CATHETER ABLATION REIMBURSEMENT GUIDE - …€¦ · · 2018-02-16Medicare Severity Diagnosis...
8
Updated January 1, 2016 CATHETER ABLATION REIMBURSEMENT GUIDE
Transcript of CATHETER ABLATION REIMBURSEMENT GUIDE - …€¦ · · 2018-02-16Medicare Severity Diagnosis...
Updated January 1, 2016
CATHETER ABLATION REIMBURSEMENT GUIDE

January 1, 20162 of 7
TABLE OF CONTENTSAblation Catheters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3CryoAblation Catheters ¡ Arctic Front™ Cardiac CryoAblation Catheter, Arctic Front Advance™ Cardiac CryoAblation Catheter,
Arctic Front Advance™ ST Cardiac CryoAblation Catheter, Freezor™ Cardiac CryoAblation Catheter, Freezor™ MAX Cardiac CryoAblation Catheter
Conventional Radiofrequency (RF) Ablation Catheters ¡ Marinr™ Conventional Radiofrequency (RF) Ablation Catheter, RF Conductr™ MC Conventional
Radiofrequency (RF) Ablation Catheter, and RF Contactr™ Conventional Radiofrequency (RF) Ablation Catheter, Enhancr™ Conventional Radiofrequency (RF) Ablation Catheter
Coverage for Catheter Ablation Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4MedicareOther Payers
Physician Services Coding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Catheter AblationDiagnostic Electrophysiologic Study (EPS)
Inpatient Hospital Coding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5ICD-9-CM1 crosswalk to ICD-10-PCS2 Procedure CodesMedicare Severity Diagnosis Related Group (MS-DRG) Assignments
Outpatient Hospital Coding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Comprehensive Ambulatory Payment Classification (C-APCs):Medicare Hospital Outpatient Catheter Ablation C-Code Listing
Diagnosis Codes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7ICD-9-CM crosswalk to ICD-10-CM3 Diagnosis Codes
For questions or for more information, please contact Medtronic at 1 (866) 877-4102.
The coding suggestions and coding guidelines in this guide do not replace seeking coding advice from the payer and/or your own coding staff. The ultimate responsibility for correct coding lies with the provider of services. Please contact your local payer for interpretation of the appropriate codes to use for specific procedures. Medtronic makes no guarantee that the use of this information will prevent differences of opinion or disputes with Medicare or other third-party payers as to the correct form of billing or the amount that will be paid to providers of service.
Where reimbursement is requested for the use of a product that may be inconsistent or not expressly specified in the FDA cleared or approved labeling (e.g., instructions for use, operator’s manual, or package insert), consult with your billing advisors or payers for advice on handling such billing issues. Some payers may have policies that make it inappropriate to submit claims for such items or related services.

January 1, 2016
ABLATION CATHETERSArctic Front™, Arctic Front Advance™, and Arctic Front Advance™ ST Cardiac CryoAblation Catheters
Catheter IndicationArctic Front™, Arctic Front Advance™, and Arctic Front Advance™ ST Cardiac CryoAblation Catheters
Treatment of drug refractory recurrent symptomatic Paroxysmal Atrial Fibrillation (PAF)
The Arctic Front™, Arctic Front Advance™, and Arctic Front Advance™ ST Cardiac CryoAblation catheters deliver refrigerant (via the CryoConsole) through an inflatable balloon to remove heat from tissue, freezing and disabling unwanted electrical circuits in the pulmonary veins that may contribute to PAF. The Cryoballoon’s shape achieves contact over a broad area to create the barriers that prevent these electrical currents from entering the heart’s atria. The FlexCath™ and the FlexCath Advance™ Steerable Sheaths position the Arctic Front™, Arctic Front Advance™, and Arctic Front Advance™ ST Cardiac Cryoballoon in the heart.
Freezor™ Cardiac CryoAblation Catheters
Catheter Indication and UseFreezor™ Cardiac CryoAblation Catheter
Treatment of Atrioventricular Nodal Re-entry Tachycardia (AVNRT).
Freezor™ MAX Cardiac CryoAblation Catheter
Treatment of PAF. Used in conjunction with the Arctic Front Advance™ Cryoballoon to:¡ Provide touch-up cryoablation and complete the Pulmonary Vein Isolation (PVI)
process as needed¡ Cryoablate focal trigger sites¡ Create the ablation line between the inferior vena cava and the tricuspid valve
The Freezor™ and Freezor™ MAX Cardiac CryoAblation Catheters are deflectable, single-use, electrophysiology catheters designed to ablate cardiac tissue using cryothermal energy. Refrigerant is directed via the CryoConsole through these devices, creating precise, focal lesions.
Conventional Radiofrequency (RF) Ablation Catheters
Catheter IndicationRF Marinr™ MC Multi-Curve Steerable Ablation Catheter RF catheters are indicated for use with the Medtronic RF
generator to deliver RF energy for intracardiac ablation of accessory atrioventricular (AV) conduction pathways associated with tachycardia for the treatment of AV nodal re-entrant tachycardia (AVNRT) and for creation of complete AV block in patients with a difficult to control ventricular response to an atrial arrhythmia.
RF Marinr™ SC Single-Curve Steerable Ablation Catheter
RF Conductr™ MC Multi-Curve Bidirectional Ablation Catheter
RF Contactr™ Dual-Curve Ablation Catheter
RF Enhancr™ II Single-Curve Ablation Catheter
Conventional RF Ablation Catheters are used in conjunction with a Medtronic RF power generator to produce therapeutic, heat-based energy at a targeted area of cardiac tissue. RF energy, delivered via the catheter, destroys tissue integral to the onset and maintenance of most atrial tachyarrhythmias.
3 of 7
January 1, 2016
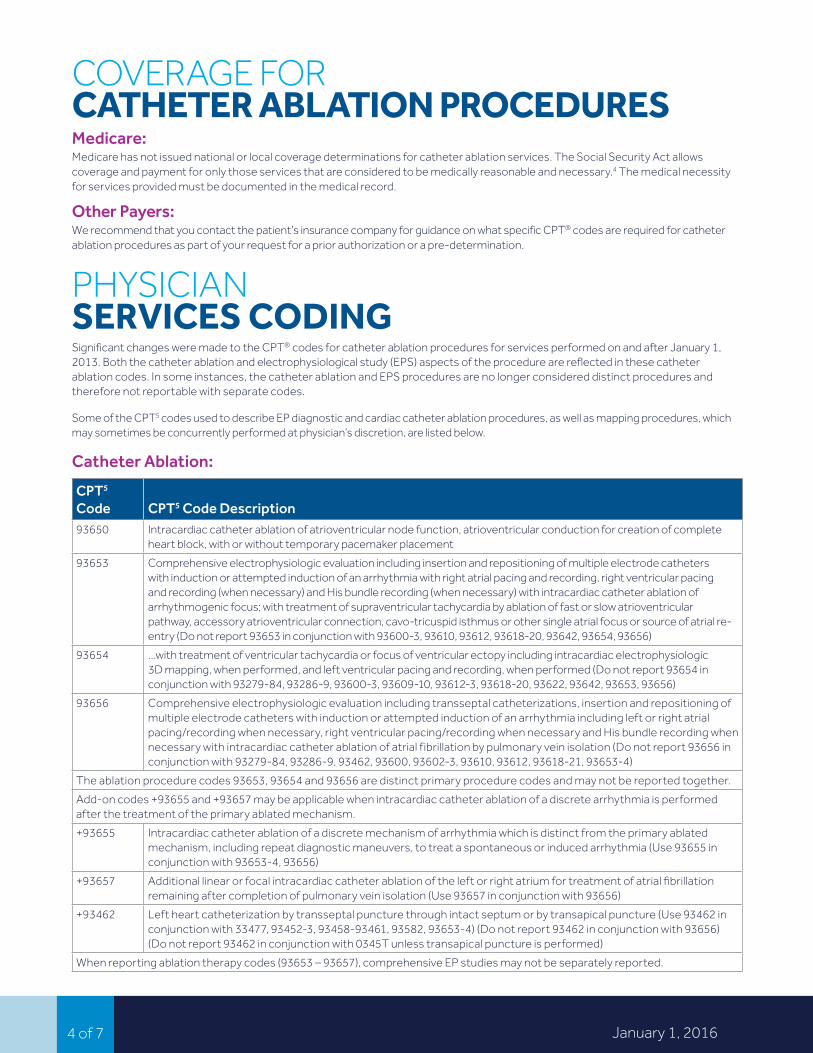
COVERAGE FOR CATHETER ABLATION PROCEDURES Medicare:Medicare has not issued national or local coverage determinations for catheter ablation services. The Social Security Act allows coverage and payment for only those services that are considered to be medically reasonable and necessary.4 The medical necessity for services provided must be documented in the medical record.
Other Payers:We recommend that you contact the patient’s insurance company for guidance on what specific CPT® codes are required for catheter ablation procedures as part of your request for a prior authorization or a pre-determination.
PHYSICIAN SERVICES CODINGSignificant changes were made to the CPT® codes for catheter ablation procedures for services performed on and after January 1, 2013. Both the catheter ablation and electrophysiological study (EPS) aspects of the procedure are reflected in these catheter ablation codes. In some instances, the catheter ablation and EPS procedures are no longer considered distinct procedures and therefore not reportable with separate codes.
Some of the CPT5 codes used to describe EP diagnostic and cardiac catheter ablation procedures, as well as mapping procedures, which may sometimes be concurrently performed at physician’s discretion, are listed below.
Catheter Ablation:
CPT5 Code CPT5 Code Description93650 Intracardiac catheter ablation of atrioventricular node function, atrioventricular conduction for creation of complete
heart block, with or without temporary pacemaker placement
93653 Comprehensive electrophysiologic evaluation including insertion and repositioning of multiple electrode catheters with induction or attempted induction of an arrhythmia with right atrial pacing and recording, right ventricular pacing and recording (when necessary) and His bundle recording (when necessary) with intracardiac catheter ablation of arrhythmogenic focus; with treatment of supraventricular tachycardia by ablation of fast or slow atrioventricular pathway, accessory atrioventricular connection, cavo-tricuspid isthmus or other single atrial focus or source of atrial re-entry (Do not report 93653 in conjunction with 93600-3, 93610, 93612, 93618-20, 93642, 93654, 93656)
93654 …with treatment of ventricular tachycardia or focus of ventricular ectopy including intracardiac electrophysiologic 3D mapping, when performed, and left ventricular pacing and recording, when performed (Do not report 93654 in conjunction with 93279-84, 93286-9, 93600-3, 93609-10, 93612-3, 93618-20, 93622, 93642, 93653, 93656)
93656 Comprehensive electrophysiologic evaluation including transseptal catheterizations, insertion and repositioning of multiple electrode catheters with induction or attempted induction of an arrhythmia including left or right atrial pacing/recording when necessary, right ventricular pacing/recording when necessary and His bundle recording when necessary with intracardiac catheter ablation of atrial fibrillation by pulmonary vein isolation (Do not report 93656 in conjunction with 93279-84, 93286-9, 93462, 93600, 93602-3, 93610, 93612, 93618-21, 93653-4)
The ablation procedure codes 93653, 93654 and 93656 are distinct primary procedure codes and may not be reported together.
Add-on codes +93655 and +93657 may be applicable when intracardiac catheter ablation of a discrete arrhythmia is performed after the treatment of the primary ablated mechanism.
+93655 Intracardiac catheter ablation of a discrete mechanism of arrhythmia which is distinct from the primary ablated mechanism, including repeat diagnostic maneuvers, to treat a spontaneous or induced arrhythmia (Use 93655 in conjunction with 93653-4, 93656)
+93657 Additional linear or focal intracardiac catheter ablation of the left or right atrium for treatment of atrial fibrillation remaining after completion of pulmonary vein isolation (Use 93657 in conjunction with 93656)
+93462 Left heart catheterization by transseptal puncture through intact septum or by transapical puncture (Use 93462 in conjunction with 33477, 93452-3, 93458-93461, 93582, 93653-4) (Do not report 93462 in conjunction with 93656) (Do not report 93462 in conjunction with 0345T unless transapical puncture is performed)
When reporting ablation therapy codes (93653 – 93657), comprehensive EP studies may not be separately reported.
4 of 7

January 1, 2016
Diagnostic Electrophysiologic Study (EPS):Coding information to be used when a physician performs a diagnostic Electrophysiologic Study (EPS) prior to a catheter ablation.
CPT5 Code CPT5 Code Description93619 Comprehensive electrophysiologic evaluation with right atrial pacing and recording, right ventricular pacing and
recording, His bundle recording, including insertion and repositioning of multiple electrode catheters, without induction or attempted induction of arrhythmia (Do not report 93619 in conjunction with 93600, 93602-3, 93610, 93612, 93618, 93620-2, 93653-7)
93620 Comprehensive electrophysiologic evaluation including insertion and repositioning of multiple electrode catheters with induction or attempted induction of arrhythmia; with right atrial pacing and recording, right ventricular pacing and recording, His bundle recording (Do not report 93620 in conjunction with 93600, 93602-3, 93610, 93612, 93618-9, 93653-7)
+93621 …with left atrial pacing and recording from coronary sinus or left atrium (Use 93621 in conjunction with 93620, 93653-4) (Do not report 93621 in conjunction with 93656)
+93622 …with left ventricular pacing and recording (Use 93622 in conjunction with 93620, 93653, 93656) (Do not report 93622 in conjunction with 93654)
+93623 Programmed stimulation and pacing after intravenous drug infusion (Use 93623 in conjunction with 93610, 93612, 93619-20, 93653-4, 93656)
+93662 Intracardiac echocardiography during therapeutic/diagnostic intervention, including imaging supervision and interpretation (Use 93662 in conjunction with 92987, 93453, 93460-2, 93532, 93580-1, 93620-2, 93653-4, 93656 as appropriate) (Do not report 92961 in addition to 93662)
93624 Electrophysiologic follow-up study with pacing and recording to test effectiveness of therapy, including induction or attempted induction of arrhythmia
Mapping is considered a distinct procedure performed in addition to a diagnostic EP study or ablation procedure
+93609 Intraventricular and/or intra-atrial mapping of tachycardia site(s) with catheter manipulation to record from multiple sites to identify origin of tachycardia (Use 93609 in conjunction with 93620, 93653, 93656) (Do not report 93609 in conjunction with 93613, 93654)
+93613 Intracardiac electrophysiologic 3-dimensional mapping (Use 93613 in conjunction with 93620, 93653, 93656) (Do not report 93613 in conjunction with 93609, 93654)
5 of 7
INPATIENT HOSPITAL CODINGICD-9-CM1 crosswalk to ICD-10-PCS2 Procedure Codes for discharges after September 30, 2015Please note that there is not always a direct crosswalk from ICD-9-CM to ICD-10-PCS. It is up to the provider to select the appropriate code(s) to represent the procedure(s) performed.
The following list is not all-inclusive.
ICD-9-CM1 Procedure Code
ICD-9-CM1
Procedure Code DescriptionICD-10-PCS2 Procedure Code
ICD-10-PCS2 Procedure Code Description
37.26 Catheter based invasive electrophysiologic testing
4A023FZ Measurement of Cardiac Rhythm, Percutaneous Approach
37.27 Cardiac mapping 02K83ZZ Map Conduction Mechanism, Percutaneous Approach
37.34 Excision or destruction of other lesion or tissue of heart, endovascular approach
02583ZZ* Destruction of Conduction Mechanism, Percutaneous Approach
*AHA Coding Clinic for ICD-10-CM and ICD-10-PCS, Volume 1 Number 4, Fourth Quarter 2014.
POSSIBLE DRG ASSIGNMENTS (MS-DRG: MEDICARE SEVERITY DIAGNOSIS RELATED GROUP)MS-DRG Brief MS-DRG Description273 Percutaneous intracardiac procedures w/MCC
274 Percutaneous intracardiac procedures w/o MCC
MCC: Major complication or comorbidity

January 1, 2016
OUTPATIENT HOSPITAL CODINGComprehensive Ambulatory Payment Classifications (C-APCs):
CPT4 Code Brief Description C-APC C-APC Description93619 Electrophysiology eval w/o arrhythmia
5212 Level 2 Electrophysiologic Procedures93620 Electrophysiology eval w/arrhythmia
93624 EP follow-up study
93650 AV node ablation
93653 SVT ablation and EP eval
5213 Level 3 Electrophysiologic Procedures93654 VT ablation and EP eval
93656 Ablation of AF by PVI with transseptal and EP evaluation
The following codes are not assigned to an APC as they are ancillary to the primary procedures. Medicare classifies the following codes with an “N” Status Indicator and does not separately reimburse hospitals for these procedures. Hospitals should report all applicable codes, including those for packaged services, according to correct coding principles.
+93462 Transseptal puncture (Use 93462 in conjunction with 33477, 93452-3, 93458-61, 93461, 93582-4) (Do not report 93642 in conjunction with 93656) (Do not report 93462 in conjunction with 0345T unless transapical puncture is performed)
+93609 Intraventricular and/or intra-atrial mapping (Use 93609 in conjunction with 93620, 93653, 93656) (Do not report 93609 in conjunction with 93613, 93654)
+93613 Intracardiac 3-dimensional mapping (Use 93613 in conjunction with 93620, 93653, 93656) (Do not report 93613 in conjunction with 93609, 93654)
+93621 Comprehensive EP evaluation; with left atrial pacing and recording from coronary sinus or left atrium (Use 93621 in conjunction with 93620, 93653-4) (Do not report 93621 in conjunction with 93656)
+93622 Comprehensive EP evaluation; with left ventricular pacing and recording (Use 93622 in conjunction with 93620, 93653, 93656) (Do not report 93622 in conjunction with 93654)
+93623 Programmed stimulation and pacing after intravenous drug infusion (Use 93623 in conjunction with 93610, 93612, 93619-20, 93653-4, 93656)
+93655 Additional ablation of discrete arrhythmia, SVT or VT (Use 93655 in conjunction with 93653-4, 93656)
+93657 Additional linear focal lesion for AF (Use 93657 in conjunction with 93656)
+93662 Intracardiac echocardiography (Use 93662 in conjunction with 92987, 93453, 93460-2, 93532, 93580-1, 93620-2, 93653-4, 93656 as appropriate) (Do not report 92961 in addition to 93662)
6 of 7
Medicare Hospital Outpatient Catheter Ablation C-Code ListingFor CY 2016, Medicare requires that only a single appropriate device code is submitted on the claim for the procedure.
C1733 – Catheter, Electrophysiology, Diagnostic/Ablation, Other than 3D or Vector Mapping, Other than Cool Tip
Device Model Number
RF Contactr™ 70256034, 70257533
RF Conductr™ MC 0786022, 0786042, 0787533, 0787544, 07857544, 07856042, 07856044, 0786044
RF Marinr™ MC 075302, 075312, 075402, 075405
5F RF Marinr™ 076514, 076515, 076583, 076584, 076585, 076586
RF Enhancr™ II 31744523, 31745523, 31745533, 39745533, 39746534
Freezor™ Cardiac CryoAblation Catheter 307F1, 307F3, 307F5
Freezor™ MAX Cardiac CryoAblation Catheter 239F3, 239F5
Arctic Front™ Cardiac CryoAblation Catheter 2AF232, 2AF282
Arctic Front Advance™ Cardiac CryoAblation Catheter 2AF234, 2AF284
Arctic Front Advance™ ST Cardiac CryoAblation Catheter 2AFAST23, 2AFAST28

January 1, 2016
C1766 – Introducer/Sheath, Guiding, Intracardiac Electrophysiological, Steerable, Other than Peel-Away
Device Model Number
FlexCath™ Steerable Sheath 3FC10, 3FC12
FlexCath Advance™ Steerable Sheath 4FC12
C1730 – Catheter, Electrophysiology, Diagnostic, Other than 3D Mapping (19 or Fewer Electrodes)
Device Model NumberTorqr™ CS Diagnostic Catheter 041565CS, 041590CS, 041865CS
Torqr,™ Soloist™ Diagnostic Catheter 041002JM, 041002UM, 041005DM, 041005JM, 041005UM, 04120DS, 04122JM, 04122UM, 04125JM, 04125UM, 441016JF, 441016U, 44216J, 44216JF, 44216U, 44516J, 44516JF, 44516U
Marinr™ CS 043302M, 043325M, 043328M
Marinr™ 072302, 072322M, 072402
Achieve™ Mapping Catheter 990063-015, 990063-020
C1731 – Catheter, Electrophysiology, Diagnostic, Other than 3D Mapping (20 or More Electrodes)
Device Model Number
StableMapr™ 04401SM, 04402SM
DIAGNOSIS CODESICD-9-CM1 crosswalk to ICD-10-CM3 Diagnosis Codes for discharges after September 30, 2015Please note that there is not always a direct crosswalk from ICD-9-CM1 to ICD-10-CM.3 It is up to the provider to select the most appropriate diagnosis code(s).
The following list is for illustrative purposes only and is not all-inclusive.
ICD-9-CM1 Diagnosis Code
ICD-9-CM1
Diagnosis Code Description
ICD-10-CM3 Diagnosis Code ICD-10-CM3 Diagnosis Code Description
427.31 Atrial fibrillation I48.0 Paroxysmal atrial fibrillation
427.32 Atrial flutter I48.3 Typical atrial flutter (type I)
I48.4 Atypical atrial flutter (type II)
I48.92 Unspecified atrial flutter
427.0 Paroxysmal supraventricular tachycardia
I47.1 Supraventricular tachycardia (includes AVNRT)
7 of 7

medtronic .com
UC201406308b EN © Medtronic 2016. Minneapolis, MN. All Rights Reserved. Printed in USA 01/2016
Medtronic710 Medtronic Parkway Minneapolis, MN 55432-5604 USA Tel: (763) 514-4000 Fax: (763) 514-4879
Toll-free: 1 (800) 328-2518(24-hour technical support for physicians and medical professionals)
References1 International Classification of Diseases, Ninth Revision of Clinical
Modification. http://www.cdc.gov/nchs/icd/icd9cm.htm. 2 International Classification of Diseases, Tenth Revision, Procedure
Coding System. https://www.cms.gov/Medicare/Coding/ICD10/2016-ICD-10-PCS-and-GEMs.html.
3 International Classification of Diseases, Tenth Revision, Clinical Modification. http://www.cdc.gov/nchs/icd/icd10cm.htm.
4 Social Security Act Section 1862 42 U.S.C. 1395y(a)(1)(A), is available at http://www.ssa.gov/OP_Home/ssact/title18/1862.htm.
5 Current Procedural Terminology (CPT) is copyright 2015 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative causes or related listings are included in CPT. The AMA assumes no liability for the data contained herein. Applicable FARS/DFARS Restrictions Apply to Government Use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for the data contained or not contained herein.
Brief Statement (for Arctic Front Advance™ Cardiac CryoAblation Catheter, CryoConsole and Freezor™ MAX Cardiac CryoAblation Catheter)
IndicationsMedtronic CryoCath™ CryoAblation system is comprised of cryoablation catheters and a CryoConsole. The Arctic Front Advance ST Cardiac CryoAblation Catheter system is indicated for the treatment of drug refractory recurrent symptomatic paroxysmal atrial fibrillation. The Freezor MAX Cardiac CryoAblation Catheter is used as an adjunctive device in the endocardial treatment of paroxysmal atrial fibrillation in conjunction with the Arctic Front Advance Cryoballoon. Please read the specific product labeling indications for use before using the cryoablation system.
ContraindicationsUse of Arctic Front Advance ST Cryoballoon is contraindicated as follows: ¡ in the ventricle because of the danger of catheter entrapment in the
chordae tendinae¡ in patients with active systemic infections¡ in conditions where the manipulation of the catheter within the heart
would be unsafe (e.g.,intracardiac mural thrombus)¡ in patients with cryoglobulinemia¡ in patients with one or more pulmonary vein stents
Use of Freezor MAX cryocatheter is contraindicated in patients with the following conditions:¡ active systemic infections¡ cryoglobulinemia¡ other conditions where the manipulation of the catheter would be
unsafe (e.g., intracardiac mural thrombus)
Warnings and PrecautionsDo not resterilize the cryoablation catheters for purpose of reuse. Use only the appropriate size of the FlexCath™ Steerable Sheath family with the Arctic Front Advance cryoablation catheters because using another sheath may damage the catheter or balloon segment. Do not inflate the balloon inside the sheath. Always verify with fluoroscopy or by using the proximal shaft visual marker that the balloon is fully outside the sheath before inflation to avoid catheter damage. Do not position the balloon within the tubular portion of the pulmonary vein to minimize phrenic nerve injury and pulmonary vein stenosis. Do not connect the cryoablation catheter to a radiofrequency (RF) generator or use it to deliver RF energy because this may cause catheter malfunction or patient harm. The catheter contains pressurized refrigerant during operation; release of this gas into the circulatory system due to equipment failure or misuse could result in gas embolism, which can occlude vessels and lead to tissue infarction with serious consequences. Always advance and withdraw components slowly to minimize the vacuum created and therefore minimize the risk
of air embolism. Do not pull on the catheter, sheath, umbilical cables, or console while the catheter is frozen to the tissue, as this may lead to tissue injury. Do not advance the balloon beyond the guide wire to reduce risk of tissue damage. Do not pass the catheter through a prosthetic heart valve (mechanical or tissue) to avoid damage to the valve, valvular insufficiency, or premature failure of the prosthetic valve. Always inflate the balloon in the atrium then position it at the pulmonary vein ostium to avoid vascular injury. Do not ablate in the tubular portion of the pulmonary vein. Monitor the status of the phrenic nerve continuously during right-sided pulmonary vein applications using an appropriate monitoring technique. Stop ablation immediately if phrenic nerve impairment is observed. Consider appropriate medical strategies to minimize the risk of damage to the lung or tracheobronchial tree and the risk of esophogeal injury. Use appropriate levels of contrast media in patients with comorbidities. Follow contrast labeling and institutional procedures regarding the appropriate medical strategies to minimize risk when using contrast media.
The CryoAblation (Arctic Front Advance and Freezor MAX) family of catheters were not studied for safety of changes in anticoagulation therapy in patients with atrial fibrillation. This equipment should be used only by or under the supervision of physicians trained in left-atrial cryoablation procedures. Cryoablation procedures should be performed only in a fully equipped facility.
Potential ComplicationsPotential complications/adverse events that may be associated with cardiac catheterization and ablation listed alphabetically below include but are not limited to: anemia; anxiety; atrial flutter; back pain; bleeding from puncture sites; blurred vision; bradycardia; bronchial constriction, bronchitis; bruising; cardiac tamponade; cardiopulmonary arrest; cerebral vascular accident; chest discomfort/pain/pressure; cold feeling; cough; death; diarrhea; dizziness; esophageal damage (including esophageal fistula); fatigue; fever; gastroparesis; headache; hemoptysis; hypotension/hypertension; lightheadedness; myocardial infarction; nausea/vomiting; nerve injury; pericardial effusion; pulmonary vein stenosis; shivering; shortness of breath; sore throat; tachycardia; transient ischemic attack; urinary infection; vasovagal reaction; visual changes.
Refer to the device technical manual for detailed information regarding the procedure, indications, contraindications, warnings, precautions, and potential complications/adverse events. For further information, please call Medtronic at 1 (800) 328-2518 and/or consult Medtronic’s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.