
C. difficile Terapia
19
12/10/2011 1 C. difficile: Terapia Francesco G. De Rosa Clinica Malattie Infettive Università di Torino Torino 30 Settembre 2009 Normal colon Thickened colon Arrows show thumbprinting Wolf, P. L. et al. N Engl J Med 2005;353:2491
Transcript of C. difficile Terapia

12/10/2011
1
C. difficile:Terapia
Francesco G. De RosaClinica Malattie Infettive
Università di Torino
Torino 30 Settembre 2009
Normal colonThickened colon
Arrows show thumbprinting
Wolf, P. L. et al. N Engl J Med 2005;353:2491

12/10/2011
2
CLOSTRIDIUM DIFFICILE COLITIS

12/10/2011
3
DIAGNOSIS
� Diarrhea within 6 weeks of antibiotic treatment
� Stool
� Mushy or liquid, varying color (may be green)
� WBCs 1/3, RBCs 1/3
� Endoscopy – for more severe or cryptic cases
� Toxin assay, positive for Toxin B (or A/B)
� Stool culture – for research or epidemiology
Logistic Regression Analysis for Prediction of Posi tive Result
of Assay for Clostridium difficile Toxin in Stool
Variable Odds ratio P
Watery diarrhea 17.4 .000
Functional capacity score of 2 or 3 9.14 .000
Use of proton pump inhibitor 6.1 .024
Albumin level <2.7 mg/dL 3.8 .001
Use of H2 blocker 3.1 .024
WBC count >13,000 cells/mL 2.7 .004
Peled et al, 2007

12/10/2011
4
C. DIFFICILE TOXINS
• Toxin A (TcdA, 308 kDa), an enterotoxin• Toxin B (TcdB, 260 kDa), a cytotoxin• Both toxins act as glycosyltransferases
and modify small GTPases within the host cell that are involved in actin polymerization and cytoskeleton structure
• Both toxins play a role in the clinical disease
THE THIRD TOXINBINARY TOXIN CDT
• Binary toxin CDT is unrelated to TcdA and TcdB but instead is related to the group of clostridial binary toxins that consist of 2 unlinked molecules. This toxin is an ADP-ribosyltransferase and, like the large clostridial toxins, ultimately acts by disruption of the host's actin cytoskeleton
• Encoded by the cdtA gene, the enzymatic component, and the cdtB gene, the binding component
• CDT <10% usual CDAD strains, but in all epidemic strains (designated REA group BI)

12/10/2011
5
McFarland, Future Microbiol 2008
RISK OF CDAD WITH VARIOUS ANTIMICROBIAL DRUGS
High risk antimicrobials• 2nd & 3rd generation cephalosporins• Clindamycin• Fluoroquinolones, especially gati, moxi, levoIntermediate risk antimicrobials• Ampicillin, amoxicillin/clav, Pip/tazo, Ticar/clav• TMP/SMX• MacrolidesLow risk antimicrobials• Aminoglycosides• Vancomycin• Metronidazole

12/10/2011
6
CDAD -NEW DEVELOPMENTS
• Increases in both sexes
• Increases most prominent in >65 years of age
• Highest rates in Northeast and Midwest
• Highest rates and recent increases in midsized hospitals (200-400 beds)
• More cases from the community (1/3rd ); many without antibiotic or health-care exposures
• Higher mortality (14% attributable mortality in Montreal)
• More colectomies
NEW EPIDEMIC STRAIN OF CLOSTRIDIUM DIFFICILE
• REA BI, PFGE type NAP1, PCR-ribotype 027, toxinotype III (formerly present in only 2-3% of hospital isolates)
• NAP1/027 produces 16 times more toxin A and 23 times more toxin B
• tcdC 18-bp deletion • Produces binary toxin • Frequently resistant to fluoroquinolones
and clindamycin
Lancet, 2005

12/10/2011
7
States with BI/NAP1/027 strain of C. difficile(N=38), November, 2007
DC
PRAK
HI
McFarland, Future Microbiol 2008

12/10/2011
8
CDI IN OHIO, 2006
Campbell et al, 2009
UPDATE ON CDI - 2008
• The U.S. experiences approximately 500,000 hospital-based cases and 150,000 community-based cases of CDI annually, with total projected annual costs of approximately $1.3 billion
• CDI reported in 23 European Union (EU) countries and is responsible for 1.1/1,000 hospital admissions. Cases of NAP1 rising, but also other epidemic serotypes are reported (Types 078, 106 & 00l).
• In EU, CDI deaths are rapidly increasing, with a 69% increase from 2004-2005 in England and Wales
• In 2002–06, deaths in the UK involving CDI = 13,189 compared with MRSA = 5,109.

12/10/2011
9
Redelings MD, et al. Emerg Inf Dis. 2007;13(9):1417-1419.
Increasing Mortality of CDI: US and UK
17
Number of death certificates mentioning Clostridium difficile and recording Clostridium difficile as the underlying cause of death, England and Wales (Note, there is no data available for 2000) from Office for National Statistics
US: 1999-2004 England and Wales: 1999-2007

12/10/2011
10
IDSA/SHEA DRAFT GUIDELINES FOR TREATMENT OF CDI (2007)
• Initial, mild-moderate– Metronidazole 500 mg po tid for 10-14 d
• Initial, severe– Vancomycin 125 mg qid 10-14 d
• Initial, complicated– No ileus, Vancomycin 500 mg po or by NG
tube qid – Ileus, Vancomycin and metronidazole, po & IV
Clostridium difficile:Sanford Medical GuidePrimary Alternative Comments
Po possibleWBC <20.000/mm 3
Metro 500 mg po x3 or 250 mg x4 /die x 10-14 days
Vanco 125 mg po x4 x10-14 days or teico 400 mg po x2/die x 10 days
Stop antibiotics if possible; relapse = 10-20%Nitazoxanide
Po possibleWBC >20.000/mm 3
Vanco 125 mg po x4 x10-14 days
Metro 500 mg po x3 x 10 days
Metro probably not as effective in severely ill patients
Post-treatment relapse
1st RelapseMetro 500 mg po x3 x 10 days
2nd RelapseVanco 125 mg po x4 x10-14 days +Rif 300 mg po x2/die
3rd RelapseVanco taper: 125 x4 x week1, bid x 1week, od x 1 week, qod x 1 week, q3d x 2-3 weeks
Post-op ileusSevere disease and toxic megacolon
Metro 500 mg iv x4/die + vanco via nasogastric tube +retrograde catheter in cecum
Vanco instillation into bowel: 500 mg to 1 liter of saline and perfuse at 1-3 ml / min to maximum of 2 grams / 24h;IV vanco not effectiveIG IV: anecdotal reports

12/10/2011
11
Relapsing C. difficile Colitis
• 20-30% of cases• Not related to severity of diarrhea, inciting
antibiotic or length of diarrhea• Strain and sensitivity is usually the same• In hospital, relapse confused with reinfection• Retreatment with the original drug possible • Half of patients have a second relapse within
4 weeks

12/10/2011
12
• Olanda, 2005 � 2008• Ceppi 027 e 078 a confronto• Incidenza 078: 3% � 13%• Caratteristiche:
– Più giovani: 67 Vs. 73 aa (p<0.01)– Comunitari: 17.5% Vs. 6.7%, OR 2,98– Terapia con FQ: 29.4% Vs. 19.8% (OR 1.02)
• 078 umano e suino sono geneticamente correlati
COMMUNITY-ACQUIRED CDAD (CA-CDAD)
6.9/100,000 (CT)7.6/100,000 (Phil)22.0/100,000 (UK)
• 22% no antibiotic exposure*• 71% no prior hospital exposure*• 25% no risk factors or underlying disease*
*Experience in Connecticut based on state-wide surveillance, 2006MMWR, 2008

12/10/2011
13

12/10/2011
14
NEW PRODUCTS FOR C. DIFFICILE
DRUG MECHANISM OF ACTION
Xifaxan®(rifaximin)
Semi-synthetic, non-absorbed rifamycin approved for E. coli diarrhea. Currently in Phase 3 trial
TolevamerOrally administered, non-absorbed polymer that binds Toxins A & B in the GI tract. Failed in 2 Phase 3 trials
Vaccine (Acambis) Toxoid vaccine targeting Toxins A & B, entering Phase II
Alinia®(nitazoxanide)
Nitrothiazole benzamide, Related to metronidazole, currently in Phase 3 trials
Mucomilk Bovine whey protein anti-C. difficile IgG delivered to colon, under study
Medarex/MBL Monoclonal antibody to Toxin A/B successful Phase 2 trial
Opt-80 (Fidaxomicin)18-membered macrocycle oral antibiotic derived from fermentation, completed one Phase 3 trial
Under ConsiderationTigecycline, daptomycin, teicoplanin, generic vancomycin, non-toxigenic C.diff (MS type) entering Phase 2 trials
COMPARATIVE TRIALS IN CDI
Cure Rates Recurrence Rates
82.9% 81.4%
70%
90%
29%
23.3%
0%
10%
20%
30%92.1%
13.3%
89.8%
80%
24.0%
OPT-801 Vanco1 Vanco2 Metro2 OPT-801 Vanco1 Vanco2 Metro2
100%
1. Based on Per Protocol population in the 1st OPT-80 Phase III CDI study in 2008.2. Tolevamer Poster# 3826 ‘Results of a Phase III Trial Comparing Tolevamer, Vancomycin and Metronidazole in Patients with Clostridium difficile-Associated Diarrhea (CDAD)’ at ICAAC in Chicago 2007.

12/10/2011
15
• 50, 100, 200 mg bid x 10 gg• Alte concentrazioni fecali, basse le
plasmatiche• Efficacia misurata su scomparsa della
diarrea dopo 10 giorno:– 10/14 = 71%, 12/15 = 80%, 15/16 = 94%
• Relapse = 5%
Activity of MetronidazoleBaynes SA et al JAC 2009
• C. difficile strains (2005–06) were studied and compared with historic isolates (1995–2001)
• Ribotypes 001 (n 586), 106 (n 581) and 027 (n 548)
• 21 (24.4%) C. difficile ribotype 001 had reduced susceptibility to metronidazole (geometric mean SGE MICs 3.51 mg/L, P < 0.001)
• Increased metronidazole MICs were confirmed by an agar incorporation method

12/10/2011
16
Rifampin Resistance by EtestCurry SR, Clin Infect Dis 2009; 48:425-9
• 470 C. difficile isolates – 51.1% during 2001–2002 and 48.9% during 2005)
from a large US teaching hospital– Rifampin sensitivity by Etest
• Rifampin resistance:– In 173 (36.8%) of 470 recovered isolates– In 167 (81.5%) of 205 epidemic clone isolates
• � Resistance common• � Previous exposure significant
Tolevamer Phase III Trial
*Severe + ≥10 bowel movements/d; WBC ≥20,000, or severe abdominal pain.**P < .05
Vancomycin Metronidazole
Response rate 109/133 (82%) 103/143 (72%)
Mild 23/27 (85%) 26/33 (79%)
Moderate 58/73 (80%) 40/53 (75%)
Severe* 28/33 (85%) 37/57 (65%)**
Relapse rate 27/103 (23%) 29/100 (29%)
Louie T, et al. ICAAC 2007. Abstract 3826.
12/10/2011
17
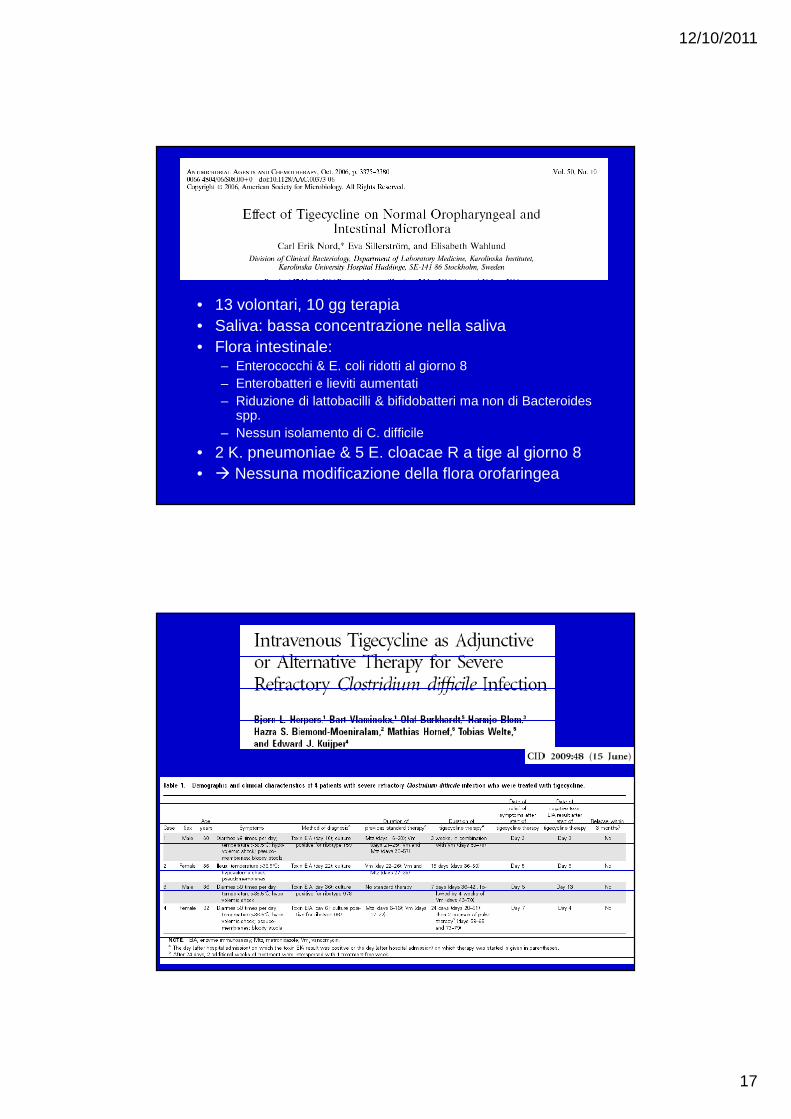
• 13 volontari, 10 gg terapia• Saliva: bassa concentrazione nella saliva• Flora intestinale:
– Enterococchi & E. coli ridotti al giorno 8– Enterobatteri e lieviti aumentati– Riduzione di lattobacilli & bifidobatteri ma non di Bacteroides
spp.– Nessun isolamento di C. difficile
• 2 K. pneumoniae & 5 E. cloacae R a tige al giorno 8• � Nessuna modificazione della flora orofaringea

12/10/2011
18

12/10/2011
19


















