CB Learnng 3 final - HistoWebhistoweb.co.za/pdf/makro_endokrien_e_web.pdf7. Sketch the arterial...
21
STUDY COMPONENT Clinical Anatomy of the Endocrine System UNIT THEME 1: HYPOPTHALAMUS; HYPOPHYSIS; PINEAL GLAND UNIT THEME 2: THYROID AND PARATHYROID UNIT THEME 3: PANCREAS; ADRENAL GLANDS UNIT THEME 4: REPRODUCTIVE ORGANS SUB-SPECIFIC OUTCOMES: This component of block III is designed to enhance the development of multi-disciplinary knowledge and problem-orientated learning abilities in order to integrate anatomical concepts applicable to the endocrine glands. SUB-UNITS: 1. Hypothalamus a. Position and relations of the hypothalamus. 2. Hypophysis a. Structure, position and relations of the hypophysis. b. Hypophyseoportal system of the hypophysis. 3. Pineal gland a. Position and relations of the pineal gland. 4. Thyroid a. Position, relations, structure and blood supply of the thyroid gland. b. Embryological development of the thyroid gland 5. Parathyroid glands a. Position of the parathyroid glands b. Anatomical variations. c. Embryological development of the parathyroid glands. . 6. Pancreas a. Structure of the pancreas. b. Vertebral heights of the various parts of the pancreas. c. Arterial blood supply and venous drainage of the pancreas. d. Relations of the pancreas 7. Adrenal glands a. Structure and relations of the adrenal glands. b. Arterial blood supply and venous drainage of the adrenal glands. c. Relationship of the autonomic plexuses to the adrenal glands. 8. Testis
Transcript of CB Learnng 3 final - HistoWebhistoweb.co.za/pdf/makro_endokrien_e_web.pdf7. Sketch the arterial...
STUDY COMPONENT
Clinical Anatomy of the Endocrine System
UNIT THEME 1: HYPOPTHALAMUS; HYPOPHYSIS; PINEAL GLAND UNIT THEME 2: THYROID AND PARATHYROID
UNIT THEME 3: PANCREAS; ADRENAL GLANDS UNIT THEME 4: REPRODUCTIVE ORGANS SUB-SPECIFIC OUTCOMES: This component of block III is designed to enhance the development of multi-disciplinary knowledge and problem-orientated learning abilities in order to integrate anatomical concepts applicable to the endocrine glands. SUB-UNITS: 1. Hypothalamus
a. Position and relations of the hypothalamus.
2. Hypophysis
a. Structure, position and relations of the hypophysis. b. Hypophyseoportal system of the hypophysis.
3. Pineal gland a. Position and relations of the pineal gland.
4. Thyroid
a. Position, relations, structure and blood supply of the thyroid gland. b. Embryological development of the thyroid gland
5. Parathyroid glands a. Position of the parathyroid glands
b. Anatomical variations. c. Embryological development of the parathyroid glands.
. 6. Pancreas
a. Structure of the pancreas. b. Vertebral heights of the various parts of the pancreas. c. Arterial blood supply and venous drainage of the pancreas. d. Relations of the pancreas
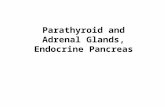
7. Adrenal glands
a. Structure and relations of the adrenal glands. b. Arterial blood supply and venous drainage of the adrenal glands.
c. Relationship of the autonomic plexuses to the adrenal glands. 8. Testis

a. General structure of the testis b. Arterial supply, venous drainage, lymph drainage and nerve supply of the
testis. c. Embryological development and descent of the testis.
9. Ovaries
a. Structure, relationships, arterial supply, venous drainage, lymph drainage and nerve supply of the ovaries.
b. Embryological development and descent of the ovaries
.
EMBEDDED KNOWLEDGE: The student must know the names and understand the position of the endocrine glands as done in block 1. The student must be able to define the differences between endocrine and exocrine glands. Know the functions of the hypothalamus.
ASSESSMENT CRITERIA: Self assessment 1. Sketch all the structures dealt with in these study unit themes. 2. Sketch the hypophyseoportal system between the hypothalamus and the hypophysis. 3. Describe the anatomical basis for the clinical syndrome that results from the
secondary pressure effects from a hypophyseal tumour. 4. List the clinical syndromes and their anatomical basis resulting from enlargement of
the thyroid. 5. Give the reason why the parathyroid bodies develop as they do. 6. Discuss the anatomical basis of the pancreas as an endocrine organ. 7. Sketch the arterial supply and the venous drainage of both adrenal glands. 8. Discuss the route of descent of the testis. Explain the arterial supply and venous
drainage. 9. List the different structures that might be implicated during enlargement of the ovaries
and explain the possible clinical picture that might develop. Peer assessment You must be able to discuss the subunits with your fellow students. Formative and summative evaluation One test on these unit themes is written during the block.
ASSESSMENT PORTFOLIO: Identification of the various components of the endocrine system with an appreciation of the clinical conditions related to the relationships and embryology of these glands.
CRITICAL SKILLS: The student must be able to: 1. Hypothalamus
a. Name and identify the position, relations and nuclei of the hypothalamus.
2. Hypophysis

a. Name and identify the position, relations and parts of the hypophysis. b. Name and identify the clinically important structures anatomically related to
the hypophysis. c. Explain the anatomical basis for bitemporal hemianopia that occurs in the
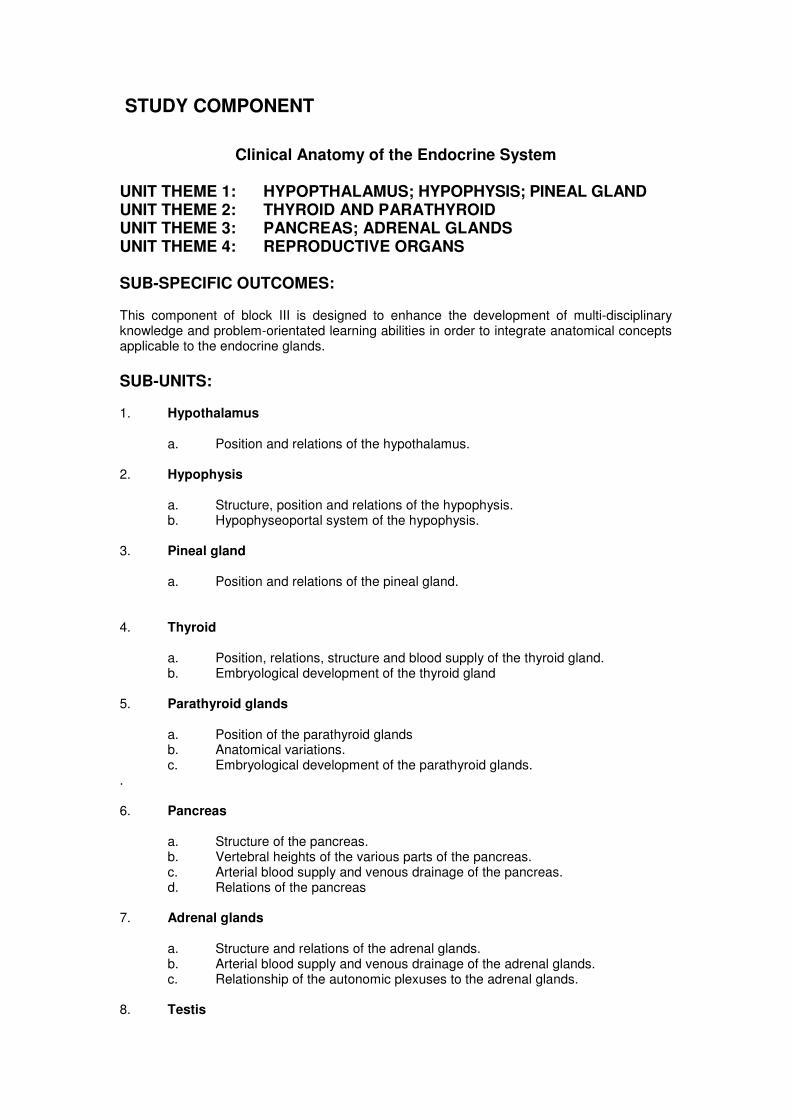
presence of a hypophyseal tumour. d. Identify the hypophyseal fossa on a lateral skull X-ray. e. Identify the hypophysis on CT (computerized tomography) or MRl (magnetic
resonance imaging). f. Describe the hypophyseoportal system of the hypophysis.
3. Pineal gland a. Name and identify the position, and relations of the pineal gland. b. Identify the position of the pineal gland on a plain film X-ray, CT or MRI of the
skull. 4. Thyroid
a. Discuss the position, relations, structure and blood supply of the thyroid gland. b. Briefly discuss the embryological development of the thyroid gland and the
clinical relevance thereof. c. Name the structures affected by enlargement of the thyroid and list the effects thereof.
d. List the relationship of the thyroid to the following clinically important structures - trachea, carotid arteries, recurrent laryngeal nerve, external laryngeal nerve, thyroidal arteries and parathyroids.
e. Identify the thyroid on CT scans or MRl. 5. Parathyroid glands
a. Briefly describe the position of the parathyroid glands and indicate the importance of anatomical variation.
b. Explain embryologically the reasons for anatomical variation in the position of the parathyroids.
6. Pancreas
a. Discuss the macroscopic structure of the pancreas. b. List the vertebral heights of the various parts of the pancreas. g. Discuss the arterial blood supply and venous drainage of the pancreas. d. Discuss the anatomical basis by which the pancreas is both an endo- and
exocrine gland. e. List the posterior relations of the head of the pancreas that may become
involved in enlargement of the tumour of the head of the pancreas. List the signs and symptoms of obstruction that may result.
f. Identify the pancreas on CT scans or MRl. 7. Adrenal glands
a. Name the structure and list the relations of the adrenal glands. b. List the arterial blood supply and venous drainage of the adrenal glands.
c. Name the relationship of the autonomic plexuses to the adrenal glands. d. Identify the regions of the adrenals on a coronal section of the glands. e. Identify the adrenals on CT scans or MRl. 8. Testis
a. Note the unexpected arterial supply, venous drainage, lymph drainage and
nerve supply of the testis.

b. Discuss the embryological descent of the testes c. Describe the general structure of the testis. d. Consider the function of the Leydig cells (interstitial cells).
9. Ovaries and Uterus a. Note the unexpected arterial supply, venous drainage, lymph drainage and
nerve supply of the ovaries. b. Discuss the embryological descent of the ovaries. c. Identify the ovaries on CT scans or MRl. d. Describe the general structure of the ovary.
REFERENCES: Clinically oriented Anatomy: Moore and Dalley 5
th edition: 105-112, 214 – 229, 239, 242,
266, 283- 289, 308 – 320, 335, 350 - 352, 393, 405- 409, 410- 429, 451- 459, 461- 466, 471- 472, 474, 475, 908 - 926, 1020, 1038, 1040, 1046, 1080, 1081-1089, 1102, 1105, 1106, 1108, 1115-1116, 1119.
Clinically oriented Anatomy: Moore and Dalley 6th
edition: 205-206; 209-210; 240; 265-268; 294-5; 382-383; 875; 878-879; 884; 961; 1039-1044.
Human Anatomy: JH Meiring et al: 48-54, 63-67, 168 – 172, 190, 191, 316, 317, 378-380, 492, 493, 494, 495, 496, 547, 549, 551, 553, 555-556, 575, 598, 602-605, 620, 621-624, 731, 737, 744, 745, 747, 737-739, 744-745, 747, 753.
Gray’s Anatomy for Students: 2nd
edition: 188; 260-1; 320-22; 358-9; 448-450; 454; 825; 836; 838; 964-968
Netters’ Atlas 4th
edition: Plates 3, 5, 6, 9 - 11, 49, 74 - 76, 103, 104, 106 - 108, 120, 139, 140, 147- 151, 257, 259, 260, 278, 298, 299, 301, 304, 315, 319, 328, 329, 332, 342, 346, 347, 350, 361,369- 371, 384, 386, 387, 390
Embryology for the Health Student: Jacobs, Greyling and Meiring 63-67 Neuroanatomy: Bosman 2
nd edition: 5, 53, 54, 58, 59, 96, 97
TERMINOLOGY: Optic nerve, optic chiasma, optic tract, optic radiation, bitemporal hemianopia, infundibulum, hypophysis, thalamus, hypothalamic sulcus, hypothalamus, adenohypophysis, neurohypophysis, sella turcica, hypophyseal fossa, sphenoid bone and sinus, cavernous sinus, internal carotid artery, circle of Willis, cranial nerves: III, IV, V1, V2, VI, diaphragma sellae, pharyngeal pouches, thyroid, parathyroid, thymus, pancreas, suprarenal/ adrenal gland, testis, ductus/ vas deferens/ spermatic cord, inguinal canal, superficial and deep inguinal ring, ovary, uterine tube/ fallopian tube, CT scan, MRI.
UNIT THEME 1: HYPOTHALAMUS; HYPOPHYSIS; PINEAL GLAND
1. Name and identify the position, relations and parts of the hypothalamus, hypophysis and pineal gland. (Meiring: 316, 317, 744, 747; Netter: 6, 9-11, 103, 104, 106, 107, 147, 148, 149, 150; Moore 5
th edition: 922, 926, 1038, 1040, Moore 6
th edition: 875, 879, 961;
Neuroanatomy: 53, 58, 59, 96, 97; Gray’s: 836; 837; )

Anterior
Optic chiasma
Optic nerve
Optic tract
Mammillary
body
Midbrain
Hypophysis
Thalamus
above
hypothalamic
sulcus
Pineal
gland
Midbrain
Mammillary
body
Sphenoid
air sinus
Hypophysis
Hypothalamus
below
hypothalamic
sulcus
Optic
chiasma
Infundibulum

Optic chiasma
Pituitary gland

2. Describe the hypophyseoportal system of the hypophysis Netter plate 148
Pineal gland
Anterior
Thalamus
Hypothalamic sulcus
Hypothalamus
Optic chiasma
Infundibulum
Adenohypophysis
Neurohypophysis

3. Case study to demonstrate the relationships of the hypophysis Mrs Erasmus is diagnosed with a tumour of the hypophysis. She suspects that her vision is deteriorating, as she could not see the car in the right lane when she was overtaking another car. Her doctor examines her visual fields and makes the concomitant diagnosis of bitemporal hemianopia. 3.1 Name the relationships of the hypophysis. Moore and Dalley 5
th edition: p. 912, 1020;
Moore and Dalley 6th edition p. 961; Neuroanatomy: 5, 53, 54; Netter 4
th ed: 104,106, 107
optic chiasma anterior-superior, sphenoid air sinus inferiorly, diaphragma sellae superiorly and the left and right cavernous sinus with its contents on either side.
3.2 Is there any relationship between the 2 diagnoses made? How can a tumour of the
hypophysis cause visual disturbances? Meiring p 744, Moore and Dalley 5th edition: p.
912; Moore and Dalley 6th edition p. 875, 876
Superior extension of a pituitary tumour may cause visual symptoms owing to pressure on the optic chiasma found anterior-superior to it.
3.3 Explain bitemporal hemianopia in view of Netter plate 120, Neuroanatomy: 96, 97.
Pituitary/ Hypophysis
Optic nerve
Optic chiasma
Optic tract
Optic radiation


UNIT THEME 2: THYROID AND PARATHYROID
1. Explain the embryology of the thyroid and parathyroid gland. Meiring: 168, 169, 171, 190,191; Embryology for the Health Student: Jacobs, Greyling and Meiring 63-67 The thyroid gland develops between 1
st and 2
nd pharyngeal arch from where it descends. The inferior
parathyroid develops from the 3rd
pharyngeal pouch and descends with the thymus to a more inferior position than the superior parathyroid. The superior parathyroid develops from the 4
th
pharyngeal pouch before it descends.

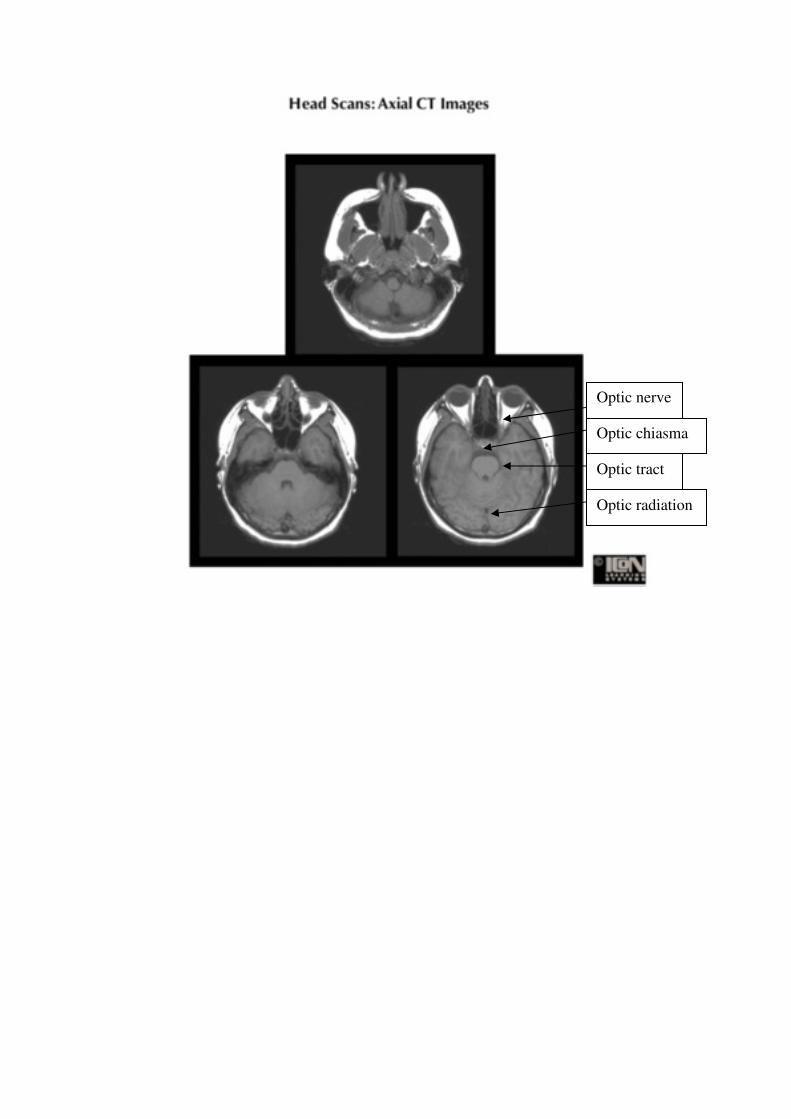
2. Identify the thyroid gland as well as its subdivisions, relationships and blood supply. (Meiring: 168-170, 172 and 745; Netter: 74, 75, 76; Moore 5
th edition: 1046, 1081-
1087, 1115-1116, 1119; Moore 6th edition: 1040-1043; Gray’s 2
nd ed.964-968)
Sternohyoid muscle
Sternothyroid muscle
Thyroid cartilage with laryngeal prominence
Superior thyroid artery
Cricoid cartillage
Isthmus
Left lobe of thyroid gland
Tracheal cartilages
Omohyoid muscle
Inferior thyroid artery
Superior laryngeal nerve
Inferior thyroid vein
Superior thyroid vein
Middle thyroid vein
Pyramidal lobe
Regional nodes:
Paratracheal
Central deep nodes:
Jugulo-omohyoideus
Inferior laryngeal nerve

Moore 6th
edition: p. 1019
3. Identify the parathyroid gland as well as its relationships. (Meiring: 171, 172 and 745; Netter: 76; Moore 5
th edition: 1087, 1088; Moore 6
th edition: 1043,
1044; Gray’s 2nd
ed.964-968)
Trachea
Left lobe of thyroid gland
Oesophagus
Vertebral body
MRI scan of the neck
R L
Inferior parathyroids
Superior parathyroids

4. Case study to demonstrate the relationships of the thyroid gland and embryology of the parathyroid glands. Meiring p168- 172, Netter: 74-76, Moore 5th edtion: 1083-1089; Moore 6th edition: 1040-1044. Embryology for the Health Student: 63, 64 On examination of mrs Jordan a swelling in the neck of 2 cm by 4 cm is felt to the left of the trachea and larynx. The mass moves superiorly when the patient swallows. Fine needle aspiration indicates the presence of a papillary carcinoma. The left lobe and isthmus of the thyroid gland are removed but the left parathyroid gland is spared. Following the surgery, Mrs Jordan complained of hoarseness for 2 weeks. Give the anatomical basis for the following - 4.1 The location of the thyroid. Left lobe is anterolateral to the larynx and trachea 4.2 The relationship between the thyroid and parathyroid glands. External to the thyroid capsule on the medial half of the posterior surface of each lobe of the thyroid inside its sheath: the superior usually 1cm superior to the inferior thyroid arteries, the inferior usually more than 1cm inferior to this artery. 4.3 The post-operative hoarseness. Hoarseness results from unilateral recurrent nerve injury: bruising or pressure of accumulated blood or serous exudates. The right and left recurrent nerves are related to the inferior pole of the thyroid gland. The right recurrent laryngeal nerve is further related to the inferior thyroid artery and its branches.
4.4 The embryological reasons for the variations in the position of the parathyroid glands. The superior parathyroid glands may be as far superior as the thyroid cartilage, and the inferior ones as far inferior as the superior mediastinum. The inferior parathyroid has a variable descent along with the thymus that also originates from the third pharyngeal cleft. The superior parathyroid originating from the fourth pharyngeal cleft descents with the thyroid not as far down as the inferior parathyroid.

UNIT THEME 3: PANCREAS AND ADRENAL GLANDS
Meiring p 547- 549, 555, 556; Netter plate: 278, 298, 299, 301, 304, 315, 319, 328, 329, 332, 342, 346, 347; Moore 5
th edition: 283-289, 314, 316-320; Moore 6
th edition 265-268 and 294-
295 1. Identify the pancreas and adrenal glands
Tail of pancreas Inferior vena
cava
Right suprarenal
gland
Superior
mesenteric artery
Right kidney
Abdominal aorta
Neck of pancreas
Body of pancreas
Head of pancreas
Uncinate process
of pancreas

2. Identify the pancreas and adrenal glands on the MRI scans
Netter plate: 350, Moore 5th edition: p.350, 351, 352; Moore 6
th edition: p.323.
L
Right Left
S
Body of pancreas
Inferior vena cava
Aorta
Tail
Body
Neck
Head
Adrenal

UNIT THEME 4: REPRODUCTIVE ORGANS
1. Identification of the structures of the male genital system.
Meiring: 598-602. 621, 622; Netter: 384, 361; Moore 5th edition: 227-228, 405-409;
Gray’s Anatomy: fig 5.46 Moore 6th edition: 376-380

2,3 Descent of testes through inguinal canal by relative growth: Meiring: 378-380; Netter: 386; Moore 5
th edition: 217, 218; Moore 6
th edition: 205
3.

4.Case study to demonstrate the descent of the testis:
A 12-year-old boy, has only one testis in his scrotum. No testis is detected in either the inguinal opening or the canal. After an MRl-scan the testis is demonstrated in the abdomen. Due to the 35-45 times increased risk of cancer in an undescended testis, especially in children older than ten years of age; it is decided to remove the testis.
Meiring: 378-380; Netter: 386; Moore: 217, 218, 220
Give the anatomical basis for the route followed during descent of the testis and the different
positions where the testis might be located.
By the 12th week of development, the testis is in the pelvis, and by 28 weeks it lies close to
the developing deep ring. The testis begins to pass through the inguinal canal during the 28th
week and takes approximately 3 days to traverse it. Approximately 4 weeks later, the testis
enters the scrotum. The undescended testis usually lies somewhere along the normal path of
its prenatal descent, commonly in the inguinal canal.
5.Identification of the structures of the female genital system. Meiring: 603-605,
Netter: 370, 371, Moore 5th edition: 416, 427-429; Moore 6th edtion: 382-384; Gray’s
Anatomy 2nd edition: fig 5.49 p.453

As for the male gonads the ovaries also develops in the abdomen before descending to the pelvis 6. Identification of the structures of the female genital system on MRI: Moore 5
th ed.: 471,
474, 475; Moore 6th ed. 437
Transverse MRI of pelvis
Anterior Rectus abdominis muscle
External iliac vessels
Lower part of uterus
Ovary
Rectum
Sacrum
Empty bladder