Cancer Project
139
Rehabilitation Systems Cancer Rehabilitation Program Implementation Manual
-
Upload
roger-campbell-ms-lion -
Category
Documents
-
view
50 -
download
3
Transcript of Cancer Project

Rehabilitation Systems
Cancer Rehabilitation Program Implementation Manual

2 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 3
Table of Contents Overview of Common Cancers .................................................................................... 6
DEFINITION ..................................................................................................................... 6
PATHOPHYSIOLOGY ........................................................................................................ 6 COMMON CANCERS ........................................................................................................ 7 DIAGNOSIS ................................................................................................................... 11 THERAPY ..................................................................................................................... 11 VACCINES AND OTHER IMMUNOTHERAPIES ARE THE SUBJECT OF INTENSIVE RESEARCH ..... 12
PALLIATIVE CARE .......................................................................................................... 12 ETHICAL ISSUES ............................................................................................................ 13
Cancer Prevalence in the United States .................................................................... 14
Staging – Diagnostics – Treatments .......................................................................... 25 CANCER SCREENING RECOMMENDATIONS ...................................................................... 27 DIAGNOSTIC TESTS AND STAGING .................................................................................. 28 SELECTED TUMOR MARKERS ......................................................................................... 29
STAGING ...................................................................................................................... 32 REFERENCES ............................................................................................................... 32
Cancer Rehabilitation Literature Review ................................................................... 34 Lab Test Educator ....................................................................................................... 39 Complete Blood Count Chart ..................................................................................... 40
Contraindications to Physical Exercise Following Cancer Diagnosis.................... 41 Cancer Exercise Precautions and Contraindications .............................................. 42
Indications for Terminating a Therapy Session ........................................................ 42
Cancer Rehabilitation Patient Assessment Form ..................................................... 46
Common Goals for Cancer Patients .......................................................................... 53 Writing Functional Goals ............................................................................................ 54
The Compendium of Physical Activities Tracking Guide ........................................ 58 1 TO 2 MET LEVEL ..................................................................................................... 58 2 TO 3 MET LEVEL .................................................................................................... 59
3 TO 4 MET LEVEL ...................................................................................................... 61 4 TO 5 MET LEVEL ...................................................................................................... 62 5 TO 6 MET LEVEL ...................................................................................................... 64
6 TO 7 MET LEVEL ...................................................................................................... 64 7 TO 8 MET LEVEL ...................................................................................................... 65 8 TO 9 MET LEVEL ...................................................................................................... 65
9 TO 10 MET LEVEL .................................................................................................... 65 Quick Reference (MET) to Functional Task Conversions ........................................ 67 SF-36 Health Survey .................................................................................................... 68 Health-Related Quality of Life Survey........................................................................ 69
6 - MINUTE WALK TEST (6MWT) ................................................................................ 75 R P E / FT ...................................................................................................................... 76 DYSPNEA ..................................................................................................................... 77 MET- MPH, Speed, Distance, Energy Conversion Chart .......................................... 78 MET Chart .................................................................................................................... 79 Plan of Treatment or Exercise Prescription and Progression ................................. 81
COMPONENTS OF A PLAN OF TREATMENT OR EXERCISE PRESCRIPTION ............................ 82

4 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
General Aerobic Exercise Recommendations........................................................... 84
Incremental Exercise Progression ............................................................................. 85
Work-Rest Ratio ........................................................................................................... 86 FUNDAMENTALS OF RESISTANCE TRAINING: PROGRESSION AND EXERCISE PRESCRIPTION . 86
Individual Therapeutic Session, SOAP Note Format ................................................ 87 SOAP NOTE .................................................................................................................. 90 Patient Education Outline from Cancer Fitness ........................................................ 92
LESSON ONE(1): CH3 MANAGING YOUR SIDE EFFECTS ................................................. 93 LESSON TWO(2): CH1 CANCER AND EXERCISE: WHAT DOES THE SCIENCE SHOW? ......... 93 LESSON THREE(3): CH2 THE BASICS OF EXERCISE DURING TREATMENT ........................ 93 LESSON FOUR(4): CH4 SETTING GOALS FOR A LIFETIME OF EXERCISE ........................... 93 LESSON FIVE(5): CH5 CANCER FITNESS FUNDAMENTALS ............................................... 93
LESSON SIX(6): CH6 CANCER FITNESS AEROBIC EXERCISE PROGRAM ........................... 94 LESSON SEVEN(7): CH8 THE CORE OF RESISTANCE EXERCISE ...................................... 94 LESSON EIGHT(8): CH11 REALIZING YOUR POTENTIAL ................................................... 94
Cancer Rehabilitation Case Study: Fatigue ............................................................... 95 Manage Common Cancer Treatment Side Effects .................................................... 98 Cancer Rehabilitation Progress Report ................................................................... 101
Program promotion and marketing .......................................................................... 103 THE TOP 10 MARKETING RULES: .................................................................................. 104
Cancer Rehab At-A-Glance ....................................................................................... 106
Course Evaluation ..................................................................................................... 112 About the Instructor .................................................................................................. 113
Suggested Reading: .................................................................................................. 114 Cancer Rehabilitation Bibliography ......................................................................... 116 Cancer Glossary ........................................................................................................ 121

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 5

6 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Overview of Common Cancers
Definition
Cancer is a class of diseases in which a group of cells display uncontrolled growth, invasion, and sometimes metastasis. These three malignant properties of cancers differentiate them from benign tumors, which are self-limited, and do not invade or metastasize. Most cancers form a tumor, but some, like leukemia, do not. The branch of medicine concerned with the study, diagnosis, treatment, and prevention of cancer is oncology.
Cancer affects people at all ages with the risk for most types increasing with age. Cancer caused about 13% of all human deaths in 2007 (7.6 million).
Cancers are caused by abnormalities in the genetic material of the transformed cells. These abnormalities may be due to the effects of carcinogens, such as tobacco smoke, radiation chemicals, or infectious agents. Other cancer-promoting genetic abnormalities may randomly occur through errors in DNA replication, or are inherited, and thus present in all cells from birth. The heritability of cancers is usually affected by complex interactions between carcinogens and the host's genome.
Genetic abnormalities found in cancer typically affect two general classes of genes. Cancer-promoting oncogenes are typically activated in cancer cells, giving those cells new properties, such as hyperactive growth and division, protection against programmed cell death, loss of respect for normal tissue boundaries, and the ability to become established in diverse tissue environments. Tumor suppressor genes are then inactivated in cancer cells, resulting in the loss of normal functions in those cells, such as accurate DNA replication, control over the cell cycle, orientation and adhesion within tissues, and interaction with protective cells of the immune system. Definitive diagnosis requires the histologic examination of a biopsy specimen, although the initial indication of malignancy can be symptomatic or radiographic imaging abnormalities. Most cancers can be treated and some cured, depending on the specific type, location, and stage. Once diagnosed, cancer is usually treated with a combination of surgery, chemotherapy and radiotherapy. As research develops, treatments are becoming more specific for different varieties of cancer. There has been significant progress in the development of targeted therapy drugs that act specifically on detectable molecular abnormalities in certain tumors, and which minimize damage to normal cells. The prognosis of cancer patients is most influenced by the type of cancer, as well as the stage, or extent of the disease. In addition, histologic grading and the presence of specific molecular markers can also be useful in establishing prognosis, as well as in determining individual treatments.
Pathophysiology
Cancers are caused by a series of mutations. Each mutation alters the behavior of the cell somewhat.
Cancer is fundamentally a disease of regulation of tissue growth. In order for a normal cell to transform into a cancer cell, genes which regulate cell growth and differentiation must be

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 7
altered. Genetic changes can occur at many levels, from gain or loss of entire chromosomes to a mutation affecting a single DNA nucleotide. There are two broad categories of genes which are affected by these changes. Oncogenes may be normal genes which are expressed at inappropriately high levels, or altered genes which have novel properties. In either case, expression of these genes promotes the malignant phenotype of cancer cells. Tumor suppressor genes are genes which inhibit cell division, survival, or other properties of cancer cells. Tumor suppressor genes are often disabled by cancer-promoting genetic changes. Typically, changes in many genes are required to transform a normal cell into a cancer cell.
There is a diverse classification scheme for the various genomic changes which may contribute to the generation of cancer cells. Most of these changes are mutation, or changes in the nucleotide sequence of genomic DNA. Aneuploidy, the presence of an abnormal
number of chromosomes, is one genomic change which is not a mutation, and may involve either gain or loss of one or more chromosomes through errors in mitosis.
Large-scale mutations involve the deletion or gain of a portion of a chromosome. Genomic amplification occurs when a cell gains many copies (often 20 or more) of a small chromosomal locus, usually containing one or more oncogenes and adjacent genetic material. Translocation occurs when two separate chromosomal regions become abnormally fused, often at a characteristic location. A well-known example of this is the Philadelphia chromosome, or translocation of chromosomes 9 and 22, which occurs in chronic myelogenous leukemia, and results in production of the BCR-abl fusion protein, an oncogenic tyrosine kinase.
Small-scale mutations include point mutations, deletions, and insertions, which may occur in the promoter of a gene and affect its expression, or may occur in the gene's coding sequence and alter the function or stability of its protein product. Disruption of a single gene may also result from integration of genomic material from
a DNA virus or retrovirus, and such an event may also result in the expression of viral oncogenes in the affected cell and its descendants.
Common Cancers
Lung cancer is a disease of uncontrolled cell growth in tissues of the lung. This growth may lead to metastasis, which is the invasion of adjacent tissue and infiltration beyond the lungs. The vast majority of primary lung cancers are carcinomas of the lung, derived from epithelial cells. Lung cancer, the most

8 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
common cause of cancer-related death in men and women, is responsible for 1.3 million deaths worldwide annually. The most common symptoms are shortness of breath, coughing (including coughing up blood), and weight loss.
The main types of lung cancer are small cell lung carcinoma and non-small cell lung carcinoma. This distinction is important, because the treatment varies; non-small cell lung carcinoma (NSCLC) is sometimes treated with surgery, while small cell lung carcinoma (SCLC) usually responds better to chemotherapy and radiation. The most common cause of lung cancer is long-term exposure to tobacco smoke. The occurrence of lung cancer in nonsmokers, who account for as many as 15% of cases, is often attributed to a combination of genetic factors, radon gas, asbestos, and air pollution, including second hand smoke.
Lung cancer may be seen on chest radiograph and computed tomography (CT scan). The diagnosis is confirmed with a biopsy. This is usually performed via bronchoscopy or CT-guided biopsy. Treatment and prognosis depend upon the histological type of cancer, the stage (degree of spread), and the patient's performance status. Possible treatments include surgery, chemotherapy, and radiotherapy. Depending on the stage and treatment, the five-year survival rate is 14%.
Breast cancer refers to cancers that originate from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the ducts with milk. There are different types of breast cancer, with different stages (spread), aggressiveness, and genetic makeup. Survival varies greatly depending on those factors; with best treatment, 10-year disease-free survival varies from 98% to 10%. Treatment includes surgery, drugs, (hormonal therapy and chemotherapy), and radiation.
Worldwide, breast cancer comprises 10.4% of all cancer incidences, making it the second most common type of non-skin cancer (after lung cancer) and the fifth most common cause of cancer death. In 2004, breast cancer caused 519,000 deaths worldwide (7% of cancer deaths; almost 1% of all deaths). Breast cancer is about 100 times more common in women than in men, but survival rates are equal in both sexes.
Some breast cancers require the hormones estrogen and progesterone to grow, and have receptors for those hormones. After surgery those cancers are treated with drugs that interfere with those hormones, usually tamoxifen, and with drugs that shut off the production of estrogen in the ovaries or elsewhere; this may damage the ovaries and end fertility. Low-risk, hormone-sensitive breast cancers may be treated with hormone therapy and radiation alone. Breast cancers without hormone receptors, or which have spread to the lymph nodes in the armpits, or which express certain genetic characteristics, are higher-risk, and are treated more aggressively. One standard regimen, popular in the U.S., is cyclophosphamide plus doxorubicin (Adriamycin), known as CA; these drugs damage DNA in the cancer, but also in fast-growing normal cells where they cause serious side effects. Sometimes a taxane drug, such as docetaxel, is added, and the regime is then known as CAT; taxane attacks the microtubules in cancer cells. An equivalent treatment, popular in Europe, is cyclophosphamide, methotrexate, and fluorouracil (CMF). Monoclonal antibodies, such as trastuzumab, are used for cancer cells that have the HER2 mutation. Radiation is usually added to the surgical bed to control cancer cells that were missed by the surgery, which

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 9
usually extends survival, although radiation exposure to the heart may cause damage and heart failure in the following years.
Prostate cancer is a form of cancer that develops in the prostate, a gland in the male reproductive system. The cancer cells may metastasize (spread) from the prostate to other parts of the body, particularly the bones and lymph nodes. Prostate cancer may cause pain, difficulty in urinating, problems during sexual intercourse, or erectile dysfunction. Other symptoms can potentially develop during later stages of the disease.
Rates of detection of prostate cancers vary widely across the world, with South and East Asia detecting less frequently than in Europe, and especially the United States. Prostate cancer tends to develop in men over the age of fifty and although it is one of the most prevalent types of cancer in men, many never have symptoms, undergo no therapy, and eventually die of other causes. This is because cancer of the prostate is, in most cases, slow-growing, symptom free and men with the condition often die of causes unrelated to the prostate cancer, such as heart/circulatory disease, pneumonia, other unconnected cancers, or old age. Many factors, including genetics and diet, have been implicated in the development of prostate cancer. The presence of prostate cancer may be indicated by symptoms, physical examinations, prostate specific antigen (PSA), or biopsy. There is controversy about the accuracy of the PSA test and the value of screening. Suspected prostate cancer is typically confirmed by taking a biopsy of the prostate and examining it under a microscope. Further tests, such as CT scans and bone scans, may be performed to determine whether prostate cancer has spread.
Treatment options for prostate cancer with intent to cure are primarily surgery, radiation therapy, and proton therapy. Other treatments, such as hormonal therapy, chemotherapy, cryosurgery, and high intensity focused ultrasound (HIFU) also exist, depending on the clinical scenario and desired outcome.
The age and underlying health of the man, the extent of metastasis, appearance under the microscope, and response of the cancer to initial treatment are important in determining the outcome of the disease. The decision whether or not to treat localized prostate cancer (a tumor that is contained within the prostate) with curative intent is a patient trade-off between the expected beneficial and harmful effects in terms of patient survival and quality of life.
Colorectal cancer, also called colon cancer or large bowel cancer, includes cancerous growths in the colon, rectum and appendix. With 655,000 deaths worldwide per year, it is the fourth most common form of cancer in the United States and the third leading cause of cancer-related death in the Western world. Colorectal cancers arise from adenomatous polyps in the colon. These mushroom-shaped growths are usually benign, but some may develop into cancer over time. The majority of the time, the diagnosis of localized colon cancer is through colonoscopy.
Invasive cancers that are confined within the wall of the colon (TNM stages I and II) are curable with surgery. If untreated, they spread to regional lymph nodes (stage III), where up

10 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
to 73% are curable by surgery and chemotherapy. Cancer that metastasizes to distant sites (stage IV) is not curable, although chemotherapy can extend survival. Radiation is used with rectal cancer
Melanoma is a malignant tumor of melanocytes which are found predominantly in skin but also in the bowel and the eye (see uveal melanoma). It is one of the less common types of skin cancer but causes the majority (75%) of skin cancer related deaths. Melanocytes are normally present in skin, being responsible for the production of the dark pigment melanin. Despite many years of intensive laboratory and clinical research, the greatest chance of cure is in the early surgical resection of thin tumors.
Around 60,000 new cases of melanoma invasive melanoma are diagnosed in the US each year, more frequently in males and in Caucasians. It is more common in Caucasian populations living in sunny climates than in other groups, or in those who use tanning salons. According to a WHO report about 48,000 melanoma related deaths occur worldwide per year.
The treatment includes surgical removal of the tumor, adjuvant treatment, chemo- and immunotherapy, or radiation therapy.
Leukemia is a cancer of the blood or bone marrow and is characterized by an abnormal proliferation (production by multiplication) of blood cells, usually white blood cells (leukocytes). Leukemia is a broad term covering a spectrum of diseases. In turn, it is part of the even broader group of diseases called hematological neoplasms.
Lymphoma is a cancer that begins in the lymphocytes of the immune system and presents as a solid tumor of lymphoid cells. They often originate like balls in lymph nodes, presenting as an enlargement of the node (a tumor). Lymphomas are closely related to lymphoid leukemias, which also originate in lymphocytes but typically involve only circulating blood and the bone marrow (where blood cells are generated in a process termed hematopoiesis) and do not usually form static tumors. There are many types of lymphomas, and in turn, lymphomas are a part of the broad group of diseases called hematological neoplasms..
Thomas Hodgkin published the first description of lymphoma in 1832, specifically of the form named after him, Hodgkin‘s lymphoma. Since then, many other forms of lymphoma have been described, grouped under several proposed classifications. The 1982 Working formulation classification became very popular. It introduced the category non-Hodgkin lymphoma (NHL), divided into 16 different diseases. However, since these different lymphomas have little in common with each other, the NHL label is of limited usefulness for doctors or patients and is slowly being abandoned. The latest classification by the WHO (2001) lists 43 different forms of lymphoma divided in four broad groups.
Some forms of lymphoma are categorized as indolent (e.g. small lymphocytic lymphoma), compatible with a long life even without treatment, whereas other forms are aggressive (e.g.
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 11
Burkitt‘s lymphoma), causing rapid deterioration and death. However, most of the aggressive lymphomas respond well to treatment and are curable. The prognosis therefore depends on the correct classification of the disease, established by a pathologist after examination of a biopsy.
Although older classifications referred to histiocytic lymphomas, these are recognized in newer classifications as of B, T or NK cell lineage. True histiocytic malignancies are rare and are classified as sarcomas.
Diagnosis
The most important diagnostic tool remains the medical history: the character of the complaints and any specific symptoms (fatigue, weight loss, unexplained anima, fever of unknown origin, paraneoplastic phenomena and other signs). Often a physical examination will reveal the location of a malignancy.
Diagnostic methods include:
Biopsy, either incisional or excisional; Endoscopy, either upper or lower gastrointestinal, bronchoscopy, or nasendoscopy; X-rays, CT scanning, MRI scanning, ultrasound and other radiological techniques; Scintigraphy, Single Photon Emission Computed Tomography, Position emission
tomography and other methods of nuclear medicine; Blood tests, including Tumor markers, which can increase the suspicion of certain
types of tumors or even be pathognomonic of a particular disease.
Apart from in diagnosis, these modalities (especially imaging by CT scanning) are often used to determine operability, i.e. whether it is surgically possible to remove a tumor in its entirety.
Generally, a "tissue diagnosis" (from a biopsy) is considered essential for the proper identification of cancer. When this is not possible, "empirical therapy" (without an exact diagnosis) may be given, based on the available evidence (e.g. history, x-rays and scans.)
Occasionally, a metastatic lump or pathological lymph node is found (typically in the neck) for which a primary tumor cannot be found. This situation is referred to as "carcinoma of unknown primary", and again, treatment is empirical based on past experience of the most likely origin.
Therapy
It depends completely on the nature of the tumor identified what kind of therapeutical intervention will be necessary. Certain disorders will require immediate admission and chemotherapy (such as ALL or AML), while others will be followed up with regular physical examination and blood tests. A detailed discussion of treatment options according to the type of cancer is at the National Cancer Institute website with sections on adult cancers, pediatric cancers, and supportive care. There is also a section on complementary and alternative methods of treatment.

12 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Often, surgery is attempted to remove a tumor entirely. This is only feasible when there is some degree of certainty that the tumor can in fact be removed. When it is certain that parts will remain, curative surgery is often impossible, e.g. when there are metastases elsewhere, or when the tumor has invaded a structure that cannot be operated upon without risking the patient's life. Occasionally surgery can improve survival even if not all tumour tissue has been removed; the procedure is referred to as "debulking" (i.e. reducing the overall amount of tumour tissue). Surgery is also used for the palliative treatment of some of cancers, e.g. to relieve biliary obstruction, or to relieve the problems associated with some cerebral tumors. The risks of surgery must be weighed up against the benefits.
Chemotherapy and radiotherapy are used as a first-line radical therapy in a number of malignancies. They are also used for adjuvant therapy, i.e. when the macroscopic tumor has already been completely removed surgically but there is a reasonable statistical risk that it will recur. Chemotherapy and radiotherapy are commonly used for palliation, where disease is clearly incurable: in this situation the aim is to improve the quality of and prolong life.
Hormone manipulation is well established, particularly in the treatment of breast and prostate cancer.
There is currently a rapid expansion in the use of monoclonal antibody treatments, notably for lymphoma (Rituximab), and breast cancer (Trastuzumab).
Vaccines and Other Immunotherapies are the Subject of Intensive Research
A vaccine is a biological preparation that improves immunity to a particular disease. A vaccine typically contains an agent that resembles a disease-causing microorganism, and is often made from weakened or killed forms of the microbe. The agent stimulates the body's immune system to recognize the agent as foreign, destroy it, and "remember" it, so that the immune system can more easily recognize and destroy any of these microorganisms that it later encounters.
Immunotherapy is a medical term defined as "Treatment of disease by inducing, enhancing, or suppressing an immune response".
Immunotherapies designed to elicit or amplify an immune response are classified as Activation Immunotherapies.
Immunotherapies designed to reduce, suppress or more appropriately direct an existing immune response, as in cases of autoimmunity or allergy, are classified as Suppression Immunotherapies.
Palliative care
Approximately 50% of all cancer cases in the Western world can be cured with radical treatment. For pediatric patients, that number is much higher. A large number of cancer patients will die from the disease, and a significant proportion of patients with incurable cancer will die of other causes. There may be ongoing issues with symptom control

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 13
associated with progressive cancer, and also with the treatment of the disease. These problems may include pain, nausea, anorexia, fatigue, immobility, and depression. Not all issues are strictly physical: personal dignity may be affected. Moral and spiritual issues are also important.
While many of these problems fall within the remit of the oncologist, palliative care has matured into a separate, closely allied specialty to address the problems associated with advanced disease. Palliative care is an essential part of the multidisciplinary cancer care team. Palliative care services may be less hospital-based than oncology, with nurses and doctors who are able to visit the patient at home.
Ethical issues
There are a number of recurring ethical questions and dilemmas in oncological practice. These include:
What information to give the patient regarding disease extent/progression/prognosis. Entry into clinical trials, especially in the face of terminal illness.. Withdrawal of active treatment. "Do Not Resuscitate‖ orders and other end of life issues.
These issues are closely related to the patients' personality, religion, culture, personal, and family life. The answers are rarely black and white. It requires a degree of sensitivity and very good communication on the part of the oncology team to address these problems properly.

14 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Prevalence in the United States
2009 Estimated US Cancer Deaths*
ONS=Other nervous system.
Source: American Cancer Society, 2009.
Men
292,540
Women
269,80026% Lung & bronchus
15% Breast
9% Colon & rectum
6% Pancreas
5% Ovary
4% Non-Hodgkinlymphoma
3% Leukemia
3% Uterine corpus
2% Liver & intrahepaticbile duct
2% Brain/ONS
25% All other sites
Lung & bronchus 30%
Prostate 9%
Colon & rectum 9%
Pancreas 6%
Leukemia 4%
Liver & intrahepatic 4%bile duct
Esophagus 4%
Urinary bladder 3%
Non-Hodgkin 3% lymphoma
Kidney & renal pelvis 3%
All other sites 25%
Lung cancer is, by far, the most common fatal cancer in men (30%), followed by prostate (9%), and colon & rectum (9%). In women, lung (26%), breast (15%), and colon & rectum (9%) are the leading sites of cancer death

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 15
US Mortality, 2006
*Includes nephrotic syndrome and nephrosis.
Source: US Mortality Data 2006, National Center for Health Statistics, Centers for Disease Control and Prevention,
2009.
1. Heart Diseases 631,636 26.0
2. Cancer 559,888 23.1
3. Cerebrovascular diseases 137,119 5.7
4. Chronic lower respiratory diseases 124,583 5.1
5. Accidents (unintentional injuries) 121,599 5.0
6. Diabetes mellitus 72,449 3.0
7. Alzheimer disease 72,432 3.0
8. Influenza & pneumonia 56,326 2.3
9. Nephritis* 45,344 1.9
10. Septicemia 34,234 1.4
Rank Cause of DeathNo. of
deaths
% of all
deaths
Cancer accounts for nearly one-quarter of deaths in the United States, exceeded only by heart diseases. In 2006, there were 559,888 cancer deaths in the US.
WASHINGTON (Reuters) - Cancer is on pace to supplant heart disease as the No. 1 cause of death worldwide in 2010, with a growing burden in poor countries thanks to more cigarette smoking and other factors, global health experts said on Tuesday.
Globally, an estimated 12.4 million people will be diagnosed with some form of cancer this year and 7.6 million people will die, the U.N. World Health Organization's International Agency for Research on Cancer said in a report.
"The global cancer burden doubled in the last 30 years of the 20th century, and it is estimated that this will double again between 2000 and 2020 and nearly triple by 2030," according to the report.
By 2030, 26.4 million people a year may be diagnosed with cancer, with 17 million people dying from it, the report forecast.
In men, lung cancer was the most common form in terms of new cases and deaths, while breast cancer was the most common type among women in new cases and deaths, according to the report. More men than women get cancer and die from it.
http://www.reuters.com/article/idUSN0918012220081209

16 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Change in US Death Rates* from 1991 to 2006
* Age-adjusted to 2000 US standard population.
Sources: US Mortality Data, National Center for Health Statistics, Centers for Disease Control and
Prevention, 2009.
17.8
63.3
34.8
313.0
215.1
43.6
180.7200.2
0
100
200
300
400
Heart diseases Cerebrovascular
diseases
Influenza &
pneumonia
Cancer
1991
2006
Rate Per 100,000
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 17
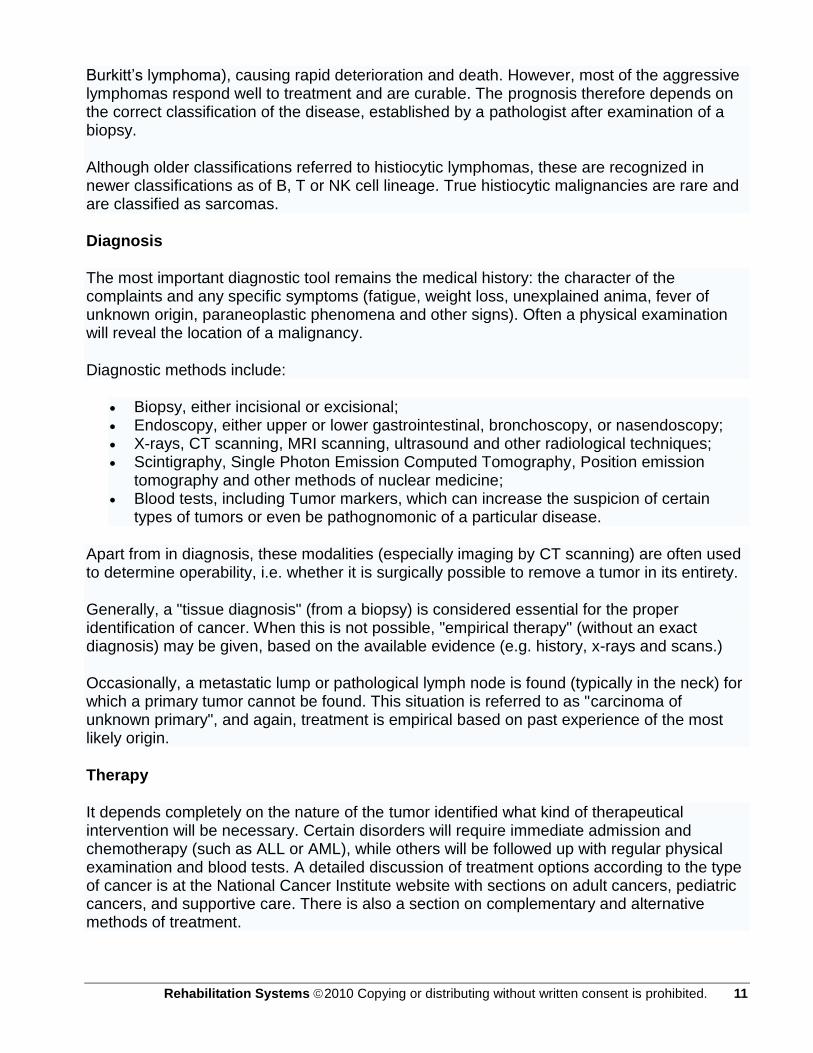
Compared to the peak rate of 215.1 per 100,000 in 1991, the cancer death rate decreased 16% to 180.7 in 2006. Rates for other major chronic diseases decreased substantially during this period.
Trends in the Number of Cancer Deaths Among Men and
Women, US, 1930-2006
0
50,000
100,000
150,000
200,000
250,000
300,000
1930 1940 1950 1960 1970 1980 1990 2000
Women
Men
Nu
mb
er
of
Ca
ncer
De
ath
s
265,000
270,000
275,000
280,000
285,000
290,000
295,000
2000
2001
2002
2003
2004
2005
2006
Men
Women
Source: US Mortality Data, 1930-2006, National Center for Health Statistics, Centers for Disease
Control and Prevention, 2009.
Despite a continuing decline in the cancer death rate from 2005 to 2006, there was an increase in the recorded number of cancer deaths in 2006 as a result of the aging and growth of the US population. The number of cancer deaths decreased by 358 in men and increased by 926 in women, resulting in a net increase of 568 cancer deaths.

18 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
230.7
138.8
190.0
159.2
186.7
95.6
142.0
105.2
313.0
159.0
0
50
100
150
200
250
300
350
400
White African
American
Asian/Pacific
Islander
American
Indian/ Alaskan
Native
Hispanic†
Men Women
*Per 100,000, age-adjusted to the 2000 US standard population.† Persons of Hispanic origin may be of any race.
Source: Surveillance, Epidemiology, and End Results Program, 1975-2005, Division of Cancer Control and
Population Sciences, National Cancer Institute, 2008.
Cancer Death Rates* by Race and Ethnicity, US, 2001-2005
Overall, cancer death rates are higher in men than women in every racial and ethnic group. African American men and women have higher rates of cancer mortality than their counterparts in every other racial and ethnic group. Asian American and Pacific Islander men and women have the lowest cancer death rates, about half the rate of African American men and women, respectively.
Note: Rates for populations other than white and African American may be affected by problems in ascertaining race/ethnicity information from medical records. This is likely to result in reported death rates that are lower than true death rates.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 19
2009 Estimated US Cancer Cases*
*Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder.
Source: American Cancer Society, 2009.
Men
766,130
Women
713,220
27% Breast
14% Lung & bronchus
10% Colon & rectum
6% Uterine corpus
4% Non-Hodgkinlymphoma
4% Melanoma of skin
4% Thyroid
3% Kidney & renal pelvis
3% Ovary
3% Pancreas
22% All Other Sites
Prostate 25%
Lung & bronchus 15%
Colon & rectum 10%
Urinary bladder 7%
Melanoma of skin 5%
Non-Hodgkin 5% lymphoma
Kidney & renal pelvis 5%
Leukemia 3%
Oral cavity 3%
Pancreas 3%
All Other Sites 19%
Now we will turn our attention to the number of new cancers anticipated in the US this year. It is estimated that about 1.5 million new cases of cancer will be diagnosed in 2009. Cancers of the prostate and breast will be the most frequently diagnosed cancers in men and women, respectively, followed by lung and colorectal cancers in both men and in women.

20 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
All Sites 68 58 10
Breast (female) 91 78 13
Colon 66 55 11
Esophagus 18 11 7
Leukemia 52 42 10
Non-Hodgkin lymphoma 66 58 8
Oral cavity 62 42 20
Prostate 99 96 3
Rectum 67 59 8
Urinary bladder 82 66 16
Uterine cervix 74 65 9
Uterine corpus 86 61 25
Cancer Survival*(%) by Race,1996-2004
*5-year relative survival rates based on cancer patients diagnosed from 1996 to 2004 and followed through 2005. Source: Surveillance, Epidemiology, and End Results Program, 1975-2005, Division of Cancer Control and
Population Sciences, National Cancer Institute, 2008.
Site White
Absolute
DifferenceAfrican
American
The 5-year relative survival rate for cancer is 68% among whites and 58% among African Americans (taking normal life expectancy into consideration). For many sites, survival rates in African Americans are 10% to more than 20% lower than in whites. This is due, in part, to African Americans being less likely to receive a cancer diagnosis at an early, localized stage, when treatment can improve chances of survival. Additional factors that contribute to the survival differential include unequal access to medical care and tumor characteristics.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 21
Trends in Five-year Relative Survival (%)* Rates, US, 1975-2004
*5-year relative survival rates based on follow up of patients through 2005. Source: Surveillance, Epidemiology, and End Results Program, 1975-2005, Division of Cancer Control and
Population Sciences, National Cancer Institute, 2008.
Site 1975-1977 1984-1986 1996-2004
All sites 50 54 66
Breast (female) 75 79 89
Colon 52 59 65
Leukemia 35 42 51
Lung and bronchus 13 13 16
Melanoma 82 87 92
Non-Hodgkin lymphoma 48 53 65
Ovary 37 40 46
Pancreas 3 3 5
Prostate 69 76 99
Rectum 49 57 67
Urinary bladder 74 78 81
The survival rates for all cancers combined and for certain site-specific cancers have improved significantly since the 1970s, due, in part, to both earlier detection and advances in treatment. Survival rates markedly increased for cancers of the prostate, breast, colon, rectum, and for leukemia. With new treatment techniques and increased utilization of screening, there is hope for even greater improvements in the not-too-distant future.

22 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Tobacco Use in the US, 1900-2005
0
500
1000
1500
2000
2500
3000
3500
4000
4500
50001900
1905
1910
1915
1920
1925
1930
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
Year
Per
Cap
ita C
igare
tte C
on
su
mp
tio
n
0
10
20
30
40
50
60
70
80
90
100
Ag
e-A
dju
ste
d L
un
g C
an
cer
Death
Rate
s*
*Age-adjusted to 2000 US standard population.
Source: Death rates: US Mortality Data, 1960-2005, US Mortality Volumes, 1930-1959, National Center for Health
Statistics, Centers for Disease Control and Prevention, 2006. Cigarette consumption: US Department of
Agriculture, 1900-2007.
Per capita cigarette
consumption
Male lung cancer
death rate
Female lung cancer
death rate
Tobacco use is a major preventable cause of death, particularly from lung cancer. The year 2004 marks the anniversary of the release of the first Surgeon General‘s report on Tobacco and Health, which initiated a decline in per capita cigarette consumption in the United States. As a result of the cigarette smoking epidemic, lung cancer death rates showed a steady increase through 1990, then began to decline among men. The lung cancer death rate among US women, who began regular cigarette smoking later than men, has begun to plateau after increasing for many decades.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 23
Note: Data from participating states and the District of Columbia were aggregated to represent the United
States.
Source: Behavioral Risk Factor Surveillance System CD-ROM (1984-1995, 1996, 1998) and Public Use Data Tape
(2000, 2003, 2005, 2007), National Center for Chronic Disease Prevention and Health Promotion, Centers for
Disease Control and Prevention, 1997, 1999, 2000, 2001, 2004, 2006, 2008.
24.2 24.4 24.1 24.4 23.6 24.3 24.7
0
5
10
15
20
25
30
35
1994 1996 1998 2000 2003 2005 2007
Year
Pre
va
len
ce
(%
)
Trends in Consumption of Five or More Recommended Vegetable
and Fruit Servings for Cancer Prevention, Adults 18 and Older,
US, 1994-2007
The American Cancer Society recommends that individuals eat five or more servings of vegetables and fruits a day for cancer prevention. Fruit and vegetable consumption may protect against cancers of the mouth and pharynx, esophagus, lung, stomach, and colon and rectum. However, there has been little improvement in consumption since the mid-1990s. About one in four adults was eating the recommended servings in 2007.

24 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Trends in Overweight* Prevalence (%), Adults 18 and Older,
US, 1992-2007
1992 1995
1998
Less than 50% 50 to 55% More than 55% State did not participate in survey
*Body mass index of 25.0 kg/m2or greater. Source: Behavioral Risk Factor Surveillance System, CD-ROM (1984-1995,
1998) and Public Use Data Tape (2004-2007), National Center for Chronic Disease Prevention and Health Promotion,
Centers for Disease Control and Prevention, 1997, 2000, 2005, 2007, 2008.
2007
This slide highlights the obesity epidemic as mentioned in the previous slide. In 2007, over 55% of adults in all states, including District of Columbia, were overweight or obese, compared to none in 1992.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 25
Staging – Diagnostics – Treatments
Cancer is suspected based on a person's symptoms, the results of a physical examination,
and sometimes the results of screening tests. Occasionally, x-rays obtained for other
reasons such as an injury, show abnormalities that might be cancer. Confirmation that
cancer is present requires other tests (termed diagnostic tests). After cancer is diagnosed, it
is staged. Staging is a way of describing how advanced the cancer has become, including
such criteria as how big it is and whether it has spread to neighboring tissue or more
distantly to lymph nodes or other organs.
Screening
Screening tests serve to detect the possibility that a cancer is present before symptoms
occur. Screening tests usually are not definitive; results are confirmed or disproved with
further examinations and tests. Diagnostic tests are performed once a doctor suspects that
a person has cancer.
Although screening tests can help save lives, they can be costly and sometimes have
psychologic or physical repercussions. Screening tests can produce false-positive results—
results that suggest a cancer is present when it actually is not. False-positive results can
create undue psychologic stress and can lead to other tests that are expensive and risky.
Screening tests can also produce false-negative results—results that show no hint of a
cancer that is actually present. False-negative results can lull people into a false sense of
security. For these reasons, there are only a small number of screening tests that are
considered reliable enough for doctors to use routinely.
Doctors determine whether a particular person is at special risk for cancer—because of
age, sex, family history, previous history, or lifestyle—before they choose to perform
screening tests. The American Cancer Society has provided cancer screening guidelines
that are widely used. Other groups have also developed screening guidelines. Sometimes
recommendations vary among different groups, depending on how the groups' experts
weigh the relative strength and importance of available scientific evidence.
In women, two of the most widely used screening tests are the Papanicolaou (Pap) test to
detect cervical cancer and mammography to detect breast cancer. Both screening tests
have been successful in reducing the death rates from these cancers in certain age groups.
In men, prostate-specific antigen (PSA) levels in the blood may be used to screen for
prostate cancer. PSA levels are high in men with prostate cancer, but levels also are
elevated in men with noncancerous (benign) enlargement of the prostate. As such, the
main drawback to its use as a screening test is the large number of false-positive results,
which generally lead to more invasive tests. Whether the PSA test should be used routinely

26 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
to screen for prostate cancer is unresolved, with varying recommendations from different
groups. Men over 50 should discuss the PSA test with their doctor.
A common screening test for colon cancer involves checking the stool for blood that cannot
be seen by the naked eye (occult blood). Finding occult blood in the stool is an indication
that something is wrong somewhere in the gastrointestinal tract. The problem may be
cancer, although many other disorders, such as ulcers, hemorrhoids, diverticulosis (small
pouches in the colon wall), and abnormal blood vessels in the intestinal walls, can also
cause small amounts of blood to leak into the stool or another nonsteroidal anti-
inflammatory drug (NSAID) or even eating red meat can temporarily produce a positive
result. Positive results on the most commonly used test can occasionally be caused by
consuming certain raw fruits and vegetables (turnips, cauliflower, broccoli, melons,
radishes, and parsnips). Some people with blood in the stool may have negative test results
because they have consumed vitamin C. Newer screening tests for occult blood that use a
different technique are much less susceptible to such errors but are somewhat more costly.
Outpatient procedures such as sigmoidoscopy and colonoscopy are also often used for
colon cancer screening.
Some screening tests can be done at home. For example, monthly breast self-examinations
may help women detect breast cancer. Periodically examining the testes may help men
detect testicular cancer, one of the most curable forms of cancer, especially when
diagnosed early. Checking the mouth for sores may help detect mouth cancer in an early
stage.
Tumor markers are substances secreted into the bloodstream by certain tumors. It was first
thought that measuring levels of these markers would be an excellent way to screen
asymptomatic people for cancer. However, tumor markers are often present to some extent
in the blood of people who do not have cancer. Finding a tumor marker does not
necessarily mean a person has cancer, and tumor markers have a very limited role in
cancer screening.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 27
Cancer Screening Recommendations
Procedure Frequency
Skin cancer
Physical examination Should be part of a routine checkup; more frequent
examinations may be needed for people at high risk for
developing skin cancer
Whole-body
photography
Not routinely needed; may be helpful for people with
multiple moles or in whom examination of the skin is difficult
Lung cancer
Chest x-ray Not recommended on a routine basis
Sputum cytology Not recommended on a routine basis
Low-dose spiral
computed tomography
Not recommended on a routine basis, but is under
investigation
Rectal and colon cancer
Stool examination for
occult blood
Yearly after age 50†
Sigmoidoscopic or
colonoscopic
examination
Every 5 years beginning at age 50 (sigmoidoscopy)†
Every 10 years beginning at age 50 (colonoscopy)
Prostate cancer
Rectal examination Yearly after age 50
Blood test for prostate-
specific antigen
Yearly after age 50
Cervical cancer
Papanicolaou (Pap) test Annual regular Pap test (or newer liquid-based Pap test
every 2 years) beginning between ages 18 and 21. Some
women 70 years of age or older who have had 3 or more
normal Pap tests in a row may choose to stop having
cervical cancer screening. For women over 30, some
doctors recommend testing every 3 years with a
conventional Pap test plus the human papillomavirus DNA
test

28 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Breast cancer
Breast self-examination Consider monthly self-examinations after age 20
Breast physical
examination by health
care provider
Every 3 years between ages 20 and 39, then yearly
Mammography Yearly, starting at age 40
*Recommendations for screening are influenced by many factors. These screening
recommendations are for asymptomatic people with an average risk of cancer. For
people with a higher risk, such as those with a strong family history of certain cancers or
those who have had a previous cancer, screening may be recommended more
frequently or to start at a younger age. Screening tests other than those listed here may
also be recommended. Furthermore, other organizations, such as the U.S. Preventive
Services Task Force, may have slightly different recommendations. A person's
physician can help the person decide when to begin screening and which tests should
be used.
†The combination of yearly stool examination for occult blood and sigmoidoscopy every
5 years is preferred over either of these options alone.
Diagnostic Tests and Staging Diagnosis
Usually, when a doctor first suspects cancer, some type of imaging study, such as x-ray,
ultrasonography, or computed tomography (CT), is performed. For example, a person with
chronic cough and weight loss might have a chest x-ray; a person with recurrent headaches
and trouble seeing might have a CT scan or magnetic resonance imaging (MRI) of their
head. Although these tests can show the presence, location, and size of an abnormal mass,
they cannot confirm that cancer is the cause. Cancer is confirmed by finding cancer cells on
microscopic examination of samples from the suspected area. Usually, the sample must be
a piece of tissue, although sometimes examination of the blood is adequate (such as in
leukemia). Obtaining a tissue sample is termed a biopsy. Biopsies can be performed by
cutting out a small piece of tissue with a scalpel, but very commonly the sample is obtained
using a hollow needle. Such tests are commonly done without the need for an overnight
hospital stay (outpatient procedure). Doctors often use ultrasonography or a CT scan to
guide the needle to the right location. Because biopsies can be painful, the person is
usually given a local anesthetic to numb the area.
In people with findings on examination or imaging tests that suggest cancer, measuring
blood levels of tumor markers may provide additional evidence for or against the diagnosis
of cancer. In people who have been diagnosed with certain types of cancer, tumor markers
may be useful to monitor the effectiveness of treatment and to detect possible recurrence of
the cancer. For some cancers, the level of a tumor marker drops following treatment and
increases if the cancer recurs

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 29
Selected Tumor Markers
Tumor Marker Description Comment About Testing
Alpha-
fetoprotein
(AFP)
Levels may be raised
in the blood of people
with cancer of the
colon. Blood levels
may also be elevated
in patients with other
cancers or
noncancerous
conditions.
Testing can be useful in diagnosing these
cancers and in monitoring treatment.
Beta-human
chorionic
gonadotropin
(ß-HCG)
This hormone is
produced during
pregnancy but also
occurs in women who
have a cancer
originating in the
placenta and in men
with various types of
testicular cancer.
Testing can be useful in diagnosing such
cancers and in monitoring treatment.
Beta2 (ß2)-
microglobulin
Levels may be raised
in people with multiple
myeloma or other
cancers of blood cells.
This test cannot be recommended for cancer
screening.
Calcitonin Produced by certain
cells in the thyroid
gland (C cells). Blood
levels elevated in
medullary thyroid
cancer.
May be used to monitor response to treatment
of medullary thyroid cancer.
Carbohydrate
antigen 125
(CA-125)
Levels may be
increased in women
with a variety of
gynecological
diseases, including
ovarian cancer.
This is not recommended for routine cancer
screening.

30 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Carbohydrate
antigen 19-9
(CA 19-9)
Levels may be
increased in people
with cancers of the
digestive tract,
particularly pancreatic
cancer.
This test cannot be recommended for cancer
screening.
Carbohydrate
antigen 27.29
(CA27.29)
Levels may be
increased in people
with breast cancer.
This test cannot be recommended for cancer
screening.
Carcinoembryo
nic antigen
(CEA)
Levels may be raised
in the blood of people
with cancer of the
colon. Blood levels
may also be elevated
in patients with other
cancers or
noncancerous
conditions.
After surgery for colon cancer, testing can be
useful in monitoring treatment and detecting
recurrence.
Lactate
dehydrogenase
Levels can be raised
for a variety of
reasons.
This test cannot be recommended for cancer
screening. However, it is useful in assessing
prognosis and monitoring treatment,
particularly for people with testicular cancer,
melanomas, and lymphomas.
Prostate-
specific antigen
(PSA)
Levels are raised in
men with
noncancerous
(benign) enlargement
of the prostate and
often are considerably
higher in men with
prostate cancer. What
constitutes a
meaningfully abnormal
level is somewhat
uncertain, but men
with an elevated PSA
level should be
evaluated further by a
doctor.
Testing can be useful in screening for cancer
and in monitoring its treatment.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 31
Thyroglobulin
Elevated blood levels
may occur in patients
with thyroid cancer or
benign thyroid
conditions.
This test cannot be recommended for routine
screening but may be helpful for monitoring
response to treatment of thyroid cancer.
*Because tumor markers can also be produced by noncancerous tissue, doctors generally
do not use them to screen healthy people. Exceptions may include PSA for prostate cancer
and AFP for patients at risk for hepatoma. In families with inherited medullary thyroid
cancer, a rare condition, calcitonin blood levels also may be a useful screening test.

32 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Staging
When cancer is diagnosed, staging tests help determine how extensive the cancer is in
terms of its location, size, growth into nearby structures, and spread to other parts of the
body. People with cancer sometimes become impatient and anxious during staging tests,
wishing for a prompt start of treatment. However, staging allows doctors to determine the
most appropriate treatment as well as helping to determine prognosis.
Staging may use scans or other imaging tests, such as x-ray, CT, MRI, bone scintigraphy,
or positron emission tomography (PET). The choice of staging test(s) depends on the type
of cancer, as different cancers involve different parts of the body. CT scanning is used to
detect cancer in many parts of the body, including the brain and lungs and parts of the
abdomen, including the adrenal glands, lymph nodes, liver, and spleen. MRI is of particular
value in detecting cancers of the brain, bone, and spinal cord.
Biopsies are often needed for staging and can sometimes be done together with the initial
surgical treatment of a cancer. For example, during a laparotomy (an abdominal operation)
to remove colon cancer, a surgeon removes nearby lymph nodes to check for spread of the
cancer. During surgery for breast cancer, the surgeon biopsies or removes lymph nodes
located in the armpit to determine whether the breast cancer has spread there; this
information along with features of the primary tumor helps the doctor determine whether
further treatment is needed. When staging is based only on initial biopsy results, physical
examination, and imaging, the stage is referred to as clinical. When the doctor uses results
of a surgical procedure or additional biopsies, the stage is referred to as pathologic. The
clinical and pathologic stage may differ.
In addition to imaging tests, doctors often obtain blood tests to see if the cancer has begun
to affect the liver, bone, or kidneys.
References
Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ, Eds. Cancer Management: A Multidisciplinary Approach. 11th ed. 2009.
The Basic Science of Oncology 4th ed. Tannock IF, Hill RP et al. (eds.) (2005). McGraw-Hill. ISBN 0-07138-774-9.
Principles of Cancer Biology. Kleinsmith, LJ (2006). Pearson Benjamin Cummings. ISBN 0-80534-003-3.
Parkin D, Bray F, Ferlay J, Pisani P (2005). "Global cancer statistics, 2002". CA Cancer J Clin 55 (2): 74–108. doi:10.3322/canjclin.55.2.74. PMID 15761078. http://caonline.amcancersoc.org/cgi/content/full/55/2/74.
Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. World Cancer Research Fund (2007). ISBN 978-0-9722522-2-5.
Cancer Medicine, 6th Edition—Textbook

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 33
Encyclopedia of Cancer—4 volume reference work Weinberg, Robert A. (September 1996). "How Cancer Arises; An explosion of research
is uncovering the long-hidden molecular underpinnings of cancer—and suggesting new therapies" (PDF). Scientific American: 62–70. http://www.bme.utexas.edu/research/orly/teaching/BME303/Weinberg.pdf. "Introductory explanation of cancer biology in layman's language".
"American Cancer Society". What We Do. http://www.cancer.org/docroot/AA/AA_2.asp?sitearea=AA&level=1.
The Merck Index, 18th Ed., 2006, editor M. Beers, Porter, N.J.: Merck&Co., Inc., p. 265, #1880.

34 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Rehabilitation Literature Review
Physical and psychological effects of exercise for cancer patients
As cancer rates continue to increase in all regions of the United States, so have the questions regarding improved treatment. One area of treatment that has been examined, but not fully implemented, is cancer rehabilitation. Measures of improved function, including the six-minute walk test and the SF-12 quality of life scale, indicate that rehabilitation, with associated patient education, provides a more comprehensive treatment of this population. Benefits have implications that cross boundaries of disease, treatment, and well-being. A review of literature highlights the effects of exercise for cancer survivors and illustrates the strengths of a monitored rehabilitation process.
Economic outcomes for cancer survivors during and after treatment
A multidisciplinary approach to oncology rehabilitation closely follows the guidelines set forth by cardiac and pulmonary rehabilitation. Therefore, cancer rehabilitation patients may realize similar outcomes. Typical economic outcomes from cardiopulmonary rehabilitation are fewer emergency department visits, lower re-hospitalization rates, decreased treatment interventions, and decreased duration per hospitalization. Program graduates typically return to work sooner, and remain actively employed longer. Patients may also experience a decrease in symptoms associated with the disease and the treatment. The goal of this review is to identify the effects of monitored exercise models and the outcomes for improved function, and patient perceptions of well-being. Physical activity should increase In a study of 32 patients with various types of cancers receiving high-dose chemotherapy, Dimeo (1999) concluded that cancer patients should not be instructed to rest, but should instead increase physical activity. Variables examined were physical function, cardiac function, fatigue, and hemoglobin concentrations. While both the control and the exercise groups showed improvement, the exercise groups‘ values were significantly statistically higher (p< .05) than those of the control group.
The Ottawa Regional Cancer Center (Segal et. al, 1999) supports these findings in their report of improved physical activity and function in a group of 254 participants. Half (50.4%) of the participants were undergoing active treatment with chemotherapy, radiation, or both. Nearly one-fourth of the participants had completed their cancer treatment more than six months previously. This finding indicated that rehabilitation needs do not disappear or diminish after completion of medical therapy. They noted that the multidimensional rehabilitation process appealed equally to patients who reported being active before diagnosis and those who reported being inactive before diagnosis. Aerobic exercise is noted in several studies to have positive effects on physical and psychological components of health-related quality of life. Courneya (2003) reported that exercise enhanced biopsychosocial mechanisms that underlie coping or self-efficacy, which may alleviate or prevent the occurrence of some of the symptoms of cancer and cancer treatments, decreasing their impact on activities of daily living. Similar outcomes were achieved in separate studies of supervised aerobic exercise using the cycle ergometer three times per week for 10-12 weeks. Physical functioning outcomes showed improvement in the 6- and 12-minute walk tests, and cycle and treadmill

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 35
tests. Participants also reported improvement in symptoms of nausea, depression, anxiety, sleep disturbances, fatigue, and emotional distress (McVicar et. al, 1989; Segal et. al, 2001; Winningham & McVicar, 1988). Fatigue Fatigue, described as lacking energy, feeling exhausted, being unable to concentrate, feeling lethargic and lacking motivation, and feelings of sleepiness, depression, and weakness (Winningham et al., 1994), is the most frequently reported symptom of cancer patients (Irvine, Vincent, Graydon, Bubela, & Thompson, 1994; King, Nail, Kreamer, Stohl, & Johnson, 1985). Exercise has been proven to alleviate levels of fatigue. Schwartz (1998) conducted a study of athletes who had cancer and found that exercise decreased the frequency, duration, and intensity of fatigue. In another study, Schwartz (2000) reported findings that women with stage II and stage III breast cancer who engaged in an 8-week, 15-30 minute aerobic exercise program four days per week had fewer days of severe fatigue with each cycle of chemotherapy as compared to non-exercisers. Cancer patients who exercised also reported an improved quality of life compared to non-exercising cancer patients. Mock and colleagues (2001) reported improved quality of life, increased physical functioning, and significantly less reports of fatigue and distress in a group of 52 women with stage I, II, or IIIa breast cancer who were receiving adjuvant chemotherapy or radiation. This group exercised 90 minutes per session for three days per week. Less active women in this group showed statistically significant decreases in reports of fatigue. Depression After fatigue, depression is the most frequently reported symptom of cancer survivors. Segar and associates (1998) reported an improvement in psychological well-being in 24 breast cancer patients. Subjects were randomly assigned to an exercise group, an exercise group with behavior modification, and a control group. The results of this study indicated a significant difference between the two exercise groups and the control group on measures of anxiety and depression. They concluded that moderate-intensity aerobic exercise is not only safe for cancer patients undergoing adjuvant therapies, but that symptoms of anxiety and depression can also be alleviated. Dimeo, et al. (1996), reported an improvement in psychological well-being in 59 cancer patients undergoing chemotherapy followed by autologous peripheral stem cell transplantation. Twenty-seven patients participated in a supervised exercise program while 32 patients were in the control group. Exercise included training on a supine bicycle ergometer for 30 minutes per day at 50% of their cardiac reserve during their hospitalization. Psychological distress and fatigue were measured using the Profile of Mood States (POMS) test and the Symptoms Checklist 90. The results showed decreased levels of fatigue and physical complaints with improvements in several values related to psychological distress. The group concluded that aerobic training during chemotherapy should be used to reduce fatigue and improve symptoms of psychological distress in people undergoing treatment for cancer. Contraindications for participation Contraindications for participation in an exercise program include uncontrolled and unstable cardiac disease, a recent change in disease status, recent stroke, uncontrolled hypertension, and coagulopathies. Any changes in disease status warrant further investigation by the physician and appropriate treatment before continuing exercise therapy (Segal et al, 1999).

36 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 37
Future Research With only a few exceptions, most of the research reviewed was performed with breast cancer survivors. While it appears that exercise is safe and effective for this population, further research is necessary to determine safe participation for other types of cancer. All of these studies provided results for cancer patients during and after cancer treatment. One area of focus that was not revealed in literature is supervised exercise prior to the initiation of cancer treatment. One measure that could provide valuable insight is whether improvement of symptoms and decreased interruption of medical therapy would be evident. It was suggested that the ability to perform activities of daily living (ADL) could be improved but not directly measured. An investigation of the correlation between exercise and improved performance of ADL‘s could provide information about this phenomenon. Conclusions The American Cancer Society (Brown et al., 2003) evaluated multiple research projects to determine evidence of best practices related to optimal nutrition and physical activity for cancer patients. They recommend that adults adopt a physically active lifestyle that includes 30 minutes of activity 5 days per week. Aerobic training can be safely used during chemotherapy and radiation treatments to relieve symptoms of fatigue, anxiety, and depression. Exercise promotes physical function and may improve performance of self-care. Supervised exercise can also be considered a valuable component of palliative care for people diagnosed with cancer who are seeking improved quality of life and extended survival.
The use of individualized exercise prescriptions are based on guidelines developed by the American College of Sports Medicine (American College of Sports Medicine Position Stand: Exercise and physical activity for older adults, 1998). These guidelines have proven safe for older adults as well as cardiac and pulmonary disease populations. All of the reviewed literature appears to have followed these guidelines, and as such can be considered safe for cancer patients.

38 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
References American College of Sports Medicine Position Stand: Exercise and physical activity for older
adults. (1998). Medicine and Science in Sports Exercise, 30(6), 992-1008. Brown, J.K., Byers, T., Doyle, C., Courneya, K.S., Demark-Wahnefried, W., Kushi, L. H., et al.
(2003). Nutrition and physical activity during and after caner treatment: an American Cancer Society guide for informed choices. CA Cancer J Clin, 53, 268-291. Retrieved March 19, 2006, from http://caonline.amcancersoc.org/cgi/content/abstract/53/5/268.
Courneya, K.S. (2003). Exercise in Cancer Survivors: An Overview of Research. Medicine and Science in Sports and Exercise, 35 (11), 1846-1852.
Dimeo, F., Bertz, H., Finke, J., Fetscher, S., Mertelsmann, R., & Keul, J. (1996). An aerobic exercise program for patients with haematological malignancies after bone marrow transplantation. Bone Marrow Transplant, 18 (6), 1157-1160.
Dimeo, F., Stieglitz, R., Novelli-Fischer, R., Fetscher, S., & Kuel, J., (1999). Effects of physical activity on the fatigue and psychological status of cancer patients during chemotherapy. Cancer, 85 (10), 2273-2277.
Irvine, D., Vincent, L., Graydon, J. E., Bubela, N., & Thompson, L. (1994). The prevalence and correlates of fatigue in patients receiving treatment with chemotherapy and biotherapy: A comparison with the fatigue experienced by healthy individuals. Cancer Nursing, 17(5), 367-378.
King, K., Nail, L., Kreamer, K., Strohl, R., & Johnson, J. (1985). Patient's descriptions of the experience of receiving radiation therapy. Oncology Nursing Forum, 12(4), 55-61.
MacVicar, M., Winningham, M., & Nickel, J. (1989). Effects of aerobic interval training on cancer patients' functional capacity. Nursing Research, 38(6), 348-351.
Mock, V., Pickett, M., Ropka, M.E., Muscari, E., Stewart, K.J., Rhodes, V.A. et al. (2001). Fatigue and quality of life outcomes of exercise during cancer treatment. Cancer Practice, 9(3), 119-27.
Schwartz, A. L. (1998). Patterns of exercise and fatigue in physically active cancer survivors. Oncology Nursing Forum, 25(3), 485-491.
Schwartz, A. L. (2000). Exercise and weight gain in breast cancer patients receiving chemotherapy. Cancer Practice, 8(5), 231-237.
Segal, R., Evans, W., Johnson, D., Smith, J., Colletta, S. P., Corsini, L. et al. (1999). Oncology rehabilitation program at the Ottawa Regional Cancer Centre: program description. CMAJ: Canadian Medical Association Journal, 161, (3), 3820-3946.
Segal, R., Evans, W., Johnson, D., Smith, J., Colletta, S.P., Gayton, J.,et al. (2001). Structured exercise improves physical functioning in women with stages I & II breast cancer: Results of a randomized controlled clinical trial. Journal of Clinical Oncology, 19(3), 657-665.
Segar, M.L., Katch, V.L., Roth, R.S., Garcia, A., Portner, T., Glickman, S. et al. (1998). The effect of aerobic exercise on self-esteem and depressive and anxiety symptoms among breast cancer survivors. Oncology Nursing Forum, 25(1), 107-113.
Winningham, M., & McVicar, M. (1988). The effect of aerobic exercise on patient reports of nausea. Oncology Nursing Forum, 15(4), 447-450.
Winningham, M, Nail, L., Burke, M., Brophy, L., Cimprich, B., Jones, L. S. et al. (1994). Fatigue and the cancer experience: The state of the knowledge. Oncology Nursing Forum, 21, 23-36.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 39
Lab Test Educator
LAB DATA: Check Hematocrit, Hemoglobin, WBC & Platelet Values.
Blood Count Normal Values
“NO” “EXERCISE”
Light Exercise
Regular Exercise
Hematocrit Females:
Males:
37% to 47%
40% to 50%
<25%
>25%
>25%
Hemoglobin Females:
Males:
12-16 g/dl.
14 to 18 g/dl.
<8 g/dl.
8-10 g/dl.
>10 g/dl.
WBC 4,000 to 10,000/mm3
<500/mm3 >500/mm3 >500/mm3
Platelets 200,000 to 400,000/mm3
<5,000/mm3 5,000 to 10,000/mm3
10,000/mm3

40 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Complete Blood Count Chart

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 41
Contraindications to Physical Exercise Following Cancer Diagnosis
Complication Precaution Complete blood counts: Hemoglobin <8.0 g/dL
Avoid high-intensity or other activities that require significant oxygen transport
Absolute neutrophil count <0.5 X 109/μL Avoid activities that may increase risk of bacterial infection (eg, swimming)
Platelet count <50 X 109/L Avoid activities that increase risk of bleeding (eg, contact sports or high-impact exercises)
Fever >38°C (100.4°F) May indicate systemic infection and should be investigated. If patients are neutropenic, they should avoid exercise altogether. Patients without neutropenia should avoid high-intensity exercise if fever is >38°C, and avoid all exercise if fever is >40°C
Ataxia, dizziness, peripheral sensory neuropathy
Avoid activities that require significant balance and coordination (eg, treadmill exercises)
Severe cachexia (loss of >35% of premorbid weight)
Loss of muscle mass usually limits exercise to mild intensity, depending on degree of cachexia
Dyspnea Investigate etiology; exercise to tolerance
Bone metastases or pain Avoid activities that increase risk of fracture at the location of the bone pain or metastases (eg, contact sports or high-impact exercises)
Severe nausea Investigate cause; exercise to tolerance Extreme fatigue or muscle weakness Exercise to tolerance Severe lymphedema Avoid upper-extremity exercises with
affected arm Dehydration Ensure adequate fluid intake, be mindful
of co-morbidities such as CHF with a fluid restriction
42 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Exercise Precautions and Contraindications
People undergoing treatment for cancer and survivors of cancer may have disease or treatment-specific obstacles to exercise training. The side effects of anti-cancer therapy are often permanent; amputations cause permanent disability; radiation and chemotherapy can cause permanent scar formation in the joints, the lung, and the heart tissues; and drug-induced cardiomyopathies usually cause a permanent limitation on cardiovascular function. Many cancer survivors can reap rewards from exercise training, because many of the benefits occur in skeletal muscle and in psychological status.
The usual precautions and contraindications for exercise should be followed. The following are the absolute and relative indications for terminating an exercise test or an exercise session as defined by the ACSM (2005).
Absolute Contraindications
Relative Contraindications
Special Prescriptive Conditions
No exercise until condition is treated, stable, or past the acute phase.
Exercise ability is based on the individual's condition. Exercise may be restricted or require medical supervision
Exercise training may require medical monitoring, special limitations, or special exercises.
Cardiovascular
Aortic aneurysm Aortic stenosis (severe) Congestive heart failure Crescendo angina Myocardial infarction (acute) Myocarditis (active or recent Pulmonary or systemic embolism (acute) Thrombophlebitis Ventricular tachycardia or other dangerous dysrhythmias
Aortic stenosis (moderate) Subaortic stenosis (severe) Marked cardiac enlargement Supraventricular dysrhythmias Ventricular ectopic activity Ventricular aneurysm Hypertension (uncontrolled) Hypertrophic cardiomyopathy Compensated congestive heart failure
Aortic or pulmonary stenosis Mild angina * Post acute infarct Cyanotic heart disease Shunts Conduction disturbances Dysrhythmias-controlled Fixed-rate pacemakers Intermittent claudication Hypertension
Infections Acute infectious diseases
Subacute, chronic, recurrent infectious diseases
Chronic infections HIV

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 43
Indications for Terminating a Therapy Session
Absolute
A drop in systolic blood pressure (10 mm. Hg. from baseline despite increases in workload, when accompanied by other indications of ischemia)
Moderate to severe angina Increasing nervous system symptoms (i.e. ataxia, dizziness or near syncope) Signs of
poor perfusion (cyanosis or pallor) Sustained ventricular tachycardia ST segment elevation (1mm.) in leads without
diagnostic Q waves (other than V1 or a VR) Technical difficulty monitoring the ECG or systolic blood pressure Subject's desire to
stop
Relative
Drop in diastolic blood pressure (10 mm. Hg.) ST or QRS changes such as excessive ST segment depression (less than 2 mm.
horizontal or down-sloping ST segment depression) or marked axis shift Arrhythmias other than sustained ventricular tachycardia, including multifocal PVC's,
triplets of PVC's, supraventricular tachycardia, heart block, or brady arrhythmias Development of bundle branch block or intraventricular conduction delay that cannot
be distinguished from ventricular tachycardia Hypertensive response (Systolic > 250 mm. Hg., Diastolic > 115 mm. Hg.) Increasing chest pain Fatigue, shortness of breath, wheezing, leg cramps or claudication
(ACSM, Guidelines for Exercise Testing and Prescription, 6th Ed., 2005, Chapter 5, p. 104, Box 5-3)
In addition to the above general guidelines, certain precautions and contraindications are specific to cancer patients and should be noted and monitored:
Monitoring physiologic responses (e.g., vital signs) to exercise is important in the immunosuppressed population. Watch closely for early signs of cardiopulmonary complications of cancer treatments, such as dyspnea, pallor, sweating, and fatigue during exercise. Patients should always monitor their pulse rate, breathing frequency, blood pressure and, when warranted, use pulse oximetry.
The Rate of Perceived Exertion (RPE) should not exceed 3 to 4 for moderate intensity training or submaximal testing.
Current guidelines recommend that patients should be advised not to exercise within two hours of chemotherapy or radiation therapy as increases in circulation may increase the effects of the treatments (Gerber, 2000).
People with cancer are advised to contact their physician if any of the following abnormal responses develop:
o Fever o Extreme or unusual tiredness or unusual muscular weakness o Irregular heartbeat, palpitations, or chest pain

44 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
o Leg pain or cramps, unusual joint pain, unusual bruising or nosebleeds o Sudden onset of nausea during exercise o Rapid weight loss, severe diarrhea or vomiting o Disorientation, confusion, dizziness, lightheadedness, blurred vision, or fainting o Pallor or gray-colored appearance o Night pain, or pain not associated with an injury
The activity level of someone with anemia also may require adjustments in exercise intensity and duration due to increases in pulse and respiratory rates from hypoxia leading to fatigue with minimal exertion. Interval exercise or bedside exercise programs should be performed during frequent but short sessions throughout the day and may be the only treatment possible in this circumstance.
It is important to monitor the hematological values in patients receiving these cancer treatments. The PT must review these values before any type of vigorous exercise or activity is initiated.
The following table is a helpful guideline to indicate when aerobic exercise may need to be re-examined in chemotherapy patients:
LAB DATA: Check the Pt’s Hematocrit, Hemoglobin, WBC & Platelet Values.
Blood Count Normal Values
“NO” “EXERCISE”
Light Exercise
Regular Exercise
Hematocrit Females:
Males:
37% to 47%
40% to 50%
<25%
>25%
>25%
Hemoglobin Females:
Males:
12-16 g/dl.
14 to 18 g/dl.
<8 g/dl.
8-10 g/dl.
>10 g/dl.
WBC 4,000 to 10,000/mm3
<500/mm3 >500/mm3 >500/mm3
Platelets 200,000 to 400,000/mm3
<5,000/mm3 5,000 to 10,000/mm3
10,000/mm3
(From Sayre & Marcoux, 1992; Pfalzer, 1988; Winningham, 1986) Exercise intensity determined by training heart rate may be difficult to use as some
people have inappropriate heart rate responses to exercise and large physiologic changes on a day-to-day basis from the disease, the treatments, or changes in medications.
Exercise intensity can be guided by heart rate response based on VO2 or metabolic equivalent (MET) levels along with monitoring of blood pressure, heart rate and rhythm, and Borg's rating of perceived exertion scale (RPE) (Pfalzer, 1987).

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 45
Compromised skeletal integrity may prevent weight-bearing activities. Non-weight-bearing aerobic activities, which may be utilized for people with bone and joint disease, include cycling, rowing, and swimming [water activities may not be appropriate for the immunosuppressed, and people with severe muscular weakness may tolerate cycling better than ambulation] (Pfalzer, 1987).
Energy-conservation techniques and work simplification may be necessary for the person with chronic fatigue and for those whose functional status is declining. Therapeutic exercise can be scheduled during periods when the person has the highest level of energy. Interval exercise may be preferred at first, with work-rest intervals beginning at the person's level of tolerance. This may include 1 minute of exercise activity followed by 1 minute of rest, then 1 minute of exercise, and so on. As the person's endurance level increases, the duration of work may be increased while the interval of rest declines.
Special patient concerns
1. Ataxia, dizziness, peripheral sensory neuropathy 2. Cachexia / malnutrition ( loss of >20% of premorbid weight) 3. Dyspnea (Shortness of breath) 4. Bone pain 5. Nausea 6. Diarrhea 7. Dehydration 8. Fatigue or muscle weakness 9. Lymphedema 10. Anemia (deficiency of hemoglobin) 11. Neutropenia (low WBC number) 12. Thrombocytopenia (low platelet count) 13. Pericarditis (inflammation of fibrous sac surrounding the heart) 14. Cardiomyopathy (deteriorated function of the myocardium) 15. Pulmonary Fibrosis (lungs become inflamed and scarred) 16. Depression, anxiety.
The above conditions are a continual consideration of ongoing assessment and adjustment in terms of contraindication, precaution and therapeutic exercise intervention adjustments. Through subjective and objective evaluations at the start of the therapeutic exercise session, appropriate adjustments are made to the therapeutic session.

46 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Rehabilitation Patient Assessment Form
Patient Information
Name: _______________________________________Date:_____________________
Address: ___________________________________Phone:______________________
Emergency Contact: __________________________Phone:_____________________
Age: _____Sex:_____Occupation:_______________Retired:_______Disabled:______
Height: _____________Weight:________Marital Status: ________________________
Insurance Provider: _____________Sessions Allowed:__________________________
Diagnosis:_________________________________Date of RX:___________________
Referring Physician:__________________ Primary Care Physician:________________
Cancer Data
Type of Cancer: ________________________________________________________
Specific Location :______________________________( left / right breast, brain, etc.)
Cancer surgery: Y: N: Type of surgery:______________________________________
Date(s) of Surgery:______________________________________________________
Presenting symptoms (Circle all that apply.)
Physical Fatigue, Cognitive Fatigue-(Chemo-Brain), Pain, Nausea, Mouth Sores,
Constipation, Diarrhea, Sleep Disturbance, Lymph edema, Peripheral Neuropathy,
Osteoporosis, Heart Disease.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 47
Post surgery and/or anti-cancer treatment type (Circle all that apply.)
Chemotherapy, Radiation, and/or Immunotherapy
Start of Treatment:_______________________________________________________
Date of final treatment:____________________________________________________
Complications; (infection, recurrence):________________________________________
Current medical concerns due to cancer:______________________________________
______________________________________________________________________
Allergies & Hospital History
Food Allergies: _______________Medication Allergies:__________________________
# of hospitalizations in past year:_________ # of days in hospital:__________________
Physical Limitation (sensory, stroke, surgeries) ________________________________

48 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Body Composition
Equipment used for this assessment includes a skinfold caliper. Take three measurements at the specified sites, then average measurements and total the averages for a score. 7 Site Skinfold:
Chest________________________________________________________
Triceps_________________________________________________________
Subscapular____________________________________________________
Axilla________________________________________________________
Suprailiac_____________________________________________________
Abdomen______________________________________________________
Thigh_________________________________________________________
TOTAL AVERAGES:
PRE:_______________________________POST:________________________________

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 49
Sleep Hygiene
#Hours: _______Pillows Used: _________Sleep Disturbances: _________What Kind: __________
Do You Snore: ________does your spouse say you snore? __________
Do you wake up to breathe? Y/N __________
Do you need to take naps daily? ___________
Do you take medication to help you sleep? __________________
Activities of Daily Life
Are you able to care for yourself? ________________________________________
Are you able to care for your home?______________________________________
Do you exercise? Y/N Type of Exercise & How Often:__________________________
Do you have exercise equipment? Y/N Type:________________________________
Special Interests & Hobbies:______________________________________________
Does cancer keep you from your activities?_________________________________
Do you live alone? _______do you have transportation?______________________
Do you need assistive devices?___________________________________________
Dietary History
Do you have trouble eating? Y/N Why?______________________________________
Do you have difficulty gaining or losing weight?______________________________
Special Diet? ____________________________________________________________
Appetite: Good______Fair______Poor_____Is this usual for you?_________________
Vitamins: Y/N Restaurants Per Week? ________________________________________
Do you consume alcohol: Y/N How Much? ____________________________________
Smoke Cigarettes: Y/N How Many? __________________________________________
Pack Years: One pack year is defined as 20 manufactured cigarettes (one pack) smoked per day
for one year. 1 pack per day x 26 years = 26 pack years.

50 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Psych Psychosocial assessment
Present Temperament: score each temperament from (1 to 10) (1=LOW) (10=HIGH).
(Angry, Worried, Sad, Impatient, Frustrated, Depressed, Anxious, Calm, Content, Cheerful, Happy)
(____)(_____)(____)(______)(_______)(________)(_____)(____)(______)(______)(_____)
Stressors / Fears /Concerns: _______________________________________________
Relaxation Techniques You Use:____________________________________________
You‘re most difficult adjustment since cancer?________________________________
Do you forget often? Y/N do you have a support system? Y/N Who?_____________
Do you understand your diagnosis? _________________________________________
Medical History
(Check ALL spaces below that apply to the patient, explain and date.)
_____Rheumatic fever / heart murmur________________________________________
_____High blood pressure_________________________________________________
_____Chest discomfort____________________________________________________
_____Heart abnormalities (racing, skipping beats)_______________________________
_____Abnormal ECG______________________________________________________
_____Heart Problems______________________________________________________
_____Coughing up blood___________________________________________________
_____Stomach or intestinal problems_________________________________________
_____Anemia____________________________________________________________
_____Stroke_____________________________________________________________
_____Sleeping problems___________________________________________________
_____Migraine or recurrent headaches________________________________________
_____Dizziness or fainting spells_____________________________________________

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 51
_____Leg pain after walking short distances__________________________________
_____Back/neck pain/injury_______________________________________________
_____Foot/ankle problems________________________________________________
_____Knee/hip problems__________________________________________________
_____Lymphedema______________________________________________________
_____High cholesterol____________________________________________________
_____Diabetes__________________________________________________________
_____Thyroid problems___________________________________________________
_____Lung disease______________________________________________________
_____Respiratory problems/asthma__________________________________________
_____Chronic or recurrent cough____________________________________________
_____Disease of arteries__________________________________________________
_____Increased anxiety / depression_________________________________________
_____Recurrent fatigue___________________________________________________
_____Arthritis___________________________________________________________
_____Swollen/stiff/painful joints_____________________________________________
_____Epilepsy___________________________________________________________
_____Vision/hearing problems_______________________________________________
Physical Assessment
1. Range Of Motion: _______________________________________________________
2. Strength: 1RM / 3RM, ____________________________________________________
3. Functional Capacity / Independence: 6 Minute Walk Test.
PRE: Distance:________Time:________HR:________RPE:________DYSP/FTg:_______
POST:Distance:________Time:________HR:________RPE:________DYSP/FTg:_______

52 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Patient Goal Setting
List the Short Term Goals on Lines 1 – 3 for Cancer Rehabilitation.
List the Long Term Goals for the Patient‘s Quality of Life on Lines 4 – 5.
1. _____________________________________________________________________
2. _____________________________________________________________________
3. _____________________________________________________________________
4. _____________________________________________________________________
5. _____________________________________________________________________
Additional Notes
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
Therapist:__________________________________________ Date:________________

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 53
Common Goals for Cancer Patients
1. Pt will begin balance/proprioception training to overcome the chemotherapy induced peripheral neuropathy, 2. achieving a 41 on the Berg Balance Scale in order to independently drive to the grocery store to pick up necessary 3. food items. 4. Pt will begin gait training to overcome the chemotherapy induced peripheral neuropathy and foot drop deficiencies 5. by achieving an independence score on the Tinetti Gait Instrument in order to safely navigate the sidewalk while 6. taking the trach out to the curb. 7. Pt will take part in cancer symptom management lessons in order to control cancer treatment side-effects which 8. deteriorate function. With this coping strategies development, pt will increase functional independence to ambulate 9. 500 feet to maintain the capacity for self care, driving to doctors appointments and to receive cancer treatments. 10. Pt will be independent with pursed lip breathing to prevent anxiety attacks while maintaining blood oxygen saturations 11. above 90 % Sp02 12. Pt will be independent ambulating 600 feet in order to walk to and in the church building. 13. Pt will increase LE Strength from 3/5 to 4/5 to stand up from commode. 14. Pt will increase UE strength from 2/5 to 3/5 in order to reach shower head for adjustment. 15. Pt will increase ambulation from 200 feet to 400 feet to increase pt‘s walking capability to reach the garage. 16. Pt shall strengthen LE from 2/5 to 4/5 from a seated to standing position that results in pt‘s ability to navigate 17. stairs in home. 18. Pt seeks LE & UE strength increase from 1/5 to 3/5 to pick up laundry basket and set it on table. 19. Pt seeks UE strength increase from 1/5 to 2/5 to enable hair dressing, an over the head strength requirement. 20. Pt seeks an ambulation functional increase from 200 feet to 500 feet that produces the capacity to use public 21. transportation in order to attend doctor‘s appointments. 22. Pt shall increase walking and standing capacity from 1.5 MET to 3.0 MET in order to clean kitchen and cook meals. 23. Pt shall seek UE & LE strength and balance gains from 3/5 to 4+/5 to safely walk to and operate the riding lawn 24. mower. 25. Pt shall increase function from 1.5 MET to 2.0 MET to restore self care tasks of toileting, bathing, & dressing. 26. Pt will increase abdominal strength from 1/5 to 3/5 to support abdominal breathing patterns for increased control 27. of shortness of breath and oxygenation in order to overcome lung cancer breathing difficulties. 28. Pt seeks balance increases lost to corticosteroid-induced muscle wasting to reduce falls-risks and to safely 29. navigate stairs. 30. Pt seeks strength gains lost to corticosteroid-induced muscle wasting to reduce falls risk and stand up from chairs. 31. Pt shall gain UE ROM over head from ___degrees to___degrees to reach food items from upper shelves.

54 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Writing Functional Goals
Principle
Functional capacity and the writing of functional goals must relate to activities of daily living for rehabilitation outcome relevance. Goal setting must be a partnership, where the therapist and the patient work together to establish functional short term and outcome goals. Goal setting takes place during the initial evaluation and is documented on the 700/701.
Each therapist needs to identify how they will reach the patients goals in measurable, objective, and functional terms. Ask yourself, ―Are the goals measurable, objective, or functional?‖ With goals established, the therapist may refer to ‗The Compendium of Physical Activities Tracking Guide‘.
Look up the functional goal and record the MET work load required to perform the goal. For example:
―pt will care for home chores such as vacuum floors, fix meals, take the trash out, make
the bed, and clean the tub w/o assistance‖
Look the functional task up in the Compendium.
See a sample of the Compendium on the next page.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 55
MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT 2.5; home activities; multiple household tasks in general, light effort
2.5; home activities; cleaning, dusting, changing linen, taking out trash
2.3; home activities; wash dishes - standing
2.5; home activities; wash dishes; clearing dishes from table – walking
2.0; home activities; cooking or food preparation - general
2.5; home activities; serving food, setting table - walking or standing
2.5; home activities; cooking or food preparation – walking
2.5; home activities; feeding family pet, cat, dog, small animals
2.5; home activities; putting away groceries, carrying groceries
2.3; home activities; food shopping, standing or walking
2.3; home activities; non-food shopping, standing or walking
2.3; home activities; ironing
2.0; home activities; implied standing - laundry, fold or hang clothes
2.0; home activities; making bed
2.5; home activities; watering plants
2.5; home activities; building a fire inside
3.5; home activities; vacuuming
Achieving the desired goals requires a functional capacity of 3.5 MET. However, the patient at the time of evaluation or start of the program demonstrated a functional capacity of 2.0 MET. Therefore, therapists must define the methods which will progress the patient to the desired functional goals. This is called the plan of care, plan of treatment or an exercise prescription. This methodology is documented in the Tx Justification on the 700/710.

56 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Purpose
Physical and Occupational Therapists are required to document patient outcomes
on the Department of Health and Human Services Plan of Treatment, 700 & 701,
etc. Human physiological outcomes at rest and during activity are well known,
translating measurements (MET) allows therapists to applying scientific principles
to the assessment of everyday functional capacity. The validity of metabolic equivalents
(MET) and it‘s relationship to functional capacity or physical activity is central to the
Compendium of Physical Activities Tracking Guide. The Compendium was developed
for use in epidemiologic studies to standardize the assignment of (MET) intensities in
physical activity. The Compendium has been used in studies worldwide to assign
intensity units (MET) to physical activity and to develop innovative ways to assess
energy expenditure in physical activity.
Procedure
Knowing where to find (MET) provides the therapist with validated information for this
(MET) to Functional Capacity translation method.
Most aerobic exercise equipment includes an instrument panel
for test, measurement and control. This panel will be the source
of (MET) or (Kcal) measurement during therapeutic exercise.
Take the time to locate the (MET) / (Kcal) read out display
The conversion method consists of taking the (MET) data from
the instrument panel just before ending steady state exercise,
take the (MET) value and compare it to the physical activity
tracking guide to reveal equivalent functional tasks.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 57
For example, If one walks on the tread mill for 15 minutes at 3.0 (MET)s, one can reasonably perform any 3.0 (MET) task listed in The Compendium of Physical Activities Tracking Guide for 15 minutes.

58 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
The Compendium of Physical Activities Tracking Guide
MET LEVEL / CATAGORY / FUNCTIONAL TASK EQUIVALENT
1 to 2 MET LEVEL 0.9; inactivity; quiet sleeping 1.5; home activities; reclining with baby 1.0; inactivity; lying quietly, watching television 1.0; inactivity; lying quietly, doing nothing, lying in bed awake 1.0; inactivity; sitting quietly and watching television 1.0; inactivity; sitting quietly, sitting smoking, listening to music 1.2; inactivity; standing quietly (standing in a line) 1.0; inactivity; reclining in a chair - talking or talking on phone 1.0; inactivity; reclining in a chair – reading 1.0; inactivity; meditating 1.5; lawn and garden; watering lawn or garden, standing or walking 1.5; miscellaneous; sitting - card playing, playing board games 1.8; miscellaneous; sitting - writing, desk work, typing 1.8; miscellaneous; standing - talking or talking on the phone 1.5; miscellaneous; sitting - talking or talking on the phone 1.8; miscellaneous; sitting - studying, general, including reading - writing 1.8; miscellaneous; sitting - class, note-taking or class discussion 1.8; miscellaneous; standing – reading new paper waiting for bus 1.5; miscellaneous; sitting - arts and crafts, light effort 1.8; miscellaneous; standing - arts and crafts, light effort 1.5; miscellaneous; family reunion, genealogy, sitting, talking, eating 1.8; music playing; accordion 1.5; occupation; farming, milking by machine, light effort 1.3; occupation; police, riding in a squad car (sitting) 1.5; occupation; sitting - light office work, general 1.5; occupation; sitting meetings, general, and/or with talking involved 1.5; occupation; typing, electric, manual or computer 1.0; self care; sitting on toilet 1.5; self care; bathing (sitting) 1.5; self care; eating (sitting) 1.0; self care; taking medication, sitting or standing 1.0; self care; having hair or nails done by someone else, sitting 1.5; sexual activity; active, vigorous effort 1.3; sexual activity; general, moderate effort 1.0; sexual activity; passive, light effort, kissing, hugging 1.0; transportation; riding in a car or truck 1.0; transportation; riding in a bus 1.0; religious activities; sitting in church, attending a ceremony 1.5; religious activities; sitting in church, talking or singing 1.3; religious activities; sitting, reading religious materials at home 1.2; religious activities; standing in church (quietly), standing quietly 1.0; religious activities; kneeling in church/at home (praying) 1.8; religious activities; standing, talking in church 1.5; religious activities; eating at church

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 59
1.5; religious activities; typing, electric, manual, or computer 1.5; volunteer activities; sitting - meeting, general 1.5; volunteer activities; sitting - light office work, in general 1.5; volunteer activities; typing, electric, manual, or computer
2 to 3 MET LEVEL 2.5; conditioning exercise; stretching, hatha yoga 2.5; conditioning exercise; mild stretching 2.5; fishing and hunting; fishing from boat, sitting 2.0; fishing and hunting; fishing, ice, sitting 2.5; fishing and hunting; hunting, bow and arrow or crossbow 2.5; fishing and hunting; hunting, duck, wading 2.5; fishing and hunting; pistol shooting or trap shooting, standing 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen, taking out trash 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; non-food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside 2.0; home activities; standing - light (pump gas, change light bulb, etc.) 2.5; home activities; sitting-playing with children–light, only active periods 2.8; home activities; standing - playing with children – light, active periods 2.5; home activities; child care: sitting/kneeling - dressing, bathing 2.5; home activities; sit, playing with animals, light, only active periods 2.8; home activities; stand, playing with animals, light, only active periods 2.8; home activities; walk/run, playing w/animals, light, only active periods 2.5; lawn and garden; mowing lawn, riding mower 2.5; lawn and garden; walking, applying fertilizer or seeding a lawn 2.3; miscellaneous; standing - drawing (writing), casino gambling 2.0; miscellaneous; standing, with movement – miscellaneous 2.0; miscellaneous; sitting - arts and crafts, moderate effort 2.0; miscellaneous; touring/traveling/vacation involving walking and riding 2.5; miscellaneous; camping involving standing, walking, sitting 2.0; music playing; cello 2.5; music playing; conducting 2.0; music playing; flute (sitting) 2.0; music playing; horn 2.5; music playing; piano or organ 2.5; music playing; trumpet 2.5; music playing; violin

60 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
2.0; music playing; woodwind 2.0; music playing; guitar, classical, folk (sitting) 2.5; occupation; bakery, light effort 2.3; occupation; bookbinding 2.0; occupation; directing traffic (standing) 2.5; occupation; chambermaid, making bed (nursing) 2.5; occupation; custodial work - cleaning sink and toilet, light effort 2.5; occupation; custodial work - dusting, light effort 2.5; occupation; custodial work - vacuuming, light effort 2.0; occupation; farming, moving animals, driving, light effort 2.5; occupation; farming, driving harvester, cutting hay, open irrigation 2.5; occupation; farming, driving tractor 2.6; occupation; horse racing, walking speed 2.3; occupation; printing (standing) 2.5; occupation; police, directing traffic, shouting commands (standing) 2.0; occupation; police, driving a squad car (sitting) 2.5; occupation; shoe repair, general 2.5; occupation; sitting; moderate (riding mower/forklift, crane operation) 2.5; occupation; tailoring, cutting 2.5; occupation; tailoring, general 2.0; occupation; tailoring, hand sewing 2.5; occupation; tailoring, machine sewing 2.0; occupation; walking on job, less than 2.0 mph, very slow 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; sports; billiards 2.5; sports; croquet 2.5; sports; darts, wall or lawn 2.5; sports; football or baseball, playing catch 2.5; sports; horseback riding, walking 2.0; transportation; automobile or light truck (not a semi) driving 2.0; transportation; flying airplane 2.5; transportation; motor scooter, motorcycle 2.5; walking; bird watching 2.5; walking; pushing or pulling stroller with child or walking with children 2.0; walking; household walking from room to room 2.0; walking; walking, less than 2.0 mph, level ground, strolling, very slow 2.5; walking; walking, 2.0 mph, level, slow pace, firm surface 2.5; walking; walking from house to car or bus, from car or bus to go places 2.5; walking; walking to neighbor‘s house to socialize, visit, or teach 2.8; walking; walking, 2.5 mph, downhill 2.5; water activities; boating, power 2.5; religious activities; sitting, playing an instrument at church 2.0; religious activities; standing, singing in church, active participation 2.0; religious activities; walk/stand to usher for religious purposes

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 61
2.5; religious activities; serving food at church 2.0; religious activities; preparing food at church 2.3; religious activities; washing dishes/cleaning kitchen at church 2.5; religious activities; standing - moderate (lifting 50 lbs) 2.5; volunteer activities; sitting - moderate work 2.3; volunteer activities; standing - light work (filing, talking, assembling)
3 to 4 MET LEVEL 3.0; conditioning exercise; bicycling, stationary, 50 watts, very light effort 3.5; conditioning exercise; calisthenics, home exercise, general 3.5; conditioning exercise; rowing, stationary, 50 watts, light effort 3.0; conditioning exercise; weight lifting 3.0; dancing; ballroom, slow (e.g. waltz, foxtrot, slow dancing) 3.0; fishing and hunting; fishing, general 3.5; fishing and hunting; fishing from river bank, standing 3.3; home activities; carpet sweeping, sweeping floors 3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.0; home activities; cooking Indian bread on an outside stove 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors 3.0; home activities; carrying small children 3.0; home activities; child care: standing - dressing, bathing, grooming 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; home repair; wiring, plumbing 3.0; lawn and garden; riding snow blower 3.5; lawn and garden; trimming shrubs or trees, power cutter 3.0; lawn and garden; picking fruit off trees, picking fruits/vegetables 3.0; lawn and garden; walking/standing - picking up yard, light 3.0; lawn and garden; walking, gathering gardening tools 3.0; miscellaneous; standing - arts and crafts, moderate effort 3.5; miscellaneous; standing - arts and crafts, vigorous effort 3.5; music playing; trombone 3.0; music playing; guitar, rock and roll band (standing) 3.5; music playing; marching band, drum major (walking) 3.5; occupation; carpentry, general 3.0; occupation; custodial work - buffing the floor with electric buffer 3.5; occupation; custodial work - general cleaning, moderate effort 3.5; occupation; custodial work - mopping, moderate effort 3.0; occupation; custodial work - take out trash, moderate effort 3.0; occupation; custodial work - vacuuming, moderate effort 3.5; occupation; electrical work, plumbing work

62 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
3.5; occupation; farming, chasing cattle, non-strenuous (walking) 3.0; occupation; farming, milking by hand, moderate effort 3.5; occupation; locksmith 3.0; occupation; machine tooling, welding 3.0; occupation; standing; light/moderate, assemble/repair heavy parts 3.5; occupation; standing; moderate, assembling at fast rate, lifting 50 lbs 3.5; occupation; tailoring, weaving 3.3; occupation; walking on job, 3.0 mph, in office, moderate speed 3.8; occupation; walking on job, 3.5 mph, in office, brisk speed 3.0; occupation; walking, 2.5 mph, slowly and carrying 25 pounds 3.0; occupation; walking, gathering things at work, ready to leave 3.0; occupation; working in scene shop, theater actor, backstage employee 3.5; sports; archery (non-hunting) 3.0; sports; frisbee playing, general 3.0; sports; golf, miniature, driving range 3.5; sports; golf, using power cart 3.5; sports; horseback riding, saddling horse 3.0; sports; horseshoe pitching, quoits 3.0; sports; shuffleboard, lawn bowling 3.5; sports; trampoline 3.0; sports; volleyball, non-competitive 3.0; transportation; driving heavy truck, tractor, bus 3.5; walking; carrying infant or 15 pound load 3.0; walking; loading /unloading a car 3.0; walking; downstairs 3.0; walking; loading /unloading a car 3.0; walking; walking, 2.5 mph, firm surface 3.3; walking; walking, 3.0 mph, level, moderate pace, 3.8; walking; walking, 3.5 mph, level, brisk, firm surface 3.0; water activities; sailing, boat sailing, windsurfing, ice sailing, general 3.0; water activities; surfing, body or board 3.0; water activities; water volleyball 3.5; winter activities; snowmobiling 3.3; religious activities; walking, 3.0 mph, moderate speed 3.8; religious activities; walking, 3.5 mph, not carrying anything 3.0; religious activities; cleaning church
4 to 5 MET LEVEL 4.0; bicycling; bicycling, <10 mph, leisure, to work or for pleasure 4.8; dancing; ballet or modern, twist, jazz, tap, jitterbug 4.5; dancing; general 4.5; dancing; ballroom, fast (disco, folk, square), line dancing 4.0; fishing and hunting; digging worms, with shovel 4.0; fishing and hunting; fishing from river bank and walking 4.0; home activities; multiple household tasks all at once, vigorous effort 4.0; home activities; sweeping garage, sidewalk or outside of house 4.0; home activities; walk/run - playing with children – moderate 4.0; home activities; elder care, disabled adult, only active periods

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 63
4.0; home activities; walk/run, playing with animals, moderate 4.0; home repair; automobile body work 4.5; home repair; carpentry, finishing or refinishing cabinets or furniture 4.5; home repair; caulking, except log cabin 4.5; home repair; laying or removing carpet 4.5; home repair; laying tile or linoleum, repairing appliances 4.5; home repair; painting 4.5; home repair; sanding floors with a power sander 4.5; home repair; scraping and painting 4.5; home repair; washing fence, painting fence 4.5; lawn and garden; mowing lawn, power mower 4.5; lawn and garden; operating snow blower, walking 4.5; lawn and garden; planting seedlings, shrubs 4.5; lawn and garden; planting trees 4.3; lawn and garden; raking lawn 4.0; lawn and garden; raking roof with snow rake 4.0; lawn and garden; sacking grass, leaves 4.5; lawn and garden; trimming shrubs or trees, manual cutter 4.5; lawn and garden; weeding, cultivating garden 4.0; lawn and garden; gardening, general 4.0; music playing; drums 4.0; music playing; marching band, playing an instrument (walking) 4.0; occupation; bakery, general, moderate effort 4.0; occupation; custodial work – feathering arena floor, moderate effort 4.0; occupation; farming, chasing cattle or other livestock on horseback 4.0; occupation; farming, feeding small animals, milk bottle for calf, goat 4.5; occupation; farming, feeding cattle, horses 4.5; occupation; farming, hauling water for animals, general hauling water 4.5; occupation; forestry, sawing, power 4.0; occupation; forestry, weeding 4.5; occupation; furriery – raise mink for fur coats 4.0; occupation; machine tooling, tapping and drilling 4.0; occupation; masseur, masseuse, manual therapy (standing) 4.5; occupation; orange grove work 4.0; occupation; police, making an arrest, taking command (standing) 4.0; occupation; lifting items continuously, 10 – 20 lbs, with limited walking 4.0; occupation; tailoring, pressing, starching 4.0; occupation; walking, 3.0 mph, moderately and carrying 25 lbs 4.0; occupation; walking, pushing a wheelchair 4.5; occupation; walking, 3.5 mph, briskly and carrying 25 pounds 4.5; running; jogging on a mini-tramp 4.5; sports; badminton, social singles and doubles, general 4.5; sports; basketball, shooting baskets 4.0; sports; coaching: football, soccer, basketball, baseball, swimming, etc. 4.0; sports; curling 4.5; sports; golf, general 4.5; sports; golf, walking and carrying clubs 4.3; sports; golf, walking and pulling clubs 4.0; sports; gymnastics, general

64 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
4.0; sports; softball, officiating 4.0; sports; table tennis, ping pong 4.0; sports; tai chi 4.0; walking; pushing a wheelchair, non-occupational setting 4.0; water activities; swimming, treading water, moderate effort, general 5 to 6 MET LEVEL 5.5; conditioning exercise; health club exercise, general 5.0; dancing; aerobic, low impact 5.5; dancing; ballroom, dancing fast 5.0; fishing and hunting; hunting, general 5.0; home activities; maple syruping/sugar bushing 5.0; home activities; walk/run-playing with children–vigorous 5.0; home activities; walk/run, playing with animals, vigorous 5.0; home repair; caulking, chinking log cabin 5.0; home repair; cleaning gutters 5.0; home repair; hanging storm windows 5.0; home repair; painting the outside of the house 5.0; home repair; spreading dirt with a shovel 5.0; lawn and garden; carrying, loading or stacking wood 5.0; lawn and garden; clearing land, hauling branches 5.0; lawn and garden; digging sandbox 5.0; lawn and garden; digging, spading, filling garden with compost 5.0; lawn and garden; laying sod 5.5; lawn and garden; mowing lawn, general 5.5; lawn and garden; mowing lawn, walk, power mower 5.5; occupation; construction, outside, remodeling 5.5; occupation; farming, shoveling grain 5.0; occupation; forestry, ax chopping, (SLOW) 5.0; occupation; forestry, hoeing 5.0; occupation; walking, carrying objects about 25 to 49 pounds 5.0; sports; cricket (batting, bowling) 5.0; sports; softball or baseball, fast or slow pitch, general 5.0; sports; tennis, doubles 5.0; walking; using crutches 5.0; walking; walking, 4.0 mph, level, firm surface 5.0; walking; walking, grass track 5.0; water activities; snorkeling 5.5; winter activities; ice skating, moderate effort 5.0; winter activities; skiing, downhill, light effort
6 to 7 MET LEVEL 6.0; bicycling; 10-12 mph 6.0; fishing and hunting; fishing in stream, in waders 6.0; fishing and hunting; hunting, deer, elk, large game 6.0; fishing and hunting; hunting, pheasants or grouse 6.0; home activities; butchering animals 6.0; home activities; moving furniture, household items 6.0; home repair; carpentry, outside house, installing rain gutters 6.0; lawn and garden; chopping wood, splitting logs

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 65
6.0; lawn and garden; gardening with heavy power tools, tilling a garden 6.0; lawn and garden; mowing lawn, walk, hand mower 6.0; lawn and garden; shoveling snow, by hand 6.0; occupation; coal mining, general 6.0; occupation; farming, care of animals (grooming, brushing, shearing) 6.0; occupation; forestry, planting by hand 6.0; occupation; horse grooming 6.5; occupation; horse racing, trotting 6.5; occupation; truck driving, loading and unloading truck 6.0; occupation; using heavy power tools such jackhammers 6.0; sports; boxing, punching bag 6.0; walking; carrying 16 to 24 lb load, upstairs 6.0; walking; hiking, cross country 6.5; walking; marching, rapidly, military 6.0; walking; walking, 3.5 mph, uphill 6.3; walking; walking, 4.5 mph, level, firm surface 6.0; water activities; swimming, leisurely, not lap swimming, general
7 to 8 MET LEVEL 7.5; home activities; carrying groceries upstairs 7.5; home repair; carpentry, sawing hardwood 7.0; occupation; forestry, sawing by hand 7.0; occupation; masonry, concrete 7.0; running; jogging, general 7.0; sports; basketball, officiating 7.0; sports; racquetball, casual, general 7.0; sports; tennis, general 7.0; walking; backpacking
8 to 9 MET LEVEL 8.0; walking; up stairs 8.0; bicycling; bicycling, general 8.0; occupation; carrying heavy loads, such as bricks 8.0; occupation; farming, baling hay, cleaning barn, vigorous effort 8.0; occupation; fire fighter, hauling hoses on ground 8.5; occupation; shoveling, digging ditches 8.0; running; running, 5 mph (12 min/mile) 8.0; sports; basketball, game
9 to 10 MET LEVEL 9.0; walking; carrying load upstairs, general 9.0; home activities; moving household items upstairs, carrying furniture 9.0; sports; football, competitive 10.0; walking; carrying 50 to 74 lb load, upstairs

66 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
References:
Barbara Ainsworth, William Haskell, Arthur Leon, David Jacobs, Jr., Henry Montoye, James Sallis & Ralph Paffenbarger, Jr. Compendium of physical activities: classification of energy costs of human physical activities. Medicine and Science in Sports and Exercise 25: 71-80, 1993. Wasserman K, Hansen JE, Sue DY, Whipp BJ, Casaburi R. Principles of exercise testing and interpretation, 3rd ed. Baltimore: Lippincott Williams & Wilkins; 1999. Wasserman K. Cardiopulmonary exercise testing and cardiovascular health. Armonk, NY: Futura; 2002. Principles of Exercise Testing and Interpretation; Including Pathophysiology. Karlman Wasserman, James E. Hansen, Darryl Y. Sue, Brian J. Whipp, William W. Stringer, M.D. - 2005 - 585 pages Sue DY. Integrative cardiopulmonary testing: basis and application. Medicine, Exercise, Nutrition and Health 1994;3:32-35. Whipp BJ, Davis JA, Torres F, et al. A test to determine parameters of aerobic function during exercise. J Appl Physiol: Resp Environ Exerc Physiol 1981;50:217-221 Beaver WL, Wasserman K, Whipp BJ. A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol 1986;60:2020-2027 Cohen-Solal A. Cardiopulmonary exercise testing in chronic heart failure. In: Wasserman K, ed. Exercise gas exchange in heart disease. Armonk, NY: Futura Publishing Co, 1996:17-35. Hansen, JE, Wasserman, K (1996) Pathophysiology of activity limitation in patients with interstitial lung disease. Chest 109,1556-1576

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 67
Quick Reference (MET) to Functional Task Conversions
3.0; home activities; cleaning, wash car, wash windows, clean garage 3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, genera 3.5; home activities; vacuuming 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing - packing/unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; lawn and garden; riding snow blower 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; music playing; conducting 2.5; music playing; piano or organ 2.5; music playing; violin 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation - general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside
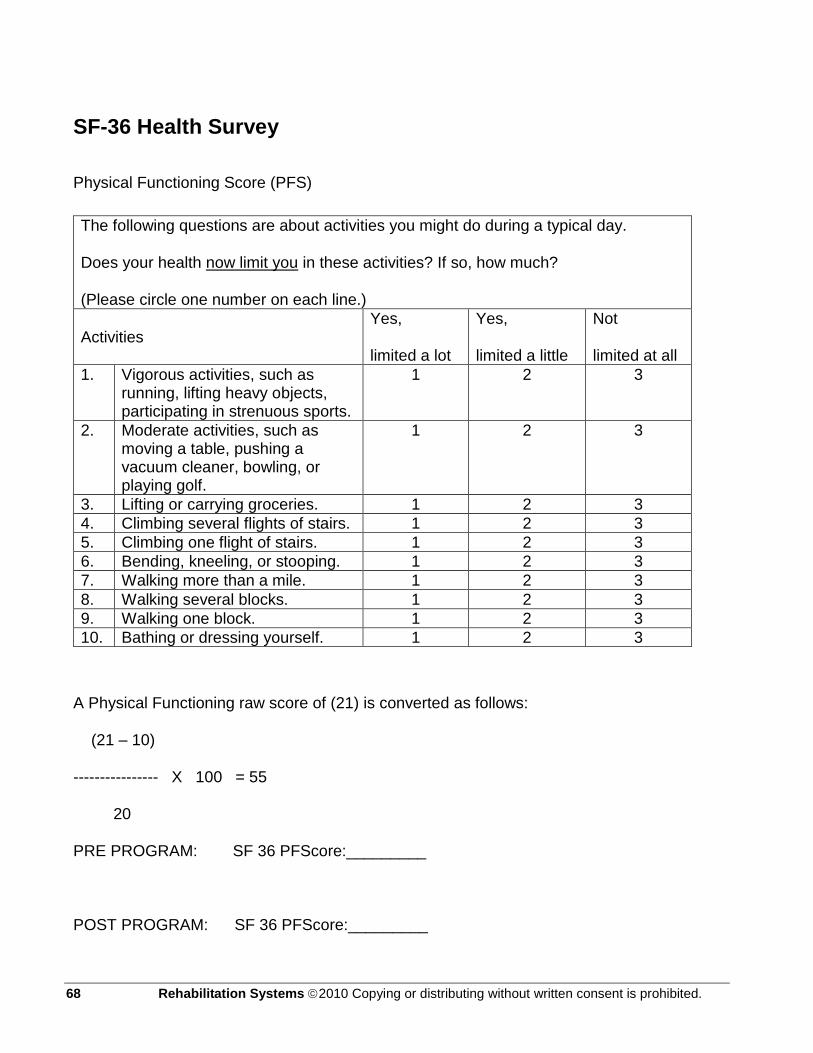
68 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
SF-36 Health Survey
Physical Functioning Score (PFS)
A Physical Functioning raw score of (21) is converted as follows:
(21 – 10)
---------------- X 100 = 55
20
PRE PROGRAM: SF 36 PFScore:_________
POST PROGRAM: SF 36 PFScore:_________
The following questions are about activities you might do during a typical day.
Does your health now limit you in these activities? If so, how much?
(Please circle one number on each line.)
Activities Yes,
limited a lot
Yes,
limited a little
Not
limited at all
1. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports.
1 2 3
2. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf.
1 2 3
3. Lifting or carrying groceries. 1 2 3
4. Climbing several flights of stairs. 1 2 3
5. Climbing one flight of stairs. 1 2 3
6. Bending, kneeling, or stooping. 1 2 3
7. Walking more than a mile. 1 2 3
8. Walking several blocks. 1 2 3
9. Walking one block. 1 2 3
10. Bathing or dressing yourself. 1 2 3

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 69
Health-Related Quality of Life Survey
SF-12v2™ Health Survey TO BE COMPLETED BY THE PATIENT
NAME ______________________________ DATE _______________
Directions: This survey asks for your views about your health. This information will help you keep track of how you feel and how well you are able to do your usual activities. If you are unsure about how to answer a question, please give the best answer you can. Mark only one answer for each question.
Excellent Very Good Good Fair Poor
1. In general would you say your health is:
The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much?
Yes, limited a lot
Yes, limited a
little
No, not limited at all
2. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf
3. Climbing several flights of stairs
During the past 4 weeks how much time have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
All the time Most of the time
Some of the time
A little of the time
None of the time
4. Accomplished less than you would like
5. Were limited in kind of work or other activities
During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling anxious or depressed)?
All the time Most of the time
Some of the time
A little of the time
None of the time
6. Accomplished less that you would like
7. Did work or activities less carefully than usual
8. During the past 4 weeks how much did pain interfere with your normal work (including both work outside the home and housework)?
Not at all A little bit Moderately Quite a bit
Extremely
These questions are about how you feel and how things have been during the past 4 weeks. Please give the answer that comes closest to how you have been feeling.
All the time Most of the time
Some of the time
A little of the time
None of the time
9. Have you felt calm and peaceful?
10. Did you have a lot of energy?
11. Have you felt downhearted and/or depressed?
12. How much of the time has your physical or emotional health interfered with social activities (like visiting with friends, relatives, etc.)?
Divide the total score: ______÷56 = __________ _____X5 _____X4 _____X3 _____X2 _____X1
www.rehabsys.com

70 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Therapist signature: ___________________________________ Date: ___________________
Department of Health and Human Services Healthcare Financing Administration
FORM HCFA-700 (11-91) Part A _______ Part B________ Other______
PLAN OF PROGRESS FOR REHABILITATION
(Complete for INITIAL CLAIMS ONLY)
1. Patient‘s LAST NAME
FIRST NAME M.I. 2. PROVIDER NUMBER 3. HICN
4. PROVIDER NAME 5. MEDICAL REC NUMBER (OPTIONAL)
6. ONSET DATE 7. SOC DATE
8. TYPE
□ Physical Therapy
9. PRIMARY DIAGNOSIS
Pertinent Medical DX)
10. TREATMENT DIAGNOSIS 11. Visits From SOC
12. PLAN of TREATMENT/FUNCTIONAL GOALS 13. Freq/Duration (3/wk X 4 wk)
GOALS (Short term)
OUTCOME (Long term)
PLAN Skilled services required:
1)
1) __Bed Mobility __Transfer training __Gait training __Balance re-ed __Therapeutic ex.
Specify OTHER:
__ROM Contracture mgmt. __W/C training __Muscle re-ed __Energy cons. Modalities
__Pt/caregiver training __Home program __Equipment needs __Safety skills __Other (specify)
2)
3)
2)
4)
5)
14. SIGNATURE
(professional establishing POC, including professional designation)
15. CERTIFICATION
FROM ______________ THROUGH_______________N/A ___________
16. I CERTIFY THE NEED FOR THESE SERVICES FURNISHED UNDER THIS PLAN OF TREATMENT AND WHILE UNDER MY CARE Physician signature: ____________________________________
Date: 17. ON FILE (print/type physician name)
18. INITIAL ASSESSMENT
age_____ M/F Rehab potential_______________
19. PRIOR HOSPITALIZATION ____________ to___________ N/A_____
20. HX and level of function at start of care:
21. 6-MINUTE WALK TEST ASSESSMENT
Min tolerated
Distance
Heart Rate
% spO2
RPE
Dyspnea
FiO2
22. Tx Justification:

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 71
Cancer Rehabilitation goal writing and documentation for the 700/701 forms:
Functional capacity and the writing of functional goals must relate to activities of daily living for
23. Signature (Or name of professional, including professional designation.) 24. Date
25. Service Dates
FROM _____________ THROUGH _____________

72 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
rehabilitation outcome relevance. Goal setting must be a partnership, where the therapist and the patient work together to establish functional short term and outcome goals. Goal setting is identifying realistic functional expectations with your patient. This process takes place during the initial evaluation and is documented on the 700 and 701 thereafter.
Each therapist needs to identify how they will reach the patients goals in measurable, objective, and functional terms. Ask yourself, are the goals: Measurable, objective, & functional ?
Cancer Rehabilitation Building Blocks for Writing Functional Goals

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 73
Pt will begin balance/proprioception training to overcome the chemotherapy induced peripheral neuropathy, achieving a 41 on the Berg Balance Scale in order to independently drive to the grocery store to pick up necessary food items. Pt will begin gait training to overcome the chemotherapy induced peripheral neuropathy and foot drop deficiencies by achieving an independence score on the Tinetti Gait Instrument in order to safely navigate the sidewalk while taking the trach out to the curb. Pt will take part in cancer symptom management lessons in order to control cancer treatment side-effects which deteriorate function. With this coping strategies development, pt will increase functional independence to ambulate 500 feet to maintain the capacity for self care, driving to doctors appointments and to receive cancer treatments. Pt will be independent with pursed lip breathing to prevent anxiety attacks while maintaining blood oxygen saturations above 90 % Sp02 Pt will be independent ambulating 600 feet in order to walk to and in the church building. Pt will increase LE Strength from 3/5 to 4/5 to stand up from commode. Pt will increase UE strength from 2/5 to 3/5 in order to reach shower head for adjustment. Pt will increase ambulation from 200 feet to 400 feet to increase pt‘s walking capability to reach the garage. Pt shall strengthen LE from 2/5 to 4/5 from a seated to standing position that results in pt‘s ability to navigate stairs in home. Pt seeks LE & UE strength increase from 1/5 to 3/5 to pick up laundry basket and set it on table. Pt seeks UE strength increase from 1/5 to 2/5 to enable hair dressing, an over the head strength requirement. Pt seeks an ambulation functional increase from 200 feet to 500 feet that produces the capacity to use public transportation in order to attend doctor‘s appointments. Pt shall increase walking and standing capacity from 1.5 MET to 3.0 MET in order to clean kitchen and cook meals. Pt shall seek UE & LE strength and balance gains from 3/5 to 4+/5 to safely walk to and operate the riding lawn mower. Pt shall increase function from 1.5 MET to 2.0 MET to restore self care tasks of toileting, bathing, & dressing. Pt will increase abdominal strength from 1/5 to 3/5 to support abdominal breathing patterns for increased control of shortness of breath and oxygenation in order to overcome lung cancer breathing difficulties. Pt seeks balance increases lost to corticosteroid-induced muscle wasting to reduce falls-risks and to safely navigate stairs. Pt seeks strength gains lost to corticosteroid-induced muscle wasting to reduce falls risk and stand up from chairs. Pt shall gain UE ROM over head from ___degrees to___degrees to reach food items from upper shelves. Pt shall obtain UE & LE strength gains from 1/5 to 3/5 to reduce falls & osteoporosis fractures resulting from corticosteroid-induced bone mineral wasting. Pt shall increase functional capacity from 1.5 MET to 3.3 MET in order to mop kitchen Floors. Pt seeks a functional increase from 2.0 MET to 3.5 MET which will enable the bathing of his dog. Pt seeks a functional increase from 2.0 MET to 3.8 MET which will enable him to scrub the bathtub, his most difficult home chore.
(MET) to Functional Task Conversions
(MET) Categories: Functional Tasks:
3.0; home activities; cleaning, wash car, wash windows, clean garage

74 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
3.5; home activities; mopping 3.0; home activities; cleaning, house or cabin, general work 3.5; home activities; vacuuming 3.8; home activities; scrubbing floors, on hands and knees, bathtub 3.5; home activities; standing – packing / unpacking boxes 3.0; home activities; implied walking - putting away household items 3.0; home activities; walking - light, non-cleaning shut/lock doors 3.5; home activities; standing - bathing dog, and cat –small animals 3.0; home repair; automobile repair, general 3.0; home repair; carpentry, general, workshop 3.0; home repair; painting, papering, plastering, scraping 3.0; home repair; put on and or removal of tarp 3.0; lawn and garden; riding snow blower 2.0; self care; standing - getting ready for bed, in general 2.0; self care; dressing, undressing (standing or sitting) 2.0; self care; talking and eating (standing) 2.0; self care; grooming, shaving, brushing teeth, washing hands 2.5; self care; hairstyling 2.0; self care; showering, toweling off (standing) 2.5; music playing; conducting 2.5; music playing; piano or organ 2.5; music playing; violin 2.5; home activities; multiple household tasks in general, light effort 2.5; home activities; cleaning, dusting, changing linen 2.3; home activities; wash dishes - standing 2.5; home activities; wash dishes; clearing dishes from table – walking 2.0; home activities; cooking or food preparation – general 2.5; home activities; serving food, setting table - walking or standing 2.5; home activities; cooking or food preparation – walking 2.5; home activities; feeding family pet, cat, dog, small animals 2.5; home activities; putting away groceries, carrying groceries 2.3; home activities; food shopping, standing or walking 2.3; home activities; ironing 2.0; home activities; implied standing - laundry, fold or hang clothes 2.0; home activities; making bed 2.5; home activities; watering plants 2.5; home activities; building a fire inside

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 75
6 - MINUTE WALK TEST (6MWT)
Name: ___________________________ Date: _________
Resting Data:
HR RPE SOBr %
spO2
FiO2/
LPM
6MWT HR RPE SOBr %spO
2 FiO2/LPM
Distance Walked
1 MIN
Checkmark
2 MIN
Checkmark
3 MIN
Checkmark
4 MIN
Checkmark
5 MIN
Checkmark
6 MIN
Checkmark
TOTALS
Checkmarks = 100 ft, 100 ft = one length.
Total feet:
Comments: i.e., signs and symptoms, angina, dizziness, stopped/paused before 6 minutes, reason why, etc.
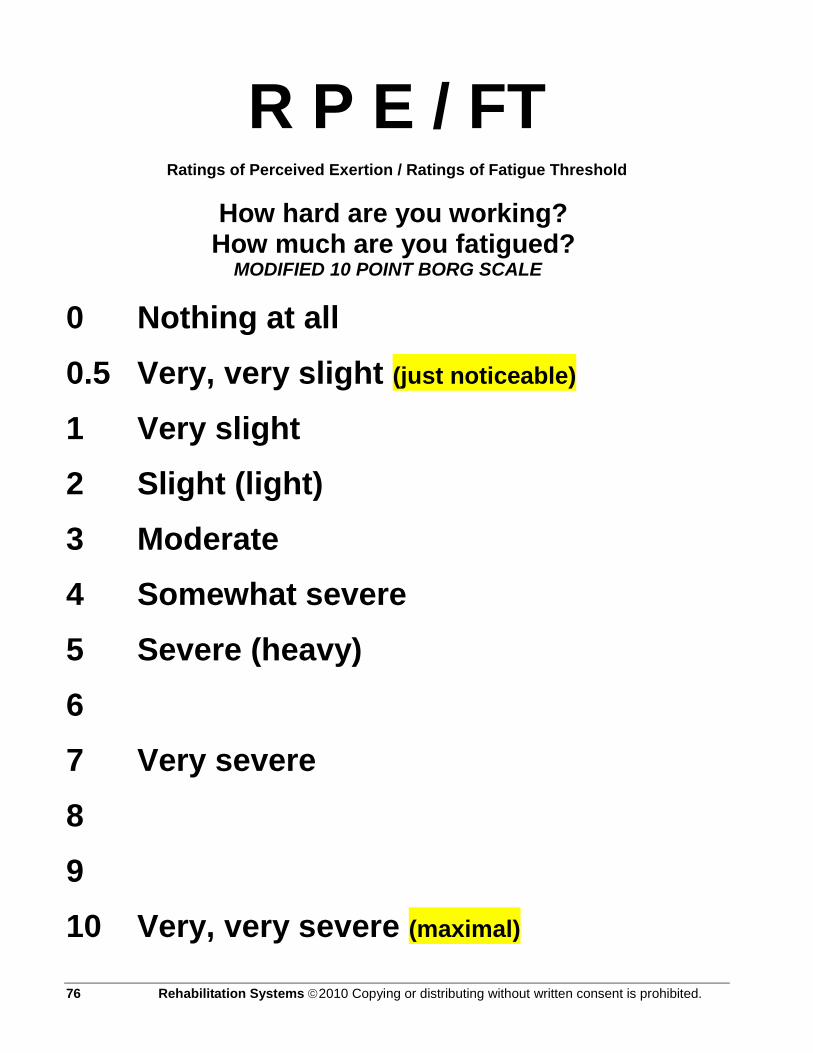
76 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
R P E / FT Ratings of Perceived Exertion / Ratings of Fatigue Threshold
How hard are you working? How much are you fatigued?
MODIFIED 10 POINT BORG SCALE
0 Nothing at all
0.5 Very, very slight (just noticeable)
1 Very slight
2 Slight (light)
3 Moderate
4 Somewhat severe
5 Severe (heavy)
6
7 Very severe
8
9
10 Very, very severe (maximal)
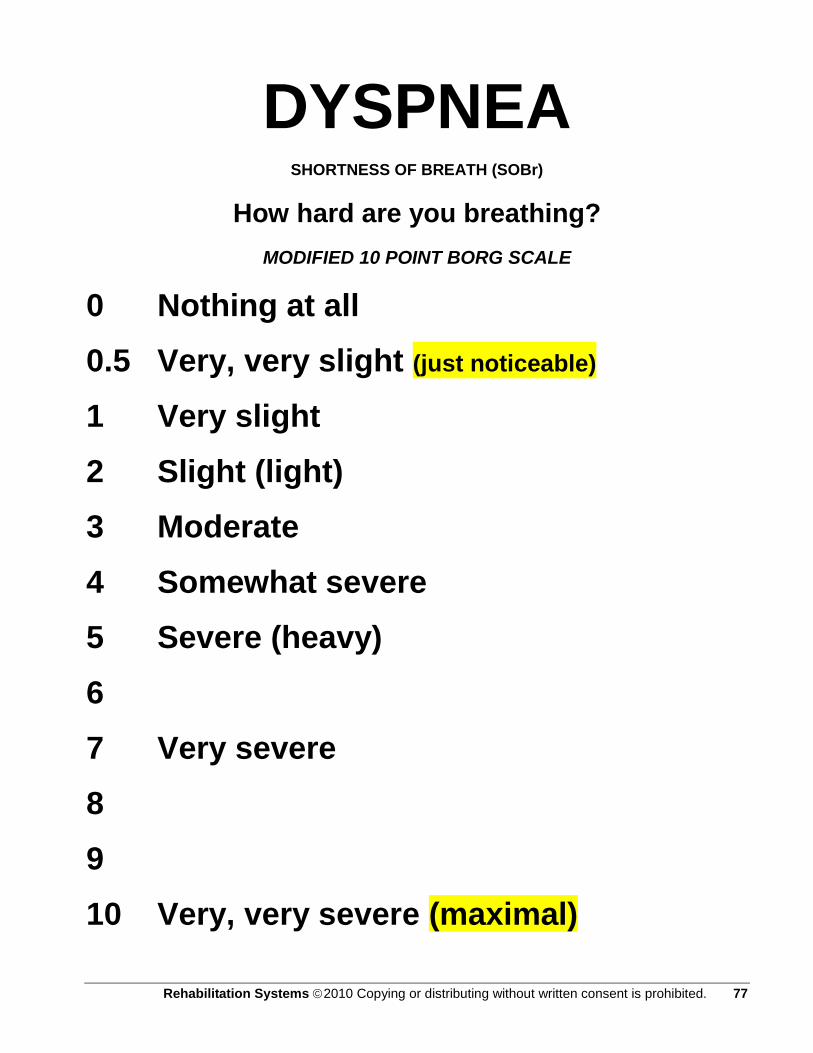
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 77
DYSPNEA SHORTNESS OF BREATH (SOBr)
How hard are you breathing?
MODIFIED 10 POINT BORG SCALE
0 Nothing at all
0.5 Very, very slight (just noticeable)
1 Very slight
2 Slight (light)
3 Moderate
4 Somewhat severe
5 Severe (heavy)
6
7 Very severe
8
9
10 Very, very severe (maximal)

78 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
MET- MPH, Speed, Distance, Energy Conversion Chart
MPH Ft Per Min 6MWT / Ft (MET) kcal / min Notes:
0.1 8.8 52.8 1.07 5.35
0.2 17.6 105.6 1.15 5.75
0.3 26.4 158.4 1.22 6.1
0.4 35.2 211.2 1.3 6.5
0.5 44 264 1.38 6.9
0.6 52.8 316.8 1.45 7.25
0.7 61.6 369.6 1.53 7.65
0.8 70.4 422.4 1.61 8.05
0.9 79.2 475.2 1.68 8.4
1 88 528 1.76 8.8
1.1 96.8 580.8 1.84 9.2
1.2 105.6 633.6 1.91 9.55
1.3 114.4 686.4 1.99 9.95
1.4 123.2 739.2 2.07 10.35
1.5 132 792 2.14 10.7
1.6 140.8 844.8 2.22 11.1
1.7 149.6 897.6 2.3 11.5
1.8 158.4 950.4 2.37 11.85
1.9 167.2 1003.2 2.45 12.25
2 176 1056 2.52 12.6
2.1 184.8 1108.8 2.6 13
2.2 193.6 1161.6 2.68 13.4
2.3 202.4 1214.4 2.76 13.8
2.4 211.2 1267.2 2.83 14.15
2.5 220 1320 2.91 14.55
2.6 228.8 1372.8 2.99 14.95
2.7 237.6 1425.6 3.06 15.3
2.8 246.4 1478.4 3.14 15.7
2.9 255.2 1531.2 3.22 16.1
3 264 1584 3.29 16.45
MPH Ft Per Min 6MWT / Ft (MET) kcal / min References: Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR Jr, Schmitz KH,
Emplaincourt PO, Jacobs DR Jr, Leon AS. Compendium of Physical Activities: An update of activity codes and MET intensities. Medicine and Science in Sports and Exercise, 2000;32 (Suppl):S498-S516. http://prevention.sph.sc.edu/tools/docs/documents_compendium.pdf

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 79
MET Chart
A MET or metabolic equivalent is the amount of energy used by the body to perform a physical activity or daily task. At rest, the average person has an oxygen consumption of 1 MET (or 3.5 ml/kg-min). MET values increase as more activity is performed.
Any activity in the ______ MET category you should tolerate easily.
1. For an 8 hour work day, you should be able to perform activities in the _____ MET occupational category.
2. For exercise, recreation and activities of daily living (ADL) lasting one jour or less, you should be able to tolerate activities in the _____ MET category.
3. Lifting, pushing or pulling may cause a rapid increase in your heart rate and blood pressure. Do not lift more than _____ pounds. Do not strain or hold your breath at any time. In general, activity involving the arms is more stressful to your cardiovascular system than leg exercise because your arm muscles are smaller and less efficient than your leg muscles.
METs Exercise Recreational Occupational Activities of Daily Living (ADL)
1.5-2.0 METs
Strolling 1-1.5 mph 1 miles in 40-60min
Knitting; Playing cards; Sewing; Watching TV
Desk work; Driving auto/truck; Sitting doing light assembly; Typing; Using hand tools; writing
Brushing hair/teeth, Light housework, Making bed; Partial bath; Polishing furniture; Washing clothes
2.0-3.0 METs
Walking, level 2.0-2.5 mph, 1 mile in 24-30min Cycling, level outdoors-5mph
Horseback riding (walk); Light golf (power cart); Playing musical instrument; Shuffleboard; Woodworking
Bartending; Crane operation; Standing doing light or medium assembly; TV/auto/car repair; Working heavy lever
Cooking; Driving car; Ironing; riding lawn mower; Scrubbing floor; walls, cars, windows; Showering; Sweeping; Tub bath
3.0-4.0 METs
Walking 3.0-4.0 mph, 1 mile in 15-20min Cycling, outdoors
5.5 mph
Billiards; Bowling; Canoeing; Croquet; Fly fishing; Golf (pulling cart); Shopping; Volleyball (non-competitive)
Baling hay; Driving heavy truck; heavy machine assembly; Janitorial work; Light welding; Operating large levers; Plastering; Plumbing; Stocking shelves
Cleaning windows; Climbing stairs (slowly); General House work; Kneeling; Light work; Packing/unpacking; Power lawn mowing (light); Sexual intercourse; Stocking shelves; Vacuuming
4.0-5.0 METs
Walking 3.5-4.0 mph 1 mile in 15-17 min Cycling, 8 mph Calesthenics Swimming (20 yd/min)
Ballet; Dancing; Gardening (how, weeding, digging), Golf (carrying clubs); Table tennis; Tennis (doubles); Volleyball
Building interior of house; Carrying trays/dishes; Farm work (sporadic); House painting, Lifting, carrying objects(20-40 lb); Light carpentry; Mechanic work
Raking leaves, shoveling light loads
5.0-6.0 METs
Walking 4.0-4.5 mph
Canoeing (4m/hr); Gardening (digging); Skating
Handyman work (moving, shoveling);
Raking leaves, shoveling light loads

80 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
1 mile in 13-15 min Biking, 10 mph
(ice/roller); Social/square dancing; Softball/baseball (non-game); Stream fishing
Heavy Carpentry; Putting in sidewalk
6.0-7.0 METs
Walking/jogging, 4.0-5.0 mph 1 mile in 12-13 min Biking, 11 mph Swimming (breaststroke)
Backpacking (light); Badminton; Hiking; Hunting; Horseback riding (trot), Skiing (cross country 2.5 mph); Skiing (light downhill); quare dancing; Tennis (singles)
Exterior home building; Lifting, carrying objects (45-64 lb); Shoveling (10/min, 9 lb); Splitting wood
Lawn mowing (push mower); Snow shoveling (light snow)
7.0-8.0 METs
Walking, 5 mph 1 mile in 12 min Biking (outdoors) 12 mph Swimming (backstroke), 40 yd/min
Badminton (competitive); Basketball (non-game); Canoeing (5 mph); golf (carrying bag); Horseback (gallop); Skiing (downhill, vigorous)
Ascending stairs with 17 lb load; Lifting, carrying (65-84 lb); Moving heavy furniture; Sawing
8.0-9.0 METs
Jog/run 5.5 mph Biking (outdoors) 13 mph Swimming (breaststroke) 40 yd/min Rowing machine; Rope jumping (60-80 skips/min)
Basketball (non-game); Handball/squash/racquetball; Mountain climbing; Soccer (non-team); Touch football; Tour skiing
Lifting, carrying (85-100 lb); Moving heavy furniture (moving van work); Shoveling (14 lb scoops, 10 scoops/min); Using heavy tools
9.0-10.0 METs
Jog/run, 6 mph 1 mile in 10 min
Football (competitive); sledding/tobogganing
Heavy labor; Lumberjack; Shoveling (16 lb scoops)
Ascending stairs carrying 54 lb
11.0+ METs
Run 7 mph (11.5 METs) 8 mph (13.5 METs)
Competitive sports: Basketball, Handball, Racquet, Rowing

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 81
Plan of Treatment or Exercise Prescription and Progression
Principle In patients with Cancer, disability is primarily a result of anti-cancer treatment with progressive deconditioning. As the disease progresses, limited functional capacity makes exertion unpleasant and leads to an increasingly sedentary lifestyle. Shortness of breath (breathlessness) and exercise intolerance are the most incapacitating symptoms patients develop. A counter-measure to progressive functional decline in patients with cancer is exercise training. For cancer patients, low to moderate-intensity aerobic exercise training should be performed to maintain endurance, strength, and function. The goal of exercise at this time is to maintain function and prevent the loss of endurance and strength. Anti-cancer treatments exhaust physical and emotional reserves, so the goal of low to moderate-intensity aerobic exercise training is to maintain these resources. Cancer patients are easily fatigued, but benefit from low to moderate-intensity aerobic activities. Aerobic exercise during and after anti-cancer treatment maintains or significantly retards the loss of strength and endurance and assists in countering signs and symptoms associated with psychosocial ills. Additionally, special modifications in the type of exercise performed may be required if orthopedic limitations, such as range of motion deficits, occur as a result of surgery.
For ―lung cancer‖ patients, irreversible destruction of the lung is a hallmark which must be worked around by accessing compensatory systems to achieve functional independence. Significant ventilation-perfusion mismatch impairing maximal gas exchange. Additionally, the work of breathing is increased secondary to increased airway resistance and hyperinflation. Increased muscle mass and a better vascular system will help improve peripheral extraction of oxygen, which will lead to better physical activity. Evaluate the patients need for bronchodilator therapy, mucolytics or supplemental oxygen during exercise. Therapists will find that frequent follow-up, encouragement and reassurance are integral to the success of the rehabilitation process. Progress in exercise tolerance may be minimal in this population, however diligent participation can reduce symptoms, reverse anxiety and depression, and increase the ability to perform activities of daily living.
Purpose It has clearly been demonstrated that exercise is beneficial for cancer patients. Structured exercise protocols and less demanding protocols for very low level cancer patients alike produced significant improvement in exercise tolerance. Exercise has been shown to improve the quality of life and therefore should be an integral adjunctive treatment for all cancer patients.

82 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Components of a Plan of Treatment or Exercise Prescription
A Plan of Treatment or exercise prescription generally includes the following specific recommendations:
Type of exercise or activity (i.e. strength training, walking, cycling, swimming, chopping wood, fishing, cleaning house, washing the car…)
Specific workloads (i.e. MPH, MET, FPM-walking speed, Kcal/min, )
Duration-(variable) and frequency-(fixed:3 X Wk) of the activity or exercise session
Intensity guidelines – Target heart rate (THR) range and estimated rate of (RPE), (SOBr), (Fatigue).
Precautions or contraindications regarding ratings of perceived exertion, ratings of fatigue, shortness of breath and oxygen saturation should be kept in focus in order to prevent overtraining. Remember to keep oxygen saturation > 88% Sp02 at all times during the therapeutic exercise session, additionally an orthopedic, cardiac or co-morbidity concern may require close supervision.
The 6 Minute Walk Test (6MWT) is used to establish the exercise prescription of the patient in both the in & out patient setting. Many cancer patients will not likely complete the full (6MWT). However, the information collected from the test is valuable. Special attention should be paid to Ratings of Fatigue (FT), Oxygen Saturation (%Sp02), Ratings of Perceived Exertion (RPE), Dyspnea (SOBr), Heart Rate (HR), and Fraction of Inspired Oxygen or Liters Per Minute (Fi02/ LPM) when identifying exercise intensity.
Subjective vs. Objective Measurements Subjective measurements are (RPE), (SOBr) (Fatigue) Objective measurements are (HR), (%Sp02), (Fi02/LPM).
Low stress threshold V. High stress threshold (Resiliency) Low stress threshold is categorized by high subjective ratings with low objective measurements. High stress threshold is categorized by low subjective ratings with high objective measurements.
If the Heart Rate remains low 80 to 100 and RPR-FT/SOBr are high between 6 and 7, one may conclude that the patient has a lower stress threshold or deconditioned functional capacity and is appropriate to start at a lower intensity level of RPE/SOBr of 2 to 3. Conversely, if the patient achieves a Heart Rate of 100 to 120 and reports an RPE-FT/SOBr of 3 to 4, this patient has a higher stress threshold and is appropriate to start at a moderate intensity level of RPE-FT/SOBr of 3 to 4.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 83
Procedure
Sure and safe progression is consistently achieved in the COPD diseased population with incremental increases in prescriptive exercise intensity, type, and duration. Start Low and Go Slow.
Exercise Dose – Response Relationship
With A Gradual Upslope In Progression
Moderate Intensity (Better for Outpatient programs)
Medicare B, Outpatient Programs-(OP).
(OP Clinic, SNF, ALF, ILF, Home)
Low Intensity (Better for Inpatient programs)
Medicare A, RUG, Inpatient Programs.
(SNF, HHA)
Exercise to promote functional independence Activity to maintain function or prevent deconditioning
Accumulate 60 minutes 3 days per week. RPE 4-6 on 10 point scale. Typically: Out Patient Programs.
Accumulate 15-25 minutes of activity that is well-tolerated three times a day, 4 to 5 days per week and gradually increase exercise time and intensity, RPE 2-4 on 10 point scale. Typically: In Patient Programs.

84 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
General Aerobic Exercise Recommendations Parameter Recommendation and Comment
Mode
Most exercises involving large muscle groups are appropriate, but walking, cycling, and NuStep, are especially recommended. The key is to modify exercise mode based on acute or chronic treatment effects of pulmonary exacerbations.
Frequency At least 3 times/wk, but daily exercise may be preferable for severely
deconditioned inpatients performing lighter-intensity and shorter-duration exercises.
Intensity Moderate intensity, depending on patient's current fitness level and
severity of side effects from treatments. Guidelines include 50%-75% VO2max or HRreserve, 60%-70% HRmax, or an RPE of 4-6. HRreserve is the best guideline if HRmax is estimated rather than measured.*
Duration At least 20-30 min of continuous activity, but this
goal may require multiple intermittent shorter bouts (eg, 5-10 min) with rest intervals in deconditioned patients or those experiencing severe side effects of treatment.
Progression Initial progression should be in frequency and
duration. Only when these goals are met should intensity be increased. Progression should be slower and more gradual for deconditioned patients or those with severe side effects of treatment.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 85
Incremental Exercise Progression
The time completed on the 6 Minute Walk Test (6MWT) sets the starting point for exercise duration. The patient completes 3 minutes on the (6MWT), this patient starts with exercise duration of 3 minutes, with a 3 minute rest period followed by 3 more minutes of exercise, and this is ―interval training‖. Below is an example of incremental exercise progression.
Aerobic Training
Session WORK REST INTERVAL WORK
Strength Training
50-70%-1RM
Session 1 3 MIN Tread Mill 1 x 8
Session 2 3 MIN 3:00 3 MIN 1 x 8
Session 3 3 MIN 2:30 3 MIN 1 x 8
Session 4 3 MIN 2:00 3 MIN 1 x 10
Session 5 3 MIN 1:30 3 MIN 1 x 10
Session 6 3 MIN 1:00 3 MIN 1 x 10
Session 7 3 MIN 0:30 3 MIN 1 X 12
Session 8 6 MIN End of interval 0:00 0 MIN 1 X 12
Session 9 7 MIN Tread Mill 1 X 12
Session 10 8 MIN Tread Mill 2 x 8
Session 11 6 MIN ADD: CE, NS, UBE 3 MIN 2 x 8
Session 12 6 MIN CE or NS or UBE 4 MIN 2 x 8
Session 13 7 MIN CE or NS or UBE 4 MIN 2 x 10
Session 14 7 MIN CE or NS or UBE 5 MIN 2 x 10
Session 15 7 MIN CE or NS or UBE 6 MIN 2 x 10
Session 16 7 MIN CE or NS or UBE 7 MIN 2 X 12
Session 17 8 MIN CE or NS or UBE 7 MIN 2 X 12
Session 18 8 MIN CE or NS or UBE 8 MIN 2 X 12
Session 19 9 MIN CE or NS or UBE 8 MIN 3 X 8
Session 20 9 MIN CE or NS or UBE 9 MIN 3 X 8
Session 21 10 MIN CE or NS or UBE 9 MIN 3 X 10
Session 22 10 MIN CE or NS or UBE 10 MIN 3 X 10
Session 23 11 MIN CE or NS or UBE 10 MIN 3 X 12
Session 24 11 MIN CE or NS or UBE 11 MIN 3 X 12 CE: Cycle Ergometer
NS: NuStep
UBE: Upper Body Ergometer

86 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Work-Rest Ratio
The Work-Rest-Ratio (WRR) as a method of interval training serves best at the beginning of the low level patients program and should follow the One-to-One (1:1) (WRR) rule, i.e., Work 3 minutes: Rest 3 minutes: Work 3 minutes. The Work-Rest-Ratio-Interval (WRRI) should decrease in 30 second increments from threptic session to therapeutic session or as the patient tolerates without fatigue hangovers. Once the (WRRI) has been closed, the therapist may add one (1) minute of exercise duration per exercise session or as the patient tolerates without fatigue hangovers. (Causing a ―Fatigue Hangover‖ is a cardinal sin) The optimal aerobic activity segment should seek to reach the following ―Best Case Scenario‖.
GOAL: Best Case Scenario; 15 minutes walking/treadmill, 15 minutes cycling, with 20 minutes of upper and lower extremity strength training exercises.
Prescribing exercise in the chronic diseased population requires a significant amount of planning and encouragement. The plan of treatment or exercise prescription should proceed gradually since most individuals are extremely limited in the amount of exercise tolerated secondary to fatigue, anti-cancer therapy debilitation, deconditioning, exertional distress or hypersensitivity to exertion.
References
United States Army Center for Health Promotion and Preventive Medicine 5158 Blackhawk Road. Aberdeen Proving Ground, Maryland 21010-5403 MAJ Robert L. Gauer, MD, FACSM, LTC Francis G. O.Connor, MD, FACSM COL Willis B. Campbell, MD, Ph.D., MPH, FACSM Fundamentals of Resistance Training: Progression and Exercise Prescription KRAEMER, WILLIAM J.; RATAMESS, NICHOLAS A. Medicine & Science in Sports & Exercise: April 2004 - Volume 36 - Issue 4 - pp 674-688 Is the 6 Min Walk Test An Acceptable Measure of Progression in Cardiac Rehabilitation Programmes? Derman, E W FACSM; Dreyer, L A; Schwellnus, M P FACSM; Noakes, T D FACSM. Medicine & Science in Sports & Exercise: May 2001 - Volume 33 - Issue 5 - p S319 H15g Free Communication/Poster Adults With Chronic Diseases and Disabilities Exercise in Rehabilitation Medicine, 2nd Edition Sliwa, James A. D.O. Medicine & Science in Sports & Exercise: November 2006 - Volume 38 - Issue 11 - p 2036

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 87
Individual Therapeutic Session, SOAP Note Format
Principle Each therapeutic session is an opportunity to provide exercise in a controlled and monitored environment, and education that not only enhances exercise, but also improves all aspects of function. Each session will build on the previous session in both fitness and knowledge.
Purpose Exercise sessions should focus on individual needs and aim to progress the patient to a higher level of functioning. Patient goals should be discussed and reviewed at various points throughout the sessions to assist in measuring progress. Documentation during each session also helps both therapists and patients measure success.
Procedure
Subjective
Record subjective information that the patient reports, such as, how they are feeling or sleeping.
Objective
Record a productive chough, or sleep disturbance such as waking up to breathe.
Measurements
HR (Heart Rate)
BP (Blood Pressure)
% spO2
RPE/SOBr/Fatigue
Physiological Changes During Exercise
What do these measurements mean? You expect the heart rate to increase with exertion. You should also see an increase in blood pressure with exercise. Oxygen usage will increase, but the % sp O2 should remain above 88% at all times during exercise. Any sudden change in any of the baseline measurements or subjective reporting indicates a need to decrease or even stop the exercise. Monitoring changes will allow you to determine whether to increase or decrease the intensity of the therapeutic session or seek medical attention from the patient‘s physician.
88 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Aerobic Exercise
There are various modes that can be used for aerobic exercise. Ideally two modes of aerobic exercise will provide variety if the patient can tolerate the exercise duration. The treadmill is the most important mode of aerobic training as it easily translates into ADL's and functional independence.
All aerobic exercise must begin with a 3 min warm up and conclude with a 3 min cool down at minimal loads.
Aerobic training requires only one warm up and one cool down. Transitioning between equipment is exempt from WU & CD workloads.
COPD patients often have balance and falls-risk issues so they must be monitored for safety while on exercise equipment. As a rule, most COPD patients will require balance and gait training to counter the lean tissue waisting that occurs from chronic corticoid steroid use.
Resistance Exercise
Resistance exercise is patient dependent; therefore, adjusting intensity, and volume should be considered based on patient needs, ability, and history.
Resistance exercise is very important for LE & UE as it translates into ADL's.
Resistance exercise is an emerging research focus for COPD patients as it‘s revealing functional outcomes equivalent to aerobic exercise training.
Resistance exercise progression is outlined in the following guidelines: o Sets & Reps:
1x8, 1x10, 1x12, 2x8, 2x10, 2x12, 3x8, 3x10, 3x12.
ROM exercise may be ―medically necessary‖, thus, ROM therapy should be carefully attended to.
Patient Education
Exercise sessions will include education associated with your condition. Successive education will build on previous education. You will be asked to read about the benefits of exercise and proper exercise, and you will be given tips for making everyday tasks easier.
8 sessions should be taught and documented.
Patient education is a partnership, ask the patient to pre-read, and then cover the section & answer questions once a week in a 15-minute lesson session.
Follow-up
Complete SOAP notes and documentation.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 89
Assessment
Document how the patient tolerated the exercise session using intensity, duration, frequency, and mode (IDFM).
Plan
Document goals and/or changes for the next session using IDFM.
Measurements
Allow the patient to cool down, and then collect final measurements and compare to baseline measurements. The resting heart rate should be within 8 beats of the baseline.

90 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
SOAP NOTE
Cancer Rehabilitation
Session # Patient Name: Date:
Subjective: Patient feels (check one) О Good О Fair О Poor
Objective:
Resting Measurements Aerobic Exercise
Start Tx End Tx Requirement Type Duration Int HR BP %SpO2 FiO2
HR HR <100 to DC
Warm up (3 Min)
BP BP <200/110
%spO2
%spO2
>88%
FiO2 FiO2 Keep % spO2 >88
Education:
Notes:
Cool Down (3 Min)
RPE/DYSP/Fatigue
(1-10)
Strength Training
Sets
(1-3)
Reps
(8-12)
Load
(lbs)
Leg Press
Chest Press
Overhead Press
Pull Downs
Rowing
Assessment:
Planning:
Therapist

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 91
Patient Education Manual: CANCER FITNESS
By Author; Anna L. Schwartz, FNP, Ph.D., FAAN. Present 1 lesson a week for 8 weeks, see education module
(CaR) is a 24 session program, 3 sessions a week for 8 weeks
Check CPT CODE
97001 Orientation: Intake Evaluation, H&P
Set patient‘s rehab goals in Functional and MET terms
Present 1 lesson a week for 8 weeks, see lessons below
Administer 6MWT-97750, SF-12 HQoL Survey-97530.
Write exercise prescription from the 6MWT
97530 Lesson 1: Managing Your Side Effects
97530 Lesson 2: Cancer and Exercise: What Does the Science Show
97530 Lesson 3: The Basics of Exercise During Treatment
97530 Lesson 4: Setting Goals for a Lifetime of Exercise
97530 Lesson 5: Cancer Fitness Fundamentals
97530 Lesson 6: Cancer Fitness Aerobic Exercise Program
97530 Lesson 7: The Core of Resistance Exercise
97530 Lesson 8: Realizing your potential
97110 Provide the Home Exercise Program (HEP)
Administer 6MWT-97750, SF-12-97530 HQoL Survey
Write /send progress letter to MD
Invite patient to attend phase 3 maintenance program

92 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Patient Education Outline from Cancer Fitness
By: Anna L. Schwartz Ph.D.
Eight (8) Chapter synopses lessons will be presented for patient education as outlined below. There will be (1) (15) minute lesson delivered each week during the eight week program for a total of eight (8) lessons. The synopses outline below will guide Therapists to discuss ―Key Points‖ of Cancer Fitness.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 93
Lesson One(1): CH3 Managing Your Side Effects
Key Points:
*Learn to manage your side effects early in your treatment. *If your management techniques are not working as well as you would like, work with your health care team to develop a better plan. *Manage your side effects early before they get bad. This is especially true of pain and nausea – take your medication regularly, as prescribed. *Know that your side effects can be managed. *Ask for help if you aren‘t feeling well. *Drink adequate amounts of fluid. *If your side effects are not controlled, it is difficult to exercise.
Lesson Two(2): CH1 Cancer and Exercise: What Does the Science Show?
Key Points:
*Maintaining or increasing your physical fitness during cancer treatment can improve your quality of life, reduce the number and intensity of your side effects, and help in your recovery.
*Exercise does not need to be hard or cause discomfort.
*Exercise done in short sessions, spaced out over the day, can decrease side effects from treatment.
*The functional ability losses from inactivity and rest take a long time to rebuild. These declines contribute to prolonged fatigue after treatment.
*Research is continuing to help us understand the effects of exercise during cancer treatment and survivorship.
Lesson Three(3): CH2 The Basics of Exercise During Treatment
Key Points:
*When and how to Start. Exercise after Surgery. *Exercise during chemotherapy, immunotherapy, and radiotherapy. *Exercise despite treatment-related limitations. *When to go easy and take a day off. *Setting your limits. *Exercise Precautions.
Lesson Four(4): CH4 Setting Goals for a Lifetime of Exercise
Key Points:
*Starting an exercise program takes commitment and determination, but the rewards will be there for you. *Examine your barriers and excuses to exercise, and make a plan to succeed. *Set your own goals that are reasonable and achievable.
Lesson Five(5): CH5 Cancer Fitness Fundamentals
Key Points:

94 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
*Exercise is safe for cancer patients. *Exercise should be fun: not make you feel uncomfortable. *Exercise programs should be individually tailored to your ability and needs. *Use the rating of perceived exertion (RPE) scale to determine how hard you are exercising. *Adapt exercise to match your physical abilities so you can reap the many physical and emotional rewards.
Lesson Six(6): CH6 Cancer Fitness Aerobic Exercise Program
Key Points:
*Type of Aerobic activity. *Frequency of activity. *Intensity of activity. *Duration of activity. *Activity and Chemotherapy. *Exercise Logs. *Coming back to life.
Lesson Seven(7): CH8 The Core of Resistance Exercise
Key Points:
*Don‘t start resistance exercise until you are at least 4 weeks past surgery, unless your doctor gives you permission. *Start slowly and expect to progress slowly. *Notice any unusual changes in your body. If you are at risk for or have lymph edema, measure the girth of your arm or leg every morning. If you notice swelling, contact your health care team or your physical therapist. It is important to intervene early. *Before beginning your resistance exercise program session, think about standing tall and strong, relax your face, and breathe deeply. *Do each exercise slowly, and work your muscles through a full range of motion.
Lesson Eight(8): CH11 Realizing your potential
Key Points:
Bringing our lives into balance and pursuing interests and activities that we enjoy fosters intensity, concentration, and enthusiasm. The pursuit of excellence does not happen without commitment, passion, and a focused plan. Success does not happen by accident. Our dreams and our persistent struggle to make them real determine our future.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 95
Cancer Rehabilitation Case Study: Fatigue
Introduction Fatigue is one of the most common, distressing and frustrating side effects of cancer and its treatment (1). While red blood cell growth factors (erythropoietin) have greatly reduced the fatigue associated with anemia, patients continue to be confronted with fatigue that interferes with normal physical and emotional function both during and following treatment. Cancer treatment related fatigue is associated with reduced physical strength, aerobic function, cognitive dysfunction, and depressed mood (2). Fatigue is generally reported to be worse among younger patients (3). While some chemotherapy regimens may cause more fatigue than others, there are no risk factors for disabling levels of fatigue. Patient Overview KC is a 66 year old woman with stage III breast cancer. She received neo-adjuvant chemotherapy with doxorubicin (A), cyclophosphamide (C) and paclitaxel (T) (ACT). After 6 weeks of treatment she had achieved a good tumor response, shrinking approximately 3cm and was a candidate for breast conservation surgery. One month following the completion of surgery she returned to continue chemotherapy and completed the dose dense ACT regimen. To prevent neutropenia she received granulocyte-colony stimulating factor (G-CSF; e.g. filgrastim), and when her hemoglobin fell below 11G/dl she was started on erythropoietin to correct her anemia. Although KC tolerated treatment well, from a medical perspective, she continued to experience worsening fatigue, and complained of feeling irritable and moody, and reported problems with her memory. These side effects were troubling enough that KC didn‘t feel comfortable doing her usual activities and felt safest at home. She stopped going to the grocery store, asking her husband to help with this and other chores. She was assessed for depression and started on Wellbutrin XL 300mg daily. Within two weeks of starting Wellbutrin XL her symptoms of depression improved. However, her fatigue persisted and during the second half of chemotherapy she became increasingly sedentary only leaving the house for medical appointments. KC would walk from her house to the car and then to the infusion room and be exhausted and out of breath. The more she protected herself and tried to rest the worse she felt not only physically, but emotionally. Fatigue was taking its toll on her as she became more and more debilitated from trying to reduce her fatigue by resting and doing nothing. As KC neared the completion of chemotherapy she vocalized great concern about her ability to continue on with treatment and begin radiation therapy; she was just too weak. At this point, KC was referred to the local cancer rehabilitation program. The cancer rehabilitation program required KC to commit to exercising with a therapist 3 days a week. A systematic, step-by-step approach was taken to increase KC‘s aerobic capacity and muscle strength. Each exercise session KC started off with a slow warm-up on a recumbent bicycle and then increased her exercise intensity to approximately 60 – 70% of her predicted maximum heart rate. She pedaled at this intensity for varying periods of time – less time when she initially stated the program and gradually increasing the duration at this intensity. Her aerobic exercise program was paced so that she had two weeks of pushing herself and then a week of recovery. During recovery weeks, KC‘s duration and intensity of aerobic exercise was reduced by approximately 25% so her body could adapt to the stresses of exercise. Following each aerobic exercise session, KC would complete at least 2 different upper body and 2 lower body resistance exercises. These exercises were usually completed on a weight machine, but she was also taught how to do these exercises with Thera-Bands™, rubber bands of varying thickness and resistance. Initially, KC completed 1 set of 8

96 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
repetitions and worked up to doing 2 sets of 10 repetitions before moving up to a heavier weight or Thera-Bands™ with greater resistance. KC began radiation during the 3rd week of the exercise program. She continued to complain of fatigue but was able to walk into the clinic without becoming exhausted and was beginning to do more of her usual activities. KC reported that although she was still overwhelmed at times by her fatigue, that her mood and general outlook on life was better. She was starting to ―feel like a survivor‖ and as though she could make it through the full course of radiation therapy. KC continued to attend the complete 8-week cancer rehabilitation program and then entered phase 2 of the program, transition to home-based exercise. During the transition period, the therapist spent time teaching KC how to follow the strength training exercise at home with the Thera-Bands™. The aerobic exercise program was also reviewed. KC continued to exercise with her therapist one day a week for 4-weeks, and then was on her own with weekly or biweekly telephone calls to help her stay with the program (4). After 6-weeks of exercise at home, KC started to slide and was not completing the target exercises. She returned to the supervised setting and realized that having someone to exercise with and report to was what she needed to follow the program. Through the cancer rehabilitation program, KC was introduced to another survivor who lived in her area and the two began exercising together on a regular basis. Outcome Over the course of 16-weeks, KC increased her aerobic capacity by 32%, and her muscle strength by 19%. She resumed all of her normal activities and reported feeling better than she felt before breast cancer. Her new-found strength and fitness had resolved the fatigue problems associated with disuse and debilitation. The prompt use of granulocyte-colony stimulating factor prevented neutropenia and associated complications, and erythropoietin corrected KC‘s anemia. The use of Wellbutrin XL alleviated the mood disturbance experienced during treatment. Discussion The etiology of cancer-related fatigue is unknown, but a neurophysiologic model suggests that chemotherapy and biotherapy may impair the central and peripheral nervous system and those medications that act on the CNS may compound fatigue (5). Other significant etiologies of fatigue should be considered: pain, infection, depression, sleep deprivation, anemia, nutritional status, heart failure from anthracycline therapy, hypothyroidism, cardiopulmonary insufficiency, medications and activity level. Fatigue assessment ideally should begin before treatment is initiated. Measuring fatigue on a 0 to 10 (no fatigue to worst imaginable fatigue) is clinically feasible, relevant, and can determine clinically important differences in fatigue that might indicate when intervention is necessary (6). Interventions that have demonstrated efficacy in reducing fatigue, when other causes have been ruled-out or addressed (e.g. anemia, neutropenia, etc…), include education, physical activity, energy conservation, and medications (7, 8, 9, 10). Ideally, a comprehensive multidisciplinary treatment approach would be used to determine the best intervention for a patient. Treatment decisions should be based on physical examination, laboratory tests, and psychosocial assessment of the individual. In this case study, KC‘s fatigue persisted despite correction of anemia, and initiation of an anti-depressant. While KC‘s health was improved by these interventions, the cause of her ongoing fatigue appears to be related to declines in functional ability associated with inactivity (11, 12). The progressive, individualized exercise program improved KC‘s functional ability and muscle strength, while the medications corrected her anemia and depression. Cancer-related fatigue is a complex
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 97
and all too common side effect of treatment that needs to be assessed early. Approaches to intervention need to consider a wide variety of causes and multiple different treatments may be required to maintain optimal health during treatment. References 1. Curt, G.A., Breitbart, W., Cella, D., Groopman, J.E., Horning, S.J., Itri, L.M., et al (2000). Impact of cancer-related fatigue on the lives of patients: New findings from the Fatigue Coalition. Oncologist, 5, 353-360. 2. Mock, V., (2001). Fatigue management: Evidence and guidelines for practice. Cancer, 92(6Suppl.), 1699-1707/ 3. Bower, J.E., Ganz, P.A., Desmond, K.A., Rowland, J.H., Meyerowitz, B.E., & Belin, T.R. (2000). Fatigue in breast cancer survivors: Occurrence, correlates, and impact on quality of life. Journal of Clinical Oncology, 18, 743-753. 4. Schwartz A.L., & Winters, K. (2006). Promoting Physical Activity in Cancer Survivors. In A. McTiernan (Eds). Physical Activity, Energy Balance, and Cancer: Etiology and Prognosis. Marcel Dekker Publishing. 5. National Comprehensive Cancer Network (2003). Practice guidelines for cancer-related fatigue. Jenkinton, PA: Author. 6. Schwartz, A.L. Meek, P.M., Nail, L.M., Fargo, J., Lundquist, M., Donofrio, M., Grainger, M., Throckmorton, T., Mateo, M. (2002). Measurement of fatigue: Determining minimally important clinical differences. J. Clinical Epidemiology, 55, 239-245. 7. Schwartz, A.L., Thompson, J.A., & Masood, N. (2002). Interferon-induced fatigue in patients with melanoma: A pilot study of exercise and methylphenidate. Oncology Nursing Forum, 29, E85-90. 8. Mock, V. (2003). Clinical excellence through evidence-based practice: Fatigue management as a model. Oncology Nursing Forum, 30, 787-796. 9. Schwartz, A.L. (1999). Fatigue mediates the effects of exercise on quality of life in women with breast cancer. Quality of Life Research, 8, 529-538. 10. Barsevick, A., Dudley, W., Beck, S., Sweeney, C., Whitmer, K., & Nail, L.M. (2004). A randomized clinical trial of energy conservation for cancer-related fatigue. Cancer, 100, 1302-1310. 11. Winters, K. & Schwartz, A.L. (2006). Quality of Life and Fatigue in Breast Cancer. In A. McTiernan (Eds). Physical Activity, Energy Balance, and Cancer: Etiology and Prognosis. Marcel Dekker Publishing. 12. Schwartz, A.L. (2004). Physical Activity After A Cancer Diagnosis: Psychosocial Outcomes. Cancer Investigations.

98 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Manage Common Cancer Treatment Side Effects
It is recommended by Oncology clinicians that one learn to manage cancer treatment side-effects before starting cancer rehabilitation. While knowing how to manage side –effects before rehabilitation may be optimal; it may not be the norm. At the beginning of cancer treatment there are numerous factors and conditions which typically overwhelm most patients. Thus, cancer rehabilitation may be the first focused learning opportunity patients have on managing side-effects.
Thus, knowing how to educate and treat the cancer patient population provides a significant intervention opportunity for Physical Therapy. It is through the delivery of information, care and skills that the Physical Therapist becomes a lifelong consultant to the cancer population.
Rehabilitation during treatment has been proven within the scientific community to benefit and improve the outcomes of cancer treatment. Yet, the cancer patient will not be able to fully enjoy these benefits if pain and nausea prevent them from engaging in therapeutic prescriptive exercise.
Therapeutic, prescriptive exercise can reduce nausea, fatigue and other cancer side-effects. It is important to teach cancer patient the standard methods of managing symptoms before symptoms prohibit meaningful participation in cancer rehabilitation.
The most common side-effects that besiege cancer patients are listed below:
1. Physical Fatigue 2. Cognitive Fatigue Chemo-Brain 3. Pain 4. Nausea 5. Mouth Sores 6. Constipation 7. Diarrhea 8. Sleep Disturbance 9. Lymph edema 10. Peripheral Neuropathy 11. Osteoporosis 12. Heart Disease

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 99
1. Physical Fatigue is the most common side-effect and is associated with all cancers and treatments. A patient must identify patterns of fatigue and then plan activities during their peak energy zone. Cancer and cancer treatment causes patients to suffer from Anemia (a lack of red blood cells) thus oxygen saturation may be an issue for the exercising cancer patient. Cognitive Fatigue, Chemo-Brain is a lack of memory and mental acuity which results in delayed response mental activity, chemo-brain may remain for months, even a year or two after cancer therapy.
2. Pain can come from the cancer tumor and or cancer treatment. Radiation therapy can cause skin breakdown, chemotherapy can cause mouth sores, skin irritation, ulcers, and sometimes infections in the mouth and throat. Pain is also experienced from chronic headaches.
3. Nausea and vomiting are common side-effects of many cancer treatments. Both chemotherapy and radiation can cause nausea. Drugs for nausea are called Anti-emetics and are very effective.
4. Mouth Sores are common chemotherapy side-effects. Mouth sores, thrush, white patches caused by yeast infections are part of chemotherapy. Cancer therapy causes a painful and red mouth which makes eating and swallowing very difficult.
5. Constipation is caused by the lack of activity, changes in eating habits and the lack of fluid intake. Being constipated can cause significant belly pain and discomfort. Exercise is very helpful in overcoming constipation.
6. Diarrhea is caused by chemotherapy and radiation. This is especially true if radiation is being done in the abdominal region of the body.
7. Sleep Disturbances, pain and irritation disrupt normal body functioning which cause significant sleep disturbances. Thus, sleep medication will be necessitated to overcome sleep deprivation.
8. Lymphedema, swelling in the arms or legs may result from surgery or radiation. The swelling can start immediately after surgery or therapy or it can start several months later. Physical Therapy will need to be prepared to manage the inevitable occurrence of Lymphedema.
9. Peripheral Neuropathy, Certain types of chemotherapy (Vincristine, Paclitaxel, Cisplatin) and tumors can injure the peripheral nerves, causing numbness in the affected areas.
10. Long-Term side-effects of treatment and cancer. Osteoporosis. Bone loss occurs during treatment and is a silent, asymptomatic side-effect. Chemotherapy (Doxorabicin, Methotrexate, Prednisone, & Decadron) cause bone wasting which are greatest in pre-menopausal women. This represents the breast cancer population to the largest extent.
11. Heat Disease, Many cancer treatments cause weight gain and inactivity. Cancer survivors are four (4) times more likely to die from a heart attack then their health cancer-free counterpart.
These are the primary side-effects we will have the responsibility to teach the cancer population to manage well during cancer rehabilitation.

100 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Part A Part B Other
Physical Therapy
PLAN Skilled Services Required:
GOALS (Short Term) Gait Training ROM/Contracture Mgmt.
Balance Re-ed Home Program
Outcome (Long Term) Therapeutic ex. Pt/Caregiver Training
Muscle Re-Ed Safety Skills
Energy Cons. Equipment Needs
Other
N/A
20. INITIAL ASSESSMENT 19. PRIOR HOSPITALIZATION FROM to
Age M / F Rehab Potential
Hx and level of function at start of care:
Min tolerated
Distance
HR
%SPO2
RPE
Dyspnea
FIO2
Min tolerated
Distance
HR
%SPO2
RPE
Dyspnea
FIO2
22. SERVICE DATES FROM THROUGH
FORM HCFA-700 (11-91)
2)
Tx Justification:
15. PHYSICIAN SIGNATURE 16. DATE
N/A
DISCONTINUE SERVICESORCONTINUE SERVICES
18. ON FILE (Print/type physician's name)
N/A
5)
21. FUNCTIONAL LEVEL(end of billing period) PROGRESS REPORT:
3. HICN
10. TREATMENT DIAGNOSIS
6. ONSET DATE 7. SOC DATE
FIRST NAME M.I. 2. PROVIDER NUMBER
4. PROVIDER NAME MEDICAL RECORD NO. (Optional)
DEPARTMENT OF HEALTH AND HUMAN SERVICES
HEALTH CARE FINANCING ADMINISTRATION
(professional establishing POC including professional designation)13. Signature
12. PLAN OF TREATMENT FUNCTIONAL GOALS
PLAN OF TREATMENT FOR OUTPATIENT REHABILITATION (COMPLETE FOR INITIAL CLAIMS ONLY)
1. PATIENT'S LAST NAME
14. FREQ/DURATION (e.g. 3/wk x wk.)
11. VISITS FROM SOC
1)
8.TYPE: 9. PRIMARY DIAGNOSIS
2)
1)
From
17. CertificationI CERTIFY THE NEED FOR THESE SERVICES FURNISHED UNDER THIS PLAN
OF TREATMENT AND WHILE UNDER MY CARE
3)
4)
THROUGH
__
Assessment
__
__
6 minute walk test
6 minute walk test Assessment
__
__
__

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 101
Cancer Rehabilitation Progress Report
Dear Dr. XXXX
Patient: XXXX Age:63 Date: April 22, 2008
Admitting Diagnosis: COPD 496
Baseline Data Completion Data
Date 02/08/05 04/15/05
Resting HR, BP, SaO2%, FiO2 94 89 RA 72 94 RA
Exercising HR, BP, SaO2%, FiO2 117 88 RA 109 90 RA
Exercise Duration & Intensity –
Cycle
3 min Level 1 5 min Level 2
Exercise Duration & Intensity - Treadmill
1 min 1 mph 7 min 2 mph
Rating of Perceived Exertion (1-10) 5 = working hard 3 = working moderately
SF – 36, Physical Function 28 74
SF – 12, H- QOL 31 83
Rating of Perceived Dyspnea (1-10) 5 = very SOB 3 = moderately SOB
6 Minute Walk Test Note Pt terminated test at 00:04:27 Pt completed walk test
6MWT – Distance 738 feet 1,342 feet
Comments on Training and Compliance: XXX is strong willed; she worked diligently in almost every exercise session. The greatest gain was seen in muscular strength. Compliance was an issue as XXX refused to use supplemental oxygen for exercise training. This refusal was ultimately a barrier to further progress in the program; hence, XXX was discharged early (26 visits V. 36 visits) due to non compliance to oxygen saturation guidelines.
Signs, Symptoms and Changes: Ratings of Perceived Exertion improved from 6 to 3. Ratings of Dyspnea improved from 6 to 3 as well. Oxygen de saturation was a continual battle. We used interval training to provide an exercise stimulus resulting in physiological adaptation to increased work.
Patient Education: XXX took part in learning about the following: Medication and Equipment for self care, Physical fitness, Chest Physical Therapy, Airway Management, Stress Management, Relaxation, Nutrition for COPD Patients, Disorders of the Respiratory System.
Current Home Activity Guidelines: XXX has purchased a Tread Mill and will continue this program at home. She may come back to Pulmonary Physical Therapy to join a phase three program at no cost.
Thank you, for this referral.
Sincerely, John Doe, Therapist
118
72
70
68
64
128
112
122

102 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
DATE: October 14, 2009.
TO: J. Doe M.D.
RE: John Doe
Cancer Rehabilitation Discharge Summary
OVERALL PROGRESS: POOR FAIR GOOD EXCELLENT
Compliance: Good. Mr Doe was in attendance three times a week and we committed to improving his health.
Six minute walk test: Pt able to make improvements with 6 min walk test improving from 350 ft and terminating test at 2 min 37 sec to 740 ft and completing test. Pt required no supplemental oxygen and was able to maintain %SPO2 at 97 and above.
Patient Education: Pt received education on medications and equipment for self-care, physical fitness, chest physical therapy, airway management, stress management, relaxation, and nutrition for cancer patients, and disorders of the respiratory system.
Home Exercise Program: Pt needs further instructions and pictures to understand his home exercise program. Pt instructed to walk 3-5 times per week
Additional Comments: Pt took encouragement during treatment to push himself. Pt motivation was at first poor, but really took off after session 9 which resulted in good overall progress.
Thank you for this referral,
John Doe
Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 103
Program promotion and marketing
The Art of Communication:
Communication is at the heart of engaging professionals as one delivers and receives messages designed to accomplish the common purposes of health care service delivery.
The Nature of A Good Relationship:
It‘s all about giving and receiving. But when it comes to communication, we need to be aware and artful in how we ―give‖ our message, so that we can ―receive‖ the response we‘d like.
Value Determination:
It comes down to awareness of your own values and those of the people you have relationships with. By values, I don‘t mean the high ideals of honesty, ethics, liberty, etc. Rather, we are talking about your priorities and the things (or people, activities, goals) that are most important to you. These are normally the things that you spend your most time and money on, how you fill your space and spend your energy.
For example, a stay-at-home mom probably has her priorities fixed on her kids and will spend her money on school books and kids‘ clothes before even thinking of luxuries like a gym membership. A training athlete values his fitness so much that he couldn‘t imagine not going to the gym or buying the latest technology in running shoes and wouldn‘t even notice the 50% discount on kiddie‘s sneakers. Another clue to picking up on people‘s values is to listen to what direction they steer a conversation.
Whatever is highest on your values is where you have the most order, motivation and inspiration. On the other side, you tend to procrastinate on the things that are lowest on your values, which have the most disorder and chaos. Every single person‘s values are different and they act as lenses through which we view and filter the world around us. If you expect people to live and react according to your unique values, you‘re living in a fantasy and setting yourself up for disappointment.
However, once you recognize different people‘s priorities, you can start to communicate in a way that builds lasting and meaningful relationships, whether it‘s in business, social circles or family.
Art of Communication:
The art of communication is in communicating your values in terms of the values of others. Ask yourself, how can I phrase what I want so that it serves the other person‘s values in some way? What‘s important to me and what‘s important to them and how can I link the two? This is of course the constant dilemma of life, as no two conversations will be exactly alike. However, you can discern common trends through the process of relationship building, the foundation the art of communication.
104 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
The Top 10 Marketing Rules:
10. Be online. Today, you can't afford not to be online. More and more consumers are going online to search, research and purchase items and for many of them, if you aren't there, they won't even know you exist. Having an online presence today is not only easier than you think, it's less expensive than it's ever been. And with over 2 million people in US and Canada going online regularly, can you really afford to not be there? See www.gocancerrehab.com
9. Know thyself. Trying to be all things to all people pulls your business in too many directions. Take stock of what your business does best and play up the strengths. Your business will go much further as the place that builds great surf boards than the place that builds okay skateboards, surfboards, sand boards and kite boards.
8. Give it up. Give up your business's time and money for a greater cause. Volunteer in the community to shed light on causes that either you are passionate about or that fall in line with your business philosophy. The time and money that you spend giving to others will come back to you ten-fold through good press, good will and a good reputation.
7. Be professional. If you want your business to be taken seriously, be professional in all your actions and communications. Fliers with dated clip-art that look like they were typed up in a word processor will scream amateur to potential clients and you'll be lucky if they even read the content you spent all night writing. On the flip side, a professional flier on high quality paper projects a higher-grade of business that has their act together and knows what they are doing.
6. Take care of your existing clients. It takes time and money to bring in new clients. Cut the amount of both in half and use the remaining to make sure your current clients are happy with your products and services. Get their opinions on their experience with your business and then take action on the things that were reviewed as subpar. Offer incentives for frequent buyers or users. You'll not only boost their loyalty to your business but you'll also grow the amount of good press about it.
5. Think outside the box. Consumers are blasted with so many messages a day, they've become experts at tuning them out. The trick is to catch them off guard in unexpected ways to reach them. I once saw a fish market that hired a local artist to chalk seafood on the sidewalks in a one mile radius from the store. It not only increased foot traffic but also introduced the young store to the local community in such a different way that it was written up in the community paper. We, as

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 105
consumers, like clever and unique ways to get our attention. Just remember to stay within the social and legal confines of your area.
4. Network. Not everyone inside your industry is your competition. We each have specialties that we excel in and many times, enjoy doing. Get to know others in your industry and learn their specialties. When a client is looking for something that isn't quite your cup of tea, refer them to someone who specializes in it. This not only harbors good will within the industry and builds your reputation but it also lets your clients know that you are looking out for their best interests, a thought that will keep them coming back.
3. Know it all. Become an industry expert within your niche. You know a lot about your business and can help show other people the way. Start by giving little presentations at your local chamber of commerce, then slowly move up into small trade shows and take off from there. Before you know it, you will become the "it" person whenever anyone has a questions about your industry. But be forewarned - it's a good idea to make sure you know what you're talking about. Not quite there yet? Read up and attend other experts' lectures and speeches until you're confident that you're prepared for all the criticism and questions that come along with calling yourself an expert.
2. Set goals. Without business goals you're a dead man (or woman) walking. How do you expect to grow your business without knowing where you're going? And while you're at it, put numbers to it; try to make your goals as objective as possible. Otherwise they'll end up like a new year's resolution, thrown out with the leftover turkey.
1. Measure Measure Measure. Our top marketing tip is to measure all of your marketing efforts. Ask customers how they heard about you, offer incentive for surveys filled out, use unique phone numbers and URLs to track your direct mail campaign. There are a billion and one ways to grow your business's visibility and now there are 2 billion ways to measure how they are working. Measure everything and then cut out the efforts that yield the lowest return on investment. You're a small business and don't have the budget of Pepsi-Cola to just throw marketing money down the drain.

106 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Rehab At-A-Glance

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 107

108 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 109

110 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 111

112 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Course Evaluation
Roger K. Campbell, M.S., CS, MFT-c.
The purpose of this evaluation is to gather input so that we may improve this course and how it is taught and therefore help you improve your learning. We are the only ones looking at your responses, and we will report back to you on the feedback received if you desire, you may email us at: [email protected] 1. What are the strongest features of this course and of our teaching? In other words, what contributes most to your learning experience?
2. What specific suggestions do you have for changes that we can make to improve the course or how it is taught?
3. Is the pace of the course: (Too Fast) (Just Right) (Too Slow)

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 113
About the Instructor
Roger K. Campbell, M.S., CET, MFT-c.
Roger started his exercise science career in 1983 as an Army Master Fitness Trainer, where he physically prepared troops
for combat readiness and sports performance. With the GI Bill, Campbell obtained a Bachelor of Science Degree in Exercise
Science from Utah State University, followed by a Master of Science Degree from the University of Utah, in Clinical Exercise
Physiology. While earning a masters degree, Campbell also served as the Health and Fitness Program Director of
the Murray City Fire Department, which focused on the human performance demands and physical integrity needs of
firefighters.
Campbell's greatest passion however, is working for the functional restoration and independence of medically complex
patients. While serving the University of Utah's Lung Transplant program, Campbell realized that greater restorative
measures could, and should, be implemented to improve functional abilities of patients, and has set his focus on their
rehabilitation pathway. Campbell spends his best energies devoted to developing, duplicating, and maintaining specialized
rehabilitation programs.
Campbell is the creator of www.gocancerrehab.com, a growing cancer rehabilitation network of care designed to increase
access to restorative services, delivered by physical medicine professionals caring for people touched by cancer. Campbell's
mission is the duplication of specialized rehabilitation programs in large and small communities alike.
Additionally, Campbell is committed to the educational development of health care professionals as a serving panel member
of the industries-first, accredited Cancer Specialist certification prepared by the American College of Sports Medicine
(ACSM) and the American Cancer Society (ACS).

114 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Suggested Reading:
The American Cancer Society www.cancer.org http://riskfactor.cancer.gov/areas/weight/ http://www.cancer.gov/cancertopics/factsheet/Risk/obesity http://www.cancer.gov/cancertopics/pdq/supportivecare/nutrition http://www.cancer.gov/cancertopics/chemotherapy-and-you http://www.cancer.gov/cancertopics/factsheet/Detection/staging http://www.cancer.gov/cancertopics/factsheet/Sites-Types/metastatic Oncology Nursing Society http://www.ons.org/clinical/prevention/risk/cancerRisk.shtml http://www.cancersymptoms.org/neutropenia/index.shtml National Lymphedema Network http://www.lymphnet.org/
ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities J. Larry Durstine and Geoffrey Moore Human Kinetics P. O. Box 507 Champaign, IL 61825-5076 1-(800)-747-4457 www.humankinetics.com Breast Cancer Recovery Exercise Program, 2nd ed. Anna Schwartz & Naomi Aaronson Desert Southwest Fitness http://www.dswfitness.com Cancer Fitness: Exercise programs for patients and survivors Anna Schwartz Simon & Schuster http://www.simonsays.com Exercise and Cancer Recovery Carol Schneider, Carolyn Dennehy, Susan Carter Human Kinetics P. O. Box 507 Champaign, IL 61825-5076 1-(800)-747-4457 www.humankinetics.com Handbook of Cancer Survivorship Michael (Ed) Feuerstein Springer New York, NY http://www.springer.com/public+health/book/978-0-387-34561-1

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 115
Cancer symptoms management (3rd ed) Connie Henke Yarbro, Margaret Hansen Frogge, Michelle Goodman Jones and Barlett Publishers Sudbury, MA http://www.jbpub.com/catalog/9780763721428/ Cancer Prevention and Management through Exercise and Weight Control Anne McTiernan Taylor & Francis Group http://www.taylorandfrancis.com Handbook of Cancer Survivorship Micheal Feurstein Exercise motivation and behavior change. (pp. 113-132). Springer www.springer.com (www.amazon.com)

116 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Cancer Rehabilitation Bibliography
Adamsen, L, Midtgaard, J., Rorth, M., Borregaard, N., Andersen, C., Quist, M., Meller, T., Zacho, M., Madsen, J.K., Knutsen L. Feasibility, physical capacity and multidimensional exercise program for cancer patients undergoing chemotherapy. Support Care Cancer. 2003; 11:707-716.
Agency for Healthcare Research and Quality: Effectiveness of Behavioral Interventions to Modify Physical Activity Behaviors in General Populations and Cancer Patients and Survivors. Rockville, MS, US Department of Health and Human Services, ASRQ publication 04-E027-2, 2004, pp 107-111.
Brockow, M.M., Exercise for women receiving adjuvant therapy for breast cancer (Review). The Cochrane Collaboration. Published by John Wiley & Sons, LTD 2007.
Brown, JK, Byers T., Doyle W, Et al Nutrition and Physical activity during and after cancer treatment: An American Cancer Society guide for informed choices. CA Cancer J Clin 2003; 53:268-291.
Blanchard, CM., Stein, KD, Baker, F, et al Association between current lifestyle behaviors and health-related quality of life in breast, colorectal and prostate cancer survivors. Pshcyol. Health 2004; 19:1-13.
Burnham, T.R. Wilcox, A. Effects of exercise on physiological and psychological variables in cancer survivors. Med Sci Sport Exerc. 2002; 34:1863-1867.
Coleman, M.P, Rachet, B., Woods, L.M. et al Trends and socioeconomic inequities in cancer survival in England and Wales up to 2001. Br. J. Cancer, 2004; 90:1367-1373.
Courneya, K Exercise in cancer survivors: An overview of research. Med Sci Sports Exerc 2003; 35:1846-1852.
Courneya, K. Friedenreich, C. Physical exercise and quality of life following cancer diagnosis A literature review. Ann Behav Med 2005; 21:171-179.
Courneya, K.S., Friedeneich, C.M., Framework PEACE: An organizational model for examining physical exercise across the cancer experience. Ann Behav Med 2001; 23:262-72.
Courneya, KS, Mackey JR, Bell, GJ, Jones, LW, Field, CJ, Fairey AS Randomized controlled trial of exercise training in postmenopausal breast cancer survivors: cardiopulmonary and quality of life outcomes J Clin Oncol 2003; 21:1660-1668.
Damush, T.M., Perkins, A., Miller, K. The implementation of an oncologist referred, exercise self-management program for older breast cancer survivors. Psycho-oncology 2006; 15:884-890.
Demark-Wahnefried, W., Pinto, B., M., Gritz, E. R. Promoting health and physical function among cancer survivors: Potential for prevention and questions that remain. J Clin Oncol 2006; 24:5125-5131.
Demark-Wahnefried, W., Peterson, B., McBride, C et al: Current health behaviors and readiness to pursue life-style changes among men and women diagnosed with early stage prostate and breast carcinomas. Cancer 2000; 88:674-684.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 117
Dimeo, FCHM, Tilmann, H., BErtz, L.Kanz, R., Mertelsmann, and J Keul Aerobic exercise in the rehabilitation of cancer patients after high dose chemotherapy and autologous peripheral stem cell transplantation. Cancer, 1997; 79:717-1722.
Doyle, C., Kushi, L.H., Byers, T., Courneya, K.S., Demark-Wahnefried, W., Grant, B. et al Nutrition and physical activity during and after cancer treatment: An American Cancer Society Guide for Informed Choices. 2006; 56: 323-353.
Durak, E.P., & Lilliy P.C. The application of an exercise and wellness program for cancer patients: a preliminary outcomes report. J. Strength Cond Res 1998; 12:3-6.
Galvao D.A., Newton R.U Review of exercise intervention studies in cancer patients. J. Clin Oncol 2005; 23: 899-909.
Holmes, M.D., Chen, WY, Feskanich D. et al Physical activity and survival after breast cancer diagnosis. JAMA 2005; 293:2479-86.
Hong, S., Bardwell, W.A., Natarajan, L., Flatt, S.W., Rock, C.L., Newman, V.,A., Madlensky, L., Mills, P.J., Misdale, J.E., Thomson, C.A., Hajek, R.A., Chilton, J.A., Pierce, J.P., Correlates of physical activity level in breast cancer survivors participating in the Women‘s Health Eating and Living (WHEL) Study. Breast Cancer Res Treat 2007; 101:225-232.
Humpel, N., Iverson, D.C. Review and critique of the quality of exercise recommendations for cancer patients and survivors. Supportive Care Cancer 2005; 23: 493-502.
Jemal, A., Murray, T., Samuels, A., Chafoor, A., Ward, E., Tun, M., Cancer statistics 2007. CA Cancer J Clin 2008; 53:5-26.
Jones, LW, Demark-Wahnefried W. Diet, exercise and complementary therapies after primary treatment for cancer. Lancet 2006; 7:1017-1026.
Jones, LS, Courneya, KS, Fairey, AS et al Effects of an oncologist‘s recommendation to exercise on self-reported exercise behavior in newly diagnosed breast cancer survivors: A single-blind randomized controlled trial. Ann Behav Med 2004; 28:105-113.
Keats, M.R., Courneya, K.S., Danileson, S., & Whitsett, S.F. Leisure time physical activity and psychosocial well-being in adolescents after cancer diagnosis. J. Pediatr Oncol. Nurs. 1999; 16:180-188.
Kendall, A.R., Mahue-Giangreco, M., Carpenter, C.L., Ganz, P.A., Leslie, B. Influence of exercise activity on quality of life in long-term breast cancer survivors. Qual Life Res. 2005;14:361-71.
Knols, R., Aaronson, N.K., Uebelhart, D., Fransen, J., Aufdemkampe, G. Physical exercise in cancer patients during and after medical treatment: A systematic review of randomized and controlled clinical trials. J. Clin Oncol 2005; 23: 38303842.
Korjstjen, I., Mesters, Ilse, M., vanDer Peet, E., Gijesen, B., van den Borne, B. Quality of life of cancer survivors after physical and psychosocial rehabilitation. European J. Ca Prev 2006; 15:541-547.
Lowe, SS, Watanabe, SM, Courneya, KS. Physical activity as a supportive care intervention in palliative care patients: A systematic review. (In Review).
Lui, RDK, Chinapaw, MJM, Huijgens, PC, van Mechelen, W. Physical exercise interventions in haematological cancer patients, feasibile to conduct but effectiveness to be established: A systematic literature review. Cancer Treat Rev, 2008; 10:1016-1020.

118 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
McKenzie, DC, Kalda, AL Effects of upper extremity exercise on secondary lymphedema in breast cancer patients: a pilot study. J. Clin Oncol 2003; 21:721-727.
Mc Neely ML, Parliament, M., Courneya, KS, et al A pilot study of a randomized controlled trial to evaluate the effects of progressive resistance exercise training on shoulder dysfunction caused by spinal accessory neurapraxia/neurectomy in head and heck cancer survivors. Head Neck 2004; 26:518-30.
McKelly, M., Kristin L Campbell, Rowe, B.H., Klassen, T.P., Mackey, J.R., Courneya, K.S. Effects of exercise on breast cancer survivors: a systematic review and meta-analysis. CMAJ 2006; 175:34-41.
McTiernan, A. Physical activity after cancer: Physiologic outcomes. Cancer Invest 2004; 22:68-81.
Meyerhardt, J.A. Giovannucci, E.L., Holmes, M.D. et al. Physical activity and survival after colorectal cancer diagnosis. J. Clin Oncol 2006; 24: 3527-34.
Meyerhardt, JA, Heseltine, D., Niedzwiecki, D. et al Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol 2006; 24:3535-41.
Milne, H.M., Wallman, K.E., Gordon, S., Courneya, K.S. Effects of a combined aerobic and resistance exercise program in breast cancer survivors: a randomized controlled trial. Breast Cancer Res Treat 2007;s10549-007.
Mitchell, T.L., Yakiwchuk, C.V., Griffin, K.L., Gray, R.E., Fitch, M.I. Survivor dragon boarding: A vehicle to reclaim and enhance life after treatment for breast cancer. Health Care for Women International. 2007;2:122-140.
Mock, V., Atkinson, A., Barsevick, A., Blackwell, S., Cella, D., Cianfrocca, ME, et al. NCCN (v.1.2003). Cancer-related fatigue clinical practice guidelines in oncology. J. Natl Comp Cancer Network 1:308-331, 2003.
Mutrie, N., Campbell, A.M., Whyte, F., McConnachie, A., Emslie, C., Lee, L., Kearney. N., Walkter, A., Ritchie, D. Benefits of supervised group exercise programme for women being treated for early stage breast cancer: programmatic randomized controlled trial. BMJ, doi:10.1136/bmj.39094.AE (published February 2007).
National Coalition for Cancer Survivorship (home page on the Internet). Glossary. (cited September 25, 2007). Available from: http://canceradvocacy.org/resources/glossary.aspx
Ohira, T., Schmitz, K.H., Ahmed, R.L., Lee, D. Effects of weight training on quality of life in recent breast cancer survivors. Cancer. 2006; 106, 2076-2083.
Pinto, BM, Maruyama, NC Exercise in the rehabilitation of breast cancer survivors. Psychooncology 1999; 8:191-206.
Porock, D.L., Kritjannson, L.J., Tinnelly, T., Duke, T., & Blight, J. An exercise intervention for advanced cancer patients experiencing fatigue: a pilot study. J. Palliat. Care 2000; 16: 30-36.
Rauscher, G.H., Hawley, S.T. Earp, J.A. Baseline predictors of initiation vs maintenance of regular mammography use among rural women. Prev Med 2005; 40:822-830.
Schmitz KS, Holtzman, J., Courneya, KS, et al Controlled physical activity trials in cancer survivors: Systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 2005; 14:1588-595.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 119
Schwartz, AL. Weight change in women who do and do not exercise during adjuvant chemotherapy for breast cancer. Cancer Practice. 2000; 8:231-237.
Schwartz, AL. Fatigue mediates the effects of exercise on quality of life in women with breast cancer. Quality of Life Research. 1999; 8:529-538.
Schwartz, AL. Cancer. In ACSM‘s Exercise Management for persons with chronic disease and disability. (2nd Edition). Human Kinetics. 2003. 166-172.
Schwartz, AL. Physical activity after a cancer diagnosis: Psychosocial outcomes. Cancer Invest 2004; 22:82-92.
Schwartz, A.L. (1999). Fatigue mediates the effects of exercise on quality of life in women with breast cancer. Quality of Life Research, 8, 529-538.
Schwartz, A. L., Meek., P.M., Nail, L.M., Fargo, J., Lundquist, M., Donofrio, M., Grainger, M., Throckmorton, T., Mateo, M. Measurement of fatigue. Determining minimally important clinical differences. J Clin Epidemiol 2002; 553: 239-44.
Schwartz, AL, Mori, M, Gao, R, Nail, LM, King, ME. Exercise reduces daily fatigue in women with breast cancer receiving chemotherapy. Med Sci Sports Ex. 2001; 33:718-723.
Schwartz, A.L., Thompson, J.T., Masood, N. (2002). Interferon Induced fatigue In Melanoma: A pilot study of exercise and methylphenidate. Oncology Nursing Forum 29,7 web feature.
Schwartz A.L., & Winters, K. Promoting Physical Activity in Cancer Survivors. In A. McTiernan (Eds). Physical Activity, Energy Balance, and Cancer: Etiology and Prognosis. Marcel Dekker Publishing; 2006.
Schwartz, A.L., Winters, K., Gallucci, B. Exercise effects on bone mineral density in premenopausal and postmenopausal women with breast cancer receiving adjuvant chemotherapy. Oncology Nursing Forum 2007; 34, 627-642.
Segal. R. J., Reid, R.D. Courneya, K. Resistance exerciser in men receiving androgen therapy for prostate cancer. J. Clin Oncol 2003; 21:1653-1659.
Segar ML, Katch VL, Roth RS, et al. The effect of aerobic exercise on self esteem and depressive and anxiety symptoms among breast cancer survivors. Oncol Nurs Forum. 1998;25(1):107-113.
Thorsen, L, Courneya, KS, Steninson, C, Fossa, SD. A systematic review of physical activity in prostate cancer survivors: outcomes, prevalence and determinants. Supportive Care Cancer. 2008;16:987-997.
Thorsen, L., Skovlund, E., Stomme, SB., Hornslien, K., Dahl, A., Fossa, S.D. Effectiveness of physical activity on cardiorespiratory fitness and health-related quality of life in young and middle-aged cancer patients shortly after chemotherapy. J Clinical Oncol. 2005; 23:2378-2388.
U.S. Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Washington DC: National Cancer for Chronic Disease Prevention and Health Promotion; 2005.
Vallance, J.K.H., Courneya, K.S., Jones, L.W., Reiman, T. Differences in quality of life between non-Hodgkin‘s lymphoma survivors meeting and not meeting public health exercise guidelines. Psycho-oncology 2005; 14:979-991.
Wilkie, D.J., Schwartz, A.L., Huang, H., Ko, N, Liao, W., Yu, D., Hairabedian, D., Zong, S. (2005). Computerized Aerobic Exercise Education for Patients Reduces Cancer-Related Fatigue. American Journal of Health Behavior.

120 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Winters, KM, Bennett, JA, Nail, L, Schwartz, AL. Strength, physical activity and age predictors in older breast cancer survivors. Oncol Nsg Forum. 2008; 35:815-821
Winters, K. & Schwartz, A.L. Quality of Life and Fatigue in Breast Cancer. In A. McTiernan (Eds). Physical Activity, Energy Balance, and Cancer: Etiology and Prognosis. Marcel Dekker Publishing; 2006.
Young-McCaughan, S., Mays, M.Z., Arzola, S.M., Yoder, L.H., Dramiga, S.A., Leclerc, K.M., Caton, J.R., Sheffler, R.L., Nowlin, M.U. Change in exercise tolerance, activity and sleep patterns and quality of life in patients with cancer participating in a structured exercise program. Oncol Nurs Forum. 2003;30,441-453.
Young-McCaughan, S., & Sexton, D.L. (1991). A retrospective investigation of the relationship between aerobic exercise and quality of life in women with breast cancer. Oncology Nursing Forum, 18, 751-757.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 121
Cancer Glossary
A
Acquired immune deficiency syndrome (AIDS)
AIDS is a viral disease that destroys the body's ability to fight infections, leaving the body susceptible to many other diseases. AIDS is also known as Autoimmune Immunodeficiency Syndrome
Acute
A sudden onset of symptoms or disease.
Adenocarcinoma
See Carcinoma.
Adenoma
A benign tumor made up of glandular tissue. For example, an adenoma of the pituitary gland may cause it to produce abnormal amounts of hormones.
Adrenal glands
Two small organs near the kidneys that release hormones.
AFP (Alpha fetoprotein)
A tumor marker.
Alopecia
The loss of hair, which may include all body hair as well as scalp hair.
Analgesic
Any drug that relieves pain. Aspirin and acetaminophen are mild analgesics.
Anemia
A condition in which a decreased number of red blood cells may cause symptoms including tiredness, shortness of breath, and weakness.
Anorexia
The loss of appetite.

122 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Antibody
A substance formed by the body to help defend it against infection.
Antiemetic agent
A drug that prevents or controls nausea and vomiting.
Antifungal agent
A drug used to treat fungal infections.
Antigen
Any substance that causes the body to produce natural antibodies.
Antineoplastic agent
A drug that prevents, kills, or blocks the growth and spread of cancer cells.
Arrhythmia
An irregular heartbeat.
Aspiration
The process of removing fluid or tissue, or both, from a specific area.
Autoimmunity
A condition in which the body's immune system mistakenly fights and rejects the body's own tissues.
Axilla
The armpit.
Axillary nodes
Lymph nodes - also called lymph glands found in the armpit (axilla).
B
Barium enema
The use of a milky solution (barium sulfate) given by an enema to allow x-ray examination of the lower intestinal tract.
Barium swallow

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 123
The use of a milky solution (barium sulfate) given orally to allow x-ray examination of the upper intestinal tract.
Benign growth
A swelling or growth that is not cancerous and does not spread from one part of the body to another.
Biopsy
The surgical removal of tissue for microscopic examination to aid in diagnosis.
Blood cells
Minute structures produced in the bone marrow; they consist of red blood cells, white blood cells, and platelets.
Blood count
The number of red blood cells, white blood cells, and platelets in a sample of blood.
Bone marrow
The spongy material found inside the bones. Most blood cells are made in the bone marrow.
Bone marrow biopsy and aspiration
The procedure by which a needle is inserted into a bone to withdraw a sample of bone marrow.
Bone marrow suppression
A decrease in the production of blood cells. Bone marrow suppression is a side effect of chemotherapy treatment in come cases
Bone marrow transplant
The infusion of bone marrow into a patient who has been treated with high dose chemotherapy or radiation therapy. Patients may use their own marrow, which in some cases has been frozen.
Allogeneic
The infusion of bone marrow from one individual (donor) to another.
Autologous
The infusion of a patient's own bone marrow previously removed and stored.

124 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Syngeneic
The infusion of bone marrow from one identical twin into another.
Bone scan
A picture of the bones using a radioactive dye that shows any injury, disease, or healing. This is a valuable test to determine if cancer has spread to the bone, if anticancer therapy has been successful, and if affected bony areas are healing.
Breast self-examination (BSE)
A manual self-examination of the breasts.
Bronchoscopy
The insertion of a flexible, lighted tube through the mouth into the lungs to examine the lungs and airways.
C
Cancer
A group of diseases in which malignant cells grow out of control and spread to other parts of the body. Find more information on Cancer.
Cancer in situ
The stage where the cancer is still confined to the tissue in which it started.
Candidiasis
A common fungal infection.
Carcinogen
A substance that causes cancer. For example, nicotine in cigarettes is a carcinogen that causes lung cancer.
Carcinoma
A type of cancer that starts in the skin or the lining of organs.
Adenocarcinoma
A malignant tumor arising from glandular tissue.
Basal cell carcinoma

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 125
The most common type of skin cancer.
Bronchogenic carcinoma
A cancer originating in the lungs or airways.
Cervical carcinoma
A cancer of the cervix (the neck of the uterus).
Endometrial carcinoma
A cancer of the lining of the uterus.
Squamous cell carcinoma
Cancer arising from the skin or the surfaces of other structures, such as the mouth, cervix, or lungs.
Cardiomegaly
An enlargement of the heart.
CAT scan (CT scan)
A test using computers and x-rays to create images of various parts of the body.
CEA (Carcinoembryonic antigen)
A blood tumor marker.
Cellulitis
The inflammation of an area of the skin (epithelial layer).
Central venous catheter
A special intravenous tubing that is surgically inserted into a large vein near the heart and exits from the chest or abdomen. The catheter allows medications, fluids, or blood products to be given and blood samples to be taken.
Cervical nodes
Lymph nodes in the neck.
Chemotherapy
The treatment of cancer with drugs is called chemotherapy.

126 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Adjuvant chemotherapy
Chemotherapy given to kill any remaining cancer cells, usually after all detectable tumor is removed by surgery or radiotherapy.
Combination chemotherapy
The use of more than one drug during cancer treatment.
Chronic
Persisting over a long period of time.
Colonoscopy
A procedure to look at the colon or large bowel through a lighted, flexible tube.
Colony-stimulating factor (CSF)
An injectable substance used to stimulate the bone marrow to produce more cells.
Colostomy
A surgical procedure by which an opening is created between the colon and the outside of the abdomen to allow stool to be emptied into a collection bag.
Colposcopy
Examination of the vagina and cervix with an instrument called a colposcope.
Congestive heart failure
A buildup of fluid in the lungs or extremities, or both (especially the legs). This occurs if the heart cannot pump the blood adequately.
Cyst
An accumulation of fluid or semisolid material within a sac.
Cystitis
An inflammation of the bladder.
D
Drug resistance
The result of cells' ability to resist the effects of a specific drug.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 127
Dysphagia
Difficulty in swallowing.
Dyspnea
Difficult or painful breathing; shortness of breath.
Dysuria
Difficult or painful urination.
E
Edema
The accumulation of fluid in part of the body.
Effusion
A collection of fluid in a body cavity, usually between two adjoining tissues. For example, a pleural effusion is the collection of fluid between two layers of the pleura (the lung's covering).
Electrocardiogram (EKG or ECG)
A test that takes recordings of the electrical activity of the heart.
Endoscopy
A procedure looking at the inside of body cavities, such as the esophagus (food pipe) or stomach.
Erythema
Redness of the skin.
Erythrocyte
The red blood cell that carries oxygen to body cells and carbon dioxide away from body cells.
Esophagitis
Inflammation of the esophagus (food pipe).
Estrogen
A female hormone produced primarily by the ovaries.

128 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Estrogen receptor assay (ER assay)
A test that determines if breast cancer is stimulated by the hormone estrogen.
Excision
Surgical removal.
Extravasation
The leaking of intravenous fluids or medications into tissue surrounding the infusion site. Extravasation may cause tissue damage.
F
Fine-needle aspirate
A procedure in which a needle is inserted, under local anesthesia, to obtain a sample for the evaluation of suspicious tissue.
Fistula
An abnormal opening between two areas of the body.
Frozen section
A technique in which tissue is removed and then quick-frozen and examined under a microscope by a pathologist.
G
Granulocyte
A type of white blood cell that kills bacteria.
Guaiac test
A test that checks for hidden blood in the stool.
H
Hematocrit (Hct)
The percentage of red blood cells in the blood. A low hematocrit measurement indicates anemia.
Hematologist
A doctor who specializes in the problems of blood and bone marrow.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 129
Hematology
The science that studies the blood.
Hematuria
Blood in the urine.
Hemoccult (Guaiac) test
A test that checks for hidden blood in the stool.
Herpes simplex
The most common virus that causes sores often seen around the mouth, commonly called cold sores.
Herpes zoster
A virus that settles around certain nerves causing blisters, swelling, and pain. This condition is also called shingles.
Hodgkin's disease
A cancer that affects the lymph nodes. See Lymphoma.
Hormones
Substances secreted by various organs of the body that regulate growth, metabolism, and reproduction.
Hospice
A concept of supportive care to meet the special needs of patients and family during the terminal stages of illness. The care may be delivered in the home or hospital by a specially trained team of professionals.
Human immunodeficiency virus (HIV)
The virus that causes AIDS.
Human leukocyte antigen test (HLA)
A special blood test used to match a blood or bone marrow donor to a recipient for transfusion or transplant.
Hyperalimentation
The intravenous administration of a highly nutritious solution.

130 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
I
Ileostomy
A surgical opening in the abdomen connected to the small intestine to allow stool to be emptied into a collection bag.
Immunity (Immune system)
The body's ability to fight infection and disease.
Immunosuppression
Weakening of the immune system that causes a lowered ability to fight infection and disease.
Immunotherapy
The artificial stimulation of the body's immune system to treat or fight disease.
Infiltration
The leaking of fluid or medicines into tissues, which can cause swelling.
Infusion
Delivering fluids or medications into the bloodstream over a period of time.
Infusion pump
A device that delivers measured amounts of fluids or medications into the bloodstream over a period of time.
Injection
Pushing a medication into the body with the use of a syringe and needle.
Intramuscular (IM) injection
Into the muscle.
Intravenous (IV) injection
Into the vein.
Subcutaneous injection
Into the fatty tissue under the skin.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 131
Interferon
A naturally produced chemical released by the body in response to viral infections. Interferon can be artificially produced and used as a form of immunotherapy.
Interleukin
A naturally produced chemical released by the body.
L
Laryngectomy
The surgical removal of the larynx.
Lesion
A lump or abscess that may be caused by injury or disease, such as cancer.
Leukemia
Cancer of the blood. White blood cells may be produced in excessive amounts and are unable to work properly.
Leukocyte
See White blood cell.
Leukopenia
A low number of white blood cells.
Lumpectomy
See Mastectomy-Segmental.
Lymphangiogram
A test to look at the lymph nodes.
Lymphatic system
A network that includes lymph nodes, lymph, and lymph vessels that serves as a filtering system for the blood.
Lymphedema
Swelling either from obstructed cancerous lymph nodes or from surgically removed lymph nodes.

132 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Lymph nodes
Hundreds of small oval bodies that contain lymph. Lymph nodes act as our first line of defense against infections and cancer.
Lymphocytes
White blood cells that kill viruses and defend against the invasion of foreign material.
Lymphoma
A cancer of the lymphatic system. Doctors differentiate the different lymphomas by the type of cell that is involved in the makeup of the tumor. Treatments depend on the type of cell that is seen.
M
Malignant tumor
A tumor made up of cancer cells of the type that can spread to other parts of the body.
Mammogram (Mammography)
A low-dose x-ray / picture of the breasts to determine whether abnormal growths or cysts are present.
Mastectomy
The surgical removal of the breast.
Mastectomy - Segmental (lumpectomy)
Removal of the lump and a small amount of surrounding breast tissue.
Mastectomy - Simple (modified mastectomy)
Removal of the entire breast.
Mastectomy - Radical
Removal of the entire breast along with underlying muscle and lymph nodes of the armpit.
Melanoma
A cancer of the pigment-forming cells of the skin or the retina of the eye.
Metastasize

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 133
To spread from the first cancer site, for example, breast cancer that spreads to the bone.
Monoclonal antibodies
Artificially manufactured antibodies specifically designed to find targets on cancer cells for diagnostic or treatment purposes.
MRI (Magnetic resonance imaging)
A sophisticated test that provides in-depth images of organs and structures in the body.
Mucosa (Mucous membranes)
The lining of the mouth and gastrointestinal tract.
Mucositis
Inflammation of the lining of the mouth or gastrointestinal tract.
Myelogram
An x-ray procedure by which a dye is injected into the spinal column to show any pathology of the spinal cord.
Myeloma
A malignant tumor of the bone marrow associated with the production of abnormal proteins.
Myelosuppression
A decrease in the production of red blood cells, platelets, and some white blood cells by the bone marrow.
N
Neoplasm
A new growth of tissue or cells; a tumor that is generally malignant.
Neutropenia
A decreased number of neutrophils, a type of white blood cell.
Non-Hodgkin's lymphoma

134 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
A cancer of the lymphatic system. Non-Hodgkin's lymphoma is related to Hodgkin's disease but is made up of different cell types. See Lymphoma.
O
OCN (Oncology certified nurse)
A registered nurse who has met the requirements and successfully completed a certification examination in oncology.
Oncologist
A doctor who specializes in oncology.
Oncology
The study and treatment of cancer. Doctors who specialize in oncology are called oncologists.
Oncology clinical nurse specialist
A registered nurse with a master's degree who specializes in the education and treatment of cancer patients.
P
Palliative treatment
Treatment aimed at the relief of pain and symptoms of disease but not intended to cure the disease.
Pap (Papanicolaou) smear
A test to detect cancer of the cervix.
Paracentesis
Removing fluid from the abdomen using local anesthesia and needle and syringe.
Pathological fracture
A break in a bone usually caused by cancer or some disease condition.
Pathology
The study of disease by the examination of tissues and body fluids under the microscope. A doctor who specializes in pathology is called a pathologist.
Petechiae

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 135
Tiny areas of bleeding under the skin, usually caused by a low platelet count.
Phlebitis
A painful inflammation of the veins.
Photosensitivity
Extreme sensitivity to the sun, leaving the patient prone to sunburns. This can be a side effect of some cancer drugs and radiation.
Placebo
An inert substance often used in clinical trials for comparison.
Platelet (Plt)
Cells in the blood that are responsible for clotting.
Platelet count
The number of platelets in a blood sample.
Polyp
A growth of tissue protruding into a body cavity, such as a nasal or rectal polyp. Polyps may be benign or malignant.
Port - Implanted
A catheter connected to a quarter-sized disc that is surgically placed just below the skin in the chest or abdomen. The tube is inserted into a large vein or artery directly into the bloodstream. Fluids, drugs, or blood products can be infused, and blood can be drawn through a needle that is stuck into the disc. Examples: Port-o-cath, Infusaport, Lifeport.
Port - Peritoneal
A catheter connected to a quarter-sized disc that is surgically placed in the abdomen. The catheter is inserted to deliver chemotherapy to the peritoneum (abdominal cavity).
Primary tumor
The original cancer site. For example, breast cancer that has spread to the bone is still called breast cancer.
Progesterone
One of the female hormones produced by the ovaries.

136 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Progesterone-receptor assay
A test that determines if breast cancer is stimulated by the hormone progesterone.
Prognosis
The projected outcome of a disease; the life expectancy.
PSA (Prostate-specific antigen)
A marker used to determine prostate disease; it may be benign or malignant.
Prosthesis
Artificial replacement of a missing body part.
Protocol
A treatment plan.
R
Radiation therapy
X-ray treatment that damages or kills cancer cells.
Radiologist
A doctor who specializes in the use of x-rays to diagnose and treat disease.
Recurrence
The reappearance of a disease after a period of remission.
Red blood cells (Erythrocytes)
Cells in the blood that deliver oxygen to tissues and take carbon dioxide from them.
Red blood count (RBC)
The number of red blood cells seen in a blood sample.
Regression
The shrinkage of cancer growth.
Relapse
The reappearance of a disease after its apparent cessation.

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 137
Remission
Complete or partial disappearance of the signs and symptoms of disease.
Risk factor
Anything that increases a person's chances of developing cancer, for example, smoking and lung cancer.
S
Sarcoma
A malignant tumor of muscles or connective tissue such as bone and cartilage.
Chondrosarcoma
A malignant tumor of cartilage that usually occurs near the ends of the long bones.
Ewing's sarcoma
A malignant tumor starting in bone, affecting the bones of extremities. It often appears before the age of 20.
Shingles
See Herpes zoster.
Side effects
Secondary effects of drugs used for disease treatment.
Sigmoidoscopy
The visual examination of the rectum and lower colon using a tubular instrument called a sigmoidoscope.
Sputum
Secretions produced by the lungs.
Staging
Determination of extent of the cancer in the body.
Steroids
A type of hormone.

138 Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited.
Stoma
An artificial opening between two cavities or between a cavity and the surface of the body.
Stomatitis
Temporary inflammation and soreness of the mouth.
Systemic disease
A disease that affects the entire body instead of a specific organ.
T
Taste alteration
A temporary change in taste perception.
Testicular self-examination (TSE)
A simple manual self-examination of the testes.
Thoracentesis (Pleural tap)
A procedure to remove fluids from the area between the two layers (pleura) covering the lung.
Thrombocytopenia
An abnormally low number of platelets (thrombocytes). If the platelet count is too low, bleeding could occur.
Tracheostomy
A surgical opening through the trachea in the neck to provide an artifical airway.
Tumor
An abnormal overgrowth of cells. Tumors can be either benign or malignant.
U
Ultrasound examination
The use of high frequency sound waves to aid in diagnosis.
Ureterostomy

Rehabilitation Systems 2010 Copying or distributing without written consent is prohibited. 139
A surgical procedure consisting of cutting the ureters from the bladder and connecting them to an opening (see Stoma) on the abdomen, allowing urine to flow into a collection bag.
V
Venipuncture
Puncturing a vein in order to obtain blood samples, to start an intravenous drip, or to give medication.
Vesicant
A medication or agent that may cause blistering.
Virus
A tiny infectious agent that is smaller than bacteria. The common cold is caused by a virus, and the herpes simplex virus causes cold sores.
W
White blood cells (WBC)
General term for a variety of cells responsible for fighting invading germs, infection, and allergy-causing agents. Specific white blood cells include granulocytes and lymphocytes.
White blood count (WBC)
The actual number of white blood cells seen in a blood sample.
X
X-ray
High-energy electromagnetic radiation used to diagnose and treat disease. Diagnostic test using high energy to visualize internal body organs. See Radiation therapy.