
catheter based management of pulmonary embolism
88
CATHETER BASED THERAPY FOR ACUTE PULMONARY EMBOLISM 11-12-2017 1
-
Upload
amit-verma -
Category
Health & Medicine
-
view
85 -
download
0
Transcript of catheter based management of pulmonary embolism
CATHETER BASED THERAPY FOR ACUTE PULMONARY EMBOLISM
11-12-2017
1

OBJECTIVES
Classification Rationale for Lysis Catheter directed therapy Recent literature
TERMINOLOGY
• “CATHETER-BASED THERAPY” (CBT)- refers to the use of any of several devices and techniques in the pulmonary artery (PA) with or without low-dose thrombolytic therapy.
• “CATHETER-DIRECTED THROMBOLYSIS” (CDT) - refers to the infusion of thrombolytics into the PA via an infusion catheter with multiple exit ports, placed into the PA, preferably into the embolus.
3

STATISTICS
300k-600k per year.1-2 per 1000 people, or as high as 1 in 100 .
Overall 30 day mortality = 9-11% At 3 months = 8.6- 17% Sudden death is presenting symptom in ~ 34%
2012: 166,665 primary admissions for PE.In-hospital mortality ~ 3%
Most commonly from lower extremity DVT.Evidence of DVT in > 50%
CDC.GOV; Agency for Healthcare Research and Quality

High risk
Moderate/intermediate risk
Low risk
• Sustained hypotension (systolicBP <90 mmHg for ≥15 min)
• Inotropic support
• Pulseless
• Persistent profound bradycardia (HR <40 bpm with signs or symptoms of shock)
• Systemically normotensive(systolic BP ≥90 mmHg)
• RV dysfunction
• Myocardial necrosis
• Systemically normotensive(systolic BP ≥90 mmHg)
• No RV dysfunction
• No myocardial necrosis
RV dysfunction•RV/LV ratio > 0.9 or RV systolic dysfunction on echo•RV/LV ratio > 0.9 on CT•Elevation of BNP (>90 pg/mL)•Elevation of NTpro-BNP (>500 pg/mL)•ECG changes:
• new complete or incomplete RBBB• anteroseptal ST elevation or depression• anteroseptal T-wave inversion
Jaff et al. Circulation 2011;123(16):1788-1830.
Jaff et al. Circulation 2011;123(16):1788-1830.
BACKGROUND AND DEFINITIONS
Patient risk stratification (per AHA Scientific Statement 20111)
Massive PE Submassive PE Minor/Nonmassive PE
High risk Moderate/intermediate risk Low risk
– Sustained hypotension (systolic BP<90 mmHg for ≥15 min)– Inotropic support– Pulselessness– Persistent profound bradycardia (HR
<40 bpm with signs or symptoms of shock)
– Systemically normotensive (systolic BP ≥90 mmHg)
– RV dysfunction– Myocardial necrosis
– Systemically normotensive (systolic BP ≥90 mmHg)
– No RV dysfunction– No myocardial necrosis
massive PE
submassive PE
minor PE
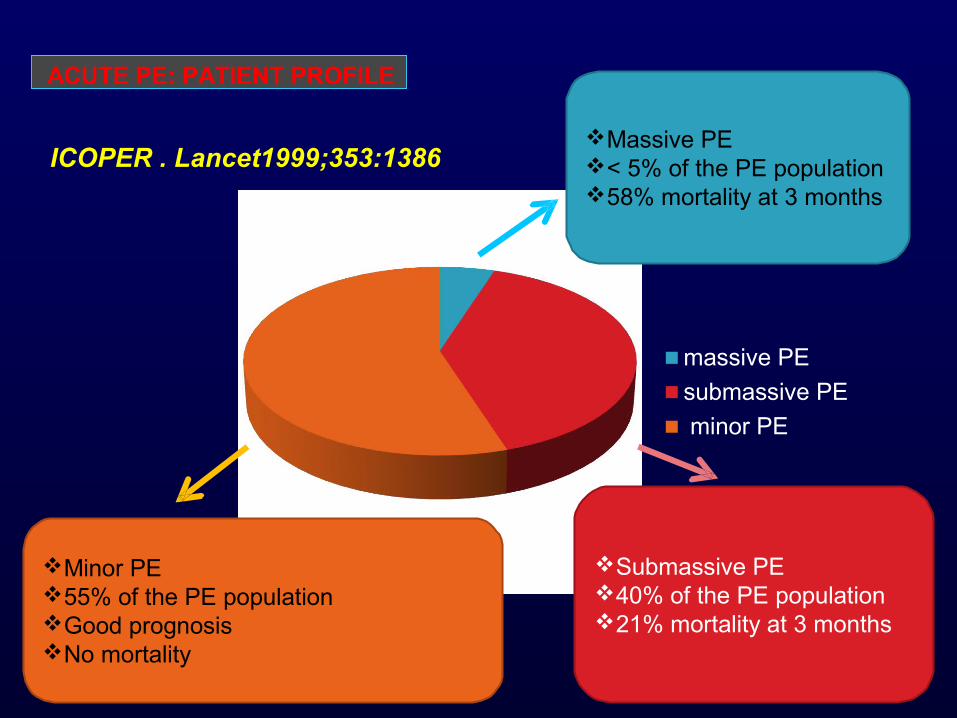
Massive PE< 5% of the PE population58% mortality at 3 months
Submassive PE40% of the PE population21% mortality at 3 months
Minor PE55% of the PE populationGood prognosisNo mortality
ACUTE PE: PATIENT PROFILE
ICOPER . Lancet1999;353:1386
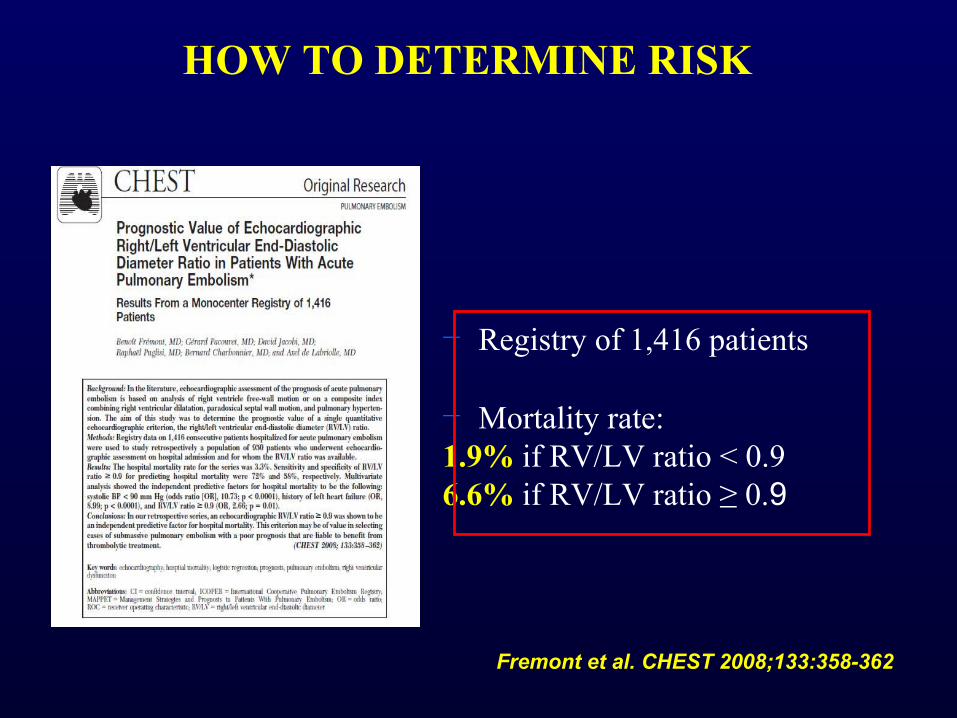
− Registry of 1,416 patients
− Mortality rate:1.9% if RV/LV ratio < 0.96.6% if RV/LV ratio ≥ 0.9
Fremont et al. CHEST 2008;133:358-362
HOW TO DETERMINE RISK

− Retrospective analysis of 120 patients with hemodynamically stable PE based on chest CT
− PE-related mortality at 3 months:
17% if RV/LV ≥ 1.5 8% if 1.0 ≤ RV/LV < 1.5 0% if RV/LV < 1.0
Van der meer et al. Radiology 2005; 235:798-803.
HOW TO DETERMINE RISK
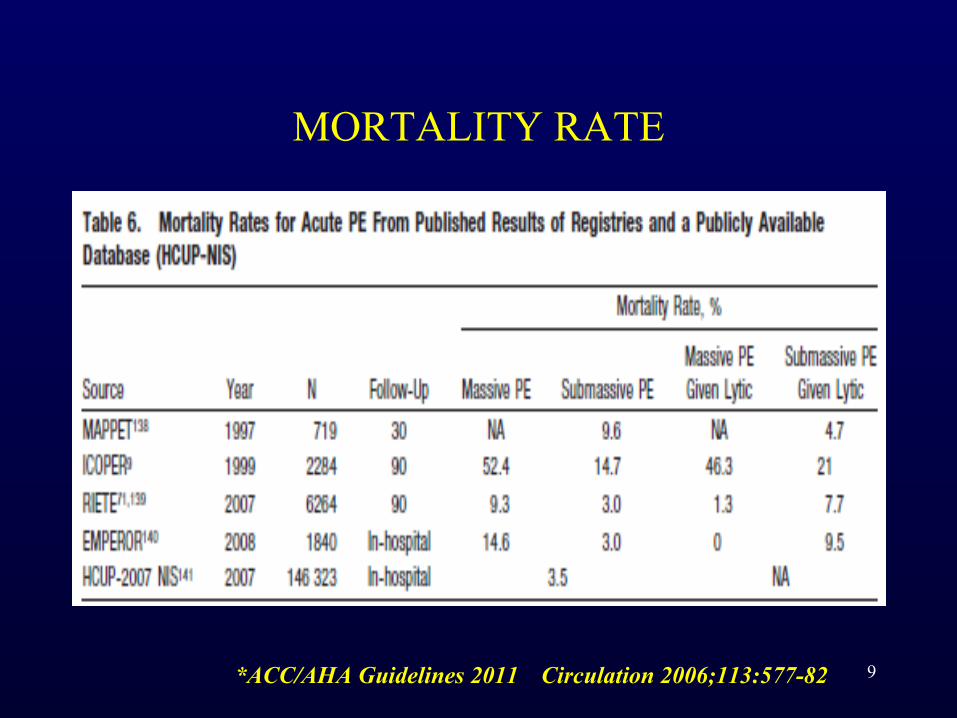
MORTALITY RATE
9*ACC/AHA Guidelines 2011 Circulation 2006;113:577-82
10
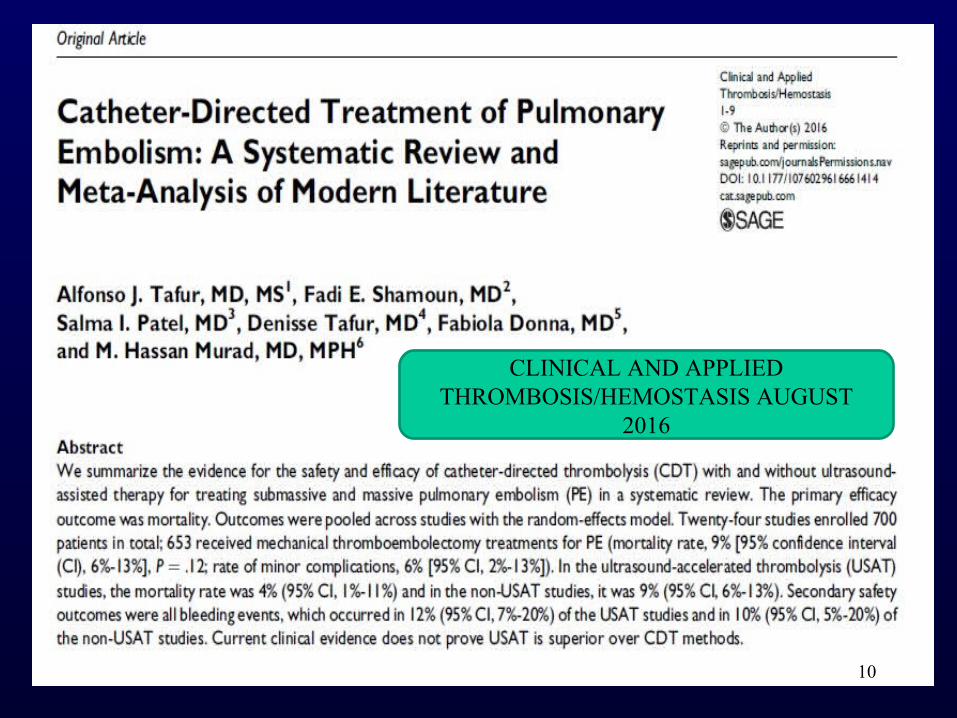
CLINICAL AND APPLIED THROMBOSIS/HEMOSTASIS AUGUST
2016
11
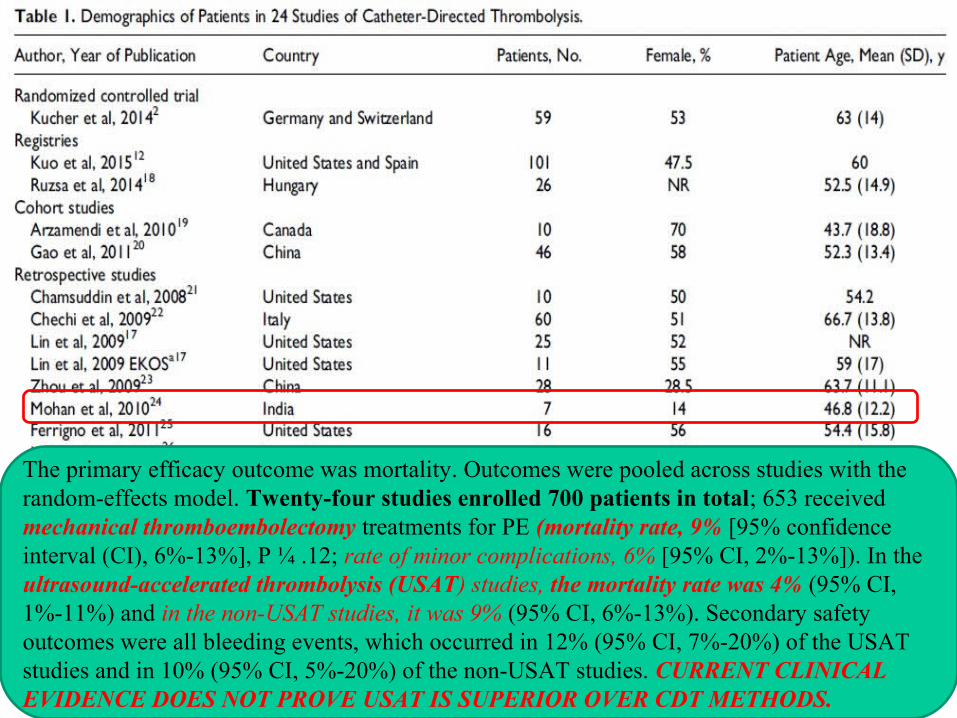
The primary efficacy outcome was mortality. Outcomes were pooled across studies with the random-effects model. Twenty-four studies enrolled 700 patients in total; 653 received mechanical thromboembolectomy treatments for PE (mortality rate, 9% [95% confidence interval (CI), 6%-13%], P ¼ .12; rate of minor complications, 6% [95% CI, 2%-13%]). In the ultrasound-accelerated thrombolysis (USAT) studies, the mortality rate was 4% (95% CI, 1%-11%) and in the non-USAT studies, it was 9% (95% CI, 6%-13%). Secondary safety outcomes were all bleeding events, which occurred in 12% (95% CI, 7%-20%) of the USAT studies and in 10% (95% CI, 5%-20%) of the non-USAT studies. CURRENT CLINICAL EVIDENCE DOES NOT PROVE USAT IS SUPERIOR OVER CDT METHODS.
Various studies report presence of right ventriculardysfunction (RVD) as a predictor of poor clinical outcomes:
1.Mortality
2.Adverse events
3.VTE recurrence
WHY TREAT SUBMASSIVE PE PATIENTS AGGRESSIVELY?
PULMONARY EMBOLISM RESPONSE TEAM(PERT)
• Multiple centers have formed multidisciplinary pulmonary embolism response teams (PERT) to engage specialists from different backgrounds to discuss treatment options and provide immediate advice and therapy for patients in the massive and submassive categories.
13
PERT PROTOCOL
14
PERT PROTOCOL
15
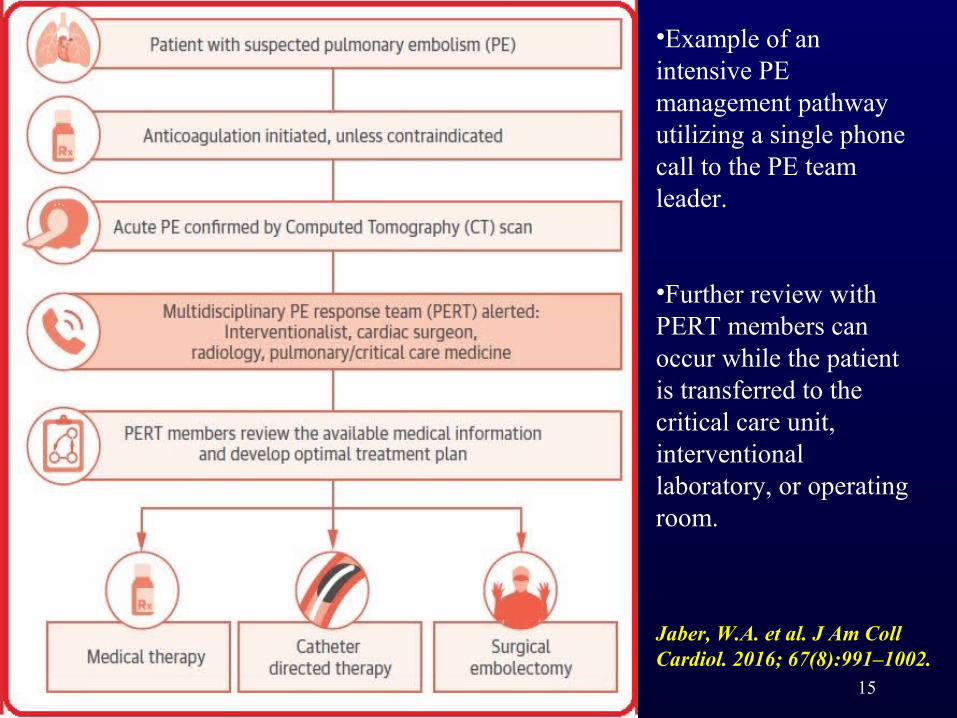
•Example of an intensive PE management pathway utilizing a single phone call to the PE team leader.
•Further review with PERT members can occur while the patient is transferred to the critical care unit, interventional laboratory, or operating room.
Jaber, W.A. et al. J Am Coll Cardiol. 2016; 67(8):991–1002.

16ER PE Protocol Utilizing PERT Consultation and sPESI Score

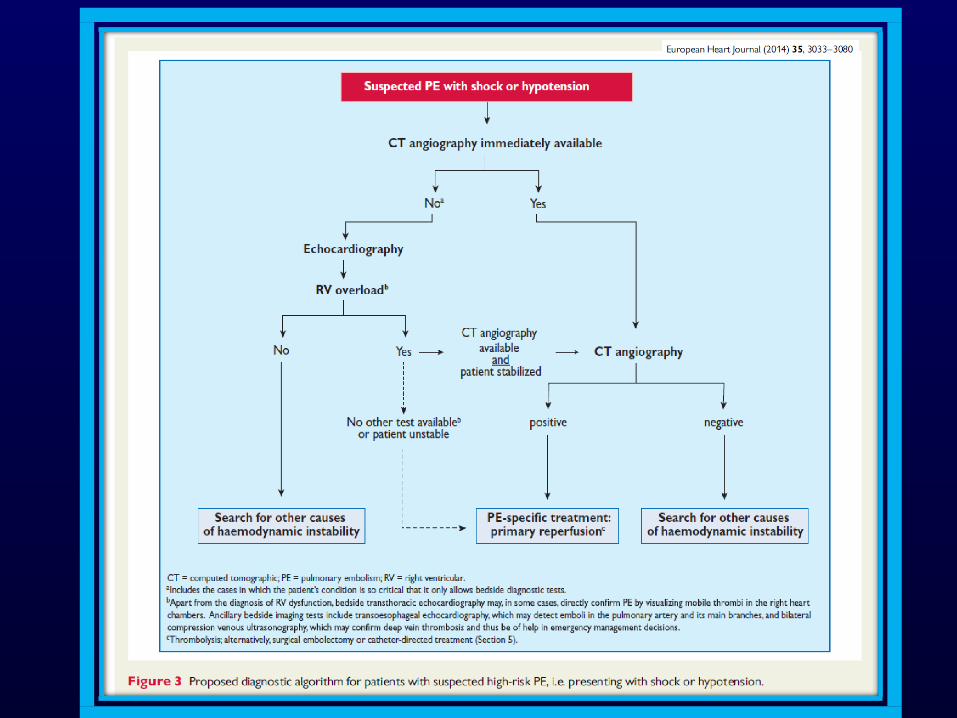
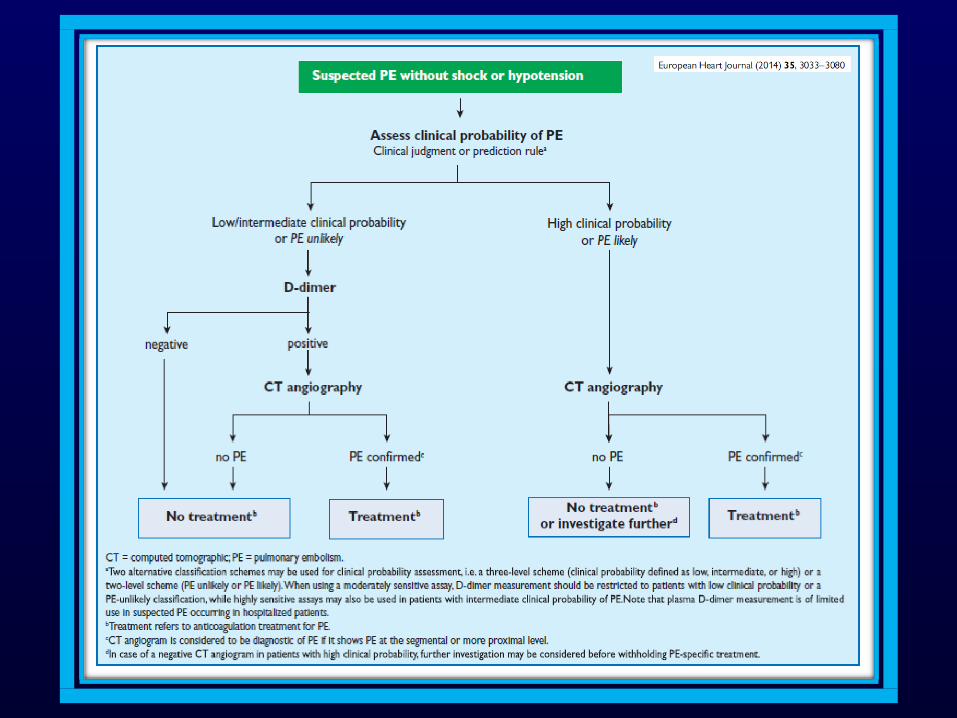
17European Heart Journal, Volume 35, Issue 43, 14 November 2014, Pages 3033–3073
20
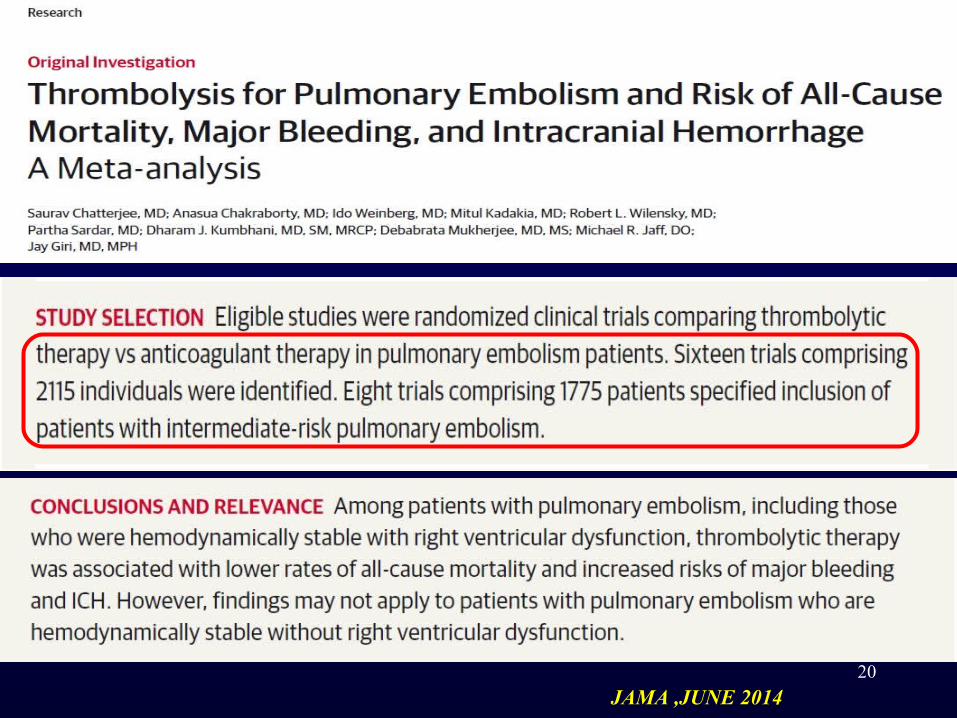
JAMA ,JUNE 2014
1/16/2016
16
RCT’S COMPARING SYSTEMIC THROMBOLYSIS PLUS ANTICOAGULATION WITYH ANTICOAGULATION ALONE
IN PATIENTS WITH ACUTE PE.
RISKS AND BENEFITS COMPARED
15 RCT’SN= 2057
PATIENTS
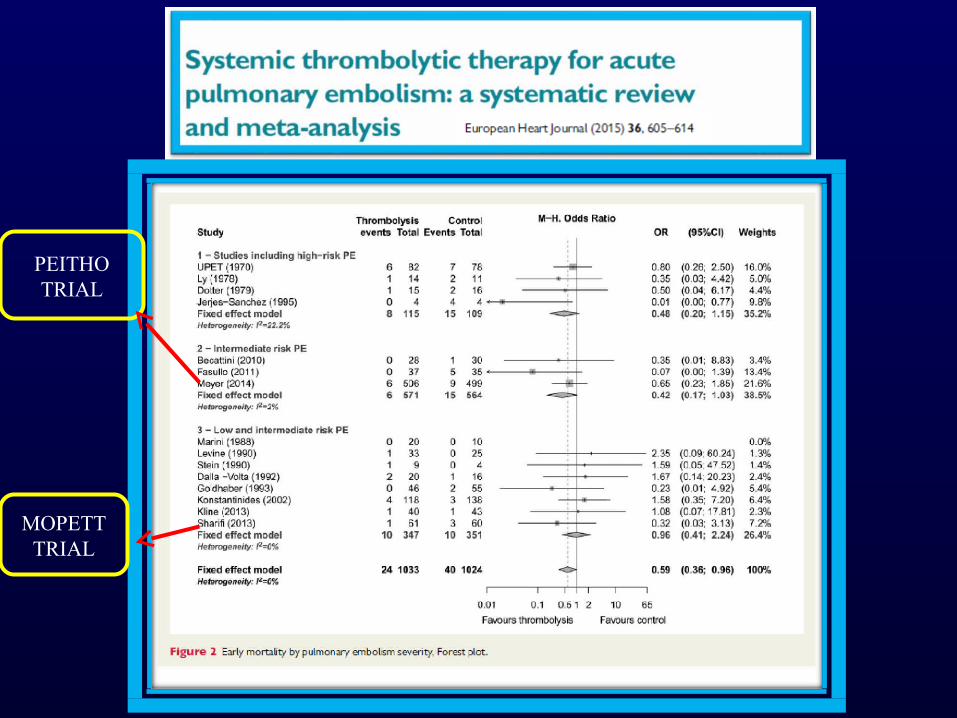
PEITHO TRIAL
MOPETTTRIAL

BENEFIT OF IV THROMBOLYSIS IN SUBMASSIVE OR INTERMEDIATE RISK PE
• PEITHO Trial
• Primary Objective:
• To investigate the clinical benefits (efficacy) of thrombolysis with tenecteplase over placebo in normotensive patients with acute intermediate risk PE ‐ (both treatment arms receive standard heparin anticoagulation)
• Secondary Objective:• To assess the safety of tenecteplase
in patients with intermediate risk ‐PE
APRIL,2014
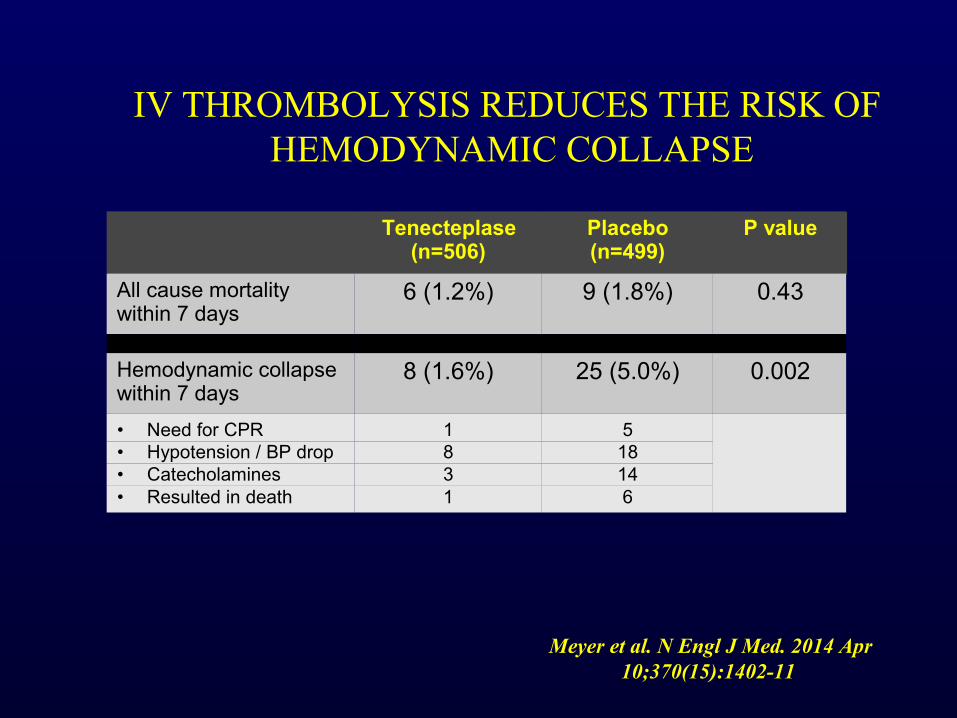
IV THROMBOLYSIS REDUCES THE RISK OF HEMODYNAMIC COLLAPSE
Tenecteplase (n=506)
Placebo (n=499)
P value
All cause mortality within 7 days
6 (1.2%) 9 (1.8%) 0.43
Hemodynamic collapse within 7 days
8 (1.6%) 25 (5.0%) 0.002
• Need for CPR 1 5• Hypotension / BP drop 8 18• Catecholamines 3 14• Resulted in death 1 6
Meyer et al. N Engl J Med. 2014 Apr 10;370(15):1402-11
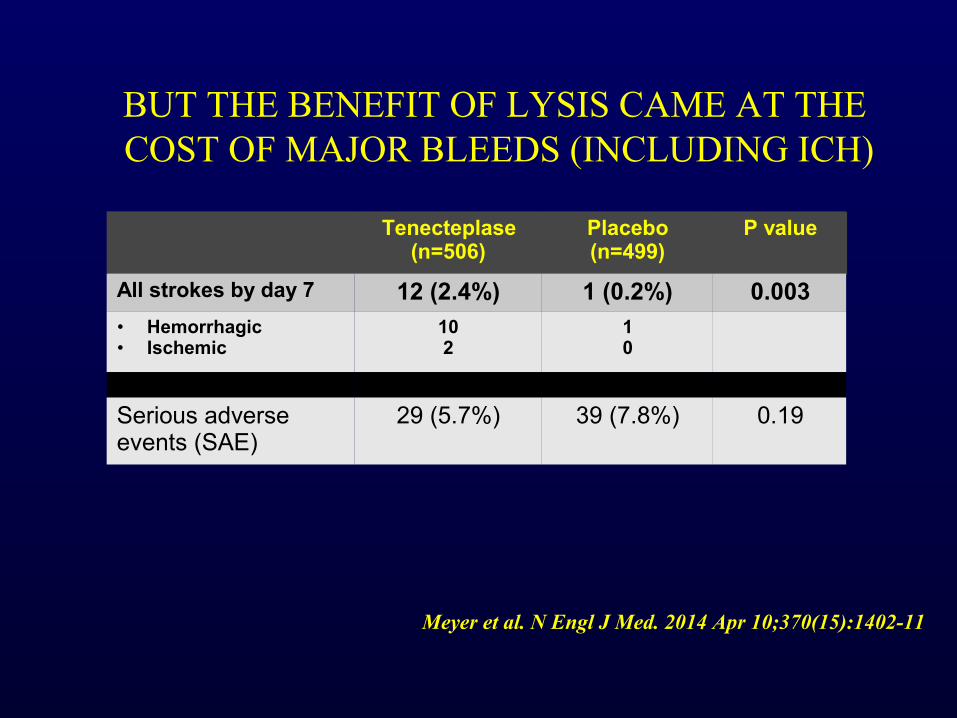
BUT THE BENEFIT OF LYSIS CAME AT THE COST OF MAJOR BLEEDS (INCLUDING ICH)
Meyer et al. N Engl J Med. 2014 Apr 10;370(15):1402-11
Tenecteplase (n=506)
Placebo (n=499)
P value
All strokes by day 7 12 (2.4%) 1 (0.2%) 0.003
• Hemorrhagic• Ischemic
102
10
Serious adverse events (SAE)
29 (5.7%) 39 (7.8%) 0.19

CRITERIA FOR THROMBOLYSIS IN PULMONARY EMBOLISM : PRINCIPAL INCLUSION CRITERIA
1. Massive pulmonary embolism
2. Anatomically small or moderate PE with hemodynamic instability
3. Hemodynamically stable, but RV dysfunction detected on baseline echocardiogram
27
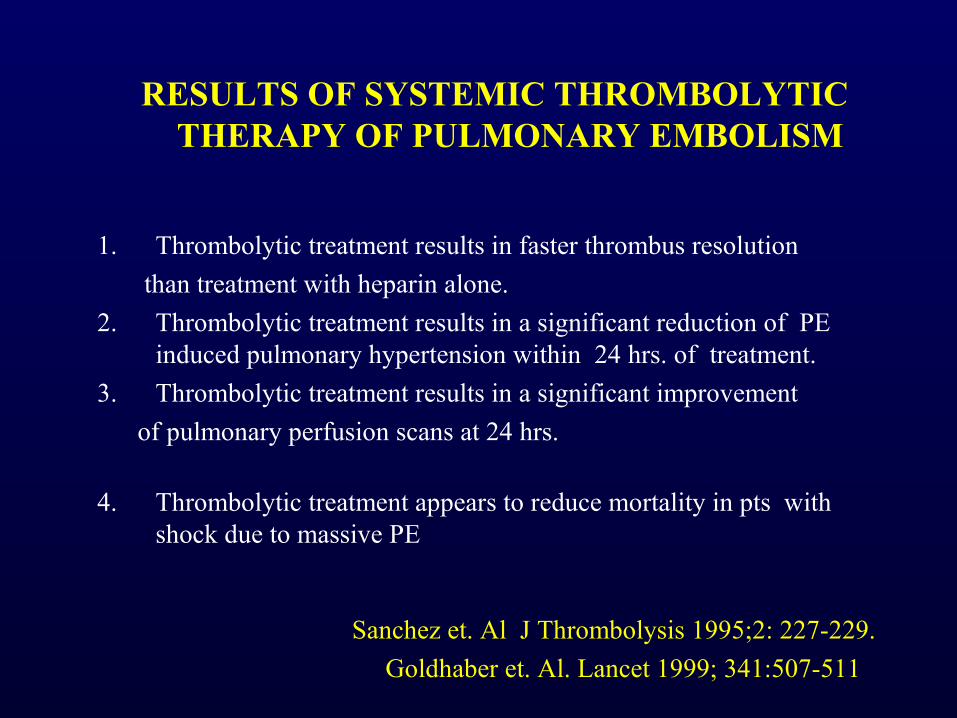
RESULTS OF SYSTEMIC THROMBOLYTIC THERAPY OF PULMONARY EMBOLISM
1. Thrombolytic treatment results in faster thrombus resolution
than treatment with heparin alone.
2. Thrombolytic treatment results in a significant reduction of PE induced pulmonary hypertension within 24 hrs. of treatment.
3. Thrombolytic treatment results in a significant improvement
of pulmonary perfusion scans at 24 hrs.
4. Thrombolytic treatment appears to reduce mortality in pts with shock due to massive PE
Sanchez et. Al J Thrombolysis 1995;2: 227-229.
Goldhaber et. Al. Lancet 1999; 341:507-511
RESULTS OF THROMBOLYTIC THERAPY OF PULMONARY EMBOLISM
5. Thrombolytic treatment does not reduce mortality or incidence of recurrent PE in hemodynamically stable pts.
6. Thrombolytic treatment possibly improves hemodynamic response to exercise.
(Arcasoy,Chest 1999; 115:1695-1707)
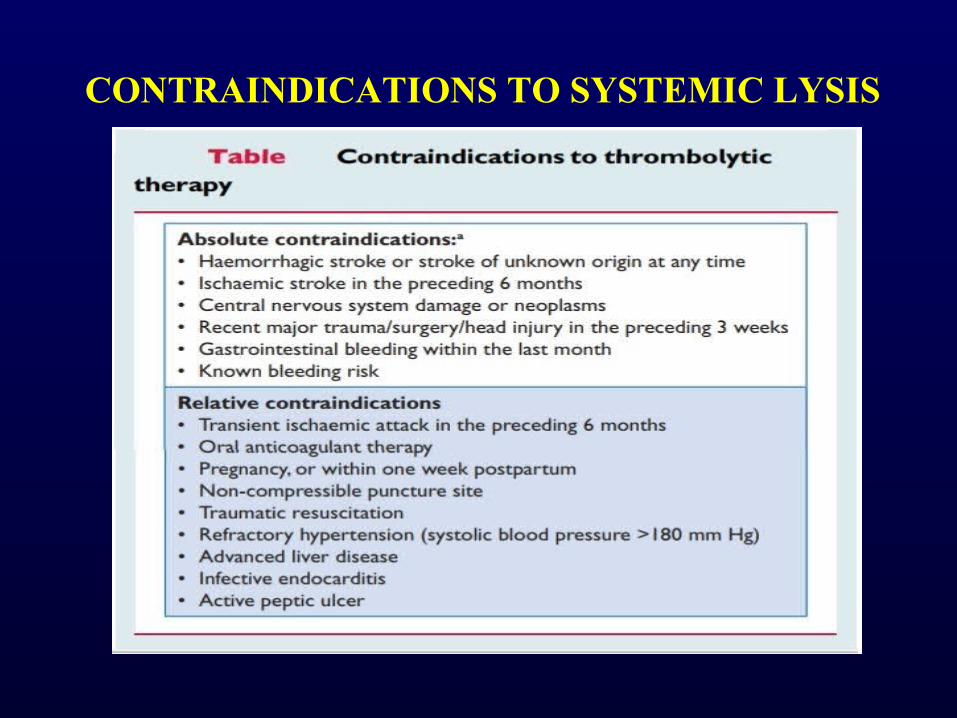
CONTRAINDICATIONS TO SYSTEMIC LYSIS
CATHETER BASED THERAPIES
• Alternative or additive treatment for massive PE• Wide variety of devices and techniques, with goal of
rapidly reducing clot burden:
1. Intra thrombus lytic administration
2. Thrombus fragmentation
3. Thrombus aspiration

CONSENSUS STATEMENT SUMMARIES
32

GUIDELINES
33
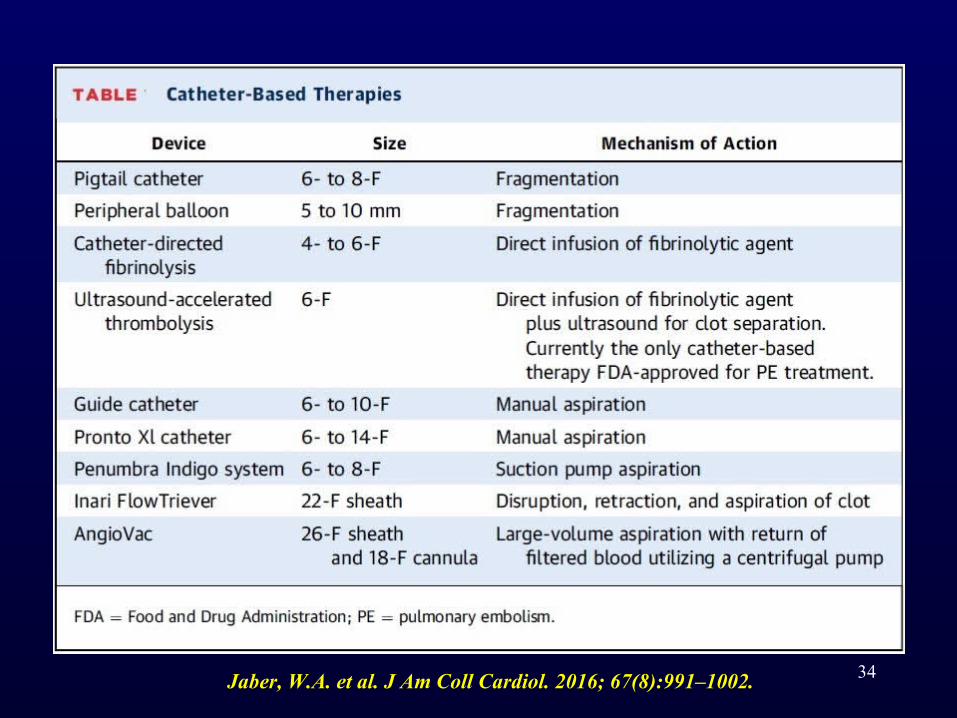
34Jaber, W.A. et al. J Am Coll Cardiol. 2016; 67(8):991–1002.

35
Respir Crit Care Med 2017;38:73–83.
CATHETER-DIRECTED THROMBOLYSIS VIA INFUSION CATHETERS
• Catheter-directed thrombolysis via multi-sidehole infusion catheters is the least technically challenging.
• Relatively superior.
36

• In recent prospective registry of 101 massive and submassive PE patients treated with catheter-based therapy (mostly local fibrinolysis), there was a significant decrease in PA pressure and improvement in RV function, with no reported major complications, major bleeding, or strokes.
PERFECT registry Chest 2015;148:667–73.
• In a series of 52 PE patients treated with CDF, a more prominent hemodynamic benefit was obtained in patients with symptom duration <14 days, as compared with those with a longer symptom duration.
Engelberger RP et al.Eur Heart J 2015;36:597–604.
37
INDICATIONS
• Stabilized massive PE who have contraindications to systemic fibrinolysis .
• In patients with intermediate-high–risk PE (those with RV dysfunction and increased biomarkers), particularly those deemed at increased bleeding risk with full-dose systemic fibrinolysis.
38

PROCEDURE
• Internal jugular or femoral venous access with ultrasound guidance is obtained.
• For femoral access, ultrasound is used to rule out iliofemoral thrombus.
• A catheter (e.g., balloon-tipped, pigtail, or multipurpose) is carefully advanced to the main PA, where pressure and blood oxygen saturation sampling are obtained.
• Contrast injection into the main PA or selectively into each PA can be performed to identify the location of the thrombi; these are typically in the main and/or lower main PA branch.
39

• Power injection may be necessary (e.g., at 15 to 20 m/s for a total of 30 ml selectively in each main PA) if location of the thrombi is not clear and pulmonary pressure is not severely elevated.
• An exchange-length soft- or j-tipped wire is placed in the lower PA branch, and the diagnostic catheter is exchanged for an infusion catheter, which has a treatment zone of 6 to 12 cm through which t-PA may be infused into the clot.
• A second infusion catheter may be placed in the contralateral PA through a second venous sheath, if needed, using the same technique.
40

• A commonly used t-PA dose is 0.5 to 1.0 mg/h per catheter.
• The total t-PA dose is typically between 12 and 24 mg, delivered over 6 to 24 h.
• Lowdose, weight-adjusted heparin infusion is usually continued during t-PA infusion, with a target partial thromboplastin time on the low end of the therapeutic range (e.g., 40 to 60 s).
• Commonly available infusion catheters – Cragg-McNamera catheter, Fountain catheter Unifuse catheter
41
• The risk of intracranial hemorrhage is <0.2%.
SEATTLE II Study. J Am Coll Cardiol Intv2015;8:1382–92
PERFECT: Registry.Chest 2015;148:667–73..
Engelberger RP, et al Eur Heart J 2015;36:597–604.
42

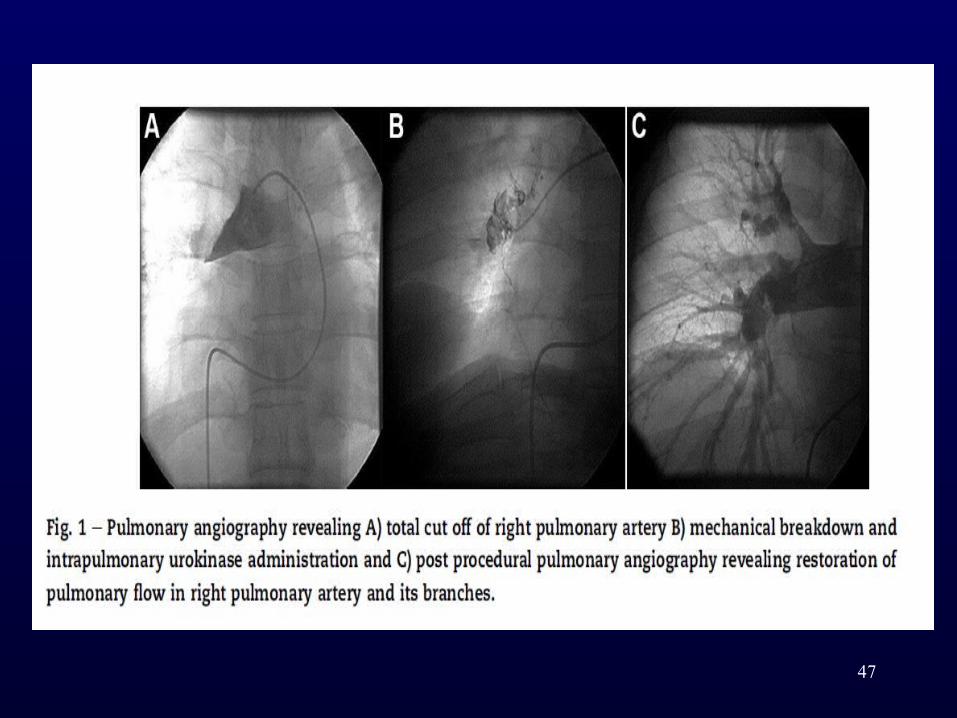
CATHETER FRAGMENTATION FOLLOWED BY LOCAL INTRAPULMONARY
THROMBOLYSIS
• GOAL OF THERAPY - Breakdown the large central fresh clot into multiple small fragments to achieve partial reperfusion for thrombolysis to act and not complete removal of thrombus.
• The proposed mechanisms of improved thrombolytic action are increased exposure of fresh clot surfaces caused by fragmentation accelerating the thrombolytic action.
43

• In addition when there is total occlusion of pulmonary artery occlusion by an embolus, any fluid infused will theoretically make only evanescent contact with thrombus and be washed into the nonoccluded ipsilateral and contralateral pulmonary artery.
• After fragmentation, infused thrombolytics will have greater contact with the distal thrombus throughout the pulmonary arterial tree.
Tajima H et al AJR Am J Roentgenol. 2004;183:589e595. Mohan et al. Indian Heart Journal 66(20 14)294 e301
44
45Tajima H, Murata S, Kumazaki T, et al. AJR Am J Roentgenol. 2004;183:589e595.
CONCLUSION. Hybrid treatment with mechanical fragmentation using a rotating pigtail catheter combined with local fibrinolysis and manual clot aspiration resulted in a rapid and safe improvement in the hemodynamic condition of patients with acute massive pulmonary thromboembolism. This hybrid treatment appears to be especially useful in patients at high
risk for right ventricular failure and is a minimally invasive alternative to surgical embolectomy
46Indian Heart Journal 66 (2014)294e301
Conclusions: Rapid reperfusion of pulmonary arteries with mechanical fragmentation by pigtail catheter followed by intrapulmonary thrombolysis results in excellent immediate and intermediate term outcomes in patients presenting with high risk pulmonary embolism.
47

ULTRASOUND - ASSISTED LYSIS
• Ultrasound-assisted thrombolytic infusion catheters achieve accelerated thrombolysis using ultrasound waves.
• The EndoWave System (EKOS System) consists of a 5-Fr 106-cm long catheter containing microinfusion pores within the 6–50 cm treatment segment of the catheter that optimize the interface of thrombus with an ultrasound core wire that contains small transducers allowing for delivery of ultrasound waves to the thromboembolus .
48
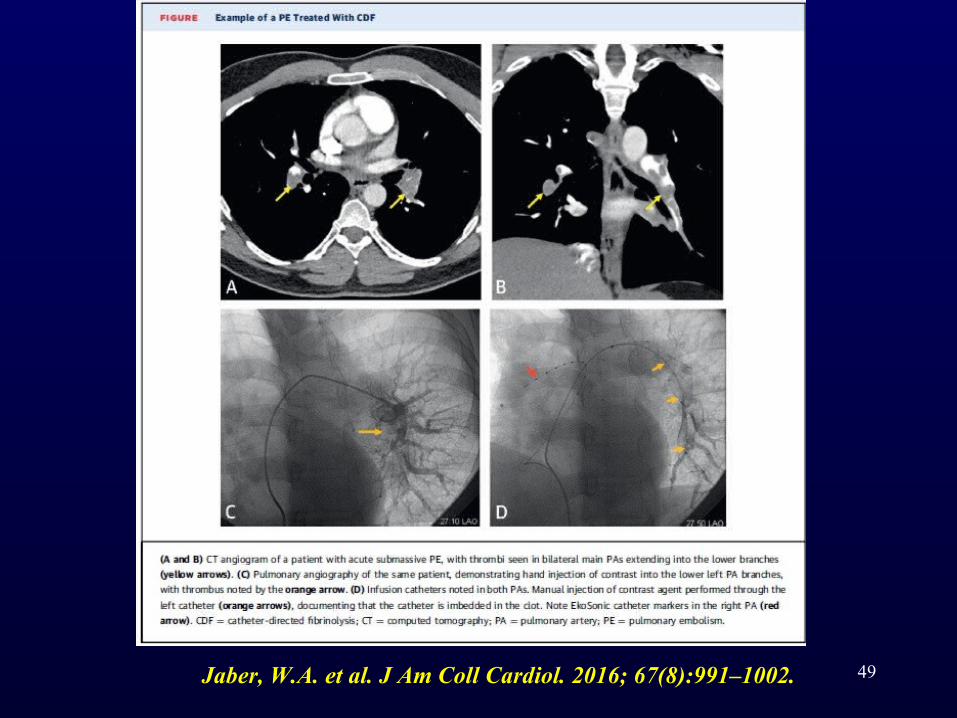
49Jaber, W.A. et al. J Am Coll Cardiol. 2016; 67(8):991–1002.

• Following access to the PA and angiographic examination, exchange is made over a 0.035-inch guidewire for EndoWave catheters containing the ultrasound core wire.
• The catheter also contains a port for tPA infusion (e.g., 0.5 mg/hour per catheter if bilateral, or 1 mg/hour per unilateral catheter), a port for saline to cool heat generated by the ultrasound waves, and an interface cable connected to a control unit in order to deliver ultrasound waves.
• Typically, tPA administration is performed over 18–24 hours.
50
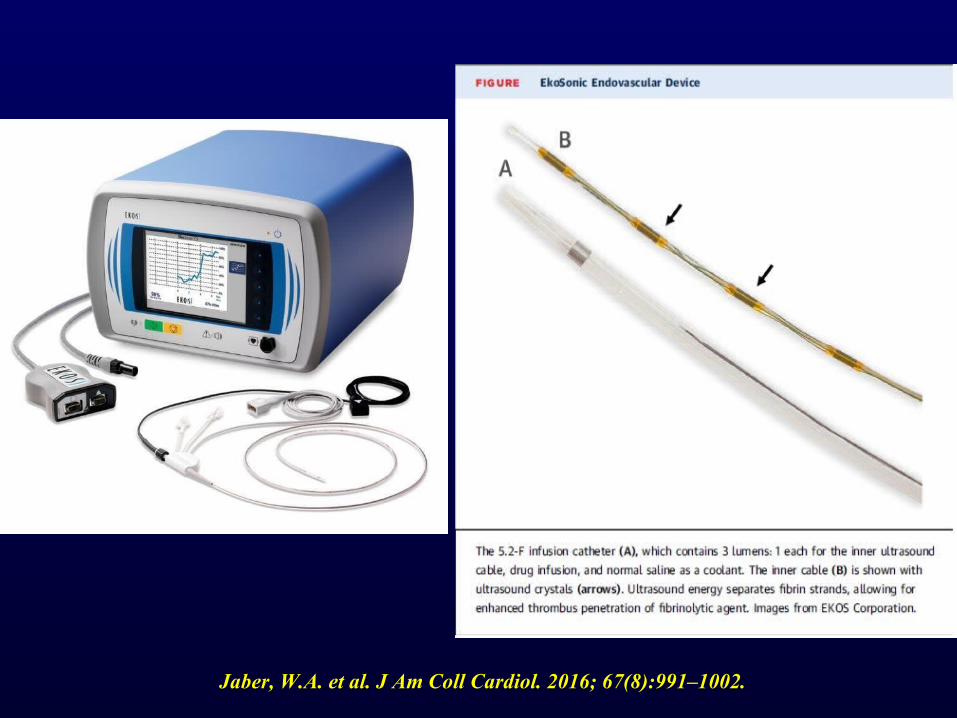
Jaber, W.A. et al. J Am Coll Cardiol. 2016; 67(8):991–1002.



54
Conclusions—In PE patients at intermediate risk, a standardized USAT regimen was superior to anticoagulation with heparin alone in reversing RV dilatation at 24 hours,
without an increase in bleeding complications.
ULTIMA TRIAL NOVEMBER 13, 2013
55
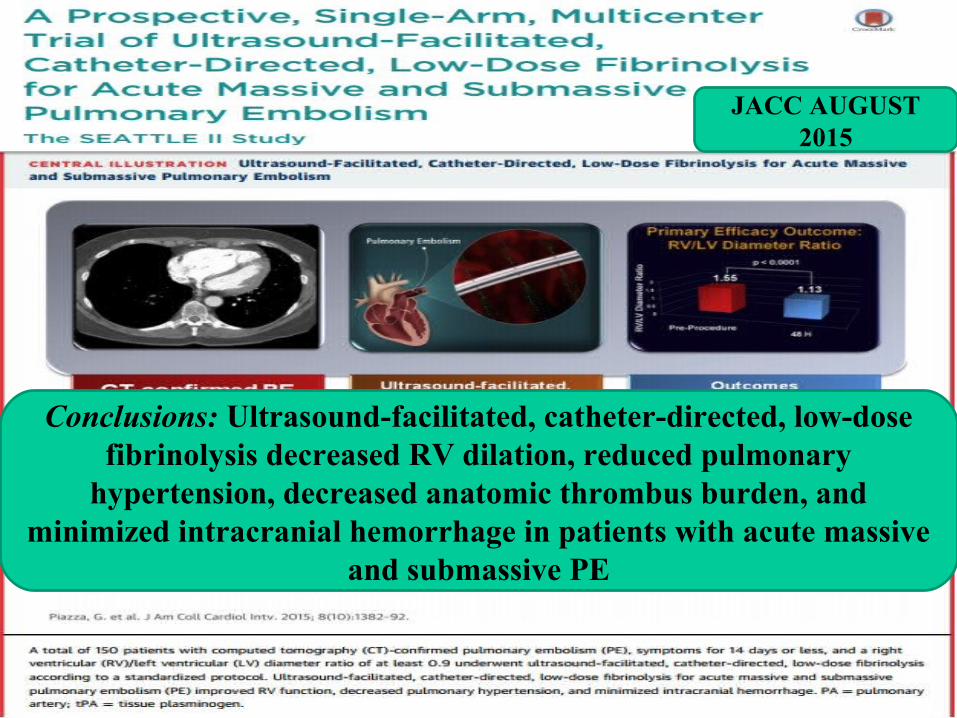
Conclusions: Ultrasound-facilitated, catheter-directed, low-dose fibrinolysis decreased RV dilation, reduced pulmonary
hypertension, decreased anatomic thrombus burden, and minimized intracranial hemorrhage in patients with acute massive
and submassive PE
JACC AUGUST 2015
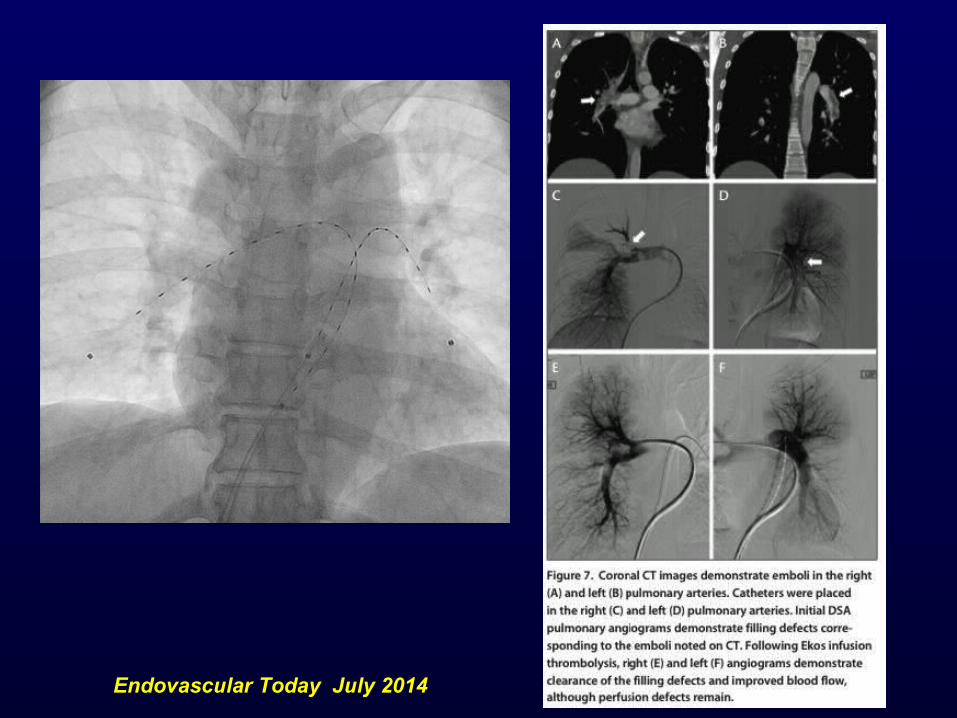
Endovascular Today July 2014
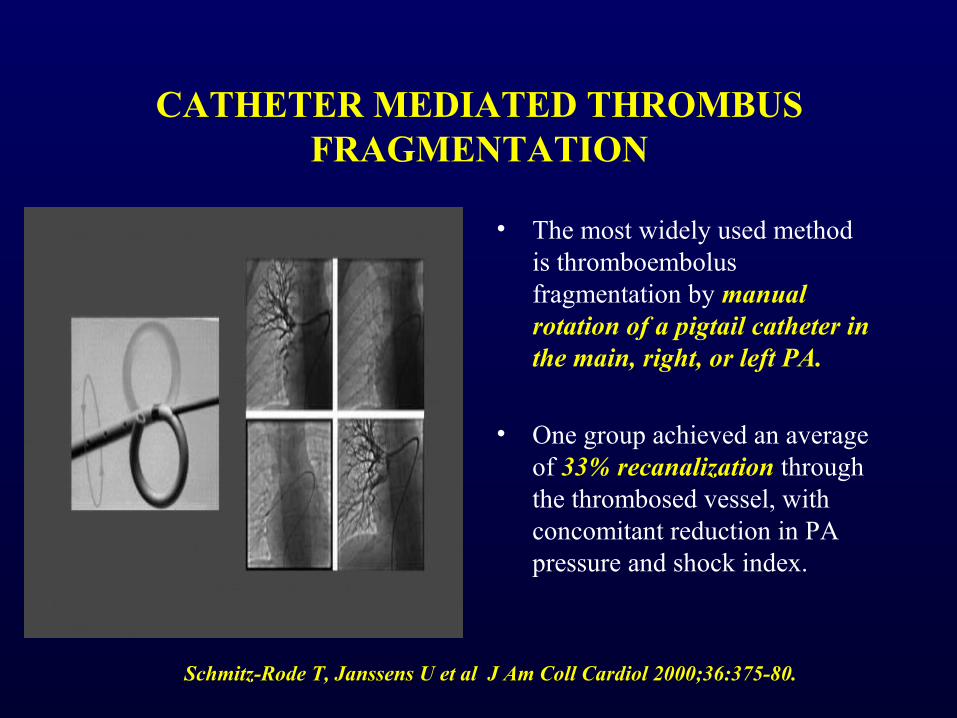
CATHETER MEDIATED THROMBUS FRAGMENTATION
• The most widely used method is thromboembolus fragmentation by manual rotation of a pigtail catheter in the main, right, or left PA.
• One group achieved an average of 33% recanalization through the thrombosed vessel, with concomitant reduction in PA pressure and shock index.
Schmitz-Rode T, Janssens U et al J Am Coll Cardiol 2000;36:375-80.

TECHNIQUE – RHEOLYTIC THROMBECTOMY
• Rheolytic thrombectomy involves thromboembolus fragmentation using a saline jet directed from the tip of the catheter with simultaneous emulsified thrombus removal via a separate channel .
1. Amplatz thrombectomy device
2. the Cordis hydrolyser hydrodynamics thrombectomy catheter
3. the Oasis Thrombectomy System
4. the AngioJet Rapid Thrombectomy System.
58

TECHNIQUE – RHEOLYTIC ASPIRATION
• The AngioJet system employs BERNOULLI HYDRODYNAMICS: high velocity moving fluid has low central pressure, creating a vacuum, with preferential movement of surrounding molecules into the center of the fluid.
• The AngioJet device rapidly infuses heparinized saline, up to 360 mph, via the catheter endhole, reducing local pressure to a −600 mmHg, extracting soft thrombus into the catheter via a distal sideport .

60

61
BLACK BOX
WARNING BY FDA
CATHETER-MEDIATED THROMBOEMBOLUS ASPIRATION
• The Greenfield embolectomy device : first catheter designed for percutaneous embolectomy .
• No longer commercially available due to its large profile necessitating venous cut down or direct surgical PA access, and challenging steerability, which limited its use.
62

ANGIOVAC DEVICE
• Newer device• Hampered by bulky size requiring 24-Fr introducer sheath
access, difficulty accessing the PA, and requirement of veno-venous bypass .
• For treatment IVC thrombosis in the setting of PE and can result in resolution of significant thrombus burden captured in an extracorporeal filter using veno-venous bypass and cardiac pump.
63

64
Diagram of AngioVac insertion and reinfusion circuit. The cannulahas been inserted into the right internal jugular vein. Blood and thrombus is aspiratedthrough the filter canister, allowing clot capture utilizing a centrifugal pump canister,
prior to return of blood to the patient via the reinfusion cannula placed into the femoralvein.

65
(A) AngioVac cannula. (B) Example of thrombus captured in the filter canister. Images from Angiodynamics.

66
PRONTO XL EXTRACTION CATHETER
• Its pigtail shape can be used for thromboembolus extraction from the main PA, and the straight tip version from segmental PAs.
• The pigtail version can also be used like a rotational catheter to manually fragment thrombus, simultaneously suctioning clot via distal sideholes using a 60-mL syringe.
• This device is FDA-approved for peripheral application.
67
FLOW TRIEVER DEVICE
• The FlowTriever catheter is a recently released device that has FDA approval for removal of emboli and thrombi from blood vessels
• It requires a 22-F venous sheath and consists of 3 parts: the Flow Restoration Catheter, which is made up of 3 self-expanding nitinol disks; the Aspiration Guide Catheter; and the Retraction Aspirator Device.
• The FlowTriever device is advanced over the wire and into the thrombus, where the expandable disks are deployed using a pin and pull method.
• The disks and disrupted thrombus are then retracted and removed through the aspiration catheter.
68

69
(A) The flow restoration catheter (FRC) is used to enmesh clots and is pulled through theaspiration guide catheter (AGC) utilizing (B) the retraction aspirator device (RAD).

70

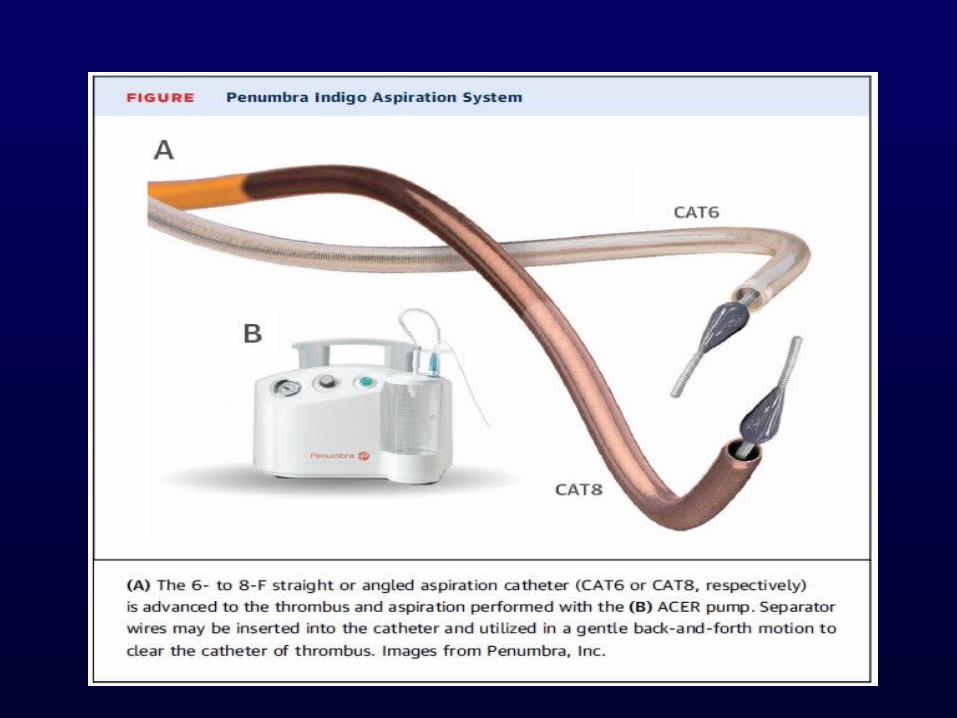
PENUMBRA INDIGO THROMBECTOMY SYSTEM
• The Indigo mechanical thrombectomy system consists of a pump, 6- to 8-F straight or angled catheters, and a Separator device.
• It is approved for thrombus removal in both peripheral arterial and venous systems.
• An advantage is that it only requires an 8-F venous sheath and can be placed into the PA system quickly, in an over-the-wire technique.
71
72
EXTRACORPOREAL MECHANICALOXYGENATION
• Extracorporeal membrane oxygenator (ECMO) placement has been described in case reports of patients with massive PE, as it has the potential to unload the RV and, importantly, provides oxygenation during massive PE to allow for RV recovery .
• The ability of the interventional team to place the ECMO underscores the importance of a multidisciplinary approach.
• In many institutions, PERT members are also ECMO service members.
73Carroll BJ et al Am J Cardiol 2015;116:1624–30.

SURGICAL EMBOLECTOMY
• Surgical therapy is considered a last resort for acute PE and is offered only to patients in extremis.
• Significant advances in cardiac surgical techniques have led to an impressive reduction in operative mortality, which is as low as 6% in the current era.
Yalamanchili K et al . Ann Thorac Surg 2004;77:819–23.• 27 consecutive surgical pulmonary embolectomy patients,
there was no in-hospital mortality and a 10-year actuarial survival rate of 93%; both late mortalities were unrelated to PE or related therapy.
Lattouf O et al.World J Cardiovasc Surg 2013;3:190–7.
74

VENA CAVA FILTER
• Placement of an inferior vena cava (IVC) filter is indicated in patients with acute PE who have absolute contraindications to anticoagulation or in patients who have recurrent PE, despite adequate anticoagulation.
• The position of the filter below or above the renal veins depends on the absence or presence of renal vein thrombus, respectively.
• Retrievable filters are preferable because they are associated with lower complication rates.
Weinberg I et al. J Am Coll Cardiol Intv 2013;6:539–47.75
76
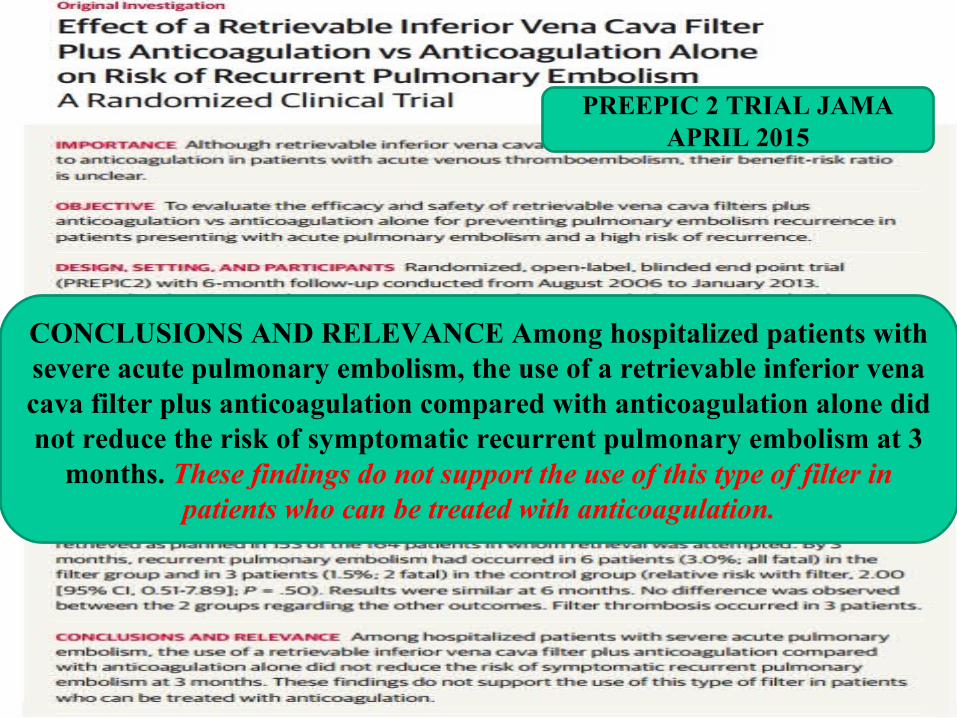
CONCLUSIONS AND RELEVANCE Among hospitalized patients with severe acute pulmonary embolism, the use of a retrievable inferior vena cava filter plus anticoagulation compared with anticoagulation alone did not reduce the risk of symptomatic recurrent pulmonary embolism at 3
months. These findings do not support the use of this type of filter in patients who can be treated with anticoagulation.
PREEPIC 2 TRIAL JAMAAPRIL 2015
• Both the American and the European guidelines do not recommend routine use of IVC filters in patients with PE.
• However, 3 large analyses, including a U.S. nationwide hospital sample and a study from Japan , suggest that IVC filters may result in better outcomes in patients with massive or intermediate high– risk PE.
Stein PD et al Am J Med 2012;125:478–84.
Isogai T et alAm J Med 2015;128:312.e23–31.
77

POST-INTERVENTION
• Maintenance of anticoagulation post-intervention is critical to prevent recurrent clot formation.
• Also they are at risk of access site bleeding.• Bleeding risk can be reduced by holding the heparin drip
for 1 to 2 h after sheath removal, then restart without a bolus.
• Warfarin is administered on the night of the procedure, and parenteral anticoagulation and warfarin are overlapped until the international normalized ratio is 2 to 3 for at least 24 h.
American College of Chest Physicians evidence based clinical practice guidelines. Chest 2012;141: e419S–94S.
78

• Novel oral anticoagulants, including rivaroxaban, dabigatran, apixaban, and edoxaban, can be used.
• If an alternative anticoagulant agent is utilized, heparin alone for the first 24 to 48 h post-intervention and then discontinuation of the heparin at the time of the first alternative anticoagulant agent dosing.
• This strategy does not include dabigatran or edoxaban usage, which require at least 5 days of parenteral therapy before initiation.
79
KEY STUDIES REGARDING TREATMENT OF PE WITH SYSTEMIC THROMBOLYSIS,
CATHETER-DIRECTED THERAPY AND IVC FILTER PLACEMENT - SUMMARY
80

81
82

83
APRIL 2015
84
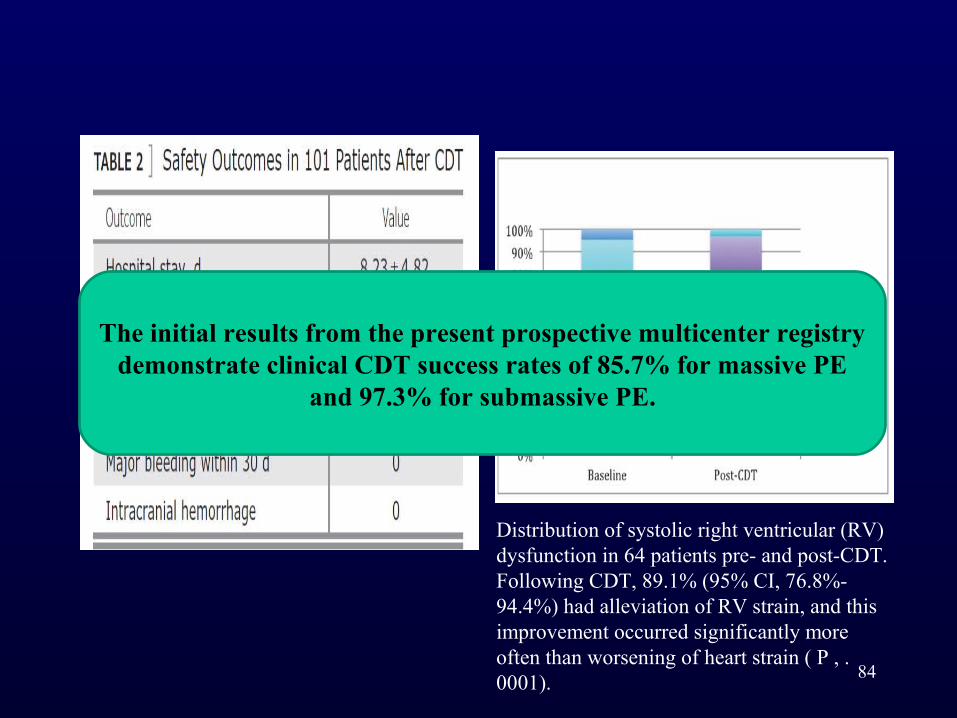
Distribution of systolic right ventricular (RV) dysfunction in 64 patients pre- and post-CDT. Following CDT, 89.1% (95% CI, 76.8%-94.4%) had alleviation of RV strain, and this improvement occurred significantly more often than worsening of heart strain ( P , .0001).
The initial results from the present prospective multicenter registry demonstrate clinical CDT success rates of 85.7% for massive PE
and 97.3% for submassive PE.
85
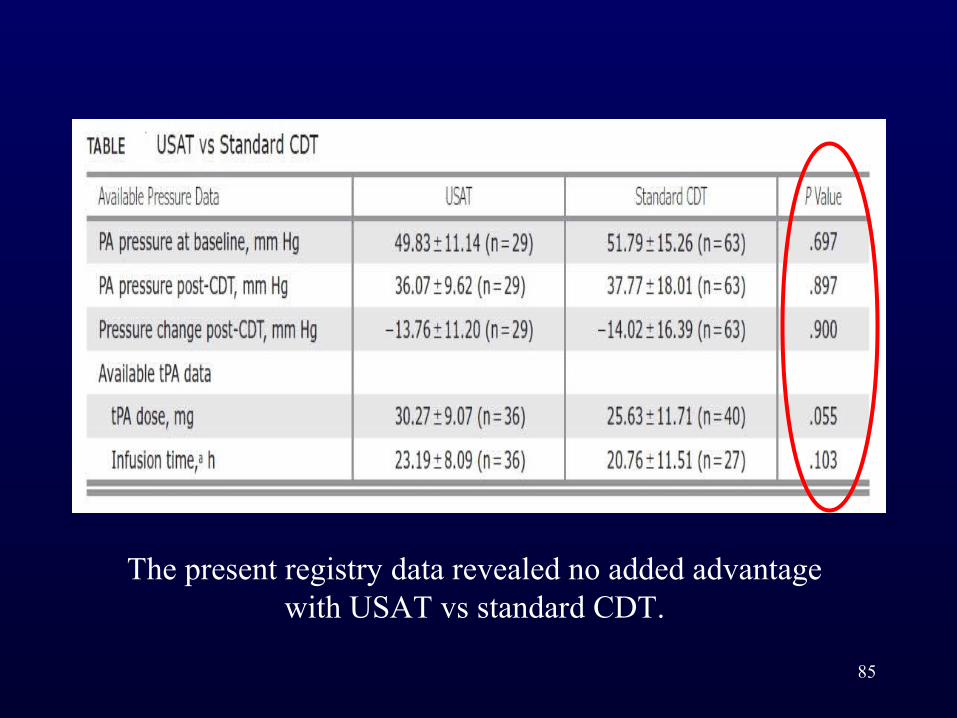
The present registry data revealed no added advantage with USAT vs standard CDT.

86Chest 2015;148(3):667 - 673
CONCLUSIONS: CDT improves clinical outcomes in patients with acute PE while minimizing the risk of
major bleeding. At experienced centers, CDT is a safe and effective treatment of both acute massive and
submassive PE.

CONCLUSIONS
• CDF with use of the EKOS catheter is the only FDA-approved catheter-based therapy for use in treatment of acute PE.
• Other catheter-based therapies focus on direct thrombus removal without use of fibrinolytic agents and may be an option for patients who either cannot receive fibrinolysis or cannot wait for CDF to take effect.
87
• Surgical embolectomy reasonable to reserve it for patients with massive PE and shock, who have contraindications to fibrinolysis, who have failed other treatments, or who have concomitant intracardiac thrombus or paradoxical embolus.
• Similar to a “Code Stroke” or “Code STEMI,” PE should be considered as a “lung attack,” and appropriate resources utilized.
88










