Cervical Cytology: Latest Screening and Management Guidelines...Triage of Abnormal Pap Test Results...
61
Cervical Cytology: Latest Screening and Management Guidelines Anna-Barbara Moscicki, MD University of California, Los Angeles
Transcript of Cervical Cytology: Latest Screening and Management Guidelines...Triage of Abnormal Pap Test Results...

Cervical Cytology: Latest Screening and Management
GuidelinesAnna-Barbara Moscicki, MD
University of California, Los Angeles

Disclosures
I have no disclosures related to this talk

OBJECTIVES Compare the performance characteristics of the
Pap vs co-testing vs HPV test alone Discuss the evidence supporting co-testing and
primary HPV testing Discuss management strategies of abnormal
screening Discuss what is new on the horizon

Women equate Pap test with Pelvic exam

But few knew that Pap was
actually a man’s name!!!
The Pap test has been widely used in the U.S. since the mid 1950s
Papanicolaou

CERVICAL CANCER TRENDS 1945-1985
American Cancer Society 1991

LIMITATIONS OF THE PAP TEST
Recent review of studies in developed countries cite a sensitivity of 44-65% for a single Pap test
– Sensitivity of a result of ASC-US or worse to identify CIN 2+
Inter-reviewer reliability of Pap is low– <50% for dx of ASC-US and LSIL
Cytology is poor at detecting adenocarcinoma in situWhitlock EP, Ann Intern Med 2011;155:687–97. Stoler, Schiffman. JAMA 2001;285:1500

After 3 or more negative cervical cytology exams in women aged 30 – 64, the incidence of CIN 3 within 3 years is only 0.019%.
Sawaya et. al. N Eng J Med 2003
With multiple repeat Pap tests over a woman’s life, the sensitivity increases dramatically!

Can we find something better in
deeper waters ?

Then there was a duh moment….


IF YOU DON’T HAVE HPV, YOU ARE NOT LIKELY TO GET CERVICAL CANCER!
– But if you do have HPV your risk increases:
– RR for developing cervical cancer for woman HPV 16 + is 434 compared with HPV neg.

WE KNOW THE CAUSE OF CERVICAL CANCER: HPV
We also know that Hepatitis B and C cause liver cancer

WE KNOW THE CAUSE OF CERVICAL CANCER: HPV
We also know that Hepatitis B and C cause liver cancer
But we don’t screen everyone for liver cancer We screen people who we know are infected

ABSOLUTE RISKS OF DEVELOPING CERVICAL INTRAEPITHELIAL NEOPLASIA GRADE 3 (CIN3) OR WORSE IN WOMEN WITH NORMAL CYTOLOGICAL FINDINGS AT BASELINE IN RELATION
TO VARIOUS MEASURES OF HUMAN PAPILLOMAVIRUS (HPV) STATUS
Kjaer et al, JNCI 2010

Kaiser Permanent of Norther Californa: VALUE OF HPV TESTING VERSUS PAP SMEARS (A) AND VALUE ADDED BY PAP SMEARS TO HPV TESTING (B)
Katki HA et al, Lancet Oncol 2011

5-YEAR CUMULATIVE RISKS OF CIN2 OR WORSE (A) AND CIN3 OR WORSE (B) BY ENROLMENT HPV TEST AND FINELY-CATEGORISED ENROLMENT PAP SMEARS
Katki HA et al, Lancet Oncol 2011

POSITIVE HPV DIAGNOSES MORE AIS AND ADENOCARCINOMA THAN CYTOLOGY ALONE
331,818 WOMEN ENROLLED IN KAISER N. CAL
Significantly more AIS and AdenoCA diagnosed over 5 yrs if initial screen:
•HPV + vs Pap + (p<0.0001) •HPV + / Pap – vs HPV -- / Pap + (p<0.0001)
AIS AdenocarcinomaTotal 70 27Pap Negative 42 (60%) 23 (85%)Pap Positive 28 (40%) 4 (15%)HPV Positive 56 (80%) 21 (78%)Pap -- / HPV + 31 (44%) 17 (63%)Pap + / HPV -- 3 (4%) 0
Katki, Kinney, et al Lancet oncol.2011;12:663-72

Risk of precancer/cancer for each Pap smear result
Katki et al, J Low Genit Tract Dis, 2013

Implicit Risk Thresholds used in current Pap-only screening
Katki et al, J Low Genit Tract Dis, 2013
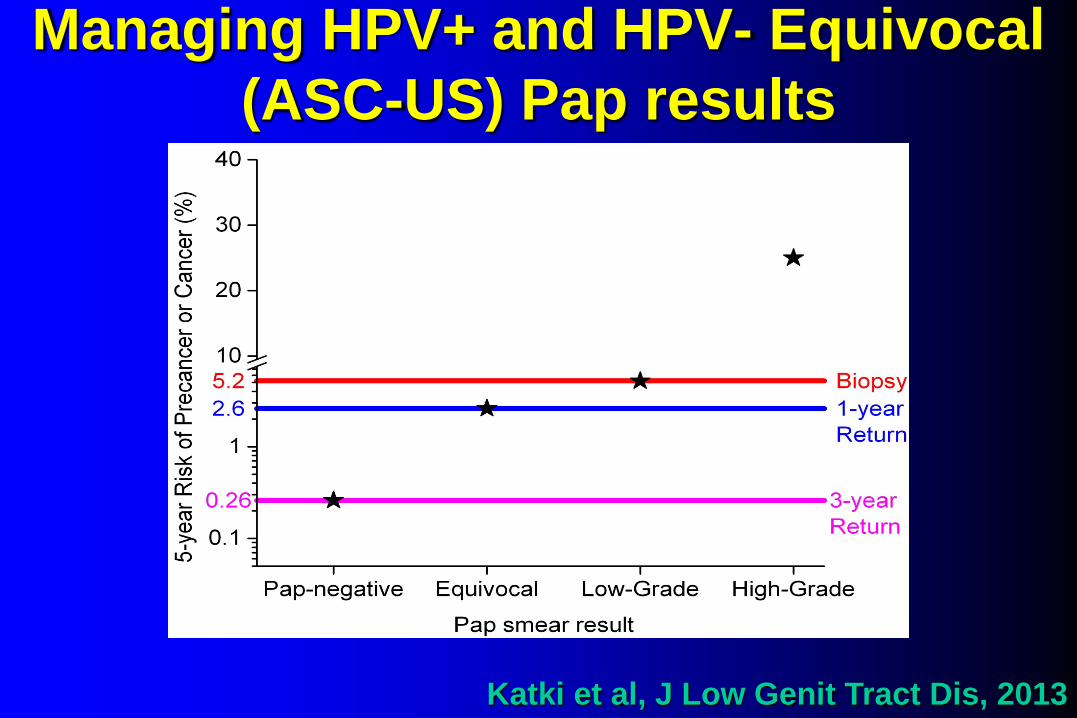
Managing HPV+ and HPV- Equivocal (ASC-US) Pap results
Katki et al, J Low Genit Tract Dis, 2013

Managing HPV+ and HPV-Low-Grade (LSIL) Pap results
Katki et al, J Low Genit Tract Dis, 2013
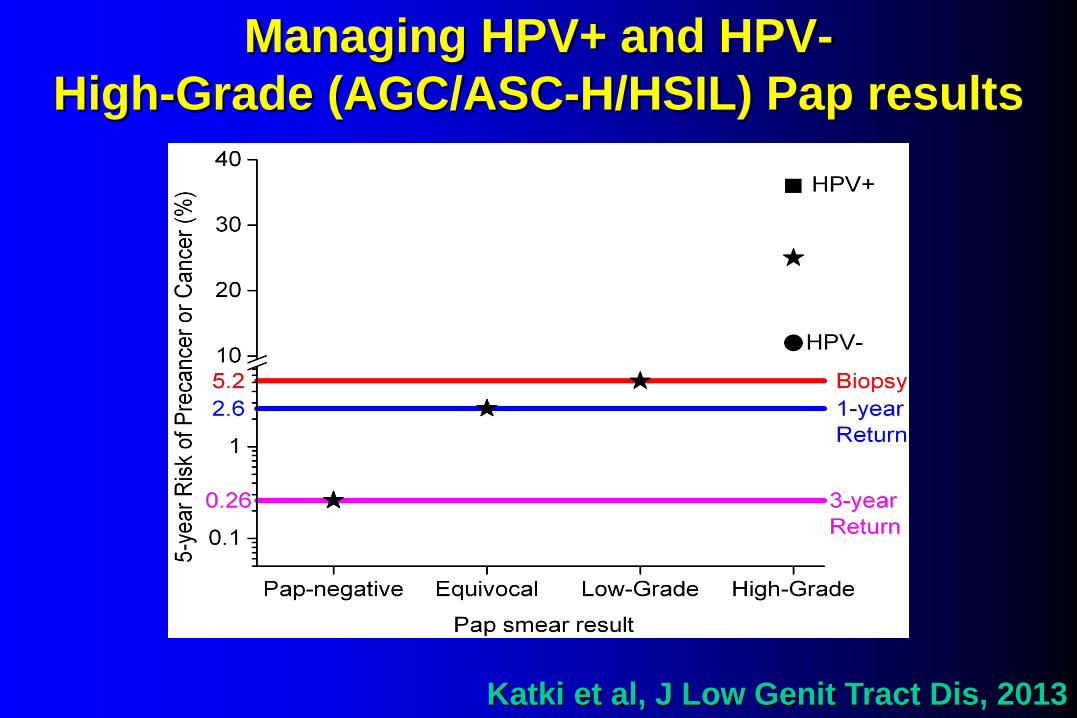
Managing HPV+ and HPV-High-Grade (AGC/ASC-H/HSIL) Pap results
Katki et al, J Low Genit Tract Dis, 2013

Managing HPV+ and HPV-Pap-negative results
Katki et al, J Low Genit Tract Dis, 2013

HPV AND CYTOLOGY ‘‘COTESTING’’ EVERY 5 Y (PREFERRED) (AGE 30-65)
Cotest negative or HPV-negative ASC-US:– Rescreen with cotesting in 5 y
HPV-positive ASC-US or cytology of LSIL or more severe:– Colposcopy
Saslow D et al, CA Cancer J Clin 2012

MANAGEMENT OF WOMEN > AGE 30, WHO ARE CYTOLOGY NEGATIVE, BUT HPV POSITIVE
ASCCP Management Guidelines 2013

Why Pap at all?
PAP SMEARHANGING ON

24,295 women from 7 primary HPV screening studies in 6 European countries Adding cytology to an HPV test (cotesting) added little further protection
Dillner, et al. BMJ, 2008;337;a1754.
HPV alone vs HPV with cytology has similar “negative” screening performances
Inci
denc
e of
CIN
3+pe
r 10
000
Cytology-HPV–Cytology–/HPV–
100
80
60
40
20
00 12 24 36 48 60 72

Study Number Cytology HPV Cotest
Joint European cohort40 24,295 0.50% 0.11% 0.06%
Kaiser registry41 1,011,095 0.31% 0.34% 0.11%
ATHENA24 42,209 0.8% 0.3% 0.3%
VUSA42 25,873 0.26% 0.06% 0.05%
Kaiser 10-y43* 20,810 0.53% 0.24% 0.16%
*After 45 months
Risk of CIN 3+ After Negative ScreenMultiple studies, 3-y follow-up


On April 24, 2014 the FDA approved extended indications for the Roche COBAS HPV test to
include primary screening in women aged >25 using a limited, defined protocol

ATHENA PATIENT FLOWCROSS-SECTIONAL PHASE FOR PRIMARY HPV EFFECTIVENESS
RocheWright et al Gynecol Oncol 2015

Prevalence of HPV+ by AgeResults from ATHENA7
Wright et al Gynecol Oncol 2015


n=6,767
n=22,625

PROPORTION OF WOMEN WITH ≥CIN3 WHO HAVE NEGATIVE CYTOLOGY (NILM)and HPV POSITIVE ATHENA
Roche

CIN 3+
Predictive Value of HPV Genotyping3-y risk of CIN for all women ≥ 25 y, ATHENA study30

CANDIDATE SCREENING ALGORITHMHPV WITH 16/18 GENOTYPING AND REFLEX CYTOLOGY
RocheFDA approved 2014

Strategy Sensitivity Specificity PPV NPV
Cytology 40.3(34.6-46)
97.9(97.7-98)
23.9(21.0-26.8)
99.0(98.8-99.2)
Cotesting 63.4(56.7-70.1)
95.1(94.8-95.3)
17.8(15.8-19.8)
99.4 (99.2-99.5)
Primary HPV 64.8(58.4-71.1)
95.2(95-95.5)
18.5(16.4-20.6)
99.4(99.2-99.5)
Comparisons of Strategies in Women ≥ 30Y-ATHENA StudyPerformance measures for detecting CIN 3+ over 3 y*30
*Verification adjusted over the entire 3 y

Primary HPV TrialsNTCC Phase II1 HPV Focal2 FINNISH3
N 35,471 20,394 109,932Age 35-60 35-65 35-65# Rounds(Interval)
2 (3 yrs) 1 (2-4yrs) 1 (5yrs)
Screening hrHPV alone vs CC hrHPV w/ LBC triage vs. LBC w/HPV triage
hrHPV w/CC triage vs. CC
RR for CIN3+ 1 2.37 (1.4 to 3.9) 1.7 (1.1 to 2.8) 1.6 (1.2 to 2.0)
2 0.23 (0.07 to 0.82) - -
Colposcopy Referrals IG: 5.87%CG: 2.5 %
IG: 3.8%CG: 2.1%
IG: 0.9%CG: 1.0%
1Ronco et al Lancet Oncol 20102 Ogilvie G et al Int J Cancer 20173 Zorzi M et al BJOG 2017

HPV as Primary ScreeningImportant remaining issuesScreening interval: No US data on safety beyond 3 y; other countries adopting 5-7 y interval
Age of initiation: FDA approval for ≥25 y; lots of colposcopies in women 25-29 y
Triage of HPV+: Only two tests on market and FDA approved one algorithm; other strategies may prove more effective

What’s next?

What’s next?
Dual staining P16INK4a (cyclin-dependent kinase inhibitor and
is overexpressed in the presence of E7 oncoprotein) already used for confirmation of CIN2
Ki67 (proliferation-associated antigen related to DNA replication)

Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: Results from a sub-study nested into the ATHENA trial
Wright et al, Gyn Oncol, 2017
Dual-stained cytology more sensitive, but not more specific than Pap cytology for triaging HPV-positive women
Referral of HPV16/18 positive women combined with dual-stained cytology triage of women pos for 12 other HPV provided higher sensitivity for CIN3+ compared to Pap cytology

Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: Results from a sub-study nested into the ATHENA trial
Wright et al, Gyn Oncol, 2017
Dual-stained cytology more sensitive, but not more specific than Pap cytology for triaging HPV-positive women
Referral of HPV16/18 positive women combined with dual-stained cytology triage of women pos for 12 other HPV provided higher sensitivity for CIN3+ compared to Pap cytology
p16/Ki-67 dual-stained cytology, either alone or combined with HPV16/18 genotyping, represents a promising approach as a sensitive and efficient triage for colposcopy of HPV-positive women when primary HPV screening is utilized
SUMMARY HPV co-testing is becoming the mainstay of
cervical cancer screening starting at age 25-30 yrs HPV primary screening cytology triage is likely to
replace co-testing HPV testing detects CIN 3+ earlier and more
sensitive to detect AIS HPV 16/18 positivity meets the threshold for
immediate referral to colposcopy HPV primary screening has a low PPV; DS may
assist in effecient triage

What about immunosuppressed women?
At risk for cervical cancer
HIV Solid organ transplant Autoimmune Disease

Current Cervical Cancer Screening
Recommendations for HIV infected women <30 year
• Screening should start within 1 year of the onset of sexual activity (no
later than 21 yr).
• Cervical cytology at the time of initial diagnosis with HIV and then
annual.
•If the results of the 3 consecutive tests are normal, follow up screening
should be every 3 years.
•Co-testing is not recommended.

HIV-Infected Women Aged ≥30 years:
•Continue throughout a woman’s lifetime (and not end at 65 years of
age).
•Either cytology only or co-testing is acceptable for screening but co-
testing preferred.
•Primary HPV screening has not been addressed.
• Cytology alone and ASC-US with HPV triage: the same as <30 years
of age.
•Co-test negative repeat cervical cancer screening in 3 years.
•Cytology negative/hrHPV return in one year.

Triage of Abnormal Pap Test Results
• ASC-US/ HPV + referral to colposcopy regardless of age.
• If HPV testing is not available or not done or negative, then
repeat cytology in 6 to 12 months.
• For any result > ASC-US on repeat cytology, referral to
colposcopy regardless of age.
• LSIL or worse (including ASC-H, AGC and HSIL) referral to
colposcopy regardless of age.

Risk of CIN 2+ among WLHIV following 1, 2 or 3 consecutive negative cytology results (Cyt-), by CD4 cell count at final cytology: compared with the general population risk benchmark for recommending women be rescreened in 3 years (3-year return).
Robbins. AIDS, 2017
All 3 fall above risk

Risk of CIN 2+ among WLHIV following ASC-US cytology, by CD4R cell count, compared with general population risk benchmarks for recommending women be rescreened in 3 years return vs 6–12 months vs immediate colposcopy.
Robbins. AIDS, 2017

Are women with iatrogenic immunosuppression similar or at greater risk than HIV infected
women?

Definition for High Risk* Screening:
IBD and RA: – women on chronic (> 3months) corticosteroids
or immunomodulators (methotrexate, azathioprine, or mercaptopurine).
SLE : - all women regardless of medication status
*Screen as HIV >500Women not at high risk can follow general population

Definition for High Risk* Screening:
SOT and HSCT w/GVHD (systemic or genital): – Screen as if HIV CD4+ <500
HSCT (no GVDH) : - Screen as if HIV CD4+ >500
Women not at high risk can follow general population

Diabetes Mellitus
DM: no increased risk but adherence may be questionable and there should be due diligence to maintain routine screening

Screening for high risk immunosuppressed women (non-HIV) <30 years
Similar to CDC recommendation for HIV-Start within 1 year of immunosuppression or diagnosis-Screening should start within 1 year of sexual debut-Cytology ONLY recommended-Screen every 3 years-If previously unscreened or underscreened, screen annually for 3 consecutive cytologies
-Similar to HIV <500 (Robbins et al) for SOT, GVHD-If previous documented 3 normal cytologies may go to screening interval every 2years

Screening for high risk immunosuppressed women (non-HIV) >30 years
Similar to CDC Recommendation for HIV CD4>500-Start within 1 year of immunosuppression -Cytology or co-testing every 3 years--if unscreened or underscreened, perform annual testing until 3 consecutive normal-screen through-out person’s lifetime
Similar to HIV CD4 <500 (SOT and GVHD):- Cytology-/hrHPV-: 2 year return
-
Robbins. AIDS, 2017

Management of abnormal cytology
Similar to CDC Recommendation for HIV
ASCUS (HPV unknown or HPV negative) return in 6-12 months if severely immunocompromised consider colposcopy
Cytology-/hrHPV+ : 1 year returnCytology-/HPV 16/18: referral to colposcopy
Robbins. AIDS, 2017


Thank You