Principi di sintesi organica – Anno Accademico 2008-2009 1 Principi di sintesi organica parte 1.

of 7
Upload
henry-paredesCategory
view
213download
08/18/2019 Bron Qui Ol It is Principi 2016
1/7
Copyright 2016 American Medical Association. All rig hts reserved.
EffectofOxygen Desaturations onSubsequentMedical Visits
in Infants DischargedFrom the Emergency Department
WithBronchiolitis
Tania Principi,MD, FRCPC,MSc;AllanL. Coates, MD;Patricia C. Parkin, MD, FRCPC;Derek Stephens,MSc;
ZeliaDaSilva,RT; Suzanne Schuh, MD,FRCPC
IMPORTANCE Reliance on pulse oximetry has been associated with increased hospitalizations,
prolonged hospital stay, and escalation of care.
OBJECTIVE To examine whether there is a difference in theproportion of unscheduled
medical visitswithin 72 hours of emergencydepartment dischargein infants with
bronchiolitis whohave oxygen desaturations to lower than 90%for at least 1 minuteduring
home oximetry monitoring vs those without desaturations.
DESIGN, SETTING, AND PARTICIPANTS Prospective cohort study conducted from February 6,
2008,to April 30, 2013,at a tertiary care pediatric emergencydepartment in Toronto,Ontario, Canada, among118 otherwise healthy infants aged 6 weeks to 12 monthsdischarged
home from theemergency department with a diagnosisof acute bronchiolitis.
MAINOUTCOMES AND MEASURES The primary outcome was unscheduledmedical visits for
bronchiolitis, includinga visit to any healthcare professional due to concerns about
respiratory symptoms,within 72 hours of discharge in infants with and without
desaturations. Secondary outcomes included examination of the severity and duration of the
desaturations, delayed hospitalizations within 72 hours of discharge,and the effect of activity
on desaturations.
RESULTS A totalof 118infantswere included (mean [SD] age, 4.5 [2.1] months; 69 male
[58%]). During a mean (SD) monitoring periodof 19 hours 57 minutes (10hours37 minutes),
75 of 118infants(64%) hadat least 1 desaturationevent(median continuous duration,3 minutes 22 seconds; interquartile range,1 minute54 seconds to 8 minutes 50 seconds).
Among the 118 infants,59 (50%) hadat least 3 desaturations, 12 (10%) haddesaturation for
more than 10%of themonitored time, and51 (43%)had desaturations lasting 3 or more
minutes continuously. Of the75 infants whohad desaturations, 59 (79%) haddesaturation to
80% orlessfor atleast 1 minute and 29 (39%) had desaturationto 70% or lessfor atleast
1 minute. Of the75 infants with desaturations, 18 (24%) hadan unscheduled visit for
bronchiolitisas compared with 11 of the 43 infants without desaturation (26%) (difference,
−1.6%; 95% CI,−0.15 to ; P = .66).One of the75 infants with desaturations (1%) and2 of the
43 infants without desaturations (5%)were hospitalized within 72 hours (difference, −3.3%;
95% CI,−0.04 to 0.10;P = .27). Among the62 infants with desaturations whohad diary
information,48 (77%) experienced them duringsleepor while feeding.
CONCLUSIONS AND RELEVANCE The majority of infants with mild bronchiolitisexperienced
recurrent or sustained desaturations after discharge home. Children with and without
desaturations hadcomparable rates of returnfor care, with no difference in unscheduled
return medical visits and delayed hospitalizations.
JAMAPediatr . doi:10.1001/jamapediatrics.2016.0114
Published onlineFebruary29, 2016.
Editorial
AuthorAudioInterviewat
jamapediatrics.com
Author Affiliations: Research
Institute,The Hospital for SickChildren, Toronto, Ontario, Canada
(Principi, Coates, Parkin, Stephens,
Schuh); Departmentof Pediatrics,
TheHospital for SickChildren,
Toronto,Ontario,Canada (Principi,
Parkin, DaSilva, Schuh).
Corresponding Author: Suzanne
Schuh, MD,FRCPC, Departmentof
Pediatrics, TheHospital for Sick
Children, 555 UniversityAve,
Toronto,ON M5G 1X8,Canada
Research
Original Investigation
(Reprinted) E1
Copyright 2016 American Medical Association. All rig hts reserved.
wnloaded From: http://archpedi.jamanetwork.com/ by a GAZI UNIVERSITESI User on 03/01/2016
http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0090&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114mailto:[email protected]:[email protected]:[email protected]:[email protected]://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0090&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114
8/18/2019 Bron Qui Ol It is Principi 2016
2/7
Copyright 2016 American Medical Association. All rig hts reserved.
Bronchiolitis is themost commonlowerrespiratory tract
infectionamong infants, characterized by wheeze and
respiratory distress. To date, the benefit of pharma-
cotherapy in the treatment of bronchiolitishas notbeen dem-
onstrated, and adequate hydration and oxygenation consti-
tuteimportant disposition criteria forthisdisease.-Following
the introduction of routine oximetry in the s, thehospi-
talization ratefor bronchiolitisrose from . per to .
per . Experts feel that this increase in hospital admis-
sions may have happened owing to a high reliance on
oximetry.- Currently, bronchiolitis represents the leading
cause of infant hospitalizations in theUnited States, at an es-
timated annual cost of $. billion.
The recent American Academy of Pediatrics bronchiolitis
guideline suggests that physicians may choose not to admin-
ister supplemental oxygen to children with oxygen satura-
tions of %and greater. However,the criteriafor using oxy-
gen therapy vary widely,,, without evidence that oxygen
saturations predict diseaseprogression. Indeed, pulse oxim-
etry in bronchiolitis is sometimes used as a proxy for illness
severity despite poorcorrelationbetween theseparameters.
This focus on and credence given to oximetry may in part re-
late to lackof evidence on the natural history of desaturations
in bronchiolitis, which are often transient, self-resolving,
and frequently not accompanied by increased respiratory
distress.
Transient desaturationsoccur in young healthy infants,
especially during sleep, and may also occur in infants with
mild bronchiolitis at home. Although it is known that many
infants with bronchiolitis remainin thehospitalowing to de-
saturations whenotherclinical discharge criteriaare met,no
studyto ourknowledgehas investigateddesaturationsin bron-
chiolitis after discharge home from the emergency depart-
ment (ED) and theireffect onuse of healthcareresources. De-
saturations occurring in infants with mild bronchiolitis in anED often resultin hospitalizations or prolonged hospital stay.
Information on the frequency, severity, and effect of desatu-
rationsin infantswith mildbronchiolitiswill helpto shedlight
on the natural course of bronchiolitis and may provide a bet-
ter perspective on the clinical significance of these events.
The primary objective of this study of infants with acute
bronchiolitis was to determine whether there is a difference
in the proportion of unscheduled medical visits within
hours of ED discharge in infants with desaturations to less
than % for at least minute during home oximetry moni-
toring vs those without desaturations. Secondary objectives
were to describe the duration and frequency of the desatura-
tions and to examine the association between desaturationsand both all-cause medical visits within hours and
delayed hospitalizations.
Methods
StudyDesignandPopulation
This was a prospective cohort study comparing outcomes of
infants discharged home with acute bronchiolitis from a ter-
tiary care pediatric ED between February , , and April
, . We included previously healthy infants aged
weeks to months diagnosed as having bronchiolitis,
defined as the first episode of respiratory distress with
coryza, cough, wheezing or crackles, and tachypnea or chest
retractions. Children with cardiopulmonary, neuromuscu-
lar, immunologic, hematologic, or airway anomalies, prema-
turity with weeks’ gestation or less, or known chronic
hypoxia were excluded, as were those needing inpatient care
and those with poor command of the English language. Writ-
ten informed consent was obtained from all participating
families. The Hospital for Sick Children Research Ethics
Board approved the study.
StudyProcedure
Infants diagnosed as having acutebronchiolitis aboutto be dis-
charged home from theED, without the need forsupplemen-
taloxygen,werescreened foreligibility andapproachedfor en-
rollment by trained research nurses on duty between noon
and midnight daysperweek. Theymaintained a logof all po-
tentiallyeligiblechildren. A structured datacollectionform wasused to document presenting demographic and clinical para-
meters. Six portable oxygen saturation monitors (Radical-;
Masimo Corp) were used for home monitoring.
Prior todischargehome,thestudynurses appliedthe satu-
ration probe to a foot of theparticipating infants andsecured
itspositionwitha self-adherent wrap andsockto minimize the
possibility of displacement. Parents were asked to keep the
monitor connected to an electrical outlet whenever possible
to avoid battery drainand instructed to avoid submerging the
infant’s foot in water. Because the standard of home care in
childrenwith bronchiolitisdoes notincludeoximetry, thestudy
monitor threshold alarms and the display of saturation val-
ues were turned off. We did use an alarm for probe dislodg-ment and instructed caretakers in how to reapply the probe.
The caretakerswerealso askedto fill outa brief diary, with in-
formation regarding the timeof sleeping,feeding, or sittingin
a car seat.
Follow-up
The study monitors and diaries were collected from patients’
homes by a courier service anddelivered to ourhospital’s de-
partmentof respiratory therapy for dataanalysis. Using stan-
dard interviewingtechniques, thestudynurses,blindedto the
KeyPoints
Question: Is there a difference in unscheduled medical visits
within 72 hoursof emergency departmentdischarge in infants
with bronchiolitis withvs without desaturations during home
oximetry monitoring?
Findings: In this cohortstudyof 118infants, 64% ofinfants hadat
least1 desaturation event. Unscheduled medical visitsoccurred in
24%of infants with desaturations vs 26%withoutdesaturations,
a nonsignificant difference.
Meaning:Themajorityof infants withmild bronchiolitis
experience desaturations afterdischarge home. Desaturations
do notpredictthe need for additional medical visits.
Research Original Investigation Oxygen Desaturations AfterDischargeof Infants WithBronchiolitis
E 2 JA MA P ed iat ri cs Published onlineFebruary 29,2016 (Reprinted) jamapediatrics.com
Copyright 2016 American Medical Association. All rig hts reserved.
wnloaded From: http://archpedi.jamanetwork.com/ by a GAZI UNIVERSITESI User on 03/01/2016
http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114
8/18/2019 Bron Qui Ol It is Principi 2016
3/7
Copyright 2016 American Medical Association. All rig hts reserved.
oximetry results, conducted telephone follow-up of all par-
ticipants hours after discharge to identify unscheduled
medical visits for bronchiolitis and delayed hospitalizations.
Definitions
Desaturationswere definedas atleast documenteddesatura-
tionto lessthan% lasting minuteor more. Major desatura-
tions were definedas thefollowing:recurrent, ie,consisting of
atleastdesaturationstolessthan%foratleastminute;pro-
longed, ie,saturationsof less than % for%or more of the
monitored time; or sustained, ie, saturations of lessthan %
lasting or moreminutes continuously. Unscheduledmedical
visit was defined as a visit to any health care professional due
toconcernabout respiratorysymptoms. Tofurther evaluate dif-
ferencesin oxygensaturationsbetween the cohorts, a cumu-
lative hypoxemia score was calculated based on the following
previouslypublished formula withminor modification to fit
our data capture method: [(percentage of recording time with
oxygen saturation of % to %) × .] + [(percentage of re-
cording time with oxygen saturation of % or less) × ].
OutcomeMeasuresThe oxygen saturation data were downloaded and analyzed
from the study monitors using specialized software(PROFOX
Oximetry Software; PROFOX Associates, Inc). This software
wascustomizedby PROFOX Associates,Inc to capturethe key
datapointsfor desaturationeventsas defined in thisstudy. This
provided accurateand consistent analysisof the downloaded
data and generated a comprehensive report for each patient.
ThePROFOXsoftwaretechnology also allowed forthe analy-
sisof only valid sampling, excluding any artifactsor poor sig-
nal. This software eliminatesartifacts and distinguishes poor
tracingsfrom true desaturations. The PROFOX technology has
beenusedclinically around the worldand was alsousedin sev-
eral researchstudies.
The respiratory therapistwas blindedto the infants’ outcome and the software independently de-
termined whether there wasa desaturation event, ie,oxygen
saturation less than % for at least minute. The compre-
hensive report also included the number of desaturation
events, duration of desaturation, mean oxygen saturation,
and percentage of time spent with saturations between %
and % as well as less than %.
In keeping with the aforementioned definitions, partici-
pants were divided into those with desaturations and those
without as well as those with major desaturations and those
without. The primary outcome measure was an unscheduled
medical visit for bronchiolitis within hours of discharge in
infants withand without desaturations.
,
Thesecondaryout-comes werethe following: ()to describethe durationand fre-
quency of desaturations; () to examine the association be-
tween desaturations and all-cause medical visits within
hours, delayed hospitalizations, and infant activity such as
sleepingand feeding;and () to determinethe association be-
tweenmajor desaturationsand unscheduled medical visits. We
also investigated the association between desaturation and
plausible predictors thereof such as age, duration of respira-
torydistress,previous visits forbronchiolitis,history of atopy,
estimated feeding less than % of the usual amount, pre-
senting ED oxygen saturation, Respiratory Disease Assess-
ment Instrument severity level at discharge from theED, and
the useof inhaled epinephrine in the ED.The Respiratory Dis-
ease Assessment Instrument (range of possible scores, -)
is used in bronchiolitis studies to quantify the degree of re-
spiratoryabnormality by using severityof chest retractionsand
wheezing. Exploratory outcomes included a determination
of the cumulative hypoxemia score and mean oxygen satu-
ration in infants with desaturations and those without.
Sample Size
The sample size was estimated to provide % power for a
targeted % difference in the primary outcome between
the groups. Based on previous literature, we have estimated
the overall proportion of bronchiolitis revisits at %.
Assuming revisit rates of % and % in infants with vs
without desaturation, respectively, and further estimating
that % of infants with bronchiolitis have desaturation dur-
ing sleep, we estimated a sample size requirement of
approximately analyzable patients, with experiencing
desaturations and not.
StatisticalAnalysis
A statistician blinded to the study hypothesis carried out the
analysis using SAS version . statistical software (SAS Insti-
tute, Inc). Becausethe primary hypothesis was-sided(ie, do
infantswith desaturationexperiencemore revisitsthan those
without desaturation?), the difference in the primary out-
comebetween thegroupswas comparedusingthe -sidedun-
adjusted Fisher exacttest. All otheranalyseswere -tailed. The
Fisherexact test wasalso used to detect the difference in all-
causemedical visitsandhospitalizationsin the groupsas well
as forthe calculationof thedifferenceintheunscheduledmedi-
cal visits in infantswith andwithoutmajor desaturations. The
relevant% confidence intervalswere determined. Univari-ate analysis was used to identify patient characteristics to be
included in the multiple logistic regression, which deter-
mined whether there was a significant independent associa-
tion between unscheduled visits for bronchiolitis as a depen-
dent variable and the aforementioned plausible predictors
thereof. Clinicallysignificant,uncorrelated variables with uni-
variate P < . were included in thefinalmodel. Toselect the
final model, α = . was used for statistical significance.
Results
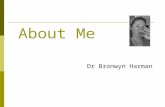
Duringthe study period, patients were screened, metenrollment criteria,and were enrolled inthe study(Figure).
A total of patients presented outside the study hours and
were missed. Most refusals occurred because of a lack of
interest in research;some parents felthomemonitoring would
incur too much inconvenience. The mean (SD) age of the in-
cluded childrenwas comparable with that of those whowere
missedand thosewho refused participation(.[.], .[.],
and . [.] months, respectively). Of the patients who
agreed to participate, had both successful follow-up and
oximetry records and participants had diary data.
Oxygen Desaturations After Discharge of Infants WithBronchiolitis Original Investigation Research
jamapediatrics.com (Reprinted) JAMA Pediatrics Published onlineFebruary 29, 2016 E3
Copyright 2016 American Medical Association. All rig hts reserved.
wnloaded From: http://archpedi.jamanetwork.com/ by a GAZI UNIVERSITESI User on 03/01/2016
http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114
8/18/2019 Bron Qui Ol It is Principi 2016
4/7
Copyright 2016 American Medical Association. All rig hts reserved.
Among the infants included in the analysis ( male
[%]), the infants with andwithout desaturations had com-
parablecharacteristics, withthe exceptionof morepriormedi-
cal visits in the group with desaturations (Table ). However,
this difference was not significant when adjusted for mul-
tiple comparisons. Overall, the mean (SD) monitoring pe-
riod was hours minutes( hours minutes). The mean
duration of monitoring was . hours (% CI, .-.) in
children with desaturations and . hours (% CI, .-
.) in those without desaturations ( P = .).
PrimaryOutcomeOf the infants, (%) had unscheduled medical visits
for bronchiolitis within hours of the index ED visit: re-
turned to their primary care physician, visited an ED, and
both saw their primary care physician and visitedan ED. Ten
of the returninginfants (%) received additional medica-
tion: received albuterol, received inhaled corticosteroids,
received oralcorticosteroids, received antibiotics,and re-
ceived inhaled epinephrine. Among the infants, (%)
had at least desaturation to less than % lasting minute
or longerand (%) had no desaturations.Of the infants
with desaturations, (%) spent more than minute with
oxygensaturationsof %or lessand (%) spent morethan
minute with oxygen saturations of % or less. The median
continuous desaturation lasted minutes seconds (inter-
quartile range[IQR], minute seconds to minutes sec-
onds) andthe median percentage of monitoredtime spent with
oxygen saturations below % was .% (IQR, .%-.%).
There were infantswith unscheduled medical visits for
bronchiolitis symptoms among the infants with desatura-
Figure. Enrollment of PatientsInto theStudy
1019 Patients screened
139 Enrolled
118 Analyzed
880 Excluded671 Did not meet eligibility criteria
154 Comorbidities
145 Previous wheeze
26 Did not speak English
18 Admitted to hospital
5 Previously enrolled
3 Outside catchment area
2 Did not meet age criteria
1 No telephone
7 Other/unknown
209 Refused to participate
310 Did not meet definitionof bronchiolitis
10 Lost to follow-up
10 Had no oximetry data
1 Admitted before leavingemergency department
Table 1.DemographicandClinicalCharacteristics of theParticipatingInfantsa
CharacteristicDesaturation(n = 75)
No Desaturation(n = 43) Difference (95% CI)
Age, mean (SD), mo 4.6 (2.3) 4.4 (2.1) 0.2 (−0.66 to 1.02)
Male, No. (%) 41 (55) 28 (65) −10 (−0.29 to 0.08)
Temperature ≥38°C within 48 h, No. (%) 44 (59) 28 (65) −6 (−0.25 to 0.12)
History of atopy, No. (%) 57 (77) 33 (77) 0 (−0.16 to 0.16)
Family history of atopy, No. (%) 36 (48) 26 (60) −12 (−0.31 to 0.06)
Duration of respiratory distress,mean (SD), h
49 (33) 49 (77) 0 (−20.5 to 20.3)
Previous medical visit, No. (%) 52 (70) 21 (49) 21 (0.02 to 0.39)
Feeding
8/18/2019 Bron Qui Ol It is Principi 2016
5/7
Copyright 2016 American Medical Association. All rig hts reserved.
tions (%) vs returning infants among the without de-
saturations(%)(difference, −.%;% CI,−.to; P = .)
(Table ).
SecondaryOutcomes
All-cause medical visits within hours of enrollment were
made by of the infantswith desaturations(%)vs of
the infants withoutdesaturations (%) (difference, −.%;
% CI, −. to .; P = .). One of the infants with de-
saturations (%) and of the without desaturations (%)
werehospitalizedwithin hours (difference, −.%; %CI,
−. to .; P = .) (Table ).
Among the participating infants, (%) experi-
enced major desaturations at home; infants (%) had re-
current desaturations, (%) had prolonged desaturations,
and (%) had sustained desaturations. Unscheduled medi-
cal visits for bronchiolitis symptoms were made by of the
infants with major desaturations (%) as compared with
of the infants without major desaturations (%) (dif-
ference, −.%; %CI, −.to .; P = .). Themediancu-
mulative hypoxemic score was . (IQR, . to .) in in-
fants with desaturations and . (IQR, . to .) in thosewithout desaturations (difference, .; % CI, . to .;
P < .). An increasein thecumulative hypoxemicscore was
not associated withincreasedunscheduledmedical visits (rela-
tive risk = ; P = .).
Based on the univariate analysis, the following variables
were included in the multivariate regression: family history
of atopy, previous medical visit,feeding less than % of the
usual amount, and the use of inhaled epinephrine in the ED.
The multivariable regression analysis showed the previous
medical visits to be independently associated with desatura-
tion (odds ratio = .; % CI, .-.; P = .). Of the in-
fants with desaturations, (%) had diary information. Of
these infants, (%) experienced desaturations duringsleep or while feeding.
Discussion
Our study shows that the majority of infants with mild bron-
chiolitisexperienced recurrent or sustained desaturationsaf-
ter discharge home.Children with and without desaturations
hadcomparable rates of returnfor care, with no difference in
unscheduled return medical visits and delayed hospitaliza-
tions within hours. These findings challenge the concept
that infants with desaturations were sicker and suggest that
pulse oximetryis notan effectivetool topredict morbiditylead-
ing to escalated return for care.
Bronchiolitis occurs in young infants who are subject to
numerous age-related physiological factors that make this
population hypoxia prone. Episodic hypoxia with saturation
nadirs as low as % to % have been previously docu-
mented in healthy young infants.,Sleeping state, feeding,
sitting in a car seat, and air travel augment the probability of
desaturations, ,- and the first factors also proved to be
true in this study.
Oxygen saturation is routinely used for assessment of
bronchiolitis, often with an expectation that an oximetry
readingrepresents a keyindicator of a child’s healthandiden-
tifieschildrenat riskfor deterioration.However, to datethere
is no informationabout howdesaturations, which occur with-
out a change in respiratory status yet are severe and long
enough to trigger monitor alarms, affect outcomes. Typi-
cally, oximeter alarmsare preset at saturationthresholds in the
vicinity of %. If the saturation reading reaches below this
threshold, the intensity of monitoring is frequently escalatedand supplemental oxygen therapy begun. To accommodate
practice variation in oximetry interpretation-andgiventhe
lackof evidenceas totheoptimalsaturation threshold onwhich
to act,the latestAmericanAcademy of Pediatrics guideline in-
cludes an option not to initiateoxygen therapyin infantswith
saturation of %or greater. Perceived needfor supplemen-
taloxygenin bronchiolitis is reported asthe sole reasonforhos-
pitalization, prolongation of hospital stay, delay in discharge
from observation units, and use of oxygen after discharge
home.,,- The results of this study suggest that infants
withbronchiolitis whoaredeemedsuitablefor dischargehome
from a respiratoryand hydration pointof view should notun-
dergo further oximetry measurements. Thisopinionhas beenexpressed in a recent editorial on the frequency of oximetry
monitoring in bronchiolitis that points out that well-
hydrated infants withbronchiolitisand saturationsof %or
greater shouldgo home and notbe monitored further. Are-
centmultisite randomized trial of continuous vs intermittent
oximetry concludedthat intermittentmonitoring can be rou-
tinely considered in stable inpatients with bronchiolitis, ow-
ing to lackof associated escalation of care,diagnostic testing,
or respiratory interventions. One advantage of spot check-
ing is that this approach is less likely to detect transient de-
Table2.Outcomesof InfantsWith andWithoutDesaturation
OutcomeDesaturation(n = 75)
No Desaturation(n = 43) Difference (95% CI)a
Primary
Unscheduled medical visits, No. (%) 18 (24) 11 (26) −1.6 (−0.15 to )
Secondary
All-cause medical visits, No. (%) 24 (32) 16 (37) −5.2 (−0.13 to 0.23)
Hospitalizations, No. (%) 1 (1) 2 (5) −3.3 (−0.04 to 0.10)
Exploratory
Cumulative hypoxemic score,median (IQR)
10.7 (2.7 to 22.6) 0.5 (0.25 to 0.75) 10.2 (6.6 to 13.8)
Abbreviation:IQR, interquartile
range.
a
Differences are expressedasdifferencein percentages where
appropriate and as difference in
medians for valuesnot expressed
as percentages.
Oxygen Desaturations After Discharge of Infants WithBronchiolitis Original Investigation Research
jamapediatrics.com (Reprinted) JAMA Pediatrics Published onlineFebruary 29, 2016 E5
Copyright 2016 American Medical Association. All rig hts reserved.
wnloaded From: http://archpedi.jamanetwork.com/ by a GAZI UNIVERSITESI User on 03/01/2016
http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114
8/18/2019 Bron Qui Ol It is Principi 2016
6/7
Copyright 2016 American Medical Association. All rig hts reserved.
saturations of questionable significance. The results of our
study underscore the conclusion of the aforementioned trial
that thedesaturations missed by intermittentoximetry moni-
toring are likely clinically unimportant in the context of sat-
isfactory clinicalstatus.Of note, many of ourparticipantswith
desaturations would have undergone significant medical in-
terventions if they had been in a hospital monitoring setting.
Our definition of a desaturation event may be perceived
as arbitrary because it was based on expert opinion and ob-
served practice of interpreting oximetry results for escala-
tion of c are. Nevertheless, we have also demonstrated a lack
of association between the hypoxemic index in our popula-
tion andboth unscheduled returnmedical visitsand delayed
hospitalizations, which strengthens the study result. An-
other limitation of ourstudy is the lack of informationon out-
comes beyond hours.It is therefore possible that somechil-
dren required return for care after this time. However, most
escalation of bronchiolitismanagementhappens within theini-
tialfew daysfollowingED discharge.Althoughwe cannot gen-
eralize our study results to the inpatient population, many
stable infants with mild to moderate bronchiolitis are ob-
servedand monitoredin theED setting prior todischarge.Such
infants with self-resolving desaturations should not be sub-
jected to unnecessary medical interventions. The results of
this study also do notapplyto infants with chronic desatura-
tionsdue to chronic respiratory conditions. Theeffect of brief
hypoxia on the developing brainis not wellcharacterized and
is well beyondthe scope of this study. While chronic hypoxia
in infants andlow sleepsaturationin school-aged childrenhave
been linked to suboptimal academic performance, there is
no evidence that transient desaturations during acute bron-
chiolitis are associated with adverse outcomes.
Conclusions
Themajority of infantswithmild bronchiolitis experienced re-
currentor sustained desaturations after discharge home. Chil-
drenwith and without desaturationshad comparable rates of
return forcare,with no differencein unscheduled return medi-
cal visits and delayed hospitalizations. Pulse oximetry is not
an effective tool to predict subsequent return for care.
ARTICLE INFORMATION
Accepted for Publication: January 5, 2016.
Published Online: February 29,2016.
doi:10.1001/jamapediatrics.2016.0114.
Author Contributions: Dr Principi hadfull accessto
allof thedatain thestudy andtakes responsibility
forthe integrityof thedataand theaccuracyof the
data analysis.
Study concept and design: Principi, Coates, Parkin,
Schuh.
Acquisition, analysis, or interpretation of data: All
authors.
Drafting of themanuscript:Principi, Coates, Schuh.
Critical revision of themanuscriptfor important
intellectual content: All authors.
Statistical analysis: Stephens.
Obtained funding: Principi, Schuh.
Administrative, technical, or material support:
Principi, DaSilva, Schuh.
Study supervision: Principi, Schuh.
Conflict of Interest Disclosures: Nonereported.
Funding/Support: This studywas supported bythe
Physician’s Services IncorporatedFoundation and
the Canadian Association of Emergency Physicians.
Roleof the Funder/Sponsor:Thefundershad no
rolein thedesign andconductof thestudy;
collection, management,analysis,and
interpretation of the data;preparation, review, or
approval of themanuscript; anddecisionto submit
the manuscriptfor publication.
REFERENCES
1. StangP,Brandenburg N,CarterB. The economic
burdenof respiratory syncytial virus-associated
bronchiolitis hospitalizations. Arch Pediatr Adolesc
Med . 2001;155(1):95-96.
2. PlintAC, Johnson DW, Patel H,et al;Pediatric
Emergency Research Canada(PERC). Epinephrine
and dexamethasonein children withbronchiolitis.
N EnglJ Med . 2009;360(20):2079-2089.
3. SmythRL, Openshaw PJ. Bronchiolitis. Lancet .
2006;368(9532):312-322.
4. AmericanAcademyof Pediatrics Subcommittee
on Diagnosis and Managementof Bronchiolitis.
Diagnosis and management of bronchiolitis.
Pediatrics. 2006;118(4):1774-1793.
5. Scottish Intercollegiate GuidelinesNetwork.
Bronchiolitisin children: a national clinical
guideline. http://www.sign.ac.uk/pdf/sign91.pdf.
Accessed July14, 2014.
6. BarbenJ, KuehniCE, Trachsel D,Hammer J;
SwissPaediatric RespiratoryResearchGroup.
Management of acutebronchiolitis: can evidence
basedguidelinesalter clinical practice? Thorax .
2008;63(12):1103-1109.
7. Corneli HM,ZorcJJ,Mahajan P, etal;
BronchiolitisStudy Group of the Pediatric
EmergencyCare AppliedResearchNetwork
(PECARN).A multicenter,randomized, controlled
trial of dexamethasonefor bronchiolitis.NEngl JMed .
2007;357(4):331-339.
8. Ralston SL,Lieberthal AS,Meissner HC,et al;
American Academy of Pediatrics.Clinical practice
guideline:the diagnosis, management, and
preventionof bronchiolitis. Pediatrics. 2014;134(5):
e1474-e1502.
9. Shay DK,Holman RC,NewmanRD, LiuLL,
StoutJW, Anderson LJ.Bronchiolitis-associated
hospitalizations amongUS children, 1980-1996.
JAMA. 1999;282(15):1440-1446.
10. LangleyJM, LeBlanc JC,SmithB, WangEE.
Increasingincidenceof hospitalization for
bronchiolitisamong Canadian children,
1980-2000. J Infect Dis. 2003;188(11):1764-1767.
11. MalloryMD,ShayDK, Garrett J,Bordley WC.
Bronchiolitismanagement preferencesand the
influenceof pulse oximetry andrespiratoryrate on
thedecision to admit. Pediatrics. 2003;111(1):e45-e51.
12. SchuhS, FreedmanS, Coates A, etal. Effect
of oximetry on hospitalization in bronchiolitis:
a randomizedclinical trial. JAMA. 2014;312(7):
712-718.
13. Hasegawa K, TsugawaY, BrownDF, Mansbach
JM, Camargo CA Jr.Trendsin bronchiolitis
hospitalizations in the United States, 2000-2009.
Pediatrics. 2013;132(1):28-36.
14. ZorcJJ, Hall CB. Bronchiolitis: recent evidence
on diagnosis and management. Pediatrics. 2010;125
(2):342-349.
15. Wang EE,Law BJ, BoucherFD, etal. Pediatric
Investigators CollaborativeNetworkon Infections
in Canada(PICNIC)studyof admission and
management variation in patients hospitalizedwith
respiratory syncytial virallower respiratory tract
infection. J Pediatr . 1996;129(3):390-395.
16. Hunt CE,CorwinMJ,Lister G,et al;
CollaborativeHome Infant MonitoringEvaluation
(CHIME) StudyGroup. Longitudinal assessmentof
hemoglobinoxygen saturationin healthy infants
duringthe first 6 monthsof age. J Pediatr . 1999;135
(5):580-586.
17. MokJY, McLaughlinFJ, PintarM, HakH,
Amaro-GalvezR, Levison H. Transcutaneous
monitoring of oxygenation: whatis normal? J Pediatr .
1986;108(3):365-371.
18. SchroederAR, MarmorAK, Pantell RH,
NewmanTB. Impactof pulseoximetryand oxygen
therapy on lengthof stay in bronchiolitis
hospitalizations. Arch Pediatr Adolesc Med . 2004;
158(6):527-530.
19. KaditisAG,Katsouli G,Malakasioti G,KaffeK,
Gemou-EngesaethV, AlexopoulosEI. Infants with
viral bronchiolitisdemonstrate two distinct
patterns of nocturnal oxyhaemoglobin
desaturation. Acta Paediatr . 2015;104(3):
e106-e111.
20. DawsonJA, KamlinCO, VentoM, etal.
Defining the reference rangefor oxygen saturation
forinfantsafterbirth.Pediatrics. 2010;125(6):
e1340-e1347.
21. Norwood A, MansbachJM, Clark S,Waseem M,
Camargo CA Jr.Prospective multicenterstudy of
bronchiolitis: predictors of an unscheduledvisit
afterdischarge from the emergencydepartment.
Acad EmergMed . 2010;17(4):376-382.
Research Original Investigation Oxygen Desaturations AfterDischargeof Infants WithBronchiolitis
E 6 JA MA P ed ia tric s Published onlineFebruary 29,2016 (Reprinted) jamapediatrics.com
Copyright 2016 American Medical Association. All rig hts reserved.
wnloaded From: http://archpedi.jamanetwork.com/ by a GAZI UNIVERSITESI User on 03/01/2016
http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.ncbi.nlm.nih.gov/pubmed/11177073http://www.ncbi.nlm.nih.gov/pubmed/11177073http://www.ncbi.nlm.nih.gov/pubmed/11177073http://www.ncbi.nlm.nih.gov/pubmed/11177073http://www.ncbi.nlm.nih.gov/pubmed/19439742http://www.ncbi.nlm.nih.gov/pubmed/19439742http://www.ncbi.nlm.nih.gov/pubmed/19439742http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/17015575http://www.ncbi.nlm.nih.gov/pubmed/17015575http://www.ncbi.nlm.nih.gov/pubmed/17015575http://www.sign.ac.uk/pdf/sign91.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/10535434http://www.ncbi.nlm.nih.gov/pubmed/10535434http://www.ncbi.nlm.nih.gov/pubmed/10535434http://www.ncbi.nlm.nih.gov/pubmed/14639549http://www.ncbi.nlm.nih.gov/pubmed/14639549http://www.ncbi.nlm.nih.gov/pubmed/14639549http://www.ncbi.nlm.nih.gov/pubmed/12509594http://www.ncbi.nlm.nih.gov/pubmed/12509594http://www.ncbi.nlm.nih.gov/pubmed/12509594http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/23733801http://www.ncbi.nlm.nih.gov/pubmed/23733801http://www.ncbi.nlm.nih.gov/pubmed/23733801http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/8804328http://www.ncbi.nlm.nih.gov/pubmed/8804328http://www.ncbi.nlm.nih.gov/pubmed/8804328http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/20370776http://www.ncbi.nlm.nih.gov/pubmed/20370776http://www.ncbi.nlm.nih.gov/pubmed/20370776http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.ncbi.nlm.nih.gov/pubmed/20370776http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/20439604http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/25492521http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/15184214http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/3950817http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/10547246http://www.ncbi.nlm.nih.gov/pubmed/8804328http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/20100768http://www.ncbi.nlm.nih.gov/pubmed/23733801http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/25138332http://www.ncbi.nlm.nih.gov/pubmed/12509594http://www.ncbi.nlm.nih.gov/pubmed/14639549http://www.ncbi.nlm.nih.gov/pubmed/10535434http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/25349312http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/17652648http://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.ncbi.nlm.nih.gov/pubmed/18723582http://www.sign.ac.uk/pdf/sign91.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/17015575http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/16860701http://www.ncbi.nlm.nih.gov/pubmed/19439742http://www.ncbi.nlm.nih.gov/pubmed/11177073http://www.ncbi.nlm.nih.gov/pubmed/11177073http://jama.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0114&utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114
8/18/2019 Bron Qui Ol It is Principi 2016
7/7
Copyright 2016 American Medical Association. All rig hts reserved.
22. Lowell DI,Lister G,Von Koss H, McCarthyP.
Wheezing in infants: the response to epinephrine.
Pediatrics. 1987;79(6):939-945.
23. PlintAC, Johnson DW, WiebeN, etal. Practice
variation amongpediatricemergencydepartments
in the treatmentof bronchiolitis. Acad Emerg Med .
2004;11(4):353-360.
24. McLaughlinMJ, Sainani KL. Bonferroni,Holm,
and Hochberg corrections:fun names, serious
changes top values. PM R. 2014;6(6):544-546.
25. American Thoracic Society.Cardiorespiratory
sleepstudies in children:establishment of
normative data and polysomnographicpredictors
of morbidity. Am J Respir Crit Care Med . 1999;160
(4):1381-1387.
26. Udomittipong K, StickSM, Verheggen M,
Oostryck J,Sly PD, Hall GL.Pre-flighttestingof
preterm infants withneonatal lungdisease:
a retrospective review. Thorax . 2006;61(4):
343-347.
27. Samuels MP. Theeffectsof flightand altitude.
Arch Dis Child . 2004;89(5):448-455.
28. LeeAP,Yamamoto LG,Relles NL. Commercial
airlinetravel decreases oxygen saturation in
children. Pediatr EmergCare . 2002;18(2):78-80.
29. Mower WR,SachsC, Nicklin EL,SafaP,Baraff
LJ.Effect of routine emergencydepartmenttriage
pulseoximetry screeningon medical management.
Chest . 1995;108(5):1297-1302.
30. Cunningham S, McMurray A. Observational
study of twooxygensaturation targetsfor
discharge in bronchiolitis. Arch Dis Child . 2012;97
(4):361-363.
31. VoetsS, vanBerlaer G, Hachimi-Idrissi S.Clinical
predictors of the severity of bronchiolitis. Eur J EmergMed . 2006;13(3):134-138.
32. HallCB, PowellKR, MacDonaldNE, etal.
Respiratorysyncytialviral infection in children with
compromisedimmune function. N EnglJ Med .
1986;315(2):77-81.
33. HallCB, WeinbergGA, BlumkinAK, etal.
Respiratorysyncytialvirus-associated
hospitalizations amongchildren less than24
monthsof age. Pediatrics. 2013;132(2):e341-e348.
34. Shaw KN,Bell LM,ShermanNH. Outpatient
assessmentof infants withbronchiolitis. Am J Dis
Child . 1991;145(2):151-155.
35. Prescott WA Jr,Hutchinson DJ. Respiratory
syncytial virus prophylaxisin special populations:is
it somethingworth consideringin cystic fibrosis
and immunosuppression? J Pediatr Pharmacol Ther .
2011;16(2):77-86.
36. Unger S,Cunningham S.Effect of oxygen
supplementationon length of stayfor infants
hospitalized withacute viralbronchiolitis.Pediatrics.
2008;121(3):470-475.
37. Bajaj L, Turner CG,Bothner J.A randomized
trial of home oxygentherapyfrom theemergency
department for acutebronchiolitis. Pediatrics.
2006;117(3):633-640.
38. SandweissDR, CorneliHM, KadishHA. Barriers
to discharge froma 24-hour observation unit forchildren withbronchiolitis. Pediatr EmergCare .
2010;26(12):892-896.
39. Cunningham S. Intermittent monitoringof
oxygen saturationin infants and children withacute
bronchiolitis: peekaboo pediatrics or good clinical
care? JAMA Pediatr . 2015;169(10):891-892.
40. McCulloh R, KosterM, Ralston S,et al.Use of
intermittent vs continuous pulseoximetryfor
nonhypoxemic infants and youngchildren
hospitalizedfor bronchiolitis: a randomizedclinical
trial. JAMAPediatr . 2015;169(10):898-904.
41. Urschitz MS, Wolff J,SokollikC, et al.Nocturnal
arterial oxygen saturation and academic
performancein a communitysample of children.
Pediatrics. 2005;115(2):e204-e209.
Oxygen Desaturations After Discharge of Infants WithBronchiolitis Original Investigation Research
jamapediatrics.com (Reprinted) JAMA Pediatrics Published onlineFebruary 29, 2016 E7
Copyright 2016 American Medical Association. All rig hts reserved.
http://www.ncbi.nlm.nih.gov/pubmed/3295741http://www.ncbi.nlm.nih.gov/pubmed/3295741http://www.ncbi.nlm.nih.gov/pubmed/3295741http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/24769263http://www.ncbi.nlm.nih.gov/pubmed/24769263http://www.ncbi.nlm.nih.gov/pubmed/24769263http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/15102638http://www.ncbi.nlm.nih.gov/pubmed/15102638http://www.ncbi.nlm.nih.gov/pubmed/15102638http://www.ncbi.nlm.nih.gov/pubmed/11973496http://www.ncbi.nlm.nih.gov/pubmed/11973496http://www.ncbi.nlm.nih.gov/pubmed/11973496http://www.ncbi.nlm.nih.gov/pubmed/7587433http://www.ncbi.nlm.nih.gov/pubmed/7587433http://www.ncbi.nlm.nih.gov/pubmed/7587433http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/23878043http://www.ncbi.nlm.nih.gov/pubmed/23878043http://www.ncbi.nlm.nih.gov/pubmed/23878043http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/26322674http://www.ncbi.nlm.nih.gov/pubmed/26322674http://www.ncbi.nlm.nih.gov/pubmed/26322674http://www.ncbi.nlm.nih.gov/pubmed/26322819http://www.ncbi.nlm.nih.gov/pubmed/26322819http://www.ncbi.nlm.nih.gov/pubmed/26322819http://www.ncbi.nlm.nih.gov/pubmed/15653790http://www.ncbi.nlm.nih.gov/pubmed/15653790http://www.ncbi.nlm.nih.gov/pubmed/15653790http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.jamapediatrics.com/?utm_campaign=articlePDF%26utm_medium=articlePDFlink%26utm_source=articlePDF%26utm_content=jamapediatrics.2016.0114http://www.ncbi.nlm.nih.gov/pubmed/15653790http://www.ncbi.nlm.nih.gov/pubmed/26322819http://www.ncbi.nlm.nih.gov/pubmed/26322674http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/21088635http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/16510641http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/18310194http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/22477829http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/1994678http://www.ncbi.nlm.nih.gov/pubmed/23878043http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/3724802http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/16679876http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/21388970http://www.ncbi.nlm.nih.gov/pubmed/7587433http://www.ncbi.nlm.nih.gov/pubmed/11973496http://www.ncbi.nlm.nih.gov/pubmed/15102638http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/16449269http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/10508833http://www.ncbi.nlm.nih.gov/pubmed/24769263http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/15064208http://www.ncbi.nlm.nih.gov/pubmed/3295741