Cancer in Idaho: Data Update & Strategic Plan Objectives Idaho Cancer Policy Agenda Meeting April...
79
Cancer in Idaho: Data Update & Strategic Plan Objectives Idaho Cancer Policy Agenda Meeting April 25, 2014 Chris Johnson, Epidemiologist Cancer Data Registry of Idaho [email protected]
-
Upload
jennifer-lyons -
Category
Documents
-
view
213 -
download
0
Transcript of Cancer in Idaho: Data Update & Strategic Plan Objectives Idaho Cancer Policy Agenda Meeting April...

Cancer in Idaho: Data Update &
Strategic Plan Objectives
Idaho Cancer Policy Agenda MeetingApril 25, 2014
Chris Johnson, EpidemiologistCancer Data Registry of Idaho

2
3 Handouts

3
Cancer
• 100+ different diseases• Since 2008, #1 cause of death in Idaho
– About 22% of deaths are from cancer• In 2011 in Idaho:
7,263 new invasive cases
849 new in situ cases
2,559 cancer deaths
30% of those diagnosed this year will die of cancer within five years

4
Leading Cause of Death by AgeIdaho 2012
• Cancer is the leading cause of death among age groups 45-54, 55-64 and 65-74

5
Trends in Crude Mortality Rates, Idaho

6
Why is Cancer the Leading Cause of Death in Idaho?
• Competing risks– Why are heart disease/stroke deaths down?
• “Statins and Smoking”– Decreases in blood cholesterol levels and
uncontrolled hypertension (risk factors), mostly through medication
– Improvements in medical treatments for blocked arteries, stroke
– Lower smoking rates in Idaho

7
Cancer Risk Factors

8
Levels of Disease Prevention
• Primary Prevention– Aims to prevent the disease from
occurring– Reduces incidence
• Secondary Prevention– After the disease has occurred but
before symptoms– Aims to find and treat disease early
• Tertiary Prevention– Goals are to improve treatment
outcomes, prevent complications

9
Measures of cancer burden:
incidence, mortality,
YPLL
Colon & Rectum Cancer
Behavior: smoking, physical activity, diet, screening
Lung Cancer, Tobacco, other
Tobacco-related Cancers
Melanoma Breast Cancer

Lung Cancer/Smoking Constellation

11
Lung Cancer
• Idaho 2011:– 838 new cases – 616 deaths
• By far the leading cause of cancer death among both men and women – Each year, more people die of lung cancer than
of colon, breast, and prostate cancers combined– Lung cancer has a poor prognosis; nearly 90%
of persons with lung cancer die of the disease

12
Lung Cancer Risk Factors
• Smoking causes ~85% of lung cancer deaths• Radon – 2nd leading cause of lung cancer
– About 10% of lung cancer deaths– Leading cause of lung cancer among non-
smokers• Secondhand smoke• Asbestos, arsenic, chromium, nickel, other
substances in workplace• Air pollution, including diesel exhaust

13
Smoking
• Accounts for at least 30% of all cancer deaths
• Population attributable risk varies by cancer site for other smoking-related cancers:
– Larynx– Oral Cavity– Nose and
Sinuses– Pharynx– Esophagus
– Stomach– Pancreas– Cervix– Kidney– Bladder– Ovary
– Colon & Rectum– AML

14
Counseling & Interventions
• The USPSTF recommends that clinicians ask all adults about tobacco use and provide tobacco cessation interventions for those who use tobacco products.– Grade: A recommendation: there is high certainty
that the net benefit is substantial.

15
USPSTF Screening Recommendation (Dec 2013)
• The USPSTF recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults ages 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years.– Screening should be discontinued once a person has
not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery.
• Screening cannot prevent most lung cancer–related deaths, and smoking cessation remains essential.

16
Drilling Down into CCAI Strategic Plan Measures
2. Reduce the lung cancer death rate
6. Reduce the oropharyngeal cancer death rate
18. Decrease the proportion of adults aged 18+ who are current smokers
19. Reduce tobacco use by adolescents
23. Reduce the proportion of males who use smokeless tobacco

17
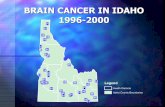
Lung Cancer State Map

18
Lung Cancer Trends - Idaho

19
Lung Cancer Age-Specific Rates, Idaho, 2007-2011

20
Variation and Disparities in Lung Cancer in Idaho
• Geographic• Race/ethnicity• Area-based SES measures

21
County Maps of Smoking and Lung Cancer Incidence & Mortality
Smoking 11-12 Inc 07-11 Mort 08-12
1
2
3
4
5
7
6
Idaho
Owyhee
Lemhi
Custer
Valley
Elmore
Butte
Blaine
Cassia
Boise
Clark
Bonner
Ada
Shoshone
Bingham
Clearwater
CaribouPower
Fremont
Adams
Latah
Twin Falls
Bonneville
Oneida
Camas
Kootenai
Boundary
Washington
JeffersonGem
Benewah
Jerome
Lincoln
Bannock
Bear Lake
GoodingMinidoka
Lewis
Franklin
Nez Perce
Canyon
TetonMadison
Payette
1
2
3
4
5
7
6
Idaho
Owyhee
Lemhi
Custer
Valley
Elmore
Butte
Blaine
Cassia
Boise
Clark
Bonner
Ada
Shoshone
Bingham
Clearwater
CaribouPower
Fremont
Adams
Latah
Twin Falls
Bonneville
Oneida
Camas
Kootenai
Boundary
Washington
JeffersonGem
Benewah
Jerome
Lincoln
Bannock
Bear Lake
GoodingMinidoka
Lewis
Franklin
Nez Perce
Canyon
TetonMadison
Payette
1
2
3
4
5
7
6
Idaho
Owyhee
Lemhi
Custer
Valley
Elmore
Butte
Blaine
Cassia
Boise
Clark
Bonner
Ada
Shoshone
Bingham
Clearwater
CaribouPower
Fremont
Adams
Latah
Twin Falls
Bonneville
Oneida
Camas
Kootenai
Boundary
Washington
JeffersonGem
Benewah
Jerome
Lincoln
Bannock
Bear Lake
GoodingMinidoka
Lewis
Franklin
Nez Perce
Canyon
TetonMadison
Payette

22
Smoking Prevalence, Idaho 2012
* In 2012, about 190,000 adult smokers in Idaho.

23
Smoking Prevalence, Idaho 2012

24
Smoking Prevalence, Idaho 2012

25
Area-Based Measures
• Used methods based on Harvard School of Public Health Disparities Geocoding Project– Geocoded cancer incidence data– Used area-based socioeconomic measures
(ABSMs) to characterize both the cases and population
– Computed rates stratified by the area-based measure of socioeconomic status
– Ran multilevel models and will be showing the effects that were statistically significant

26
Census Tract 2010Poverty
American Community Survey 2007-2011
1
2
3
4
5
7
6
Idaho
Owyhee
Lemhi
Custer
Valley
Elmore
Butte
Blaine
Cassia
Boise
Clark
Bonner
Ada
Shoshone
Bingham
Clearwater
CaribouPower
Fremont
Adams
Latah
Twin Falls
Bonneville
Oneida
Camas
Kootenai
Boundary
Washington
JeffersonGem
Benewah
Jerome
LincolnBannock
Bear Lake
GoodingMinidoka
Lewis
Franklin
Nez Perce
Canyon
TetonMadison
Payette
Census Tracts 2010
Census_Tract_Poverty_ACS_0711
0% - <5% poverty
05% - <10% poverty
10% - <20% poverty
20% + poverty

27
Census Tract 2010Uninsured
American Community Survey 2008-2012
1
2
3
4
5
7
6
Idaho
Owyhee
Lemhi
Custer
Valley
Elmore
Butte
Blaine
Cassia
Boise
Clark
Bonner
Ada
Shoshone
Bingham
Clearwater
CaribouPower
Fremont
Adams
Latah
Twin Falls
Bonneville
Oneida
Camas
Kootenai
Boundary
Washington
JeffersonGem
Benewah
Jerome
Lincoln
Bannock
Bear Lake
GoodingMinidoka
Lewis
Franklin
Nez Perce
Canyon
TetonMadison
Payette
Census Tracts 2010
Census_Tract_Uninsured_ACS_0812
<15% uninsured
15% - <25% uninsured
25% - <35% uninsured
35%+ uninsured

28
Lung Cancer Incidence by Census Tract % Uninsured

29
Potentially Averted Lung Cancer Cases, 2007-2011
Area Uninsured Status Person-Years Observed Expected Cases Percent<15% uninsured 1,588,827 606 606 - 0.0%15% - <25% uninsured 2,961,564 1,499 1,293 206 13.7%25% - <35% uninsured 2,123,378 1,320 1,022 298 22.5%35%+ uninsured 1,074,624 708 490 218 30.7%Total 7,748,393 4,133 3,412 721 17.4%
Expected counts = age-specific rates from low uninsured area applied to populations of other areas.
Uninsured Status-Related Population Attributable FractionLung & Bronchus Cancer Incidence, Idaho, 2007-2011
Case Counts Potentially Averted

30
Lessening the Burden from Lung Cancer
• Primary Prevention– Don’t smoke!– Test for radon
• Secondary Prevention– LDCT among high risk population
• Tertiary Prevention– Ensure quality treatment
• Access to care• Concordant with guidelines (e.g. NCCN)• Clinical trials

31
Using the Drill-Down Results
• Target geographic areas• Disparities by:
– Income– Education– Uninsured– LGBT

Colon & Rectum Cancer Constellation

33
Colon & Rectum Cancer
• Idaho 2011:– 639 new invasive cases– 17 new in situ cases– 222 deaths
• Of cancers affecting both men and women, second leading cause of cancer death

34
Colon & Rectum Cancer Risk Factors
• UK (2011) study estimates 54% of colon & rectum cancer cases are attributable to lifestyle factors:
Br J Cancer. 2011; 105(Suppl 2): S77–S81.
– Red and preserved meat consumption (21%)– Overweight and obesity (13%)– Low fiber diet (12%)– Alcohol (12%)– Tobacco (8%)– Physical inactivity (3%)– Other [infections, radiation] (4%)
• The percentages reflect the effect of removing one cause of cancer independently of other causes, and there is overlap, so the total is less than the sum

35
USPSTF Recommendation (Oct 2008):
• The USPSTF recommends screening for colorectal cancer using fecal occult blood testing, sigmoidoscopy, or colonoscopy in adults beginning at age 50 years and continuing until age 75 years.– Grade: A recommendation – there is high
certainty that the net benefit is substantial.

36
Colorectal Cancer Screening
• CDC: “If everyone aged 50 years or older had regular screening tests, at least 60% of deaths from this cancer could be avoided.”
• Colorectal cancer screening helps find precancerous polyps so they can be removed before they turn into cancer. In this way, colorectal cancer is prevented.
• Screening tests also can find colorectal cancer early, when the chance of cure is better.

37
CCAI Strategic Plan ObjectivesPertaining to Colon & Rectum Cancer
• 5 – Mortality• 9 – Incidence• 15 – Late stage CRC among persons aged 50+• 16 – CRC Screening• 21 – Overweight• 22 – Physical activity

38
Colon & Rectum Cancer State Map

39
Colorectal Cancer ScreeningIdaho 2012, Ages 50-75

40
Colorectal Cancer ScreeningIdaho 2012, Ages 50-75

41
Colorectal Cancer ScreeningIdaho 2012, Ages 50-75

42
Colon & Rectum Cancer Trends

43
Colon & Rectum Cancer Incidence by Race/Ethnicity, 2007-2011
Race/Ethnicity Count Pop Rate Rate Ratio Ratio P-ValueNon-Hispanic White 2,872 6,623,464 39.2Hispanic (any Race) 97 848,174 32.7 0.83 0.120Black 9 74,451 31.8 0.81 0.662American Indian/Alaska Native 38 144,202 46.8 1.20 0.379Asian or Pacific Islander 26 126,108 31.7 0.81 0.332

44
Colon & Rectum Cancer Incidence by Census Tract % Poverty

45
Potentially Averted Colon & Rectum Cancer Cases, 2007-2011
Area Uninsured Status Person-Years Observed Expected Cases Percent0% - <5% poverty 528,593 161 161 - 0.0%5% - <10% poverty 2,015,643 770 654 116 15.0%10% - <20% poverty 3,905,375 1,639 1,386 253 15.5%20% + poverty 1,298,778 497 380 117 23.5%Total 7,748,389 3,067 2,581 486 15.8%
Expected counts = age-specific rates from low poverty area applied to populations of other areas.
Poverty Status-Related Population Attributable FractionColorectal Cancer Incidence, Idaho, 2007-2011
Case Counts Potentially Averted

46
Lessening the Burden from Colon & Rectum Cancer
• Primary Prevention– Healthy diet, Healthy BMI, Physical activity– Don’t smoke
• Secondary Prevention– Colon & rectum cancer screening
• Tertiary Prevention– Ensure quality treatment
• Access to care• Concordant with guidelines (e.g. NCCN)• Clinical trials

47
Using the Drill-Down Results
• Target geographic areas• Disparities by:
– Income– Education– Area-based SES

Breast Cancer Constellation

49
Breast Cancer (Female)
• Idaho 2011:– 1,006 new invasive cases– 225 new in situ cases– 194 deaths
• Among Idaho women, breast cancer is:– the most common cancer (incidence)– 2nd most common for mortality

50
Breast Cancer Risk Factors• Risk Factors you Cannot Change
– Aging – Race and ethnicity– Genetic risk factors
• 5-10% of breast cancers are hereditary• BRCA1 and BRCA2
– Family history• 15% of women who get breast cancer have a
family history; 85% do not.– Dense breast tissue– Certain other breast conditions (LCIS, DCIS,
atypical ductal or lobular hyperplasia) – Number of menstrual cycles– Previous chest radiation– Diethylstilbestrol exposure

51
Breast Cancer Risk Factors
• Lifestyle-related factors– Birth control– Hormone therapy after menopause– Drinking alcohol– Being overweight or obese after menopause– Lack of physical activity
• Unclear factors– Chemicals in the environment– Tobacco smoke– Night work

52
Idaho Breast Cancer Trends

53
30% Reduction In Breast Cancer Mortality Since 1980s
• How much due to screening?– Goal is to treat cancer earlier, when a cure is
more likely• How much due to treatment?
– Adjuvant tamoxifen lowers breast cancer mortality by nearly a third in long term studies of women with ER+ breast cancers (about 75 percent of those diagnosed) • There were greater improvements in mortality
among women with ER+ than ER- tumors (SEER 1990-2003).

54
Mammography Screening Recommendations
for Women at Average Risk
• Women at higher risk of breast cancer may need to be screened earlier and more often than other women.
American Cancer Society
National Cancer Institute
National Comprehensive Cancer Network
United States Preventive
Services Task Force
Every year starting at age 40
Every 1-2 years starting at age 40
Every year starting at age 40
Every 2 yearsAges 50-74

55
JAMA Review – Pace & KeatingApril 2014
• 450 articles from 1960 to 2014 reviewed for evidence on the mortality benefit and chief harms of mammography screening.– Mortality benefit of mammography is “modest”
• 15% reduction of breast cancer mortality for women in their 40s, and 32% for women in their 60s.
– Risks of harm from screening are “significant”• Over 10 years of annual mammograms, 61% with
false-positive result.• 19% of cancers represent overdiagnosis
– Clinicians must focus on informed screening decisions based on individual risk of a breast cancer diagnosis.

56
CCAI Strategic Plan ObjectivesPertaining to Breast Cancer
• 3 – Mortality• 11 – Late stage incidence rate ages 40+• 17A- Biennial mammogram 40+• 17B- Biennial mammogram 50-74

57
Breast Cancer Mortality

58
Breast Cancer Incidence

59
Mammography ScreeningIdaho 2012, Females 40+

60
Lessening the Burden from Breast Cancer
• Primary Prevention– Overweight and obesity, Physical activity
• Secondary Prevention– USPSTF – recommends biennial screening
mammography for women aged 50 to 74 years• Tertiary Prevention
– Ensure quality treatment• Access to care• Concordant with guidelines (e.g. NCCN)• Clinical trials

Melanoma of the Skin Constellation

62
Melanoma of the Skin
• Idaho 2011:– 443 new invasive cases– 385 new in situ cases– 57 deaths.
• Melanoma is the 5th most common cancer in Idaho in terms of incidence and 14th most common site for cancer deaths.
• Unreported cases from in-office labs continues to be an issue for most states.– Meaningful Use 2 may help improve melanoma
reporting.

63
USPSTF Recommendations:
• [2009] Not enough evidence to recommend for or against routine screening (total body examination by a doctor) to find skin cancers early.
• [2012] Recommends counseling children, adolescents, and young adults aged 10 to 24 years who have fair skin about minimizing their exposure to ultraviolet radiation to reduce risk for skin cancer.– Insufficient evidence to assess the balance of
benefits and harms of counseling adults older than age 24 years.

64
CCAI Strategic Plan ObjectivesPertaining to Skin Cancer
• 8 – Mortality• 27 – Tanning appliances grades 9-12• 28 – Sunburn adults• 29 – Tanning appliances adults

65
Melanoma of the Skin Mortality

66
Melanoma of the Skin Incidence

67
Melanoma of the Skin Trends

68
Sunburn among Adults, Idaho 2012

69
Sunburn among Adults, Idaho 2012

70
Indoor Tanning among AdultsIdaho 2012

71
Indoor Tanning among AdultsIdaho 2012

72
Indoor Tanning among ChildrenIdaho 2013

73
Lessening the Burden from Melanoma of the Skin
• Primary Prevention– Avoiding excessive sun exposure– Avoiding intense, intermittent, UV exposure– Preventing sunburns– Prompt self-referral to physician for changing nevi
• Secondary Prevention– USPSTF – not enough evidence to recommend
for or against routine screening• Tertiary Prevention
– Ensure quality treatment• Access to care, guidelines, clinical trials

74
Using the Drill-Down Results
• Target geographic areas • Focus on the young and the affluent for sunburn
– Young females for indoor tanning

75
Hospitals & Clinical Trials

76
American College of SurgeonsCommission on Cancer (CoC)
Cancer Programs in Idaho (n=7)
• Eastern Idaho Regional Medical Center• Kootenai Medical Center• Portneuf Medical Center• Saint Alphonsus Regional Medical Center• St. Joseph Regional Medical Center• St. Luke's Magic Valley Medical Center• St. Luke’s Regional Medical Center/MSTI
– About 70% of Idaho resident cancer cases seen at one of these facilities

77
Clinical Trial Enrollment

78
The Future of Cancer in Idaho
• As Idaho’s population increases and we live longer, we can expect more cases of cancer and cancer deaths in the future

79
Lessening the Burden• Primary Prevention – Decreases Incidence
– Don’t smoke! Test for radon– Obesity & physical activity– Skin cancer prevention– Vaccinations for Hep B and HPV
• Secondary Prevention - Screening– Breast– Colorectal– Lung
• Tertiary Prevention - Ensure Quality Treatment– Access to care, Clinical trials– Concordant with guidelines (e.g. NCCN)