CASUISTIC INTRODUCTION IN OPHTALMIC PATHOLOGY FOR...
27
CASUISTIC INTRODUCTION IN OPHTALMIC PATHOLOGY FOR TRAINEES AND GENERAL PATHOLOGISTS Case 7 Maria-Rosa Bella Cueto Hospital Universitari Parc Taulí Sabadell (Barcelona). Spain. I declare no conflict of interests
Transcript of CASUISTIC INTRODUCTION IN OPHTALMIC PATHOLOGY FOR...

CASUISTIC INTRODUCTION IN OPHTALMIC PATHOLOGY FOR TRAINEES AND GENERAL PATHOLOGISTS
Case 7
Maria-Rosa Bella Cueto
Hospital Universitari Parc Taulí
Sabadell (Barcelona). Spain.
I declare no conflict of interests

CLINICAL INFORMATION
• Man 83 years old
• Lesion in the lateral free margin of the upper left eyelid, of 5 mm, since one year ago, suggestive of basocellular carcinoma
• Rapid grow in the last two months, reaching 30 x 20 mm.








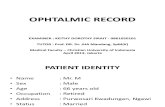
CK20
CAM5.2

SPT
CROM ENE
TTF-1

NF
IMMUNOHISTOCHEMISTRY
Positive:
- CAM 5.2
- AE1/AE3
- CK20
- 34βe12
- BerEP4
- EMA
- Chromogranin
- Synaptophysin
- CD56
- Enolase
- Neurofilaments
Sometimes positive:
- CK7
Negative:
- TTF-1

Ki67 45%

DIAGNOSIS:
- MERKEL CELL CARCINOMA
- 30 mm (post-fixation: 23 mm)
- No lymphatic , venous or perineural invasion
- Free margins (2 mm)
- pT2 pNX

FOLLOW-UP
• Radiotherapy 45 Gy• Radiodermitis g.1• 12 months later: “in transit” metastasis: nodular lesion (2,2 cm.) affecting
dermis and subcutaneous tissue in temporal anterior region. Resection with free margins.
• Now free of disease, five years after the first surgery.

• Primary cutaneous neuroendocrine carcinoma
• Toker 1972: Trabecular carcinoma of the skin
• Cell of origin? Merkel cell
– Some kind of cutaneous stem cell
• Composite cases (squamous cell carcinoma, basocellular carcinoma, skin appendages carcinoma)
• Incidence: ≈ 1/100.000 persons/year
MERKEL CELL CARCINOMA

CLINICAL FEATURES - AEIOU
• Asymptomatic• Expanding rapidly• Immune suppression• Older than 50 years• Ultraviolet exposed site
– Periorbitary region: 5-20%– Eyelid: 2,5 -10%
upper>lower
• Spontaneous regression– after incisional biopsy or FNAB
• Presentation in lymph node without known primary➢Spontaneous regression?➢Origin in lymph node?
Clinical differential diagnosis: skin tumours, chalazion, dermoid cyst

PATHOPHYSIOLOGY
• Merkel cell polyomavirus (MCPyV)
– Integrated to the genoma
– Large T and small T antigens
• Interfere with P53 and RB1 function
– IHC CM2B4 (Large T antigen)
– Few somatic mutations
– (Better prognosis)?
• UV radiation related
– High number of mutations associated to UV damage
– Epidermotropism
– Mutations in TP53 and RB1 genes
– Composite tumours or divergent differentiation
– (Poorer prognosis?)
– Larger cells


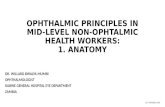
DIFFERENTIAL DIAGNOSIS
• Blue small cell morphology
– Basal cell carcinoma
– Melanoma
– Sebaceous carcinoma
– Lymphoma
– PNET/Ewing sarcoma
– ….
– Metastasis of lung small cell carcinoma
– Exceptional cases: MCC TTF-1+ or CK20-, LSCC CK20+
Neuroendocrine markersDot pattern (CK20, neurofilaments)
Specific tumour markersGlycogen, EWS/FLI-1
TTF-1
CM2B4

Basal cell carcinoma

• Merkel cell carcinoma has its own staging system
• Eyelid carcinoma staging excludes Merkel cell carcinoma
pT Merkel cell carcinoma
• pTis: In situ primary tumor
• pT1 : ≤ 2 cm
• pT2: > 2 cm ≤ 5 cm
• pT3: > 5 cm
• pT4: Primary tumour invades fascia, muscle, cartilage or bone
Better consider clinical or fresh size
pN Merkel cell carcinoma
• pNX: cannot be assessed (previously removed for other causes or not removed
• pN0: no lymph node metastasis
• pT1: metastasis in lymph regional nodes– pN1a(sn): clinically occult, identified only by sentinel node biopsy
– pN1a: clinically occult in lymph node dissection
– pN1b: clinically or radiologically detected, microscopically confirmed
• pN2: In transit metastasis without lymph node metastasis
• pN3: In transit metastasis with lymph node metastasis
STAGING AJCC/UICC 8TH ED.

STAGING AJCC/UICC 8TH ED.
pM Merkel cell carcinoma
• pM0: No distant metastasis detected on clinical or radiological exams
• pM1: Distant metastasis microscopically confirmed– pM1a: to distant skin, distant subcutaneous tissue, or distant lymph(s) node(s
– pM1b: to lung
– pM1c: other distant sites
In transit metastasis:
Metastasis discontinuous from primary tumour,
located between the primary tumour and the draining
regional nodes, or distal to the primary tumour
Prognostic stage groups
• From 0 to IV
• Changes from 7th to 8th ed.

OTHER PRONOSTIC FACTORS
• Heavy peritumoral lymphocytic infiltrate
• Greater tumour thickness (Breslow)
• Infiltrative tumour growth
• Lymphovascular invasion
• >10 mitotic figures /hpf
• Invasion in subcutaneous tissue
• P63 expression
5 YEAR SURVIVAL:
- N0: 75%
- N1: 60%
- M1: 25%

CLINICAL MANAGEMENT
• Confirm diagnosis (incisional biopsy)• Clinical/radiological N status
➢ N0: Excision of the tumour (5mm margin)+ sentinel lymph node biopsy➢ Positive: Excision of the tumour (5mm margin) + lymphadenectomy
• Pathological N status:➢pN0: Radiotherapy to primary site ± draining lymph nodes chain➢Positive: Clinical/radiological M status
➢M0: Radiotherapy primary site + lymphadenectomy or Radiotherapy to draining lymph nodes chain
➢M1: consider the following alone or multimodal treatment: Radiotherapy, surgery, chemotherapy, immunotherapy
PD-L1 inhibitors as adjuvant or neoadjuvant therapy?

MERKEL CELL CARCINOMA - FINAL REMARKS
• AEIOU
• Usually typical morphology and immunohistochemical pattern
• Two physiopathological pathways
• Spontaneous regression
• Specific TNM - in transit metastasis
• Promising role of immunotherapy