia.
Tactile agnosia consists of the inability torecognize objects by touch when tactile andproprioceptive sensibilities remain intact in thepart of the body being tested. Patients with tactileagnosia often have disturbances of body image.Lesions of the supramarginal gyrus (area 40)usually underlie tactile agnosia.
Auditory agnosia involves the failure of apatient with intact hearing to recognize specificsounds, including speech, music, or familiarnoises. Bilateral lesions of the posterior part of thesuperior temporal convolution (area 22) areresponsible for this condition.
ApraxiasApraxia can be defined as loss of the ability tocarry out correctly certain movements in responseto stimuli that normally elicit these movements.This deficit occurs in the absence of weakness,sensory loss, or disturbance of language compre-hension. Accomplishing a complex act requiresthe integrity of a large part of the cerebral cortex.There must first be an idea or a mental formula-tion of the plan to carry out the movement. Thisformulation must then be transferred by associa-tion fibers to the motor system, where it can beexecuted. Apraxias usually result from lesionsinterrupting connections between the site offormulation of a motor act and the motor areasresponsible for its execution.
Ideomotor apraxia consists of the inability toperform a complex motor task despite awarenessof the task the patient intends to perform. Patientswith this disorder can perform many complex actsautomatically but cannot carry out the same actson command. A lesion of the supramarginal gyrusof the dominant parietal lobe underlies thisdisorder.
Ideational apraxia refers to failures in carry-ing out sequences of acts, although individualmovements can be made correctly. This form ofapraxia results from lesions in the dominantparietal lobe or the corpus callosum.
Kinetic (motor) apraxia involves the inability
to execute fine acquired movements and resultsfrom disease of the contralateral frontal lobe.Gait apraxia consists of difficulty in initiatingand continuing smoothly the movements neededfor walking. It results from bilateral disease of thefrontal lobes. Typically, the patient appears tohave the feet ‘‘glued to the floor,’’ because thepatient makes a series of incomplete walkingmovements of the legs, then may stride for one ortwo steps, only to develop another series ofincomplete ambulatory movements.
AphasiasFacile use of language and speech is a remarkableattribute of the human brain—one that no otheranimal shares. Language refers to the vocabularyand syntactic rules needed for communication.Speech refers to the production of spoken lan-guage. Dysarthria can be defined as a distur-bance in the execution of speech and often occurswithout a disorder of language. Aphonia involvesthe inability to produce sounds. Aphasia consistsof a disorder of language caused by a defect ineither the production or the comprehension ofvocabulary or syntax.
Beginning early in life, nearly everyone selec-tively develops one hemisphere of the brain moreintensively than the other in the processes re-quired for language. Usually, the left side of thebrain assumes the leading role, and the personbecomes right-handed. Right-handedness indi-cates the preferential use of the right hand in mostor all unimanual activities, and it is usuallyassociated with preferential use of the right eyefor monocular visual functions and the right footfor motor acts such as kicking. Approximately90% of people in the United States use the righthand preferentially, and essentially all of themhave left-hemisphere dominance for language.About 10% of people use the left hand preferen-tially, but about half of them nevertheless haveleft-hemisphere dominance. The remaining left-handed people have right-hemisphere dominanceor mixed left and right dominance. Aphasiaappears only if a lesion involves the languageareas of the dominant hemisphere. Childrendisplay a preference for the use of the right or lefthand from an early age, so it is unclear whencerebral dominance for language actually occurs.In any case, cerebral dominance for language is aplastic phenomenon; that is, it can be changed, upto the age of about 7 years. For example, a
190 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 17/19 Pg: 190 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 17/19 Pg: 190 BLACK Team:

right-handed child 5 years of age who suffers aninjury in the language areas of the left cerebralhemisphere will lose speech initially, but willlearn to speak again in 1 or 2 years. An adultcannot recover speech to this extent after damageto the language areas of the left hemisphere.
Three regions of the dominant cerebral hemi-sphere serve important roles in aphasia: Broca’sarea, Wernicke’s area, and the intervening areaof parietal lobe (the parietal operculum). Broca’sarea, the anterior speech region, lies in the inferiorfrontal gyrus just rostral to the site of the motorrepresentation of the face (Fig. 20–9). The regionincludes Brodmann’s areas 44, 45, and 47. Asmentioned previously, Wernicke’s area lies in theposterior part of the superior temporal gyrus onthe convexity of the brain and extends onto theupper surface of the temporal lobe. The posteriorpart of Brodmann’s area 22 lies central toWernicke’s area. Wernicke’s area connects withBroca’s area through a series of neuronal relays inthe cerebral cortex from the temporal lobe aroundthe posterior end of the fissure of Sylvius into thelower parietal lobe and running forward into thefrontal lobe. Functionally, Wernicke’s area pro-
vides the capacity to recognize speech patternsrelayed from the left primary auditory cortex.Information about incoming speech patternsmoves to Broca’s area, which generates theproper pattern of signals to the speech muscula-ture for the production of meaningful speech.Three general forms of aphasia have been recog-nized that relate to Broca’s area, Wernicke’s area,and the intervening cerebral cortex.
Lesions of Broca’s area lead to nonfluent(also termed motor, anterior, or Broca’s) apha-sia (Fig. 20–9). The patient produces spokenlanguage slowly and effortfully, with poorlyproduced sounds and ungrammatical, telegraphicspeech that deletes many prepositions, nouns,and verbs. The patient has extreme difficultyin expressing certain grammatical words andphrases. The phrase, ‘‘no ifs, ands, or buts’’proves to be particularly difficult for affectedpersons to speak. Phrases or sentences can berepeated only poorly. The patient usually com-prehends spoken and written language, but be-comes frustrated and discouraged by the difficultywith speech. Vascular lesions of Broca’s areaoften involve the underlying white matter and
FIGURE 20–9. Cerebral cortical areas that are important for language. A visual image ofa word is projected from the calcarine cortex (1) into the visual association areas 18 and19 (2) to the region of the angular gyrus (3). Information is then transferred to Wernicke’sarea (W) to arouse the learned auditory form of the word. This information is then trans-ferred by corticocortical connections (4) across the parietal operculum (P) to Broca’s area(B), which contains programs that control (5) the cortical motor region in the precentralgyrus involved in speech.
ZFig. 20-9
CHAPTER 20 CEREBRAL CORTEX AND THALAMOCORTICAL CONNECTIONS � 191
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 18/19 Pg: 191 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 18/19 Pg: 191 BLACK Team:

thereby damage the internal capsule. Conse-quently, right hemiplegia usually accompaniesBroca’s aphasia.
Lesions of Wernicke’s area lead to fluent(also termed sensory, posterior, or Wernicke’s)aphasia (Fig. 20–9). The patient produces spokenlanguage more rapidly than normal, with pre-served grammatical construction. The patientcannot find the correct words to express thoughts,however, and may omit words or use circumlo-cutions, may use words without precise mean-ings, or may substitute words. Substitutions ofone word for another are called verbal parapha-sias. Literal paraphasia involves the substitu-tion of a well-articulated but inappropriate pho-neme in a word (e.g., saying pork for cork).Words may be produced that consist of randomcollections of sounds; these are termed neolo-gisms. The patient has poor comprehension ofspeech and poor repetition of phrases or sen-tences. The patient often does not recognize thespeech difficulty and may show no concern aboutit. Because lesions of Wernicke’s area are farremoved from MI and the internal capsule,patients with Wernicke’s aphasia usually do nothave hemiplegia.
Lesions of the conduction pathway fromWernicke’s area to Broca’s area cause conduc-tion aphasia by disconnecting the speech recog-nition area from the speech execution area. Thiscondition usually causes fluent aphasia with poorrepetition of spoken language. Despite phoneticerrors, comprehension of spoken language usu-ally remains preserved.
Posteriorly placed vascular lesions affectingspeech may damage the angular gyrus (area 39) inassociation with injury to Wernicke’s area. In-farction of the angular gyrus of the dominanthemisphere results in loss of the ability to read(alexia) and write (agraphia) in the absence ofprimary visual or motor impairment.
The preceding paragraphs describe localization
of the regions that control various aspects oflanguage. Individual patients vary greatly, how-ever, in the precise location of small subregions ofcortex that control various language skills withinthese large areas. Individual brains also appear tovary in the number of cortical loci within theseregions that control language. As a consequenceof this individual variability, partial lesions ofthese general cortical regions in the dominanthemisphere may not produce predictable lan-guage deficits. The effects of any given lesiondepend on the number and distribution of lan-guage processing sites within Broca’s area andWernicke’s areas in the afflicted individualpatient.
Case Follow-upThe man with the right-sided weakness andnonfluent aphasia was thought to haveischemia (diminished blood flow) of the ante-rior portion of the left cerebral hemisphereaffecting Broca’s area and the underlyingwhite matter, with extension to the internalcapsule. An imaging study of the head withcomputed tomography revealed no evi-dence of hemorrhage in the brain, and becausethe patient had been seen within 3 hours ofthe onset of his difficulty, he was given intra-venous tissue plasminogen activator. Thismedication has the capacity of breaking downalready formed clots of blood in the vascu-lature. The result was a gradual return ofstrength in the right limbs and full recovery oflanguage functions over the next 24 hours.Further evaluation of the patient revealed thathe had two untreated risk factors for stroke:high blood pressure and hypercholesterolemia.These disorders were treated with antihyper-tensive medication and a cholesterol-loweringagent. He was also given one aspirin per dayas prophylaxis against further strokes. He con-tinues to do well 5 years after this event.
192 � SECTION 5 FOREBRAIN
#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 19/19 Pg: 192 COLOR Team:#7900 @sunultra1/raid/CLS_books/GRP_davis/JOB_gilman/DIV_ch20 5/9/02 11 Pos: 19/19 Pg: 192 BLACK Team: