Case Conference #3 Amaro-Aribon A2. Diagnostic approach to pleural effusion.
52
Case Conference #3 Amaro-Aribon A2
-
Upload
jeffry-bradley -
Category
Documents
-
view
219 -
download
1
Transcript of Case Conference #3 Amaro-Aribon A2. Diagnostic approach to pleural effusion.

Case Conference #3
Amaro-AribonA2

Diagnostic approach to pleural effusion

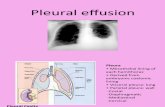
• The history and physical examination are critical in guiding the evaluation of pleural effusion.
• Chest examination of a patient with pleural effusion– dullness to percussion, decreased or absent tactile fremitus, decreased
breath sounds, and decreased voice transmission, mediastinal shift to the opposite side
• Chest x-ray
Approach to a Patient with Pleural Effusion
Diagnostic Approach to Pleural Effusion in Adults, www.aafp.org/afp/20060401/1211.html

• The first step in the evaluation of patients with pleural effusion is to determine whether the effusion is a transudate or an exudate.
Diagnostic approach to pleural effusion
Harrison’s Internal Medicine 17th edition p.1658
Transudative pleural effusion Exudative pleural effusion Occurs when systemic factors that influence the formation and absorption of pleural fluid are altered
Occurs when local factors that influence the formation and absorption of pleural fluid are altered
The leading causes are :•left ventricular failure•cirrhosis
The leading causes are :•bacterial pneumonia•malignancy•viral infection•pulmonary embolism

• Transudative and exudative pleural effusions are distinguished by measuring the lactate dehydrogenase (LDH) and protein levels in the pleural fluid.
• Thoracentesis– invasive procedure to remove fluid or air from the pleural space
for diagnostic or therapeutic purposes
Harrison’s Internal Medicine 17th edition p.1658
Diagnostic approach to pleural effusion

• Perform diagnostic thoracentesis:– if the etiology of the effusion is unclear – if the presumed cause of the effusion does not respond to
therapy as expected. • Pleural effusions do not require thoracentesis:
– if they are too small to safely aspirate (<1 cm thickness on a lateral decubitus film)
– if their presence can be explained by underlying congestive heart failure, etc.
Diagnostic approach to pleural effusion
http://emedicine.medscape.com/article/299959-diagnosis

Light’s criteria• Exudative pleural effusions meet at least one of the following
criteria, whereas transudative pleural effusions meet none:1. pleural fluid protein/serum protein >0.5 2. pleural fluid LDH/serum LDH >0.6 3. pleural fluid LDH more than two-thirds normal upper limit
for serum
Diagnostic approach to pleural effusion
Harrison’s Internal Medicine 17th edition p.1658

•The criteria misidentify ~25% of transudates as exudates. If one or more of the exudative criteria are met and the patient is clinically thought to have a condition producing a transudative effusion, the difference between the protein levels in the serum and the pleural fluid should be measured.
•If this gradient is greater than 31 g/L (3.1 g/dL), the exudative categorization by the criteria can be ignored because almost all such patients have a transudative pleural effusion.
Diagnostic approach to pleural effusion
Harrison’s Internal Medicine 17th edition p. 1658

• The primary reason to make this differentiation is that additional diagnostic procedures are indicated with exudative effusions to define the cause of the local disease.
• If a patient has an exudative pleural effusion, the following tests on the pleural fluid should be obtained: • description of the fluid• glucose level• differential cell count• microbiologic studies • cytology
Harrison’s Internal Medicine 17th edition p. 1658
Diagnostic approach to pleural effusion

Harrison’s Internal Medicine 17th edition p. 1658

Interpretation of the Arterial Blood Gas

Arterial Blood Gas
Parameter Patient’s ABG Normal Values
pH 7.51 7.35-7.45
pCO2 45.6 mmHg 35-45 mmHg
HCO3 36.4 mEq/L 22-26 mEq/L
pO2 58.1 mmHg 80-100 mmHg
P/F ratio 181 400 (60 y/o and below)

Interpretation
• pH- 7.51 Alkalosis• pCO2- 45.66 mmHg• HCO3- 36.4 mEq/L• pO2- 58.1 mmHg Hypoxia• P/F ratio- 181 Hypoxia
Partially Compensated Metabolic Alkalosis with Hypoxia

ACR criteria for SLE

1982 American College of Rheumatology Criteria for SLE
• The presence of 4 of the 11 criteria yields a sensitivity of 85% and a specificity of 95% for SLE.
http://www.ncbi.nlm.nih.gov/pubmed/15580984

1982 American College of Rheumatology Criteria for SLE
Malar rash Fixed erythema over malar areas, sparing nasolabial folds
Discoid rash Erythematous raised patches with keratotic scaling and follicular plugging
Photosensitivity Skin rash after exposure to sunlight, history or physical exam
Oral ulcers Oral or nasopharyngeal, painless, by physical exam
Nonerosive arthritis Tenderness, swelling, effusion in 2 or more peripheral joints
Pleuritis or pericarditis Convincing history or physical exam or ECG or other evidence
Renal disorder >0.5g protein/d or 3+ or cellular casts
Seizures, psychosis Not due to drugs, metabolic derangement, etc
Hematologic disorder Hemolytic anemia or leukopenia (<4000 twice) or lymphopenia (<1500 twice) or thromobocytopenia (<100,000) without other causes
Immunologic disorder Anti-dsDNA or anti-Sm or antiphospholipid antibodies (anticardiolipin, lupus anticoagulant, or false positive test for syphilis)
Positive ANA Higher titers generally more specific (>1:160); must be in the absence of medications associated with drug-induced lupus
Braunwald, et.al Harrison’s Priniciples of Internal Medicine 17th ed. 2006. pg 2077http://www.ncbi.nlm.nih.gov/pubmed/15580984

Reasons for immunocompromised state of the Patient

Immunocompromised state in our Patient:
• Patient has Systemic Lupus Erythematosus• Patient is on the following medications:– Steroids (Methlyprednisolone)– Immunosuppressants (cyclophosphamide)– Biologics (Rituximab)

Systemic Lupus Erythematosus
• Autoimmune disease– An illness that occurs when the body tissues are attacked
by its own immune system inflammation and tissue damage
• An individual with lupus is more susceptible to infection than most people for two reasons: – Lupus directly affects a person's immune system and
reduces his or her ability to prevent and fight infection. – Many of the drugs used to treat lupus suppress the
function of the immune system and leave the body more prone to infection.

Effects Of Medications Used In The Treatment Of Lupus
• Steroids (methlyprednisolone)• Cytotoxic drugs (cyclophosphamide)• Rituximab - a monoclonal antibody that
lowers B cell counts• increase a person's susceptibility to infections
because they suppress both abnormal and normal immune system function
• Reactivation of dormant infectious organisms

Chronic Steroid Use
• Methlyprednisolone– Useful in treatment of inflammatory and
autoimmune reactions– Reverses increased capillary permeability and
suppressing PMN activity may decrease inflammation
• Methylprednisolone and other corticosteroids can mask signs of infection and impair the body's natural immune response to infection.

Mode of Action, Antimicrobial coverage and side effects of piperacillin-tazobactam and
fluconazole

Piperacillin-Tazobactam
• It exerts its bactericidal activity by inhibition cell wall synthesis.
• Tazobactam, a triazolylmethyl penicillanic acid sulphone, is a potent inhibitor of many beta-lactamases, in particular the plasmid mediated enzymes which commonly cause resistance to penicillins and cephalosporins including third-generation cephalosporins.

Commonly susceptible species Gram positive aerobes
Gram negative aerobes
Gram positive anaerobes
Gram negative anaerobes
Brevibacterium spp Enterococcus faecalis Listeria monocytogenes Staphylococcus spp. methicillin-sensitive Streptococcus pneumoniae Streptococcus pyogenes Group B streptococci Streptococcus spp*
Branhamella catarrhalis Citrobacter koseri Haemophilus influenzae* Haemophilus spp. Proteus mirabilis Salmonella spp. Shigella spp.
Clostridium spp. Eubacterium spp. Peptococcus spp. Peptostreptococcus spp.
Bacteroides fragilis* Bacteroides fragilis group Fusobacterium spp. Porphyromonas spp. Prevotella spp*
* Clinical effectiveness against this has been demonstrated in the registered indications. ($) Species showing natural intermediate susceptibility (+) Species for which high resistance rates (more than 50%) have been observed in one or more areas/ countries/regions within the EU.

Species for which resistance may be a problem
Gram positive aerobes Gram negative aerobes Gram negative anaerobes
Staphylococcus aureus, methicillin-sensitive Staphylococcus epidermis, methicillin-sensitive Enterococcus avium ($) Enterococcus faecium (+ $) Propionibacterium acnes ($) Viridans streptococci
Actinobacter spp (+ $) Burkholderia cepacia Citrobacter freundii Enterobacter spp. Escherichia coli * Klebsiella spp. Proteus, indole positive Pseudomonas aeruginosa* Pseudomonas spp. * Pseudomonas stutzeri $ Serratia spp.
Bacteroides spp. *
* Clinical effectiveness against this has been demonstrated in the registered indications. ($) Species showing natural intermediate susceptibility (+) Species for which high resistance rates (more than 50%) have been observed in one or more areas/ countries/regions within the EU.

Inherently resistant organismsGram positive aerobes Gram negative aerobes
Corynebacterium jeikeium Staphylococcus spp. methicillin resistant
Legionella spp Stenotrophomonas maltophilia +$
* Clinical effectiveness against this has been demonstrated in the registered indications. ($) Species showing natural intermediate susceptibility (+) Species for which high resistance rates (more than 50%) have been observed in one or more areas/ countries/regions within the EU.

Adverse Reaction

Adverse Reaction

Fluconazole

Antimicrobial coverage
• Blastomyces dermatitidis • Candida spp. (except C. krusei and C. glabrata) • Coccidioides immitis• Cryptococcus neoformans• Epidermophyton spp. • Histoplasma capsulatum • Microsporum spp. • Trichophyton spp.
https://online.epocrates.com/u/10a635/fluconazole

Adverse ReactionsSerious Reactions Common Reactions
hepatotoxicityseizuresleukopeniaagranulocytosisthrombocytopeniaangioedemaanaphylaxisStevens-Johnson syndrometoxic epidermal necrolysisQT prolongationtorsades de pointes
nauseaheadacherashvomitingabdominal paindiarrheadyspepsiataste changesdizzinesselevated liver transaminases
https://online.epocrates.com/u/10a635/fluconazole

ANTIPHOSPHOLIPID SYNDROMECLINICAL MANIFESTATIONS

Cerebrovascular Manifestations
• cerebral ischemia (arterial thrombosis involves the brain in up to 35% of cases, causing transient ischemic attacks or strokes)
• venous sinus thrombosis • chorea • migraine • transverse myelopathy • seizures

Cerebrovascular Manifestations
• Sneddon syndrome • multi-infarct dementia • retinal venous thrombosis • multiple-sclerosis-like symptoms • psychosis

Cardiac Manifestations
• valvular disease (most commonly mitral regurgitation) affects 10-35% of the patients
• Libman-Sachs endocarditis • coronary artery disease • cardiomyopathy • intracardiac thrombosis

Vascular Disease
• peripheral deep vein or recurrent superficial thromboses
• Venous thrombosis, particularly of the lower limb, occurs in up to 50% of patients with the syndrome.

Pulmonary Manifestations
• pulmonary embolism • pulmonary hypertension • intraalveolar pulmonary hemorrhage • adult respiratory distress syndrome (ARDS) • fibrosing alveolitis

Renal Manifestations
• renal vein and/or artery thrombosis (main branches)
• glomerular and small artery thrombosis • cortical atrophy

Endocrine System Disease
• Addison's disease • hypopituitarism

Hematological Manifestations
• thrombocytopenia • autoimmune hemolytic anemia • bleeding (extremely rare)

Gastrointestinal Manifestations
• Budd-Chiari syndrome • esophageal necrosis • intestinal ischemia • hepatic necrosis

Skin Manifestations
• livedo reticularis • skin ulceration • cutaneous necrosis and infarction • gangrene of digits

Obstetric Manifestations
• The risk of pregnancy loss in women with antiphospholipid antibodies is greatest from the 10th week of gestation onward (fetal period)
• The complications in pregnancy can also include preterm labor, low birth weight, preeclampsia, and stillbirth.

Diagnosis Criteria/Definition

Diagnosis criteria/definition
• thrombosis (arterial and/or venous) • recurrent abortions (>2) • thrombocytopenia and positive aCL or LA ,
occurring twice with an interval of at least 3 months

Clinical Criteria

Clinical Criteria
• one or more episodes of venous, arterial or small vessel thrombosis and/or pregnancy morbidity.
• Pregnancy morbidity was defined as follows – one or more unexplained deaths of a morphologically
normal fetus at or beyond the 10th week of gestation, or – one or more premature deaths at or before the 34th
week of gestation because of severe preeclampsia or eclampsia, or
– three or more unexplained consecutive abortions before the 10th week of gestation

Laboratory Criteria
• IgG and/or IgM aCL in medium or high titers measured by a standard enzyme-linked immunoassay and/or LA detected according to the guidelines of the International Society of Thrombosis and Hemostasis, twice ore more, with an interval of at least 6 weeks between tests. Thus, in clinical practice a diagnostic workup for antiphospholipid antibodies should be considered in all patients with venous or arterial thrombosis and fetal loss for which there is no alternative explanation, particularly in the presence of recurrent manifestations

Complication of SLE and chronic steroids in this patient.

Complications of SLE• Patient’s azotemia, would lead to kidney failure
– Symptoms like bloody stools, changes in mental status, edema, etc.
• Hemolytic anemia– Symptoms like dark urine, splenomegaly, inc. heart rate,etc.
• Myocarditis– Symptoms like irregular heart beat, edema, etc.
• Seizures• Serositis (pleural effusion or pericardial effusion) Thrombocytopenia
– Symptoms like bruising, epistaxis, rash, etc
• Infections• Reccurence of previous illnesses
– As the same degree or worse caseHarrison’s Principle of Internal Medicine, 17th ed.

Complications of SLE• CNS Lupus
(“Neurological disorders in systemic lupus erythematosus patients” by Hawro, T.; et.al. in the journal of Pol Merkur Lekarski. 2009 Jan;26(151):43-8.)
Results: Headache (38.64%) most prevalent symtoms Cerebrovascular disease(31.82%), prevalent among SLE patients with more
active lupus course Seizures (13,64%)
Mononeurpathy (13,64%) Cognitive impairment (6,82%)
Polineuropathy (4,55%) Cranial neuropathy (2,77%)
Acute confusional state (2,27%)
Conclusion: High prevalence of nervous system manifestation in SLE indicates the need for neurological care in SLE patients. Headache is frequent but low specific sign of neuropsychiatric lupus. Neurological disease should incline toward more intense immunosuppressive therapy which may delay the nervous system destruction

Complications of Chronic steroids
• Neurologic Complications• Myopathy• Ocular Complications • Hyperglycemia• Gastrointestinal Complications
– Peptic Ulcer Disease • Pancreatitis • Infection• Bone• Avascular Necrosis • Osteoporosis
Management of Chronic Steroid use by Keenan. Clinics in Chest MedicineVolume 18, Issue 3, 1 September 1997, Pages 507-520