Case presentation ( lab investigations of congenital anomalies )
51
Rania Mohamed El-Sharkawy r [email protected] Lecturer of clinical chemistry, MRI-Alexandria University ,CPHQ,LSSGB Health governance –MRI-Alex university unit coordinator IHI Egypt & NAHQ member
-
Upload
rania-el-sharkawy -
Category
Health & Medicine
-
view
359 -
download
0
description
Congenital anomalies are very hard to detect by the lab investigations ,proper lab investigations and assessment is a challenge and this case is one of the challenges.
Transcript of Case presentation ( lab investigations of congenital anomalies )

Rania Mohamed [email protected]
Lecturer of clinical chemistry, MRI-Alexandria University ,CPHQ,LSSGBHealth governance –MRI-Alex university unit coordinator
IHI Egypt & NAHQ member

Case study presentation

A four years old female child ,born with physiological neonatal jaundice . At the age of six months she presented with an attack of :
Bile stained vomitus
Epigastric and right hypochondrial pain
Pallor & fatigue
CASE PRESENTATION
The attack lasted for 7-10 days

• These attacks were repeated, twice at the age of two years and 3 times at the age of three ,and twice at the age of four .These last two attacks were associated with fever????
• In between the attacks the girl was totally free except for transient attacks of epigastric pain
• During these attacks the following was done:
CASE PRESENTATION

Ultrasonography
Magnetic resonance cholangiography
CT following oral & IV contrast media
IMAGING TECHNIQUES

Mild dilatation of the Gall Bladder
Dilatation and irregular caliber of the common bile duct with (3-5 ) 5 mm stones , no intrahepatic biliary dilatation
The spleen was slightly enlarged
Liver and pancreas were totally free
In between the attacks there were no stones but the G.B remained dilated and also was the CBD
IMAGING TECHNIQUES POSITIVE FINDINGS

The following
Laboratory
Investigations
were done

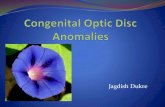
AST & ALT AT THE AGE OF TWO YEARS

AST & ALT AT THE AGE OF THREE YEARS

AST & ALT AT THE AGE OF FOUR YEARS
January February April0
200
400
600
800
1000
1200
1400
1600
1800
Distribution of AST and ALT at the age of four
AST ALT Normal
Months
Mea
n


Total and direct bilirubin

Total and direct bilirubin

Total and direct bilirubin
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
January February April
Mean
Months
Distribution of total bil and direct bil in 2009(age of 4)
Total bilerubin Direct bilerubin
Normal total bilerubin Normal direct bilerubin


Alkaline phosphatase AT THE AGE OF TWO YEARS

Alkaline phosphatase AT THE AGE OF THREE YEARS

Alkaline phosphatase AT THE AGE OF FOUR YEARS
January February April0
100
200
300
400
500
600
700
800
Distribution of Alk in 2009 in between the age of (4-5)
Alk Upper normal Lowest normal
Months
Mea
n


GAMA GLUTMYLE TRANSFERASE
AT THE AGE OF TWO YEARS
0
50
100
150
200
250
300
350
February March April May July November December
Mea
n
MonthsDistribution of GGT in 2007(age of 2)
CGT Upper normal Lowest normal

GAMA GLUTMYLE TRANSFERASE
AT THE AGE OF THREE YEARS
0
100
200
300
400
500
600
700
800
February March April May July November
Mea
n
MonthsDistribution of GGT in 2008(age of 3)
CGT Upper normal Lowest normal
0
100
200
300
400
500
600
700
800
February March April May July November
Mea
n
MonthsDistribution of GGT in 2008(age of 3)
CGT Upper normal Lowest normal
0
100
200
300
400
500
600
700
800
February March April May July November
Mea
n
MonthsDistribution of GGT in 2008 between the age of (3-4)
CGT Upper normal Lowest normal

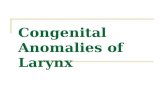
GAMA GLUTMYLE TRANSFERASE
IN THE AGE OF FOUR YEARS
January February April0
50
100
150
200
250
300
350
400
Distribution of GGT in 2009 at the age of 4
CGT Upper normal Lowest normal
Months
Mea
n


CASE PRESENTATION
(5)ALL VIRAL INFECTIONS WERE EXCLUDED:1. Hepatitis A virus IgM2. Hepatitis B3. Hepatitis c4. EBV IgM 5. CMV IgM
OTHER LAB. TESTS…….
(1) Normal PT & PTT
(2) Hb : 9.5 g/dl (Reference range 11.5-14.5)
(4) Cholesterol 220 mg/dl (140-200 mg/dl)
(3) Bile salts : 3.0 µmol/l ( Reference up to 8.1)

CASE PRESENTATION
OTHER LAB. TESTS…….
(6)Autoimmune tests:•Antinuclear Abs …..Negative
•Antismooth muscle Abs……Negative
•Antimitochondrial Abs……..Negative
•Antineutrophil cytoplasmic Abs….Negative
•Anti liver kidney microsomal Abs……Positive

• OTHER LAB. TESTS…….•Plasma protein 6.7 mg/dl
•Albumin 3.5 mg/dl
•Globulins 3.2(2.0-3.8)
•Serum IgG 704.0 mg% ( 730.0-1350.0)
•Serum IgM 66.8 mg% (80.0-150.0)
• Serum IgA 62.3mg/dl (70.0-227.0md/dl)






SUMMARY
CASE PRESENTATION
CLINICALLY• Bile stained vomitus• Epigastric and right hypochondrial pain• Pallor & Fatigue
RADIOLOGICALLY• Mild dilatation of the Gall bladder• Dilatation and irregularity of the common bile duct with (3-5 ) 5
mm stones that disappear in between the attacks• The spleen is slightly enlarged
LABORATORY• Marked elevation of AST & ALT• Elevated ALK & GGT• Mild anemia• PositiveLKM1Abs

WHAT IS THE MOST LIKELY DIAGNOSIS?
WHAT IS THE D.D OF THIS CASE?

WHAT IS THE DIFFERENTIAL DIAGNOSIS?
1. Cholestatic liver diseases
2. Autoimmune Hepatitis
What findings are WITH?
What findings are AGANIST?
3. Hemolytic anemias??????

CASE PRESENTATION
Hemolytic anemia
WITH•Age of incidence•Mild spleenomegaly•Hb 9.5 mg/dl
AGAINST•Normal trace urobilinogen in urine•CBC is normal with normochromic normocytic anemia•No reticulocytes•Coomb`s test negative•Osmotic fragility test negative•Sickling test negative•Normal Hb electrophoresis ( Hb A 97% & Hb A2 3%

• Normal level of alpha 1 antitrypsin• Seronegativity for IgM Antiviral hepatitis• Negative CMV• Negative EBV• Low ethanol ingestion• No recent use of hepatotoxic drugs• Serum gammaglobulins IgG> 1.5% of normal• Positive ANA,ASMA, LKM1
Autoimmune Hepatitis(International autoimmune hepatitis Group)
Liver biopsy to rule out other lesions

Type I:
Autoimmune HepatitisType I:-female> male-Any age-With other autoimmune disease-Positive ANA, ASMA,Antiactin, increased gamma globulins in 97% of cases
Type II:-Girls ages 2-14 years--Signs of fatigue & abdominal pain-LKM1 & increased gamma globulins
Type III:-female> male-Age between 20-40-Positive SLA

CASE PRESENTATION
Autoimmune Hepatitis
WITH•Age of incidence( 2-14)•Female> Male•Signs of fatigue&abd pain•Mild spleenomegaly•ElevatedAST & ALT•Elevated ALK & GGT•Increased ALKM1Abs•Negative CMV,EBV
AGAINST•Normal imaging of the liver•Normal Bilirubin????•No increase in gamma globulins

CASE PRESENTATION
CHOLESTATIC LIVER DISEASES1. Mechanical Bile Duct Obstruction ( STONES)2. Primary Biliary Cirrhosis3. Primary Sclerosing Cholangitis4.Autoimmune cholangitis5.Congenital anomaly in the CBD6. Drug Induced Cholestasis

CASE PRESENTATION
CHOLESTATIC LIVER DISEASES2. Primary Biliary Cirrhosis
WITH •Fatigue(70%)•Spleenomegaly (15%)•Gallstones (30%)•Elevated Aminotransferases•Elevated GGT & ALP•Elevated cholesterol
AGAINST•Age of the case (50 years)•Imaging (no periportal halo sign) •Usually associated with other autoimmune disease•Increased bilirubin•Positive antimotochondrial Abs(sene 98%, spec 96%) & negative Antinuclear Abs(35%)

CASE PRESENTATION
CHOLESTATIC LIVER DISEASES3. Primary Schelerosing Cholangitis
WITH•Symptoms(Fatigue 66%,Abd pain 50%,Fever/ cholangitis 13-45%)•spleenomegaly•Elevated Aminotransferases(3x increase)•Elevated ALP(3x higher)•Normal bilirubin
AGAINST•Age of the case (30 years)•Predominates in males•Imaging shows no beading of the bile duct•Positive Antineutrophil cytoplasmic Abs ( ANCA) in 80% of cases

CASE PRESENTATION
CHOLESTATIC LIVER DISEASES3. Autoimmune cholangitis
Liver biopsy is the gold standard
Same picture of primary biliray cirrhosis with negative AMA may overlap with autoimmune hepatitis

CASE PRESENTATION
CHOLESTATIC LIVER DISEASES1. Mechanical Bile Duct Obstruction
( STONES)•Bile stained vomitus•Presence of stones by imaging techniques•Increased plasma activities of canalicular enzymes ALP & GGT• Increased cytosolic enzymes AST & ALT•Bilirubin is not increased so this is partial obstruction

A Question needs to be answered?
WHAT ARE THE CAUSES OF STONE FORMATION?

There are three types of biliary stones…….
•Pigmented stone
•Mixed stone
•Cholesterol stone

There are three types of biliary stones…….
•Cholesterol stone
•Bile is supersaturated with cholesterolSupported by increased cholesterol ( diet or genetic)
•Decreased bile acid secretion (terminal ileal disease, cholestatic liver diseases)

There are three types of biliary stones…….
Pigmented Stone
Hemolytic anemia
1.CBC2.
Reticulocytes
3. Coomb`s negative
4.Osmotic fragility negative2.Sickling
test
Deconjugation of bilirubin due to cholestasis & infection
1.Stone formation2.Congenital anomaly

Anatomical deformities in the bile duct at the level of the duodenum (Ampullary
dysfunction)This could be diagnosed and treated by ERCP
Congenital anomalies
Due to the her age 4 years
and her size ERCP couldn't be done
8.3 - 10.3 years
SO if these attacks become life threatening so Cholecystectomy and biliary diversion is the only solution

• Colestatic form of liver disease associated lately with ascending cholangitis needs ERCP for Diagnosis and treatment
• Autoimmune hepatitis (type II) and/or autoimmune cholangitis
• need liver biopsy for further assessment
FINAL DIAGNOSIS
I HOPE THAT WE COULD HELP HER TO GET HER SMILE BACK

THANK YOU