
Case Presentation - Malignant Pleural Effusion Edited
117
• No greater opportunity, responsibility, or obligation can fall to the lot of a human being than to become a physician. In the care of the suffering, [the physician] needs technical skill, scientific knowledge, and human understanding. . . . Tact, sympathy, and understanding are expected of the physician, for the patient is no mere collection of symptoms, signs, disordered functions, damaged organs, and disturbed emotions. [The patient] is human, fearful, and hopeful, seeking relief, help, and reassurance. • –Harrison's Principles of Internal Medicine, 1950
-
Upload
christian-gallardo-md -
Category
Documents
-
view
1.615 -
download
2
description
My Second Case Management Regarding Mesothelioma and Malignant Pleural Effusion
Transcript of Case Presentation - Malignant Pleural Effusion Edited

• No greater opportunity, responsibility, or obligation can fall to the lot of a human being than to become a physician. In the care of the suffering, [the physician] needs technical skill, scientific knowledge, and human understanding. . . . Tact, sympathy, and understanding are expected of the physician, for the patient is no mere collection of symptoms, signs, disordered functions, damaged organs, and disturbed emotions. [The patient] is human, fearful, and hopeful, seeking relief, help, and reassurance.
• –Harrison's Principles of Internal Medicine, 1950

Malignant Pleural Effusion
Christian Gallardo, MD

Objectives
• To discuss a case of Pleural effusion and its approach.
• To discuss the approach to Transudative and Exudative Pleural Effusion using the Light’s Criteria.
• To discuss the Diagnosis and Treatment strategies for Malignant Mesothelioma

General Data
• F.E. • 74/M• Las Pinas• Roman Catholic

Chief Complaint
Difficulty of Breathing

History of Present Illness
2 weeksPTA
•Cough, non productive•No Hemoptysis•No Colds•No Fever•No Chest Pain•No DOB•No Orthopnea, No PND•No Consult done•No Medications taken

History of Present Illness
1 weekPTA
•Still with non productive cough•Chest pain, G4/10•pricking in character, •radiating to the shoulder, < 1 minute, precipitated by breathing
•No Orthopnea, No PND•No Hemoptysis•No swelling of the legs•Consulted •Medications:•Cefixime 200mg BID•Ambroxol 75mg OD

History of Present Illness
Few HoursPTA
•Persistence of increased severity of chest pain and non productive coughing•Difficulty of Breathing•Fever, One episode, Low Grade (38C)•No chills•No colds
CONSULT

Past Medical History• Hypertension Stage II
• Maintained on Losartan 50mg/tab 1 tab OD• Type 2 DM
• Maintained on Metformin 500mg/ tab 1 tab OD• CAD
• Maintained on Clopidogrel 75mg/tab 1 tab OD
Trimetazidine 35mg 1 tab TID
Simvastatin 40mg OD HS• S/P Coronary Angiogram (7/26/2008) - UPHR• S/P PTCA of LAD (7/26/2008) - UPHR• S/P IABP Insertion R Femoral Artery (7/26/2008) -
UPHR• S/P ORIF Right Forearm (1994) - UPHR• S/P Cholecystectomy (1982) - ?

Family Medical History
• (-) Hypertension• (-) DM• (-) Bronchial Asthma• (-) Heart Disease• (-) Thyroid disease• (-) Blood Dyscrasia• (-) Cancer

Personal and Social History
• (-) Non smoker• (-) Alcoholic beverage drinker• Retired Office Employee

Review of Systems
• General: (+) Weight Loss 20% for 2 months• HEENT: (-) blurring of visions, (-) sorethroat • Gastroenterology: (-) abdominal pain, (-) diarrhea, (-)
constipation, (-) melena, (-) hematochazia• GUT: (-) dysuria, (-) oliguria (-)anuria • Endocrinology: (-) polyuria, polydipsia, polyphagia, • Musculoskeletal: (-) myalgia• Hematology: (-)easy brusability• Neurology: (-) neuropathy, (-)seizures

Physical Examination
• General: • conscious, coherent, not in respiratory distress
• Vital Signs: • BP: 110/70mmHg RR:24 cpm• CR: 101 bpm, regular T: 38. 1 C
• Skin: • Good skin turgor, no rashes, no jaundice
• HEENT: • Anicteric sclera, pink palpebral conjunctivae, no
tonsillopharyngeal congestion, no nasoaural discharge, no cervicolymphadenopathy, JVP at 9 cm

Physical Examination
• Chest and Lung: • Symmetrical chest expansion, no lagging, no
retractions, dull at percussion at left base, decreased breath sounds at left base, decreased tactile and vocal fremitus at left base, fine crackles at left base
• Heart: • Adynamic precordium, normal rate, regular rhythm, PMI at
6th ICS at MCL, normal S1 and S2, (-) S3 and S4, no murmurs.
• Abdomen: • Flat, soft, normoactive bowel sounds, non-tender. Liver
span: 8 cm, Intact Traube’s space, No Organomegaly
• Extremities: • Full pulses, no edema, extremities with full range of motion

Neurological Examination• Oriented to time, person and place, (-) dysmetria• (-) dysdiadochokinesia, can do FTNT, (-) nystagmus• Cranial Nerves:
• I: can smell• II: 2-3mm PERTL, Fundoscopy: (+) ROR, Clear
Media, Distinct Cup borders, CDR: 1:3, AVR: 2:3, No exudates, No Hemorrhage
• III, IV, VI: Full EOM• V: (+) bilateral corneal reflex, good masseter tone• VII: (-) facial asymmetry• VIII: can hear• IX, X: (+) gag Reflex• XI: can equally shrug shoulder• XII: no tongue deviation

Neurological Examination
• (-) Babinski (-) Brudzinski• (-) Nuchal Rigidity
++5/5
++5/5 100%
5/55/5
++
++100%
100%
100%
++ ++
++++
5/5 5/5
5/5
5/5100%
100%
100%
100%

Salient Features• Male • 74 years old• Cough, non productive• Chest Pain, pricking in character• Shortness of Breath• Hypertensive and Diabetic• Known with CAD• Non- Smoker• Chest and Lung:
• Symmetrical chest expansion, no lagging, no retractions, dull at percussion at left base, decreased breath sounds at left base, decreased tactile and vocal fremitus at left base, fine crackles at left base

Differential Diagnosis
Dyspnea
Cardiac
Acute Coronary Syndrome
Congestive Heart Failure
Pulmonary
Pleural Effusion
Pneumonia PTB Maligna
ncy
Pulmo Embolism

Admitting Impression
• Pleural Effusion Probably secondary to • Parapneumonic process• PTB • Malignancy
• HCVD, Congestive Heart Failure NYHC I Secondary to CAD
• S/P AMI• S/P PTCA• DM Type 2

Course in the Wards• VS: 110/70 CR: 104 RR: 23 T: 38.1 • Venoclysis • Diagnostics
• Cardiac Enzymes were not Requested• Therapeutics
• 1. Paracetamol + tramadol (Dolcet)• 2. Salbutamol + Ipratropium Br
(Combivent) q 8 hrs.• 3. Ambroxol 75mg 1 tab OD• 4. Paracetamol 500mg 1 tab q 4 hrs
for fever• 5. Paracetamol 300mg 1 ampule Q4
hrs for fever
1st Hospital Day
CBC
Hematocrit 31
Hemoglobin 113
WBC 14.5
Segmenters 86
Lymphocytes 06
Monocytes 07
Eosinophils 01
Platelet Count 373
Chest Xray CardiomagalyAtheromatous AortaPleural Effusion, Left
Left Lateral Decubitus
Presence of Shifting Density Towards the Dependent Portion of the Right Hemithorax, Suggestive of Pleural Fluid
12 lead ECG Sinus TachycardiaLeft Atrial EnlargementComplete Right Bundle Branch BlockAnterior Wall Myocardial Infarction, Old
Serum Sodium 135 mmol/LSerum Potassium 4.5mmol/LSerum BUN 4.5 mmol/LSerum Creatinine 68 umol/LSGPT 49 U/LCBG 112 mg/dL

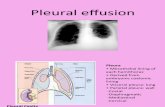
Anatomy of Pleura
• The pleura • Serous membrane that covers the lung
parenchyma, the mediastinum, the diaphragm, and the rib cage.
• Visceral pleura • Covers the lung parenchyma, not only
at its points of contact with the chest wall, diaphragm, and mediastinum but also in the inter-lobar fissures.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Anatomy of Pleura
• Parietal pleura• Lines the inside of the thoracic cavities. • Subdivided
• Costal• Mediastinal• Diaphragmatic
• The visceral and the parietal pleura meet at the lung root.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Anatomy of Pleura
• Pleural fluid• Normally present between the parietal
and the visceral pleura. • Acts as a lubricant and • Allows the visceral pleura covering the
lung to slide along the parietal pleura lining the thoracic cavity during respiratory movements.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Physiology of Pleural Fluid
• It is believed that the fluid that normally enters the pleural space originates in the capillaries in the parietal pleura
• Human beings• Amount of pleural fluid formed daily in a
50-kg individual = approximately 15 mL • The mean lymphatic flow from one
pleural space = 0.40 mL/kg/hour
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Physiology of Pleural Fluid
• Pleural fluid accumulates when the rate of pleural fluid formation exceeds the rate of pleural fluid absorption.
• Normally, there should be a small amount (0.01 mL/kg/hour) of fluid constantly enters the pleural space from the capillaries in the parietal pleura.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Physiology of Pleural Fluid
• Almost all of this fluid is removed by the lymphatics in the parietal pleura, which have a capacity to remove at least 0.20 mL/kg/hour.
• Note that the capacity of the lymphatics to remove fluid exceeds the normal rate of fluid formation by a factor of 20.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

The most common cause of increased pleural fluid formation is increased interstitial fluid in the lung. The amount of edema in the
lung exceeds 5 g/gram of dry lung weight, pleural fluid accumulates, irrespective of
whether the edema is due to high-protein or low-protein fluid
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Radiologic Signs• When more fluid accumulates, it spills over into
the posterior costophrenic angle and obliterates that sinus as viewed in the lateral projection.
• The normally sharp posterior costophrenic angle is obliterated by a shallow, homogeneous shadow whose upper surface is meniscus-shaped.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Course in the Wards• Levofloxacin 750mg 1 tablet OD
• Patient’s Meds:• 1. Essentiale Forte 1 Tab TID• 2. Losartan 50mg 1 tab OD• 3. Clopidogrel 75mg 1 tab OD• 4. Digoxin 0.25 mg 1 tab OD• 5. Metformin 500mg 1 tab OD • 6. Simvastatin 40mg 1 tab OD
HS• 7. Vit B Complex 1 Tab OD• 8. Trimetazidine 35mg 1 tab OD

Course in the Wards• 02 saturation: 97%-98% at 2
lpm via nasal cannula• Sputum AFB for 3 collection• Sputum GS/CS
Sputum AFB x 3 Collection Negative for Acid Fast Bacilli
Sputum GS/CS Gram Stain: Pus Cells: < 25/OIFEpithelial: < 25/OIFGram Positive cocci single and PairGram Negative Short Rods: Few

Couse in the Wards
• Levodropropizine (Levopront) 1 tsp TID PO
• Chest UTZ with Mapping
2nd Hospital Day
Chest Mapping Ultrasound Free fluid in both pleural cavities, more in the left. Approximate Volume in 24cc in the right and 818cc in the left

Ultrasound
• Ultrasound is more accurate than plain chest radiography for estimating pleural fluid volume and aids thoracentesis.
• In a series of 320 patients, Yang et al found that pleural effusions with complex septated, complex non-septated, or homogeneously echogenic patterns are always exudates, whereas hypoechoic effusions can be either transudates or exudates.
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Course in the Wards• No Difficulty of Breathing, No
chest pain• VS Stable
• Refered to Cardio Service for CP Clearance
• Started on HR (Rimactazid) 300mg 1 Tab OD and Ethambutol 400mg/tab 1 tab BID
• Tramadol tablet was started
3rd Hospital Day

Course in the Wards With Epigastric discomfort after
taking HR (Rimactazid), No Difficulty of Breathing, No Chest Pain
VS Stable
• Post thoracentesis• Tea colored pleural fluid of 850
cc
• Repeat CXR: Pneumothorax L 10%• O2 increased at 5 lpm
4th Hospital Day
Pleural Protein 19.6
Serum Protein 56.7
Pleural LDH 215
Serum LDH 399
SGPT 62
SGOT 23
ALK Phosphtase 178
Albumin 29.5
Globulin 27
A:G 1.08
Conjugated biirubin 1.4
Unconjugated bilirubin 16.7
Repeat CXR Decrease in the Volume of Pleural Effusion on the Left Following Thoracentesis
Marginal Pneumothorax on the Left
Gram Stain Pus Cells: (+1)Red Blood Cells: FewNo Bacterial Organism Seen
Culture and Sensitivity No Growth after 48 hrs
Color Yellowish
Character Hazy
RBC 1894 cells/ CU MM
WBC 256 cells/ CU MM
Differential Count All Lymphocytes seen

Exudative VS Transudative
Transudativ
e
• Systemic factors influencing the formation or absorption of pleural fluid are altered so that pleural fluid accumulates
• Left ventricular failure, ascites, and decreased serum oncotic pressure with hypoproteinemia.
Exudative
•Pleural surfaces or the capillaries in the location where the fluid originates are altered such that fluid accumulates•Pleural malignancy, para-pneumonic effusions, and pulmonary embolism
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Light, Richard. Pleural Diseases. 5th Edition. 2007©

Light, Richard. Pleural Diseases. 5th Edition. 2007©

Light, Richard. Pleural Diseases. 5th Edition. 2007©

Light, Richard. Pleural Diseases. 5th Edition. 2007©

Patient with Abnormal Chest Xray
Suspected Pleural fluid
Blunting of Costophrenic angle
Lateral Decubitus Chest Radiograph,
Chest CT, Ultrasound
Fluid Thickness >
10mm
Yes
Algorithm 2
No
Observe
Pleural Effusion Unlikely
Light, Richard. Pleural Diseases. 5th Edition. 2007©
Algorithm for distinguishing transudative
from exudative pleural effusions

Yes
Suspected Pleural fluid
Diagnostic ThoracentesisAny of the following met?PF/ Serum Protein >0.5PLDH/Serum LDH >0.6
Pleural LDH > 2/3rd Upper Normal LimitYes
Probable Exudate
CHF or Cirrhosis?
NoExudate
Apperance of Pleural Fluid; Glucose of Pleural Fluid; Cytology and Differential Count; Plerual Fluid Marker for TB
Yes
Serum Fluid
Gradient >3.1
No
Transudate
Treat CHF or
Nephrosis
Light, Richard. Pleural Diseases. 5th Edition. 2007©
Algorithm for distinguishing transudative
from exudative pleural effusions

Pleural Fluid Protein Patient’s Values
Light’s Criteria
Pleural Protein / Serum Protein
19.6 0.34
56.7
Pleural LDH /Serum LDH
215 0.53
399
Pleural LDH > 2/3rd the upper limits of N serum LDH
215(N: 313 -618)
215< 412
Is the Light’s Criteria for diagnosing an Exudative
Pleural Effusion Fulfilled ? Transudative
Pleural Effusion

Light’s Criteria• Light criteria have an overall diagnostic
accuracy of 93% but commonly misclassify effusions (approximate diagnostic accuracy, 65%) when any 1 of the 3 criteria has a value near its cutoff point.
• Light criteria can be effectively used to categorize effusions as exudates because they are associated with the increased permeability of pleural membranes or the breakdown of intrapleural cells, allowing high–molecular weight constituents to concentrate in the pleural space.
Heffner, J and Klein, J. Recent Advances in the Diagnosis and Management of Malignant Pleural
Effusion, Mayo Clin Proctocol, 2008;83(2):235-250

Light’s Criteria
• For many years, a pleural fluid protein level of 3.0 g/dL was used to separate transudates from exudates, with exudative pleural effusions characterized by a protein level above 3.0 g/dL (13,14).
• Light's criteria identified 98% of the exudates correctly, but they were less accurate in identifying transudates, misclassifying 19 of 112 (17%)
Light, Richard. Pleural Diseases. 5th Edition. 2007©

BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Pleural Fluid Findings Suggestiveof Malignant Pleural Effusion (MPE)
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Pleural Fluid Findings Suggestiveof Malignant Pleural Effusion (MPE)
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Why Transudative?
• Malignant pleural effusions were transudative in 1.5% of malignant mesotheliomas, 6.8% of metastatic diseases, and 11.1% of paramalignant effusions. Cytological examination of pleural fluid in patients with unexplained transudative effusion is essential to rule out malignant processes.
Gonlugur, T., Gonlugur, M. Transudates in Malignancy: Still a Role for Pleural Fluid: Ann Acad Med Singapore 2008;37:760-3

Why Transudative?
• Transudative malignant effusions are generally due to early stages of mediastinal node involvement, atelectasis, or concomitant congestive heart failure.
Gonlugur, T., Gonlugur, M. Transudates in Malignancy: Still a Role for Pleural Fluid: Ann Acad Med Singapore 2008;37:760-3

Gross Apperance of Pleural Fluid
• Most transudative and many exudative pleural effusions • Clear, straw colored, nonviscid, and
odorless• Blood tinged
• Pleural fluid RBC count is between 5,000 and 10,000/mm3
• Turbid pleural fluid• increased cellular content or increased
lipid content
The appearance of the pleural fluid and any odour should be noted. [C]
A pleural fluid haematocrit is helpful in the diagnosis of haemothorax.
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Gross Appearance of Pleural Effusion
• Turbid pleural fluid that clears with centrifugation • Pleural infection
• Turbidity persists after centrifugation, • Chylothorax or a pseudochylothorax
• Chocolate sauce or anchovy paste • Amebiasis with a hepatopleural fistula
• High viscosity • Suggestive of malignant mesothelioma;
2nd to an elevated pleural fluid hyaluronic acid level
Light, Richard. Pleural Diseases. 5th Edition. 2007©

RBC Count
• Bloody• Hematocrit should be obtained on the
fluid• Hct > 1%
• Malignant pleural disease, • Pulmonary embolus• Traumatically induced pleural
effusion • Hct >50% of that of the peripheral blood
• Hemothorax - consider performing a tube thoracostomy
Light, Richard. Pleural Diseases. 5th Edition. 2007©

WBC Count
• Pleural fluid WBC count is of limited diagnostic use.
• Most transudates • Have WBC counts below 1,000/mm3,
• Most exudates • Have WBC counts above 1,000/mm3
• Parapneumonic effusions• Pleural fluid WBC counts above
10,000/mm3
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Neutrophils
• Predominate in pleural fluid resulting from acute inflammation as with pneumonia, pancreatitis, pulmonary embolization, subphrenic abscess, and early tuberculosis
• Interleukin (IL-8) appears to be one of the primary chemotaxins for neutrophils in the pleural space
• The significance of neutrophils in an exudative pleural effusion is that they indicate acute inflammation of the pleural surface.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Lymphocytes
• Probably has a malignant disease, tuberculous pleuritis, or a pleural effusion after CABG surgery
• Almost all of the effusions secondary to tuberculosis, but only two thirds of the effusions secondary to malignant disease had predominantly small lymphocytes
Light, Richard. Pleural Diseases. 5th Edition. 2007©
Differential cell counts on the pleural fluid
Pleural lymphocytosis is common in malignancy and tuberculosis.
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Protein Measurements
• The pleural fluid protein levels • Generally higher in exudative pleural
effusions than in transudative pleural effusions.
• Pleural fluid protein levels • Not useful in separating the various
types of exudative effusions, however, because the protein level in most exudates is elevated to a comparable degree
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Glucose Level
• Low pleural fluid glucose level (<60 mg/dL) indicates• Parapneumonic effusion• malignant disease• rheumatoid disease• tuberculous pleuritis
• The lower the pleural fluid glucose level, the more likely that one is dealing with a complicated parapneumonic pleural effusion.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Lactic Acid Dehydrogenase Measurement
• The higher the LDH, the more inflamed the pleural surfaces
• All Effusions with elevated pleural fluid LDH levels • Seen in most malignant effusions
Light, Richard. Pleural Diseases. 5th Edition. 2007©

pH Measurements• Transudative PE,
• Pleural fluid pH is usually higher than the simultaneous blood pH• Active transport of bicarbonate from the
blood into the pleural space• Exudative PE
• Pleural fluid pH falls substantially below that of the arterial pH
• If the pleural fluid pH is below 7.0, • Complicated parapneumonic effusion
• Therapeutic thoracentesis or tube thoracostomy
Light, Richard. Pleural Diseases. 5th Edition. 2007©
pH
pH should be performed in all non-purulent effusions.[B]
In an infected effusion a pH of <7.2 indicates the need for tube drainage.
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Tests for Diagnosing Pleural Tuberculosis
• Adenosine Deaminase Measurement• Higher in tuberculous pleural effusions
than in other exudates • Cutoff level of between 40 and 45 U/L is
used with levels above this being indicative of tuberculosis• The higher the level, the more likely
the patient is to have tuberculosis
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Course in the Wards Shortness of Breathness with epigastric
pain VS Stable
Repeat CXR: Pneumothorax 80%
Clopidogrel discontinued
Stat CTT: 400cc drained, blood tinge, (+) fluctuations
O2 at 5 lpm via nasal cannula
Post CTT: Reexpansion of L Lung
ICU Transfer
6th Hospital Day
12 lead ECG Sinus TachycardiaComplete Right Bundle Branch BlockAnterior Wall Myocardial Infaraction, Old
Ultrasound of Abdomen Negative Sonographic Study of the Kidneys, Ureters and Urinary Bladder. Normal sized Prostrate Glands; Negative for Mass
Repeat CXR 80% Pnumothorax
Repeat CXR after 6 hrs Post CTT
Complete Reexpansion of the Left Lung with Resoption of the Pleural Fiud Along the Left Costophrenic Area

Pneumothorax
• Air in the pleural space, that is, air between the lung and the chest wall
• Spontaneous pneumothoraces• Ooccur without antecedent trauma or
other obvious cause• Traumatic pneumothoraces
• Occur from direct or indirect trauma to the chest.
• Iatrogenic pneumothorax• An intended or inadvertent consequence of
a diagnostic or therapeutic maneuver
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Complications of Pneumothorax
• The most common complication of thoracentesis is pneumothorax.
• When three different series involving 459 patients are combined, 51 of the patients (11%) developed a pneumothorax and chest tubes were necessary in 9 (2%).
• In a more recent report, the incidence of pneumothorax was 4% in a series of 506 thoracenteses and 2% received a chest tube (18).
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Complications of Pneumothorax
• Thoracentesis is probably the third leading cause of iatrogenic pneumothorax. • Incidence: 5%
• Approximately 20% to 50% of those with a pneumothorax requiring a chest tube
• The incidence of pneumothorax can be decreased if the thoracentesis is performed by experienced interventional radiologists with ultrasound guidance.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Indication for Chest Drain Insertion
BTS guidelines for the insertion of a chest drain. D Laws, E Neville, J Duffy, on behalf of the British Thoracic Society Pleural Disease
Group, a subgroup of the British Thoracic Society Standards of Care Committee, Thorax 2003;58(Suppl II):ii53–ii59

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT output: 500mL/day
Clopidogrel Resumed Decreased O2 at 2 lpm
Tramadol was given for pain
8th Hospital Day

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT output: 350cc/day
Cell Cytology
11th Hospital Day
Cell Cytology of Pleural Fluid
Reddish Fluid and a volume approximately 600ml for cell cytologic Evaluation
Chronic Inflammatory Pattern with Reactive Mesothelial Hyperplasia
Repeat Pleural Fluid Cytology: Atypical Mesothelial Cells

Cytologic Examinations
• The nuclei of malignant cells may exceed 50 µm in diameter, in contrast with mesothelial cell nuclei, which rarely exceed 20 µm in diameter.
• Small lymphocytes, by comparison, have a diameter of approximately 10 µm.
• Mesotheliomas tend to have true papillary aggregation, multinucleation with atypia, and cell-to-cell apposition, whereas adenocarcinomas tend to have acinus-like structures and balloon-like vacuolation
Light, Richard. Pleural Diseases. 5th Edition. 2007©
Cytology
Malignant effusions can be diagnosed by pleural fluid cytology alone in only 60% of cases.
If the first pleural cytology specimen is negative, this should be repeated a second time. [B]
Both cell blocks and fluid smears should be prepared for examination and, if the fluid has clotted, it needs to be fixed and sectioned as a histological section. [B]
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT output: 400cc/day
Immunohistochemical Staining CEA, CK 7, Calretenin, CK
20
12th Hospital Day

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT output: 200cc/day
Bone Scan
Contemplated Pleurodesis if CTT output is < 100cc/day
13th Hospital Day
Bone Scintigraphy No Evidence of Bone Metastasis

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT output: 0cc/day
CT Scan of Chest
Pleurodesis done Doxurubicin
15th Hospital DayNon-Contrast and Contrast CT
Bilateral Pleural Effusion, Larger Amount on the Left side
The Tip of the Thoracotomy Tube is in the Left Major Fissure
Small Amount of Fluid Collections in the Pericardial Sac
Ground Glass Opacity in the Left <Lower Lobe Secondary to Compressive Atelectasis or infiltrates

Prerequisites for Pleurodesis
• Significant symptoms that are relieved when pleural fluid is evacuated
• Evidence of complete re-expansion of the lung without evidence of bronchial obstruction or fibrotic-trapped lung
• Daily tube drainage is less than 150 mL/day• Reserved for those cases where there is no
other therapeutic alternative, or when this has already failed
• If the patient undergoing pleurodesis is receiving corticosteroid therapy
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Light, Richard. Pleural Diseases. 5th Edition. 2007©
CT Scan
• Useful in distinguishing empyema with air fluid levels from lung abscess
• Identify pleural thickening, which suggests that the patient has an exudative effusion. • In one study, 36 of 59 exudative effusions
(61%) had associated pleural thickening, whereas only 1 of 27 transudates (4%) had associated pleural thickening (45).
• An added bonus with CT is the clear demonstration of bone pathology such as metastases or tuberculosis.
CT Scan
CT scans for pleural effusion should be performed with contrast enhancement. [C]
In cases of difficult drainage, CT scanning should be used to delineate the size and position of loculated effusions. [C]
CT scanning can usually differentiate between benign and malignant pleural thickening.
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Course in the Wards (-) DOB, comfortable VS Stable Decreased Breath Sounds at L
CTT removed
17th Hospital Day

Course in the Wards (-) DOB, comfortable VS Stable Discharged
Home Medications: HR (Rimactactazid) 300mg/tab 1
tablet OD E 400mg/tab 1 tablet BID before
meals Ipratropium + Salbutamol beulization
every 8 hrs. Lactulose 15 ml OD HS Pantoprazole 40mg/tab 1 tab OD HS
21th Hospital Day

Course in the Wards Home Medications:
Cefixime 200mg/tab 1 tablet BID PO Digoxin 0.25 mg/tab 1 tablet OD PO Clopidogrel 75mg/tab 1 tablet OD
PO Losartan 50mg/tab 1 tablet OD PO Simvastatin 80 mg/ tab 1 tablet OD
PO Metformin 500mg/tab 1 tablet OD
PO Trimetazidine 1 tablet BID PO Essentiale Forte 1 capsule BID PO
21th Hospital Day
Immunochemical StainingCEA (-)
CK 7 (+)
CK20 (-)
Calretenin (+)

Immunochemical Staining
• Best markers for adenocarcinoma • Carcinoembryonic antigen (CEA) • MOC-31 (or B72.3, Ber-EP4, or BG8)
• Best markers for mesothelioma • Calretinin and cytokeratin
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Final Diagnosis
• Malignant Pleural Effusion Secondary to Mesothelioma
• HCVD, Congestive Heart Failure NYHC I Secondary to CAD
• S/P AMI• S/P PTCA• DM Type 2, controlled

Clinical Manifestation of Pleural Effusion
• Pleuritic chest pain • Inflammation of the pleura, specifically,
the parietal pleura as the visceral pleura does not have pain fibers.
• Dull, aching chest pain rather than pleuritic chest pain• Pleural malignancy
• Either pleuritic chest pain or dull, aching chest pain • The parietal pleura is probably involved
and that the patient - exudative pleural effusion.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Clinical Manifestation of Pleural Effusion
• A second symptom - dry, nonproductive cough• The mechanism is not clear, although it
may be related to pleural inflammation • Lung compression by the fluid may
bring opposing bronchial walls into contact, stimulating the cough reflex
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Clinical Manifestation of Pleural Effusion
• The third symptom is dyspnea. • PE acts as a space-occupying process
in the thoracic cavity and therefore reduces all subdivisions of lung volumes
• Larger PE obviously cause a significant reduction in lung volumes.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Clinical Manifestations of Pleural Effusion
• Tactile fremitus:• Absent or attenuated because the fluid
absorbs the vibrations emanating from the lung
• Much more reliable than percussion for identifying both the upper border of the pleural fluid and the proper site to attempt a thoracentesis.
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Clinical Manifestations of Pleural Effusion
• Percussion:• Dull or flat• Dullness is maximum at the lung bases
where the thickness of the fluid is the greatest
• If the dullness shifts as the position of the patient is changed, one can be almost certain that free pleural fluid is present
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Clinical Manifestations of Pleural Effusion
• Breath Sounds:• Auscultation over the pleural fluid
characteristically reveals decreased or absent breath sounds
• Pleural rub. • Coarse, creaking, leathery sounds
most commonly heard during the latter part of inspiration and the early part of expiration, producing a to-and-fro pattern of sound
Light, Richard. Pleural Diseases. 5th Edition. 2007©

Epidemiology – Malignant Mesotehlioma
• There is widespread variation in the incidence of malignant mesothelioma in England: two Strategic Health Authorities have 30 cases annually while two have 100 cases per year.
• Asbestos fibres are the cause of most cases of mesothelioma. Evidence from two British studies suggests that the proportion of men with mesothelioma directly attributable to occupational asbestos exposure may be about 85%, and this is consistent with evidence from studies in other countries.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Epidemiology – Malignant Mesothelioma
• Malignant mesothelioma will increase in incidence over the next 5–10 years. It is inexorably progressive with a very poor 5-year survival and a median survival of 8– 14 months.
• Simian virus 40 (SV40), a DNA virus, has been implicated as a cofactor in the causation of malignant mesothelioma
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Epidemiology – Malignant Mesothelioma
• Mesothelioma • Fifth to seventh decades• 70–80% of cases occur in men• Between the ages of 20 to 40 years
usually have a history of childhood exposure
• Typical presenting features are those of chest pain, dyspnea or both
• Physical examination is usually unremarkable except for signs of pleural effusion and pleural thickening due to tumour infiltration
Moore, J., Parker, R, Wiggins J. Review, Malignant MesotheliomaOrphanet Journal of Rare Diseases 2008, 3:34 doi:10.1186/1750-
1172-3-34

Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Pathophysiology
• Four principal processes by which asbestos affects the pleura.• First, asbestos fibers may irritate the
pleura.• Shape of asbestos fibers• Fibers penetrating the lung induce
disease manifested • Scarring (plaques) • Frank malignant process
(malignant mesothelioma).
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Pathophysiology• Second, asbestos fibers may sever or
pierce the mitotic spindle of cells and thereby disrupt mitosis
• Third, asbestos induces the generation of ironrelated reactive oxygen species that cause DNA damage
• Fourth, asbestos induces phosphorylation of the mitogen-activated protein (MAP) kinases and of extracellular signal–regulated kinases (ERK) 1 and 2
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Key Biologic Features of Malignant Mesothelioma
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Suspected malignantmesothelioma:
diagnostic algorithm
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Diagnostics Imaging for Malignant Mesothelioma
• Contrast-enhanced CT • Primary imaging modality used for the
evaluation of suspected malignant pleural disease.
• Malignant or inflammatory pleural disease enhances strongly, and the contrast allows differentiation between thickened pleura, effusion and underlying aerated or collapsed lung.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Diagnostics Imaging for Malignant Mesothelioma
• CT features used to distinguish malignant from benign pleural disease were• (1) circumferential pleural thickening, • (2) nodular pleural thickening, • (3) parietal pleural thickening 1 cm,• (4) mediastinal pleural involvement.• Specificities:100%, 94%, 94% and 88%
respectively.• Sensitivities: 41%, 51%, 36% and 56%
respectively.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Diagnostics Imaging for Malignant Mesothelioma
• Magnetic resonance imaging (MRI)• Limited role in the evaluation of malignant
mesothelioma• MRI, with its ability to scan in any plane,
has been used to accurately assess resectability prior to radical surgery
• 18F-fluorodeoxyglucose positron emission tomography (FDG PET)• May be useful in differentiating benign from
malignant pleural disease and might guide choice of biopsy site.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee



Histopathological analysis
• Malignant mesothelioma • EMA• Calretinin• WT1• Cytokeratin 5/6• HBME-1 (an anti–mesothelial cell
antibody) or• Mesothelin (more than 85 percent of
epithelioid
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Immunochemical Staining
• Electrochemiluminescence and micro-particle enzyme immunoassays of PF can detect tumor markers none of the available tumor markers has sufficient diagnostic yield to be used in routine clinical practice.
• Groups of immunohistochemical markers could lead to a diagnosis in approximately 80% of patients with malignant mesothelioma.
Heffner, J and Klein, J. Recent Advances in the Diagnosis and Management of Malignant Pleural Effusion, Mayo Clin Proctocol,
2008;83(2):235-250

BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Histopathological analysis
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Management of Malignant Mesothelioma
• Treatment Strategy:• Management of the pleural effusion.• Indications for prophylactic radiotherapy to
intervention sites.• Indications for chemotherapy.• Immediate supportive care requirements.• Compensation issues.• Suitability for radical surgery.• Suitability for clinical trial entry.• Referral to the specialist multidisciplinary
team.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee
Moore, J., Parker, R, Wiggins J. Review, Malignant MesotheliomaOrphanet Journal of Rare Diseases 2008, 3:34 doi:10.1186/1750-
1172-3-34

Treatment Strategy: Surgery
• Extrapleural pneumonectomy (EPP) (or pleuropneumonectomy)• Eradicate all macroscopic disease,
ideally with good clearance margins.• Operative mortality: 4–9%• Significant complications: Over 60% of
patients• A median survival of 19 months
following this radical operation with adjuvant chemotherapy and radiotherapy
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Surgery
• Debulking operation (cytoreductive surgery)• Less radical approach• Can be performed by VATS or thoracotomy• Has been reported to be effective in
preventing fluid recurrence • May also be associated with increased
survival although, like EPP, it has not yet been tested in a randomized trial
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Pleurodesis
• Early pleurodesis is a key aim for symptom control and prevention of the development of a trapped lung.
• Thoracoscopy is an extremely useful diagnostic and therapeutic tool.
• Calibrated talc is the pleurodesis agent of choice.
• Indwelling pleural catheters are useful for symptom control in cases of trapped lung or where chemical pleurodesis has failed.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Pleurodesis• Talc is the most effective sclerosant available for
pleurodesis. [B]• A small number of patients (<1%)may develop
acute respiratory failure following talc administration. [B]
• Tetracycline ismodestly effective, has few severe side effects, and is the preferred sclerosant to minimise adverse event rates. [B]
• Bleomycin is an alternative sclerosant with a modest efficacy rate but is expensive. [B]
• Pleuritic chest pain and fever are the most common side effects of sclerosant administration. [B]
BTS guidelines for the investigation of a unilateral pleuraleffusion in adults, Thorax 2003;58(Suppl II):ii8–ii17

Treatment Strategy: Pleurodesis
• Sterile talc• Currently the most effective freely available
pleurodesis • Dose of the talc should not exceed 4 g,
• Should be calibrated to avoid the rare risk of the development of ARDS
• The intercostal tube should be clamped for 1 h after sclerosant administration and, in the absence of excessive fluid drainage (.250 ml/day), removed 24–48 h later.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee
Moore, J., Parker, R, Wiggins J. Review, Malignant MesotheliomaOrphanet Journal of Rare Diseases 2008, 3:34 doi:10.1186/1750-
1172-3-34

Treatment Strategy: Pleurodesis
• Success rates (complete and partial response) for talc slurry range from 88% to 100% with a mean of 90%.
• In a recent randomised trial between talc slurry (5 g) and bleomycin (60 units), 90% of the talc group achieved a complete response at 2 weeks compared with 79% of the bleomycin group, which was statistically insignificant.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Radiotherapy
• Palliative radiotherapy provides pain relief in about half of all patients.
• Palpable masses respond to radiotherapy in about half of all patients.
• Breathlessness and superior vena caval obstruction rarely respond to radiotherapy.
• Prophylactic radiotherapy may reduce chest wall implantation following invasive procedures, but may be most applicable for patients with a better prognosis and after more invasive procedures.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Radiotherapy
• The current recommendation • Patients of good performance status
(and therefore longer survival) who have chest wall wounds should be referred for radiotherapy promptly and treated with a three-fraction schedule.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Chemotherapy
• In general, palliative chemotherapy should be considered for all patients with performance status 0–2.
• The objective response rate that should be expected is of the order of 20–40%, and two randomised controlled trials have shown significant differences in survival between regimens, implying that chemotherapy may extend the life expectancy of some patients with mesothelioma.
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Chemotherapy
BTS statement on malignant mesothelioma in the UK, 2007British Thoracic Society Standards of Care Committee

Treatment Strategy: Chemotherapy
• Until recently, all reviews of chemotherapy for malignant mesothelioma reported poor response rates (typically less than 15 to 20 percent) and, because of these low rates, did not recommend a standard of care.
• In a multicenter phase 3 study involving 448 patients, those treated with pemetrexed plus cisplatin had a longer overall median survival (12.1 months) than those treated with cisplatin alone (9.3 months) and had an objective response rate (shrinkage of the tumor by at least 50 percent) of 41 percent.
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

New Approaches to Treatment for Mesothelioma
Bruce W.S. Robinson, M.D., and Richard A. Lake, Ph.D. Advances in Malignant Mesothelioma. New England Journal Medicine
2005;353:1591-603.

Key Points:
• The most common cause of increased pleural fluid formation is increased interstitial fluid in the lung.
• Light's criteria identified 98% of the exudates correctly, but they were less accurate in identifying transudates, misclassifying 19 of 112 (17%).
• Pleural lymphocytosis is common in malignancy and tuberculosis.
• Ultrasound is more accurate than plain chest radiography for estimating pleural fluid volume and aids thoracentesis.

Key Points:
• Thoracentesis is probably the third leading cause of iatrogenic pneumothorax.
• CT features used to distinguish malignant from benign pleural disease.
• Groups of immunohistochemical markers could lead to a diagnosis in approximately 80% of patients with malignant mesothelioma.
• Calibrated talc is the pleurodesis agent of choice for Malignant Mesothelioma.
• Patients should be offered Surgery, Radiotherapy and Chemotherapy depending on the treatment strategy.













![Management of Malignant Pleural Effusion...Asymptomatic patients with either a malignant or a paramalignant effusion need not be treated initially [9]. Malignant pleural effusion will](https://static.fdocuments.us/doc/165x107/5f8bc67cd3c5026bc44819fe/management-of-malignant-pleural-effusion-asymptomatic-patients-with-either-a.jpg)

